THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON
|
|
|
- Calvin Lawrence
- 6 years ago
- Views:
Transcription


1 THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON
2 DISCLOSURES + BACKGROUND No. Centre de formation médicale du NB Orthopaedic residency Université de Sherbrooke Orthopaedic Trauma Fellowship, Auckland City Hospital
3 OBJECTIVES Prehospital management Initial assessment in the ER Initial treatment in the ER The management of hemodynamic instability Preparation for definitive care Outcomes
4 INTRO Pelvic ring # VS acetabulum #


5 INTRO Pelvic ring # VS acetabulum #
.")

6 INTRO Pelvic ring fracture VS Acetabulum fracture Both high energy injuries (in non-osteoporotic pts). Ring more associated with life threatening haemorrhage Acetabulum more associated with long term threat to hip



7 INTRO Pelvic ring # classification Lateral compression Vertical shear Open book Acetabulum # classification Hip dislocated or not Associated femoral neck fracture or not Smashed or not so bad
8 PRE HOSPITAL MANAGEMENT Level of aggression energy of mechanism

9 PRE HOSPITAL MANAGEMENT Traumatic hemipelvectomy: Improvements in the last decennia illustrated by 2 case reports T.K. Timmers,a, D. Tiren,a P.F. Hulstaert,a P.P.A. Schellekens,b and L.P.H. Leenena We re going straight to the OR, NOW.
 -MSK (70%) -Urological")
10 PRE HOSPITAL MANAGEMENT Life threatening, hours to days Associated injuries frequent: -CNS -Chest -Abdo (40%) -MSK (70%) -Urological (12%)

11 PRE HOSPITAL MANAGEMENT Life threatening, weeks to months, because of complications

12 PRE HOSPITAL MANAGEMENT Circulatory collapse from pelvic facture is the exception rather than the rule.
13 PREHOSPITAL MANAGEMENT Use of pelvic binders is advocated by most and has been endorsed by NB Trauma Program. Ambulance New Brunswick procedures for paramedics should direct use of the pelvic binder for all patients with an unstable pelvis. Assess and correct vital signs. Warm IV fluids + pack wounds + immobilize.
14 INITIAL ASSESSMENT IN ER A
15 INITIAL ASSESSMENT IN ER A B
16 INITIAL ASSESSMENT IN ER A B C
17 INITIAL ASSESSMENT IN ER Is there an injury to the pelvis or acetabulum? Is it contributing to hypovolemic shock? Is there an injury I can identify and treat acutely in the ER? Visual inspection Physical exam AP pelvis film

18 INITIAL ASSESSMENT IN ER Essential to expose and observe the skin, front and back. Inquire from EMS personnel as to the integrity of the skin under a pelvic binder
19 INITIAL ASSESSMENT IN ER Other clues to pelvic injury : Leg length discrepancy External rotation of lower limb Bruising and swelling over crest, pubis or perineum Neurological abnormality
20 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY In the setting of hemodynamic instability, radiological cues to pelvic instability are probably best sought out, rather than manipulation ( springing ) of the pelvis. Alternatively, one may push inwards so as to identify any open book component.
21 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY If instability is felt to be present (with inward force), APPLY BINDER.
22 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY Manipulating the pelvis in an unstable patient may cause dislodgement of a clot and more bleeding. It generally becomes a safer maneuver after hours.

23 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY Binder = Sheet = Ex Fix Binders and sheets should be applied over greater trochanters

24 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY Binder = Sheet = Ex Fix Binders and sheets should be applied over greater trochanters

25 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY

26 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY Volume of a sphere = (4/3) πr 3
27 INITIAL ASSESSMENT IN ER + MANAGEMENT OF HEMODYNAMIC INSTABILITY Shock on presentation to ER is highest predictor of mortality (approx 15% overall). Other predictors of mortality include : Large number of blood products over any given timeframe High ISS Venous or cancellous bleeding 80-90% Arterial bleeding in 10-20% (may be higher)

28 MANAGEMENT OF HEMODYNAMIC INSTABILITY Common arterial sources of bleeding Gluteal vessels Corona Mortis
 of the true pelvis which is")
29 MANAGEMENT OF HEMODYNAMIC INSTABILITY Pelvic venous plexus - valveless Bleeding will eventually tamponade due to filling (by blood or sponges) of the true pelvis which is extraperitoneal.
30 MANAGEMENT OF HEMODYNAMIC INSTABILITY Large bore access Warm fluids quickly No response to 2 L crystalloid = initiate transfusion protocol or as per local institution Tranexamic Acid Obtain AP pelvis + trauma CT ideally Further treatment depends on other injuries + needs Lancet Jul 3;376(9734): doi: /S (10) Epub 2010 Jun 14. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised
31 MANAGEMENT OF HEMODYNAMIC INSTABILITY For every 3 minutes of haemodynamic instability in the trauma bay, mortality goes up by roughly 1% Haemodynamically unstable patients should ideally leave the trauma bay within 45 minutes. For those exsanguinating on arrival with sbp less than 70 mm Hg unresponsive to rescucitation, immediate transfer to the OR is indicated.
32 MANAGEMENT OF HEMODYNAMIC INSTABILITY Crash Laparotomy No Yes Unstable fracture pattern Pelvic packing + Ex-Fix simultaneously or Presence of arterial injury on CT* Yes No Still unstable Angio Find other source Fractures of the Pelvis and Acetabulum - 4th ed The EAST Practice Management Guidelines Work Group The Royal Melbourne Hospital HAEMODYNAMICALLY UNSTABLE PELVIC FRACTURE GUIDELINE
33 INITIAL ASSESSMENT IN ER AND MANAGEMENT OF HEMODYNAMIC INSTABILITY : TO EMBOLIZE OR NOT TO EMBOLIZE? AP pelvis Open book = potential to embolize
34 INITIAL ASSESSMENT IN ER AND MANAGEMENT OF HEMODYNAMIC INSTABILITY AP pelvis Vertical Shear = potential to embolize

35 INITIAL ASSESSMENT IN ER AND MANAGEMENT OF HEMODYNAMIC INSTABILITY AP pelvis Lateral compression?

36 INITIAL ASSESSMENT + TREATMENT IN ER If pelvic injury is felt to be present, someone needs to do a rectal and vaginal exam in search of blood May be an open fracture! -Antibiotics -Diverting colostomy -Vaginal repair Mortality for open pelvis fracture is 5-50% Associated injury rate 100%
37 INITIAL ASSESSMENT + TREATMENT IN ER Blood at urinary meatus Bladder rupture or urethral tear What to do? -Inflate foley at meatus (2cc) -Inject contrast up Foley (10cc) -Retrograde urethrogram -Take x-ray as last cc is going in if normal -Advance Foley and do retrograde cystogram (350cc) or contrast CT cystogram

38 INITIAL ASSESSMENT + TREATMENT IN ER

39 INITIAL ASSESSMENT + TREATMENT IN ER Intraperitoneal bladder rupture

40 INITIAL ASSESSMENT + TREATMENT IN ER Extraperitoneal bladder rupture
41 INITIAL ASSESSMENT The AP Pelvis Credit : Dr. Wilber
42 INITIAL ASSESSMENT Credit : Dr. Wilber

43 INITIAL ASSESSMENT Credit : Dr. Wilber
44 INITIAL ASSESSMENT Iliopectineal line Credit : Dr. Wilber
45 INITIAL ASSESSMENT Ilioischial line Credit : Dr. Wilber
46 INITIAL ASSESSMENT Teardrop Credit : Dr. Wilber
47 INITIAL ASSESSMENT Sourcil Credit : Dr. Wilber
48 INITIAL ASSESSMENT Anterior Wall Credit : Dr. Wilber
49 INITIAL ASSESSMENT Posterior Wall Credit : Dr. Wilber
50 INITIAL ASSESSMENT Credit : Dr. Wilber
51 INITIAL ASSESSMENT AP Pelvis Will identify all injuries that require urgent treatment. -Open book type pelvic ring injury with right sacroiliac diastasis

52 INITIAL ASSESSMENT AP Pelvis Pelvic recoil or application of binder will make the injury seem milder.
53 INITIAL ASSESSMENT Vertical shear pelvic ring injury
54 INITIAL ASSESSMENT Vertical shear pelvic ring injury

55 INITIAL ASSESSMENT Binders may make lateral compression type pelvic ring injuries or acetabular injuries worse! Initial Treatment of Pelvic Injuries with Commercially Available Pelvic Binders Results in Displacement of Acetabular Fractures - JBJS
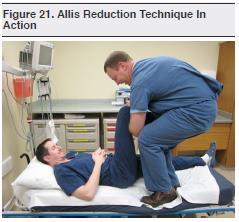
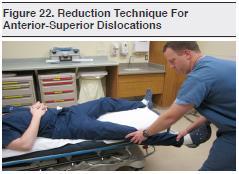
56 INITIAL ASSESSMENT AP Pelvis : other important injuries Hip dislocation

57 INITIAL ASSESSMENT AP Pelvis Hip dislocation

58
59

60 INITIAL ASSESSMENT AP Pelvis Hip dislocation Good to get post reduction CT scan
61 INITIAL ASSESSMENT AP Pelvis Femoral neck fracture in a person in whom it would be undesirable to commit arthroplasty.
62 INITIAL ASSESSMENT Femoral neck fracture in a person in whom it would be undesirable to commit arthroplasty.
63 INITIAL ASSESSMENT AP Pelvis Predict 24h transfusion requirements and mortality High grade open book = 18 units, 30% mortality Vertical shear = 8 units, 25% mortality High grade lateral compression = 7 units, 14% mortality *These relationships have not been reproduced in more recent studies Kregor JOT 2007 Starr JT 2002

64 DEFINITIVE CARE Dr. Wagg (SJRH) and myself have created a call list to help direct these patients for definitive care. NBTP coordinator will have instructions as to who it is best to get in touch with for the patient with a pelvic or acetabular fracture within our province.

65 DEFINITIVE CARE

66
67

68

69 DEFINITIVE CARE

70 DEFINITIVE CARE

71 DEFINITIVE CARE
72 IN SUMMARY - THE 5% YOU SHOULD REMEMBER Manage hypovolemic shock aggressively. Check for associated injuries (perineum). Spend time looking at the AP pelvis and identify embolizable # patterns. Reduce any non-concentric hip that doesn't have an associated femoral neck fracture. These patients require the input and effort of a large multidisciplinary team.
73 ?
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
The Acute Management of Pelvic Ring Injuries
 The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical Module. Pelvic Injury Trauma. Princess Alexandra Hospital Emergency Department. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Surgical Approaches for Fractures and Injuries of the Pelvic Ring
 Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised
Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Northern Trauma Network. Management of Haemodynamically Unstable Patients with Pelvic Injury
 Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay
 Dr Tamás Bodzay") Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Pelvic Trauma. Ø Pelvis: The most important area of the body. Ø Pelvic injuries often represent multisystem
 Pelvic Trauma Jim Holliman, M.D. FACEP Associate Professor of Surgery / Emergency Medicine Director, Center for International Emergency Medicine M.S. Hershey Medical Center Penn State University Hershey,
Pelvic Trauma Jim Holliman, M.D. FACEP Associate Professor of Surgery / Emergency Medicine Director, Center for International Emergency Medicine M.S. Hershey Medical Center Penn State University Hershey,
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Classification, management and outcomes of severe pelvic ring fractures
 Classification, management and outcomes of severe pelvic ring fractures School of Public Health and Preventive Medicine, Monash University The Alfred Hospital, Royal Melbourne Hospital, Epworth Health
Classification, management and outcomes of severe pelvic ring fractures School of Public Health and Preventive Medicine, Monash University The Alfred Hospital, Royal Melbourne Hospital, Epworth Health
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
10/24/18. Bones. Innominate Bone. Hip Socket (Acetabulum) Ligaments. Pubic symphysis Sacroiliac Ligaments Front (anterior) Back (posterior)
 Ligaments. Pubic symphysis Sacroiliac Ligaments Front (anterior) Back (posterior)") Pelvic Fractures David Shearer, MD, MPH Asst. Professor Department of Orthopaedic Surgery UCSF/ZSFG Orthopaedic Trauma InsJtute Mini- medical school 2018 Overview: Pelvic Fractures Anatomy Types of Injuries
Pelvic Fractures David Shearer, MD, MPH Asst. Professor Department of Orthopaedic Surgery UCSF/ZSFG Orthopaedic Trauma InsJtute Mini- medical school 2018 Overview: Pelvic Fractures Anatomy Types of Injuries
ABC of Emergency Radiology
 ABC of Emergency Radiology It is possible for the non-specialist to interpret pelvic radiographs accurately Important anatomical considerations THE PELVIS P A Driscoll, R Ross, D A Nicholson FIG i-line
ABC of Emergency Radiology It is possible for the non-specialist to interpret pelvic radiographs accurately Important anatomical considerations THE PELVIS P A Driscoll, R Ross, D A Nicholson FIG i-line
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
RADIOLOGY OF THE NORMAL ACETABULUM. X-ray X-ray X-ray. Figure. Figure ILIAC OBLIQUE VIEW OBTURATOR OBLIQUE VIEW AP VIEW
 RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH
 IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH Introduction Pelvic fractures occur in approximately 113,000 persons in the United States each year [1], and have a major
IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH Introduction Pelvic fractures occur in approximately 113,000 persons in the United States each year [1], and have a major
Center for Reconstructive Urethral Surgery Guido Barbagli Center for Reconstructive Urethral Surgery Arezzo - Italy
 Guido Barbagli Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it 23 rd ANNUAL EAU CONGRESS Sub-plenary Session on Male urinary incontinence 26 29 March 2008 Milan Italy Incontinence following
Guido Barbagli Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it 23 rd ANNUAL EAU CONGRESS Sub-plenary Session on Male urinary incontinence 26 29 March 2008 Milan Italy Incontinence following
T-PODResponder Pelvic Stabilization Device
 T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
TNP Teaching Station E Focus: Intubated Patient, Interpersonal Violence
 TNP Teaching Station E Focus: Intubated Patient, Interpersonal Violence Objective Upon completion of this teaching station the learner will be able to: 1. demonstrate appropriate assessment for a hemodynamically
TNP Teaching Station E Focus: Intubated Patient, Interpersonal Violence Objective Upon completion of this teaching station the learner will be able to: 1. demonstrate appropriate assessment for a hemodynamically
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
REBOA - Real World. Lena M. Napolitano, MD
 REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
Guido Barbagli. Center for Reconstructive ti Urethral lsurgery
 Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
The functional outcome of surgically treated unstable pelvic ring fractures by open reduction, internal fixation
 Original Research Medical Journal of Islamic Republic of Iran, Vol. 25, No. 2, Aug 2011, pp. 87-93 The functional outcome of surgically treated unstable pelvic ring fractures by open reduction, internal
Original Research Medical Journal of Islamic Republic of Iran, Vol. 25, No. 2, Aug 2011, pp. 87-93 The functional outcome of surgically treated unstable pelvic ring fractures by open reduction, internal
Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends
 ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
5/31/2018. Ipsilateral Femoral Neck And Shaft Fractures. Ipsilateral Neck-Shaft Fractures Introduction. Ipsilateral Neck-Shaft Fractures Introduction
 Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
A Patient s Guide to Stress Fractures of the Hip
 A Patient s Guide to Stress Fractures of the Hip Introduction Stress fractures of the hip once most commonly affected military personnel who marched and ran day after day. Today, stress fractures of the
A Patient s Guide to Stress Fractures of the Hip Introduction Stress fractures of the hip once most commonly affected military personnel who marched and ran day after day. Today, stress fractures of the
Hip Fractures. Anatomy. Causes. Symptoms
 Hip Fractures A hip fracture is a break in the upper quarter of the femur (thigh) bone. The extent of the break depends on the forces that are involved. The type of surgery used to treat a hip fracture
Hip Fractures A hip fracture is a break in the upper quarter of the femur (thigh) bone. The extent of the break depends on the forces that are involved. The type of surgery used to treat a hip fracture
M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH
 Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Orthopedics - Dr. Ahmad - Lecture 2 - Injuries of the Upper Limb
 The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
Complex Fractures and Hip Dislocations
 IMAGING OF HIP PAIN Patients may present with acute (< 2 weeks) or chronic hip pain. Acute pain may be related or not related to an acute traumatic event such as fall or trauma from a motor vehicle accident.
IMAGING OF HIP PAIN Patients may present with acute (< 2 weeks) or chronic hip pain. Acute pain may be related or not related to an acute traumatic event such as fall or trauma from a motor vehicle accident.
The Hip Joint. Exercises and Injuries
 The Hip Joint Exercises and Injuries Pelvis Abnormalities To appreciate the abnormalities that may occur, picture a box around the pelvis. The two most common situations are: 1.the pelvis is tilted forward
The Hip Joint Exercises and Injuries Pelvis Abnormalities To appreciate the abnormalities that may occur, picture a box around the pelvis. The two most common situations are: 1.the pelvis is tilted forward
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
DISLOCATION AND FRACTURES OF THE HIP. Dr Károly Fekete
 DISLOCATION AND FRACTURES OF THE HIP Dr Károly Fekete 1 OUTLINE Epidemiology Incidence Anatomy Patient s examination, clinical symptons Diagnosis Classification Management Special complications 2 EPIDEMIOLOGY,
DISLOCATION AND FRACTURES OF THE HIP Dr Károly Fekete 1 OUTLINE Epidemiology Incidence Anatomy Patient s examination, clinical symptons Diagnosis Classification Management Special complications 2 EPIDEMIOLOGY,
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Lower Extremity Dislocations: Management and Triage on the Field
 Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Emergent Management of Pelvic Ring Fractures with Use of Circumferential Compression
 This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Emergent Management of Pelvic Ring Fractures with Use of Circumferential
This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Emergent Management of Pelvic Ring Fractures with Use of Circumferential
Observation on closed reduction and internal fixation with external fixation in treating unstable pelvic fracture.
 Biomedical Research 2017; 28 (15): 6911-6915 ISSN 0970-938X www.biomedres.info Observation on closed reduction and internal fixation with external fixation in treating unstable pelvic fracture. Wei-Zhou
Biomedical Research 2017; 28 (15): 6911-6915 ISSN 0970-938X www.biomedres.info Observation on closed reduction and internal fixation with external fixation in treating unstable pelvic fracture. Wei-Zhou
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Your Practice Online
 P R E S E N T S Your Practice Online Disclaimer This information is an educational resource only and should not be used to make a decision on hip resurfacing or arthritis management. All decisions about
P R E S E N T S Your Practice Online Disclaimer This information is an educational resource only and should not be used to make a decision on hip resurfacing or arthritis management. All decisions about
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
MANAGEMENT OF FRACTURE. Sudi maiteh (seminar 2 )
") MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
MANAGEMENT OF FRACTURE Sudi maiteh (seminar 2 ) Management of fracture Subjects : _ general management of fractures & Orthopedic patient evaluation _ Closed and open fractures management (Conservative,
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Urethral Injuries: Realignment vs. Delayed Reconstruction
 Urethral Injuries: Realignment vs. Delayed Reconstruction E. Charles Osterberg, MD Assistant Professor of Surgery (Urology) Dell Medical School Chief of Urology and Genitourinary Reconstruction None Disclosures
Urethral Injuries: Realignment vs. Delayed Reconstruction E. Charles Osterberg, MD Assistant Professor of Surgery (Urology) Dell Medical School Chief of Urology and Genitourinary Reconstruction None Disclosures
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
HIP FOLLOW-UP. Thank you for your attention to this matter. If you have any questions, please contact us for assistance. Thomas P.
 HIP FOLLOW-UP It is important to review the status of your hip implant(s) during an office visit at six weeks, one year, two years, and every other year postoperatively thereafter for your safety even
HIP FOLLOW-UP It is important to review the status of your hip implant(s) during an office visit at six weeks, one year, two years, and every other year postoperatively thereafter for your safety even
Analysis of the Importance of Sacroiliac Joint Fractures as a Prognostic Factor of the Patients with Pelvic Fractures
 ORIGINARL ARTICLE J Trauma Inj 2018;31(1):6-11 http://doi.org/10.20408/jti.2018.31.1.6 JOURNAL OF TRAUMA AND INJURY Analysis of the Importance of Sacroiliac Joint Fractures as a Prognostic Factor of the
ORIGINARL ARTICLE J Trauma Inj 2018;31(1):6-11 http://doi.org/10.20408/jti.2018.31.1.6 JOURNAL OF TRAUMA AND INJURY Analysis of the Importance of Sacroiliac Joint Fractures as a Prognostic Factor of the
FAI syndrome with or without labral tear.
 Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Injuries to Muscles, Bones and Joints. Emergency Medical Response
 Injuries to Muscles, Bones and Joints Lesson 33: Injuries to Muscles, Bones and Joints You Are the Emergency Medical Responder You are patrolling the state park where you are the emergency medical responder
Injuries to Muscles, Bones and Joints Lesson 33: Injuries to Muscles, Bones and Joints You Are the Emergency Medical Responder You are patrolling the state park where you are the emergency medical responder
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder
 Case Reports in Urology Volume 2012, Article ID 430746, 4 pages doi:10.1155/2012/430746 Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder Hazim H. Alhamzawi, 1 Husham
Case Reports in Urology Volume 2012, Article ID 430746, 4 pages doi:10.1155/2012/430746 Case Report Delayed Presentation of Traumatic Intraperitoneal Rupture of Urinary Bladder Hazim H. Alhamzawi, 1 Husham
A Patient s Guide to Arthroscopy of the Hip
 A Patient s Guide to Arthroscopy of the Hip Introduction A hip arthroscopy is a procedure where a small video camera attached to a fiberoptic lens is inserted into the hip joint to allow a surgeon to see
A Patient s Guide to Arthroscopy of the Hip Introduction A hip arthroscopy is a procedure where a small video camera attached to a fiberoptic lens is inserted into the hip joint to allow a surgeon to see
Stoppa Approach for Anterior Plate Fixation in Unstable Pelvic Ring Injury
 Original rticle Clinics in Orthopedic Surgery 2016;8:243-248 http://dx.doi.org/10.4055/cios.2016.8.3.243 Stoppa pproach for nterior Plate Fixation in Unstable Pelvic Ring Injury Hyoung-Keun Oh, MD, Suk
Original rticle Clinics in Orthopedic Surgery 2016;8:243-248 http://dx.doi.org/10.4055/cios.2016.8.3.243 Stoppa pproach for nterior Plate Fixation in Unstable Pelvic Ring Injury Hyoung-Keun Oh, MD, Suk
Clinical Practice Guidelines: Can I Learn to Live With Them? What s in the News These Days 2/11/2016. Excessive Costs of Medical Care
 Orthopaedic Trauma Fracture Care: Pushing the Envelope San Diego Clinical Practice Guidelines: Can I Learn to Live With Them? Andrew H. Schmidt, MD What s in the News These Days Excessive Costs of Medical
Orthopaedic Trauma Fracture Care: Pushing the Envelope San Diego Clinical Practice Guidelines: Can I Learn to Live With Them? Andrew H. Schmidt, MD What s in the News These Days Excessive Costs of Medical
How I Do It - Evaluation of the Urethra
 How I Do It - Evaluation of the Urethra Parvati Ramchandani, MD Professor, Radiology and Surgery University of Pennsylvania Medical Center Philadelphia, PA, USA Disclosure of Commercial Interest Neither
How I Do It - Evaluation of the Urethra Parvati Ramchandani, MD Professor, Radiology and Surgery University of Pennsylvania Medical Center Philadelphia, PA, USA Disclosure of Commercial Interest Neither
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Open pelvic fracture: the killing fracture?
 Hermans et al. Journal of Orthopaedic Surgery and Research (2018) 13:83 https://doi.org/10.1186/s13018-018-0793-2 RESEARCH ARTICLE Open Access Open pelvic fracture: the killing fracture? E. Hermans 1*,
Hermans et al. Journal of Orthopaedic Surgery and Research (2018) 13:83 https://doi.org/10.1186/s13018-018-0793-2 RESEARCH ARTICLE Open Access Open pelvic fracture: the killing fracture? E. Hermans 1*,
Unstable fractures of the pelvis treated with a trapezoid compression frame
 Acta Orthop Scand 55, 325-329, 1984 Unstable fractures of the pelvis treated with a trapezoid compression frame Sixteen patients with unstable pelvic fractures were treated by early reduction and fixation
Acta Orthop Scand 55, 325-329, 1984 Unstable fractures of the pelvis treated with a trapezoid compression frame Sixteen patients with unstable pelvic fractures were treated by early reduction and fixation
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Pelvic ring fractures: what to expect
 Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Pelvic ring fractures: what to expect
 Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Hassan R. Mir, MD, MBA, FACS
 DISCLOSURES Hassan R. Mir, MD, MBA, FACS Paid Consultant for a Company or Supplier Smith & Nephew Zimmer Biomet Trice Medical Stock or Stock Options Core Orthopaedics OrthoGrid Systems Research Support
DISCLOSURES Hassan R. Mir, MD, MBA, FACS Paid Consultant for a Company or Supplier Smith & Nephew Zimmer Biomet Trice Medical Stock or Stock Options Core Orthopaedics OrthoGrid Systems Research Support