TB-Free California: How close are we? How can we get closer?
|
|
|
- Brendan Evelyn Andrews
- 5 years ago
- Views:
Transcription


1 TB-Free California: How close are we? How can we get closer? California TB Controllers Association April 21, 2015 Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology Section


2 Acknowledgments Local TB Control Programs Lisa Pascopella Peter Oh Janice Westenhouse Christy Pak Phil Lowenthal Tambi Shaw Clinton McDaniel Melissa Ehman Katya Salcedo Jenny Flood 2 Graph courtesy Malcolm Barry-Kao, age 6
3 TB in California Time to Elimination Source of TB Cases Outline (Sub)Populations with TB Current TB prevention activities Getting closer to Elimination Areas for improvement in current activities Possible new TB control activities 3
 Sources: U.S. Census Bureau Decennial Censuses, American Community Survey, and the Department of Homeland Security. 4")
4 Pop 38.8 million > 10 million immigrants (27% of CA pop.) ~25% of foreign-born in U.S. Estimated 2.5 million undocumented 50% of all children with an immigrant parent ~25% of TB in U.S. From Public Policy Institute of California ( Sources: U.S. Census Bureau Decennial Censuses, American Community Survey, and the Department of Homeland Security. 4
5 TB in California Time to Elimination Source of TB Cases 5
6 TB Diagnosed in CA every 4 hours Each = 1 TB case (Total = 2147) 6

")
7 TB Diagnosed in CA every 4 hours Foreign-born: 77% US-born: 22% Each = 1 TB case (Total = 2147) 7
8 Elimination Definitions Goal Goal Rate Cases in California* End of TB Epidemic <100 cases/million 3,880 Pre-elimination < 10 cases/million 388 Elimination <1 case / million 39 *Based on 2014 US Census Estimate of California Population: 38.8 million WHO. Framework towards TB Elimination in Low-Incidence Countries
9 Number of TB Cases Tuberculosis Cases and Case Rates 6,000 5,000 4,000 3,000 2,000 1, California, , TB Cases TB Rate , Case Rate per 100,000 9
10 Projected years of TB pre-elimination and elimination in California Rate per 1 Million Actual Current decline (-3.95%) Required for 2040 Elimination (-14.35%) Pre-Elimination Elimination Year
11 Projected years of TB pre-elimination and elimination in California 1000 Rate per 1 Million Actual Current decline (-3.95%) Required for 2040 Elimination (-14.35%) Pre-Elimination Elimination Year
12 How do TB Cases Occur in California? Importation TB within 1 year of US arrival Recent Transmission Reactivation of remote infection ~2,000 TB Cases Per Year 12
13 Clues to Source of TB Cases Source Importation Epidemiologic Clues Foreign-born TB diagnosed within 1 year of arrival to U.S. Recent transmission (within ~2-3 years) Reactivation of remote infection Genotype clustering Aged < 5 years TB in known contacts Linked cases on RVCT TB >5 years after arrival to U.S. TB in persons aged 65 years old Cases that are not from importation or recent transmission 13
14 How do TB Cases Occur in California? Importation TB within 1 year of US arrival 835 of 11,149 cases occurred within 1 year of arrival in US 7.5% Reactivation of remote infection Cases not from importation or recent transmission: 75.5% ~2,000 TB Cases Per Year Recent Transmission 26% genotype clustering within county (3 year window) 8% with indication of transmission within 2 years on RVCT Midpoint = 17% 14
15 7% Proportion of TB Cases among children < 5 years California, % of TB cases 6% 5% 4% 3% 2% 1% 0% 2.6%
16 TB Cases within 1 year of arrival in U.S. California, Number of TB Cases % 16% 14% 12% 10% 8% 6% 4% 2% 0% % of TB Cases TB Cases % of Cases 16
17 TB Cases by Age Group and Median Age, California, Number of cases
18 TB Cases by Age Group and Median Age, California, Number of cases % -10% -22% -14% -26% Median Age USB FB
19 TB cases by years in US at TB report 0 California, yr 1-10 yrs yrs >20 yrs % -14% -30% -12% 19
20 (Sub)populations with TB Healthcare workers Corrections HIV
21 Number of Cases TB cases among healthcare workers, California % foreign-born Foreign-born HCW US-born HCW % of TB Cases Percent of TB Cases 21
22 TB Cases Diagnosed in Corrections California, Corrections % of TB Cases 5.0% 4.5% % Number of Cases % 3.0% 2.5% 2.0% 1.5% % of All TB Cases % 0.5% % 22
23 Incidence Rate per 100,000 Population TB Incidence Rates by Type of Correctional Facility California, State Prison Incidence Rate Local Jail Incidence Rate Non-Corrections Incidence Rate Slide courtesy Clinton McDaniel Year TB Diagnosed
24 Proportion of TB patients HIV-infected California % Proportion of TB-HIV 4.2% N=86 Count Year 24
25 Healthcare workers, HIV infected, corrections residents Historical intense focus for TB control Now declining or stable TB (each <5% of TB) Not main drivers of current TB cases 25
26 (Sub)populations with TB Foreign-born
27 25 California Case Rates by Nativity Foreign-born U.S.-born TB Rate per 100, Total
28 Countries of Birth for Foreign Born Persons with TB California, 2014 N=1,666 Mexico 446 Philippines 354 Vietnam Other 205 China 145 India % 20% 40% 60% 80% 100% 28
29 Years in US at TB Diagnosis California, TB Cases Years in US 29
30 TB Cases Years in US at TB Diagnosis California, B-notification cases* Years in US *Cases diagnosed in domestic evaluation of abnormal preimmigration CXR 30
31 Years in US at TB Diagnosis California, TB Cases % in US > 5.9 years Median 16.0 yrs 25Q Q Q 37.3 Years in US 31
32 Years in US at TB Diagnosis California, % in US > 5.9 years 700 TB Cases % in US >16 years Median 16.0 yrs 25Q Q Q Years in US 32
33 Constant rate of reactivation from TB infection after immigration Avg rate per 100,000 = 31.8 Years after immigration with a normal pre-immigration chest radiograph Filipino immigrants to California Walter et al AJRCC
34 TB Prevention through screening and treatment of TB Infection Immigrants and other new arrivers 34
35 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Immigration Status at First US Entry persons with TB California, % Immigrant Visa n=683 Screened (for active disease) 9% Refugee/Asylee /Family n=150 5% Student/Worker n=74 Not screened * Includes persons from counties with policies against collecting immigration status information 3% Tourist n=45 23% Other (includes undocumented) n=383 Probably Not screened 18% Unknown* n=300 35
36 Newcomers to California Examples Number per year TB screening required? New immigrants Green Card holders Refugees 200,000 Nonimmigrant Admissions Tourists Students Workers 11,000,000 (640,000 students/ workers) No legal status Undocumented Yes No N/A? Source: US Dept of Homeland Security. Yearbook of Immigration Statistics
37 TB Screening of New Immigrants Legal Permanent Residents B-notification Apply Overseas N=100,000 / year Active case finding only Evaluated overseas CXR (TST for children) Abnormal CXR 3 sputa smear and cx If no active TB Domestic follow-up by health department Data easily available Status adjustors Apply in US N=100,000/year Active and latent testing Evaluated by civil surgeons TST or IGRA CXR for positives (>5mm) No requirement for treatment or referral if no active TB Is LTBI treatment given? Data not available Source: U.S. Dept of Homeland Security. 37
38 % of Arrivers* with active TB within 6 mos of arrival California 4.5% 4.0% 4.1% 3.5% 3.4% 3.0% Pre-immigration sputum culture 2.5% 2.0% 1.5% 1.0% 1.6% 1.2% 1.7% 1.4% 0.9% 1.3% 0.5% 0.0% ** *B1 notification arrivers: abnormal pre-immigration CXR **Jan-June only 38
39 100% 80% Treatment for arrivers with abnormal pre-immigration CXR California, % 40% 20% Unknown No treatment LTBI treatment 0% ATS Class 2 n=1191 ATS Class 4 n=2505 Persons evaluated in California including with a CXR 39
40 New Arriver Screening Gaps Many not screened at all (visitors, undocumented) Of those screened great majority not screened for LTBI Even among those screened by health departments >40% don t start treatment No data from civil surgeons 40
41 TB Prevention through screening and treatment of TB Infection Longstanding Residents of California 41
42 20,000 Evaluation and Treatment of Contacts care cascade California, ,000 10,000 33% of infected contacts complete treatment 5,000 0 Elicited (100%) Evaluated (88%) Infected (21%) Treatment started (54%) Treatment completed (62%) 42
43 Evaluation and Treatment of Contacts care cascade California, , Contacts 15,000 Opportunity 10,000 5, * Elicited (100%) Evaluated (88%) Infected (21%) Treatment started (54%) Treatment completed (62%) * Estimated based on proportion infected among those evaluated 43
44 TBI infections estimated by applying nativity and race/ethnicity-specific TB infection rates from 44 NHANES (Bennett et al 2008 and Shea et al 2014) to the California population 2.5 Million Estimated TB Infections California US Born 0.5 Million Foreign Born 2 Million 0% 20% 40% 60% 80% 100%
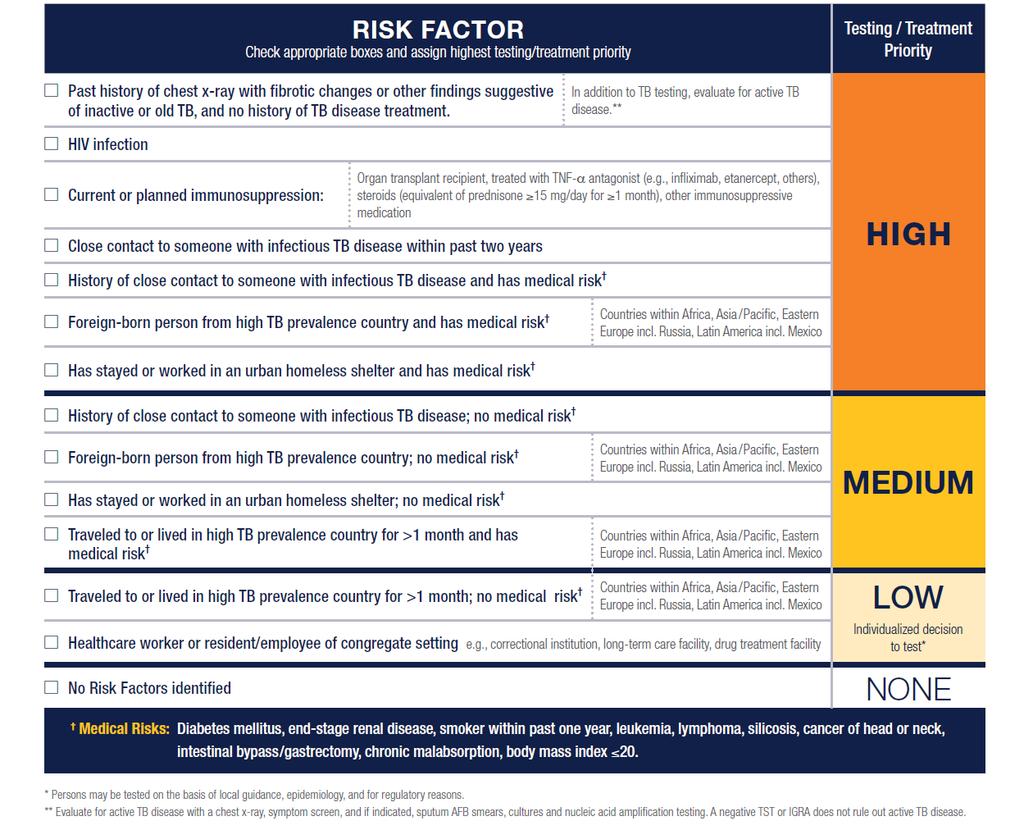
45 Who to Test for LTBI? Risk of Exposure Risk of Progression 45
46 Medical Risk Factors among persons with TB by nativity California, 2014 Total n (%) US-born % Foreign-born % Diabetes 508 (24.7) 13.9% 27.3% ESRD 82 (4.0) 2.9% 4.2% HIV positive 86 (4.2) 9.9% 3.5% Other immunosuppression Post-organ transplantation 124 (6.0) 5.0% 6.3% 23 (1.0) 0.5% 1.3% TNF-antagonist rx 20 (1.0) 0.5% 1.1% 1+ co-morbidity 723 (35.2) 30.2% 36.5% Persons aged 15 46
47 TB Rate by Diabetes, Age, and Nativity California, (Persons aged 18) Case Rate per 100, Diabetes No Diabetes United States or Canada Foreign-born Demlow et al, BMC Public Health 2015 Sources: Denominator: California Health Interview Survey Numerator: CA TB Registry 47
48 TBI infections estimated by applying nativity and race/ethnicity-specific TB infection rates from 48 NHANES (Bennett et al 2008 and Shea et al 2014) to the California population 2.5 Million Estimated TB Infections California US Born 0.5 Million Foreign Born 2 Million 0% 20% 40% 60% 80% 100%
49 Estimated TB Infections and Cases Among Selected Medical Risk Groups California Medical Risk Total Current smokers* Diabetes Immune suppression** ESRD*** HIV/AIDS Organ transplant Total Population 6,518,613 3,650,000 2,322, ,213 78, ,900 26,700 FB with LTBI 368, , ,000 10,925 4,200 3,600 1,200 Total with LTBI 450, , ,200 15,841 5,200 5,400 1,600 Relative Risk of Progression Estimated Case number (FB) 1, Total Estimated Cases 1, Actual cases (2014) Cases estimated using baseline annual rate of progression from Shea et al, 2014: for FB and for USB FB = foreign-born * Excludes 93,000 smokers that have diabetes ** Includes only estimates of total population with inflammatory bowel disease and rheumatoid arthritis ***Includes all patients including those s/p kidney transplant 49
50 Estimated TB Infections and Cases California US Born Foreign Born 38 M Populatn. 1,970,238 (5%) Medical Risk medical risk: current smoking, DM, HIV, ESRD, organ transplant, and those having another indication for immunosuppression (inflammatory bowel disease or rheumatoid arthritis) 50
51 Estimated TB Infections and Cases California US Born Foreign Born 38 M Populatn. 1,970,238 (5%) Medical Risk 2.5 M TB infections 368,434 (14%) medical risk: current smoking, DM, HIV, ESRD, organ transplant, and those having another indication for immunosuppression (inflammatory bowel disease or rheumatoid arthritis) 51
52 Estimated TB Infections and Cases California US Born Foreign Born 38 M Populatn. 1,970,238 (5%) Medical Risk 2.5 M TB infections 368,434 (15%) Medical Risk 2,147 TB Cases 1,098 (51%) 0% 20% 40% 60% 80% 100% medical risk: current smoking, DM, HIV, ESRD, organ transplant, and those having another indication for immunosuppression (inflammatory bowel disease or rheumatoid arthritis) 52
53 How many Californians are being Group tested for TB Infection now? Estimated Number tested annually TB risk Healthcare workers 1,443,000 Low Status adjusters (civil surgeons) 105,000 Moderate-High Contacts 17,000 High B-notification arrivers 5,000 High Very High Others? varied Total 1,570,000 *Source for healthcare worker data: California Healthcare Workforce Clearinghouse ( 53


54 Improvements and Possible New TB Control Activities In order to achieve elimination by
55 Areas for Improvement in Current Activities In order to achieve elimination by 2040 Treat higher proportion of persons known to have TB infection: Contacts B-notification arrivers Status adjusters More testing of highest risk Risk assessment Get highest risk patients through LTBI care cascade 55
56 56
57 Possible New Activities Alter new arriver screening? Identify TB infection in overseas evaluations Expand to other types of arrivers Linkage to TB infection treatment for domestic evaluation Make latent TB infection reportable? 57
58 Projected years of TB pre-elimination and elimination in California Rate per 1 Million Current decline (-3.95%) Required for 2040 Elimination (-14.35%) Pre-Elimination Elimination 42,400 Cases averted Year
59 We have done it before 59
60 Number of Tuberculosis Cases, California, ,000 6,000 5,000 4,000 3,000 2,000 1,000 0 Constant 1985 rates Year 2013 Projected case count calculated by applying the nativity-specific rate to population denominators 60
61 Number of Tuberculosis Cases, California, ,000 Constant 1985 rates 6,000 5,000 4,000 3,000 Difference = 44,373 (since 1992) 2,000 1, Year 2013 Projected case count calculated by applying the nativity-specific rate to population denominators 61
62 62
Tuberculosis Elimination Jennifer Flood, MD, MPH Pennan Barry, MD, MPH NAR-NTCA February 25, 2016
 Tuberculosis Elimination Jennifer Flood, MD, MPH Pennan Barry, MD, MPH NAR-NTCA February 25, 2016 Picture source: http://www.lovethispic.com/uploaded_images/12860-california-dreamin.jpg Questions What
Tuberculosis Elimination Jennifer Flood, MD, MPH Pennan Barry, MD, MPH NAR-NTCA February 25, 2016 Picture source: http://www.lovethispic.com/uploaded_images/12860-california-dreamin.jpg Questions What
TB EPIDEMIOLOGY. Outline. Estimated Global TB Burden, TB epidemiology
 TB EPIDEMIOLOGY TB Clinical Intensive Course Curry International Tuberculosis Center September 30, 2015 Varsha Nimbal, MPH Tuberculosis Control Branch California Department of Public Health 1 Outline TB
TB EPIDEMIOLOGY TB Clinical Intensive Course Curry International Tuberculosis Center September 30, 2015 Varsha Nimbal, MPH Tuberculosis Control Branch California Department of Public Health 1 Outline TB
TB in California: Costs, Transmission, and Selecting from the Latent Pool
 TB in California: Costs, Transmission, and Selecting from the Latent Pool Pennan Barry, MD, MPH Tuberculosis Control Branch California Department of Public Health California Tuberculosis Controller s Association
TB in California: Costs, Transmission, and Selecting from the Latent Pool Pennan Barry, MD, MPH Tuberculosis Control Branch California Department of Public Health California Tuberculosis Controller s Association
TB Infection Who is Testing and Treating? TB Control and Elimination: Current Dilemma. Span of TB Control: 2010
 TB Infection Who is Testing and Treating? Jennifer Flood, M.D., M.P.H. California Department of Public Health Tuberculosis Control Branch Jennifer.Flood@cdph.ca.gov 1 TB Control and Elimination: Current
TB Infection Who is Testing and Treating? Jennifer Flood, M.D., M.P.H. California Department of Public Health Tuberculosis Control Branch Jennifer.Flood@cdph.ca.gov 1 TB Control and Elimination: Current
California TB program updates
 California TB program updates CAPHLD Conference Nov 6, 2017 Pennan Barry, M.D., M.P.H. Chief, Surveillance and Epidemiology Section Lead MD, California MDR TB Service pennan.barry@cdph.ca.gov Outline California
California TB program updates CAPHLD Conference Nov 6, 2017 Pennan Barry, M.D., M.P.H. Chief, Surveillance and Epidemiology Section Lead MD, California MDR TB Service pennan.barry@cdph.ca.gov Outline California
Tuberculosis Epidemiology
 Tuberculosis Epidemiology TB CLINICAL INTENSIVE COURSE Curry International Tuberculosis Center October 18, 2017 Varsha Hampole, MPH Tuberculosis Control Branch California Department Of Public Health Outline
Tuberculosis Epidemiology TB CLINICAL INTENSIVE COURSE Curry International Tuberculosis Center October 18, 2017 Varsha Hampole, MPH Tuberculosis Control Branch California Department Of Public Health Outline
The Epidemiology of Tuberculosis in Minnesota,
 The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
The Epidemiology of Tuberculosis in Minnesota, 2011 2015 Minnesota Department of Health Tuberculosis Prevention and Control Program (651) 201-5414 Tuberculosis surveillance data for Minnesota are available
TB Intensive Minneapolis, Minnesota September 23-26, 2008
 TB Intensive Minneapolis, Minnesota September 23-26, 2008 TB in the Foreign-Born Population: Background and Demographic Overview Marge Higgins, LSW September 24, 2008 TB in the Foreign-Born Population
TB Intensive Minneapolis, Minnesota September 23-26, 2008 TB in the Foreign-Born Population: Background and Demographic Overview Marge Higgins, LSW September 24, 2008 TB in the Foreign-Born Population
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
4/25/2012. The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB
 Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Sindy M. Paul, MD, MPH, FACPM May 1, 2012 The information on patterns of infection and disease can assist in: Assessing current and evolving trends in TB morbidity, including resistance Identifying people
Pediatric Tuberculosis in Los Angeles County: An Update
 Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
Pediatric Tuberculosis in Los Angeles County: An Update Julie Higashi, MD PhD Director, Tuberculosis Control Program March 2, 2019 0 Pediatricians will be the driving force of TB elimination in California
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
Update on the 2007 TB Technical Instructions. Adriene Rister TB Control Coordinator Mainely TB: April 14, 2011
 Update on the 2007 TB Technical Instructions Adriene Rister TB Control Coordinator Mainely TB: April 14, 2011 Annual Estimate of Migrants Entering the U.S. Refugees: 50,000-70,000 Immigrants: ~1 million
Update on the 2007 TB Technical Instructions Adriene Rister TB Control Coordinator Mainely TB: April 14, 2011 Annual Estimate of Migrants Entering the U.S. Refugees: 50,000-70,000 Immigrants: ~1 million
Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination
 IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
IUATLD North American Region Conference February 24, 2017 Vancouver, BC Expanding Latent Tuberculosis Infection Testing and Treatment to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
The Public Health Impact of TB in the Correctional System. Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer
 The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
2016 Annual Tuberculosis Report For Fresno County
 206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
206 Annual Tuberculosis Report For Fresno County Cases Rate per 00,000 people 206 Tuberculosis Annual Report Fresno County Department of Public Health (FCDPH) Tuberculosis Control Program Tuberculosis
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges
 Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Detection and Treatment of Tuberculosis in Correctional Facilities: Opportunities and Challenges David Karol, MD, MA Bureau of Prisons, FMC Butner Duke University Medical Center June 26, 2013 No Disclosures
Revised Technical Instructions for Civil Surgeons. October 9, 2018
 Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
Revised Technical Instructions for Civil Surgeons October 9, 2018 Speakers Joanna Regan Centers for Disease Control and Prevention Shereen Katrak California Department of Public Health Pennan Barry California
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of Tuberculosis Denver TB Course
 Epidemiology of Tuberculosis Denver TB Course Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver
Epidemiology of Tuberculosis Denver TB Course Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver
WASHINGTON STATE COMMUNICABLE DISEASES OF PUBLIC HEALTH SIGNIFICANCE FOR THE CIVIL SURGEON
 WASHINGTON STATE COMMUNICABLE DISEASES OF PUBLIC HEALTH SIGNIFICANCE FOR THE CIVIL SURGEON SCOTT LINDQUIST MD MPH WASHINGTON STATE DEPARTMENT OF HEALTH STATE EPIDEMIOLOGIST FOR COMMUNICABLE DISEASES FOREIGN-BORN
WASHINGTON STATE COMMUNICABLE DISEASES OF PUBLIC HEALTH SIGNIFICANCE FOR THE CIVIL SURGEON SCOTT LINDQUIST MD MPH WASHINGTON STATE DEPARTMENT OF HEALTH STATE EPIDEMIOLOGIST FOR COMMUNICABLE DISEASES FOREIGN-BORN
Disclosures. TB and CoMorbidities Challenges and Opportunities. Burden of TB. Outline of the lecture. Target testing for TB Infection TB HIV 3/25/2012
 Disclosures TB and CoMorbidities Challenges and Opportunities E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine, Brown University Providence, Rhode Island No financial disclosures
Disclosures TB and CoMorbidities Challenges and Opportunities E. Jane Carter, M.D. Associate Professor of Medicine Alpert School of Medicine, Brown University Providence, Rhode Island No financial disclosures
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB Epidemiology Robert Petrossian July 18, 2012 Robert Petrossian has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 TB Epidemiology Robert Petrossian July 18, 2012 Robert Petrossian has the following disclosures to make: No conflict of interests No relevant
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
The American Experience with TB Elimination
 Reaching the Goal of TB Elimination by 2035 March 3, 2015 The American Experience with TB Elimination John Jereb, M.D. Medical officer Division of Tuberculosis Elimination National Center for HIV/AIDS,
Reaching the Goal of TB Elimination by 2035 March 3, 2015 The American Experience with TB Elimination John Jereb, M.D. Medical officer Division of Tuberculosis Elimination National Center for HIV/AIDS,
MEMORANDUM. Re: Guidance for follow-up of newly-arrived individual with Class B1 Tuberculosis Pulmonary Tuberculosis, no treatment
 MEMORANDUM To: From: Local Board of Health John Bernardo, MD, Tuberculosis Medical Officer Jennifer Cochran, MPH, Division Director Division of Global Populations and Infectious Disease Prevention Bureau
MEMORANDUM To: From: Local Board of Health John Bernardo, MD, Tuberculosis Medical Officer Jennifer Cochran, MPH, Division Director Division of Global Populations and Infectious Disease Prevention Bureau
Tuberculosis Populations at Risk
 Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
Tuberculosis Populations at Risk One-third of the world is infected with TB, an average of one new infection per second Two million people died from tuberculosis in 2010, 1 every 20 seconds TB is the leading
The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination
 Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Four Corners TB and HIV Conference November 3, 2015 Durango, CO The Tip of the Iceberg: Addressing Latent Tuberculosis Infection to Accelerate Tuberculosis Elimination Philip LoBue, MD National Center
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Contact Investigation in the Correctional Setting Jessica Quintero, BAAS March 24, 2011 Jessica Quintero, BAAS has the following disclosures to make: No
TB in Corrections Phoenix, Arizona March 24, 2011 Contact Investigation in the Correctional Setting Jessica Quintero, BAAS March 24, 2011 Jessica Quintero, BAAS has the following disclosures to make: No
MEMORANDUM. Re: Guidance for follow-up of newly-arrived Individual with a Class B1 Tuberculosis Extrapulmonary Tuberculosis
 MEMORANDUM To: From: Local Board of Health John Bernardo, MD, Tuberculosis Medical Officer Jennifer Cochran, MPH, Division Director Division of Global Populations and Infectious Disease Prevention Bureau
MEMORANDUM To: From: Local Board of Health John Bernardo, MD, Tuberculosis Medical Officer Jennifer Cochran, MPH, Division Director Division of Global Populations and Infectious Disease Prevention Bureau
Report on Tuberculosis in California, 2012
 Golden Gate University School of Law GGU Law Digital Commons California Agencies California Documents 2012 Report on Tuberculosis in California, 2012 California Department of Public Health Follow this
Golden Gate University School of Law GGU Law Digital Commons California Agencies California Documents 2012 Report on Tuberculosis in California, 2012 California Department of Public Health Follow this
2008 Tuberculosis Report
 2008 Tuberculosis Report County of Sacramento Department of Health and Human Services Division of Public Health Page 1 Table of Contents Figure 1. Tuberculosis Incidence Rates, County of Sacramento Vs
2008 Tuberculosis Report County of Sacramento Department of Health and Human Services Division of Public Health Page 1 Table of Contents Figure 1. Tuberculosis Incidence Rates, County of Sacramento Vs
Epidemiology of TB: A Local and National Overview
 Epidemiology of TB: A Local and National Overview Sonal S. Munsiff, MD Director, Bureau of Tuberculosis Control NYC Department of Health and Mental Hygiene Medical Officer, DTBE, CDC February 4, 24 Tuberculosis
Epidemiology of TB: A Local and National Overview Sonal S. Munsiff, MD Director, Bureau of Tuberculosis Control NYC Department of Health and Mental Hygiene Medical Officer, DTBE, CDC February 4, 24 Tuberculosis
Global, National, Regional
 Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Epidemiology of TB: Global, National, Regional September 13, 211 Edward Zuroweste, MD Chief Medical Officer Migrant Clinicians Network Assistant Professor of Medicine Johns Hopkins School of Medicine Epidemiology
Tuberculosis Elimination
 Tuberculosis Elimination Where We ve Been, Where We re Going Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination Centers for Disease Control and Prevention Disclosures / Disclaimer
Tuberculosis Elimination Where We ve Been, Where We re Going Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination Centers for Disease Control and Prevention Disclosures / Disclaimer
2015 Annual Report Tuberculosis in Fresno County. Department of Public Health
 215 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org Number of Cases Rate per 1, Population 215 Tuberculosis Annual Report Fresno County Department of Public Health
215 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org Number of Cases Rate per 1, Population 215 Tuberculosis Annual Report Fresno County Department of Public Health
TB trends and TB genotyping
 Management of a TB Contact Investigation for Public Health Workers Albuquerque, NM October 1, 214 TB trends and TB genotyping Marcos Burgos MD October 1, 214 Marcos Burgos, MD has the following disclosures
Management of a TB Contact Investigation for Public Health Workers Albuquerque, NM October 1, 214 TB trends and TB genotyping Marcos Burgos MD October 1, 214 Marcos Burgos, MD has the following disclosures
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012
 TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
TB in Prisons and Jails Albuquerque, New Mexico November 28, 2012 Challenges of TB Treatment in Special Populations in Corrections Marcos Burgos, MD November 28, 2012 Marcos Burgos, MD has the following
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Arizona Annual Tuberculosis Surveillance Report
 Arizona Annual Tuberculosis Surveillance Report 2014 Table of Contents I. Executive Summary 1 II. Case Rates 3 III. Cases and Case Rates by Race and Ethnicity 4 IV. Cases by Gender 4 V. Cases and Case
Arizona Annual Tuberculosis Surveillance Report 2014 Table of Contents I. Executive Summary 1 II. Case Rates 3 III. Cases and Case Rates by Race and Ethnicity 4 IV. Cases by Gender 4 V. Cases and Case
2014 Annual Report Tuberculosis in Fresno County. Department of Public Health
 214 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org Tuberculosis (TB) is a common communicable disease caused by the bacterium Mycobacterium tuberculosis and occasionally
214 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org Tuberculosis (TB) is a common communicable disease caused by the bacterium Mycobacterium tuberculosis and occasionally
Haley Blake Sage Nagai, MPH. Disease Investigation and Intervention Specialists Tuberculosis Treatment and Control Clinic
 Haley Blake Sage Nagai, MPH Disease Investigation and Intervention Specialists Tuberculosis Treatment and Control Clinic Discuss the prevalence of tuberculosis in Clark County Describe factors influencing
Haley Blake Sage Nagai, MPH Disease Investigation and Intervention Specialists Tuberculosis Treatment and Control Clinic Discuss the prevalence of tuberculosis in Clark County Describe factors influencing
Essential Mycobacteriology Laboratory Services in the Era of MDR- and XDR-TB: A TB Controller s Perspective
 Essential Mycobacteriology Laboratory Services in the Era of MDR- and XDR-TB: A TB Controller s Perspective James Watt, MD, MPH Acting Chief, Tuberculosis Control Branch California Department of Public
Essential Mycobacteriology Laboratory Services in the Era of MDR- and XDR-TB: A TB Controller s Perspective James Watt, MD, MPH Acting Chief, Tuberculosis Control Branch California Department of Public
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers
 Questions and Answers for Health Care Providers") Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Latent Tuberculosis Infection (LTBI) Questions and Answers for Health Care Providers Who Should Be Screened for Latent Tuberculosis Infection (LTBI)?... 2 What tests are used to screen for LTBI?... 2 How
Annual Tuberculosis Report Oregon 2007
 Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in Alameda County, 2014 Alameda County Public Health Department
 Tuberculosis in Alameda, 214 Alameda Public Health Department Tuberculosis (TB) is a preventable and curable disease that remains one of the leading causes of death worldwide. TB is a communicable disease
Tuberculosis in Alameda, 214 Alameda Public Health Department Tuberculosis (TB) is a preventable and curable disease that remains one of the leading causes of death worldwide. TB is a communicable disease
Tuberculosis & Refugees in Philadelphia
 Tuberculosis & Refugees in Philadelphia Philadelphia TB Control Program Daniel P. Dohony, MPH Philadelphia TB Control Program Health Information Portal Website: hip.phila.gov Contains Information On» Disease
Tuberculosis & Refugees in Philadelphia Philadelphia TB Control Program Daniel P. Dohony, MPH Philadelphia TB Control Program Health Information Portal Website: hip.phila.gov Contains Information On» Disease
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
LTBI monitoring and evaluation in the Netherlands
 LTBI monitoring and evaluation in the Netherlands 17 th Wolfheze Workshops 2015, Den Haag Connie Erkens MD MPH Senior TB consultant Content presentation Epidemiology Target groups for programmatic LTBI
LTBI monitoring and evaluation in the Netherlands 17 th Wolfheze Workshops 2015, Den Haag Connie Erkens MD MPH Senior TB consultant Content presentation Epidemiology Target groups for programmatic LTBI
Please distribute a copy of this information to each provider in your organization.
 HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
HEALTH ADVISORY TO: Physicians and other Healthcare Providers Please distribute a copy of this information to each provider in your organization. Questions regarding this information may be directed to
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis in Alameda County, 2012
 Tuberculosis in Alameda County, 212 Alameda County Public Health Department Tuberculosis Overview Tuberculosis (TB) is a preventable and curable disease that remains one of the leading causes of death
Tuberculosis in Alameda County, 212 Alameda County Public Health Department Tuberculosis Overview Tuberculosis (TB) is a preventable and curable disease that remains one of the leading causes of death
Tuberculosis in Alameda County, 2009
 Tuberculosis in Alameda County, 29 Alameda County Public Health Department Tuberculosis Overview Tuberculosis (TB) is a communicable disease caused by the bacteria Mycobacterium tuberculosis. TB is spread
Tuberculosis in Alameda County, 29 Alameda County Public Health Department Tuberculosis Overview Tuberculosis (TB) is a communicable disease caused by the bacteria Mycobacterium tuberculosis. TB is spread
Interpretation of TST & IGRA results. Objectives
 Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Interpretation of TST & IGRA results Randall Reves, MD, MSc Volunteer Clinician Denver Metro TB Program and Division of Infectious Diseases, Department of Medicine University of Colorado Denver Objectives
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach:
 Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach: Lori A. Soos MA, BSN, RN, Niagara University Deborah Penoyer, MS, RN, SUNY Geneseo Learning
Tuberculosis Screening and Targeted Testing of College and University Students: Developing a Best Practice Approach: Lori A. Soos MA, BSN, RN, Niagara University Deborah Penoyer, MS, RN, SUNY Geneseo Learning
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
11/1/2017. Disclosures. Update In Tuberculosis, Indiana Outline/Objectives. Pathogenesis of M.tb Global/U.S. TB Burden, 2016
 Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
Disclosures Update In Tuberculosis, Indiana 2017 Bradley Allen, MD, PhD, FACP, FIDSA Indiana University School of Medicine Division of Infectious Diseases Roudebush VAMC Indianapolis Medical Consultant,
TB Outbreak Investigation in Fishery Workers, Maryland. Cassandra Althauser PHASE Internship Maryland Department of Health and Human Hygiene
 TB Outbreak Investigation in Fishery Workers, Maryland Cassandra Althauser PHASE Internship Maryland Department of Health and Human Hygiene Airborne Transmission Tuberculosis Small droplet nuclei (
TB Outbreak Investigation in Fishery Workers, Maryland Cassandra Althauser PHASE Internship Maryland Department of Health and Human Hygiene Airborne Transmission Tuberculosis Small droplet nuclei (
ANNUAL TUBERCULOSIS REPORT OREGON Oregon Health Authority Public Health Division TB Program November 2012
 ANNUAL TUBERCULOSIS REPORT OREGON 211 Oregon Health Authority Public Health Division TB Program November 212 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-211... page
ANNUAL TUBERCULOSIS REPORT OREGON 211 Oregon Health Authority Public Health Division TB Program November 212 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-211... page
Who is at Risk of TB?
 Who is at Risk of TB? Lisa Armitige, MD, PhD September 20, 2017 Screening for Tuberculosis Infection September 20, 2017 Harlingen, TX EXCELLENCE EXPERTISE INNOVATION Lisa Armitige, MD, PhD has the following
Who is at Risk of TB? Lisa Armitige, MD, PhD September 20, 2017 Screening for Tuberculosis Infection September 20, 2017 Harlingen, TX EXCELLENCE EXPERTISE INNOVATION Lisa Armitige, MD, PhD has the following
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Contact Investigation San Antonio, Texas January 14-15, 2013
 Contact Investigation San Antonio, Texas January 14-15, 2013 Detecting and Handling a TB Outbreak Jessica Quintero, BAAS January 15, 2013 Jessica Quintero, BAAS has the following disclosures to make: No
Contact Investigation San Antonio, Texas January 14-15, 2013 Detecting and Handling a TB Outbreak Jessica Quintero, BAAS January 15, 2013 Jessica Quintero, BAAS has the following disclosures to make: No
2013 Annual Report Tuberculosis in Fresno County. Department of Public Health
 2013 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org In 2013, provisional data indicates that tuberculosis (TB) affected 3.0 / 100,000 people in the United States
2013 Annual Report Tuberculosis in Fresno County Department of Public Health www.fcdph.org In 2013, provisional data indicates that tuberculosis (TB) affected 3.0 / 100,000 people in the United States
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service
 Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
Primary Care and TB Control Dr Helen Booth Consultant Thoracic Physician, UCLH Clinical Lead, Integrated TB NCL-Service North Central London TB Service TBService@nhs.net After Action Review Could we have
TB Contact Investigation
 Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Investigation of Contacts of Persons with Infectious Tuberculosis, 2005
 1 Investigation of Contacts of Persons with Infectious Tuberculosis, 2005 Daniel P. Dohony, MPH Division of Tuberculosis Elimination Centers for Disease Control and Prevention and Philadelphia TB Control
1 Investigation of Contacts of Persons with Infectious Tuberculosis, 2005 Daniel P. Dohony, MPH Division of Tuberculosis Elimination Centers for Disease Control and Prevention and Philadelphia TB Control
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Tuberculosis in Chicago 2007
 City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
City of Chicago Communicable Disease Information Department of Public Health Richard M. Daley, Mayor May 2008 Terry Mason, MD, FACS, Commissioner www.cityofchicago.org/health/ West Side Center For Disease
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program
 Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program") Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
State of the State in TB Control
 State of the State in TB Control Jason Stout, MD, MHS Wake County TB Medical Consultant NC TB Medical Director Division of Infectious Diseases, Duke University Medical Center Disclosures-Funding NIH (grant)
State of the State in TB Control Jason Stout, MD, MHS Wake County TB Medical Consultant NC TB Medical Director Division of Infectious Diseases, Duke University Medical Center Disclosures-Funding NIH (grant)
Laboratory Diagnosis for MDR TB
 Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
TRANSLATIONAL APPROACHES TO PREDICTING TUBERCULOSIS RISK: FROM ADMINISTRATIVE DATA TO TRANSCRIPTIONAL BIOMARKERS NICHOLAS DAVID WALTER
 TRANSLATIONAL APPROACHES TO PREDICTING TUBERCULOSIS RISK: FROM ADMINISTRATIVE DATA TO TRANSCRIPTIONAL BIOMARKERS by NICHOLAS DAVID WALTER BA, Middlebury College, 1994 MS, University of California, Berkeley,
TRANSLATIONAL APPROACHES TO PREDICTING TUBERCULOSIS RISK: FROM ADMINISTRATIVE DATA TO TRANSCRIPTIONAL BIOMARKERS by NICHOLAS DAVID WALTER BA, Middlebury College, 1994 MS, University of California, Berkeley,
Contact Investigation Overview
 Contact Investigation Overview Jan Dougan, RN May 4, 2017 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Jan Dougan, RN has the following disclosures to make: No conflict
Contact Investigation Overview Jan Dougan, RN May 4, 2017 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Jan Dougan, RN has the following disclosures to make: No conflict
TB Control in Finland - the role of THL
 TB Control in Finland - the role of THL Hanna Soini THL, Department of Health Security 1 TB in Finland 1950-2014 12000 10000 8000 6000 TB ulkomaalaiset TB yhteensä 4000 2000 0 1950 1955 1960 1965 1970
TB Control in Finland - the role of THL Hanna Soini THL, Department of Health Security 1 TB in Finland 1950-2014 12000 10000 8000 6000 TB ulkomaalaiset TB yhteensä 4000 2000 0 1950 1955 1960 1965 1970
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Global TB Burden, 2016 estimates
 TUBERCULOSIS EPIDEMIOLOGY LOCAL, STATE, NATIONAL, GLOBAL Office of Communicable Disease Epidemiology Global TB Burden, 216 estimates Total TB Estimated number of TB cases 1.4 million 14 per 1, Estimated
TUBERCULOSIS EPIDEMIOLOGY LOCAL, STATE, NATIONAL, GLOBAL Office of Communicable Disease Epidemiology Global TB Burden, 216 estimates Total TB Estimated number of TB cases 1.4 million 14 per 1, Estimated
Overview of Contact Investigation Guidelines
 Overview of Contact Investigation Guidelines Jessica Quintero, M.Ed. TB Contact Investigation 101 May 4-5, 2016 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed. has the following
Overview of Contact Investigation Guidelines Jessica Quintero, M.Ed. TB Contact Investigation 101 May 4-5, 2016 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed. has the following
Jennifer Lam MPH candidate 2009 Johns Hopkins Bloomberg School of Public Health. Preceptors: Wendy Cronin, PhD MT(ASCP), Cathy Goldsborough, RN
, Cathy Goldsborough, RN") Jennifer Lam MPH candidate 2009 Johns Hopkins Bloomberg School of Public Health Preceptors: Wendy Cronin, PhD MT(ASCP), Cathy Goldsborough, RN Phase Symposium: May 6, 2009 Background & Rationale Maryland
Jennifer Lam MPH candidate 2009 Johns Hopkins Bloomberg School of Public Health Preceptors: Wendy Cronin, PhD MT(ASCP), Cathy Goldsborough, RN Phase Symposium: May 6, 2009 Background & Rationale Maryland
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE May 8-11, 2018 TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE May 8-11, 2018 TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the
Outline. Tuberculosis (TB) Medical Evaluation for TB 5/5/2014. Chest Radiograph with Lower Lobe Cavity
 Medical Evaluation for TB 5/5/2014. Chest Radiograph with Lower Lobe Cavity") Jean Beinemann RN, Terri Boxrucker RN, and LT Dee Dee Downie MPH Outline The disease The outbreak The response The conclusions May 18, 2014 Wisconsin Public Health Association Annual Meeting Tuberculosis
Jean Beinemann RN, Terri Boxrucker RN, and LT Dee Dee Downie MPH Outline The disease The outbreak The response The conclusions May 18, 2014 Wisconsin Public Health Association Annual Meeting Tuberculosis
Table 9. Policy for Tuberculosis Surveillance and Screening
 Policy for Tuberculosis Surveillance and Screening Purpose: to identify active cases of tuberculosis or latent TB among residents and staff of the nursing home in order to prevent transmission in this
Policy for Tuberculosis Surveillance and Screening Purpose: to identify active cases of tuberculosis or latent TB among residents and staff of the nursing home in order to prevent transmission in this
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Cost-Effectiveness of Preventing Tuberculosis in Prison Populations Zachary Taylor, M.D., M.S., and Cristy Nguyen, M.P.H.
 109 Cost-Effectiveness of Preventing Tuberculosis in Prison Populations Zachary Taylor, M.D., M.S., and Cristy Nguyen, M.P.H. Reported TB Cases, United States, 1953 97 110 Reported TB Cases, United States,
109 Cost-Effectiveness of Preventing Tuberculosis in Prison Populations Zachary Taylor, M.D., M.S., and Cristy Nguyen, M.P.H. Reported TB Cases, United States, 1953 97 110 Reported TB Cases, United States,
2017/2018 Annual Volunteer Tuberculosis Notice
 Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Lewis Center for Educational Research Academy for Academic Excellence Norton Science and Language Academy Business Offices 17500 Mana Road Apple Valley, CA 92307 E-mail: hr@lcer.org 760-946-5414 Fax 760-946-9193
Intensified TB case finding among PLHIV and vulnerable population Identifying contacts Gunta Kirvelaite
 Intensified TB case finding among PLHIV and vulnerable population Identifying contacts Gunta Kirvelaite Riga East Clinical hospital, Centre for tuberculosis and lung diseases. Head of outpatient department.
Intensified TB case finding among PLHIV and vulnerable population Identifying contacts Gunta Kirvelaite Riga East Clinical hospital, Centre for tuberculosis and lung diseases. Head of outpatient department.
LATENT TUBERCULOSIS. Robert F. Tyree, MD
 LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
LATENT TUBERCULOSIS Robert F. Tyree, MD 1 YK TB OFFICERS Ron Bowerman Elizabeth Roll Mien Chyi (Pediatrics) Cindi Mondesir (Pediatrics) The new guys: Philip Johnson Robert Tyree 2009 CDC TB CASE DEFINITION
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Monitoring & evaluation LTBI management in the Netherlands. Key lessons.
 Monitoring & evaluation LTBI management in the Netherlands. Key lessons. Gerard de Vries, MD MSc PhD, Coordinator TB control the Netherlands, KNCV Tuberculosis Foundation/RIVM-CIb Global WHO Consultation
Monitoring & evaluation LTBI management in the Netherlands. Key lessons. Gerard de Vries, MD MSc PhD, Coordinator TB control the Netherlands, KNCV Tuberculosis Foundation/RIVM-CIb Global WHO Consultation
Therapy for Latent Tuberculosis Infection
 Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
Screening and Treatment of LTBI in TB Control in the US Margarita Elsa Villarino MD MPH Division of TB Elimination, CDC April 14, 2004 TB Prevention and Control in the United States The fundamental strategies
9. Screening in Special Situations
 9. Screening in Special Situations Screening is the practice of identifying a condition or illness, which could benefit from early diagnosis, preventative or curative intervention. 318 Screening should
9. Screening in Special Situations Screening is the practice of identifying a condition or illness, which could benefit from early diagnosis, preventative or curative intervention. 318 Screening should