28 Periacetabular Resections
|
|
|
- Sharleen Lawrence
- 5 years ago
- Views:
Transcription
1 Malawer Chapter 28 22/02/ :54 Page Periacetabular Resections Martin Malawer OVERVIEW The traditional treatment of periacetabular sarcomas has been a classical hemipelvectomy; that is, an amputation through the sacroiliac joint and symphysis pubis. Limb-sparing surgery, i.e. periacetabular resection and reconstruction, has been notoriously difficult. Tumors of the periacetabular area are difficult to treat and traditionally have a high complication and morbidity rate. The surgical alternatives for reconstruction of a periacetabular defect have been iliofemoral arthrodesis, ischiofemoral arthrodesis, or flail extremity. Within the past decade the development of a saddle prosthesis by Waldemar-Link (Hamburg, Germany) has made the reconstruction of periacetabular defects more satisfactory and has dramatically decreased surgical morbidity. The surgical anatomy of the pelvis must be well understood in order to perform a periacetabular resection safely. The key to success is wide exposure both anteriorly, i.e., retroperitoneal (ilioinguinal incision) and posteriorly, a large gluteus maximus fasciocutaneous flap to expose the retrogluteal area. The retrogluteal area consists of the ilium, sciatic notch, sciatic nerve, and hip joint. This combined exposure permits safe dissection of large tumors of the acetabulum and preservation of the important neurovascular and visceral structures. Reconstruction can easily be performed through this approach. Imaging studies are extremely important in order to determine the extent of the tumor within the periacetabular region of the pelvis. The tumor must be confined to the lower portion of the ilium and the periacetabulum but may extend into the pubic rami. Specifically, a combination Type II and III pelvic resection can be performed versus a pure Type II, periacetabular resection. CT, MRI, and bone scan is required to determine the level of iliac resection as well as the sites of the other osteotomies. Angiography is required to determine iliac vessel displacement, especially the hypogastric (internal iliac) artery, and venography is utilized to determine the presence of intramural tumor thrombi. The hypogastric artery is usually ligated. CT scan, in conjunction with MRI, is useful to determine the extraosseous component and the extension into the pelvis as well as the retrogluteal area. The utilitarian incision of the pelvis is used to expose the retroperitoneal area to mobilize the iliac vessels and to mobilize the tumor. The superior pubic ramus is identified anteriorly by retraction of the iliac femoral vessels. Posteriorly, the sciatic notch in the ilium is identified and an osteotomy is performed through the sciatic notch with the sciatic nerve protected. The third osteotomy is through the ischium or the posterior column, depending on the exact location of the tumor. The entire periacetabular tumor can then removed posteriorly after detaching the sacrospinous ligament Several different methods of reconstruction have been developed over the past two decades: ischiofemoral arthrodesis, pelvic allograft, iliofemoral arthrodesis, and a flail hip; however, this chapter will emphasize the use of the saddle prosthesis. The chapter will discuss the use of the saddle prosthesis, its unique surgical and technical considerations (especially of a notchplasty) and the muscle reconstruction required in order to obtain a good functional result.
2 Malawer Chapter 28 22/02/ :54 Page Musculoskeletal Cancer Surgery INTRODUCTION Five percent of primary malignant bone tumors involve the pelvis. Osteosarcoma in adolescents, Ewing s sarcoma in children, and chondrosarcoma in adults are the most common primary sarcomas in this location. More commonly, though, neoplasms involving the pelvis occur as a result of metastatic spread from the breast, lung, prostate, kidney, or thyroid. Diffuse involvement of the pelvis is often seen, but bony destruction of the periacetabulum is of greatest concern as patients often present with severe pain and dysfunction that may not respond to limited weight-bearing and radiotherapy alone. Tumors arising in the periacetabular region of the pelvis pose a difficult problem (Figure 28.1). Classically, hemipelvectomy was the primary means of surgical intervention. With the advent of aggressive chemotherapy, better imaging studies and more advanced surgical techniques, limb-sparing resections have been carried out for primary malignancies of the pelvis and metastatic lesions that have failed other forms of treatment. Periacetabular resections should accomplish the goal of achieving an adequate tumor resection with minimal morbidity followed by a reliable and functional reconstruction. Techniques of surgical reconstruction include: ischiofemoral arthrodesis, iliofemoral arthrodesis, pelvic allograft, custom prosthesis, flail extremity, and, more recently, a custom saddle prosthesis. Given the complexity of the anatomy and the use of adjuvant therapies that require an uncomplicated and expedient postoperative recovery, osseous pelvic resections remain one of the greatest surgical challenges. This chapter will discuss the senior author s experience with saddle prostheses as a means of safe, reliable, pelvic reconstruction. UNIQUE ANATOMIC CONSIDERATIONS Pelvic Muscles The pelvis is virtually covered by muscle that acts as a barrier to tumor extension into adjacent vessels and nerves. This is especially true of tumors arising in the ilium and periacetabular region. 1. Iliacus. This muscle provides protection from tumors extending from the inner cortex of the ilium. It often contains the tumor until it becomes very large, and usually provides an adequate margin of resection. 2. Gluteus medius and minimus. These muscles cover the superior and inferior aspects of the outer cortex of the ilium. 3. Piriformis. This muscle, which extends from the sacrum to the greater trochanter, fills the greater sciatic notch and tends to protect the sciatic nerve from tumors that extend in this area. Neurovascular Bundle 1. Femoral vessels and nerve. Tumors arising from the superior pubic ramus are close to these structures (see Figure 28.1). A thick neurovascular sheath usually protects them from tumor extension. If necessary, the femoral vessels and nerve can be carefully dissected free from the sheath, leaving it with the resected specimen. 2. Sciatic nerve. Tumors extending from the ilium into the sciatic notch may be immediately adjacent to this nerve. Usually the nerve is not directly infiltrated and can be dissected free from the tumor pseudocapsule. Bladder/Urethra The bladder is separated from the anterior pubis by thick fibrous tissue that is an extension of the pecten pubis and the retropubic fat. The urethra, located just inferior to the symphysis pubis, is separated from it by the arcute ligament. The surgeon must protect these structures when dealing with tumors arising from the anterior pelvis. Sacroiliac Joint Extension of tumor across the joints of the pelvis is frequently reported. Careful preoperative and intraoperative evaluation of the sacroiliac joint is necessary (Figure 28.2). Pelvic tumor extension, in particular chondrosarcoma, can be difficult to evaluate even with modern imaging modalities. Pelvic Veins Tumor thrombi within the large pelvic veins has been reported for pelvic sarcomas. Meticulous preoperative evaluation with the use of MRI and venography is necessary. IMAGING STUDIES Appropriate imaging studies are the key to successful resection of tumors of the pelvis and acetabulum. Computerized tomography (CT), magnetic resonance imaging (MRI), angiography, and bone scintigraphy (three-phase bone scan) are the most useful preoperative studies. For tumors of the pelvis and acetabulum with a large extraosseous component, a venogram may be warranted if there is evidence of distal obstruction.

 Initial CT scan demonstrating a small lesion of the acetabulum within the superior medial wall.")

 Staging angiography shows no displacement of the external iliac artery or common femoral artery.")
3 Malawer Chapter 28 22/02/ :54 Page 425 Periacetabular Resections 425 A B D C Figure 28.1 Periacetabular chondrosarcoma. There is a small, intraosseous, high-grade chondrosarcoma of the superior pubic ramus that extends along the medial wall and into the posterior acetabulum. (A) Initial CT scan demonstrating a small lesion of the acetabulum within the superior medial wall. (B) CT scan demonstrating the anterior and posterior extent of the periacetabuluar tumor. Note the biopsy is performed anteriorly away from the major vessels. Biopsies are generally not performed posteriorly in case a hemipelvectomy flap is required. (C) Staging angiography shows no displacement of the external iliac artery or common femoral artery. There is minimal tumor vascularity. (D) Postoperative radiograph (9 months) following a partial pelvic resection (Type II/III). Note the sclerosis around the saddle prosthesis, which is a common finding denoting increased heterotopic bone along the saddle. This bone provides additional stability.



4 Malawer Chapter 28 22/02/ :54 Page Musculoskeletal Cancer Surgery The information to be obtained from each of these studies is as follows: Radiographs The radiographic characterization of most bone lesions on the initial plain films of the pelvis usually gives an indication of whether the tumor is a primary sarcoma, metastatic lesion, or benign process. These findings may be very subtle, however, so that one must be extremely cautious in their interpretation (e.g. chondrosarcoma of the pelvis). A patient with persistent pain in the hip or pelvic region, despite normal plain radiographs, should be further evaluated with additional imaging studies. Bone Scan The bone scan is used to assess the extent of tumor involvement and to evaluate for metastases. The flow phase and blood pool images are also helpful in assessing tumor vascularity. Tumor extension into the ilium and pelvic columns must be evaluated. CT Scan Because it shows mineralization, CT is superior to MRI for visualizing subtle cortical destruction, calcification or ossification, and fracture (Figure 28.3). This remains the study of choice by many for evaluation of the degree of cortical destruction of the pelvis, which is often critical in the periacetabular region (i.e. in evaluating the acetabular dome and columns of the pelvis). CT provides more reliable imaging for determination of the effects of induction chemotherapy and bone response. It is considered complementary to MRI in evaluating softtissue extent and displacement of adjacent nerves and vessels. Careful evaluation of iliac extension is required. Figure 28.2 A large chondrosarcoma of the ilium involving the adjacent sacral alar. CT scans are extremely useful in determing SI joint and sacral alar involvement. If the sacrum is involved, a limb-sparing resection and even a hemipelvectomy often cannot be performed. MRI Magnetic resonance is the imaging method of choice for detecting tumor extension into the hip joint, sacroiliac joint, or sacrum, and extension into the superior A B Figure 28.3 MRI scan and CT scan of an extremely large chondrosarcoma arising from the wing of the ilium and the periacetabular bone. (A) MRI: the high-intensity area represents gross tumor permeating through the ilium. Note that there is no intrapelvic extension. (B) CT scan: the large soft-tissue component is seen arising from the underlying ilium. It approaches the SI joint but a resection can be performed through the sacral alar. In general, CT scans are more helpful than MRI scans for determining bony involvement.

5 Malawer Chapter 28 22/02/ :54 Page 427 Periacetabular Resections 427 pubic rami and ischial region (Figure 28.3). MRI shows the fat of the marrow with superior contrast, and is therefore the best modality to demonstrate intraosseous tumor extension. This is extremely important in tumors that demonstrate subtle infiltration within the ilium, such as chondrosarcoma. MRI is superior for evaluation of soft-tissue tumor extent and for evaluating critical neurovascular structures (i.e. sacral plexus and iliac vessels) (Figure 28.4). If tumor extends to the superior pubic ramus or the ischium, then a combined Type II/III resection is required. Arteriography/Venography Although MRI and MRA (magnetic resonance arteriography) can be used to visualize the pelvic vessels, arteriography remains the most useful study for evaluating tumor vascularity and anatomy. It more accurately assesses the vascular anatomy, including anatomic variants and anomalies. Arteriography is the most reliable study to determine the response to neoadjuvant chemotherapy. The venous flow phase is useful to detect venous occlusion or tumor thrombi. If there is any suggestion of venous occlusion, a formal venogram should be performed. The femoral vessels are often displaced by large periacetabular tumors. Biopsy The biopsy technique and placement is of paramount importance in periacetabular tumors as the risk of peritoneal and pelvic contamination is considerable and local control is a greater challenge (Figure 28.1). A misplaced or poorly performed biopsy can lead to extensive soft-tissue contamination and render resection difficult or not feasible. A poorly performed biopsy may be the primary reason a patient has a hemipelvectomy, and it may even interfere with softtissue flaps necessary for wound coverage. Most patients with periacetabular tumors are best served with a needle biopsy placed in the incision line of the planned future resection. CT guidance should be used unless there is a large extraosseous component that is easily accessible and away from critical neurovascular structures. The needle biopsy is performed anteriorly. The posterior approach should be avoided so as not to contaminate the gluteus maximus, hip joint, femoral vessels, and femoral nerve. A patient who has a needle biopsy that does not provide a definitive diagnosis should undergo an open incisional biopsy in the operating room, with special emphasis on biopsy placement and ensuring adequate tissue for diagnosis. Figure 28.4 MRI scan of a high-grade sarcoma arising from the ilium, crossing the SI joint, and involving the L5 transverse process. This tumor is considered to be unresectable due to the extension along the sacrum and the lumbar spine. MRI scans are invaluable in determining extraosseous soft-tissue extension of bony tumors. INDICATIONS AND CONTRAINDICATIONS OF LIMB-SPARING SURGERY Most primary periacetabular tumors can be resected without amputating the lower extremity. Periacetabular resection is indicated in cases in which; (1) surgical margins similar to those obtained with a hemipelvectomy can be accomplished; (2) the resection (and reconstruction) can preserve a reasonably functional limb; (3) the life expectancy and general physical status of the patient justify the procedure. Contraindications include: (1) local recurrence following a previous limbsparing resection unless the recurrence can be widely resected or the amputation offers no oncologic benefit; (2) tumor extension posteriorly across the sacroiliac joint with involvement of the sacral nerves and nerve root foramen; (3) tumors which extensively infiltrate the soft tissues of the pelvis and extend into the thigh with or without involvement of the sciatic nerve; (4) poor overall physical status or limited life expectancy. DESCRIPTION OF IMPLANTS Saddle Prosthesis The saddle prosthesis was originally designed for reconstruction in patients who sustained extensive loss of acetabular bone after failed total hip arthroplasty. Similar defects are often encountered following periacetabular tumor resection, with previously described reconstruction techniques being fraught with high local morbidity and complication rates. Since 1988 the authors have used the saddle prosthesis, with favorable results, for reconstruction of the pelvis following Type

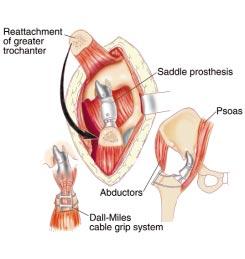
6 Malawer Chapter 28 22/02/ :55 Page Musculoskeletal Cancer Surgery II and Type II/III periacetabular resections for primary sarcomas and in patients with metastatic disease. Since its initial development the prosthesis has undergone several design changes to address design-related problems. The unique and crucial surgical considerations for implanting the saddle prosthesis should be emphasized. These include: retaining at least 2 cm of remaining ilium following tumor resection, creating a notch within the remaining ilium that is within the depth of the saddle component and is located in the thickest (medial) portion of bone, retaining the iliopsoas and abductor muscles and adjusting the pelvic femoral tension with the correct interpositional base component length (see Surgical Technique, below). The metal saddle component rests on a polyethylenebearing sleeve which rotates on a peg attached to the base component (Figure 28.5). The base component is available in several lengths to accommodate variable amounts of bone loss following tumor resection. The base is attached to the stem taper in place of a femoral head. A Figure 28.5 (see also following page) (A) Saddle prosthesis for periacetabular replacement and reconstruction. The saddle prosthesis (Waldemar-Link, Hamburg, Germany) was originally developed for use in total hip revision surgery. This prosthesis is now used to reconstruct the pelvis following periacetabular resections. The prosthesis consists of three components; the femoral stem, base element (body), and the saddle portion that articulates with the ilium. (B) Degrees of motion of saddle prosthesis. The saddle is free to rotate on the body component. The entire prosthesis can abduct, adduct, flex, and extend through the saddle and iliac articulation. (C) Periacetabular resection (Type III) with the saddle prosthesis reconstruction. (D) Reconstruction. Photograph of the pelvic bony structure. The lines demarcating the extent of a periacetabular resection. The superacetabular osteotomy can be performed close to the acetabulum or as high as the sciatic notch (as shown). The lower the osteotomy, the more stable the prosthesis. The osteotomy along the superior pubic ramus can be made along the medial wall up to the symphysis pubis. The osteotomy of the inferior pubic ramus or pubic bone can be performed at several different levels according to the oncological needs. In general, periacetabular reconstructions are performed with a saddle prosthesis (Waldemar-Link, Hamburg, Germany). (E) Type II and Type III combined pelvic resection for a large, high-grade chondrosarcoma reconstructed with a saddle prosthesis. Note the typical reossification which occurs around the pericapsular structure (forms around the saddle component). This reactive bone is typically seen between 12 and 16 months. This reactive bone (arrows) increases the stability of the prosthesis. Adequate reconstruction consists of the preservation of the iliacus muscle, the abductor muscles, and the use of a notch within the ilium to create stability for the saddle.
.")

 can occur in the saddle prosthesis,")

7 Malawer Chapter 28 22/02/ :55 Page 429 Periacetabular Resections 429 B D E C Figure 28.5 C E A blunt-tipped set screw engages a circumferential groove in the peg (without placing any load on the metal). The set screw prevents the saddle and base component from dislocating. A locking pin located within the conical recess of the base engages an eccentric slot in the face of the taper. This prevents rotational instability within the conical mounting. This is necessary because axial forces (depending on the length of the base component) can occur in the saddle prosthesis, unlike an implant with a spherical femoral head. Anatomy The saddle component of the prosthesis articulates against a notch that the surgeon makes in the medial portion of the remaining ilium. One horn of the saddle lies within the true pelvis and is covered by the iliopsoas muscle. The other horn of the saddle is located outside the pelvis and is covered by the gluteus medius and minimus muscles.
8 Malawer Chapter 28 22/02/ :55 Page Musculoskeletal Cancer Surgery Motion The articulation between the saddle and iliac bone permits the leg to be turned in any direction (Figure 28.5C). Rotation is made possible within the articulation between the saddle and the base component. SURGICAL GUIDELINES 1. The utilitarian incision is utilized to expose both the anterior (internal) and posterior (extrapelvic) aspects of the pelvis. The ilioinguinal incision is utilized to develop the retroperitoneal plane and the posterior gluteus maximus fasciocutaneous flap is utilized to develop the retrogluteal space. 2. The iliac vessels are initially mobilized and the hypogastric artery is identified and may be ligated. The sciatic and femoral nerves are identified and protected. 3. The level of osteotomy through the ilium is identified from within the pelvis as well as the superior pubic rami. Identification of the superior pubic rami requires mobilization of the external iliac and femoral vessels as they cross the ramus. 4. A large posterior myocutaneous flap is developed with the gluteus maximus muscle. The gluteal maximus muscle is detached from the iliotibial band and femur so as to be retracted posteriorly. This exposes the retrogluteal space; the ilium, sciatic notch, sciatic nerve, and hip joint. 5. The ischium is identified through the posterior incision and is osteotomized above the level of the biceps tendon insertion. 6. Complete removal of the periacetabulum requires the release of the sacrospinous ligament and some of the pelvic floor musculature. 7. Reconstruction of the periacetabular defect is performed with the saddle prosthesis (Link, Hamburg, Germany). Postoperative immobilization is required for days with the lower extremity in abduction to protect the prosthesis and the abductor muscles. A hip abduction brace is utilized for 3 months. Physical therapy and rehabilitation requires 6 9 months to become fully ambulatory with a cane. RECONSTRUCTION FOLLOWING RESECTION OF PRIMARY PERIACETABULAR TUMORS Saddle Prosthesis Schematic of Surgical Procedures (Figures ) Notchplasty (Figure 28.6) A notch is created in the remaining ilium using a highspeed burr. The notch should be placed in the thickest region of the remaining bone (usually medial). The notch accommodates the saddle component of the saddle prosthesis and its depth matches that of the saddle. When positioned intraoperatively the notch between the two horns of the saddle prosthesis is perpendicular to the notch created in the bone. The notch facilitates articulation between the saddle prosthesis and the remaining ilium and lends stability during subsequent hip motion (Figure 28.6). Preparation of the Proximal Femur The proximal femur is prepared as for a standard femoral component. The proximal femur intramedullary canal is reamed to accept the largest diameter stem and allow for a 2-mm circumferential cement mantle. Once reaming is completed, and the appropriate-sized stem (diameter and length) is selected, a distal femoral cement plug is inserted to a depth of 2 cm below the tip of the selected femoral stem. The femoral canal is then irrigated with saline and packed with gauze. Once the cement (PMMA) is prepared, the gauze is removed and femoral prosthesis is cemented within the proximal femur. Trial Reduction (Figure 28.7) A reduction using trial components is critical in assessing the accurate length of the base component (intercalary segment) and determining optimum softtissue tension. The base component length selected should be determined by the distance between the ilium and femoral neck cuts, as the length indicated on the base component is the total length from the notch of the saddle to the femoral collar. A base component should be selected where reduction is barely possible with minimum play in the reduced joint. The surgeon should be able to reattach the abductor mechanism to its anatomic position on the osteotomized greater trochanter. A trial reduction can also determine areas where the saddle component may impinge on the existing notch during intraoperative range of motion. These areas can be further contoured with a high-speed burr to prevent impingement (which may result in limited motion or dislocation). Hip motion (flexion to at least 90 degrees, extension to 30 degrees, abduction to 45 degrees, adduction to neutral, and rotation) should be possible without evidence of impingement or dislocation. Abductor Mechanism Reconstruction (Figure 28.8) The osteotomized greater trochanter and abductors are reattached to their original location using cables. If the greater trochanter was included in the resected
 Photograph following a periacetabular resection showing the remaining ilium (IL), sciatic nerve (S), the greater trochanteric osteotomy (G), and the femoral head.")
 in the ilium.")

9 Malawer Chapter 28 22/02/ :55 Page 431 Periacetabular Resections 431 A B Figure 28.6 (A) Photograph following a periacetabular resection showing the remaining ilium (IL), sciatic nerve (S), the greater trochanteric osteotomy (G), and the femoral head. This defect is reconstructed with a saddle prosthesis. This necessitates removal of the femoral head with the insertion of the femoral component, a base element, and a saddle that articulate with the notch (made by the surgeon) in the ilium. (B) Intraoperative photograph demonstrating the creation of the deep notch (large arrows). The notch gives immediate stability to the prosthesis and permits an articulation between the saddle and the ilium. The saddle is not cemented or otherwise fixed into this notch. The tension of the muscles and the body of the prosthesis creates the tension that is required. The abductors, psoas, and iliacus muscles must be placed under appropriate tension to maintain stability of the prosthesis (AB shows abductor muscles; IC shows the iliacus muscle; S shows the sciatic nerve). (C) Reduction of the saddle prosthesis into the iliac notch (IL). The notch (solid arrows) must be as deep as the saddle and permit approximately 45 of flexion and extension, as well as abduction and adduction. The gluteal muscles have already been opposed to the greater trochanter with a cable grip system. Closure then consists of reattaching the abductors and closing the ilioinguinal incision. C (or prosthesis). The gluteus maximus muscle is then reattached to its insertion using nonabsorbable suture. Wound Closure The wound is copiously irrigated with saline. A large chest tube drain is inserted beneath the fascial closure. The subcutaneous tissue is closed over suction drains using absorbable suture. The skin is closed with suture or staples. specimen the abductor mechanism is reattached to the prosthesis using 3 mm Dacron tapes. Soft-tissue tension and prosthetic stability are again tested once the abductor mechanism reconstruction is complete. The piriformis and short external rotator muscles are brought forward and reattached to the proximal femur Functional and Rehabilitation Considerations Function In general, patients who undergo resection and reconstruction for a periacetabular tumor are able to ambulate (with or without a cane) following rehabilitation. It may take up to 1 year to regain motor strength, especially if the hip abductors were reconstructed or a more extensive resection was required (Type II/III). Rehabilitation The rehabilitation process is dependent on the extent of tumor resection (bone and soft tissue), the required

10 Malawer Chapter 28 22/02/ :55 Page Musculoskeletal Cancer Surgery A Figure 28.7 (see also following pages) (A) Surgical exposure. Utilitarian pelvic incision. The ilioinguinal incision permits exposure of the retroperitoneal space and mobilization of the iliac vessels, femoral nerve, and sciatic nerve. This permits exposure of the medial wall of the acetabulum as well as the ilium and the superior pubic ramus. (B) A large posterior fasciocutaneous flap based medially permits the release of the gluteus maximus. The gluteus maximus muscle is detached from the iliotibial band and the femur, and it is rotated posteriorly. This provides exposure of the ilium, sciatic notch, sciatic nerve, and hip joint. Through this posterior incision the proximal iliac osteotomy is performed, as well as ischial osteotomy. The periacetabular tumor is removed through this incision following the release of the sacrotuberous ligament. (C) Schematic diagram of the mobilization of the periacetabular structures and the three osteotomies which are necessary for a complete resection of the acetabulum. The superacetabular osteotomy is performed through the sciatic notch, the superior pubic ramus is transected at the level of the retracted femoral vessels, and the infra-acetabular osteotomy is performed above the level of the ischium. Once all three osteotomies are completed the acetabulum can be removed through the posterior incision by detaching the sacrospinous ligament. (D) Schematic of the close-up of the superior pubic ramus osteotomy. The femoral triangle and nerve are identified and retracted. The superior pubic ramus is identified and the pectineus muscle is transected. This permits exposure of the superior pubic ramus which is then protected by a Cobra retractor and is osteotomized with a high-speed drill. (E) (page 431) Schematic diagram of the infra-acetabular osteotomy. The osteotomy is performed through the posterior incision above the level of the origin of the biceps femoris. A Cobra retractor is inserted along the inferior border of the ischium and is placed into the obturator foramen in order to protect the adjacent soft tissues. Once these osteotomies are performed, the sacrospinous ligament can be palpated and released off of the spine. (F) (page 431) A notch is made in the supra-acetabular roof or remaining ilium for the saddle prosthesis to sit in. A high-speed burr is used. (G) (page 431) Schematic diagram of the saddle prosthesis reduced into the notch. The femoral stem is cemented into the femur. The size of the base element is chosen to make a tight fit on reduction. The greater trochanter is fixed with cables. The abductor and psoas muscle tension keeps the prosthesis reduced. (H) (page 431) Schematic diagram of the saddle prosthesis following a periacetabular resection (Type II) for a sarcoma and radical curettage for a large acetabular metastasis.



11 Malawer Chapter 28 22/02/ :55 Page 433 Periacetabular Resections 433 B C D Figure 28.7 B D



12 Malawer Chapter 28 22/02/ :55 Page Musculoskeletal Cancer Surgery E F G H Figure 28.7 E H
 AP radiograph of the pelvis with a saddle prosthesis in place. Note the reactive bone around the saddle component. This is commonly seen 6 months following surgery.")
.")
 (arrow). (C) CT scan showing a typical saddle prosthesis in good position.")
13 Malawer Chapter 28 22/02/ :55 Page 435 Periacetabular Resections 435 A B Figure 28.8 Postoperative radiographs and CT scans demonstrating common postoperative radiographic findings. (A) AP radiograph of the pelvis with a saddle prosthesis in place. Note the reactive bone around the saddle component. This is commonly seen 6 months following surgery. It often increases the stability of the prosthesis by creating a painless pseudoarthrosis. Despite the AP radiograph appearance, one cannot be certain that the saddle is actually reduced within the notch (one prong anterior and one prong posterior to the wing of the ilium). Therefore, (B) a 45 oblique radiograph of the affected side of the pelvis is required. This photograph demonstrates that the saddle is in excellent position to the remaining wing of the ilium (IL) (arrow). (C) CT scan showing a typical saddle prosthesis in good position. Despite the artifact from the metal, one can visualize the anterior and posterior prongs of the saddle on opposite sides of the ilium. This scan correlates with the plain radiograph. If there is any question of reduction of the saddle, both an oblique radiograph and a CT scan are required. Note, it is not uncommon to see a large mass around the saddle prosthesis body several months after surgery. This is routinely seen and represents a large pseudocapsule filled with reactive fluid (similar to that seen around symptomatic non-unions). C reconstruction, and the overall condition of the patient. Initially, patients who have undergone a periacetabular tumor resection and reconstruction are kept in bed with the operative extremity placed in balanced suspension. This provides more reliable elevation of the extremity and minimizes mobility while the incision begins to heal. This is continued for 3 4 days or until the wound is checked and all of the drains removed. All wound drainage tubes are left in place until the drainage is less than ml per 24 h period. Once the incision is healing, and the drains have been removed, the
14 Malawer Chapter 28 22/02/ :55 Page 436 patient is placed in a hip abduction orthosis with a pelvic band (if the hip abductors were reconstructed) and gait training is initiated. Patients who have undergone a saddle prosthetic reconstruction begin ambulation with a walker or crutches, weight-bearing as tolerated. Although weightbearing is progressed as tolerated, patients who have undergone a hip abductor repair are encouraged to protect the soft-tissue reconstruction (and remain in the brace) for approximately 6 weeks. Initially, motion is encouraged within the limits of the brace (60 degrees of flexion, no extension, abduction, or adduction). Patients are encouraged to perform straight-leg raises and knee and ankle motion exercises. Once the brace is removed, range of motion is progressed and hip flexor and abductor strengthening is begun. Patients are instructed on total hip precautions and discouraged from flexing the hip greater than 90 degrees or crossing their legs.
Overview on Pelvic Resections: Surgical Considerations and Classifications
 13282_ON-17.qxd 3/22/09 10:45 AM Page 1 Chapter 17 Overview on Pelvic Resections: Surgical Considerations and Classifications Ernest U. Conrad III, Jason Weisstein, Jennifer Lisle, Amir Sternheim, and
13282_ON-17.qxd 3/22/09 10:45 AM Page 1 Chapter 17 Overview on Pelvic Resections: Surgical Considerations and Classifications Ernest U. Conrad III, Jason Weisstein, Jennifer Lisle, Amir Sternheim, and
A Two-incision Approach for En Bloc Resection of Periacetabular Tumors with Illustrations from acadaver
 60 2014 Chinese Orthopaedic Association and Wiley Publishing Asia Pty Ltd SURGICAL TECHNIQUE A Two-incision Approach for En Bloc Resection of Periacetabular Tumors with Illustrations from acadaver Chang-an
60 2014 Chinese Orthopaedic Association and Wiley Publishing Asia Pty Ltd SURGICAL TECHNIQUE A Two-incision Approach for En Bloc Resection of Periacetabular Tumors with Illustrations from acadaver Chang-an
The Hip (Iliofemoral) Joint. Presented by: Rob, Rachel, Alina and Lisa
 Joint. Presented by: Rob, Rachel, Alina and Lisa") The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
The Lower Limb. Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa
 The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
Lectures of Human Anatomy
 Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Main Menu. Joint and Pelvic Girdle click here. The Power is in Your Hands
 1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
First practical session. Bones of the gluteal region
 First practical session 2017 Bones of the gluteal region The Hip bone The hip bone is made of: 1 The ilium: superior in position 2 The ischium:postero-inferior in position 3 The pubis: antero-inferior
First practical session 2017 Bones of the gluteal region The Hip bone The hip bone is made of: 1 The ilium: superior in position 2 The ischium:postero-inferior in position 3 The pubis: antero-inferior
The thigh. Prof. Oluwadiya KS
 The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
LAB Notes#1. Ahmad Ar'ar. Eslam
 LAB Notes#1 Ahmad Ar'ar Eslam 1 P a g e Anatomy lab Notes Lower limb bones :- Pelvic girdle: It's the connection between the axial skeleton and the lower limb; it's made up of one bone called the HIP BONE
LAB Notes#1 Ahmad Ar'ar Eslam 1 P a g e Anatomy lab Notes Lower limb bones :- Pelvic girdle: It's the connection between the axial skeleton and the lower limb; it's made up of one bone called the HIP BONE
Surgical Anatomy of the Hip. Joseph H. Dimon
 Surgical Anatomy of the Hip Joseph H. Dimon The hip joint is a deep joint surrounded by large and powerful muscles necessary for its proper function. Essential neurovascular structures lie in front and
Surgical Anatomy of the Hip Joseph H. Dimon The hip joint is a deep joint surrounded by large and powerful muscles necessary for its proper function. Essential neurovascular structures lie in front and
Zimmer MIS Mini-Incision THA Anterolateral Approach
 Zimmer MIS Mini-Incision THA Anterolateral Approach Retractor Placement Guide Optimizing exposure and preserving soft tissue during MIS THA Minimally invasive surgery allows you to follow the basic principles
Zimmer MIS Mini-Incision THA Anterolateral Approach Retractor Placement Guide Optimizing exposure and preserving soft tissue during MIS THA Minimally invasive surgery allows you to follow the basic principles
The University Of Jordan Faculty Of Medicine THE LOWER LIMB. Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan
 The University Of Jordan Faculty Of Medicine THE LOWER LIMB Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Gluteal Region Cutaneous nerve supply of (Gluteal region) 1. Lateral cutaneous
The University Of Jordan Faculty Of Medicine THE LOWER LIMB Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Gluteal Region Cutaneous nerve supply of (Gluteal region) 1. Lateral cutaneous
Identify the muscles associated with the medial compartment of the thigh. Identify the attachment points of the medial thigh muscles.
 L 8 A B O R A T O R Y Thigh MEDIAL THIGH Identify the muscles associated with the medial compartment of the thigh. Identify the attachment points of the medial thigh muscles. Identify the actions of these
L 8 A B O R A T O R Y Thigh MEDIAL THIGH Identify the muscles associated with the medial compartment of the thigh. Identify the attachment points of the medial thigh muscles. Identify the actions of these
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Gluteal region DR. GITANJALI KHORWAL
 Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Joints of the lower limb
 Joints of the lower limb 1-Type: Hip joint Synovial ball-and-socket joint 2-Articular surfaces: a- head of femur b- lunate surface of acetabulum Which is deepened by the fibrocartilaginous labrum acetabulare
Joints of the lower limb 1-Type: Hip joint Synovial ball-and-socket joint 2-Articular surfaces: a- head of femur b- lunate surface of acetabulum Which is deepened by the fibrocartilaginous labrum acetabulare
rotation of the hip Flexion of the knee Iliac fossa of iliac Lesser trochanter Femoral nerve Flexion of the thigh at the hip shaft of tibia
 Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
ANATOMY TEAM GLUTEAL REGION & BACK OF THIGH
 ANATOMY TEAM GLUTEAL REGION & BACK OF THIGH OBJECTIVES By the end of this lecture, the student should be able to identify and discuss: Contents of gluteal region: Groups of Glutei muscles and small muscles
ANATOMY TEAM GLUTEAL REGION & BACK OF THIGH OBJECTIVES By the end of this lecture, the student should be able to identify and discuss: Contents of gluteal region: Groups of Glutei muscles and small muscles
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Baraa Ayed حسام أبو عوض. Ahmad Salman. 1 P a g e
 4 Baraa Ayed حسام أبو عوض Ahmad Salman 1 P a g e Today we are going to cover these concepts: Iliotibial tract Anterior compartment of the thigh and the hip Medial compartment of the thigh Femoral triangle
4 Baraa Ayed حسام أبو عوض Ahmad Salman 1 P a g e Today we are going to cover these concepts: Iliotibial tract Anterior compartment of the thigh and the hip Medial compartment of the thigh Femoral triangle
Figure 1 - Hip and Pelvis
 Hip Figure 1 - Hip and Pelvis The terms hip and pelvis are frequently used interchangeably, but strictly speaking, the pelvis is a girdle of bones and the hip is a joint. The pelvis consists of The sacrum
Hip Figure 1 - Hip and Pelvis The terms hip and pelvis are frequently used interchangeably, but strictly speaking, the pelvis is a girdle of bones and the hip is a joint. The pelvis consists of The sacrum
Lower limb summary. Anterior compartment of the thigh. Done By: Laith Qashou. Doctor_2016
 Lower limb summary Done By: Laith Qashou Doctor_2016 Anterior compartment of the thigh Sartorius Anterior superior iliac spine Upper medial surface of shaft of tibia 1. Flexes, abducts, laterally rotates
Lower limb summary Done By: Laith Qashou Doctor_2016 Anterior compartment of the thigh Sartorius Anterior superior iliac spine Upper medial surface of shaft of tibia 1. Flexes, abducts, laterally rotates
Bony Anatomy. Femur. Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity
 Hip Anatomy Bony Anatomy Femur Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity Bony Anatomy Pelvic Girdle Acetabulum 3 bones
Hip Anatomy Bony Anatomy Femur Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity Bony Anatomy Pelvic Girdle Acetabulum 3 bones
Lesson 24. A & P Hip
 Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
*smith&nephew CONTOUR
 Surgical Technique *smith&nephew CONTOUR Acetabular Rings CONTOUR Acetabular Rings Surgical technique completed in conjunction with Joseph Schatzker MD, BSc (Med.), FRCS (C) Allan E. Gross, MD, FRCS (C)
Surgical Technique *smith&nephew CONTOUR Acetabular Rings CONTOUR Acetabular Rings Surgical technique completed in conjunction with Joseph Schatzker MD, BSc (Med.), FRCS (C) Allan E. Gross, MD, FRCS (C)
ANTERIOR TOTAL HIP ARTHOPLASTY
 ANTERIOR TOTAL HIP ARTHOPLASTY And Other Approaches Bill Rhodes PTA 236 Total Hip Arthoplasty (THA) Background THA, also know as Total Hip Replacement Regarded as the most valued development in orthopedics
ANTERIOR TOTAL HIP ARTHOPLASTY And Other Approaches Bill Rhodes PTA 236 Total Hip Arthoplasty (THA) Background THA, also know as Total Hip Replacement Regarded as the most valued development in orthopedics
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil Khouri MD, MSc, Ph.D
 Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Hip joint and pelvic girdle. Lower Extremity. Pelvic Girdle 6/5/2017
 Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
The Hip Joint. Shenequia Howard David Rivera
 The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
Preoperative Planning. The primary objectives of preoperative planning are to:
 Preoperative Planning The primary objectives of preoperative planning are to: - Determine preoperative leg length discrepancy. - Assess acetabular component size and placement. - Determine femoral component
Preoperative Planning The primary objectives of preoperative planning are to: - Determine preoperative leg length discrepancy. - Assess acetabular component size and placement. - Determine femoral component
To classify the joints relative to structure & shape
 To classify the joints relative to structure & shape To describe the anatomy of the hip joint To describe the ankle joint To memorize their blood & nerve supply JOINTS: Joints are sites where skeletal
To classify the joints relative to structure & shape To describe the anatomy of the hip joint To describe the ankle joint To memorize their blood & nerve supply JOINTS: Joints are sites where skeletal
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT. Dr Farooq Khan Aurakzai. Dated:
 Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
VerSys LD/Fx Cemented and Press-Fit Hip Prostheses. Surgical Technique IMAGE TO COME. Versatile solutions for total and partial hip replacement
 VerSys LD/Fx Cemented and Press-Fit Hip Prostheses Surgical Technique IMAGE TO COME Versatile solutions for total and partial hip replacement VerSys LD/Fx Cemented and Press-Fit Hip Prostheses VerSys
VerSys LD/Fx Cemented and Press-Fit Hip Prostheses Surgical Technique IMAGE TO COME Versatile solutions for total and partial hip replacement VerSys LD/Fx Cemented and Press-Fit Hip Prostheses VerSys
The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking
 1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
SURGICAL AND APPLIED ANATOMY
 Página 1 de 6 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "37 - HIP DISLOCATIONS
Página 1 de 6 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "37 - HIP DISLOCATIONS
Bones of Lower Limb. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Bones of Lower Limb Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Bones of the lower limb Hip Bone Made up of 3 bones: 1) Ilium (flat), superior in position 2) Ischium (L), postero-inferior
Bones of Lower Limb Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Bones of the lower limb Hip Bone Made up of 3 bones: 1) Ilium (flat), superior in position 2) Ischium (L), postero-inferior
SURGICAL EXPOSURES SURGERY OF THE HIP
 1 of 24 11/19/03 1:11 PM SURGICAL EXPOSURES SURGERY OF THE HIP by R. CALANDRUCCIO In: Atlas of Orthopaedic Surgery Volume 3 Lower Extremity; Editors: Laurin, CA, Riley Jr. LH, Roy-Camille R Reprinted with
1 of 24 11/19/03 1:11 PM SURGICAL EXPOSURES SURGERY OF THE HIP by R. CALANDRUCCIO In: Atlas of Orthopaedic Surgery Volume 3 Lower Extremity; Editors: Laurin, CA, Riley Jr. LH, Roy-Camille R Reprinted with
Skeletal System Module 13: The Pelvic Girdle and Pelvis
 OpenStax-CNX module: m47993 1 Skeletal System Module 13: The Pelvic Girdle and Pelvis Donna Browne Based on The Pelvic Girdle and Pelvis by OpenStax College This work is produced by OpenStax-CNX and licensed
OpenStax-CNX module: m47993 1 Skeletal System Module 13: The Pelvic Girdle and Pelvis Donna Browne Based on The Pelvic Girdle and Pelvis by OpenStax College This work is produced by OpenStax-CNX and licensed
EXTENDED TROCHANTERIC OSTEOTOMY SURGICAL TECHNIQUE FPO EXTENSIVELY COATED FIXATION
 EXTENDED TROCHANTERIC OSTEOTOMY SURGICAL TECHNIQUE FPO EXTENSIVELY COATED FIXATION SINCE 1983 PREOPERATIVE PLANNING EXPLANTATION OPTIONS the cement from inside the cement canal until the bone/ cement bond
EXTENDED TROCHANTERIC OSTEOTOMY SURGICAL TECHNIQUE FPO EXTENSIVELY COATED FIXATION SINCE 1983 PREOPERATIVE PLANNING EXPLANTATION OPTIONS the cement from inside the cement canal until the bone/ cement bond
Mohammad Ashraf. Abdulrahman Al-Hanbali. Ahmad Salman. 1 P a g e
 - 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
- 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
Overview of Surgical Resection of Space Sarcomas
 13282_ON-33.qxd 3/31/09 4:50 PM Page 1 Chapter 33 Overview of Surgical Resection of Space Sarcomas Amir Sternheim, Tamir Pritsch, and Martin M. Malawer BACKGROUND The three main extracompartmental spaces
13282_ON-33.qxd 3/31/09 4:50 PM Page 1 Chapter 33 Overview of Surgical Resection of Space Sarcomas Amir Sternheim, Tamir Pritsch, and Martin M. Malawer BACKGROUND The three main extracompartmental spaces
North of England Bone and Soft Tissue Tumour Service
 North of England Bone and Soft Tissue Tumour Service Guidelines for rehabilitation after replacement of the proximal femur Proximal femoral replacement surgery is usually carried out as part of treatment
North of England Bone and Soft Tissue Tumour Service Guidelines for rehabilitation after replacement of the proximal femur Proximal femoral replacement surgery is usually carried out as part of treatment
C. Bones of the Pelvic Girdle
 C. Bones of the Pelvic Girdle 1. 2 coxal bones (a.k.a hip bones): -bony pelvis is made up of hip bones, sacrum, & coccyx -pelvic bones are large & heavy & attach to the axial skeleton via sacrum/coccyx
C. Bones of the Pelvic Girdle 1. 2 coxal bones (a.k.a hip bones): -bony pelvis is made up of hip bones, sacrum, & coccyx -pelvic bones are large & heavy & attach to the axial skeleton via sacrum/coccyx
Muscles of Gluteal Region
 1 The Gluteal Region In the gluteal region the skin is tough with many layers underneath. Directly under it is the superficial fascia followed by the deep fascia then the muscles and the bones of the thigh.
1 The Gluteal Region In the gluteal region the skin is tough with many layers underneath. Directly under it is the superficial fascia followed by the deep fascia then the muscles and the bones of the thigh.
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Acland's DVD Atlas of Human Anatomy. Transcript for Volume Robert D Acland
 Acland's DVD Atlas of Human Anatomy Transcript for Volume 2 2007 Robert D Acland This free downloadable pdf file is to be used for individual study only. It is not to be reproduced in any form without
Acland's DVD Atlas of Human Anatomy Transcript for Volume 2 2007 Robert D Acland This free downloadable pdf file is to be used for individual study only. It is not to be reproduced in any form without
Following a tradition of success. VerSys Heritage Primary Hip Prosthesis Surgical Technique
 Following a tradition of success VerSys Heritage Primary Hip Prosthesis Surgical Technique VerSys Heritage Primary Hip Prosthesis 1 Surgical Technique For VerSys Heritage Primary Hip Prosthesis Dennis
Following a tradition of success VerSys Heritage Primary Hip Prosthesis Surgical Technique VerSys Heritage Primary Hip Prosthesis 1 Surgical Technique For VerSys Heritage Primary Hip Prosthesis Dennis
RECOVERY. P r o t r u s i o
 RECOVERY P r o t r u s i o TM C a g e RECOVERY P r o t r u s i o TM C a g e Design Features Revision acetabular surgery is a major challenge facing today s total joint revision surgeon. Failed endo/bi-polars,
RECOVERY P r o t r u s i o TM C a g e RECOVERY P r o t r u s i o TM C a g e Design Features Revision acetabular surgery is a major challenge facing today s total joint revision surgeon. Failed endo/bi-polars,
MIAA. Minimally Invasive Anterior Approach Surgical technique
 MIAA Minimally Invasive Anterior Approach Surgical technique Contents Introduction 3 With-Table MIAA technique 4 A1. Patient positioning/draping 4 A2. Skin incision 4 A3. Muscular dissection 4 A4. Muscle
MIAA Minimally Invasive Anterior Approach Surgical technique Contents Introduction 3 With-Table MIAA technique 4 A1. Patient positioning/draping 4 A2. Skin incision 4 A3. Muscular dissection 4 A4. Muscle
Anterior and Medial compartments of the thigh. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Rx90 Total Hip System Acetabular Series
 Rx90 Total Hip System Acetabular Series The Rx90 Total Hip System was developed by Stanley Asnis, M.D., in conjunction with David Dines, M.D. and Micheal Errico M.D., Co-Section-Chiefs of the North Shore
Rx90 Total Hip System Acetabular Series The Rx90 Total Hip System was developed by Stanley Asnis, M.D., in conjunction with David Dines, M.D. and Micheal Errico M.D., Co-Section-Chiefs of the North Shore
Lecture 10 Arteries and veins of the upper limb
 Lecture 10 Arteries and veins of the upper limb 1. Identify the Subclavian, axillary, brachial (deep and superficial), radial and ulnar arteries and superficial/deep palmar arches 2. Describe the major
Lecture 10 Arteries and veins of the upper limb 1. Identify the Subclavian, axillary, brachial (deep and superficial), radial and ulnar arteries and superficial/deep palmar arches 2. Describe the major
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
TaperFill. Surgical Technique
 TaperFill Surgical Technique Table of Contents Indications and Contraindications 3 TaperFill Hip Size Charts 4-5 DJO Surgical 9800 Metric Boulevard Austin, TX (800) 456-8696 www.djosurgical.com Preoperative
TaperFill Surgical Technique Table of Contents Indications and Contraindications 3 TaperFill Hip Size Charts 4-5 DJO Surgical 9800 Metric Boulevard Austin, TX (800) 456-8696 www.djosurgical.com Preoperative
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
28 Surgical Technique
 Surgical Technique 10 12 14 16 18 20 22 24 28 26 Technique described by James L. Guyton, MD Campbell Clinic Memphis, Tennessee James W. Harkess, MD Campbell Clinic Memphis, Tennessee David G. LaVelle,
Surgical Technique 10 12 14 16 18 20 22 24 28 26 Technique described by James L. Guyton, MD Campbell Clinic Memphis, Tennessee James W. Harkess, MD Campbell Clinic Memphis, Tennessee David G. LaVelle,
Triple Pelvic Osteotomy
 Triple Pelvic Osteotomy Peter Templeton and Peter V. Giannoudis 2 Indications Acetabular dysplasia with point loading, lateral migration, and painful limp. Hip joint should be reasonably congruent in abduction
Triple Pelvic Osteotomy Peter Templeton and Peter V. Giannoudis 2 Indications Acetabular dysplasia with point loading, lateral migration, and painful limp. Hip joint should be reasonably congruent in abduction
The os coxae or hip bone consists of three flat bones, ilium, ischium and pubis, which fuse together to form the acetabulum.
 The os coxae The os coxae or hip bone consists of three flat bones, ilium, ischium and pubis, which fuse together to form the acetabulum. The ilium extends from the acetabulum upwards forming the lateral
The os coxae The os coxae or hip bone consists of three flat bones, ilium, ischium and pubis, which fuse together to form the acetabulum. The ilium extends from the acetabulum upwards forming the lateral
Snapping Hip and Impingement
 Snapping Hip and Impingement Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Board: GE,
Snapping Hip and Impingement Jon A. Jacobson, M.D. Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures: Consultant: Bioclinica Advisory Board: GE,
RADIOLOGY OF THE NORMAL ACETABULUM. X-ray X-ray X-ray. Figure. Figure ILIAC OBLIQUE VIEW OBTURATOR OBLIQUE VIEW AP VIEW
 RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
VerSys Fiber Metal Taper Hip Prosthesis. Surgical Technique
 VerSys Fiber Metal Taper Hip Prosthesis Surgical Technique VerSys Fiber Metal Taper Hip Prosthesis Surgical Technique 1 VerSys Fiber Metal Taper Hip Prosthesis Surgical Technique Table of Contents Preoperative
VerSys Fiber Metal Taper Hip Prosthesis Surgical Technique VerSys Fiber Metal Taper Hip Prosthesis Surgical Technique 1 VerSys Fiber Metal Taper Hip Prosthesis Surgical Technique Table of Contents Preoperative
MUSCULOSKELETAL LOWER LIMB
 MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
Applied anatomy of the hip and buttock
 CHAPTER CONTENTS The hip joint e9 Capsule and ligaments e9 s e0 Flexor muscles................... e0 Extensor muscles.................. e Abductor muscles.................. e Adductor muscles..................
CHAPTER CONTENTS The hip joint e9 Capsule and ligaments e9 s e0 Flexor muscles................... e0 Extensor muscles.................. e Abductor muscles.................. e Adductor muscles..................
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil khouri
 Dr. Nabil khouri Appendicular Skeleton The appendicular skeleton is made up of the bones of the upper and lower limbs and their girdles Two girdles: Pectoral girdles attach the upper limbs to the body
Dr. Nabil khouri Appendicular Skeleton The appendicular skeleton is made up of the bones of the upper and lower limbs and their girdles Two girdles: Pectoral girdles attach the upper limbs to the body
Anatomage Table Instructors Guide- Lower Limb
 The Lower Limb Anatomage Table Instructors Guide- Lower Limb Table of Contents Lower Limb 1- The Skeletal System...3 1: Hip Bone...3 2: Hip Joint and Femur...4 3: Patella and Knee Joint...7 4: Tibia, Fibula,
The Lower Limb Anatomage Table Instructors Guide- Lower Limb Table of Contents Lower Limb 1- The Skeletal System...3 1: Hip Bone...3 2: Hip Joint and Femur...4 3: Patella and Knee Joint...7 4: Tibia, Fibula,
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
Versys Advocate V-Lign and Non V-Lign Cemented Hip Prosthesis
 Versys Advocate V-Lign and Non V-Lign Cemented Hip Prosthesis Surgical Technique Traditional Design. Innovative Features. Versys Advocate V-Lign and Non V-Lign Cemented Hip Prosthesis 1 Versys Advocate
Versys Advocate V-Lign and Non V-Lign Cemented Hip Prosthesis Surgical Technique Traditional Design. Innovative Features. Versys Advocate V-Lign and Non V-Lign Cemented Hip Prosthesis 1 Versys Advocate
Case Study: Christopher
 Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
7.5. Posterior Approach for MIS with Image-Free Computer-Assisted Navigation. L.D. Dorr, A.G. Yun. Introduction. The Process of Posterior MIS THR
 7.5 Posterior Approach for MIS with Image-Free Computer-Assisted Navigation L.D. Dorr, A.G. Yun Introduction This chapter will describe the technique of the posterior mini-incision of average 8 cm length.
7.5 Posterior Approach for MIS with Image-Free Computer-Assisted Navigation L.D. Dorr, A.G. Yun Introduction This chapter will describe the technique of the posterior mini-incision of average 8 cm length.
DISSECTION SCHEDULE. Session I - Hip (Front) & Thigh (Superficial)
 & Thigh (Superficial)") DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
DePuy LPS Limb Preservation System
 DePuy LPS Limb Preservation System surgical techniques Significant bone loss requiring extensive reconstruction around the hip and knee is often required following the treatment of malignant bone tumors,
DePuy LPS Limb Preservation System surgical techniques Significant bone loss requiring extensive reconstruction around the hip and knee is often required following the treatment of malignant bone tumors,
The Bernese Periacetabular Osteotomy: A Review of Surgical Technique
 10.5005/jp-journals-10017-1004 ORIGINAL RESEARCH DOJ The Bernese Periacetabular Osteotomy: A Review of Surgical Technique The Bernese Periacetabular Osteotomy: A Review of Surgical Technique Steven A Olson
10.5005/jp-journals-10017-1004 ORIGINAL RESEARCH DOJ The Bernese Periacetabular Osteotomy: A Review of Surgical Technique The Bernese Periacetabular Osteotomy: A Review of Surgical Technique Steven A Olson
Integral 180 Surgical Technique
 Integral 180 Surgical Technique The Integral 180 and 225 are part of the Alliance Family Total Hip System. The Integral 225 femoral component is marketed for use with bone cement in the United States.
Integral 180 Surgical Technique The Integral 180 and 225 are part of the Alliance Family Total Hip System. The Integral 225 femoral component is marketed for use with bone cement in the United States.
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
5 Testing the Muscles of the Lower Extremity
 C H A P T E R 5 Testing the Muscles of the Lower Extremity Hip Flexion Hip Flexion, Abduction, and External Rotation with Knee Flexion Hip Extension Hip Abduction Hip Abduction from Flexed Position Hip
C H A P T E R 5 Testing the Muscles of the Lower Extremity Hip Flexion Hip Flexion, Abduction, and External Rotation with Knee Flexion Hip Extension Hip Abduction Hip Abduction from Flexed Position Hip
SURGICAL TECHNIQUE. Protrusio Cage A COMPREHENSIVE ACETABULAR REVISION SYSTEM
 SURGICAL TECHNIQUE Protrusio Cage A COMPREHENSIVE ACETABULAR REVISION SYSTEM Important: This essential product information does not include all of the information necessary for selection and use of a device.
SURGICAL TECHNIQUE Protrusio Cage A COMPREHENSIVE ACETABULAR REVISION SYSTEM Important: This essential product information does not include all of the information necessary for selection and use of a device.
Optimum implant geometry
 Surgical Technique Optimum implant geometry Extending proven Tri-Lock heritage The original Tri-Lock was introduced in 1981. This implant was the first proximally coated tapered-wedge hip stem available
Surgical Technique Optimum implant geometry Extending proven Tri-Lock heritage The original Tri-Lock was introduced in 1981. This implant was the first proximally coated tapered-wedge hip stem available
Distal Femoral Resection
 Distal Femoral Resection Annie Arteau, Bruno Fuchs Introduction This text is a general description of a distal femoral resection. Focus is on anatomical structures and muscle resection. Each femoral resection
Distal Femoral Resection Annie Arteau, Bruno Fuchs Introduction This text is a general description of a distal femoral resection. Focus is on anatomical structures and muscle resection. Each femoral resection
Tradition Hip Primary Surgical Technique
 Design Rationale Many total hip designs in today s marketplace do not take advantage of the known forces present in the femur. Long term stability of a total hip prosthesis requires an implant design and
Design Rationale Many total hip designs in today s marketplace do not take advantage of the known forces present in the femur. Long term stability of a total hip prosthesis requires an implant design and
Cap. Tissue Preserving Total Hip Arthroplasty. SURGICAL TECHNIQUE - SuperCap Tissue Preserving Total Hip Arthroplasty
 Cap Tissue Preserving Total Hip Arthroplasty SURGICAL TECHNIQUE - SuperCap Tissue Preserving Total Hip Arthroplasty Table of Contents Chapter 1 Introduction Chapter 2 Surgical Technique 4 Patient Positioning
Cap Tissue Preserving Total Hip Arthroplasty SURGICAL TECHNIQUE - SuperCap Tissue Preserving Total Hip Arthroplasty Table of Contents Chapter 1 Introduction Chapter 2 Surgical Technique 4 Patient Positioning
The hip: Built for endurance and mobility
 The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
Table 2. First Generated List of Expert Responses. Likert-Type Scale. Category or Criterion. Rationale or Comments (1) (2) (3) (4)
 (2) (3) (4)") Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
lesser trochanter of femur lesser trochanter of femur iliotibial tract (connective tissue) medial surface of proximal tibia
 medial surface of proximal tibia") LOWER LIMB MUSCLES OF THE APPENDICULAR SKELETON The muscles that act on the lower limb fall into three groups: those that move the thigh, those that move the lower leg, and those that move the ankle, foot,
LOWER LIMB MUSCLES OF THE APPENDICULAR SKELETON The muscles that act on the lower limb fall into three groups: those that move the thigh, those that move the lower leg, and those that move the ankle, foot,
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
PLR. Proximal Loading Revision Hip System
 PLR Proximal Loading Revision Hip System The PLR splined revision stem is designed to recreate the natural stresses in the revised femur, where proximal bone may be compromised. PLR Hip System Design Considerations
PLR Proximal Loading Revision Hip System The PLR splined revision stem is designed to recreate the natural stresses in the revised femur, where proximal bone may be compromised. PLR Hip System Design Considerations
Triple Osteotomy of the Innominate Bone
 Triple Osteotomy of the Innominate Bone From the Shriners Hospital for Crippled Children, Philadelphia ABSTRACT:In forty-five patients, twenty-three with congenital dislocations and the rest with paralytic
Triple Osteotomy of the Innominate Bone From the Shriners Hospital for Crippled Children, Philadelphia ABSTRACT:In forty-five patients, twenty-three with congenital dislocations and the rest with paralytic
Posterior Flap Hemipelvectomy
 13282_ON-21.qxd 5/13/09 9:04 M Page 1 Chapter 21 Posterior Flap Hemipelvectomy Martin M. Malawer and James C. Wittig CKGROUND Despite increasingly effective chemotherapy and advances in limb-sparing surgery
13282_ON-21.qxd 5/13/09 9:04 M Page 1 Chapter 21 Posterior Flap Hemipelvectomy Martin M. Malawer and James C. Wittig CKGROUND Despite increasingly effective chemotherapy and advances in limb-sparing surgery
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Bones of the Lower Limb Bone Structure Description Notes. border of the superior ramus. inferolaterally from the pubic symphysis
 Bones of the Lower Limb Bone Structure Description Notes pubis an angulated bone the forms the anterior part of the pelvis one of three bones that form the os coxae: ilium, ischium, pubis; its forms 1/5
Bones of the Lower Limb Bone Structure Description Notes pubis an angulated bone the forms the anterior part of the pelvis one of three bones that form the os coxae: ilium, ischium, pubis; its forms 1/5
operative technique Kent Hip
 operative technique Kent Hip The Kent Hip Operative Technique The Kent Hip was developed by Mr Cliff Stossel, FRCS in Maidstone, Kent, UK and first implanted in 1986. It was designed to deal with problems
operative technique Kent Hip The Kent Hip Operative Technique The Kent Hip was developed by Mr Cliff Stossel, FRCS in Maidstone, Kent, UK and first implanted in 1986. It was designed to deal with problems
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Zimmer M/L Taper Hip Prosthesis. Surgical Technique
 Zimmer M/L Taper Hip Prosthesis Surgical Technique Zimmer M/L Taper Hip Prosthesis 1 Zimmer M/L Taper Hip Prosthesis Surgical Technique Table of Contents Preoperative Planning 2 Determination of Leg Length
Zimmer M/L Taper Hip Prosthesis Surgical Technique Zimmer M/L Taper Hip Prosthesis 1 Zimmer M/L Taper Hip Prosthesis Surgical Technique Table of Contents Preoperative Planning 2 Determination of Leg Length