AAA: Latest In Treatment & Technology
|
|
|
- Mark Franklin
- 5 years ago
- Views:
Transcription
1 AAA: Latest In Treatment & Technology Majdi Ashchi, DO, FACC, FSCAI, FSVM, FABVM C (904) W(904)
2 Educate Primary Care Physicians and providers on: AAA incidence Diagnostic modalities, Pros & Cons Surgical, Endovascular or Medical Treatment Options Discuss briefly Endoleak History, Brief Examples of cases Risk Factors If time allows, discuss Popliteal aneurysm

3 NONE DISCLOSURES


4
5 Aneurysm Definition A localized dilatation of the aorta with an increase in diameter of >1.5 times its normal diameter Over the last three decades, incidence has tripled 1.5 million people in the US have AAAs Men present 4:1 over women 15,000 deaths annually due to ruptured AAAs in the US 13 th leading cause of death Most AAAs are infrarenal patients often have other aneurysms, including iliac (41%) and femoropopliteal (15%) Hypertension (30 40%) Smoking (6:1) > 50,000 procedures per year for AAA repair 6

6 AAA Incidence and Location Incidence of aortic aneurysms Each year, physicians diagnose approximately 200,000 people in the United States with AAA. ( pages/patient information)
7 Risk Factors Major Risk Factors Current or former smoker A history of smoking has been associated with a 3- to 5- fold increase in AAA prevalence across all age groups Family history of AAA Age over 60 Gender Abdominal aneurysms are 5-10x more common in men than women 5% of US males over 60 are estimated to have a AAA Incidence significantly increases >55 y.o. men & >70 y.o. in women

8 Most significant concern: risk of rupture Mortality assd with AAA rupture (raaa) Up to 67% die prior to reaching hospital 20% deaths due to rupture die before repair Overall average = 49% Annual deaths from raaa decreased since advancement of EVAR in 1990s Increase in elective repair Improved detection and management of HTN Medicare inpt admissions for raaa Decreased from 23.2 to 12.8/100,000 medicare population AAA
9 Diagnostic Methods History & Physical exam, palpation and auscultation Abdominal Ultrasound Commonly used as a primary screening tool Provides details of the vessel wall and plaque Computed Tomography Arteriography (CTA) Most accurate test to determine size and location Readily available Eliminates the need for invasive angiography but requires IV contrast
10 Aneurysm : History Possible symptoms : Abdominal pain Pain in the lower back that may extend to the buttocks, groin or legs Pulsating sensation in the abdomen Symptoms indicating a rupture : Sudden onset of severe back or abdominal pain Nausea Dizziness, fainting and/or sudden weakness
11 AAA diagnosis Many AAAs are asymptomatic Physical exam Palpable, pulsatile mass mid-abdomen Limited in obese pts Evaluate popliteal fossa 20% pts with AAA will have popliteal aneurysm May (rarely) present with blue toe syndrome Distal embolization of mural thrombus

12 BLUE TOE SYNDROME

13 AAA diagnosis: Imaging Plain film/xray Incidental finding lumbar spine/abdominal film DUS Most common initial dx tool Readily available, low cost No radiation Limitations Can underestimate absolute size Limited role in procedure planning Rules in/rules out USPSTF recommends one-time DUS screening for males 65-75yo who have EVER smoked
14 AAA diagnosis: Imaging CTA Gold standard for absolute size/dimensions Advantages Best spatial resolution of modalities Readily available Multiplanar/3D reconstructions Disadvantages Ionizing radiation Iodinated contrast

15 Preprocedural assessment CT angiography Helical imaging from celiac to CFA mm slice thickness cc iodinated contrast Post processing Sagittal & coronal reconstructions Center line measurements for length Infrarenal neck measurement Iliac diameter, tortuosity, occlusive disease

16 When to Treat DESCRIPTION OF AORTIC ANEURYSM Elective repair of AAA is recommended when the maximal aneurysm diameter is 5.5 cm or more 6 Fusiform Aneurysm Saccular Aneurysm Aneurysms that have a saccular morphology may be considered for repair even if < 5 cm in diameter Aneurysms that have a fusiform morphology may be considered for repair if they are painful, have caused distal embolization, or are rapidly enlarging (>0.5 cm/year) 5
17 AAA Treatment Options Medical Management / Monitor Wait, watch and control hypertension Typically reserved for aneurysms < 5 cm that are not rapidly expanding or causing symptoms Most commonly monitored with regular CT scans or ultrasound examinations
18 AAA: Role of pharmacology Goals Slow rate of growth Reduce perioperative morbidity in AAA repair Reduce CV risk factors which may reduce AAA growth rate Antibx Rx Tetracycline/doxycycline/roxithromycin Small studies Aneurysm expansion decreased vs. placebo Statins Affect MMP-9 expression in cell cultures At least 2 studies showing attenuation of aneurysm growth ACE inhibitors Small studies showing less aneurysm growth, less likely to present with rupture
19 AAA Treatment Options Surgical Treatment Elective repair has a perioperative mortality rate of about 3 5% 22-30% morbidity High risk surgical group includes: cardiac, renal, pulmonary disease, and morbid obesity Patients > 75 years of age have a higher perioperative mortality rate Average 7 to 10 days hospitalization Emergency repair: mortality 40 50% Coronary events are the leading cause of death following repair of AAAs
20 AAA Treatment Options Rupture Risk Diameter (cm) (% per year) < > 8 0% 0.5-5% 3-15% 10-20% 20-40% 30-50% AAA Expansion Rate 14 Although a number of studies have found that small AAAs expand at approximately 0.5 cm in diameter per year, individual patients show considerable variation in aneurysm expansion rates
21 AAA natural history: Rupture risk (ROR) Maximum AAA diameter (cm) 5-yr rupture rate (%) <4.0 2 UK Small Aneurysm Trial: Females 3x ROR vs. males >7.0 75

22 Open Surgical Repair Results of Standard Open Repair Effective and durable but 4-5% mortality in population-based studies 15,16,17 Recovery 2-4 months 18 High risk patients often denied repair 19 5-year survival rate of 46% 9
 Anchoring and secure fixation of endoluminal device above")

23 Endovascular Repair Principles of Endovascular Aortic Repair (EVAR) Anchoring and secure fixation of endoluminal device above and below AAA in normal arterial segments Hemostatic seals exclude AAA from circulation Exclusion and depressurization prevent AAA rupture
24 Endovascular Aneurysm Repair (EVAR) Initial work 1991 Parodi Initial FDA approval of 2 devices (AneuRx & Ancure) 1999 At least 6 currently approved devices Medtronic Talent Medtronic AneuRx Cook Zenith Gore Excluder Endologix Powerlink Several other devices undergoing investigation
25 AAA devices-soup Aptus: Endostaple, FDAapproved but not the graft; Bolton: Treovance, not approved; Cook: Zenith; Zenith Flex, FDA-approved; Zenith LP, not approved; and now Zenith Fenestrated, FDAapproved - customized; Cordis: Incraft, not approved; Endologix: Powerlink, FDA-approved; Nellix, not approved; Gore: Excluder; Excluder C3, FDAapproved; Lombard: Aorfix, not approved; Medtronic: AneuRx; Talent; Endurant, all FDA-approved; Trivascular: Ovation, HDE FDA approved; Vascutek: Anaconda, not approved.
26 The evolution of EVAR Advantages Less perioperative morbidity & mortality 25% fewer cardiac/pulmonary complications Fewer ICU days Shorter LOS Disadvantages Long term data limited vs. open repair Follow-up more regimented 1-3m, 6m, 12m, annual CT/CTA Contrast/Radiation concerns Anatomy dependent Not everyone a candidate for EVAR
27 The evolution of EVAR Clinical evidence EVAR EVAR vs 539 open repair 30-day mortality EVAR 1.7% vs open 4.7% 2 intervention rate EVAR 9.8% vs open 5.8% All-cause mortality ~28% 4yr 3% less aneurysm-related death with EVAR EVAR more expensive, higher reintervention
28 The evolution of EVAR Practice trends Increasing # AAAs treated with EVAR vs. open Device improvements Lower profile delivery systems Reliable closure devices Many physicians now performing EVAR percutaneously




29 Device toolbox

30
31 AAA Endovascular Repair Potential Benefits of EVAR Shorter hospital stay; 1-3 days vs days Safer option for high risk patients: most have significant concomitant disease (e.g., CAD, COPD) Anesthesia: General = shorter time and less blood loss Regional = epidural Local = percutaneous (closure devices) Overall lower morbidity Lower mortality rate Patient comfort
32 AAA Endovascular Repair (EVAR) Lower operative mortality rate than open repair Lower operative mortality rate for ruptured AAA than open repair Short recovery period EVAR allows patients who were felt to be inoperable to be operated upon now; as a result of the lower operative mortality rates. However EVAR does not improve long term survival compared to open repair due to the very short long term survival rate among AAA patients and some late ruptures in the EVAR patients (In EVAR 1, a total of 524 of the 1252 patients (42%) Patients died during a median follow up of 6 years, but only 76 (5%) died of aneurysm rupture.)
33

34

35

36

37 snorkling

38


39 Case 86yo WM presents to ER with increasing abd pain


40 EVAR: 86 yo WM

41 Post-EVAR follow-up CT gold standard Precontrast Important to see Ca++ thrombus Arterial phase CTA protocol Best for detecting large endoleaks Delayed Can detect slow-filling, late endoleak Especially important if aneurysm sac expanding
42 Endoleak Filling and/or pressurization of the aneurysm sac following EVAR?? Is pressurization sufficient to confer same risk of rupture based on sac size?? Type 1 Proximal at infrarenal neck Distal at distal attachment site (usually common iliac arteries Frequently due to aneurysmal degeneration of neck or device migration ( passive fixation ) Type 2 Retrograde Usually from paired lumbar arteries & IMA** Type 3 At junction/overlap of graft components Type 4 porosity leak graft material/procedural anticoagulation
43 Type 1 endoleak Usually detected intraoperatively Can develop late infrarenal neck degenerates or graft undersized Resulting in device migration (passive fixation) Usually very obvious Confers significant rupture risk Treated by extension cuff


44 Type 1 endoleak


45 Type 1 endoleak
46 Type 2 endoleak Represents persistent flow in sac Requires inflow & outflow Usually from large IMA or paired lumbar arteries Can occur from ANY branch that arises from aneurysm sac Accessory renal arteries Questionable as to pressurization and rupture risk Frequently resolve spontaneously Usually only treated in setting of sac enlargement


47 Type 2 endoleak - lumbar


48 Type 2 endoleak - embolization




49 Type 2 endoleak IMA & acc renal
50 Post-EVAR follow-up Protocol Routine post-op office visit 1-2weeks Contrast-enhanced 3m, 6m, 12m, annually thereafter if no endoleak May be able to use DUS in good hands with plenty of time In CRI pts, may use DUS or noncontrast CT to assess sac size Limited info

51 Post-EVAR follow-up Other imaging Ultrasound Can be used for pts w/cri Tech-dependent, labor-intensive MRA Limited role Nuclear medicine Ability to detect late endoleak but not source Much less spatial resolution
52 Conclusion AAA frequently discovered incidentally Lspine films, CT for other reasons Early AAA dx potentially saves lives Screening efforts warranted in at risk groups EVAR assd with less periop M&M Technology improvement has led to EVAR now 60-70% all aneurysm repair 2 intervention more common with EVAR Most pts willing to accept this for easier recovery


53 g GORE DEVICE
54 Iliac Artery Aneurysms
55 Iliac artery aneurysms are similar to AAA except Harder to diagnose due to they inaccessible location to palpation and ultrasound Higher mortality rate than AAA if the rupture Usually associated with AAA Operate when they reach 3 cm Most are treated with endovascular techniques

56
57
58
59 Popliteal Artery Aneurysms
60 Definition If the enlargement is 1.5 times the size of the diameter of the normal adjacent segment of artery. Most clinicians consider 2 cm as the threshold diameter for a popliteal artery aneurysm All should be operated upon to prevent complications
61 Popliteal artery aneurysms are different! Most present as asymtomatic pulsating mass behind the knee Or they cause chronic or acute ischemia due to thrombosis of the entire popliteal artery or due to distal embolization. Very unlikely to rupture as other aneurysms do; 0-7% in most series.
62
63 epidemiology Occur basically in men; 95% + Frequently bilateral;50% Associated with abdominal aortic aneurysms: 36% Most common aneurysm of the lower leg;70%. They are relatively uncommon: 7.4 per 100,000 people. In a patient treated for a popliteal artery aneurysm the likelihood of developing an other aneurysm at a remote site in the next 10 years is estimated at 50%
64 Diagnosis Important to diagnose before symptoms or complication occur, especially acute limb ischemia. Physical examination may reveal a prominent pulsation felt in the popliteal space, especially with the knee in moderate flexion. Duplex ultrasound is clearly the screening test of choice and has been shown to be superior to physical examination in detecting popliteal artery aneurysms.
65 Imaging Once a decision has been made to treat, additional anatomical information is required. Traditionally, contrast-enhanced angiography has been best used to identify points of inflow and suitable outflow target vessels for bypass

66

67
68 Natural History Popliteal artery aneurysms are an insidious process that may cause no symptoms for an extended period of time. Frequently, the first evidence of their presence is an ischemic complication. It must be recognized that the natural history of many popliteal artery aneurysms is one of progressive enlargement and the ultimate development of symptoms or ischemic complications or both. The most feared complication is irreversible limb ischemia requiring amputation secondary to either sudden aneurysm thrombosis or extensive distal embolization. On average, the risk of developing thromboembolic complications was 35% in three years with amputation rate of 25%. In cases with nonpulsatile pulses on initial presentation the likelihood of complications is far higher (86%).
69 Elective Surgical Treatment The primary objective of treatment of popliteal artery aneurysms is to exclude them from the circulation. Two approaches; medical and posterior Small or fusiform aneurysms are best approached medially by conventional bypass with aneurysm ligation. For large, saccular aneurysms, particularly those with symptoms attributable to compression or adjacent structures, direct exposure from the posterior approach with interposition grafting within the sac is preferable unless an aneurysm extends too far proximally.
70
71 Elective Surgical Treatment For large, saccular aneurysms, particularly those with symptoms attributable to compression or adjacent structures, direct exposure from the posterior approach with interposition grafting within the sac is preferable unless an aneurysm extends too far proximally.

72

73
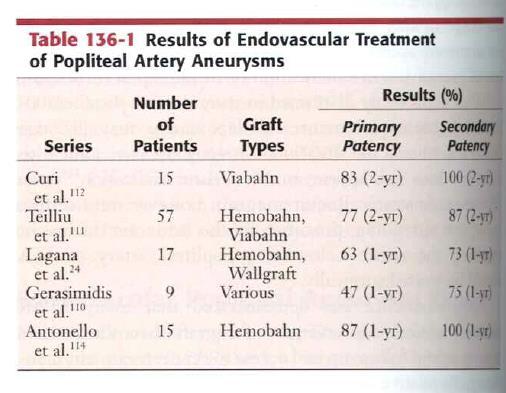
74 Endovascular Popliteal Artery Aneurysm Repair (EPAR) Currently, long-term results of EPAR are unknown and the short-term results generally demonstrate patency rates inferior to those of open surgery and a higher rate of re-intervention. Most surgeons have generally reserved EPAR for patients in whom the risk related to anesthesia and surgery are prohibitive and who have appropriate anatomy for endograft implantation.
75
76 Endovascular Popliteal Artery Aneurysm Repair (EPAR) As with endovascular abdominal aortic aneurysm repair EPAR is constrained by primary anatomy. Patients with thrombosed aneurysms or occluded SFA cannot have a stent graft placed and require conventional surgical bypass.
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Current Status of EVAR for Infrarenal AAA. 31 st Annual Florida Vascular Society. PENN Surgery
 Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Optimizing Accuracy of Aortic Stent Grafts in Short Necks
 Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
Current Status of Abdominal Aortic Stent Grafts. John R. Laird Professor of Medicine Director of the Vascular Center UC Davis Medical Center
 Current Status of Abdominal Aortic Stent Grafts John R. Laird Professor of Medicine Director of the Vascular Center UC Davis Medical Center Autumn Greetings Disclosure Statement of Financial Interest Within
Current Status of Abdominal Aortic Stent Grafts John R. Laird Professor of Medicine Director of the Vascular Center UC Davis Medical Center Autumn Greetings Disclosure Statement of Financial Interest Within
Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag
 Let the CAT Scan Out of the Bag") Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag Joseph-Vincent V. Blas, MD Division of Vascular Surgery Department of Surgery Greenville Health System University of South
Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag Joseph-Vincent V. Blas, MD Division of Vascular Surgery Department of Surgery Greenville Health System University of South
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
Management of Endoleaks
 Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Faculty Disclosure. Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management. Background.
 Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management Faculty Disclosure I disclose the following financial relationships: UCSF Vascular Symposium 2013 Receive grant/research
Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management Faculty Disclosure I disclose the following financial relationships: UCSF Vascular Symposium 2013 Receive grant/research
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
A New EVAR Device for Infrarenal AAAs
 A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS
 Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
Disclosures. EVAR follow-up: actual recommendation. EVAR follow-up: critical issues
 Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Abdominal Aortic Aneurysm 가천대길병원 이상준
 Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
 Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
Young-Guk Ko, M.D., Dangas G, J Am Coll Cardiol Intv 2012;5:1071 All-cause Mortality Dangas Severance G, J Am Coll Cardiovascular Cardiol Intv Hospital, 2012;5:1071 Yonsei University Health System Aneurysm-related
Ovation. Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic
 Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Degeneration of the Neck Post Implementation - a New Era of AAA Stent
 Degeneration of the Neck Post Implementation - a New Era of AAA Stent New Mexico Heart Institute Albuquerque, New Mexico USA - Gore Current FDA-Approved EVAR Devices Sealing Mechanism Endologix Lombard
Degeneration of the Neck Post Implementation - a New Era of AAA Stent New Mexico Heart Institute Albuquerque, New Mexico USA - Gore Current FDA-Approved EVAR Devices Sealing Mechanism Endologix Lombard
INCRAFT system: Update from the Pivotal INSPIRATION Study
 INCRAFT system: Update from the Pivotal INSPIRATION Study Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh
INCRAFT system: Update from the Pivotal INSPIRATION Study Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC
 Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton, FL, USA Disclosures
Anatomy-Driven Endograft Selection for Abdominal Aortic Aneurysm Repair S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton, FL, USA Disclosures
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Technique and Tips for Complicated AAA Cases with Stent Graft
 Technique and Tips for Complicated AAA Cases with Stent Graft Seung-Woon Rha, MD, PhD FACC, FAHA, FESC, FSCAI, FAPSIC Cardiovascular Center, Korea University Guro Hospital Mar 15, 2018 LINC AP 2018 Endoleak;
Technique and Tips for Complicated AAA Cases with Stent Graft Seung-Woon Rha, MD, PhD FACC, FAHA, FESC, FSCAI, FAPSIC Cardiovascular Center, Korea University Guro Hospital Mar 15, 2018 LINC AP 2018 Endoleak;
Management of Endoleaks
 Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Trattamento Endovascolare degli Aneurismi dell Aorta Addominale con Colletto Prossimale Ostile:
 Trattamento Endovascolare degli Aneurismi dell Aorta Addominale con Colletto Prossimale Ostile: Risultati Precoci e a Medio Termine in Esperienza Monocentrica A.Lauricella - R.Silingardi Chirurgia Vascolare,
Trattamento Endovascolare degli Aneurismi dell Aorta Addominale con Colletto Prossimale Ostile: Risultati Precoci e a Medio Termine in Esperienza Monocentrica A.Lauricella - R.Silingardi Chirurgia Vascolare,
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Conflicts of Interest. When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Summary. Infrarenal EVAR for short necks 2y postop
 When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
Less Invasive EVAR Transitioning to a Fast-Track Protocol
 Less Invasive EVAR Transitioning to a Fast-Track Protocol Mario Lachat, MD University of Zurich Department of Cardiovascular Surgery Switzerland LINC 2015 1 Disclosure Speaker name: Mario Lachat, MD I
Less Invasive EVAR Transitioning to a Fast-Track Protocol Mario Lachat, MD University of Zurich Department of Cardiovascular Surgery Switzerland LINC 2015 1 Disclosure Speaker name: Mario Lachat, MD I
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment
 Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY
 SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
Popliteal Artery Aneurysms: Diagnosis and Repair Options
 Deepak N. Deshmukh DO April 27, 2018 Popliteal Artery Aneurysms: Diagnosis and Repair Options No Disclosures Popliteal Artery Aneurysms (PAAs) Male Predominanace Most common peripheral Aneurysm (70%) 30-50%
Deepak N. Deshmukh DO April 27, 2018 Popliteal Artery Aneurysms: Diagnosis and Repair Options No Disclosures Popliteal Artery Aneurysms (PAAs) Male Predominanace Most common peripheral Aneurysm (70%) 30-50%
TriVascular Ovation Prime Abdominal Stent Graft System
 TriVascular Ovation Prime Abdominal Stent Graft System Science of the Seal O-Ring Sealing Technology O-Ring Sealing in Proven Engineering Solutions O-rings are designed to seal by blocking the flow of
TriVascular Ovation Prime Abdominal Stent Graft System Science of the Seal O-Ring Sealing Technology O-Ring Sealing in Proven Engineering Solutions O-rings are designed to seal by blocking the flow of
LOWERING THE PROFILE RAISING THE BAR
 LOWERING THE PROFILE RAISING THE BAR INNOVATIVE LOW PROFILE. ADVANCED CLINICAL PERFORMANCE. The AFX TM Endovascular AAA System integrates anatomical fixation with an advanced delivery system and graft
LOWERING THE PROFILE RAISING THE BAR INNOVATIVE LOW PROFILE. ADVANCED CLINICAL PERFORMANCE. The AFX TM Endovascular AAA System integrates anatomical fixation with an advanced delivery system and graft
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
NEW INNOVATIONS IN ENDOLEAK MANAGEMENT
 DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
Considerations for a Durable Repair
 Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS)
") Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Hostile Proximal Neck: A New Conformable EVAR Device
 Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Use of Aptus Heli-FX EndoAnchor implants with standard endografts to strengthen seal in hostile anatomies:
 Use of Aptus Heli-FX EndoAnchor implants with standard endografts to strengthen seal in hostile anatomies: technical tips, case experience and clinical results CACVS Medtronic Symposium Paris, France January
Use of Aptus Heli-FX EndoAnchor implants with standard endografts to strengthen seal in hostile anatomies: technical tips, case experience and clinical results CACVS Medtronic Symposium Paris, France January
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry
 Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm
 Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Endovascular options of treating iliac aneurysms
 Endovascular options of treating iliac aneurysms Marek Majewski Department of Vascular Surgery of P. Desgranges Henri Mondor Hospital University Paris XII Créteil, France Common Iliac Artery Aneurysms
Endovascular options of treating iliac aneurysms Marek Majewski Department of Vascular Surgery of P. Desgranges Henri Mondor Hospital University Paris XII Créteil, France Common Iliac Artery Aneurysms
Prospective Study of the E-liac Stent Graft System in Patients with Common Iliac Artery Aneurysm: 30-Day Results
 Prospective Study of the E-liac Stent Graft System in Patients with Common Iliac Artery Aneurysm: 30-Day Results J. Brunkwall MD, Ph.D, FEBVS On behalf of the Pliant study groups E-liac Stent Graft System
Prospective Study of the E-liac Stent Graft System in Patients with Common Iliac Artery Aneurysm: 30-Day Results J. Brunkwall MD, Ph.D, FEBVS On behalf of the Pliant study groups E-liac Stent Graft System
Evolution of gender-related differences in outcome of EVAR
 Evolution of gender-related differences in outcome of EVAR Erik Debing Department of Vascular Surgery University Hospital Brussels Disclosure Speaker name: ERIK DEBING... I have the following potential
Evolution of gender-related differences in outcome of EVAR Erik Debing Department of Vascular Surgery University Hospital Brussels Disclosure Speaker name: ERIK DEBING... I have the following potential
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES
 CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED.
 EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED. A/Prof. B. Patrice Mwipatayi MD, MMed (Surg), MClinEd (Melb), FCS, FRACS Department of Vascular Surgery, Royal
EXPERIENCE AFTER 500 ENDOLUMINAL STENT GRAFTS. DEVICES SPECIFIC OUTCOME AND LESSONS LEARNED. A/Prof. B. Patrice Mwipatayi MD, MMed (Surg), MClinEd (Melb), FCS, FRACS Department of Vascular Surgery, Royal
Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy!
 We have a Durable Solution to Short Necks That s so Easy!") Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy! David H. Deaton, MD Vascular Surgery / University of South Carolina / Palmetto Health Chief Medical
Now that Endoanchors are Approved (and paid for) We have a Durable Solution to Short Necks That s so Easy! David H. Deaton, MD Vascular Surgery / University of South Carolina / Palmetto Health Chief Medical
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
Reduction in cardiovascular related adverse events following active sac management with Nellix vs. EVAR: Are there biological advantages?
 February 1, 2018 Reduction in cardiovascular related adverse events following active sac management with Nellix vs. EVAR: Are there biological advantages? Patrick Berg M.D. Marienhospital Kevelaer Germany
February 1, 2018 Reduction in cardiovascular related adverse events following active sac management with Nellix vs. EVAR: Are there biological advantages? Patrick Berg M.D. Marienhospital Kevelaer Germany
Abdominal Aortic Aneurysm (AAA)
") Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Aortic Triumph or Tragedy. Sean Lyden, MD Cleveland Clinic Cleveland, Ohio
 Aortic Triumph or Tragedy Sean Lyden, MD Cleveland Clinic Cleveland, Ohio Disclosures Consultant: Phillips, Endologix, Shockwave, Abbott, BSC, Medtronic, PQ Bypass VIVA Physicians 501c3 Board Member Stock
Aortic Triumph or Tragedy Sean Lyden, MD Cleveland Clinic Cleveland, Ohio Disclosures Consultant: Phillips, Endologix, Shockwave, Abbott, BSC, Medtronic, PQ Bypass VIVA Physicians 501c3 Board Member Stock
Durability of The Endurant Stent-Graft through 5 Years
 Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Hypogastric Preservation Using Retrograde Endovascular Bypass
 Hypogastric Preservation Using Retrograde Endovascular Bypass Mathew Wooster MD, Adam Tanious MD, Brad Johnson MD, Murray Shames MD, Paul Armstrong MD, Martin Back MD Florida Vascular Society 30 th Annual
Hypogastric Preservation Using Retrograde Endovascular Bypass Mathew Wooster MD, Adam Tanious MD, Brad Johnson MD, Murray Shames MD, Paul Armstrong MD, Martin Back MD Florida Vascular Society 30 th Annual
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Is EVAS a proper choice in women?
 Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts
 Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
EndoVascular Aneurysm Sealing (EVAS) with Nellix
 with Nellix") 1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Improving Endograft Durability with EndoAnchors
 Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU)
") October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair
 583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs
 How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
PERPHERAL ARTERY ANEURYSM. By Pooja Sharma and Susanna Sebastianpillai
 PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
Abdominal Aortic Aneurysm
 Abdominal Aortic Aneurysm David N. Duddleston, MD VP and Medical Director Southern Farm Bureau Life Jackson, Mississippi A Case Ms. Ima Bolgin,, age 54, $1.2 million, sent to you for review. Smoker, ½
Abdominal Aortic Aneurysm David N. Duddleston, MD VP and Medical Director Southern Farm Bureau Life Jackson, Mississippi A Case Ms. Ima Bolgin,, age 54, $1.2 million, sent to you for review. Smoker, ½
EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes?
 D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes? Disclosures Speaker name: Dittmar Böckler
D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes? Disclosures Speaker name: Dittmar Böckler
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type 1b Endoleak following an EVAR for Ruptured AAA
 Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
EVAS How does this Impact EVAR Therapy
 EVAS How does this Impact EVAR Therapy John S. Lane III, MD, FACS Professor and Acting Chief of Vascular Surgery University of California, San Diego PNEC, 2017 Endologix products and associated components
EVAS How does this Impact EVAR Therapy John S. Lane III, MD, FACS Professor and Acting Chief of Vascular Surgery University of California, San Diego PNEC, 2017 Endologix products and associated components
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Endoleak Sealing after AAA Endovascular Repair. When and How?
 Endoleak Sealing after AAA Endovascular Repair. When and How? Poster No.: C-1086 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Quintana Blanco, B. González Humara, E. Torres Diez, C. Jimenez
Endoleak Sealing after AAA Endovascular Repair. When and How? Poster No.: C-1086 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Quintana Blanco, B. González Humara, E. Torres Diez, C. Jimenez
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany
 Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability. Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands
 GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS
 for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS") Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS Saritphat Orrapin MD FRCS (Thailand), Thoetphum Benyakorn, Tunyarat
Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS Saritphat Orrapin MD FRCS (Thailand), Thoetphum Benyakorn, Tunyarat
Shonak Patel MD Vascular Specialists of Central Florida Assistant Professor at UCF
 Shonak Patel MD Vascular Specialists of Central Florida Assistant Professor at UCF Evaluating Aortic Disease Consider the process degenerative Atherosclerosis, dissection, connective tissue disease Treatment
Shonak Patel MD Vascular Specialists of Central Florida Assistant Professor at UCF Evaluating Aortic Disease Consider the process degenerative Atherosclerosis, dissection, connective tissue disease Treatment
14F OD Ovation Abdominal Stent Graft System
 14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
Durable outcomes. Proven performance.
 Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
Technology. The introduction of endovascular aortic repair. cover story
 Infrarenal EVAR Technology Review Steady evolution in device design and delivery has expanded endovascular repair to more patients, but further advancements are integral to this technology s future. By
Infrarenal EVAR Technology Review Steady evolution in device design and delivery has expanded endovascular repair to more patients, but further advancements are integral to this technology s future. By
Mid-term results from ANCHOR: How does this data influence the treatment algorithm for hostile EVAR anatomies
 Mid-term results from ANCHOR: How does this data influence the treatment algorithm for hostile EVAR anatomies Jean-Paul P.M. de Vries Head Department of Surgery, University Medical Centre Groningen The
Mid-term results from ANCHOR: How does this data influence the treatment algorithm for hostile EVAR anatomies Jean-Paul P.M. de Vries Head Department of Surgery, University Medical Centre Groningen The
Redo treatment and open conversion after TEVAR
 Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Redo treatment and open conversion after TEVAR Roberto Chiesa Vascular Surgery, Vita-Salute University Scientific Institute San Raffaele Milan, Italy Number of procedures Off-Label indications for TEVAR
Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster
 Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster RICHARD R. HEUSER, MD, FACC, FACP, FESC, FASCI Director Of Cardiology, St. Luke s Medical Center, Phoenix, Arizona
Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster RICHARD R. HEUSER, MD, FACC, FACP, FESC, FASCI Director Of Cardiology, St. Luke s Medical Center, Phoenix, Arizona
When and where EVAR patients should be discharged?
 When and where EVAR patients should be discharged? Joost A. van Herwaarden University Medical Center Utrecht The Netherlands Disclosure of Interest I have the following potential conflicts of interest
When and where EVAR patients should be discharged? Joost A. van Herwaarden University Medical Center Utrecht The Netherlands Disclosure of Interest I have the following potential conflicts of interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
Treatment options of late failures of EVAS. Michel Reijnen Rijnstate Arnhem The Netherlands
 Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Endoanchor-assisted TEVAR
 Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Endoanchor-assisted TEVAR May 29, 2015 NCVH2015 Grayson H. Wheatley III, MD Director of Aortic and Endovascular Surgery Associate Professor of Surgery Temple University School of Medicine Disclosures Consultant
Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Surgery Original Policy Date: December 7, 2011 Subject:
 Endovascular Stent Grafts for Abdominal Aortic Last Review Status/Date: September 2016 Page: 1 of 21 Description Endovascular grafts are minimally invasive alternatives to open surgical repair for treatment
Endovascular Stent Grafts for Abdominal Aortic Last Review Status/Date: September 2016 Page: 1 of 21 Description Endovascular grafts are minimally invasive alternatives to open surgical repair for treatment