Neuropathology Of Head Trauma. Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
|
|
|
- Clarissa Richard
- 6 years ago
- Views:
Transcription
1 Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
2 Nothing to disclose Disclosure
3 Introduction 500,000 cases/year of serious head injury in US 5 to 10% of these are fatal 2/3 of fatal cases are DOA Head injury rate 22-32/100,000 50% traffic, 20-40% GSWs, 10% falls, 5-10% assaults
4 Blunt Trauma Abrasion scraping away of the skin surface, may have patterns Contusion bruise, tearing of vessels beneath skin surface, patterns Laceration tearing open of skin and tissue, tissue bridges, patterns

5 Dicing Abrasion

6 Abrasions
7 Scalp
8 Scalp 2

9 Scalp 3
10 External Clues To Basilar Skull Fracture Ecchymoses Periorbital hematomas Battle sign Blood, brain from ear or nose Wide nasal bridge

11 Periorbital hematomas GSW ecchymoses

12 Orbital Plate Fractures fractures

13 Battle Sign


14 Scalp Lacerations
15 Gunshot Wounds Of Face Certain areas - nose, eyelids, lips, ears Entrance may look very different or unusual May lack typical appearance of abrasion rim, defect May look like tear or exit


16 GSWs GSWs
17 Sharp Wounds Of Face Do not look different from wounds elsewhere on body Not common wounds Most are through orbit, roof of mouth
18 Scalp May not see external evidence of contusion Wounds are best seen from undersurface Injuries can be easily described, measured May take sections for microscopic exam
19 Scalp subgaleal hemorrhage
20 Skull Examine calvarium - peel off periosteum - remove temporalis muscles Describe fractures Remove clavarium - look for epi- or subdural blood Look at fit of brain Remove brain - strip dura
21 Skull 2
22 Skull Fractures Linear Depressed Comminuted Diastatic Compound

23 Linear Fracture Linear fx simple fx line, crack, broad based forces

24 Ring Fracture Ring or circle fx around foramen magnum, forceful hyperextension of head on neck

25 Contrecoup Fracture Fracture of orbital plates from blow to back of head

26 Comminuted Fracture Bone broken into fragments, force over broad area


27 Depressed Fracture Bone pressed inward, small striking surface

28 Depressed Fracture 2 2 areas of depressed fractures
29 Hinge Fracture Hinge fracture across middle cranial fossae through petrous ridges of temporal bones

30 Diastatic Fracture Diastatic fracture enters or opens suture, significant force
31 Mechanisms of Traumatic Brain Injury Static loading force applied slowly > 200 msec crushing head injury Dynamic loading force applied rapidly - < 200 msec produced by direct impact to head (impact) or by causing the head to move by action to the body which causes the head to move (impulse)
32 Mechanisms Static loading rare cause of head injury Dynamic loading accounts for great majority of head injuries Impulsive loading of the head will result in inertial movement of the brain within the cranial cavity» Translational produces focal effects» Rotatory produces both diffuse and focal lesions
33 Inertial Loading Inertial loading creates differential movement of the brain and skull because of differences in rigidity of the two Dura is attached to the skull and moves separately than brain/arachnoid may tear bridging veins (SDH) and axons (tdai)
34 Impact Loading Impact loading - several effects Contact injury»scalp laceration»skull fracture»creates pressure waves into cranial cavity to cause brain contusions»inertial brain movement
35 Blunt Head Trauma Head injury may be focal or diffuse or a combination Focal - direct impact to head and can be seen with naked eye» Scalp laceration/contusion, skull fracture, EDH, focal SDH, brain contusions Diffuse from inertial loading» Interhemispheric SDH, tdai
36 Classification Of Brain Damage From Trauma I. Immediate impact injury A. Contusions and lacerations B. Diffuse axonal injury C. Penetrating injuries II. Primary complications A. Intracranial hemorrhages B. Brain swelling III. Secondary complications - ICP, hypoxia
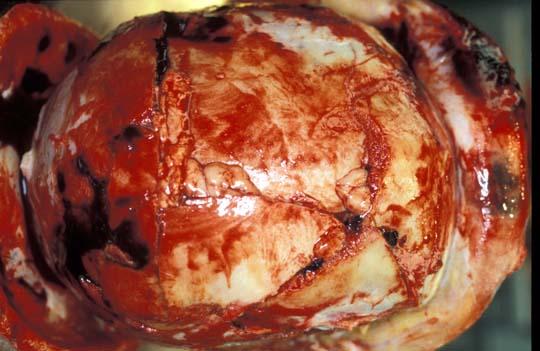
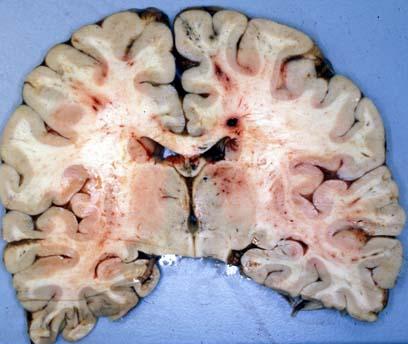
37 Immediate Impact Injury Contusion bruise, usually on crest of gyrus, clusters of small hemorrhages, wedge shaped with apex toward subcortical white Overlying subarachnoid hemorrhage Not static, increases over time Marked in alcoholics, hypertensives
38 Coup Contusions Contusion beneath point of impact Impact site can be seen on scalp Less severe than contrecoup Massive impact may cause contrecoup pattern

39 Coup Contusion

40 Coup Contusion Contusion beneath point of impact On cerebral convexity
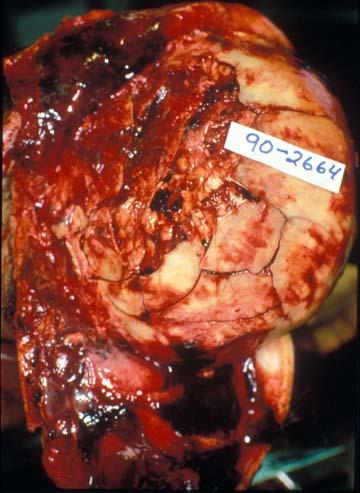
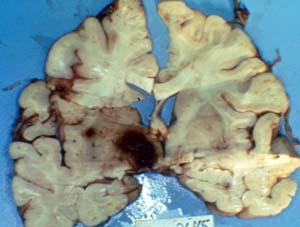
41 Contrecoup Contusion Angular acceleration with moving head impacting a surface on impact rotational movement of brain Rotational movement of brain over sphenoid bone and petrous ridges Contrecoup pattern of contusion over frontotemporal areas
42 Contrecoup Contusion Contusions opposite point of impact Over orbital surfaces, frontal poles, temporal poles Impact to back or side but sometimes front
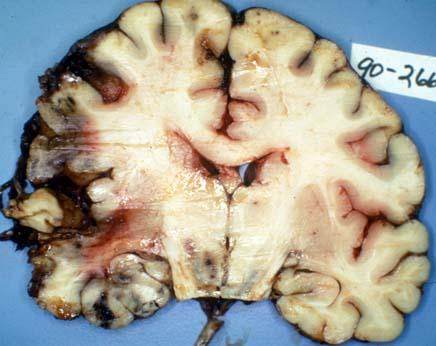
43 Contrecoup Contusion 2 Rotational shear force theory brain moves within cranial cavity in predictable ways Translational moves in straight line Rotational turns on axis, very damaging due to ridges of cranial fossae, sphenoid bones and petrous ridges

44 Contrecoup Contusions

45 Contrecoup Contusions Orbital surfaces, frontal poles, temporal lobes


46 Contrecoup Contusions Fell down stairs

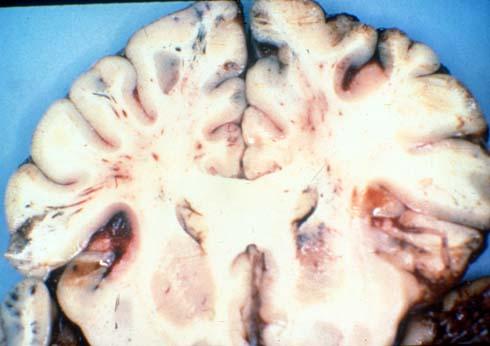
47 Contrecoup Contusions

48 Contrecoup Contusions Clusters of vertical and streak hemorrhages in cortical ribbon Subarachnoid hemorrhage over surface


49 Contrecoup Contusion old contusions
50 Other Impact Injuries CRUSHED HEAD INJURYskull is fragmented and crushed by weight of object No coup or contrecoup contusions Fracture contusions and lacerations - maceration of brain

51 rowbar Crushed Head 2

52 crowbar Crushed Head 3

53 Crushed Head 4
54 Other Impact Injuries 2 FALL FROM HEIGHT No angular acceleration of head - brain and skull fall at same rate No coup or contrecoup contusions Fractures contusions and lacerations

55 Fall From Great Height
56 Young Children Special developmental and anatomical differences Large heavy head Soft brain - unmyelinated, much water Thin, pliable skull with flat skull base Weak neck support
57 Young Children 2 Trivial falls - translational movement Either impact or shaking of significant degree results in rotational brain injury SAH, SDH, retinal hemorrhages, DAI In infants under 5 months may see contusion tears
58 Diffuse Axonal Injury Many other names in past diffuse white matter damage Acceleration deceleration of head - inertial movement of brain due to greater rigidity of skull - greater movement at periphery of brain resulting in shearing injury

59 Diffuse Axonal Injury 2 Pathology streaks or punctate hemorrhages subcortical white, corpus callosum, deep grey, periventricular white SAH, SDH Micro axonal swelling or varicosities Old loss of white, big ventricles
60 Diffuse Axonal Injury 3 Clinical picture Most often MVA, but also some falls, assaults, AHT Moderate to severe degrees produce immediate onset of unconsciousness Survivors of moderate to severe degrees - usually in vegetative state

61 DAI 4 MVA - dead at scene


62 DAI 5 MVA

63 DAI 6 MVA dead at scene


64 DAI 7 Streak and punctate hemorrhages

65 DAI 8 3days post MVA

66 9 days post MVA DAI 9


67 DAI 10 3 days old axonal bulbs BAPP



68 7 years post MVA DAI 11
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
ASPECTS REGARDING THE IMPACT SPEED, AIS AND HIC RELATIONSHIP FOR CAR-PEDESTRIAN TRAFFIC ACCIDENTS
 ASPECTS REGARDING THE IMPACT SPEED, AIS AND HIC RELATIONSHIP FOR CAR-PEDESTRIAN TRAFFIC ACCIDENTS 1 drd.eng. George TOGANEL, 2 Conf.dr.eng. Adrian SOICA Transilvania University of Brasov, Mechanical Engineery
ASPECTS REGARDING THE IMPACT SPEED, AIS AND HIC RELATIONSHIP FOR CAR-PEDESTRIAN TRAFFIC ACCIDENTS 1 drd.eng. George TOGANEL, 2 Conf.dr.eng. Adrian SOICA Transilvania University of Brasov, Mechanical Engineery
Department of Forensic Medicine, University of Dundee HEAD INJURY
 Department of Forensic Medicine, University of Dundee Lecture Notes Head Injury Scalp injury Skull fracture Intracranial haemorrhage (extradural, subdural, subarachnoid, intracerebral) Brain injury Complications
Department of Forensic Medicine, University of Dundee Lecture Notes Head Injury Scalp injury Skull fracture Intracranial haemorrhage (extradural, subdural, subarachnoid, intracerebral) Brain injury Complications
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. Railway accidents injured pedal cyclist
 Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Anatomy and Physiology. Bones, Sutures, Teeth, Processes and Foramina of the Human Skull
 Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma The face is vital to human appearance and function. Facial injuries can impair a patient
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma The face is vital to human appearance and function. Facial injuries can impair a patient
NOTICE. This document may contain graphic information that some people find disturbing. Viewer discretion is advised.
 NOTICE This document may contain graphic information that some people find disturbing. Viewer discretion is advised. Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone
NOTICE This document may contain graphic information that some people find disturbing. Viewer discretion is advised. Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
Traumatic Brain Injury. Epidemiology and Pathophysiology
 Traumatic Brain Injury Epidemiology and Pathophysiology March 10, 2017 Cherry Junn, M.D. Pinella Holder, D.O. University of Washington Disclosures None Objectives Able to define TBI using CDC criteria
Traumatic Brain Injury Epidemiology and Pathophysiology March 10, 2017 Cherry Junn, M.D. Pinella Holder, D.O. University of Washington Disclosures None Objectives Able to define TBI using CDC criteria
BATLS Battlefield Advanced Trauma Life Support
 J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
J R Army Med Corps 2002; 148: 151-158 BATLS Battlefield Advanced Trauma Life Support CHAPTER 8 HEAD INJURIES Aim 0801. On successfully completing this topic you will be able to: Discuss general management
Blow-in fracture of both orbital roofs caused by shear strain to the skull. Department of Neurosurgery, Kanto Teishin Hospital, Tokyo, Japan
 J Neurosurg 49:734-738, 1978 Blow-in fracture of both orbital roofs caused by shear strain to the skull Case report OSAMU SATO, M.D., HIROSHI KAMITANI, M.D., AND TAKASHI KOKUNAI, M.D. Department of Neurosurgery,
J Neurosurg 49:734-738, 1978 Blow-in fracture of both orbital roofs caused by shear strain to the skull Case report OSAMU SATO, M.D., HIROSHI KAMITANI, M.D., AND TAKASHI KOKUNAI, M.D. Department of Neurosurgery,
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review
 Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Brain and Cervico-Medullary Injury : Patterns and Mechanisms
 Brain and Cervico-Medullary Injury : Patterns and Mechanisms P. Ellen Grant MD Associate Professor of Radiology, HMS Director, Center for Fetal-Neonatal Neuroimaging & Developmental Science Children s
Brain and Cervico-Medullary Injury : Patterns and Mechanisms P. Ellen Grant MD Associate Professor of Radiology, HMS Director, Center for Fetal-Neonatal Neuroimaging & Developmental Science Children s
5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains
 5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains Kristen Reeder, MD Child Abuse Pediatrician, REACH Program Children s Health SM Children s Medical Center Dallas Assistant Professor
5 B s of Child Physical Abuse: Bruises, Burns, Bones, Bellies, and Brains Kristen Reeder, MD Child Abuse Pediatrician, REACH Program Children s Health SM Children s Medical Center Dallas Assistant Professor
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Central Nervous System Practical Exam. Chapter 12 Nervous System Cells. 1. Please identify the flagged structure.
 Central Nervous System Practical Exam Chapter 12 Nervous System Cells 1. Please identify the flagged structure. 2. Please identify the flagged structure. 3. Please identify the flagged structure. 4. A
Central Nervous System Practical Exam Chapter 12 Nervous System Cells 1. Please identify the flagged structure. 2. Please identify the flagged structure. 3. Please identify the flagged structure. 4. A
Thickened and thinner parts of the skull = important base for understanding of the functional structure of the skull - the transmission of masticatory
 Functional structure of the skull and Fractures of the skull Thickened and thinner parts of the skull = important base for understanding of the functional structure of the skull - the transmission of masticatory
Functional structure of the skull and Fractures of the skull Thickened and thinner parts of the skull = important base for understanding of the functional structure of the skull - the transmission of masticatory
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas
 Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas Chapter 24 Head and Facial Trauma Objectives Describe mechanism of injury, assessment,
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas Chapter 24 Head and Facial Trauma Objectives Describe mechanism of injury, assessment,
Strong, flexible mass of: Skin Fascia tissue Highly provides insulation
 1 Chapter 23 Head, Facial, & Neck Trauma 2 Introduction to Head, Facial, & Neck Injuries Common major trauma 4 million people experience head trauma annually Severe injury is most frequent cause of trauma
1 Chapter 23 Head, Facial, & Neck Trauma 2 Introduction to Head, Facial, & Neck Injuries Common major trauma 4 million people experience head trauma annually Severe injury is most frequent cause of trauma
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE
 Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE") Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
Prevention and Treatment of Injuries. Mechanical Injury. Trauma 12/11/2017. Oak Ridge High School Conroe, Texas
 Prevention and Treatment of Injuries Oak Ridge High School Conroe, Texas Mechanical Injury Force or mechanical energy is that which changes the state of rest or uniform motion of matter. When a force is
Prevention and Treatment of Injuries Oak Ridge High School Conroe, Texas Mechanical Injury Force or mechanical energy is that which changes the state of rest or uniform motion of matter. When a force is
3. The Jaw and Related Structures
 Overview and objectives of this dissection 3. The Jaw and Related Structures The goal of this dissection is to observe the muscles of jaw raising. You will also have the opportunity to observe several
Overview and objectives of this dissection 3. The Jaw and Related Structures The goal of this dissection is to observe the muscles of jaw raising. You will also have the opportunity to observe several
Slide 1. Slide 2. Slide 3
 Slide 1 Eric S. Hart, Psy.D., ABPP-CN Associate Clinical Professor Director of Adult Neuropsychology Associate Chair University of Missouri-Columbia Department of Health Psychology Slide 2 A traumatic
Slide 1 Eric S. Hart, Psy.D., ABPP-CN Associate Clinical Professor Director of Adult Neuropsychology Associate Chair University of Missouri-Columbia Department of Health Psychology Slide 2 A traumatic
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus
 Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Office of the Chief Medical Examiner Persons Present
 Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone 9199662253 REPORT OF AUTOPSY EXAMINATION DECEDENT Document Identifier B200903289 Autopsy Type ME Autopsy Name Martha
Office of the Chief Medical Examiner CB # 7580 Chapel Hill, NC 27599-7580 Telephone 9199662253 REPORT OF AUTOPSY EXAMINATION DECEDENT Document Identifier B200903289 Autopsy Type ME Autopsy Name Martha
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Chapter 7: Head & Neck
 Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Head injuries. Dr.Mohammed altamimi
 Head injuries Dr.Mohammed altamimi Pathophysiology Local effects on brain tissue Systemic effects of TBI Management protocols Patient triage and classification mechanism Types of head injuries The Primary
Head injuries Dr.Mohammed altamimi Pathophysiology Local effects on brain tissue Systemic effects of TBI Management protocols Patient triage and classification mechanism Types of head injuries The Primary
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Cranial cavity. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Cranial cavity Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-DURA MATER 2-ARACHNOID MATER 3-PIA MATER
Cranial cavity Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology The Meninges The brain in the skull is surrounded by three membranes or meninges: 1-DURA MATER 2-ARACHNOID MATER 3-PIA MATER
PTERYGOPALATINE FOSSA
 PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
Maxillofacial and Ocular Injuries
 Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
5. COMMON APPROACHES. Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2.
 5. COMMON APPROACHES Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2. 5.1. LATERAL SUPRAORBITAL APPROACH The most common craniotomy approach used in
5. COMMON APPROACHES Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2. 5.1. LATERAL SUPRAORBITAL APPROACH The most common craniotomy approach used in
The Human Brain: Anatomy, Functions, and Injury
 The Human Brain: Anatomy, Functions, and Injury Main Menu Brain Anatomy Brain Functions Injury Mechanisms Brain Anatomy Menu Skull Anatomy Interior Skull Surface Blood Vessels of the Brain Arteries of
The Human Brain: Anatomy, Functions, and Injury Main Menu Brain Anatomy Brain Functions Injury Mechanisms Brain Anatomy Menu Skull Anatomy Interior Skull Surface Blood Vessels of the Brain Arteries of
Dr. Sami Zaqout, IUG Medical School
 The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
The University Hospital/ 90! Twenty-Third.Street, N.IV./ Washington, D.C Representatives Select Committee on Assassinations Staff Member
 222 ADDENDUM D REPORT OF DAVID O. DAVIS, M.D., CONCERNING THE EXAMINATION OF THE AUTOPSY X-RAYS OF PRESIDENT JOHN F. KENNEDY, DATED AUGUST 23, 1975 REPORT OF DAVID 0. DAVIS, M.D., CONCERNING THE EXAMINATION
222 ADDENDUM D REPORT OF DAVID O. DAVIS, M.D., CONCERNING THE EXAMINATION OF THE AUTOPSY X-RAYS OF PRESIDENT JOHN F. KENNEDY, DATED AUGUST 23, 1975 REPORT OF DAVID 0. DAVIS, M.D., CONCERNING THE EXAMINATION
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
The orbit-1. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 The orbit-1 Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Orbital plate of frontal bone Orbital plate of ethmoid bone Lesser wing of sphenoid Greater wing of sphenoid Lacrimal bone Orbital
The orbit-1 Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Orbital plate of frontal bone Orbital plate of ethmoid bone Lesser wing of sphenoid Greater wing of sphenoid Lacrimal bone Orbital
SKULL AS A WHOLE + ANTERIOR CRANIAL FOSSA
 SKULL AS A WHOLE + ANTERIOR CRANIAL FOSSA LEARNING OBJECTIVES At the end of this lecture, the student should be able to know: Parts of skeleton (axial and appendicular) Parts of skull Sutures of skull
SKULL AS A WHOLE + ANTERIOR CRANIAL FOSSA LEARNING OBJECTIVES At the end of this lecture, the student should be able to know: Parts of skeleton (axial and appendicular) Parts of skull Sutures of skull
TRAUMA TO THE FACE AND MOUTH
 Dr.Yahya A. Ali 3/10/2012 F.I.C.M.S TRAUMA TO THE FACE AND MOUTH Bailey & Love s 25 th edition Injuries to the orofacial region are common, but the majority are relatively minor in nature. A few are major
Dr.Yahya A. Ali 3/10/2012 F.I.C.M.S TRAUMA TO THE FACE AND MOUTH Bailey & Love s 25 th edition Injuries to the orofacial region are common, but the majority are relatively minor in nature. A few are major
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery FACIAL FRACTURES
 Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Traumatic Head Injury
 Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries, abdominal wall muscle injury, 212 213 diaphragmatic spasm, 212 liver injury, 213 214 pancreatic injury, 216 rectus
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries, abdominal wall muscle injury, 212 213 diaphragmatic spasm, 212 liver injury, 213 214 pancreatic injury, 216 rectus
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Penetrating Trauma in Pediatric Patients. Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017
 Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Head trauma - interpreting CT scans
 Head trauma - interpreting CT scans Poster No.: C-2075 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Rihtar; Zagreb/HR Keywords: Trauma, Hemorrhage, Edema, Diagnostic procedure, CT, Neuroradiology
Head trauma - interpreting CT scans Poster No.: C-2075 Congress: ECR 2014 Type: Educational Exhibit Authors: T. Rihtar; Zagreb/HR Keywords: Trauma, Hemorrhage, Edema, Diagnostic procedure, CT, Neuroradiology
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
TRAUMATIC BRAIN INJURY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
Unit 18: Cranial Cavity and Contents
 Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Chapter 7 Part A The Skeleton
 Chapter 7 Part A The Skeleton Why This Matters Understanding the anatomy of the skeleton enables you to anticipate problems such as pelvic dimensions that may affect labor and delivery The Skeleton The
Chapter 7 Part A The Skeleton Why This Matters Understanding the anatomy of the skeleton enables you to anticipate problems such as pelvic dimensions that may affect labor and delivery The Skeleton The
CASE 1. Female 21 years old DOL: November 28, 2016
 CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
Concussion Information
 What is a Concussion? Concussion Information Information taken from the Sports Concussion Institute http://www.concussiontreatment.com A concussion is defined as a complex pathophysiological process that
What is a Concussion? Concussion Information Information taken from the Sports Concussion Institute http://www.concussiontreatment.com A concussion is defined as a complex pathophysiological process that
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Skull-2. Norma Basalis Interna. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 Skull-2 Norma Basalis Interna Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the skull is divided into
Skull-2 Norma Basalis Interna Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the skull is divided into
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes
 Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
MECHANISMS AND PATTERNS OF HEAD INJURIES IN FATAL FRONTAL AND SIDE IMPACT CRASHES
 MECHANISMS AND PATTERNS OF HEAD INJURIES IN FATAL FRONTAL AND SIDE IMPACT CRASHES P. F. Gloyns Ph.D.* S. J. Rattenbury Ph.D.* R. O. Weller M.D., Ph.D.,FRCPath.** D. C. Lestina B.S.*** *Vehicle Safety Consultants,
MECHANISMS AND PATTERNS OF HEAD INJURIES IN FATAL FRONTAL AND SIDE IMPACT CRASHES P. F. Gloyns Ph.D.* S. J. Rattenbury Ph.D.* R. O. Weller M.D., Ph.D.,FRCPath.** D. C. Lestina B.S.*** *Vehicle Safety Consultants,
Surgical management of diastatic linear skull fractures in infants
 Surgical management of diastatic linear skull fractures in infants JOHN B. THOMPSON, M.D., THOMAS H. MASON, M.D., GERALD L. HAINES, M.D., AND ROBERT J. CASSIDY, M.D. Divisions of Neurosurgery and Neurology,
Surgical management of diastatic linear skull fractures in infants JOHN B. THOMPSON, M.D., THOMAS H. MASON, M.D., GERALD L. HAINES, M.D., AND ROBERT J. CASSIDY, M.D. Divisions of Neurosurgery and Neurology,
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Only 30% to 40% of acute subdural hematoma (SDH)
") Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao
Contralateral Acute Epidural Hematoma After Decompressive Surgery of Acute Subdural Hematoma: Clinical Features and Outcome Thung-Ming Su, MD, Tsung-Han Lee, MD, Wu-Fu Chen, MD, Tao-Chen Lee, MD, and Ching-Hsiao