MUSCULOSKELETAL PHYSICAL EXAMINATION GUIDE FOR GERIATRICIANS Dixie Aragaki, MD Daniel Estrada, MD Updated
|
|
|
- Rodney Newman
- 5 years ago
- Views:
Transcription
1 MUSCULOSKELETAL PHYSICAL EXAMINATION GUIDE FOR GERIATRICIANS Dixie Aragaki, MD Daniel Estrada, MD Updated To facilitate the physical examination for common musculoskeletal ailments, this guide has been prepared for you. An efficient and thorough examination can be performed and documented with this general flow and format: 1) Inspection: landmarks, asymmetry, bony deformity, atrophy, skin changes, etc 2) Palpation: soft tissue/bony prominences, tenderness, warmth, edema/effusion, etc 3) Range of Motion: all planes (noting pain or limitations in passive and active ROM) 4) Neurovascular: include motor, sensory, reflexes, pulses (save most neurologic exam detail for spine exams) 5) Special tests: specific for each joint region Here is an abbreviated list of some Special Tests by musculoskeletal region: (see Appendix for Figures of selected tests) Neck Special tests: Spurling s (+ if referred dermatomal pain with neck extension, rotation, and axial load) Lhermitte s sign (+ if neuropathic/lancinating sensation runs down spine or limbs with neck flexion) Hoffman s Reflex (signals corticospinal tract/umn lesion) => hold wrist and middle finger in passive extension, quick flexion force is then applied to distal phalanx of the middle finger. =>Positive test: flexion of thumb (+/- flexion of index finger) Shoulder Special tests: Hawkins - + if shoulder pain with passive shoulder flexion and internal rotation - suggests subacromial impingement syndrome Yocum s - + suggests subacromial impingement syndrome Empty can - + if pain or weakness when downward force applied to shoulder held in flexion, partial abduction, and internal rotation (thumbs down) - suggests rotator cuff pathology (esp. supraspinatus) Drop arm test + if, from fully abducted position, patient unable to slowly lower arm to side (arm drops) - rare, but + suggests complete tear or major rotator cuff pathology
2 Subscapular Lift-off test - + if patient unable to internally rotate from the starting position with hand behind lower back Speed s - + if resisted shoulder flexion (with elbow in extenion) reproduces anterior shoulder pain, suggests biceps tendon pathology Scapular winging suggests peri-scapular weakness Sulcus sign - + if downward force on arm held in neutral, relaxed position causes a gap or sulcus to form below acromion; suggests either hyperlaxity or instability (i.e. ligament tear) Elbow Special testing: Elbow ligament instability (varus/valgus/anterior/posterior) Tennis elbow (lateral epicondyle pain on resisted wrist extension and passive wrist flexion): (see Cozen s, Mill s, Maudsley s tests ) Golfer s elbow (medial epicondyle pain on resisted wrist flexion and passive wrist extension) Tinel s at elbow for cubital tunnel (percussion of Ulnar nerve refers dysesthesias) Wrist/Hand Special testing: Tinel s for carpal tunnel - + if tapping on median nerve reproduces symptoms Phalen s for carpal tunnel - + if symptoms reproduced with prolonged wrist flexion Carpal tunnel compression test - + if symptoms reproduced with direct prolonged compression across Median nerve at wrist (examiner uses thumbs to press on carpal tunnel) Snuff box tenderness (for suspected Carpal bone/scaphoid fracture) Finkelstein s Test for De Quervain s tenosynovitis Observe for: Trigger finger, Dupuytren contracture Bouchard, Heberden s nodes Classic OA/RA changes L-Spine Special testing: SLR (straight leg raise AKA Lasegue s sign); can perform w/ ankle dorsiflexion as well Crossed Straight leg raise less sensitive/more specific than SLR Slump test (seated straight leg raise) more sensitive and specific than SLR Leg length discrepancy measure ASIS to ipsilateral medial malleolus and compare Facet loading test - hyperextend and laterally rotate lumbar spine to compress facet joints
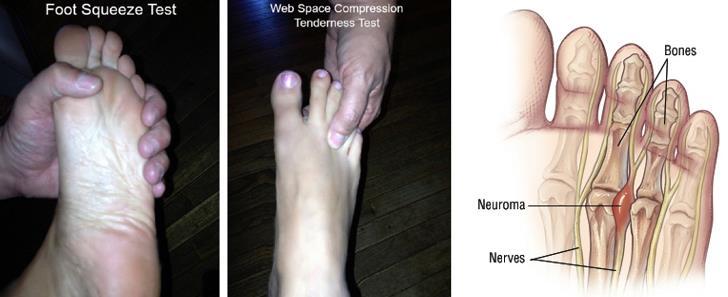
3 Hip Special Testing: Acetabular grind/compression test downward pressure into hip joint; + if pain, suggests OA Thomas test check for hip flexion contracture by starting in supine position with hips flexed toward chest. If unable to lower a leg (1 at a time) completely flat to the table, suspect tight hip flexor muscles (e.g. iliopsoas). FABER s (flex, abd, ext rot) for hip or SI joint pathology depending upon pain location Ober s: test for Tight Iliotibial Band/TFL muscle Piriformis stretch test Trendelenberg sign for weak hip abductor (+ if hip drop contralateral to weak gluteal muscles) Greater Trochanteric bursa tenderness to palpation (often concurrent with IT Band pain syndrome) Knee Special Testing: Patellar grind, compression for patellofemoral syndrome + if direct downward compression on patella recreates pain Varus/valgus stress test for LCL/MCL laxity can be tested in extension and 30⁰ flexion Pes Anserine bursa palpation Lachman s test for ACL laxity/tear. Pull tibia anteriorly with knee at degrees flexion. Ant/Post drawer test to assess ACL/PCL integrity. Force tibia anteriorly/posteriorly with knee at 90 degrees flexion. +if significant tibial movement, especially if greater than asymptomatic side Posterior Sag Sign for PCL laxity/tear. + if tibia sags posteriorly when patient is positioned supine with feet on table in knee/hip flexed position. Thessaly Test of meniscus stand on leg with knee flexed slightly, then rotate about the knee (e.g. like swiveling on a fixed leg with pivot point at the knee); + if pain or locking/clicking sensation at the joint line on medial or lateral side = high likelihood of meniscal pathology. Medial/lateral joint line Tenderness to Palpation (TTP) Ankle/Foot Special Testing: Thompson s test for Achilles tendon integrity + if absence of plantarflexion with squeezing of calf muscles - implies significant Achilles tear unable to passively plantarflex foot Pes planus/cavus (fixed/flexible) Tinel s sign for Tarsal tunnel syndrome - + if tapping posterior to medial malleolus recreates pain down plantar foot in Tibial (medial and lateral plantar nerve branches) distribution Metatarsal head medial/lateral compression (squeeze) test for Morton s neuroma Talar tilt test no hard endpoint with ankle inversion implies ligamentous laxity or disruption Anterior drawer test - + if foot translates forward upon anteriorly directed force of calcaneus at the ankle joint. Laxity implies torn Anterior TaloFibular Ligament (ATFL) lateral ankle sprain. *Observe shoe wear patterns and typical RA and gout deformities

 Test")





4 ***APPENDIX*** CERVICAL/ NEURO Spurling s (Compression) Test Relative contraindications: patient with possible C-spine instability (RA, spinal mets, myelopathy) Hoffman s Reflex SHOULDER Hawkin s (AKA Hawkins-Kennedy) Empty Can Speed s Scapular Winging Sulcus Sign

")




5 ELBOW Cozen s (Tennis Elbow) Tinel s (Ulnar Ulnar Groove) WRIST / HAND Tinel s Phalen s Carpal Compression Finkelstein Test

 Test")


6 BACK / HIP Straight Leg Raise Slump Test FABER (Patrick s) Test Ober s Acetabular grind KNEE Anterior / Posterior Drawer Lachman (only 20 deg flexion)

")



7 Valgus (force inward at knee) / Varus (out at knee) Thessaly ANKLE / FOOT Thompson Test Tinel s at Ankle Talar Tilt Squeeze/compression Test (Morton s Neuroma)
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
PRIMARY CARE EXAMINATION OF KEY JOINTS. Thomas M. Howard, MD, FACSM FFPC Sports Medicine
 PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
12. Acromioclavicular (AC) Joint Compression Test (Shear)
 Joint Compression Test (Shear)") List of Some Common Orthopedic tests: Shoulder 1. Empty Can (Supraspinatus) Test 2. Yergason Test 3. Speed's Test 4. Ludington's Sign 5. Drop Arm Test 6. Apley's Scratch Test 7. Cross-Over Impingement
List of Some Common Orthopedic tests: Shoulder 1. Empty Can (Supraspinatus) Test 2. Yergason Test 3. Speed's Test 4. Ludington's Sign 5. Drop Arm Test 6. Apley's Scratch Test 7. Cross-Over Impingement
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
Physical Exam. Jared Van Der Beek. Basics To Remember. Know the anatomy and how the muscles function.
 Physical Exam Jared Van Der Beek Jared@physio-puncture.com 1 Basics To Remember Know the anatomy and how the muscles function. Know what the special tests are looking for and understand why they are positive.
Physical Exam Jared Van Der Beek Jared@physio-puncture.com 1 Basics To Remember Know the anatomy and how the muscles function. Know what the special tests are looking for and understand why they are positive.
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering Your Musculoskeletal Exam Laurel Short, MSN, FNP-c
 Mastering Your Musculoskeletal Exam Laurel Short, MSN, FNP-c Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in the
Mastering Your Musculoskeletal Exam Laurel Short, MSN, FNP-c Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in the
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO
 Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER
 THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
Musculoskeletal Examination
 Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
Division of Student Affairs A Primer on the Musculoskeletal Examination Technique and Commonly Missed Injuries in Student Health
 Division of Student Affairs A Primer on the Musculoskeletal Examination Technique and Commonly Missed Injuries in Student Health C.S. Nasin, MD, CAQ Sports Medicine Medical Director Head Team Physician
Division of Student Affairs A Primer on the Musculoskeletal Examination Technique and Commonly Missed Injuries in Student Health C.S. Nasin, MD, CAQ Sports Medicine Medical Director Head Team Physician
SMALL GROUP SESSION 16 January 8 th or 10 th. Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
Soft Tissue Rheumatism. Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group
 Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
The examination of the painful knee. Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University
 The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System - Lower Extremities (2.9) 2.9-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System - Lower Extremities (2.9) 2.9-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Taming the Musculoskeletal Exam: İSí, se puede!
 Taming the Musculoskeletal Exam: İSí, se puede! Ronald H. Labuguen, MD UCSF Department of Family and Community Medicine NP/PA/CNM Professional Practice Conference San Francisco Department of Public Health
Taming the Musculoskeletal Exam: İSí, se puede! Ronald H. Labuguen, MD UCSF Department of Family and Community Medicine NP/PA/CNM Professional Practice Conference San Francisco Department of Public Health
Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain
 Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain ID number General health OK Affected Height cm Weight kg Heart OK Arrhythmia Murmurs
Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain ID number General health OK Affected Height cm Weight kg Heart OK Arrhythmia Murmurs
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Overview. MSK talks. Primary Care Sports Medicine. Examining the History and Examination for Common MSK Problems
 Primary Care Sports Medicine Examining the History and Examination for Common MSK Problems A n t h o n y L u k e MD, MPH, CAQ (Sport Med) Associate Professor, Director Primary Care Sports Medicine Primary
Primary Care Sports Medicine Examining the History and Examination for Common MSK Problems A n t h o n y L u k e MD, MPH, CAQ (Sport Med) Associate Professor, Director Primary Care Sports Medicine Primary
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
General Table of Contents
 General Table of Contents Detailed Table of Contents ii List of Classic Special Orthopaedic Tests ix p1 Introduct i1 Chapter I: Ankle & Foot 1 Chapter II: Knee 33 Chapter III: Hip & Innominate 79 Chapter
General Table of Contents Detailed Table of Contents ii List of Classic Special Orthopaedic Tests ix p1 Introduct i1 Chapter I: Ankle & Foot 1 Chapter II: Knee 33 Chapter III: Hip & Innominate 79 Chapter
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Foot and Ankle Physical Exam. The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers
 Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Pain Assessment Patient Interview (location/nature of symptoms), Body Diagram. Observation and Examination: Tests and Measures
, Body Diagram. Observation and Examination: Tests and Measures") Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Work Related Musculoskeletal Disorders
 Work Related Musculoskeletal Disorders Upper Extremity Disorders Carpel tunnel syndrome Cubital tunnel syndrome Thoracic outlet syndrome Raynaud s syndrome (white finger) Rotator cuff syndrome DeQuervain
Work Related Musculoskeletal Disorders Upper Extremity Disorders Carpel tunnel syndrome Cubital tunnel syndrome Thoracic outlet syndrome Raynaud s syndrome (white finger) Rotator cuff syndrome DeQuervain
IFAST Assessment. Name: Date: Sport: Review Health Risk Assessment on initial consult form. List Client Goals (what brings you here?
 IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612
 Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Ankle & Foot Anatomy Stability of the ankle is dependent
Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Ankle & Foot Anatomy Stability of the ankle is dependent
Examining the Physical Exam
 Overview Examining the Physical Exam How to Make Yours Better A n t h o n y L u k e MD, MPH, CAQ (Sport Med) University of California, San Francisco Primary Care Medicine: Update 2017 Quick approach to
Overview Examining the Physical Exam How to Make Yours Better A n t h o n y L u k e MD, MPH, CAQ (Sport Med) University of California, San Francisco Primary Care Medicine: Update 2017 Quick approach to
Examination of the Knee
 Examination of the Knee Wash your hands & Introduce the exam to the patient Positioning & Draping With the patient supine, make sure both legs are exposed in order to compare each side be sure to use draping
Examination of the Knee Wash your hands & Introduce the exam to the patient Positioning & Draping With the patient supine, make sure both legs are exposed in order to compare each side be sure to use draping
Sustained a sprained ankle
 Student Name : Student s Number : 3. Q 1. 2. Sustained a sprained ankle 1. List at least 3 key items you should ask during the history portion of an examination ( ) Possible Answers and Anything Else you
Student Name : Student s Number : 3. Q 1. 2. Sustained a sprained ankle 1. List at least 3 key items you should ask during the history portion of an examination ( ) Possible Answers and Anything Else you
Arthritic history is similar to that of the hip. Add history of give way and locking, swelling
 KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
Ligamentous and Meniscal Injuries: Diagnosis and Management
 Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
Trauma & Orthopaedic Undergraduate Syllabus
 Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
Trauma & Orthopaedic Undergraduate Syllabus Introduction The purpose of this document is to provide a recommended syllabus for medical students in Trauma & Orthopaedics (T&0). It should help students on
SIT DOWN, STAND UP, BEND OVER
 SIT DOWN, STAND UP, BEND OVER A Review of the Musculoskeletal Physical Examination Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
SIT DOWN, STAND UP, BEND OVER A Review of the Musculoskeletal Physical Examination Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Preface The first decade of the twenty-first century has witnessed the continuation of an explosion in our knowledge and understanding of all aspects of disease. Accompanying this has been the increasing
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Clinical Orthopedic Testing Review
 SIMMONDS TEST: Patient is prone Doctor flexes the patients knee to 90 degrees Doctor squeezes the patient s calf. Classical response: Failure of ankle plantarflexion Classical Importance= torn Achilles
SIMMONDS TEST: Patient is prone Doctor flexes the patients knee to 90 degrees Doctor squeezes the patient s calf. Classical response: Failure of ankle plantarflexion Classical Importance= torn Achilles
 Musculoskeletal Exams and Injections Knee Ankle Shoulder Wrist Back www.fisiokinesiterapia.biz Learning Objectives 1-Knee exam for effusion and tears of menisci and ligaments 2-Ankle exam to differentiate
Musculoskeletal Exams and Injections Knee Ankle Shoulder Wrist Back www.fisiokinesiterapia.biz Learning Objectives 1-Knee exam for effusion and tears of menisci and ligaments 2-Ankle exam to differentiate
The Knee. Two Joints: Tibiofemoral. Patellofemoral
 Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Hip Joint DX 612 Orthopedics and Neurology
 Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Anatomy. Hip Joint DX 612 Orthopedics and Neurology. Hip ROM. Palpation
 Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Solving Today s Pain and Injury Puzzle with Erik Dalton An Online Workshop for ABMP Members Session 4 Handout
 Solving Today s Pain and Injury Puzzle with Erik Dalton An Online Workshop for ABMP Members Session 4 Handout Please Note: Erik Dalton teaches his Myoskeletal Alignment Techniques with the expectation
Solving Today s Pain and Injury Puzzle with Erik Dalton An Online Workshop for ABMP Members Session 4 Handout Please Note: Erik Dalton teaches his Myoskeletal Alignment Techniques with the expectation
Osteopathic Manipulation for the Knee and Shoulder
 Osteopathic Manipulation for the Knee and Shoulder Carlton A Richie III DO FAAFP CAQ; Sports Medicine Associate Professor; Midwestern University Disclosure Statement Nothing to disclose Learning Objectives
Osteopathic Manipulation for the Knee and Shoulder Carlton A Richie III DO FAAFP CAQ; Sports Medicine Associate Professor; Midwestern University Disclosure Statement Nothing to disclose Learning Objectives
Rheumatology & Immunology. Regional pain syndromes to be covered today. Some definitions. Tendinitis. Bursitis. History. History. Exam.
 Rheumatology & Immunology Some problems are difficult, but diagnosing and treating soft tissue syndromes are not! Soft tissue syndromes one of the most common reasons patients present to their doctor.
Rheumatology & Immunology Some problems are difficult, but diagnosing and treating soft tissue syndromes are not! Soft tissue syndromes one of the most common reasons patients present to their doctor.
Contraindicated and High-Risk Exercises
 Contraindicated and High-Risk Exercises Young sub Kwon, Ph.D. ACSM RCEP, NSCA CSCS,*D Exercise Physiology Laboratory The University of New Mexico Albuquerque, NM, USA Introduction Any activity selected
Contraindicated and High-Risk Exercises Young sub Kwon, Ph.D. ACSM RCEP, NSCA CSCS,*D Exercise Physiology Laboratory The University of New Mexico Albuquerque, NM, USA Introduction Any activity selected
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
Orthopaedic Physical Examination of the Shoulder
 Orthopaedic Physical Examination of the Shoulder Feel 1. Exposure 2. Inspect from front, back, side, for asymmetry, deformities, scars, sinuses, muscle wasting (esp deltoid, supraspinatus and infraspinatus).
Orthopaedic Physical Examination of the Shoulder Feel 1. Exposure 2. Inspect from front, back, side, for asymmetry, deformities, scars, sinuses, muscle wasting (esp deltoid, supraspinatus and infraspinatus).
Disclaimer. Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient. Objectives. Anatomy
 Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
a. Demonstration & Practise of the Technique...4 b. Refining the Feel of the Technique...4 c. Practical Application to the Body Generally...
 Course Outline Course Overview Goltech Basic: Cross-Fibre Muscle Release...4 1. History & Development of Goltech...4 2. Musculo-Skeletal System as relevant to Goltech...4 3. Why Goltech cross-fibre muscle
Course Outline Course Overview Goltech Basic: Cross-Fibre Muscle Release...4 1. History & Development of Goltech...4 2. Musculo-Skeletal System as relevant to Goltech...4 3. Why Goltech cross-fibre muscle
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Arthritis and Rheumatology Clinics of Kansas Patient Education
 Arthritis and Rheumatology Clinics of Kansas Patient Education Regional Pain Syndromes Introduction: At some time in the course of life, virtually everyone will experience pain in a tendon, muscle, or
Arthritis and Rheumatology Clinics of Kansas Patient Education Regional Pain Syndromes Introduction: At some time in the course of life, virtually everyone will experience pain in a tendon, muscle, or
Knee Injury Assessment
 Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
SMALL GROUP SESSION 21B February 10 th or February 12 th. Lower Extremity Examination and Ethics Case Discussion
 SMALL GROUP SESSION 21B February 10 th or February 12 th Lower Extremity Examination and Ethics Case Discussion Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 21B February 10 th or February 12 th Lower Extremity Examination and Ethics Case Discussion Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
Prevention and Treatment of Injuries. Anatomy. Anatomy. Chapter 20 The Knee Westfield High School Houston, Texas
 Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Overview Ligament Injuries. Anatomy. Epidemiology Very commonly injured joint. ACL Injury 20/06/2016. Meniscus Tears. Patellofemoral Problems
 Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION
 Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
Exam of the Knee and Ankle I HAVE NO FINANCIAL DISCLOSURES RELEVANT TO THIS PRESENTATION Disclosures I have no relevant financial relationships with the manufacturers of any commercial products and or
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
Phase II Health Sciences as Applied to Coaching.
 Phase II Health Sciences as Applied to Coaching www.topform.us Overview What is going to be covered today is.. Skeletal System Muscular System Most common injuries to know about in your sport Part One:
Phase II Health Sciences as Applied to Coaching www.topform.us Overview What is going to be covered today is.. Skeletal System Muscular System Most common injuries to know about in your sport Part One:
Anatomy and evaluation of the ankle.
 Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
31b Passive Stretches:! Technique Demo and Practice - Lower Body
 31b Passive Stretches:! Technique Demo and Practice - Lower Body 31b Passive Stretches:! Technique Demo and Practice - Lower Body! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
31b Passive Stretches:! Technique Demo and Practice - Lower Body 31b Passive Stretches:! Technique Demo and Practice - Lower Body! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
The Swimmer s Shoulder: An Osteopathic Approach
 The Swimmer s Shoulder: An Osteopathic Approach Mary Solomon, D.O. Rainbow Babies and Children s Hospital Cleveland, OH 440-914-7865 1 I have no relevant relationships/affiliations with any proprietary
The Swimmer s Shoulder: An Osteopathic Approach Mary Solomon, D.O. Rainbow Babies and Children s Hospital Cleveland, OH 440-914-7865 1 I have no relevant relationships/affiliations with any proprietary
Practical 1 Worksheet
 Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
General Procedure and Rules
 General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
Dupuytrens contracture
 OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
OA Wrist Ganglion/Cysts Dupuytrens contracture Carpal Tunnel Syndrome Carpal Tunnel pathway For advice on management of CTS please follow link to Map of Medicine Trigger Finger Trigger finger pathway For
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Inspection. Physical Examination of the Elbow. Anterior Elbow 2/14/2017. Inspection. Carrying angle. Lateral dimple. Physical Exam of the Elbow
 of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
Contents. copyrighted material by PRO-ED, Inc. Chapter 1. Chapter 2. Chapter 3. Chapter 4. Chapter 5. Conditions in Athletic Injuries
 Acknowledgments xiii Introduction to the First Edition xv Introduction to the Second Edition xvii Chapter 1 Conditions in Athletic Injuries Anterior Cruciate Ligament (ACL) Tear 2 Biceps Tendon Strain
Acknowledgments xiii Introduction to the First Edition xv Introduction to the Second Edition xvii Chapter 1 Conditions in Athletic Injuries Anterior Cruciate Ligament (ACL) Tear 2 Biceps Tendon Strain
emoryhealthcare.org/ortho
 COMMON SOCCER INJURIES Oluseun A. Olufade, MD Assistant Professor, Department of Orthopedics and PM&R 1/7/18 GOALS Discuss top soccer injuries and treatment strategies Simplify hip and groin injuries in
COMMON SOCCER INJURIES Oluseun A. Olufade, MD Assistant Professor, Department of Orthopedics and PM&R 1/7/18 GOALS Discuss top soccer injuries and treatment strategies Simplify hip and groin injuries in
Knee Injuries. PSK 4U Mr. S. Kelly North Grenville DHS. Medial Collateral Ligament Sprain
 Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective
 On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
On Field Assessment and Management of Acute Knee Injuries: A Physiotherapist s Perspective Jessica Condliffe Physiotherapist / Clinic Manager TBI Health Wellington Presentation Outline Knee anatomy review
Please differentiate an internal derangement from an external knee injury.
 Knee Orthopaedic Tests Sports and Knee Injuries James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Knee Injury Strain, Sprain, Internal Derangement Anatomy of the Knee Please
Knee Orthopaedic Tests Sports and Knee Injuries James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Knee Injury Strain, Sprain, Internal Derangement Anatomy of the Knee Please
Anatomy and Physiology 2016
 Anatomy and Physiology 2016 O = Temporal line I = coronoid process (Mandible) A = elevates mandible (chewing) O = galea aponeurotica (layer of dense fibrous tissue which covers the upper part of the cranium)
Anatomy and Physiology 2016 O = Temporal line I = coronoid process (Mandible) A = elevates mandible (chewing) O = galea aponeurotica (layer of dense fibrous tissue which covers the upper part of the cranium)
BIOE221. Session 11. Musculoskeletal System. Bioscience Department. Endeavour College of Natural Health endeavour.edu.au
 BIOE221 Session 11 Musculoskeletal System Bioscience Department Session Objectives o Review the major structures and functions of the musculoskeletal system system in order to be able to assess its motor
BIOE221 Session 11 Musculoskeletal System Bioscience Department Session Objectives o Review the major structures and functions of the musculoskeletal system system in order to be able to assess its motor
ADOLESCENT SPORTS INJURIES. Orthopaedics in Motion April 5, 2017 John Lammli, MD
 ADOLESCENT SPORTS INJURIES Orthopaedics in Motion April 5, 2017 John Lammli, MD OVERVIEW: Shoulder Injuries Knee Injuries Leg/Ankle Injuries SHOULDER INJURIES Injuries to the shoulder girdle are vast and
ADOLESCENT SPORTS INJURIES Orthopaedics in Motion April 5, 2017 John Lammli, MD OVERVIEW: Shoulder Injuries Knee Injuries Leg/Ankle Injuries SHOULDER INJURIES Injuries to the shoulder girdle are vast and
SYLLABUS. 3 units, 53 Hours (3 Hr Lecture, 2 Hr Lab/Wk)
") SYLLABUS Name of Course: Length of Course: Course Description: Prerequisites: Course Offered by: Required Texts: Recommended Texts: Biomechanics and Examination of the Extremities DIAG 327/827(lab) 3 units,
SYLLABUS Name of Course: Length of Course: Course Description: Prerequisites: Course Offered by: Required Texts: Recommended Texts: Biomechanics and Examination of the Extremities DIAG 327/827(lab) 3 units,
Goals &Objectives. 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop:
 Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Outline. Knee Anatomy. Physical Exam Skills and Office Procedures in Orthopaedics. The quadriceps muscles extend the knee 7/23/2013
 Physical Exam Skills and Office Procedures in Orthopaedics Outline Knee exam Knee aspiration and injection Shoulder exam Subacromial bursa injection UCSF Essentials of Primary Care August 14, 2012 Carlin
Physical Exam Skills and Office Procedures in Orthopaedics Outline Knee exam Knee aspiration and injection Shoulder exam Subacromial bursa injection UCSF Essentials of Primary Care August 14, 2012 Carlin