אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים
|
|
|
- Louise Fleming
- 5 years ago
- Views:
Transcription




1 אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP היח' ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים 1


2 CP- Spectrum of pathology 2

3 Lower Limb problems in CP Spastic Quadriplegia- Hip,Pelvis, Spine Spastic Hemiplegia- Foot and Ankle 3
4 Spastic Diplegia Lower Limb Multilevel Involvement Foot/Ankle- Equinovalgus Knee- Flexion and stiffness Hip- Flexion and Internal Rotation 4
5 5

6 Pathology in CP Abnormal tone Agonist-Antagonist muscle imbalancecospasticity Longitudinal abnormalities- Stance/ Swing Rotational malalignement 6

7 Rotational abnormality Excessive Femoral anteversion External Tibial torsion Patellar instability Subluxation/Dislocation 7

8 Longitudinal abnormalities Knee Flexion Deformity Stance phase abnormalities Jump gait/crouch gait Patella alta Inferior pole fracture Patellofemoral arthritis 8

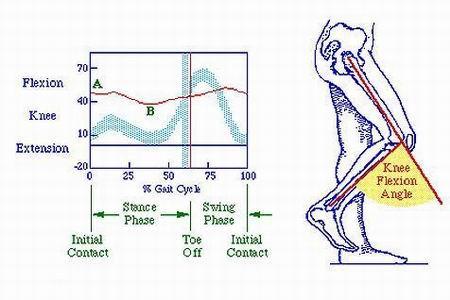
9 Longitudinal abnormalities (Rodda, Graham et al) 9

10 אתגרים... Dilemma 1 - Why?? 10

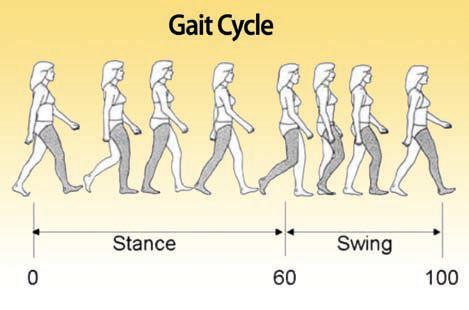
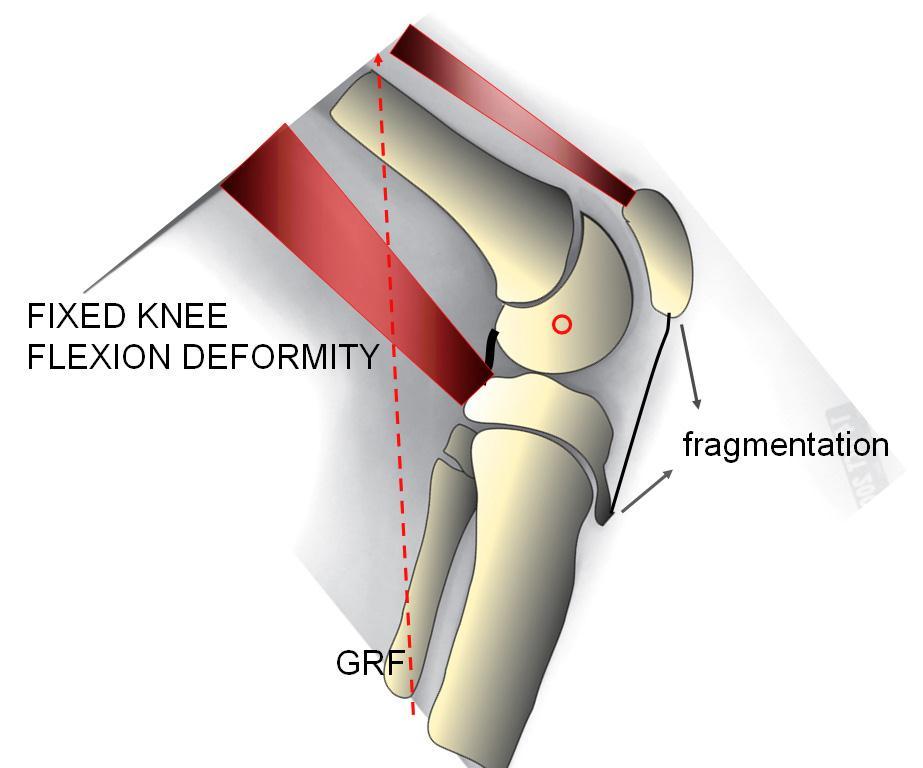
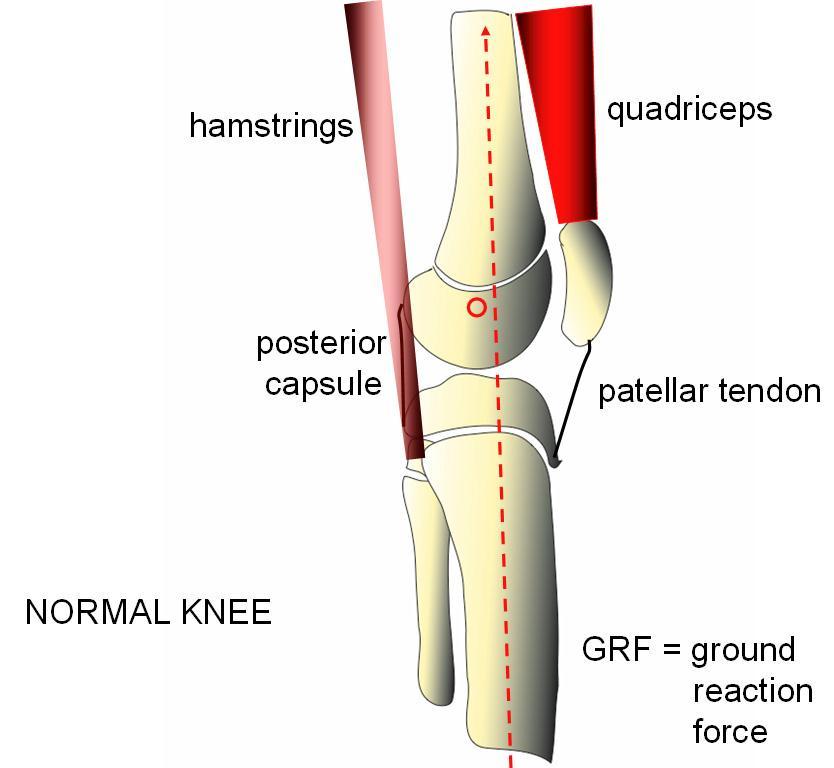
11 11 Ground Reaction force
12 12
13 Dilemma 2- Where?? Multilevel involvement! 13



14 Where?? Biarticular muscle contracture 1. Hamstrings 2. Rectus Femoris 3. Gastrocnemius דוגמה- הארכת המסטרינגס תשפר את ישור הברך אך תגרום ל- 14 Anterior pelvic tilt
2004 מונח שהוצג ע\"י CP Academy ( ההתערבות הניתוחית צריכה להתאים לחומרת")
15 Dilemma 3- How much?? לדוגמה- הארכת אכילס- יכולה לגרום ל- Crouch Selber, Graham et al. - Surgical Dose in CP )2004 מונח שהוצג ע"י CP Academy ( ההתערבות הניתוחית צריכה להתאים לחומרת הבעיה הקלינית 15

16 פתרונות... 16
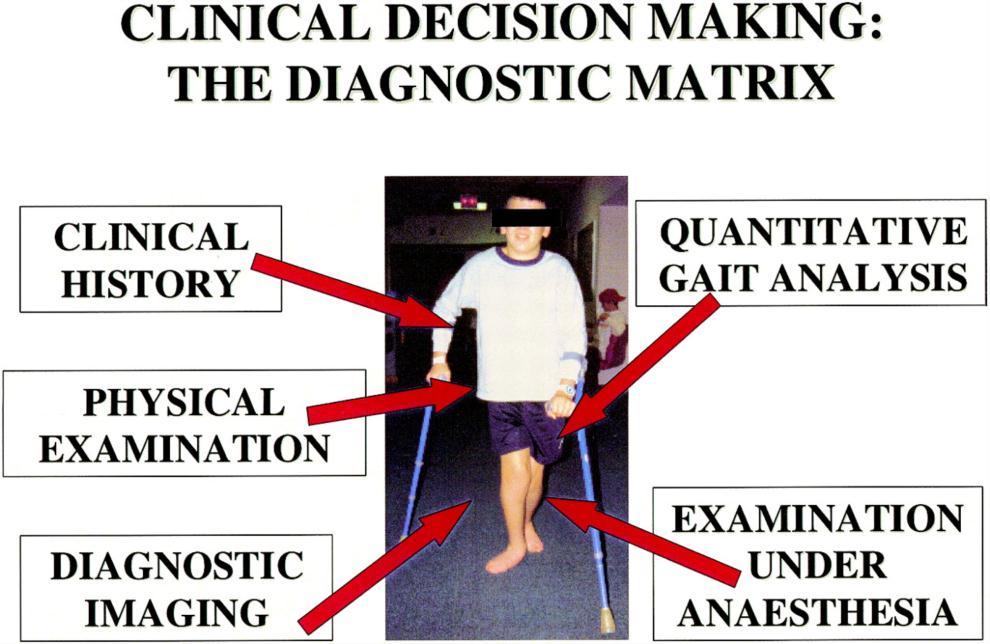


17 Evaluation (Davids et al.) 17 GMFCS/FAQ

18 Clinical history Complaints- Pain, fatigue, difficulty (not always consistent with other findings..) Level of ambulation GMFCS 18

19 Physical examination Knee flexion deformity predominates Popliteal angle (norm.-25) Differentiate from other deformities (hip, Pelvic Tilt) 19
 2. Reduce spasticity (Botulinum A, Dorsal Rhizotomy, Baclofen) 3.")
20 Treatment Gait dysfunction in CP is a combination of weakness and contracture! 1. Muscle strengthening (Isometric) 2. Reduce spasticity (Botulinum A, Dorsal Rhizotomy, Baclofen) 3. Release contracture (Surgery) 20




21 Treatment (Dilemma 4-When?) Spastic muscle contracture Botulinum /Baclofen Fixed muscle contracture Tendon lengthening/transfer Fixed muscle and joint contracture Bony procedures 21
22 Surgery Multilevel- Knee- Correct flexion contracture Hamstrings/ Femur Correct Patella Alta Hip- Release Flexion contracture Correct Anteversion Ankle- Correct equinus 22



23 Hamstring Lengthening Nonambulatory CP- GMFCS IV-V- Improve sitting- Prox. Hamstrings+ Adductor release Ambulatory spastic Diplegia- GMFCS I-II- Improve Walking- Controlled Distal Hamstrings Medial +- Lateral 23
 Indication- GMFCS-")

24 Semi-T Transfer (to Add tubercle) Indication- GMFCS- III-IV Severe knee flexion in stance Complication- Hyperextension 24


25 Risks of Hamstrings Lengthening 1. Knee hyperextension 2. Stiff knee in swing (Clearance problems) 3. Anterior pelvic tilt Solutions- Avoid Over lengthening Combine with Rectus release/transfer 25

26 Rectus Femoris Release/Transfer (to Semi-T) Rectus - Active in Swing phase Indication- Decreased knee flexion in swing Clearance problems, toe scuffing GMFCS I-II One stage with Hamstring release/2 nd stage 26
27 27
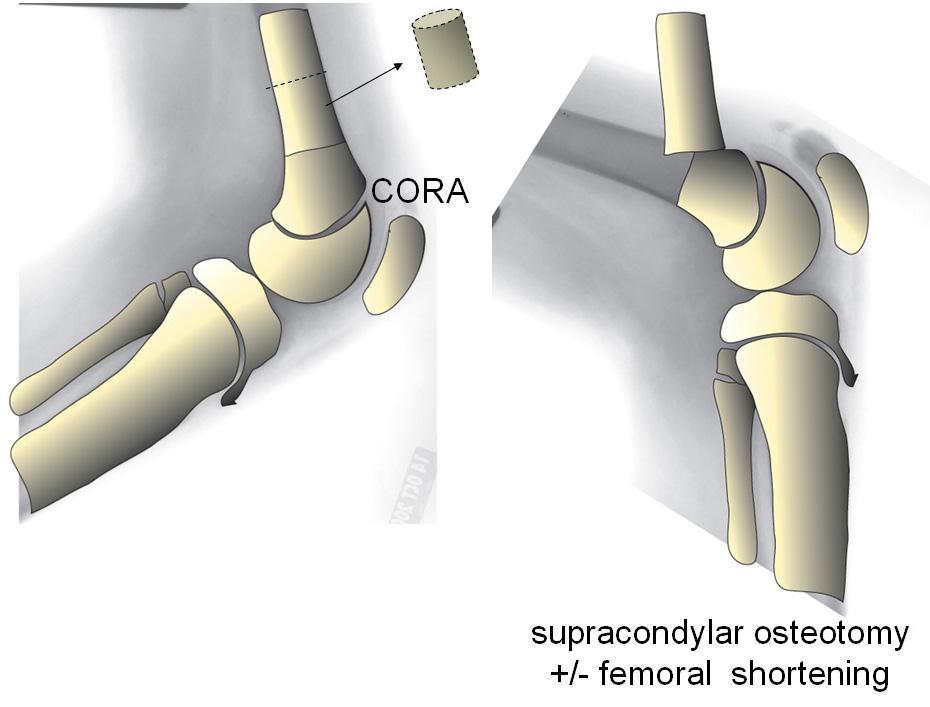

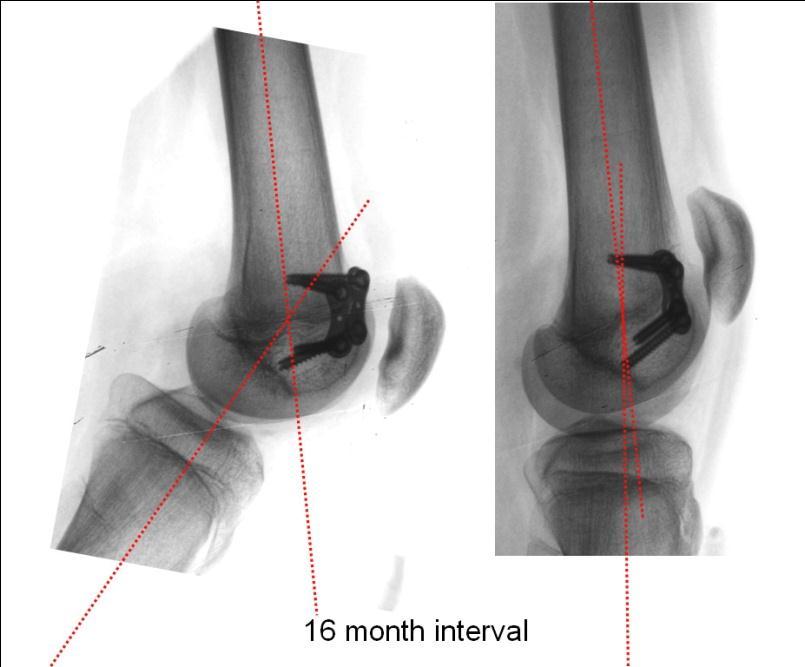
28 Bony procedures- Supracondylar Extension Osteotomy +femoral shortening 28

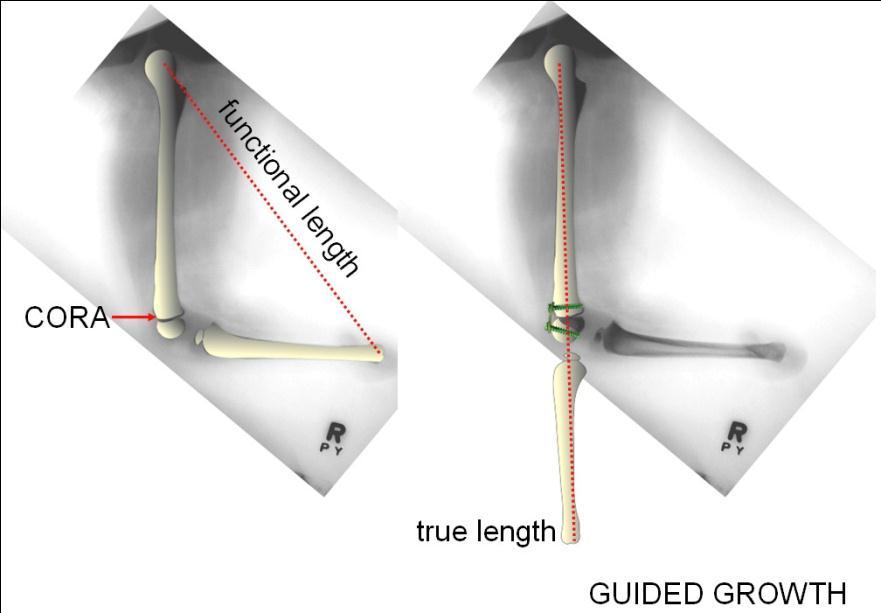
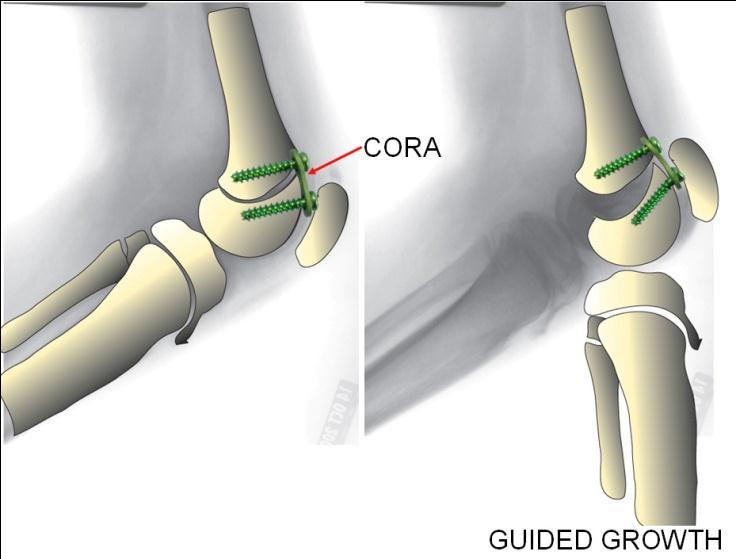

29 29 Guided Growth (When?..)
30 30


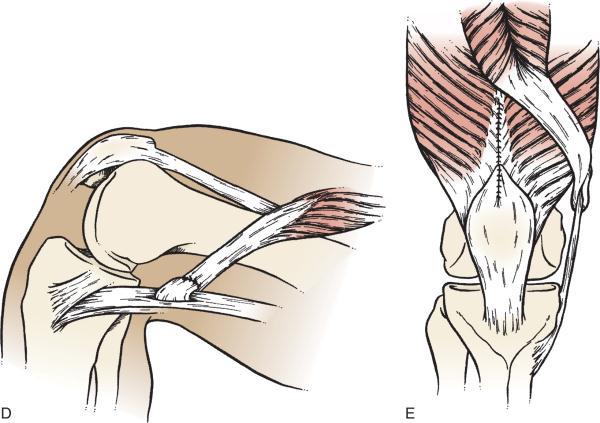
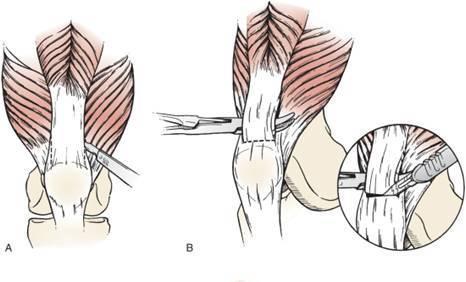
31 Patellar Tendon shortening Corrects patella alta Usually combined with correction of flexion deformity 31
32 Clinical Case 12y old, spastic diplegia 1) Clinical history- GMFCS 3 Fatigue, anterior knee pain 2) Physical exam.- Hamstrings contracture (pop. Angle -60) 3) Gait analysis- Stiff flexed knee gait pattern Crouch gait EUA- contracture without effect of spasticity Radiographs- Patella alta with fragmentation Treatment goals- 32 Relieve pain Improve walking efficiency
33 Crouch Gait Excessive knee flexion Calcaneus position of ankle during stance Excessive hip flexion Pelvis- Posterior/Neutral/Anterior Short hamstrings- only in patients with posterior pelvic tilt! Hamstrings lengthening increases anterior pelvic tilt 33

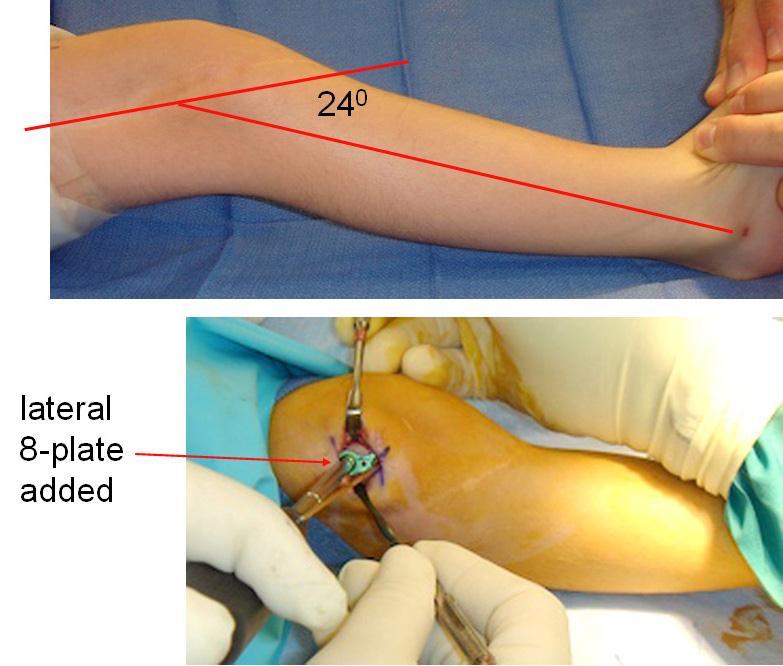
34 Plan 1) Muscle strengthening program 2) Surgery- Multilevel Hamstrings release Distal femur extension osteotomy /anterior 8-plates Patellar tendon shortening Consider Semi-T transfer Rectus release/transfer Proximal Iliopsoas release?? 3) Orthosis 34

35 אתגרים... פתרונות...? 35

36 תודה רבה... 36
Lower Extremity Orthopedic Surgery in Cerebral Palsy
 Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Management of knee flexion contractures in patients with Cerebral Palsy
 Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
10/26/2017. Comprehensive & Coordinated Orthopaedic Management of Children with CP. Objectives. It s all about function. Robert Bruce, MD Sayan De, MD
 Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB
 ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
AACPDM IC#21 DFEO+PTA 1
 Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES
 DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES TRAITMENTS NONCHIRURGICALES BOTOX PLATRES D INHIBITION APPROCHE CHIRURGICALE
DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES TRAITMENTS NONCHIRURGICALES BOTOX PLATRES D INHIBITION APPROCHE CHIRURGICALE
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy
 Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
Theuseofgaitanalysisin orthopaedic surgical treatment in children with cerebral palsy Aim of treatment Correction of functional disorder Requires analysis of function Basis for decision making Basis for
SWASH CERTIFICATION EXAM
 SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
Understanding and treating gait abnormality in Dravet syndrome
 Understanding and treating gait abnormality in Dravet syndrome Anne Stratton, MD, FAAP, FAAPMR Biennial Dravet Syndrome Foundation Family and Professional Conference July 19-22, 2018 Disclosures I have
Understanding and treating gait abnormality in Dravet syndrome Anne Stratton, MD, FAAP, FAAPMR Biennial Dravet Syndrome Foundation Family and Professional Conference July 19-22, 2018 Disclosures I have
Muscle Testing of Knee Extensors. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Case Study: Christopher
 Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Changes in lower limb rotation after soft tissue surgery in spastic diplegia
 Acta Orthopaedica 2010; 81 (2): 245 249 245 Changes in lower limb rotation after soft tissue surgery in spastic diplegia 3-dimensional gait analysis in 28 children Bjørn Lofterød 1 and Terje Terjesen 2
Acta Orthopaedica 2010; 81 (2): 245 249 245 Changes in lower limb rotation after soft tissue surgery in spastic diplegia 3-dimensional gait analysis in 28 children Bjørn Lofterød 1 and Terje Terjesen 2
Gait analysis and medical treatment strategy
 Gait analysis and medical treatment strategy Sylvain Brochard Olivier Rémy-néris, Mathieu Lempereur CHU and Pediatric Rehabilitation Centre Brest Course for European PRM trainees Mulhouse, October 22,
Gait analysis and medical treatment strategy Sylvain Brochard Olivier Rémy-néris, Mathieu Lempereur CHU and Pediatric Rehabilitation Centre Brest Course for European PRM trainees Mulhouse, October 22,
7/20/14. Patella Instability. Alignment. PF contact areas. Tissue Restraints. Pain. Acute Blunt force trauma Disorders of the Patellafemoral Joint
 Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
SURGICAL TREATMENT OF CEREBRAL PALSY
 SURGICAL TREATMENT OF CEREBRAL PALSY Chin Youb Chung, M.D. Department of Pediatric Orthopedic Surgery Seoul National University Children's Hospital Seoul National University Bundang Hospital SURGICAL TREATMENT
SURGICAL TREATMENT OF CEREBRAL PALSY Chin Youb Chung, M.D. Department of Pediatric Orthopedic Surgery Seoul National University Children's Hospital Seoul National University Bundang Hospital SURGICAL TREATMENT
USE OF GAIT ANALYSIS IN SURGICAL TREATMENT PLANNING FOR PATIENTS WITH CEREBRAL PALSY
 USE OF GAIT ANALYSIS IN SURGICAL TREATMENT PLANNING FOR PATIENTS WITH CEREBRAL PALSY Robert M. Kay, M.D. Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor, Department
USE OF GAIT ANALYSIS IN SURGICAL TREATMENT PLANNING FOR PATIENTS WITH CEREBRAL PALSY Robert M. Kay, M.D. Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor, Department
Why Would Your Child Need to See Me?
 Why Would Your Child Need to See Me? Deborah M Eastwood Great Ormond St Hospital for Children, London The Royal National Orthopaedic Hospital, UK Disclosures I am an orthopaedic surgeon and I do operate
Why Would Your Child Need to See Me? Deborah M Eastwood Great Ormond St Hospital for Children, London The Royal National Orthopaedic Hospital, UK Disclosures I am an orthopaedic surgeon and I do operate
Distal or supracondylar femoral osteotomy was first
 ORIGINAL ARTICLE Distal Femoral Osteotomy Using the LCP Pediatric Condylar 90-Degree Plate in Patients With Neuromuscular Disorders Erich Rutz, MD,*w Mark S. Gaston, MD, PhD,* Carlo Camathias, MD,* and
ORIGINAL ARTICLE Distal Femoral Osteotomy Using the LCP Pediatric Condylar 90-Degree Plate in Patients With Neuromuscular Disorders Erich Rutz, MD,*w Mark S. Gaston, MD, PhD,* Carlo Camathias, MD,* and
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? TRAMA Project. January th Clinical case presentation
 Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Cerebral Palsy Surgical Treatment 을지의대김하용
 Cerebral Palsy Surgical Treatment 2012.11.11 을지의대김하용 In the Past ( 시행착오의시기 ) RP surgery 에서 CP surgery 로젂환하면서 Trial and errors 를겪었다. 걷던아이가수술후못걷는다. Period of adductor tenotomy and TAL 이시기의특징 CP 는수술의결과가 RP
Cerebral Palsy Surgical Treatment 2012.11.11 을지의대김하용 In the Past ( 시행착오의시기 ) RP surgery 에서 CP surgery 로젂환하면서 Trial and errors 를겪었다. 걷던아이가수술후못걷는다. Period of adductor tenotomy and TAL 이시기의특징 CP 는수술의결과가 RP
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Selective Motor Control Assessment of the Lower Extremity in Patients with Spastic Cerebral Palsy
 Overview Selective Motor Control Assessment of the Lower Extremity in Patients with Spastic Cerebral Palsy Marcia Greenberg MS, PT* Loretta Staudt MS, PT* Eileen Fowler PT, PhD Selective Motor Control
Overview Selective Motor Control Assessment of the Lower Extremity in Patients with Spastic Cerebral Palsy Marcia Greenberg MS, PT* Loretta Staudt MS, PT* Eileen Fowler PT, PhD Selective Motor Control
MANUAL PRODUCT 3 RD EDITION. Pediatric Ankle Joint P: F: BeckerOrthopedic.com.
 PRODUCT MANUAL 3 RD EDITION P: 800-521-2192 248-588-7480 F: 800-923-2537 248-588-2960 BeckerOrthopedic.com Patent Pending 2018 Becker Orthopedic Appliance Co. All rights reserved. TRIPLE ACTION DIFFERENCE
PRODUCT MANUAL 3 RD EDITION P: 800-521-2192 248-588-7480 F: 800-923-2537 248-588-2960 BeckerOrthopedic.com Patent Pending 2018 Becker Orthopedic Appliance Co. All rights reserved. TRIPLE ACTION DIFFERENCE
MUSCLES OF THE LOWER LIMBS
 MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
THE HIP JOINT IN CEREBRAL PALSY
 HOSPITAL FOR JOINT DISEASES THE HIP JOINT IN CEREBRAL PALSY David S. Feldman, MD Professor of Orthopedic Surgery and Pediatrics Chief, Pediatric Orthopedic Surgery NYU/Hospital for Joint Diseases Define
HOSPITAL FOR JOINT DISEASES THE HIP JOINT IN CEREBRAL PALSY David S. Feldman, MD Professor of Orthopedic Surgery and Pediatrics Chief, Pediatric Orthopedic Surgery NYU/Hospital for Joint Diseases Define
Spasticity of muscles acting across joints in children
 ORIGINAL ARTICLE Static and Dynamic Gait Parameters Before and After Multilevel Soft Tissue Surgery in Ambulating Children With Cerebral Palsy Nicholas M. Bernthal, MD,* Seth C. Gamradt, MD,* Robert M.
ORIGINAL ARTICLE Static and Dynamic Gait Parameters Before and After Multilevel Soft Tissue Surgery in Ambulating Children With Cerebral Palsy Nicholas M. Bernthal, MD,* Seth C. Gamradt, MD,* Robert M.
DR. (PROF.) ANIL ARORA MS
 ANIL ARORA MS") Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
The influence of age at single-event multilevel surgery on outcome in children with cerebral palsy who walk with flexed knee gait
 DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY ORIGINAL ARTICLE The influence of age at single-event multilevel surgery on outcome in children with cerebral palsy who walk with flexed knee gait MARTIN ƒvehlýk
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY ORIGINAL ARTICLE The influence of age at single-event multilevel surgery on outcome in children with cerebral palsy who walk with flexed knee gait MARTIN ƒvehlýk
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Sagittal gait patterns in spastic diplegia
 Sagittal gait patterns in spastic diplegia J. M. Rodda, H. K. Graham, L. Carson, M. P. Galea, R. Wolfe From the Royal Children s Hospital, Parkville, Australia Classifications of gait patterns in spastic
Sagittal gait patterns in spastic diplegia J. M. Rodda, H. K. Graham, L. Carson, M. P. Galea, R. Wolfe From the Royal Children s Hospital, Parkville, Australia Classifications of gait patterns in spastic
Metadata of the chapter that will be visualized online
 Metadata of the chapter that will be visualized online Chapter Title Copyright Year 2013 Copyright Holder The Knee in Cerebral Palsy Springer-Verlag Berlin Heidelberg Corresponding Author Family Name Strobl
Metadata of the chapter that will be visualized online Chapter Title Copyright Year 2013 Copyright Holder The Knee in Cerebral Palsy Springer-Verlag Berlin Heidelberg Corresponding Author Family Name Strobl
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Methods Patients A retrospective review of gait studies was conducted for all participants presented to the Motion Analysis
 58 Original article Predictors of outcome of distal rectus femoris transfer surgery in ambulatory children with cerebral palsy Susan A. Rethlefsen a, Galen Kam d, Tishya A.L. Wren a,b,c and Robert M. Kay
58 Original article Predictors of outcome of distal rectus femoris transfer surgery in ambulatory children with cerebral palsy Susan A. Rethlefsen a, Galen Kam d, Tishya A.L. Wren a,b,c and Robert M. Kay
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Introduction. Research Using Motion Analysis: Movement Pathology. Objectives. Outline. Textbook gait description: Charcot-Marie-Tooth CMT
 roduction Research Using Motion Analysis: Impact in Understanding Movement Pathology Sylvia Õunpuu, MSc Kristan Pierz, MD Center for Motion Analysis Connecticut Children s Medical Center Motion analysis
roduction Research Using Motion Analysis: Impact in Understanding Movement Pathology Sylvia Õunpuu, MSc Kristan Pierz, MD Center for Motion Analysis Connecticut Children s Medical Center Motion analysis
APTA Intro to Identity. The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee THE HUMAN MOVEMENT SYSTEM
 The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
Muscles of the Thigh. 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group
 Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO
 Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Myology of the Knee. PTA 105 Kinesiology
 Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Pediatric Orthopaedic Fellowship Curriculum
 Pediatric Orthopaedic Fellowship Curriculum The Fellowship Pediatric Orthopaedic Curriculum is designed for the fellow to spend three months each in four content areas. There are five content areas comprising
Pediatric Orthopaedic Fellowship Curriculum The Fellowship Pediatric Orthopaedic Curriculum is designed for the fellow to spend three months each in four content areas. There are five content areas comprising
Toe walking gives rise to parental concern. Therefore, toe-walkers are often referred at the 3 years of age.
 IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
IDIOPATHIC TOE WALKING Toe walking is a common feature in immature gait and is considered normal up to 3 years of age. As walking ability improves, initial contact is made with the heel. Toe walking gives
The Limping Child. Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester
 The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
The Limping Child Todd Milbrandt, MD Division Chair Pediatric Orthopaedics Mayo Clinic Rochester Faculty Disclosure No disclosures relevant to this talk Practice Gap Primary Care Providers are faced with
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Ankle Valgus in Cerebral Palsy
 Ankle Valgus in Cerebral Palsy Freeman Miller Contents Introduction... 2 Natural History... 2 Treatment... 3 Diagnostic Evaluations... 3 Indications for Intervention... 3 Outcome of Treatment... 5 Complications
Ankle Valgus in Cerebral Palsy Freeman Miller Contents Introduction... 2 Natural History... 2 Treatment... 3 Diagnostic Evaluations... 3 Indications for Intervention... 3 Outcome of Treatment... 5 Complications
Hamstring and psoas length of crouch gait in cerebral palsy: a comparison with induced crouch gait in age- and sex-matched controls
 Rhie et al. Journal of NeuroEngineering and Rehabilitation 2013, 10:10 JOURNAL OF NEUROENGINEERING JNERAND REHABILITATION RESEARCH Open Access Hamstring and psoas length of crouch gait in cerebral palsy:
Rhie et al. Journal of NeuroEngineering and Rehabilitation 2013, 10:10 JOURNAL OF NEUROENGINEERING JNERAND REHABILITATION RESEARCH Open Access Hamstring and psoas length of crouch gait in cerebral palsy:
Why does it matter? Patellar Instability 7/23/2018. What is the current operation de jour? Common. Poorly taught. Poorly treated
 Patellar Instability It s Really Not That Difficult! David Shneider MD East Lansing, MI www.patellamdcom Detroit Sports Medicine Foundation July 2018 Why does it matter? Common Poorly taught Poorly treated
Patellar Instability It s Really Not That Difficult! David Shneider MD East Lansing, MI www.patellamdcom Detroit Sports Medicine Foundation July 2018 Why does it matter? Common Poorly taught Poorly treated
The Muscular System. Chapter 10 Part D. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part D The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.14: Muscles Crossing the Hip and
Chapter 10 Part D The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.14: Muscles Crossing the Hip and
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Anterior Knee Pain in Patients with Cerebral Palsy
 Original Article Clinics in Orthopedic Surgery 2014;6:426-431 http://dx.doi.org/10.4055/cios.2014.6.4.426 Anterior Knee Pain in Patients with Cerebral Palsy Young Choi, MD a, Sang Hyeong Lee, MD* a, Chin
Original Article Clinics in Orthopedic Surgery 2014;6:426-431 http://dx.doi.org/10.4055/cios.2014.6.4.426 Anterior Knee Pain in Patients with Cerebral Palsy Young Choi, MD a, Sang Hyeong Lee, MD* a, Chin
Knee Joint Assessment and General View
 Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
Anterior Knee Pain in Children. Joseph Chorley, MD Associate Professor, Pediatrics Baylor College of Medicine
 Anterior Knee Pain in Children Joseph Chorley, MD Associate Professor, Pediatrics Baylor College of Medicine Goals and Objectives To learn how to care for patients with chronic knee pain To be able to
Anterior Knee Pain in Children Joseph Chorley, MD Associate Professor, Pediatrics Baylor College of Medicine Goals and Objectives To learn how to care for patients with chronic knee pain To be able to
Muscles to know. Lab 21. Muscles of the Pelvis and Lower Limbs. Muscles that Position the Lower Limbs. Generally. Muscles that Move the Thigh
 Muscles to know Lab 21 Muscles of the Pelvis, Leg and Foot psoas major iliacus gluteus maximus gluteus medius sartorius quadriceps femoris (4) gracilus adductor longus biceps femoris semitendinosis semimembranosus
Muscles to know Lab 21 Muscles of the Pelvis, Leg and Foot psoas major iliacus gluteus maximus gluteus medius sartorius quadriceps femoris (4) gracilus adductor longus biceps femoris semitendinosis semimembranosus
Influence of surgery involving tendons around the knee joint on ankle motion during gait in patients with cerebral palsy
 Influence of surgery involving tendons around the knee joint on ankle motion during gait in patients with cerebral palsy Seung Yeol Lee, M.D., Ph.D. 1, Kyoung Min Lee, M.D., Ph.D. 2 Soon-Sun Kwon, Ph.D.
Influence of surgery involving tendons around the knee joint on ankle motion during gait in patients with cerebral palsy Seung Yeol Lee, M.D., Ph.D. 1, Kyoung Min Lee, M.D., Ph.D. 2 Soon-Sun Kwon, Ph.D.
2/24/2014. Outline. Anterior Orthotic Management for the Chronic Post Stroke Patient. Terminology. Terminology ROM. Physical Evaluation
 Outline Anterior Orthotic Management for the Chronic Post Stroke Patient Physical Evaluation Design Considerations Orthotic Design Jason M. Jennings CPO, LPO, FAAOP jajennings@hanger.com Primary patterning
Outline Anterior Orthotic Management for the Chronic Post Stroke Patient Physical Evaluation Design Considerations Orthotic Design Jason M. Jennings CPO, LPO, FAAOP jajennings@hanger.com Primary patterning
From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot. Objectives
 From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot Jan Hendryx, DO, FAAO Peek n Peak CME March 1, 2019 Objectives 1. Demonstrate knowledge of the anatomy of the lower extremity-
From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot Jan Hendryx, DO, FAAO Peek n Peak CME March 1, 2019 Objectives 1. Demonstrate knowledge of the anatomy of the lower extremity-
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes
 Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
CHAPTER 1: 1.1 Muscular skeletal system. Question - text book page 16. Question - text book page 20 QUESTIONS AND ANSWERS. Answers
 QUESTIONS AND ANSWERS CHAPTER 1: 1.1 Muscular skeletal system Question - text book page 16 Using the information on pages 12 to 14 above, complete the table below. joint joint type articulating bones associated
QUESTIONS AND ANSWERS CHAPTER 1: 1.1 Muscular skeletal system Question - text book page 16 Using the information on pages 12 to 14 above, complete the table below. joint joint type articulating bones associated
The Hip (Iliofemoral) Joint. Presented by: Rob, Rachel, Alina and Lisa
 Joint. Presented by: Rob, Rachel, Alina and Lisa") The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
Foot and Ankle Physical Exam. The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers
 Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Peggers Super Summaries: PFJ
 Patellofemoral Joint: ANATOMY: Largest sesamoid ossifying at 3-5 years of age Multiple foci having a sec ossification centre SUPEROLATERAL Helps increase moment arm PATELLOFEMORAL OA Incidence 10% of knee
Patellofemoral Joint: ANATOMY: Largest sesamoid ossifying at 3-5 years of age Multiple foci having a sec ossification centre SUPEROLATERAL Helps increase moment arm PATELLOFEMORAL OA Incidence 10% of knee
Changes in Sagittal Plane Kinematics and Kinetics after Distal Release of Medial Hamstrings in Cerebral Palsy
 J. Funct. Morphol. Kinesiol. 2016, 1, 6-15; doi:10.3390/jfmk1010006 Article Journal of Functional Morphology and Kinesiology ISSN 2411-5142 www.mdpi.com/journal/jfmk Changes in Sagittal Plane Kinematics
J. Funct. Morphol. Kinesiol. 2016, 1, 6-15; doi:10.3390/jfmk1010006 Article Journal of Functional Morphology and Kinesiology ISSN 2411-5142 www.mdpi.com/journal/jfmk Changes in Sagittal Plane Kinematics
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
The Effects of Botulinum Toxin Type-A on Spasticity and Motor Function in Children with Cerebral Palsy
 Pacific University CommonKnowledge PT Critically Appraised Topics School of Physical Therapy 2014 The Effects of Botulinum Toxin Type-A on Spasticity and Motor Function in Children with Cerebral Palsy
Pacific University CommonKnowledge PT Critically Appraised Topics School of Physical Therapy 2014 The Effects of Botulinum Toxin Type-A on Spasticity and Motor Function in Children with Cerebral Palsy
Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie
 Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie Development of hip luxation At birth these hips are normal developed,
Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie Development of hip luxation At birth these hips are normal developed,
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER
 THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh:
 5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
Main Menu. Joint and Pelvic Girdle click here. The Power is in Your Hands
 1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
Practical 1 Worksheet
 Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Topic 7: Hip and pelvis. Parts of the hip. Parts of the femur
 Topic 7: Hip and pelvis Parts of the hip Parts of the femur Classifying the hip joint Ball and socket Synovial Multiaxial Movements of the hip: Abduction/adduction Flexion/extension Medial/lateral rotation
Topic 7: Hip and pelvis Parts of the hip Parts of the femur Classifying the hip joint Ball and socket Synovial Multiaxial Movements of the hip: Abduction/adduction Flexion/extension Medial/lateral rotation
Appendix Section 1: Evaluation Section 2: Surgical planning Section 3: Children
 Appendix In order to ease the evaluation and decision-making processes and the surgical planning, the following provides commonly used scales, schematic drawings, and forms. Important, scales are not conceived
Appendix In order to ease the evaluation and decision-making processes and the surgical planning, the following provides commonly used scales, schematic drawings, and forms. Important, scales are not conceived
Arthritic history is similar to that of the hip. Add history of give way and locking, swelling
 KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
Hip joint and pelvic girdle. Lower Extremity. Pelvic Girdle 6/5/2017
 Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
Polio - A Model for Overuse and Aging. Acute Poliomyelitis. Acute Infection of Anterior Horn Motor Cells: Acute Polio Infection
 Polio - A Model for Overuse and Aging Mary Ann Keenan, M.D. Chief, Neuro-Orthopaedics Program Professor, Orthopaedic Surgery University of Pennsylvania Philadelphia, PA, USA Acute Poliomyelitis Acute viral
Polio - A Model for Overuse and Aging Mary Ann Keenan, M.D. Chief, Neuro-Orthopaedics Program Professor, Orthopaedic Surgery University of Pennsylvania Philadelphia, PA, USA Acute Poliomyelitis Acute viral
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
Investigation performed at The Royal Children s Hospital, Melbourne, Australia
 2653 COPYRIGHT 2006 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED Correction of Severe Crouch Gait in Patients with Spastic Diplegia with Use of Multilevel Orthopaedic Surgery BY J.M. RODDA, PHD,
2653 COPYRIGHT 2006 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED Correction of Severe Crouch Gait in Patients with Spastic Diplegia with Use of Multilevel Orthopaedic Surgery BY J.M. RODDA, PHD,
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity
 OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
Severe crouch gait in spastic diplegia can be prevented
 CHILDREN S ORTHOPAEDICS Severe crouch gait in spastic diplegia can be prevented A POPULATION-BASED STUDY C. Vuillermin, J. Rodda, E. Rutz, B. J. Shore, K. Smith, H. K. Graham From Royal Children s Hospital,
CHILDREN S ORTHOPAEDICS Severe crouch gait in spastic diplegia can be prevented A POPULATION-BASED STUDY C. Vuillermin, J. Rodda, E. Rutz, B. J. Shore, K. Smith, H. K. Graham From Royal Children s Hospital,
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil Khouri MD, MSc, Ph.D
 Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK. Musculoskeletal Anatomy & Kinesiology MUSCLES, MOVEMENTS & BIOMECHANICS
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology MUSCLES, MOVEMENTS & BIOMECHANICS MSAK101-I Session 7 Learning Objectives: 1. List the three types
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology MUSCLES, MOVEMENTS & BIOMECHANICS MSAK101-I Session 7 Learning Objectives: 1. List the three types
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Anterior knee pain.
 Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
The Knee. Clarification of Terms. Osteology of the Knee 7/28/2013. The knee consists of: The tibiofemoral joint Patellofemoral joint
 The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
Anatomy & Physiology. Muscles of the Lower Limbs.
 Anatomy & Physiology Muscles of the Lower Limbs http://www.ishapeup.com/musclecharts.html Muscles of the Lower Limbs Among the strongest muscles in the body. Because pelvic girdle is composed of heavy,
Anatomy & Physiology Muscles of the Lower Limbs http://www.ishapeup.com/musclecharts.html Muscles of the Lower Limbs Among the strongest muscles in the body. Because pelvic girdle is composed of heavy,
Cerebral palsy (CP) is the most common motor disability
 is the most common motor disability") CLINICAL Single- Event Multilevel Surgery to Correct Movement Disorders in Children With Cerebral Palsy Jane M. Wick, BSN, RN; Jing Feng, PhD; Ellen Raney, MD; Michael Aiona, MD ABSTRACT Cerebral palsy
CLINICAL Single- Event Multilevel Surgery to Correct Movement Disorders in Children With Cerebral Palsy Jane M. Wick, BSN, RN; Jing Feng, PhD; Ellen Raney, MD; Michael Aiona, MD ABSTRACT Cerebral palsy
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Common Apophyseal Problems in the Athlete
 Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Patellofemoral Joint. Question? ANATOMY
 Doug Elenz is a paid Consultant/Advisor for the Biomet Manufacturing Corporation. Doug Elenz, MD Team Orthopaedic Surgeon The University of Texas Men s Athletic Department Question? Patellofemoral Joint
Doug Elenz is a paid Consultant/Advisor for the Biomet Manufacturing Corporation. Doug Elenz, MD Team Orthopaedic Surgeon The University of Texas Men s Athletic Department Question? Patellofemoral Joint
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Author's personal copy
 Gait & Posture 34 (2011) 197 201 Contents lists available at ScienceDirect Gait & Posture journal homepage: www.elsevier.com/locate/gaitpost Full length article Can biomechanical variables predict improvement
Gait & Posture 34 (2011) 197 201 Contents lists available at ScienceDirect Gait & Posture journal homepage: www.elsevier.com/locate/gaitpost Full length article Can biomechanical variables predict improvement
Toe-Walking. Benign Variant or Scourge of Bipedal Locomotion? Definition. Physical Exam. Absent Heel Strike 2/28/2011
 Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch