SNAP, CRACKLE, POP. Randy L Aldret, EdD, ATC, LAT Stephanie Aldret, DO, CAQSM OOA Winter CME Seminar January 26, 2018
|
|
|
- Nathaniel Hicks
- 5 years ago
- Views:
Transcription











1 SNAP, CRACKLE, POP Randy L Aldret, EdD, ATC, LAT Stephanie Aldret, DO, CAQSM OOA Winter CME Seminar January 26,




2 OBJECTIVES Review terms to describe fractures Identify fractures that can be treated in the primary care office Review the important history and patient symptoms for various fractures Describe the physical exam findings and diagnostic tests for various fractures Describe the common management of the discussed disorders ON-FIELD/SIDELINE MANAGEMENT 2



3 INITIAL ASSESSMENT Circulation, Airway, Breathing Neurovascular function Motor function and Sensory Pulses, Color, Temperature, and Turgor Examine for tenderness and range of motion Perform a complete examination for other injuries LOC Spine Systemic injuries High index of suspicion based on mechanism of injury Immobilize while waiting for X-ray Provide analgesia Immediate fracture reduction if neurovascular compromise, severe displacement or skin tenting TYPES OF FRACTURES Traumatic Stress/Fatigue Pathologic 3


4 FRACTURE BASICS Anatomic Location Fracture Patterns Alignment Soft Tissue Status Neurovascular Status Associated Injuries ANATOMIC DESCRIPTION OF FRACTURES Location Usually use a descriptor, then document the location on the bone Examples are: distal radial shaft proximal 1/3 humeral shaft intra-articular distal tibia Note describe proximal/distal, intra-articular/extra-articular first, then bone part involved 4


5 ANATOMIC DESCRIPTION OF FRACTURES Type Overall fracture pattern Examples Spiral Segmental Transverse TYPES OF FRACTURES The severity of a fracture usually depends on the amount of force that caused the break. There are many types of fractures including: Nondisplaced fracture Typically stable Displaced fracture Often requires surgery to put the pieces back together Reduction = manipulation of fracture to restore anatomy Open fracture Broken bones that break through the skin are called open, or compound and involve much more damage to the surrounding muscles, tendons, and ligaments Open fractures have a higher risk for complications and take a longer time to heal Closed fracture Although the skin is not broken, internal soft tissues can still be badly damaged Comminuted fracture Unstable The bone shatters into three or more pieces AAOS, Patient Information 5



6 ANATOMIC DESCRIPTION OF FRACTURES Displacement The position where pieces of a fracture have moved from their normal location Fractures can be displaced or non-displaced Displacement is subdivided into 3 sub-categories: Translation Angulation Shortening Translation Angulation Shortening 6

 Mildly comminuted ( Butterfly fragment ) Severely Comminuted AVULSION FRACTURES")
 bone to which it is attached These type of fracture can occur throughout the")
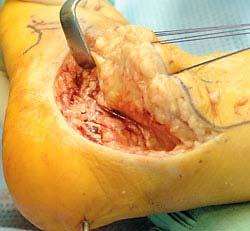
7 ANATOMIC DESCRIPTION OF FRACTURES Comminution The measure of the number of pieces of broken bone Often times this is a subjective assessment. Examples are: non-comminuted, mildly comminuted or severely comminuted Noncomminuted (Simple) Mildly comminuted ( Butterfly fragment ) Severely Comminuted AVULSION FRACTURES An avulsion fracture occurs when an injury causes a ligament or tendon to tear off (avulse) bone to which it is attached These type of fracture can occur throughout the skeleton The layman calls these chip fractures 7

 Five types")



8 SALTER-HARRIS CLASSIFICATION Only used for pediatric fractures that involve the growth plate (physis) Five types (I-V) SH Type II fracture, middle phalanx, right ring finger SH Type I fracture of the distal radius Displaced, SH Type II fracture, distal tibia SH Type IV fracture, distal tibia SH Type III fracture distal tibia 8



9 Usually a result of high energy trauma Open vs Closed SOFT TISSUE STATUS Graded by amount of soft tissue damage, energy of trauma and contamination Grade 1: wound < 1 cm, low energy and contamination Grade 2: wound 1 > 10cm, moderate energy and contamination Grade 3: wound > 10cm, high energy and gross contamination Swelling A: adequate coverage B: inadequate coverage, C: circulation impaired BLOOD SUPPLY TO BONE 9

10 ANATOMIC DESCRIPTION OF FRACTURES Describe each of the following in your report: Type Comminution Location Displacement / Translation / Shortening TREATMENT Immobilization of fracture Cast, splint or brace Traction External fixation Intramedullary nails, pins, k-wires Plate and screws, tension band wires Lag screw S T A B I L I T Y 10



11 TREATMENT In general: intra-articular fractures require anatomic reduction and rigid fixation Shaft fractures require less anatomic alignment and less rigid fixation Exception: radial shaft fractures General Concepts General Indications for Surgery: 1. Open fractures 2. Unstable fractures 3. Irreducible fractures 4. Multiple fractures 5. Fractures with bone loss 6. Fractures with tendon involvement Unstable Stable 11


12 CAST, SPLINT, CAST BRACE Advantages Non invasive Inexpensive Relatively easy to apply Disadvantages Lead to stiffness and muscle atrophy Not rigid, can not hold length Skin breakdown 12
13 First, do no harm. CASTING Most extremity injuries and stable fractures are immobilized in a position of function. Make sure that the skin is both clean and dry prior to the application of the cast or splint. No joint should be immobilized unnecessarily. When estimating the length of stockinette necessary for a short-arm or short-leg cast, make sure to allow extra so that it can be folded back and incorporated into the cast to create a finished edge. When applying cast padding, be sure to adequately pad bony prominences. Consider using materials that will allow the patient to get the cast wet. To facilitate application of the fiberglass casting tape, it should be rolled on with the roll positioned up (as if you were unrolling a rug). Apply it in a spiral fashion to the extremity, overlapping approximately 50 percent. Keep in mind that the curing time for most fiberglass products is 2-4 minutes, depending upon the brand name, type of product, and technique. Cast or splint molding should be performed until material is set, approximately 3 minutes after activated in water. Simple treatment with a cast and discharge before following the patient through a well-guided rehabilitation program is incomplete treatment. All dislocations must be reduced as soon as possible. Closed fractures do not constitute an emergency, unless there is evidence of neurovascular injury or impending skin breakdown. It is vital to give patients both verbal and take-home instructions concerning cast care. CASTING AFTER CARE INSTRUCTIONS Always make sure you have discussed proper cast/splint care with the patient and family, if appropriate. Document that you have done this. Items to cover include, but are not limited to, the following: Elevation of the injured extremity to help reduce swelling. Signs that the cast/splint is too tight include progressive pain, numbness/tingling, coldness, difficulty moving neighboring joints, and color changes in the extremity (pale or blue). Keep the cast/splint dry (unless special materials have been used). If a plaster cast/splint becomes wet, it needs to be replaced. If a fiberglass cast/splint becomes wet, the patient may try using a blow drier on a low heat setting. Do not put anything under the cast, as this could create pressure points, resulting in skin breakdown. Encourage patients to move nonimmobilized joints to enhance fluid return and decrease swelling. Allow adequate time for the cast/splint to harden before stressing it. 13










14 14







15 EXTERNAL FIXATION Advantages Allows access to soft tissue Can maintain length Disadvantages Invasive Not very rigid Indirect reduction Pin tract infections INTRAMEDULLARY NAIL Advantages Do not disrupt periosteal blood supply Can maintain length Allow for early ROM Disadvantages Invasive Indirect reduction 15






16 PLATE AND SCREWS, LAG SCREW Advantages: Most rigid Allows for direct reduction > Anatomic alignment Allows for early ROM Disadvantages Strips blood supply to bone Nondisplaced, transverse fracture of the scaphoid 16






17 17

18 SUMMARY Fracture management dictated by: Location Fracture pattern Soft tissue status Patient Factors (age, associated injuries) Fixation is a balance between rigidity and violation of the soft tissues Remember what to include in the description of fractures Type Comminution Location Displacement/Translation/Shortening Simple, transverse, non-communited midshaft radial and ulnar fractures with 30 degrees apex radial angulation. 18


19 Transverse, midshaft fractures of radius and ulna with complete displacement, shortening and ulnar angulation of the radial fracture Displaced, transverse, radial shaft fracture at the junction of the mid and distal thirds with accompanying subluxation of the distal radio-ulnar joint(druj). Management: in adults, requires surgical open reduction of the distal radius and DRUJ with internal fixation. In children the fracture can often be treated by closed reduction. 19

20 Greenstick fracture Incomplete, one cortex is not fractured (may be bowed or bent, but not fractured). Nondisplaced, 2 bone forearm shaft fractures at the junction prox. and mid. thirds in a growing skeleton. 20


21 Nondisplaced, transverse fracture of the ulna at the junction of the proximal and middle shaft. Night-stick fracture Treatment: Nondisplaced cast May require ORIF if displacement occurs Transverse, dorsally angulated, extraarticular fracture of the distal radius with an associated ulnar styloid fracture (Colle s Fracture) When describing fracture angulation and displacement with regards to the distal radius, describe the position of the distal fracture fragment with respect to the proximal fracture pattern. 21
 Comminuted Volar Barton s fracture")

22 Oblique, volarly displaced, extraarticular fracture of the distal radius (Smith s Fracture) Comminuted Volar Barton s fracture Barton s Fracture Barton s fracture is an intra-articular fracture of distal end of radius bone. Displacement can be dorsal or volar. 22


23 Nondisplaced radial styloid fracture AKA Hutchinson s fracture, Chauffeur s fracture, Backfire fracture The injury is typically caused by compression of the scaphoid bone of the hand against the styloid process of the distal radius. It can be caused by falling onto an outstretched hand. Treatment -often ORIF which is surgical realignment of the bone fragments and fixation with pins, screws, or plates. Torus or buckle fracture Here the cortex is buckled rather than fractured through as seen in greenstick fractures. Commonly used in pediatric fractures, i.e., growing bones. 23


24 Transverse, nondisplaced, impacted fracture of distal radius Transverse, completely displaced midshaft fracture of the fourth metacarpal 24


25 Transverse, angulated, slightly displaced fractures of the 4 th and 5 th MCP shafts Metacarpal fractures: Because of the mobility of the MPJ s of the ulnar two digits, considerable residual angulation can be accepted w/o compromising hand function. Advise patients that their knuckle is gone forever. 25



26 Oblique, dorsally angulated fracture of the 5 th MCP shaft. Overlapping finger due to rotational malalignment of fracture metacarpal 26





27 Oblique, displaced, intra-articular fracture of the ulnar base of the 1 st MCP Comminuted, displaced, intra-articular fracture of the base of the 1 st MCP Bennett s Fracture Rolando s Fracture Minimally displaced, comminuted, intraarticular fracture of the distal end, proximal phalanx of the index finger. Nondisplaced oblique fracture of the shaft of the proximal phalanx of the small finger. 27



28 Mallet Fracture Splinting 24/7 for six weeks. Gamekeeper s Thumb aka Skiier s Thumb Stener lesion adductor aponeurosis prevents UCL to reposition 28

29 Mallet Fracture Splinting 24/7 for 6-8 weeks THUMB MCP ULNAR COLLATERAL LIGAMENT Tear of the UCL of thumb Gamekeeper s thumb Skier s thumb Hyperabduction of the thumb MCP joint Often after a FOOSH with thumb abducted A stable UCL is needed for effective pinch Stener lesion Occurs in complete tears Distal edge of the ligament held in a displaced position by the ADDuctor aponeurosis The ligament cannot heal in normal anatomical position and residual instability occurs Treatment Partial tears usually cast immobilization or functional bracing w/ MCP in slight flexion for 4-6 weeks Complete tears get referred for surgery 29


30 Fat pad sign When fat pad sign is seen, suspect fracture of radial head. This sign represents bleeding in the joint, hemarthrosis. Oblique, nondisplaced fx. of the junction of the mid and distal thirds of the left clavicle 30






31 Oblique, comminuted, displaced fx. of the femoral shaft with 6cm of over-riding Transverse, minimally displaced fracture of the distal femur at the diaphyseal/metaphyseal junction with approx. 45degrees anterior angulation. Markedly comminuted, displaced, intraarticular tibial plateau fracture Comminuted, nondisplaced, midshaft tibial fracture with a large butterfly fragment Comminuted, moderately displaced, left tibial pilon fracture with intraarticular extension and an associated proximal fibular fracture 31



32 Transverse, nondisplaced medial malleolar fracture with associated oblique, slightly displaced, distal fibular fracture Oblique, displaced lateral malleolar fracture with lateral subluxation of the tibiotalar joint and widening of the medial joint space Comminuted, nondisplaced calcaneal fx. 32


33 Oblique, minimally displaced fx of the fifth metatarsal shaft Minimally displaced avulsion fx. of the medial base and an nondisplaced, intraarticular fx. of the medial condyle of the proximal phalanx of the great toe. 33



34 FOREFOOT FRACTURES Jones Fracture Very commonly seen fracture SLC or rigid boot is excellent treatment in most cases Certain fractures respond well to screw fixation Phalanges FOREFOOT FRACTURES Tx.: Buddy-taping and comfortable shoe 34

35 ORTHOPEDIC EMERGENCIES Compartment Syndrome Dysvascular extremities Native hip dislocations Displaced femoral neck fractures in the young patient Knee Dislocations Open fractures Septic Arthritis COMPLICATIONS Malunion Functional and /or cosmetic deformity Nonunion Infection Delayed closure necessary at times Joint extension contracture Remember protected position Loss of motion Secondary to tendon adherence Posttraumatic arthritis Failure to restore articular congruity 35
36 REFERENCES Kenneth D Amato, DO 36
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
Basic Care of Common Fractures Utku Kandemir, MD
 Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Montreal Children s Hospital McGill University Health Center Emergency Department Fracture Guideline
 Montreal Children s Hospital McGill University Health Center Emergency Department Guideline Disclaimers This document is designed to assist physicians working in our emergency department in caring for
Montreal Children s Hospital McGill University Health Center Emergency Department Guideline Disclaimers This document is designed to assist physicians working in our emergency department in caring for
Trauma-related Pediatric Orthopedic Emergencies. Javier Gonzalez del Rey, M.D. Professor Pediatrics Cincinnati Children s Hospital Medical Center
 Trauma-related Pediatric Orthopedic Emergencies Javier Gonzalez del Rey, M.D. Professor Pediatrics Cincinnati Children s Hospital Medical Center Room # 10 7 month old sick since birth Room # 11 5 y/o Fell
Trauma-related Pediatric Orthopedic Emergencies Javier Gonzalez del Rey, M.D. Professor Pediatrics Cincinnati Children s Hospital Medical Center Room # 10 7 month old sick since birth Room # 11 5 y/o Fell
Hand injuries. The metacarpal bones may fracture through the base, shaft or the neck.
 Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
Hand injuries Metacarpal injuries The metacarpal bones may fracture through the base, shaft or the neck. Shaft fractures; these are caused by direct trauma which may cause transverse # of one or more metacarpal
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
.org. Tibia (Shinbone) Shaft Fractures. Anatomy. Types of Tibial Shaft Fractures
 Shaft Fractures. Anatomy. Types of Tibial Shaft Fractures") Tibia (Shinbone) Shaft Fractures Page ( 1 ) The tibia, or shinbone, is the most common fractured long bone in your body. The long bones include the femur, humerus, tibia, and fibula. A tibial shaft fracture
Tibia (Shinbone) Shaft Fractures Page ( 1 ) The tibia, or shinbone, is the most common fractured long bone in your body. The long bones include the femur, humerus, tibia, and fibula. A tibial shaft fracture
Hand and wrist emergencies
 Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
Chapter1 Hand and wrist emergencies Carl A. Germann Distal radius and ulnar injuries PEARL: Fractures of the distal radius and ulna are the most common type of fractures in patients younger than 75 years.
7/23/2018 DESCRIBING THE FRACTURE. Pattern Open vs closed Location BASIC PRINCIPLES OF FRACTURE MANAGEMENT. Anjan R. Shah MD July 21, 2018.
 BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
16 th Annual Primary Care & Sports Medicine Symposium January 29th, 2016
 To help protect your privacy, PowerPoint has blocked automatic download of this picture. 16 th Annual Primary Care & Sports Medicine Symposium January 29th, 2016 Excellence in Orthopaedics Through Education
To help protect your privacy, PowerPoint has blocked automatic download of this picture. 16 th Annual Primary Care & Sports Medicine Symposium January 29th, 2016 Excellence in Orthopaedics Through Education
EPIPHYSEAL PLATE IN FEMUR
 Reviewing: Epiphyseal Plates (younger skeletons) eventually will disappear. Bones grow lengthwise up and down from each plate, and in a circular collar like fashion around the diaphysis. These plates will
Reviewing: Epiphyseal Plates (younger skeletons) eventually will disappear. Bones grow lengthwise up and down from each plate, and in a circular collar like fashion around the diaphysis. These plates will
11/5/14. I will try to make this painless. Great, a Fracture, Now What? Objectives. Basics for Fracture Workup. Basics for Fracture Workup
 Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Great, a Fracture, Now What? I will try to make this painless Mary Greve MS, PA-C Department of Orthopedic Surgery Trauma Team University of Iowa Hospitals and Clinics Mary-Greve@uiowa.edu Pager 2121 Objectives
Hand Fractures: When is closed treatment OK? Epidemiology in USA: Metacarpal fractures: Page 1
 Hand Fractures: When is closed treatment OK? Robert J Strauch MD Professor of Orthopaedic Surgery Columbia University New York City Epidemiology in USA: 2009 Distal radius fx s: 16/10,000 Phalangeal fx
Hand Fractures: When is closed treatment OK? Robert J Strauch MD Professor of Orthopaedic Surgery Columbia University New York City Epidemiology in USA: 2009 Distal radius fx s: 16/10,000 Phalangeal fx
PEDIATRIC CASTING AND SPLINTING HEATHER KONG, M.D. SHRINERS HOSPITAL FOR CHILDREN PORTLAND OCTOBER 7, 2017
 PEDIATRIC CASTING AND SPLINTING HEATHER KONG, M.D. SHRINERS HOSPITAL FOR CHILDREN PORTLAND OCTOBER 7, 2017 DISCLOSURES I have no financial relationship with any company or product discussed in this presentation.
PEDIATRIC CASTING AND SPLINTING HEATHER KONG, M.D. SHRINERS HOSPITAL FOR CHILDREN PORTLAND OCTOBER 7, 2017 DISCLOSURES I have no financial relationship with any company or product discussed in this presentation.
Other Upper Extremity Trauma. Inje University Sanggye Paik Hospital Yong-Woon Shin
 Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Other Upper Extremity Trauma Inje University Sanggye Paik Hospital Yong-Woon Shin Forearm Fractures Forearm fractures - the most common orthopaedic injuries in children - 30-50% of all pediatric fractures
Foot Injuries. Dr R B Kalia
 Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
PRESENTED BY: JOHN STIMLER, DO, CPC, CHC, FACEP BSA HEALTHCARE AND BSA HEALTHCARE ADVISORY GROUP
 PRESENTED BY: JOHN STIMLER, DO, CPC, CHC, FACEP BSA HEALTHCARE AND BSA HEALTHCARE ADVISORY GROUP TOPICS (1) Fracture types ICD-10-CM diagnostic coding CPT procedure coding Fracture care treatments: Manipulated
PRESENTED BY: JOHN STIMLER, DO, CPC, CHC, FACEP BSA HEALTHCARE AND BSA HEALTHCARE ADVISORY GROUP TOPICS (1) Fracture types ICD-10-CM diagnostic coding CPT procedure coding Fracture care treatments: Manipulated
Basic Radiographic Principles Part II
 Basic Radiographic Principles Part II Kristopher Avant, D.O. October 19 th, 2016 I have no disclosures relevant to the material presented in this discussion. Good Stuff!!! 1 Really? Really! Musculoskeletal
Basic Radiographic Principles Part II Kristopher Avant, D.O. October 19 th, 2016 I have no disclosures relevant to the material presented in this discussion. Good Stuff!!! 1 Really? Really! Musculoskeletal
Trauma Films for Upper Body. LCDR. Naruebade Rungrattanawilai RTN M.D., LL.B. FRCOST, DMOC
 Trauma Films for Upper Body LCDR. Naruebade Rungrattanawilai RTN M.D., LL.B. FRCOST, DMOC Objective A 42 year-old housekeeper with history of motorcycle accident. There was no external wound but she have
Trauma Films for Upper Body LCDR. Naruebade Rungrattanawilai RTN M.D., LL.B. FRCOST, DMOC Objective A 42 year-old housekeeper with history of motorcycle accident. There was no external wound but she have
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
BASIC PRINCIPLES OF HAND TRAUMA: ARE CHILDREN DIFFERENT? SUSAN THOMPSON, MD, FRCSC
 BASIC PRINCIPLES OF HAND TRAUMA: ARE CHILDREN DIFFERENT? SUSAN THOMPSON, MD, FRCSC EPIDEMIOLOGY HAND FRACTURES MAKE UP 2.3% OF ER VISITS INCIDENCE VARIES WITH AGE LOW IN TODDLERS INCREASES WITH AGE (20
BASIC PRINCIPLES OF HAND TRAUMA: ARE CHILDREN DIFFERENT? SUSAN THOMPSON, MD, FRCSC EPIDEMIOLOGY HAND FRACTURES MAKE UP 2.3% OF ER VISITS INCIDENCE VARIES WITH AGE LOW IN TODDLERS INCREASES WITH AGE (20
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
Goals. Initial management skeletal trauma. Physical Exam ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT 12/4/2010
 ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
ABC OF PRIMARY CARE MEDICINE FRACTURE MANAGEMENT Brian Feeley, MD UCSF Sports Medicine and Shoulder Surgery Goals Discuss common fractures and initial management, treatment guidelines Let your patients
Chapter XIX.1. Fractures May 2002
 Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
Case Based Pediatrics For Medical Students and Residents Department of Pediatrics, University of Hawaii John A. Burns School of Medicine Chapter XIX.1. Fractures May 2002 Annemarie Uliasz The skeletal
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
The Forearm, Wrist, Hand and Fingers. Contusion Injuries to the Forearm. Forearm Fractures 12/11/2017. Oak Ridge High School Conroe, Texas
 The Forearm, Wrist, Hand and Fingers Oak Ridge High School Conroe, Texas Contusion Injuries to the Forearm The forearm is constantly exposed to bruising and contusions in contact sports. The ulna receives
The Forearm, Wrist, Hand and Fingers Oak Ridge High School Conroe, Texas Contusion Injuries to the Forearm The forearm is constantly exposed to bruising and contusions in contact sports. The ulna receives
ACUTE HAND INJURIES FOR THE PRIMARY CARE PHYSICIAN
 Vincent Shaw, MD, FAAFP Program Director Baton Rouge General Family Medicine Residency Program Baton Rouge General Sports Medicine Fellowship ACUTE HAND INJURIES FOR THE PRIMARY CARE PHYSICIAN Disclosures
Vincent Shaw, MD, FAAFP Program Director Baton Rouge General Family Medicine Residency Program Baton Rouge General Sports Medicine Fellowship ACUTE HAND INJURIES FOR THE PRIMARY CARE PHYSICIAN Disclosures
St Mary Orthopaedic Conference. Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014
 St Mary Orthopaedic Conference Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014 Nothing to disclose Goals To discuss common orthopaedic pathologies and
St Mary Orthopaedic Conference Steven A. Caruso, MD Trenton Orthopaedic Group Trauma and Complex Fracture Surgeon October 25, 2014 Nothing to disclose Goals To discuss common orthopaedic pathologies and
Tibial Shaft Fractures
 Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Finger Mobility Deficits Fracture of metacarpal Fracture of phalanx of phalanges
 1 Finger Mobility Deficits ICD-9-CM codes: 715.4 Osteoarthrosis of the hand 815.0 Fracture of metacarpal 816.0 Fracture of phalanx of phalanges ICF codes: Activities and Participation code: d4301 Carrying
1 Finger Mobility Deficits ICD-9-CM codes: 715.4 Osteoarthrosis of the hand 815.0 Fracture of metacarpal 816.0 Fracture of phalanx of phalanges ICF codes: Activities and Participation code: d4301 Carrying
Fractures (Broken Bones)
") Fractures (Broken Bones) A fracture is a broken bone. A bone may be completely fractured or partially fractured in any number of ways (crosswise, lengthwise, in multiple pieces). Types of Fractures Bones
Fractures (Broken Bones) A fracture is a broken bone. A bone may be completely fractured or partially fractured in any number of ways (crosswise, lengthwise, in multiple pieces). Types of Fractures Bones
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
9/22/14. ! None. ! Provides non- circumferential support! Accommodates swelling! Useful for acute injuries! Held in place by elastic bandage
 Britt Marcussen, MD Sports Medicine University of Iowa! None! 1. Discuss indications for splinting! 2. Discuss advantages/disadvantages of splints! 3. Go through splinting materials! 4. Discuss casting
Britt Marcussen, MD Sports Medicine University of Iowa! None! 1. Discuss indications for splinting! 2. Discuss advantages/disadvantages of splints! 3. Go through splinting materials! 4. Discuss casting
COURSE TITLE: Skeletal Anatomy and Fractures of the Lower Arm, Wrist, and Hand
 COURSE DESCRIPTION Few parts of the human body are required to pivot, rotate, abduct, and adduct like the wrist and hand. The intricate and complicated movements of the arm, wrist, and hand exist partly
COURSE DESCRIPTION Few parts of the human body are required to pivot, rotate, abduct, and adduct like the wrist and hand. The intricate and complicated movements of the arm, wrist, and hand exist partly
Rehabilitation after Total Elbow Arthroplasty
 Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
Rehabilitation after Total Elbow Arthroplasty Total Elbow Atrthroplasty Total elbow arthroplasty (TEA) Replacement of the ulnohumeral articulation with a prosthetic device. Goal of TEA is to provide pain
A Patient s Guide to Adult Thumb Metacarpal Fractures
 A Patient s Guide to Adult Thumb Metacarpal Fractures 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com 1 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Adult Thumb Metacarpal Fractures 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com 1 DISCLAIMER: The information in this booklet is compiled
Orthopedics in Motion Tristan Hartzell, MD January 27, 2016
 Orthopedics in Motion 2016 Tristan Hartzell, MD January 27, 2016 Humerus fractures Proximal Shaft Distal Objectives 1) Understand the anatomy 2) Epidemiology and mechanisms of injury 3) Types of fractures
Orthopedics in Motion 2016 Tristan Hartzell, MD January 27, 2016 Humerus fractures Proximal Shaft Distal Objectives 1) Understand the anatomy 2) Epidemiology and mechanisms of injury 3) Types of fractures
A Patient s Guide to Adult Finger Fractures
 A Patient s Guide to Adult Finger Fractures 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 1 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Adult Finger Fractures 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 1 DISCLAIMER: The information in this booklet is compiled from a variety
Trigger Digits, Mallet Finger & Metacarpal Injuries. Joseph P. McCormick, M.D. Affinity Orthopaedics & Sports Medicine 2013
 Trigger Digits, Mallet Finger & Metacarpal Injuries Joseph P. McCormick, M.D. Affinity Orthopaedics & Sports Medicine 2013 Overview Trigger Digits: diagnosis and treatment Bonus: approach in children Mallet
Trigger Digits, Mallet Finger & Metacarpal Injuries Joseph P. McCormick, M.D. Affinity Orthopaedics & Sports Medicine 2013 Overview Trigger Digits: diagnosis and treatment Bonus: approach in children Mallet
Top 10 Ortho Urgent Care Injuries. J.C. Clark, M.D. ORA Orthopedics
 Top 10 Ortho Urgent Care Injuries J.C. Clark, M.D. ORA Orthopedics 10. Proximal Humerus Fractures Treatment Simple sling ICE, pain meds Button-down shirts Recliner to sleep in It will be up to the surgeon
Top 10 Ortho Urgent Care Injuries J.C. Clark, M.D. ORA Orthopedics 10. Proximal Humerus Fractures Treatment Simple sling ICE, pain meds Button-down shirts Recliner to sleep in It will be up to the surgeon
Calcaneus (Heel Bone) Fractures
 Fractures") Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
1/19/2018. Winter injuries to the shoulder and elbow. Highgate Private Hospital (Whittington Health NHS Trust)
") Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
Winter injuries to the shoulder and elbow Omar Haddo Consultant Orthopaedic Surgeon, Shoulder, Elbow, Hand & Wrist Specialist MBBS, BmedSci, FRCS(Orth) Highgate Private Hospital (Whittington Health NHS
PIP Joint Injuries of the Finger A Patient's Guide to PIP Joint Injuries of the Finger
 PIP Joint Injuries of the Finger A Patient's Guide to PIP Joint Injuries of the Finger Introduction We use our hands constantly, placing them in harm's way continuously. Injuries to the finger joints are
PIP Joint Injuries of the Finger A Patient's Guide to PIP Joint Injuries of the Finger Introduction We use our hands constantly, placing them in harm's way continuously. Injuries to the finger joints are
Fractures and dislocations of the fingers
 Chapter 1 Fractures and dislocations of the fingers Felix S. Chew, M.D., and Catherine Maldjian, M.D. Case 1 1 Phalangeal tuft avulsion fracture 31-year-old woman injured in a ground-level fall. Lateral
Chapter 1 Fractures and dislocations of the fingers Felix S. Chew, M.D., and Catherine Maldjian, M.D. Case 1 1 Phalangeal tuft avulsion fracture 31-year-old woman injured in a ground-level fall. Lateral
Common Limb Fractures. Mr Sheraz Malik MB BS MRCS Instructor Mr Paul Ofori-Atta Mb ChB FRCS President Motc Life UK April 2009
 Common Limb Fractures Mr Sheraz Malik MB BS MRCS Instructor Mr Paul Ofori-Atta Mb ChB FRCS President Motc Life UK April 2009 Objectives To be able to describe all characteristics of a fracture Describe
Common Limb Fractures Mr Sheraz Malik MB BS MRCS Instructor Mr Paul Ofori-Atta Mb ChB FRCS President Motc Life UK April 2009 Objectives To be able to describe all characteristics of a fracture Describe
Pediatric Phalanx Fractures
 Pediatric Phalanx Fractures Julie Balch Samora, MD/PhD/MPH March 1, 2019.... Disclosures Board/committee member: AOA, AAOS, ASSH, RJOS, POSNA Globus (spouse) Goals To identify the most common phalanx fractures
Pediatric Phalanx Fractures Julie Balch Samora, MD/PhD/MPH March 1, 2019.... Disclosures Board/committee member: AOA, AAOS, ASSH, RJOS, POSNA Globus (spouse) Goals To identify the most common phalanx fractures
Common. Common Hand Problems in Elite Athletes
 Common Hand Problems in Elite Athletes Fred Corley M.D. Dept. of Orthopaedic Surgery UTHSCSA I have no disclosures concerning this talk. The University of Texas Health Science Center @ San Antonio - Orthopaedics
Common Hand Problems in Elite Athletes Fred Corley M.D. Dept. of Orthopaedic Surgery UTHSCSA I have no disclosures concerning this talk. The University of Texas Health Science Center @ San Antonio - Orthopaedics
IC 30: Tips and Tricks for Management of Hand Fractures-Simple to Complex
 IC 30: Tips and Tricks for Management of Hand Fractures-Simple to Complex Moderator(s): Randip R. Bindra, FRCS, MCh Orth Faculty: Andrea Atzei, MD, Donald H. Lalonde, MD, David S. Ruch, MD Session Handouts
IC 30: Tips and Tricks for Management of Hand Fractures-Simple to Complex Moderator(s): Randip R. Bindra, FRCS, MCh Orth Faculty: Andrea Atzei, MD, Donald H. Lalonde, MD, David S. Ruch, MD Session Handouts
Introduction to Fractures. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3
 Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Introduction to Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 3 Definitions A fracture is an interruption in the continuity of bone Fracture = Break Fracture: mechanical damage produced in a
Bone Injuries and Treatment. Fractures and Dislocations
 Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
A Patient s Guide to Adult Metacarpal Fractures of the Hand
 A Patient s Guide to Adult Metacarpal Fractures of the Hand 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com 1 DISCLAIMER: The information in this booklet is
A Patient s Guide to Adult Metacarpal Fractures of the Hand 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com 1 DISCLAIMER: The information in this booklet is
1.3 Initi t al Tre r at e m at e m n e t Pos P iti t oning of th t e p e ati at en e t an d th t e l e imb m. F gure r 1.4.
 INTRODUCTION Immobilization of injured bones, joints, ligaments, or muscles has been practiced traditionally, if nothing else, because of the comfort that immobilization provides. The types of methods
INTRODUCTION Immobilization of injured bones, joints, ligaments, or muscles has been practiced traditionally, if nothing else, because of the comfort that immobilization provides. The types of methods
A Patient s Guide to Adult Thumb Metacarpal Fractures
 A Patient s Guide to Adult Thumb Metacarpal Fractures Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 1 DISCLAIMER: The information
A Patient s Guide to Adult Thumb Metacarpal Fractures Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 1 DISCLAIMER: The information
Fractures of the shoulder girdle, elbow and fractures of the humerus. H. Sithebe 2012
 Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Fractures of the shoulder girdle, elbow and fractures of the humerus H. Sithebe 2012 Fractures of the Clavicle (mid-shaft). Fractures of the clavicle Fractures of the clavicle Treatment- conservative.
Carpal and Finger Fractures. Donald S. Bae, MD Children s Hospital Boston
 Carpal and Finger Fractures Donald S. Bae, MD Children s Hospital Boston Objectives Epidemiology of hand and wrist injuries Discuss injuries requiring surgical care Common complications & strategies for
Carpal and Finger Fractures Donald S. Bae, MD Children s Hospital Boston Objectives Epidemiology of hand and wrist injuries Discuss injuries requiring surgical care Common complications & strategies for
DJO Global 1a Guildford Business Park Guildford Surrey GU2 8XG ENGLAND DJO EN - Rev A
 DJO Global 1a Guildford Business Park Guildford Surrey GU2 8XG ENGLAND www.djoglobal.eu 2012 DJO - 00-2417-EN - Rev A Exos Bracing Shaping Technology, Shaping Lives Exos Bracing Tru-Pull Lite A Great Alternative
DJO Global 1a Guildford Business Park Guildford Surrey GU2 8XG ENGLAND www.djoglobal.eu 2012 DJO - 00-2417-EN - Rev A Exos Bracing Shaping Technology, Shaping Lives Exos Bracing Tru-Pull Lite A Great Alternative
Upper Extremity Injury Management. Jonathan Pirie MD, Med, FRCPC, FAAP
 Upper Extremity Injury Management Jonathan Pirie MD, Med, FRCPC, FAAP Learning Objectives At the end of this session, you will be able to manage common fractures of the: 1. Humerus 2. Elbow 3. Forearm
Upper Extremity Injury Management Jonathan Pirie MD, Med, FRCPC, FAAP Learning Objectives At the end of this session, you will be able to manage common fractures of the: 1. Humerus 2. Elbow 3. Forearm
MANAGEMENT OF INTRAARTICULAR FRACTURES OF ELBOW JOINT. By Dr B. Anudeep M. S. orthopaedics Final yr pg
 MANAGEMENT OF INTRAARTICULAR FRACTURES OF ELBOW JOINT By Dr B. Anudeep M. S. orthopaedics Final yr pg INTRAARTICULAR FRACTURES Intercondyar fracture Elbow dislocation Capitellum # Trochlea # Radial head
MANAGEMENT OF INTRAARTICULAR FRACTURES OF ELBOW JOINT By Dr B. Anudeep M. S. orthopaedics Final yr pg INTRAARTICULAR FRACTURES Intercondyar fracture Elbow dislocation Capitellum # Trochlea # Radial head
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne
 Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
BCCH Emergency Department UPPER LIMB INJURIES Resource pack Developed by: RENA HEATHCOTE RN
 - 1 - BCCH Emergency Department UPPER LIMB INJURIES Resource pack Developed by: RENA HEATHCOTE RN - 2 - FRACTURES The shoulder Dislocation +/_ fracture of humeral head A dislocated shoulder generally follows
- 1 - BCCH Emergency Department UPPER LIMB INJURIES Resource pack Developed by: RENA HEATHCOTE RN - 2 - FRACTURES The shoulder Dislocation +/_ fracture of humeral head A dislocated shoulder generally follows
Management of Fractures. Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 5
 Management of Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 5 Common methods of fracture immobilization Plaster of Paris (POP): A high quality gypsum The standard method of external splinting
Management of Fractures Traumatology RHS 231 Dr. Einas Al-Eisa Lecture 5 Common methods of fracture immobilization Plaster of Paris (POP): A high quality gypsum The standard method of external splinting
Orthopedic Injuries and Immobilization.
 Orthopedic Injuries and Immobilization www.fisiokinesiterapia.biz History and Physical Exam Immediately upon presentation with a dislocation or fracture, the neurovascular and circulatory status must be
Orthopedic Injuries and Immobilization www.fisiokinesiterapia.biz History and Physical Exam Immediately upon presentation with a dislocation or fracture, the neurovascular and circulatory status must be
THE EPIDEMIOLOGY OF HAND EMERGENCIES
 THE EPIDEMIOLOGY OF HAND EMERGENCIES Dr. Adel Abdel Aziz Senior Emergency Physician Honorary Senior Clinical Lecturer, University of Southampton Training Program Director Emergency Medicine/ Health Education
THE EPIDEMIOLOGY OF HAND EMERGENCIES Dr. Adel Abdel Aziz Senior Emergency Physician Honorary Senior Clinical Lecturer, University of Southampton Training Program Director Emergency Medicine/ Health Education
Case. Case 8/29/ yo man with fever, cough. Vitals: Temp 102, HR 130, RR 20, bp 120/80. Ill appearing, crackles R side chest. Now what?
 Kate Aberger, MD August 28, 2016 Help from : Raphael Brancato DO, and Jordan Jeong DO Case 56 yo man with fever, cough Vitals: Temp 102, HR 130, RR 20, bp 120/80 Ill appearing, crackles R side chest Now
Kate Aberger, MD August 28, 2016 Help from : Raphael Brancato DO, and Jordan Jeong DO Case 56 yo man with fever, cough Vitals: Temp 102, HR 130, RR 20, bp 120/80 Ill appearing, crackles R side chest Now
MEDIAL EPICONDYLE FRACTURES
 MEDIAL EPICONDYLE FRACTURES Demographic 20% of elbow fractures 60% of which are associated with elbow dislocation. 75% in boys between 6-12 years 20% of elbow dislocation with ME fracture, the ME is incarcerated
MEDIAL EPICONDYLE FRACTURES Demographic 20% of elbow fractures 60% of which are associated with elbow dislocation. 75% in boys between 6-12 years 20% of elbow dislocation with ME fracture, the ME is incarcerated
Office Orthopedics. No conflict of interest No financial disclosures 1/31/2018
 Office Orthopedics Amin Afsari DO Orthopedic Hand and Upper Extremity Surgery Orthopedic Institute of Wisconsin Midwest Orthopedic Specialty Hospital 1 No conflict of interest No financial disclosures
Office Orthopedics Amin Afsari DO Orthopedic Hand and Upper Extremity Surgery Orthopedic Institute of Wisconsin Midwest Orthopedic Specialty Hospital 1 No conflict of interest No financial disclosures
Hand & Wrist Injuries. DR MA Manjra
 Hand & Wrist Injuries DR MA Manjra 1 Background Up to 25% of all athletic injuries General population Sport people Sport specific Position specific Multifaceted Time of season Level of athlete Parents
Hand & Wrist Injuries DR MA Manjra 1 Background Up to 25% of all athletic injuries General population Sport people Sport specific Position specific Multifaceted Time of season Level of athlete Parents
MR: Finger and Thumb Injuries
 MR: Finger and Thumb Injuries Laura W. Bancroft, M.D. Professor of Radiology University of Central Florida Florida State University Outline Normal anatomy of the fingers and thumb MR imaging protocols
MR: Finger and Thumb Injuries Laura W. Bancroft, M.D. Professor of Radiology University of Central Florida Florida State University Outline Normal anatomy of the fingers and thumb MR imaging protocols
Index. Note: Page numbers of article titles are in boldface type. Hand Clin 21 (2005)
") Hand Clin 21 (2005) 501 505 Index Note: Page numbers of article titles are in boldface type. A Antibiotics, following distal radius fracture treatment, 295, 296 Arthritis, following malunion of distal
Hand Clin 21 (2005) 501 505 Index Note: Page numbers of article titles are in boldface type. A Antibiotics, following distal radius fracture treatment, 295, 296 Arthritis, following malunion of distal
Commonly Missed Injuries of the Extremities
 Commonly Missed Injuries of the Extremities Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of Medicine San Diego, California 1. Base of skull 2. Odontoid process
Commonly Missed Injuries of the Extremities Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of Medicine San Diego, California 1. Base of skull 2. Odontoid process
Closed Proximal Phalangeal Fracture Management in Hand: An Outcome Analysis
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/577 Closed Proximal Phalangeal Fracture Management in Hand: An Outcome Analysis R Senthilkumar 1, E Kovarthini 2, Heber
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/577 Closed Proximal Phalangeal Fracture Management in Hand: An Outcome Analysis R Senthilkumar 1, E Kovarthini 2, Heber
Introduction to Fractures and Dislocations. CAPA 2016 Winnipeg, MB
 Introduction to Fractures and Dislocations CAPA 2016 Winnipeg, MB CAPA 2016 Dr. Chris Graham Orthopedic surgeon Practice primarily trauma related Assist. Prof. U of M Health Sciences Centre No conflicts
Introduction to Fractures and Dislocations CAPA 2016 Winnipeg, MB CAPA 2016 Dr. Chris Graham Orthopedic surgeon Practice primarily trauma related Assist. Prof. U of M Health Sciences Centre No conflicts
Pediatric Tibia Fractures Key Points. Christopher Iobst, MD
 Pediatric Tibia Fractures Key Points Christopher Iobst, MD Goals Bone to heal Return to full weight bearing Acceptable alignment rule of 10s 10 degrees of varus 8 degrees of valgus 12 degrees of procurvatum
Pediatric Tibia Fractures Key Points Christopher Iobst, MD Goals Bone to heal Return to full weight bearing Acceptable alignment rule of 10s 10 degrees of varus 8 degrees of valgus 12 degrees of procurvatum
Pediatric Injuries/Fractures. Rena Heathcote
 Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
Pediatric Injuries/Fractures Rena Heathcote INTRODUCTION Incidence Anatomy of the Growing Bone Injury Patterns What can we X-ray PEDIATRIC FRACTURES INCIDENCE What makes children susceptible to fractures?
A Patient s Guide to Adult Distal Radius (Wrist) Fractures
 Fractures") A Patient s Guide to Adult Distal Radius (Wrist) Fractures Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 1 DISCLAIMER: The
A Patient s Guide to Adult Distal Radius (Wrist) Fractures Suite 11-13/14/15 Mount Elizabeth Medical Center 3 Mount Elizabeth Singapore, 228510 Phone: (65) 6738 2628 Fax: (65) 6738 2629 1 DISCLAIMER: The
PEDIATRIC UPPER EXTREMITY FRACTURE MANAGEMENT JULIA RAWLINGS, MD SPORTS MEDICINE SYMPOSIUM: THE PEDIATRIC ATHLETE 2 MARCH 2018
 PEDIATRIC UPPER EXTREMITY FRACTURE MANAGEMENT JULIA RAWLINGS, MD SPORTS MEDICINE SYMPOSIUM: THE PEDIATRIC ATHLETE 2 MARCH 2018 DISCLOSURE I have nothing to disclose. 2 OBJECTIVES Discuss the diagnosis,
PEDIATRIC UPPER EXTREMITY FRACTURE MANAGEMENT JULIA RAWLINGS, MD SPORTS MEDICINE SYMPOSIUM: THE PEDIATRIC ATHLETE 2 MARCH 2018 DISCLOSURE I have nothing to disclose. 2 OBJECTIVES Discuss the diagnosis,
Elbow, forearm injuries. K. Fekete
 Elbow, forearm injuries K. Fekete 1. Outline: Fractures of the elbow Dislocation of the elbow Fractures of the forearm Special injuries 2. ANATOMY 3. Lennard Funk Anatomical reminder Three joints: Humero-ulnar
Elbow, forearm injuries K. Fekete 1. Outline: Fractures of the elbow Dislocation of the elbow Fractures of the forearm Special injuries 2. ANATOMY 3. Lennard Funk Anatomical reminder Three joints: Humero-ulnar
Location in Bone Diaphyseal Metaphyseal Articular. Epiphysis Physis Metaphysis Diaphysis Periosteum Endosteum
 Hand Therapy Review Course Curtis National Hand Center Baltimore, MD October 7 9, 2016 Fractures Rebecca J Saunders PT/CHT Epiphysis Physis Metaphysis Diaphysis Periosteum Endosteum Cortical bone compact
Hand Therapy Review Course Curtis National Hand Center Baltimore, MD October 7 9, 2016 Fractures Rebecca J Saunders PT/CHT Epiphysis Physis Metaphysis Diaphysis Periosteum Endosteum Cortical bone compact
INTERNAL FIXATION OF THE METACARPALS AND PHALANGES P. BURGE
 Riv Chir Mano - Vol. 43 (3) 2006 INTERNL FIXTION OF THE METCRPLS ND PHLNGES P. URGE Nuffield Orthopaedic Centre, Oxford, UK SUMMRY Techniques and instrumentation for open reduction and internal fixation
Riv Chir Mano - Vol. 43 (3) 2006 INTERNL FIXTION OF THE METCRPLS ND PHLNGES P. URGE Nuffield Orthopaedic Centre, Oxford, UK SUMMRY Techniques and instrumentation for open reduction and internal fixation
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 42 Caring for Clients with Musculoskeletal Trauma Musculoskeletal Trauma Tissue is subjected to more
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 42 Caring for Clients with Musculoskeletal Trauma Musculoskeletal Trauma Tissue is subjected to more
Disclosure. Pediatric Orthopedic Emergencies. I have no actual or potential conflict of interest in relation to this program or presentation.
 Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Clinical Orthopaedic Rehabilitation Volume 1 and 2
 Clinical Orthopaedic Rehabilitation Volume 1 and 2 COURSE DESCRIPTION This program is a practical, clinical guide that provides guidance on the evaluation, differential diagnosis, treatment, and rehabilitation
Clinical Orthopaedic Rehabilitation Volume 1 and 2 COURSE DESCRIPTION This program is a practical, clinical guide that provides guidance on the evaluation, differential diagnosis, treatment, and rehabilitation
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
Hand & Wrist Casey G. Batten MD Assistant Clinical Professor UCSF Sports Medicine
 Hand & Wrist Casey G. Batten MD Assistant Clinical Professor UCSF Sports Medicine Topics: Scaphoid Fracture Scapholunate Separation TFCC Injury Thumb Ulnar Collateral Lig (UCL) Injury Extensor Injury /
Hand & Wrist Casey G. Batten MD Assistant Clinical Professor UCSF Sports Medicine Topics: Scaphoid Fracture Scapholunate Separation TFCC Injury Thumb Ulnar Collateral Lig (UCL) Injury Extensor Injury /
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abscess, epidural, 822 824 Achilles tendon rupture, 894 895, 981 982 Acromioclavicular separations, shoulder pain in, 751 753 Adhesive capsulitis,
Note: Page numbers of article titles are in boldface type. A Abscess, epidural, 822 824 Achilles tendon rupture, 894 895, 981 982 Acromioclavicular separations, shoulder pain in, 751 753 Adhesive capsulitis,
Basic Principles of Fractures & Easily Missed Fractures. Mr Irfan Merchant Trauma & Orthopaedic Registrar Bedford Hospital, East of England
 Basic Principles of Fractures & Easily Missed Fractures Mr Irfan Merchant Trauma & Orthopaedic Registrar Bedford Hospital, East of England Objectives Types Fracture Patterns Fracture Healing Assessing
Basic Principles of Fractures & Easily Missed Fractures Mr Irfan Merchant Trauma & Orthopaedic Registrar Bedford Hospital, East of England Objectives Types Fracture Patterns Fracture Healing Assessing
Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University
 Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University Topics Fracture of the shaft of the femur Fractures around
Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University Topics Fracture of the shaft of the femur Fractures around