IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
|
|
|
- Suzan Parker
- 5 years ago
- Views:
Transcription
1 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer Practicum, Williamsburg, 2009
2 Learning Objectives for blunt abd.. Trauma General imaging considerations in abd.. trauma Features and grading of trauma to liver Findings often associated with liver trauma Features and grading of trauma to spleen Features and grading of trauma to pancreas
3 ROLE OF CT IN TRAUMA To guide management of patients To identify patients with internal injury To triage patients for emergent intervention: Surgery Interventional management (endovascular)
4 DEDICATED ABD. TRAUMA MDCT Contrast Materials: Oral contrast (if possible): 3 cups of 450 ml of 2.2% Gastrografin (10 ml/450 of water) IV contrast: 3 cc/sec for 150 ml Rectal contrast (for penetrating trauma: 40 cc of Conray 60% in 1000 ml normal saline: use ml as tolerated Important: Clamp bladder catheter to achieve full distention of bladder
5 DEDICATED ABD. TRAUMA MDCT 16 (64) - slice MDCT: Detector configuration: 16 (64) x mm, reconstruction thickness and interval: 5 mm Scan delay: 80 sec or smart prep,, diaphragm to ischial tuberosity Important: Single acquisition: total body trauma CT scan: head, cervical spine, chest, abdomen & pelvis Delayed scans (5 min) optional: : parenchymal organs, excretory system incl. bladder, vasc. extravasation CT cystogram for bladder injury: : cc of 20 cc of 60% contrast/500 cc of sterile saline
6 IDENTIFY/CHARACTERIZE INTRA- PERITONEAL FLUID COLLECTIONS Always use ROI for fluid in trauma! Water density ( HU) Mixed density (10-20 HU): urinary bladder, bowel, gallbladder rupture Hemoperitoneum: CT attenuation > 30 HU Sentinel clot (45-70 HU): densest close to injury Active arterial extravasation: > 100 HU


7 HEMOPERITONEUM VS. WATER-DENSE TRAUMATIC INTRAPERITONEAL FLUID 45 HU B 15 HU 10 HU 85 HU
8 IDENTIFY LIFE-THREATENING INJURIES Active extravasation Massive hemorrhage Major vascular injuries Signs of shock Bowel perforation


9 IDENTIFY ACTIVE BLEEDING Active extrav. from spleen -> > embolization
10 LIVER INJURIES Prevalence: occurs in up to 25% of patients with blunt abdominal trauma undergoing CT Mortality ~ 4-12% overall 50-80% with juxtahepatic venous injury Matthes G, Stengel D, Seifert J, et al. Blunt liver injuries in polytrauma: results from a cohort study with regular use of whole body helical computed tomography.world J Surg 2003; 27:
11 LIVER TRAUMA: IDENTIFY Liver laceration Hematoma (54 HU, 28-82) 82) Active hemorrhage (155 HU, ) Juxtahepatic venous injury (Periportal low attenuation) (Flat IVC) Willmann JK, Roos JE, Platz A, et al. Multidetector CT: detection of active hemorrhage in patients with blunt abdominal trauma. AJR 2002; 179:
12 PARENCHYMAL INJURY TO LIVER BLUNT TRAUMA: Hematoma subcapsular or intraparenchymal hematoma Laceration linear, stellate, bear claw lacerations Bleeding recognize arterial or venous injury with extrav. (overall art. extrav. = 18.4%; spleen = 17.7%) PENETRATING TRAUMA: subcapsular hematoma & linear laceration, extrav.
13 GRADING HEPATIC INJURY Hematoma (subcapsular or parenchymal) I < 1cm diameter II 1-33 cm III > 3 cm Laceration I < 1 cm deep II 1-3 cm III > 3 cm Parenchymal disruption IV 25-75% of hepatic lobe, segments V >75% of hepatic lobe, >3 segments Juxtahepatic venous injury VI vena cava, central hepatic veins, avulsion American Association for the Surgery of Trauma and as modified by Mirvis, et al, Radiology 1989;171:27-32.


14 INTRAHEPATIC LAC, GRADE III > 3 cm, no hemoperitoneum Bear Claw Lac



15 LIVER INJURY: GRADE IV AND V IV: Parenchymal disruption: 1-3 segments V: Parenchymal disruption: > 3 segments
16 BARE AREA OF THE LIVER Injury to the bare area: right lobe injury more frequent than left about 25% of liver injuries limited to bare area Liver lacerations into the bare area: usually results in retroperitoneal bleed: bleeding into right anterior pararenal space or perirenal space
17 CT PREDICTOR OF FAILURE FOR NON- OPERATIVE MANAGEMENT Active bleeding on CT Injury grade above III injury of main trunks of hepatic veins twice as likely to fail hepatic veins injured in 13% of patients with liver injury IVC injured (retrohepatic IVC: 50% mortality) Overall nonoperative success rate: 80% in adults, 97% in children Pachter HL, Knudson MM, Esrig B, Ross S, Hoyt D, Cogbill T, et al. Status of nonoperative management of blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996; 40:
18 FOLLOW-UP CT IN BLUNT LIVER TRAUMA Indications for CT in low grades: abdominal pain in RUQ, jaundice, fever, anemia or melena Indications for CT in grades IV to VI: identify complications (7 to 10 days post injury*): bile leakage (biloma, bile peritonitis; 2.8 to 7.4%) delayed hemorrhage (1.7% to 5.9%) abscess (0.6% to 4%) pseudoaneurysm of hepatic artery & hemobilia (1%) * Pachter HL, Knudson MM, Esrig B, Ross S, Hoyt D, Cogbill T, et al. Status of nonoperative management of blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996; 40:
19 BILE LEAKS AAST guidelines for grading liver injury does not take into account bile leaks Difficult to predict who will develop a bile leak Bile leak asymptomatic in up to 50% Symptoms develop if bile infected or biloma large Gallbladder injury uncommon: 2-3% 2 with blunt trauma (distended gallbladder!)



20 LIVER LAC GRADE V + BILE LEAK Percutaneous Drainage of Biloma
21 FOLLOW-UP CT FINDINGS IN BLUNT LIVER TRAUMA Hepatic repair progresses predictably: Resolution Hemoperitoneum 1 week Laceration 3 weeks Subcapsular hematoma weeks Parenchymal homogeneity weeks Hematoma, biloma years Karp MP, Cooney DR, Pros GA, et al. The nonoperative management of pediatric hepatic trauma. J Pediatr Surg 1983; 18:
22 SPLENIC INJURIES Splenic injury most commonly injured organ following blunt abdominal trauma Incidence of splenic injury splenic injury accounts for 40-50% of patients with abdominal organ injury
23 GRADING SPLENIC INJURY Subcapsular hematoma I < 10% surface area II 10-50% III > 50% or expanding Parenchymal hematoma II < 5 cm diameter III > 5 cm or expanding Laceration (parenchyma) I < 1 cm II 1-3 cm III > 3 cm Devascularization (hilar( or segmental vessel damage-> > major devasc.) IV > 25% of spleen Shattered Spleen V completely shattered or hilar vascular injury, no perfusion Moore EE, Cogbill TH, Jurkovich GH, et al. Organ injury scaling: spleen and liver (1994 revision). J Trauma 1995; 38: Shanmuganathan,, et al. Radiology 2000; 217: 75-82


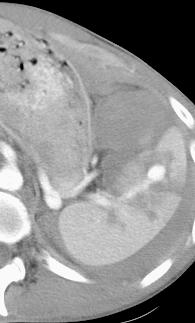
24 HILAR DEVASCULARISATION Grade IV
25 NONOPERATIVE MANAGEMENT Overall success rate: 65% Failed conservative management Grade % Surgical Intervention I 0% II 8% III 19% IV ~100% V all had initial surgery Knudson MM, Maull KI. Nonoperative management of solid organ injuries. Past, present, and future.surg Clin North Am Dec;79(6):
26 SPLENIC INJURIES: COMPLICATION Active hemorrhage hyperattenuating area on portal venous phase with persistent hyperattenuation or increase in size on 5 minute delay Pseudoaneurysm hyperattenuating area on portal venous phase with wash-out on 5 minute delay (acts like other vessels) Anderson SW, Varghese JC, Lucey BC, et al. Blunt Splenic Trauma: Delayed-Phase CT for Differentiation of Active Hemorrhage from Contained Vascular Injury in Patients. Radiology. 2007; 243:88-95.



27 SPLENIC PSEUDOANEURYSM Multiple pseudoaneurysms
28 PANCREATIC INJURIES Incidence: in 1% - 3% of blunt abd. trauma Greatest mortality when delay in Dx 70% of adults (15-30% children) have associated injuries Amylase initially is neither sensitive nor specific days later will be elevated in 80-90% Initial CT sensitivity 68-80% 80%
29 PANCREATIC INJURIES More common under 40 years of age Mechanism: compression against spine Association with liver and duodenal injuries CT findings: initially may be normal Early recognition of duct disruption important because of possible delayed complications: Fistula, pseudocyst, abscess
30 PANCREATIC ORGAN INJURY AAST SCALE Grade I (A*) minor contusion, superficial lac, duct intact Grade II (A) major contusion, major lac, duct intact Grade III (B) duct injury, distal transsection Grade IV (C) proximal transsection, ampulla injury Grade V (C) massive disruption of pancreatic head * Moore classification: Wong YC, Wang LJ, Lin BC, et al. CT grading of blunt pancreatic injuries: prediction of ductal disruption and surgical correlation. J Comput Assist Tomogr 1997; 21:
31 PANCREATIC INJURIES Grade I & II: minor/major contusion or laceration Grade III: distal duct disruption Grade IV: Proximal transsection, ampullary injury Grade V: Pancreas head, duodenal crush injury Patel et al, Br J Radiol 1998;71:
32 CT FINDINGS OF PANCREATIC INJURY Focal or diffuse enlargement/edema focal area of low attenuation = contusion look for asymmetry of the pancreatic septations heterogeneous enhancement Hemorrhage/fluid in anterior pararenal space between pancreas and splenic vein around SMA Duct injury (occurs in about 15% of patients) CT sensitivity low: ERCP or MRCP better; MDCT? implied disruption if laceration is > 50% pancreas thickness


33 PANCREATIC DISSECTION, GRADE III Immediately post trauma ERCP after CT




34 MIMICKER OF TRAUMATIC PANCREATITIS Overhydration Overhydration
35 MDCT OF PANCREATIC INJURY 9/95 (9.5%) patients with blunt abdominal trauma Six with MP duct injury, 3 without Detection of duct injury was 97.7% in pancreatic phase 100% in portal venous phase 96.8% in equilibrium phase High interobserver agreement Wong YC, Wang LJ, Fang JF, et al. MDCT of blunt pancreatic injuries: ies: can contrast- enhanced multiphasic CT detect pancreatic duct injuries? J Trauma 2008; 64:
36 TAKE HOME MESSAGE FOR INTRA- AND RETROPERITONEAL INJURY Dedicated trauma protocol Timing of iv contrast material critical (smart prep) Identify/characterize intraperitoneal fluid collections Identify active bleeding Identify abdominal parenchymal injuries Grade parenchymal injuries for management Obtain delayed scans in selected instances
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Blunt liver trauma- brief review and computed tomography role
 Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY
 CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Management of Blunt Pancreatic Trauma in Children
 Surg Today (2009) 39:115 119 DOI 10.1007/s00595-008-3823-6 Management of Blunt Pancreatic Trauma in Children IVO JURIĆ, ZENON POGORELIĆ, MIHOVIL BIOČIĆ, DAVOR TODORIĆ, DUBRAVKO FURLAN, and TOMISLAV ŠUŠNJAR
Surg Today (2009) 39:115 119 DOI 10.1007/s00595-008-3823-6 Management of Blunt Pancreatic Trauma in Children IVO JURIĆ, ZENON POGORELIĆ, MIHOVIL BIOČIĆ, DAVOR TODORIĆ, DUBRAVKO FURLAN, and TOMISLAV ŠUŠNJAR
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Multidetector CT of Blunt Abdominal Trauma 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Reviews and Commentary
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Reviews and Commentary
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists
 Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists Poster No.: C-1859 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: J. Cazejust,
Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists Poster No.: C-1859 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: J. Cazejust,
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD
 Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
Evaluating the role of liver enzymes as predictors of severity of liver injury in patients with blunt abdominal trauma
 International Journal of Research in Medical Sciences Prasad P et al. Int J Res Med Sci. 2017 Jun;5(6):2462-2467 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20172429
International Journal of Research in Medical Sciences Prasad P et al. Int J Res Med Sci. 2017 Jun;5(6):2462-2467 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20172429
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
Intraabdominal Active Bleeding: Helical CT, MDCT (64slice), DSA and Homeostatic Embolization Findings
, DSA and Homeostatic Embolization Findings") Intraabdominal Active Bleeding: Helical CT, MDCT (64slice), DSA and Homeostatic Embolization Findings Poster No.: C-2495 Congress: ECR 2012 Type: Educational Exhibit Authors: B. ALPARSLAN, N. YILDIRIM,
Intraabdominal Active Bleeding: Helical CT, MDCT (64slice), DSA and Homeostatic Embolization Findings Poster No.: C-2495 Congress: ECR 2012 Type: Educational Exhibit Authors: B. ALPARSLAN, N. YILDIRIM,
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
The role of multidetector computed tomography versus digital subtraction angiography in triaging care and management in abdominopelvic trauma
 Singapore Med J 2016; 57(9): 497-502 doi: 10.11622/smedj.2015179 The role of multidetector computed tomography versus digital subtraction angiography in triaging care and management in abdominopelvic trauma
Singapore Med J 2016; 57(9): 497-502 doi: 10.11622/smedj.2015179 The role of multidetector computed tomography versus digital subtraction angiography in triaging care and management in abdominopelvic trauma
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Acute, Blood, Trauma /ecr2015/C-2116
 The Baltimore CT Severity Index (CTSI) versus the American Association of Surgical Trauma (AAST) for grading splenic Injury on CT: Use and implications of an imaging based grading system for splenic injury
The Baltimore CT Severity Index (CTSI) versus the American Association of Surgical Trauma (AAST) for grading splenic Injury on CT: Use and implications of an imaging based grading system for splenic injury
Urogenital Injuries The role of radiology
 Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS***
 Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Conservative Management of Blunt Hepatic Trauma for Patients with High Severity Grades Injuries A Clinical Selective Prospective Study
 Med. J. Cairo Univ., Vol. 84, No. 2, June: 97-103, 2016 www.medicaljournalofcairouniversity.net Conservative Management of Blunt Hepatic Trauma for Patients with High Severity Grades Injuries A Clinical
Med. J. Cairo Univ., Vol. 84, No. 2, June: 97-103, 2016 www.medicaljournalofcairouniversity.net Conservative Management of Blunt Hepatic Trauma for Patients with High Severity Grades Injuries A Clinical
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE
 MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
Multiphase contrast-enhanced MRI for control of subacute trauma of abdomen and chest in children
 Multiphase contrast-enhanced MRI for control of subacute trauma of abdomen and chest in children Poster No.: B-0862 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Paper A. Petraikin, T. Akhadov,
Multiphase contrast-enhanced MRI for control of subacute trauma of abdomen and chest in children Poster No.: B-0862 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Paper A. Petraikin, T. Akhadov,
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Internal Injury Documentation Guidelines
 Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Abdomen and Pelvis CT (1) By the end of the lecture students should be able to:
 By the end of the lecture students should be able to:") RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
RAD 451 Abdomen and Pelvis CT (1) By the end of the lecture students should be able to: State the common indications for Abdomen and pelvis CT exams Identify possible contra indications for Abdomen and
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
abdominal trauma in children
 352 Pictorial Essay CME Article Computed tomography of blunt abdominal trauma in children Visrutaratna P, Na -Chiangmai W ABSTRACT Computed tomography (CT) plays a major role in diagnosis of blunt abdominal
352 Pictorial Essay CME Article Computed tomography of blunt abdominal trauma in children Visrutaratna P, Na -Chiangmai W ABSTRACT Computed tomography (CT) plays a major role in diagnosis of blunt abdominal
Abdominal active bleeding in the emergency room: Assessment with 64-slice MDCT
 Abdominal active bleeding in the emergency room: Assessment with 64-slice MDCT Poster No.: C-3055 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular Authors: R. Larrosa, J. M. Mellado, S. Solanas,
Abdominal active bleeding in the emergency room: Assessment with 64-slice MDCT Poster No.: C-3055 Congress: ECR 2010 Type: Educational Exhibit Topic: Vascular Authors: R. Larrosa, J. M. Mellado, S. Solanas,
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון
 Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Endovascular management of blunt trauma to the
 Endovascular Management of Abdominal Solid Organ Trauma Indications and embolic agents for successful noninvasive treatment. BY RICARDO YAMADA, MD; MARCELO GUIMARAES, MD, FSIR; AND CLAUDIO SCHÖNHOLZ, MD
Endovascular Management of Abdominal Solid Organ Trauma Indications and embolic agents for successful noninvasive treatment. BY RICARDO YAMADA, MD; MARCELO GUIMARAES, MD, FSIR; AND CLAUDIO SCHÖNHOLZ, MD
Multilevel Duodenal Injury after Blunt Trauma
 J Korean Surg Soc 2009;77:282-286 DOI: 10.4174/jkss.2009.77.4.282 증 례 Multilevel Duodenal Injury after Blunt Trauma Department of Surgery, College of Medicine, Hallym University, Chuncheon, Korea Jeong
J Korean Surg Soc 2009;77:282-286 DOI: 10.4174/jkss.2009.77.4.282 증 례 Multilevel Duodenal Injury after Blunt Trauma Department of Surgery, College of Medicine, Hallym University, Chuncheon, Korea Jeong
Efficacy of Emergent Splenic Artery Embolization in Conservative Treatment of High Grade Splenic Injury
 Chin J Radiol 2005; 30: 1-7 1 Efficacy of Emergent Splenic Artery Embolization in Conservative Treatment of High Grade Splenic Injury YU-SAN LIAO YU-FAN CHENG TUNG-LIANG HUANG PAO-CHU YU CHUNG-CHENG HUANG
Chin J Radiol 2005; 30: 1-7 1 Efficacy of Emergent Splenic Artery Embolization in Conservative Treatment of High Grade Splenic Injury YU-SAN LIAO YU-FAN CHENG TUNG-LIANG HUANG PAO-CHU YU CHUNG-CHENG HUANG
Vascular complications in percutaneous biliary interventions: A series of 111 procedures
 Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China
 Review Article Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China Jingshan Gong, Dongdong Mei, Minjie Yang, Jianmin Xu, Yangyang Zhou Department of Radiology,
Review Article Emergency CT of blunt abdominal trauma: experience from a large urban hospital in Southern China Jingshan Gong, Dongdong Mei, Minjie Yang, Jianmin Xu, Yangyang Zhou Department of Radiology,
pitfall Table 1 4 disorientation pitfall pitfall Table 1 Tel:
 11 687 692 2002 pitfall 1078 29 17 9 1 2 3 dislocation outflow block 11 1 2 3 9 1 2 3 4 disorientation pitfall 11 687 692 2002 Tel: 075-751-3606 606-8507 54 2001 8 27 2002 10 31 29 4 pitfall 16 1078 Table
11 687 692 2002 pitfall 1078 29 17 9 1 2 3 dislocation outflow block 11 1 2 3 9 1 2 3 4 disorientation pitfall 11 687 692 2002 Tel: 075-751-3606 606-8507 54 2001 8 27 2002 10 31 29 4 pitfall 16 1078 Table
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE. T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar
 ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Radiation dose considerations. > 80 million total CT scans / year in USA in 2010 (25% ED)
") Martin Gunn Department of Radiology University of Washington I have no actual or potential conflict of interest in relationship to this presentation. I do have the following declarations: Grant support:
Martin Gunn Department of Radiology University of Washington I have no actual or potential conflict of interest in relationship to this presentation. I do have the following declarations: Grant support:
ORIGINAL ARTICLE. Complications Following Renal Trauma
 ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Practice Variability in the Management of Pediatric Pancreatic Trauma
 Practice Variability in the Management of Pediatric Pancreatic Trauma Bindi Naik-Mathuria, MD and members of the Pediatric Trauma Study Group Falcone R Burd R Puapong D Mooney D Campbell B Kreyekes N Fenton
Practice Variability in the Management of Pediatric Pancreatic Trauma Bindi Naik-Mathuria, MD and members of the Pediatric Trauma Study Group Falcone R Burd R Puapong D Mooney D Campbell B Kreyekes N Fenton
Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment
 Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment Poster No.: C-1422 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Matsuura, K. Takase, T. Hasegawa, H. Ota, K.
Postpancreatectomy Hemorrhage: Imaging and Interventional Radiological Treatment Poster No.: C-1422 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Matsuura, K. Takase, T. Hasegawa, H. Ota, K.
Grade Description of injury ICD-9 AIS-90
 Scaling system for organ specific injuries Ernest E. Moore, MD, Thomas H. Cogbill, MD, Mark Malangoni, MD, Gregory J. Jurkovich, MD, and Howard R. Champion, MD Table Cervical vascular organ injury scale
Scaling system for organ specific injuries Ernest E. Moore, MD, Thomas H. Cogbill, MD, Mark Malangoni, MD, Gregory J. Jurkovich, MD, and Howard R. Champion, MD Table Cervical vascular organ injury scale
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Management of biliary complications following damage control surgery for liver trauma
 Eur J Trauma Emerg Surg DOI 10.1007/s00068-013-0304-4 ORIGINAL ARTICLE Management of biliary complications following damage control surgery for liver trauma M. Hommes G. Kazemier N. W. L. Schep E. J. Kuipers
Eur J Trauma Emerg Surg DOI 10.1007/s00068-013-0304-4 ORIGINAL ARTICLE Management of biliary complications following damage control surgery for liver trauma M. Hommes G. Kazemier N. W. L. Schep E. J. Kuipers
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience
 Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Pediatric emergencies. Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
 Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma") Department of Clinical Radiology, Munich University Hospital Pediatric emergencies Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
Department of Clinical Radiology, Munich University Hospital Pediatric emergencies Emergent Neuroimaging Acute chest (non-trauma) Acute abdomen (non-trauma) Sports injuries (trauma) Highlights/Trends Polytrauma
Intravascular Pressure as a Predictor of Injury Severity in Blunt Hepatic Trauma
 Intravascular Pressure as a Predictor of Injury Severity in Blunt Hepatic Trauma Jessica Sparks 1, Jason Stammen 2, Rodney Herriott 3, Kenneth Jones 4, John Bolte, IV 4 1 Injury Biomechanics Research Laboratory,
Intravascular Pressure as a Predictor of Injury Severity in Blunt Hepatic Trauma Jessica Sparks 1, Jason Stammen 2, Rodney Herriott 3, Kenneth Jones 4, John Bolte, IV 4 1 Injury Biomechanics Research Laboratory,
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Traumatic Retroperitoneal Injuries: Review of Multidetector CT Findings 1
 Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this
SSRG International Journal of Medical Science (SSRG-IJMS) volume 1 Issue 2 December 2014
 volume 1 Issue 2 December 2014") Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Role of CT in Evaluation of Blunt Abdominal Trauma
 International Journal of Medical Imaging 2015; 3(5): 89-93 Published online July 29, 2015 (http://www.sciencepublishinggroup.com/j/ijmi) doi: 10.11648/j.ijmi.20150305.11 ISSN: 2330-8303 (Print); ISSN:
International Journal of Medical Imaging 2015; 3(5): 89-93 Published online July 29, 2015 (http://www.sciencepublishinggroup.com/j/ijmi) doi: 10.11648/j.ijmi.20150305.11 ISSN: 2330-8303 (Print); ISSN:
Traumatic and Non Traumatic Adrenal Emergencies
 Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries
 Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
Multidetector CTA for Diagnosing Blunt Cerebrovascular Injuries 4 th Nordic Trauma Course 2006 Stuart E. Mirvis, M.D., FACR Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland
CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications
 Clinical Radiology (2004) 59, 342 348 CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications L.A. Miller, S.E. Mirvis, K. Shanmuganathan, A.S. Ohson*
Clinical Radiology (2004) 59, 342 348 CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications L.A. Miller, S.E. Mirvis, K. Shanmuganathan, A.S. Ohson*
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed