Pediatric Trauma Initial Evaluation and management
|
|
|
- Piers Wilcox
- 5 years ago
- Views:
Transcription
1 Pediatric Trauma Initial Evaluation and management
2 Head Injury Closed head injury Penetrating head injury
3 Closed Head Injury without Fractures Head injury is the most common cause of death and disability in children Approximately 7000 die each year Nearly 4 times as many permanently disabled
4 Mechanism of Injury Focal Impact Cause focal injuries, with focal deficits Inertial forces Generally result in diffuse damage Often associated with decreased level of consciousness (GCS)
5 Types of Injuries Concussion Diffuse Axonal Injury Contusion Subarachnoid and Intraventricular Hemorrhage Shaking-Impact Syndrome
6 Concussion An injury to the head sufficient to cause loss of consciousness or amnesia of the event At the beginning of the continuum of angular acceleration/deceleration injury Most often from a blunt head injury
7 Presentation Child involved in low-velocity head impact Usually brief loss of consciousness (may be prolonged) No focal neurologic deficits
8
9 Imaging Studies No absolute guidelines All patients with persistent symptoms should have a CT Plain skull films may be sufficient in infants with minimal injury, and NO neurologic deficits
10 Observation Children with mild symptoms may be observed at home with a reliable caretaker over the next 24 hours Patients with more severe injuries, or with an adverse home situation should be admitted for monitoring Sedation should be minimized to allow for serial neurologic exams Repeat imaging is indicated if there is a risk for progression of intracranial injuries, or a worsening neurologic exam
11 Seizures Early post-traumatic seizures are more common in children than adults Usually generalized, mental status returns to baseline quickly Focal seizures more indicative of focal brain injury Not associated with long-term epilepsy
12 Expanding mass lesion Usually epidural hematoma If venous bleeding, may become symptomatic in a delayed manner (days after injury) May be progression of contusions

13
14
15
16 Hyponatremia/Cerebral Edema Gradually decreasing consciousness May also have seizures
17 Vascular dissection Rare after minor trauma Most common with associated skullbase fractures Usually complain of focal neck pain
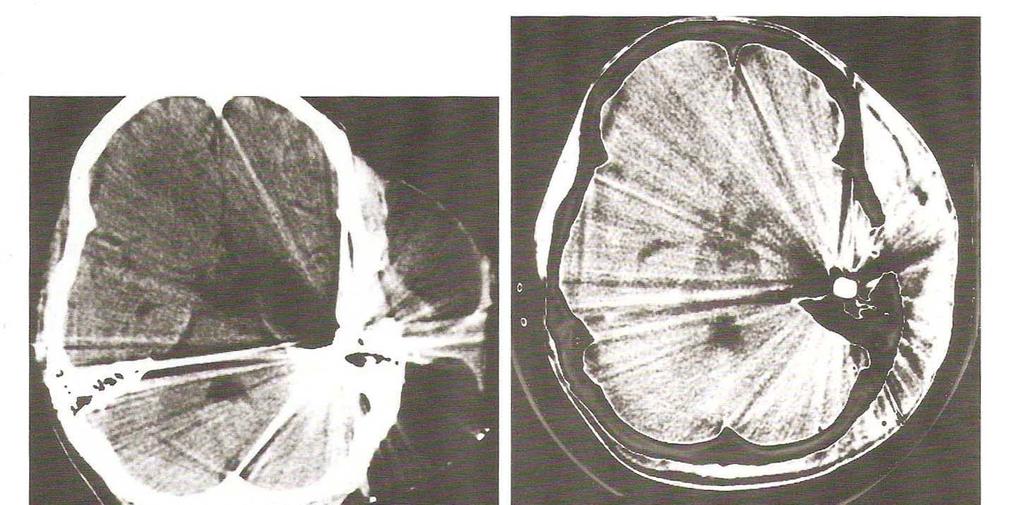
18 Diffuse Axonal Injury Usually applied to patients with loss of consciousness>6 hours, without a mass lesion on CT, or other known etiology Radiologically, see scattered petechial hemorrhages in the deep white matter, corpus callosum and brainstem on CT MRI shows diffuse white matter injuries Pathology shows axonal tears with retraction balls seen on high-power microscopy
19 Mechanism Result of large acceleration/deceleration forces Associated with motor vehicle accidents in older children and adolescents Younger children are often pedestrians struck by autos Rare in infants due to differences in anatomy
20 Presentation Immediate LOC Often accompanied by posturing, with fluctuating GCS May include cranial nerve dysfunction, including pupillary abnormalities
21 Management Initial CT shows no surgical lesion Placement of intracranial pressure monitoring device Repeat imaging if significant decrease in neurologic exam or elevated ICP
22 Hospital Course Later may develop a triad of hypertension, hyperhidrosis and hyperthermia Subsequently may go through period of agitation before regaining normal consciousness Extent of recovery is extremely variable
23 Contusion Focal lesion from an impact (coup and contre-coup) Usually progress over first few days, often cause delayed neurologic deterioration Associated with significant local brain edema
24
25 Management Medical management of seizure prophylaxis, ICP control and prevention of excessive edema first line Surgical evacuation indicated if progressive mass causes significant deterioration Goal is to remove adequate hematoma/infarcted brain to decompress normal brain tissue and prevent secondary injury
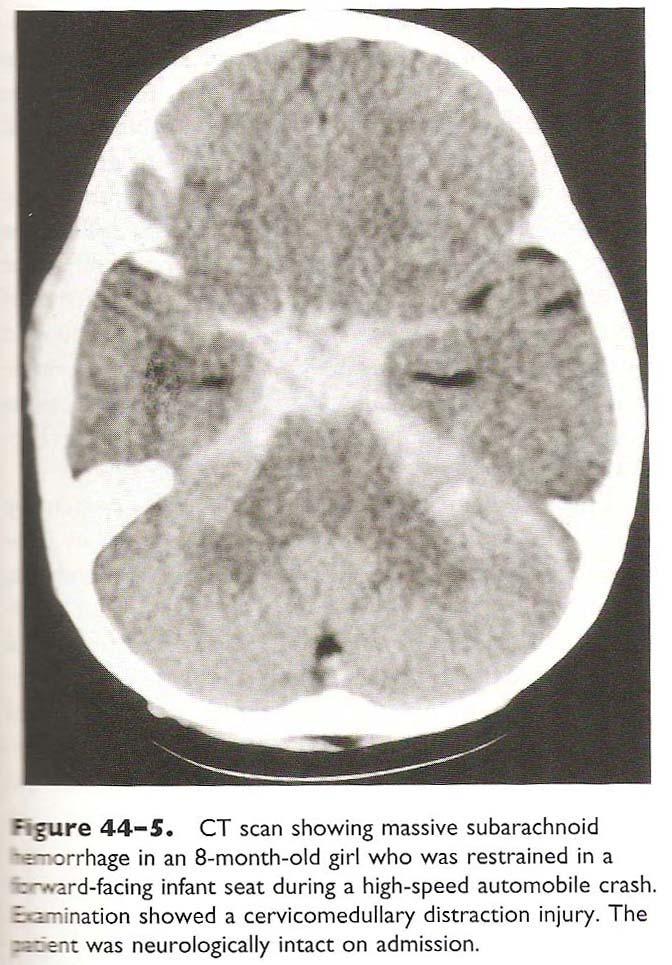
26 Subarachnoid and Intraventricular Hemorrhage Commonly occurs over convexities in association with contusion/after focal impact Diffuse basilar blood seen in occipito-cervical distraction injuries in infants or toddlers (acceleration/deceleration injury) Extent of parenchymal injury varies, but must prevent further injury due to instability Intraventricular blood most commonly seen with DAI, rarely requires specific intervention
27
28 Shaking-Impact Syndrome Non-accidental trauma Mechanism involves large forces with sudden deceleration of the head Often have associated spine injuries Immature brain probably more susceptible to this kind of injury
29
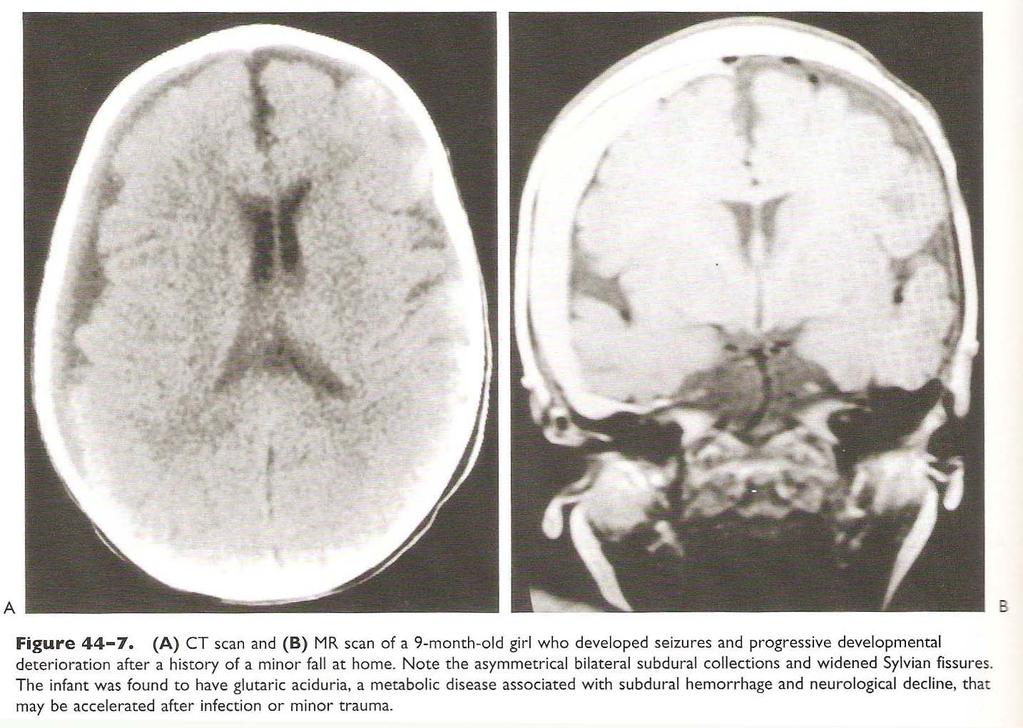
30 Presentation Caretaker often describes only new onset of symptoms (lethargy/seizure/difficulty breathing, etc ) with no or only minor trauma Examination of child shows decreased consciousness, and often external signs of trauma (bruising, soft-tissue swelling) Further exam for retinal hemorrhages (present in about 75% of patients) Radiologic survey for skeletal injuries (present in about half)
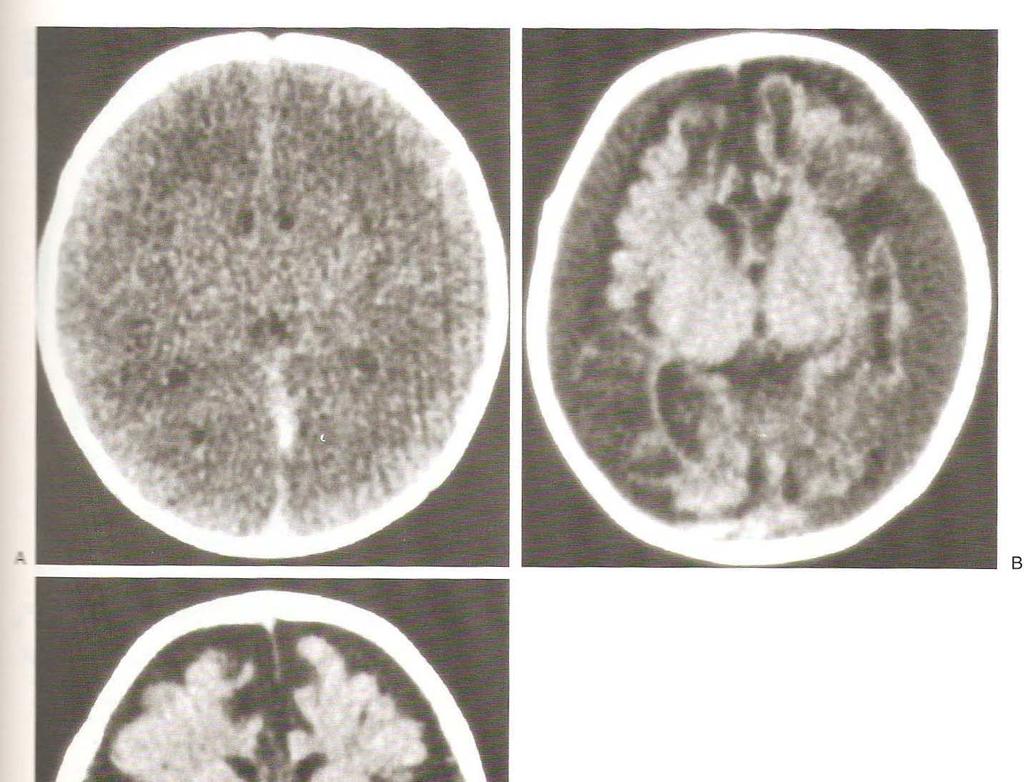
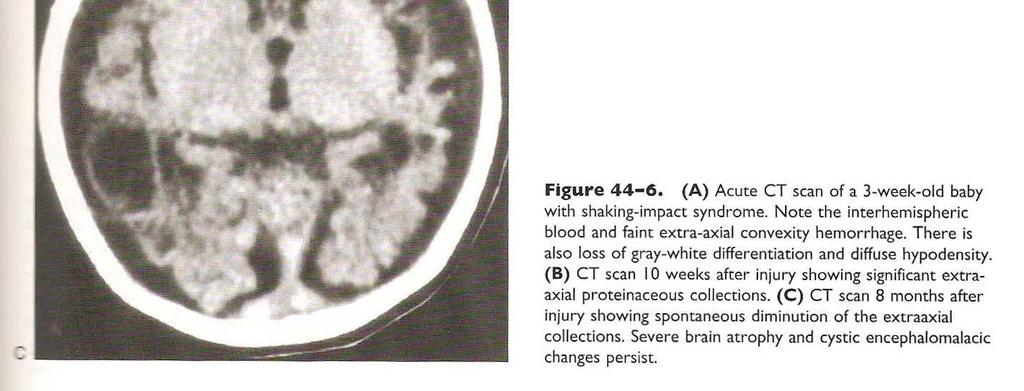
31 Brain Imaging CT or MRI will show subarachnoid or subdural hemorrhages, often of various ages mixed Parenchymal injury may be minimal, or may show infarction of most of the brain with diffuse loss of grey-white junction (visible on CT within hours)
32
33 Management ABC s-including intubation and circulatory support if necessary Rule out other organ system injuries that may require immediate treatment Seizure management/prophylaxis Control of ICP Surgical evacuation of mass lesions when necessary Search for other causes (e.g. coagulopathy, metabolic disease, vascular malformation)
34
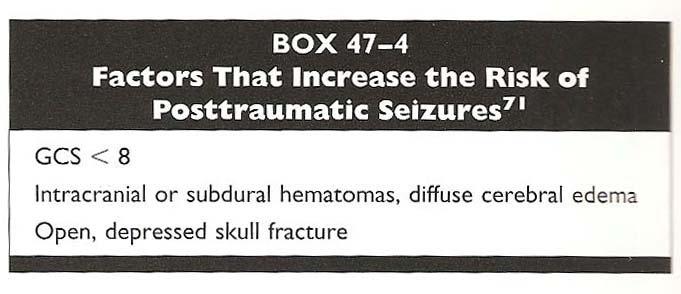
35 Posttraumatic Seizures Impact seizures (at time of event) noted in 12% of children admitted for mild head injury (concussion) Early seizures (within 1 week of trauma) in 10% overall 30-50% of patients in high-risk group (severe brain injury, focal cortical injury) 95% occur within the first 24 hours after trauma
36
37
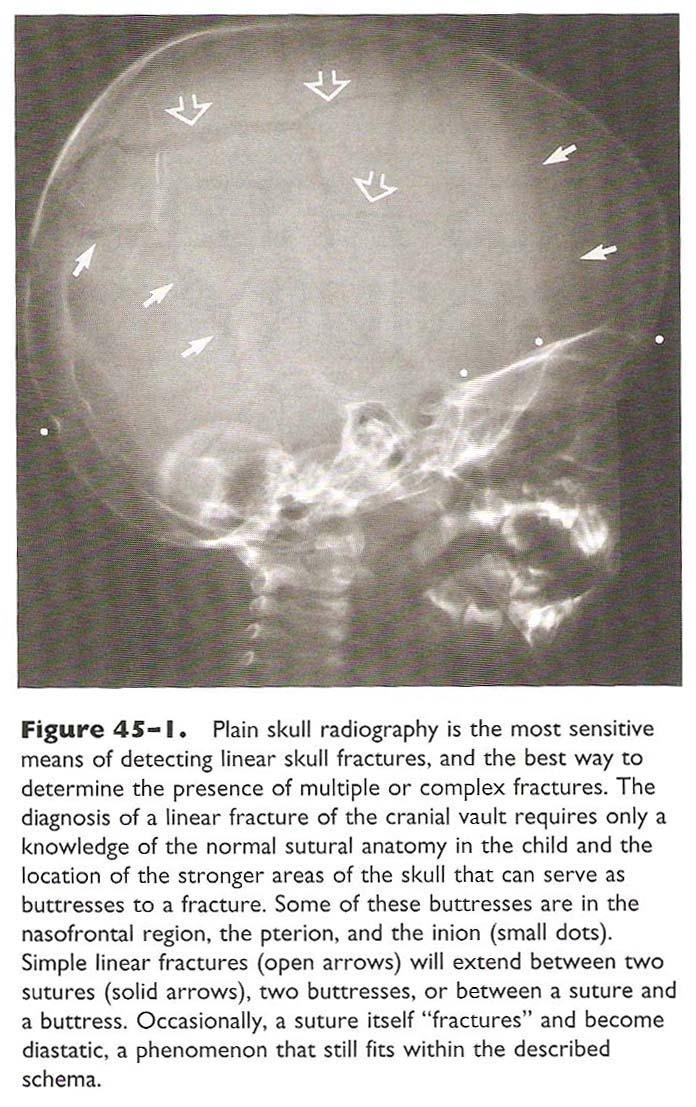
38 Closed Skull Fractures 20% of children admitted with a head injury have a concommitant skull fracture May be simple linear fracture, or more complex comminuted, depressed or skull base Convexity linear skull fractures in an infant are usually not associated with any brain injury Fractures in older children, or more complex fractures increase the likelihood of finding an intracranial injury (roughly 100X) The worse the fracture, the worse the brain injury
39 Linear Skull Fractures 2/3 of all skull fractures 30% of patients do not have signs of external trauma suggesting presence of the skull fracture, may be remote to site of cranial impact Infants with large subgaleal hematomas associated with the injury must be monitored for hemodynamic stability If patient is completely normal neurologically, and has a normal CT (other than fx), then risk of deterioration is almost 0
40
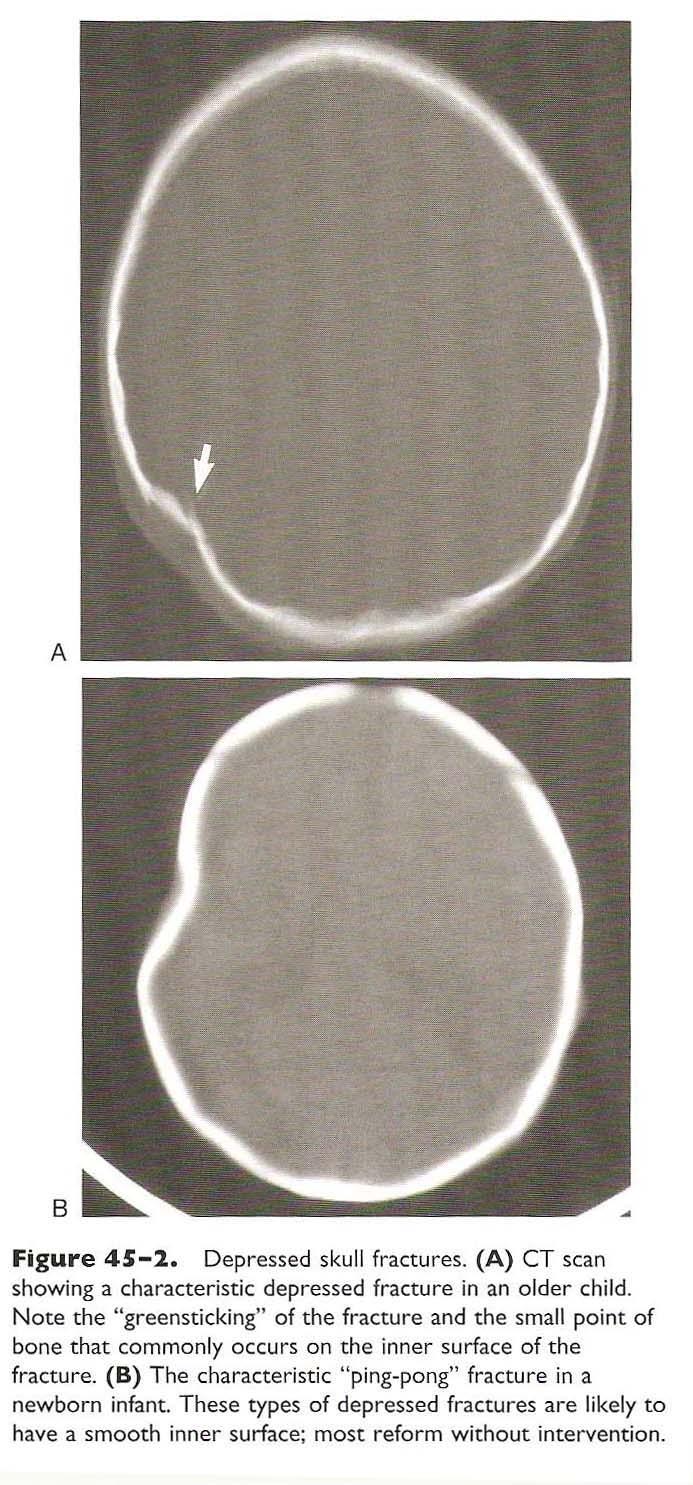
41 Depressed Skull Fractures 25% of all childhood skull fractures 50% of patients with depressed skull fractures are children Caused by high-impact focal injury Dural laceration noted in only 10% of patients 80% involve frontal or parietal bone Most common fracture in neonates (80%)
42
43 Management Neonatal ping-pong fractures should be treated immediately if there is underlying intracranial injury Isolated fractures can be observed, as many will spontaneously improve as the child grows
44 Management Fractures in older children should be elevated if there is A significant cosmetic deformity Depression of >1cm Underlying brain injury Dural laceration Surgery is safe (does not involve major sinuses)
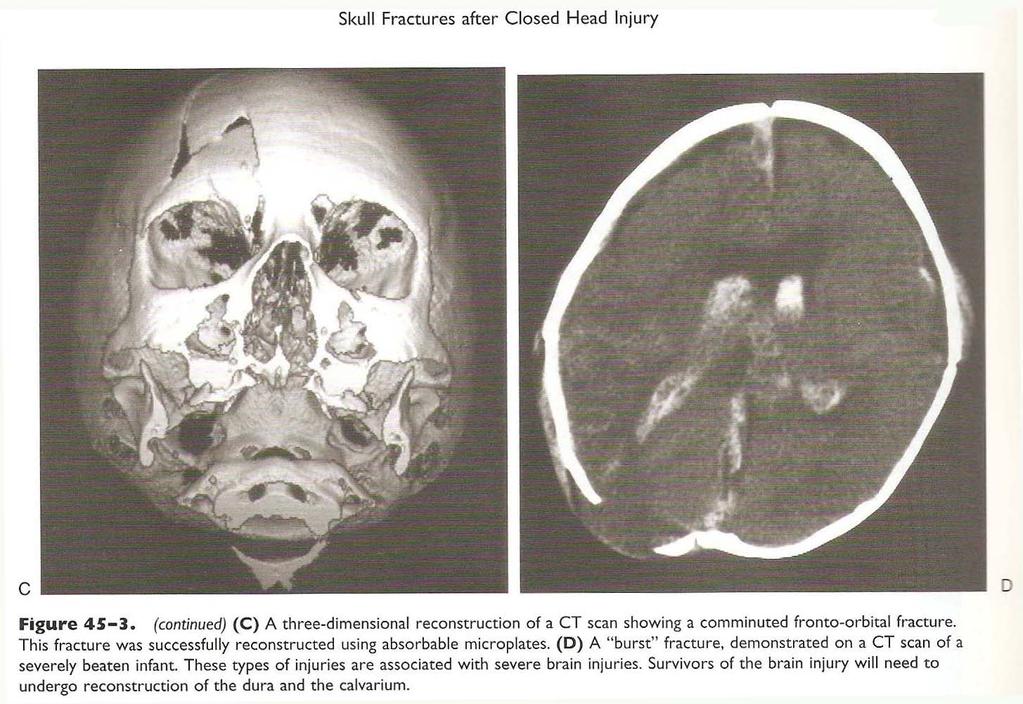
45 Comminuted/Complex Fractures As these are commonly associated with severe brain injury, cranial reconstruction is often delayed until ICP issues are resolved Fractures involving the facial bones often require reconstruction for cosmetic and functional concerns
46
47 Compound Fractures Contaminated by exposure to the environment Include open fractures, but also those involving the paranasal sinuses and middle ear
48 Frontal Sinus Fractures Frontal sinus does not appear until 8-10 years of age Significant for intracranial issues only when posterior wall is involved May be accompanied by rhinorrhea or pneumocephalus If dural compromise persists, then surgical intervention is required
49 Basilar Skull Fractures Can be associated with injury to the vasculature, cranial nerves, or ocular/auditory structures Cannot be diagnosed on plain films-rquires high-resolution CT Occur in <10% of children with head injuries

50
51 Presentation Anterior fossa fractures associated with periorbital swelling/ecchymoses (Raccoon s eyes), more commonly associated with rhinorrhea Temporal fossa/petrous fractures accompanied by ear pain, swelling, ecchymoses (Battle s sign). May see hemotympanum or external canal hemorrhage May involved otorrhea or rhinorrhea (through Eustachian tube) May have decreased hearing

52
53 Temporal Bone Fractures Longitudinal Extends anteriorly along petrous ridge Not associated with long-term complications 80% of fractures Transverse Extends through petrous bone, can disrupt cochlear/vestibular structures Often associated with permanent hearing loss/vestibular dysfunction/facial nerve palsies 20% of fractures

54
55 Management ENT consult to assess hearing/facial nerve deficits Observation for possible rhinorrhea/otorrhea-may present days or weeks after injury No indication for prophylactic antibiotics Conservative management if CSF leak occurs (almost all resolve spontaneously) If necessary, lumbar drain can be placed for a few days, rarely surgical intervention is required
56 Growing Skull Fractures Complicate less than 1% of childhood fractures Caused by dural tear followed by persistent CSF leak/cyst that prevents bony healing Treated by surgical repair of dural defect Can be diagnosed clinically in 4-6 weeks follow-up after skull fracture

57
58 Penetrating Injuries Common causes Accidental injury with sharp objects Warfare Accidental shooting Suicide Homicide
59 Presentation ABCs usually addressed in the field Usually have a focal neurologic deficit associated with tract of injury If brainstem is involved, may include altered consciousness Associated injuries may affect hemodynamic stability, and patients must be screened by the trauma surgery service Excessive hemorrhage may be noted if the patient has developed DIC due to release of thromboplastin from injured parenchyma


60
61 Management CT scan is study of choice Frequent neurochecks to monitor for developing mass lesions or increased ICP Follow-up CT at 6 hours (delayed hematomas most commonly occur 3-8 hours after initial injury) Surgery indicated To remove foreign bodies to prevent secondary complications (infection, post-traumatic aneurysm, seizures) To prevent further bleeding, edema and gliosis To eliminate mass effect Placement of intracranial pressure monitor GCS>5 Administration of antibiotics in the early period is variable. If desired, choice of antibiotic should cover appropriate contaminating organisms Contrast-enhanced imaging indicated in febrile patient to assess for possible abscess development Seizure prophylaxis for early seizures is effective, but patients are at increased risk (up to 50%) of late seizures
62
63 ICU Management Goals are to Optimize substrate delivery and cerebral metabolism Prevent herniation Target mechanisms involved in secondary injury
64 Initial Resuscitation Must address ABCs first Hypoxia and hypotension increase morbidity and mortality Rapid-sequence, neuroprotective intubation for GCS<10 Drop in GCS of 3 points Anisocoria>1mm C-spine injury compromising breathing Apnea Hypercarbia (PCO2>45) Loss of gag reflex Spontaneous hyperventilation with PCO2<25
65 Initial Resuscitation Cardiovascular assessment for adequate perfusion Resuscitation fluid should be isotonic crystalloid, followed by colloid and or blood
66 Worsening neurological status Sedation Seizures Expanding mass lesion Cerebral edema Hyponatremia Vascular dissection with CVA
67 Intracranial Pressure Monitoring No specific guidelines for children, but is reasonable to use adult guidelines Abnormal CT and GCS<9 Abnormal neuro exam with normal CT, complicated by hypotension or posturing
68
69 Cerebral Blood Flow Monitoring Stable xenon-enhanced CT Shows regional differences in blood flow, can be used to assist in management decision Radioactive xenon imaging Provides some real-time data for detection of changes in regional flow, but cannot assess anatomical abnormalities Transcranial doppler Only assesses flow through distal ICA/MCA distributions Limited utility in trauma
70 Monitoring Cerebral Metabolism Jugular venous saturation has not been studied in children, may be technically difficult due to smaller vessels Intraparenchymal PO2 monitor in adults can be used in clinical management of ICP/perfusiononly provides focal information, and is invasive PET imaging limited by long acquisition times, more useful after patient has stabilized to predict recovery
71 Maintenance Goals are to maintain cerebral perfusion CPP can be lower than in adults in infants/toddlers in young children BP support with pressors and inotropes CVP/cardiac output monitoring
72 Sedation/Paralysis Ideal to use short-acting agents to allow for neuromonitoring Use agents that do not increase ICP Narcotics Benzodiazepines Small doses barbiturates Paralysis has been associated with increased nosocomial pneumonia and longer ICU stay Increased doses of sedatives/analgesics during routine care procedures to prevent agitation
73 CSF Drainage Only possible with catheter placement, may be technically difficult in a child Allows for therapeutic treatment of increased ICP Does increase risk of meningitis/ventriculitis
74 Head Positioning HOB 30o decreases ICP Midline positioning improves venous drainage
75 Osmotic Agents Mannitol Dehydrates brain parenchyma due to blood-brain barrier Improves rheology, and allows for decreased arterial blood volume with autoregulation Hypertonic saline Perhaps has less renal toxicity Used more commonly in children to manage ICP-Na+ up to 170 without evidence of adverse effects in multiple studies Can be administered as a drip or bolus infusion
76 Hyperventilation Can be used for short-term vasoconstriction to assist in ICP management Should not maintain PCO2<30mm Hg due to risk of ischemia Should prevent hypercarbia
77 Barbiturates Used to manage refractory increased ICP by decreasing cerebral metabolic demand Should have continuous EEG monitoringendpoint is burst suppression Increases risk of hypotension and nosocomial pneumonia
78 Hypothermia Contradictory results in many studies due to increased risk of complication Use of moderate hypothermia (32o for 24-48hrs) may be used for refractory increased ICP Prevention of hyperthermia more important
79 Decompressive Craniectomy No specific guidelines for use Can reduce ICP, better outcomes likely if performed early (<48hrs after injury)
80 Controlled Arterial Hypertension If autoregulation is intact, mild hypertension ( torr) induces vasoconstriction, and reduces ICP in adults Data about specific values is not available for children (who have lower baseline pressures) Unknown effects on development of edema, possible worsening of hemorrhage
81 Complications Seizure prophylaxis in severe traumatic brain injury Prevention of hyponatremia (can be due to SIADH or cerebral salt wasting) Nutrition support Glucocorticoid use in NOT indicated in head injury
82
83 Follow-up If and when the child s mental status has returned to baseline, and has adequate oral intake, he may be discharged Parents should be informed about possible post-concussive symptoms including headaches, dizziness, nausea, irritibility, difficulty with memory/concentration Patients may not participate in contact sports until all symptoms have resolved, + 1 week (general consensus, although does not guarantee against increasingly severe head injuries with future impacts) Follow-up may be with primary physician or with neurosurgeon
84 Rehabilitation and Outcome Motor and Visual-Motor Deficits Language and Communication Deficits Behavioral Changes Cognitive Dysfunction Academic Achievement
85 Motor and Visual-Motor Deficits Observed in nearly all children with moderate-severe injury Usually have mild residual deficits Slower motor response time Developmental stage at time of injury affects future development-slower if patients injured before skill was fully developed
86 Language and Communication Expressive language more affected than receptive, recovers more slowly Young children have persistent deficits in written language Discourse most likely to have persistent deficits (not tested by routine assessment measures)
87 Behavior Increase in problem behaviors, decrease in adaptive behaviors Confusion, disorientation, agitation, withdrawal, disinhibition If pre-existing issues, may worsen even with mild head injury Severe injury greatly increases risk of persistent problems Young males at highest risk of persistent decline in adaptive behaviors
88 Cognitive Dysfunction IQ often decreased, but is a global measure, and may not detect specific cognitive deficits Performance IQ more affected than verbal IQ (may be associated to motor deficits) Memory impairment most common deficit-most associated with left hemisphere damage Verbal memory deficits may not be as noticeable until adolescence (when normal children develop this skill) Attention deficits may worsen memory function-younger children at risk for long-term effects Executive functions significantly affected in young children, and with frontal lobe injury
89 Academic Achievement Combined deficits in many areas lead to poor school performance Special education services to assist in environmental factors can improve outcomes Deficits may become more pronounced as the child grows older, since they have greater difficulty attaining new skills
90 Predictors of Outcome Injury Variables Severity Type and Extent of Injury Secondary Injuries Pre-injury Variables Age at Injury Behavioral History Premorbid Family Functioning Post-injury Variables Family Functioning Rehabilitation services
91 Primary Treatment Limited studies in children Inpatient vs Outpatient dependent on severity of injury Goals are to reintegrate into home and school setting Prevent secondary complications Retrain lost skills Learn compensatory strategies
92 Interventions Psychosocial Counseling for emotional issues Behavior management with differential reinforcement Cognitive Strengthen previously learned skills/patterns Train new behaviors to compensate for impairments
93 Adjunct Treatments Parental Interventions Parental support groups/stress management School-based Interventions Home instruction Slowly increase length of school day Special education with classroom modifications Self-instruction training
94 Conclusions Pediatric head trauma covers a large clinical spectrum Initial evaluation is important to ascertain extent of injury Management is directed toward minimizing any further secondary injury/complications Early and intensive rehabilitation after moderate to severe trauma improves long-term outcomes
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Traumatic Brain Injury
 General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
General Information Traumatic Brain Injury What you need to know Complicated condition with high variability in etiology, severity, distribution of injury, and pattern of functional impairment (Klyce,
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Neuropathology Of Head Trauma. Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
 Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8:
 Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
Virtual Mentor American Medical Association Journal of Ethics August 2008, Volume 10, Number 8: 516-520. CLINICAL PEARL The Hazards of Stopping a Brain in Motion: Evaluation and Classification of Traumatic
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Index. Note: Page numbers of article titles are in bold face type.
 Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Neurosurg Clin N Am 13 (2002) 259 264 Index Note: Page numbers of article titles are in bold face type. A Abdominal injuries, in child abuse, 150, 159 Abrasions, in child abuse, 157 Abuse, child. See Child
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
CSF Leaks. Abnormal communication between the subarachnoid space and the tympanomastoid space or nasal cavity. Presenting symptoms:
 CSF Leaks Steven Wright, M.D. Faculty Advisor: Matthew Ryan, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2005 CSF Leaks Abnormal communication
CSF Leaks Steven Wright, M.D. Faculty Advisor: Matthew Ryan, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2005 CSF Leaks Abnormal communication
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Traumatic Head Injury
 Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Traumatic Head Injury Liu Yi, MD. PhD, associate professor Dept. Neurosurgery Conception Any injury to the skull, or brain, caused by external physical forces, in stead of degenerative or congenital nature
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Head Injury: Classification Most Severe to Least Severe
 Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
Head Injury: Classification Most Severe to Least Severe Douglas I. Katz, MD Professor, Dept. Neurology, Boston University School of Medicine, Boston MA Medical Director Brain Injury Program, HealthSouth
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
TRAUMATIC BRAIN INJURY
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences TRAUMATIC BRAIN INJURY GARY STOBBE, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES The University of Washington
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes
 Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
Functional Neuroanatomy and Traumatic Brain Injury The Frontal Lobes Jessica Matthes, Ph.D., ABN Barrow TBI Symposium March 23, 2019 jessica.matthes@dignityhealth.org Outline TBI Mechanisms of Injury Types
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Traumatic Brain Injury (1.2.3) Management of severe TBI ( ) Learning Objectives
 Management of severe TBI ( ) Learning Objectives") Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Traumatic Brain Injury (1.2.3) 1.2.3.1 Management of severe TBI 1.2.3.2 Management of concussions 1.2.3.3 Sideline management for team medics/physicians 1.4.2.3.10 Controlled hyperventilation for management
Continuum of Care: Post Acute Brain Injury Rehabilitation
 Continuum of Care: Post Acute Brain Injury Rehabilitation Laura Wiggs, PT, NCS, CBIS Mentis Neuro Rehabilitation Traumatic Brain Injury (TBI) When an outside mechanical force is applied to the head and
Continuum of Care: Post Acute Brain Injury Rehabilitation Laura Wiggs, PT, NCS, CBIS Mentis Neuro Rehabilitation Traumatic Brain Injury (TBI) When an outside mechanical force is applied to the head and
Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience
 80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Slide 1. Slide 2. Slide 3
 Slide 1 Eric S. Hart, Psy.D., ABPP-CN Associate Clinical Professor Director of Adult Neuropsychology Associate Chair University of Missouri-Columbia Department of Health Psychology Slide 2 A traumatic
Slide 1 Eric S. Hart, Psy.D., ABPP-CN Associate Clinical Professor Director of Adult Neuropsychology Associate Chair University of Missouri-Columbia Department of Health Psychology Slide 2 A traumatic
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency
 Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Rhonda Dixon, DVM Section Head, Emergency and Critical Care Sugar Land Veterinary Specialty and Emergency Traumatic Brain Injury Causes Pathophysiology Neurologic assessment Therapeutic Approach Status
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
TCD IN THE NICU, PICU AND OTHER APPLICATIONS. Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
 TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C. Objectives Recognize normal and abnormal cranial blood flow patterns
Head, Face, Eyes, Ears, Nose and Throat. Neurological Exam. Eye Function 12/11/2017. Oak Ridge High School Conroe, Texas
 Head, Face, Eyes, Ears, Nose and Throat Oak Ridge High School Conroe, Texas Neurological Exam Consists of Five Major Areas: 1. cerebral testing cognitive functioning 2. Cranial nerve testing 3. Cerebellar
Head, Face, Eyes, Ears, Nose and Throat Oak Ridge High School Conroe, Texas Neurological Exam Consists of Five Major Areas: 1. cerebral testing cognitive functioning 2. Cranial nerve testing 3. Cerebellar
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Anatomy Neurological Review TCHP CCRN Review Lynelle Scullard MSN RN CCRN K CNRN Bones Lobes Vascular Cranial nerves Bones Parietal Temporal occipital Frontal Sphenoid Ethmoid Lobes Frontal Willed mvmt,
Anatomy Neurological Review TCHP CCRN Review Lynelle Scullard MSN RN CCRN K CNRN Bones Lobes Vascular Cranial nerves Bones Parietal Temporal occipital Frontal Sphenoid Ethmoid Lobes Frontal Willed mvmt,
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
diagnosis Temporal bone fractures: a clinical
 Archives of Emergency Medicine, 1988, 5, 146-150 Temporal bone fractures: a clinical diagnosis J. WALDRON & S. E. J. HURLEY Department of Ear Nose and Throat Surgery, St Mary's Hospital, London, England
Archives of Emergency Medicine, 1988, 5, 146-150 Temporal bone fractures: a clinical diagnosis J. WALDRON & S. E. J. HURLEY Department of Ear Nose and Throat Surgery, St Mary's Hospital, London, England
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as