Transclavicular Osseous Sutures for the Treatment of Displaced Distal Clavicular Fractures in Children
|
|
|
- Sibyl Richard
- 5 years ago
- Views:
Transcription
1 Transclavicular Osseous Sutures for the Treatment of Displaced Distal Clavicular Fractures in Children Jörg Schilcher, Johan Scheer and Lars Adolfsson Linköping University Post Print N.B.: When citing this work, cite the original article. Original Publication: Jörg Schilcher, Johan Scheer and Lars Adolfsson, Transclavicular Osseous Sutures for the Treatment of Displaced Distal Clavicular Fractures in Children, 2016, Journal of Orthopaedic Trauma, (30), 5, E181-E Copyright: Lippincott, Williams & Wilkins Postprint available at: Linköping University Electronic Press
2 Trans-clavicular osseous sutures for the treatment of displaced distal clavicular fractures in children. Jörg Schilcher, PhD, Johan Scheer, PhD and Lars Adolfsson, Professor All from the Department of Experimental and Clinical Medicine and Department of Orthopedic Surgery, Faculty of Health Science, Linköping University, Linköping, Sweden Correspondence Jörg Schilcher Department of Experimental and Clinical Medicine Faculty of Health Science Linköping University SE Linköping Sweden Phone: Fax: Conflicts of Interest and Source of Funding: No conflicts of interest to declare. The study was funded by Östergötland County Council, Sweden. 1
3 Summary We describe a novel surgical technique for the treatment of displaced distal clavicular fractures in children. These fractures are rare and recommendations on treatment vary. Conservative treatment might lead to persistent deformity and limitations of function. Previous reports of surgical treatment involve fracture fixation with K-wires. This requires a routine sequential reoperation to remove the implant and has been associated with serious complications in some patients. The surgical technique described here is based on osseous sutures through the clavicular shaft and coracoclavicular ligaments and is found successful for the treatment of distal clavicular fractures in children and may also be feasible for true acromioclavicular dislocations. The main principle of the technique is a fixation of the displaced clavicle via trans-clavicular drill holes, against the intact inferior periosteal sleeve at the insertion of the coracoclavicular ligaments. No temporary K-wire fixation is needed. To date, we have treated 7 patients with this technique. All fractures healed uneventfully with an excellent functional result and without skeletal deformity. 2
4 Introduction Clavicular fractures in children are common injuries and constitute between 8 to 15% of all pediatric fractures. (1-3) Of these, 10 to 21% occur in the distal third of the bone. In the lateral epiphysis of the clavicle, ossification does not occur until the age of 18 years and the majority of injuries involve the metaphyseal-epiphyseal junction and not the acromioclavicular joint itself. In displaced distal clavicular injuries the thick periosteal sleeve remains partially intact, peeling off the fractured bone like the skin from a banana. (4) The inferior part of the periosteum usually remains attached to the coracoclavicular ligaments and the diaphysis is displaced superiorly thus mimicking the radiographic appearance of acromioclavicular dislocations in adults (5). The intact periosteum enables rapid healing and good remodeling of the injured bone, making surgical interventions unnecessary in the majority of cases (6, 7). However some patients will suffer persistent osseous deformity and limited function. (4, 8-10) The inferior periosteal sleeve and coracoclavicular ligaments often remain intact in distal clavicular fractures (4) and appear to provide sufficient anchorage to keep the clavicular shaft reduced in its periosteal sleeve, maintaining stable fixation during fracture healing. Based on these conditions of the soft tissue envelope, the senior author (LA) has developed an osseous suture technique to treat these fractures without the use of K-wires. The aim of the present study was to describe the technique and report the results of 7 patients treated with this method. Patients Between 2005 and 2013, seven patients with displaced distal clavicular fractures were treated with open reduction and internal fixation using the described technique. There were two female and five male patients between 10 and 16 years of age. 3
5 Following approval from the local committee for medical ethics (DNR: 2014/406-31), all patients were retrospectively identified from our orthopaedic surgical registry and offered a follow-up examination. All identified patients gave informed consent and attended a clinical and radiographic examination in the autumn of 2014, at a mean of 6.4 years after the operation (range 1-9 years). Standard x-rays in anterior and oblique views were taken. During clinical examination range of motion, patients subjective assessment of function, and cosmesis was recorded and function was assessed using the Constant-Murley score. (11) The x-rays were assessed and the fractures classified according to the classifications proposed by Dameron and Rockwood (9) and Nenopolous et al (16). The patients demographic data, fracture classification, fixation method, and outcomes are presented in the Table. Surgical technique All surgeries were performed on consecutive patients within our healthcare district by 5 different consultant surgeons. All patients were operated on within 10 days after the initial trauma. The treating physician judged the indication for surgery after physical examination and review of radiographs and was introduced to the technique by the senior author. Preparation All patients underwent general anesthesia and were washed and draped according to institutional standards. On the operating table the patients were kept in a beach-chair position and the table was positioned to facilitate intraoperative radiography. Skin incision and deep dissection The preferred skin incision was a roughly 4 cm sagittal incision at the level of the fracture line (Figure 1). Longitudinal skin incisions should be avoided due to cosmetic disadvantages. The incision was then carried through the subcutaneous tissue down to 4
6 the superficial fascia overlying the trapezius muscle. The displaced clavicular shaft was found immediately subcutaneous while the fractured lateral end remained attached to the acromioclavicular joint capsule. If necessary the periosteum was incised slightly further to allow mobilization of the fragments. Some fibers of the trapezius muscle were found injured by the trauma in some of the patients. These were sutured at the end of the procedure. Fracture reduction and fixation The coracoid process was palpated through the intact inferior periosteum and the point where the coracoclavicular ligaments insert into the periosteal sleeve was marked with a sterile pen or suture. The medial clavicular fragment was reduced into the periosteal sleeve by lifting of the arm and shoulder girdle in a cranial direction and the fracture was then kept reduced with a clamp. Two 2 mm bicortical drill holes were drilled in the clavicular shaft exiting in the inferior cortex at the level of the coracoclavicular ligaments. A No. 2 braided and non-resorbable suture was passed from superior to inferior through the bicortical drill holes. The suture was secured in the inferior periosteum and through the coracoclavicular ligaments with a Mason- Allen stitch. The suture was then passed from inferior to superior through the other drill hole. The threads were then tightened against the superior aspect of the clavicular shaft keeping it reduced to the ligaments and into the periosteal sleeve (Figure 2A). Subsequently one unicortical hole was drilled in the superior cortex of each fracture fragment. To enhance stability and to fine-tune reduction another No. 2 braided and non-resorbable suture was passed through the unicortical drill holes in the superior cortex of each fracture fragment (Figure 2B). The thread was then tightened and provided reduction and stability along the longitudinal axis of the clavicle. Finally, 5
7 the periosteal sleeve was closed with No. 2-0 braided and resorbable sutures (Figure 2C). Postoperative Management Post-operatively a collar-cuff sling was used for three weeks. A physiotherapist instructed in active, unloaded movement exercises allowing flexion and abduction up to 90 degrees. After 3-4 weeks full range of motion was allowed and full use of the arm in every-day activities. Heavy load and contact sports was discouraged during a minimum of 8 weeks after the operation. Results All fractures healed uneventfully and reduction was maintained at early check-up visits. At an average follow-up period of 6 years (range 1-9 years) all patients reported good functional outcomes with excellent Constant-Murley scores and no remaining skeletal deformity. Final follow-up radiographs showed close to anatomic appearance of the clavicle and acromioclavicular joint in all cases (Figure 3 and 4 and Supplemental Digital Content 1). Two patients complained of hypertrophic scar formation. In both cases a skin incision parallel to the lateral clavicle had been used instead of the standard sagittal incision. On physical examination none of the clavicles appeared shorter or displaced superiorly at the distal end and no instability of the lateral end of the clavicle was neither reported nor noted during arm movements. No hypertrophic callus formation, duplication of the clavicle or ossification of the coracoclavicular ligaments were seen. Discussion 6
8 The trans-clavicular suture technique was developed to provide a surgical solution, without the need for temporary K-wire or cerclage wire fixation, in patients with severely displaced distal clavicular fractures suspected to result in a functional deficit or a poor cosmetic result if treated conservatively. All seven patients in the present series had an excellent functional and radiographic outcome at final follow-up. True acromioclavicular joint dislocations rarely occur in children below the age of 13. (5) The displacement is most often due to a lateral clavicular fracture, leaving the lateral clavicular fragment and epiphyseal growth plate in place. The capsule of the acromioclavicular joint remains undisturbed. Dameron and Rockwood (10) have popularized a classification system for distal clavicular fractures in children similar to the classification system by Rockwood for acromioclavicular injuries in adults. (12) Injuries are categorized into types I to VI with increasing numbers based on the severity and direction of displacement. Up to date it remains unclear, which of the fracture types benefit from reduction and surgical fixation to improve outcome. Although these fractures usually do not affect the acromioclavicular joint, the surrounding injury of the musculature appears similar to that occurring in acromioclavicular joint dislocations in adults. In these injuries there seems to be agreement that surgery is indicated when the soft tissue envelope is severely damaged. (13) For that reason, in the present series surgical intervention was recommended for all type V fractures but also for three patients with type III fractures in whom the displacement was apparent on the exterior and a soft tissue involvement similar to a type V lesion was suspected clinically. Also, these patients were older, having less potential for remodeling. 7
9 Furthermore, all fractures in our series were classified according to Nenopolous et al, (14) a modern classification system for distal clavicular fractures in children. All injuries in our series were graded as group 2b, 3b or 5 for which these authors recommend surgery. Group 2b injuries are transverse, displaced fractures, grade 3b injuries are displaced oblique fractures and surgery is recommended when the displacement exceeds the thickness of 2 cortices. Group 5 injuries are true acromioclavicular dislocations. In general however, the acromioclavicular ligaments, the acromioclavicular joint and most of the periosteal sleeve is intact in distal clavicular injuries providing exceptional potential for growth and remodeling. It remains unclear if these patients in our series profited from the surgical intervention since several other authors have stated that the majority of patients with fracture types I, II and III can be treated nonsurgical with a good functional and cosmetic result. (6-8, 10, 15) For the displaced fracture types IV, V and VI some authors suggest that most patients will regain full function without cosmetic deficits (6, 7). Other authors recommend that patients with grossly displaced fractures or fixed displacement should be treated with reduction and surgical fixation to prevent definitive deformity. (4, 8-10) With increasing age, and decreasing capacity to remodel a deformity the indication for surgical reduction and fixation becomes stronger. (5) Previously described treatment options for displaced fractures involve percutaneous fixation with K-wires and suture repair of the superior periosteal sleeve or more extensive soft tissue repairs without the use of hardware. (4, 16) However, severe complications caused by the migration of K-wires to the lungs and spinal canal have been reported. (17-19) Furthermore, K-wire fixation is associated with compulsory reoperations to remove the implant. This might make surgical 8
10 fixation of displaced fractures less attractive for surgeons, patients and their caretakers. Therefore the trans-clavicular suture technique described here might be a more attractive alternative in some cases. The method is a simplified modification of a previously described technique, (4, 16) aiming at using the strong point of fixation provided by the coraco-clavicular ligaments and without the use of cerclage wires. (20) Recently a similar technique, using sutures around the coracoid process, was reported to provide successful fixation in displaced type II distal clavicular fractures in adults. (21) In our series 5 different surgeons performed the surgeries on the 7 patients. This might be regarded as disadvantageous because of the very low volume per surgeon. However, we believe it emphasizes the simplicity of the technique ensuring good results even when performed seldom. Surgeries performed via a longitudinal incision had a higher likelihood to lead to unsatisfactory cosmetic results due to the formation of hypertrophic scar tissue. The extension of the incision medially towards skin areas prone to the formation of hypertrophic scars and keloids might be the reason for this. Moreover the sagittal incision should be preferred because it provides better access for suture placement and follows the course of Langer s skin lines (Figure 1), which too is cosmetically favorable. Also the risk of injuring the lateral supraclavicular nerve branch, providing skin sensation caudal to the clavicle is lower. In adults the course of this nerve is highly variable but has a consistent safe zone up to 1.9 cm medial to the acromioclavicular joint. (22) We therefore recommend the sagittal skin incision as the standard approach. The lack of a conservatively treated control group makes it impossible to evaluate the effect of the surgical procedure on the outcome. At the current level of evidence, the trans-clavicular suture technique is a safe surgical 9
11 treatment option for patients with severely displaced distal clavicular fractures where surgical reduction and fixation deems indicated to improve outcome. 10
12 References 1. Landin LA. Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population Acta Orthop Scand Suppl. 1983;202: Lichtenberg RP. A study of 2,532 fractures in children. Am J Surg. 1954;87: Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res. 1994: Falstie-Jensen S, Mikkelsen P. Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br. 1982;64: Eidman DK, Siff SJ, Tullos HS. Acromioclavicular lesions in children. Am J Sports Med. 1981;9: Black GB, McPherson JA, Reed MH. Traumatic pseudodislocation of the acromioclavicular joint in children. A fifteen year review. Am J Sports Med. 1991;19: Havranek P. Injuries of distal clavicular physis in children. J Pediatr Orthop. 1989;9: Ogden JA. Distal clavicular physeal injury. Clin Orthop Relat Res. 1984: Bakalim G, Wilppula E. Surgical or conservative treatment of total dislocation of the acromioclavicular joint. Acta Chir Scand. 1975;141: Dameron T, Rockwood C. Fractures in children. In: Rockwood C, Wilkins K, King R, eds. Philadelphia: JB Lippincott; 1984: Constant CR, Murley AHG. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;No. 214: Williams G, Nguyen V, Rockwood C. Classification and radiographic analysis of acromioclavicular dislocations. Appl Radiol. 1989;Feb: Bradley JP, Elkousy H. Decision making: operative versus nonoperative treatment of acromioclavicular joint injuries. Clin Sports Med. 2003;22: Nenopoulos SP, Gigis IP, Chytas AA, et al. Outcome of distal clavicular fracture separations and dislocations in immature skeleton. Injury. 2011;42: Masnovi ME, Mehlman CT, Eismann EA, et al. Pediatric refracture rates after angulated and completely displaced clavicle shaft fractures. J Orthop Trauma. 2014;28: Gronmark T. Surgical treatment of acromioclavicular dislocation. Acta Orthop Scand. 1976;47: Bennis S, Scarone P, Lepeintre JF, et al. Asymptomatic spinal canal migration of clavicular K-wire at the cervicothoracic junction. Orthopedics. 2008; Hegemann S, Kleining R, Schindler HG, et al. Kirschner wire migration in the contralateral lung after osteosynthesis of a clavicular fracture. Unfallchirurg. 2005;108: Mamane W, Breitel D, Lenoir T, et al. Spinal migration of a Kirschner wire after surgery for clavicular nonunion. A case report and review of the literature. Chir Main. 2009;28:
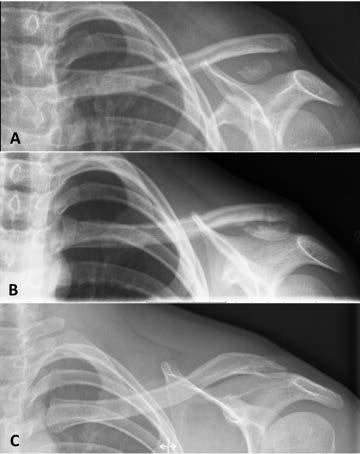
13 20. Montgomery SP, Loyd RD. Avulsion fracture of the coracoid epiphysis with acromioclavicular separation. Report of two cases in adolescents and review of the literature. J Bone Joint Surg Am. 1977;59: Duralde XA, Pennington SD, Murray DH. Interfragmentary suture fixation for displaced acute type II distal clavicle fractures. J Orthop Trauma. 2014;28: Nathe T, Tseng S, Yoo B. The anatomy of the supraclavicular nerve during surgical approach to the clavicular shaft. Clin Orthop Relat Res. 2011;469: Figure Legend Figure 1. Sagittal incision demonstrated on a right shoulder. The recommended incision runs over the distal clavicle along the lines of Langer and at the tip of the coracoid process. Apart from improved cosmesis and optimal surgical access for the repair, the incision is located at a distance from the supraclavicular nerves. (22) NZ=Nerve Zone. Figure 2. Surgical technique: Two holes are drilled in the medial fragment of the clavicle. Sutures are passed through and attached to the intact inferior periosteum with a Mason-Allen stitch (A). The sutures are then tightened against the superior aspect of the clavicular shaft and locked with a standard surgical knot. This maneuver reduces the clavicle back into the periosteal sleeve (B). Sutures are then passed through unicortical drill holes in the superior cortex of each fracture fragment and tightened. This provides reduction and stability along the longitudinal axis of the clavicle (C). The superior periosteal sleeve is then repaired. Figure 3. Twelve-year-old patient with displaced lateral clavicular fracture (A) treated with the trans-clavicular suture technique (B). At follow-up, 9 years after surgery the fracture had remodeled adequately (C). Figure 4. Twelve-year-old patient with displaced lateral clavicular fracture (A) treated with the trans-clavicular suture technique (B). At follow-up, 1 year after surgery the fracture had remodeled adequately (C). 12
14 Online supplementary material Online supplementary material 1. Thirteen-year-old patient with displaced lateral clavicular fracture (A) treated with the trans-clavicular suture technique (B). At follow-up, 8 years after surgery the fracture had remodeled adequately (C). 13
15 14
16 Table. Patient Demographics, Fracture Classification, Treatment and Outcomes Case No. Sex Age at Follow-up Dameron and Nenopoulos (16) Side Constant-Murley Constant-Murley (M/F) injury (Years) Rockwoods (9) classification (D/ND) score* score* (Years) classification (injured side) (uninjured side) 1 M 12 9 V 2b D M 13 8 V 2b D F 16 8 III 2b D M 10 7 V 3b D M 13 7 III 5 ND F 14 5 III 2b D M 12 1 V 2b ND D: Dominant. ND: Non dominant. * Constant-Murley score at final follow up.

17
18
19

20

21
Injury, Int. J. Care Injured 42 (2011) Contents lists available at ScienceDirect. Injury. journal homepage:
 Contents lists available at ScienceDirect. Injury. journal homepage:") Injury, Int. J. Care Injured 42 (2011) 376 380 Contents lists available at ScienceDirect Injury journal homepage: www.elsevier.com/locate/injury Outcome of distal clavicular fracture separations and dislocations
Injury, Int. J. Care Injured 42 (2011) 376 380 Contents lists available at ScienceDirect Injury journal homepage: www.elsevier.com/locate/injury Outcome of distal clavicular fracture separations and dislocations
AcUMEDr. LoCKING CLAVICLE PLATE SYSTEM
 AcUMEDr LoCKING CLAVICLE PLATE SYSTEM LoCKING CLAVICLE PLATE SYSTEM Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients.
AcUMEDr LoCKING CLAVICLE PLATE SYSTEM LoCKING CLAVICLE PLATE SYSTEM Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients.
WINSTA-C. Clavicle Plating System
 Clavicle Plating System Clinical Advisor Michael Kurer FRCS FRCS (Orth) Consultant Orthopaedic and Shoulder Surgeon North Middlesex University Hospital NHS Trust Table of Contents Introduction Indication
Clavicle Plating System Clinical Advisor Michael Kurer FRCS FRCS (Orth) Consultant Orthopaedic and Shoulder Surgeon North Middlesex University Hospital NHS Trust Table of Contents Introduction Indication
AC Separations & Distal Clavicle Fractures. Joshua M. Abzug, MD
 AC Separations & Distal Clavicle Fractures Joshua M. Abzug, MD Introduction Account for 10-30% of pediatric clavicle fxs Result of direct blow to shoulder or fall onto distal clavicle Mechanism Collision
AC Separations & Distal Clavicle Fractures Joshua M. Abzug, MD Introduction Account for 10-30% of pediatric clavicle fxs Result of direct blow to shoulder or fall onto distal clavicle Mechanism Collision
Clavicle fractures are common in skeletally immature patients,
 TECHNIQUE Distal Clavicle Fixation in the Skeletally Immature S. Clifton Willimon, MD, Henry B. Ellis, MD, and Peter J. Millett, MD, MSc Abstract: Distal clavicle fractures in adolescent patients may benefit
TECHNIQUE Distal Clavicle Fixation in the Skeletally Immature S. Clifton Willimon, MD, Henry B. Ellis, MD, and Peter J. Millett, MD, MSc Abstract: Distal clavicle fractures in adolescent patients may benefit
Surgical treatment of acute and chronic acromioclavicular dislocation Tossy type III and V using the Hook Plate
 Acta Orthop. Belg., 2008, 4, 441-44 ORIGINAL STUDY Surgical treatment of acute and chronic acromioclavicular dislocation Tossy type and using the Hook Plate Samir EJAM, Thomas LIND, Boe FALKENBERG From
Acta Orthop. Belg., 2008, 4, 441-44 ORIGINAL STUDY Surgical treatment of acute and chronic acromioclavicular dislocation Tossy type and using the Hook Plate Samir EJAM, Thomas LIND, Boe FALKENBERG From
Open reduction; plate fixation 1 Principles
 Executive Editor: Peter Trafton Authors: Martin Jaeger, Frankie Leung, Wilson Li Proximal humerus 11-A2 Open reduction, plate fixation Search search... Shortcuts All Preparations All Approaches All Reductions
Executive Editor: Peter Trafton Authors: Martin Jaeger, Frankie Leung, Wilson Li Proximal humerus 11-A2 Open reduction, plate fixation Search search... Shortcuts All Preparations All Approaches All Reductions
Clavicle Plating System Acu-Sinch Repair System. Surgical Technique
 Clavicle Plating System Acu-Sinch Repair System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and
Clavicle Plating System Acu-Sinch Repair System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and
Acromioclavicular joint reconstruction using anchor sutures : Surgical technique and preliminary results
 Acta Orthop. Belg., 2010, 76, 307-311 ORIGINAL STUDY Acromioclavicular joint reconstruction using anchor sutures : Surgical technique and preliminary results Yehia BASYONI, Abd-El-Rahman A. EL-GANAINY,
Acta Orthop. Belg., 2010, 76, 307-311 ORIGINAL STUDY Acromioclavicular joint reconstruction using anchor sutures : Surgical technique and preliminary results Yehia BASYONI, Abd-El-Rahman A. EL-GANAINY,
LCP Superior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle.
 Technique Guide LCP Superior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Table of Contents Introduction LCP Superior Clavicle
Technique Guide LCP Superior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Table of Contents Introduction LCP Superior Clavicle
Acromioclavicular Pseudo-dislocation with Concomitant Coracoid Process Fracture and Coracoclavicular Ligament Rupture in a 12-year-old Male
 CASE REPORT Acromioclavicular Pseudo-dislocation with Concomitant Coracoid Process Fracture and Coracoclavicular Ligament Rupture in a 12-year-old Male ABSTRACT INTRODUCTION The combination of lateral
CASE REPORT Acromioclavicular Pseudo-dislocation with Concomitant Coracoid Process Fracture and Coracoclavicular Ligament Rupture in a 12-year-old Male ABSTRACT INTRODUCTION The combination of lateral
VA-LCP Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle.
 Technique Guide VA-LCP Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Table of Contents Introduction VA-LCP Anterior
Technique Guide VA-LCP Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Table of Contents Introduction VA-LCP Anterior
Percutaneous Humeral Fracture Repair Surgical Technique
 Percutaneous Humeral Fracture Repair Surgical Technique Percutaneous Pinning Percutaneous Humeral Fracture Repair Closed reduction followed by percutaneous fixation reduces risk from soft tissue dissection
Percutaneous Humeral Fracture Repair Surgical Technique Percutaneous Pinning Percutaneous Humeral Fracture Repair Closed reduction followed by percutaneous fixation reduces risk from soft tissue dissection
Acu-Sinch Repair System. Technical Monograph
 Acu-Sinch Repair System Technical Monograph Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that improve
Acu-Sinch Repair System Technical Monograph Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that improve
Locking Clavicle Plating System. Surgical Technique
 Locking Clavicle Plating System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that
Locking Clavicle Plating System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches that
Clavicle Hook Locking Plate
 990210003 Clavicle Hook Locking Plate Clavicle Hook Locking Plate Clavicle Hook Locking Plate INDEX Indications Patient Position Surgical Technique Step 1 Approach Step 2 Reduction Step 3 Temporary Fixation
990210003 Clavicle Hook Locking Plate Clavicle Hook Locking Plate Clavicle Hook Locking Plate INDEX Indications Patient Position Surgical Technique Step 1 Approach Step 2 Reduction Step 3 Temporary Fixation
3.5 mm LCP Clavicle Hook Plates
 Part of the Synthes Locking Compression Plate (LCP ) System 3.5 mm LCP Clavicle Hook Plates Surgical Technique Table of Contents Introduction 3.5 mm LCP Clavicle Hook Plates 2 AO Principles 4 Indications
Part of the Synthes Locking Compression Plate (LCP ) System 3.5 mm LCP Clavicle Hook Plates Surgical Technique Table of Contents Introduction 3.5 mm LCP Clavicle Hook Plates 2 AO Principles 4 Indications
LCP Metaphyseal Plate for distal medial tibia. Anatomically precontoured metaphyseal plate.
 Indications The LCP Metaphyseal Plate for distal medial tibia is a preshaped plate that allows optimal treatment of juxta-articular fractures of the distal tibia extending into the shaft area. This plate
Indications The LCP Metaphyseal Plate for distal medial tibia is a preshaped plate that allows optimal treatment of juxta-articular fractures of the distal tibia extending into the shaft area. This plate
AcUMEDr. Locking Proximal Humeral Plate. PoLARUSr PHPt
 AcUMEDr Locking Proximal Humeral Plate PoLARUSr PHPt PoLARUSr PHPt LOCKING PROXIMAL HUMERAL PLATE Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons,
AcUMEDr Locking Proximal Humeral Plate PoLARUSr PHPt PoLARUSr PHPt LOCKING PROXIMAL HUMERAL PLATE Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons,
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
LCP Superior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle.
 LCP Superior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Surgical Technique This publication is not intended for distribution
LCP Superior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Surgical Technique This publication is not intended for distribution
REHABILITATION FOR SHOULDER FRACTURES & SURGERIES. Clavicle fractures Proximal head of humerus fractures
 REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta
REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta
OPERATIVE TECHNIQUE GALAXY FIXATION SHOULDER
 OPERATIVE TECHNIQUE GALAXY FIXATION SHOULDER cop2 OPERATIVE TECHNIQUE INTRODUCTION 1 FEATURES OF SHOULDER COMPONENTS 2 EQUIPMENT REQUIRED 5 PREOPERATIVE PLANNING 6 SURGICAL PROCEDURE 8 POST OPERATIVE MANAGEMENT
OPERATIVE TECHNIQUE GALAXY FIXATION SHOULDER cop2 OPERATIVE TECHNIQUE INTRODUCTION 1 FEATURES OF SHOULDER COMPONENTS 2 EQUIPMENT REQUIRED 5 PREOPERATIVE PLANNING 6 SURGICAL PROCEDURE 8 POST OPERATIVE MANAGEMENT
3.5 mm Clavicle Hook Plates
 A Single Solution for Lateral Clavicle Fractures and Acromioclavicular Joint Dislocations 3.5 mm Clavicle Hook Plates Surgical Technique Discontinued December 2017 DSUS/TRM/1016/1126(1) Table of Contents
A Single Solution for Lateral Clavicle Fractures and Acromioclavicular Joint Dislocations 3.5 mm Clavicle Hook Plates Surgical Technique Discontinued December 2017 DSUS/TRM/1016/1126(1) Table of Contents
Technique Guide. 3.5 mm LCP Periarticular Proximal Humerus Plate. Part of the Synthes locking compression plate (LCP) system.
 system.") Technique Guide 3.5 mm LCP Periarticular Proximal Humerus Plate. Part of the Synthes locking compression plate (LCP) system. Table of Contents Introduction 3.5 mm LCP Proximal Humerus Plate 2 AO Principles
Technique Guide 3.5 mm LCP Periarticular Proximal Humerus Plate. Part of the Synthes locking compression plate (LCP) system. Table of Contents Introduction 3.5 mm LCP Proximal Humerus Plate 2 AO Principles
Case Report Medial Condyle Fracture (Kilfoyle Type III) of the Distal Humerus with Transient Fishtail Deformity after Surgery
 of the Distal Humerus with Transient Fishtail Deformity after Surgery") Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9053949, 4 pages https://doi.org/10.1155/2017/9053949 Case Report Medial Condyle Fracture (Kilfoyle Type III) of the Distal Humerus with Transient
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 9053949, 4 pages https://doi.org/10.1155/2017/9053949 Case Report Medial Condyle Fracture (Kilfoyle Type III) of the Distal Humerus with Transient
Acromioclavicular (AC) Device
 Device") Acromioclavicular (AC) Device Product Information Indications Instrumentation Acromio-clavicular dislocation (acute & chronic). 7 Rockwood Type III, IV & V acromio-clavicular joint injury. Lateral clavicle
Acromioclavicular (AC) Device Product Information Indications Instrumentation Acromio-clavicular dislocation (acute & chronic). 7 Rockwood Type III, IV & V acromio-clavicular joint injury. Lateral clavicle
Humerus Block. Discontinued December 2016 DSEM/TRM/0115/0296(1) Surgical Technique. This publication is not intended for distribution in the USA.
 Surgical Technique. This publication is not intended for distribution in the USA.") Humerus Block Surgical Technique Discontinued December 2016 DSEM/TRM/0115/0296(1) This publication is not intended for distribution in the USA. Instruments and implants approved by the AO Foundation. Contents
Humerus Block Surgical Technique Discontinued December 2016 DSEM/TRM/0115/0296(1) This publication is not intended for distribution in the USA. Instruments and implants approved by the AO Foundation. Contents
PROXIMAL TIBIAL PLATE
 SURGICAL NÁSTROJE TECHNIQUE PRO ARTROSKOPII PROXIMAL INSTRUMENTS TIBIAL FOR PLATE ARTHROSCOPY Proximal Tibial Plate Description of medical device The Proximal Tibial Plate is used in epyphyseal and metaphyseal
SURGICAL NÁSTROJE TECHNIQUE PRO ARTROSKOPII PROXIMAL INSTRUMENTS TIBIAL FOR PLATE ARTHROSCOPY Proximal Tibial Plate Description of medical device The Proximal Tibial Plate is used in epyphyseal and metaphyseal
Clavicle CORE Plating System Surgical Technique
 Clavicle CORE Plating System Surgical Technique Introducing the System Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods
Clavicle CORE Plating System Surgical Technique Introducing the System Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods
LCP Superior Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle.
 LCP Superior Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Surgical Technique This publication is not intended for
LCP Superior Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Surgical Technique This publication is not intended for
NCB Proximal Humerus Plating System
 NCB Proximal Humerus Plating System Surgical Technique The right locking option for tough fractures Disclaimer This document is intended exclusively for experts in the field, i.e. physicians in particular,
NCB Proximal Humerus Plating System Surgical Technique The right locking option for tough fractures Disclaimer This document is intended exclusively for experts in the field, i.e. physicians in particular,
Coracoid Bone Conserving Acromioclavicular Joint Reconstruction using ToggleLoc Device with ZipLoop Technology
 Coracoid Bone Conserving Acromioclavicular Joint Reconstruction using ToggleLoc Device with ZipLoop Technology Surgical Technique Surgical Protocol by Peter J. Evans, MD, PhD SPORTS MEDICINE One Surgeon.
Coracoid Bone Conserving Acromioclavicular Joint Reconstruction using ToggleLoc Device with ZipLoop Technology Surgical Technique Surgical Protocol by Peter J. Evans, MD, PhD SPORTS MEDICINE One Surgeon.
Arthroscopic Stabilization of Acute Acromioclavicular Joint Dislocation using the TightRope System Surgical Technique
 Arthroscopic Stabilization of Acute Acromioclavicular Joint Dislocation using the TightRope System Surgical Technique AC Joint TightRope Fixation Background Disruption of the coracoclavicular ligaments
Arthroscopic Stabilization of Acute Acromioclavicular Joint Dislocation using the TightRope System Surgical Technique AC Joint TightRope Fixation Background Disruption of the coracoclavicular ligaments
Case Report Locked Superior Dislocation of the Acromioclavicular Joint
 Volume 2013, Article ID 508219, 4 pages http://dx.doi.org/10.1155/2013/508219 Case Report Locked Superior Dislocation of the Acromioclavicular Joint Salma Eltoum Elamin, Apurv Sinha, and Mark Webb Department
Volume 2013, Article ID 508219, 4 pages http://dx.doi.org/10.1155/2013/508219 Case Report Locked Superior Dislocation of the Acromioclavicular Joint Salma Eltoum Elamin, Apurv Sinha, and Mark Webb Department
A locking plate system that expands a surgeon s options in trauma surgery. Zimmer NCB Plating System
 A locking plate system that expands a surgeon s options in trauma surgery Zimmer NCB Plating System The Power of Choice The power of having true intraoperative options is at your fingertips. Using standard
A locking plate system that expands a surgeon s options in trauma surgery Zimmer NCB Plating System The Power of Choice The power of having true intraoperative options is at your fingertips. Using standard
In general, most clavicle fractures can be managed. A Comparison of Nonoperative and Operative Treatment of Type II Distal Clavicle Fractures
 32 Bulletin Hospital for Joint Diseases Volume 61, Numbers 1 & 2 2002-2003 A Comparison of Nonoperative and Operative Treatment of Type II Distal Clavicle Fractures Andrew S. Rokito, M.D., Joseph D. Zuckerman,
32 Bulletin Hospital for Joint Diseases Volume 61, Numbers 1 & 2 2002-2003 A Comparison of Nonoperative and Operative Treatment of Type II Distal Clavicle Fractures Andrew S. Rokito, M.D., Joseph D. Zuckerman,
Clavicle Fractures in Children and Adolescents
 Clavicle Fractures in Children and Adolescents John A. Schlechter, DO Children s Hospital Orange County Orange, CA Objectives The Bone The Fracture The Treatment The Controversies The Bone The Clavicle
Clavicle Fractures in Children and Adolescents John A. Schlechter, DO Children s Hospital Orange County Orange, CA Objectives The Bone The Fracture The Treatment The Controversies The Bone The Clavicle
Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric Patient
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 6354284, 4 pages https://doi.org/10.1155/2017/6354284 Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 6354284, 4 pages https://doi.org/10.1155/2017/6354284 Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric
Zimmer Small Fragment Universal Locking System. Surgical Technique
 Zimmer Small Fragment Universal Locking System Surgical Technique Zimmer Small Fragment Universal Locking System 1 Zimmer Small Fragment Universal Locking System Surgical Technique Table of Contents Introduction
Zimmer Small Fragment Universal Locking System Surgical Technique Zimmer Small Fragment Universal Locking System 1 Zimmer Small Fragment Universal Locking System Surgical Technique Table of Contents Introduction
Twin Tail TightRope System
 Open Stabilization of Acute Acromioclavicular Joint Dislocation using the Twin Tail TightRope System Surgical Technique Twin Tail TightRope System Open Stabilization of Acute Acromioclavicular Joint Dislocation
Open Stabilization of Acute Acromioclavicular Joint Dislocation using the Twin Tail TightRope System Surgical Technique Twin Tail TightRope System Open Stabilization of Acute Acromioclavicular Joint Dislocation
Elbow Hinge Fixator. Guided Flexion/Extension for Unstable Elbow Fractures.
 Elbow Hinge Fixator. Guided Flexion/Extension for Unstable Elbow Fractures. Surgical Technique MR Safe Radiolucent Table of Contents System Description 3 Indications and Contraindications 4 Fixation Components
Elbow Hinge Fixator. Guided Flexion/Extension for Unstable Elbow Fractures. Surgical Technique MR Safe Radiolucent Table of Contents System Description 3 Indications and Contraindications 4 Fixation Components
A locking plate system that expands a surgeon s options in trauma surgery. Zimmer NCB Plating System
 A locking plate system that expands a surgeon s options in trauma surgery Zimmer NCB Plating System The Power of Choice The power of having true intraoperative options is at your fingertips. Using standard
A locking plate system that expands a surgeon s options in trauma surgery Zimmer NCB Plating System The Power of Choice The power of having true intraoperative options is at your fingertips. Using standard
3.5 mm LCP Superior Anterior Clavicle Plates
 Part of the DePuy Synthes Locking Compression Plate (LCP ) System 3.5 mm LCP Superior Anterior Clavicle Plates Surgical Technique Table of Contents Introduction 3.5 mm LCP Superior Anterior Clavicle Plates
Part of the DePuy Synthes Locking Compression Plate (LCP ) System 3.5 mm LCP Superior Anterior Clavicle Plates Surgical Technique Table of Contents Introduction 3.5 mm LCP Superior Anterior Clavicle Plates
Acromioclavicular (AC) joint injuries account for 9% to 12% of all shoulder
 joint injuries account for 9% to 12% of all shoulder") C H A P T E R 39 ACROMIOCLAVICULAR JOINT RECONSTRUCTION Joshua A. Greenspoon Maximilian Petri Peter J. Millett Acromioclavicular (AC) joint injuries account for 9% to 12% of all shoulder injuries and are
C H A P T E R 39 ACROMIOCLAVICULAR JOINT RECONSTRUCTION Joshua A. Greenspoon Maximilian Petri Peter J. Millett Acromioclavicular (AC) joint injuries account for 9% to 12% of all shoulder injuries and are
Surgical Technique International Version. Clavicle Locking Plate
 Surgical Technique International Version Clavicle Locking Plate PERI-LOC Upper Extremity Locked Plating System Clavicle Surgical Techniquefor Table of Contents Introduction........................................................2
Surgical Technique International Version Clavicle Locking Plate PERI-LOC Upper Extremity Locked Plating System Clavicle Surgical Techniquefor Table of Contents Introduction........................................................2
MEDIAL EPICONDYLE FRACTURES
 MEDIAL EPICONDYLE FRACTURES Demographic 20% of elbow fractures 60% of which are associated with elbow dislocation. 75% in boys between 6-12 years 20% of elbow dislocation with ME fracture, the ME is incarcerated
MEDIAL EPICONDYLE FRACTURES Demographic 20% of elbow fractures 60% of which are associated with elbow dislocation. 75% in boys between 6-12 years 20% of elbow dislocation with ME fracture, the ME is incarcerated
Technique Guide. 2.4 mm Variable Angle LCP Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology.
 Technique Guide 2.4 mm Variable Angle LCP Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology. Table of Contents Introduction 2.4 mm Variable Angle LCP
Technique Guide 2.4 mm Variable Angle LCP Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology. Table of Contents Introduction 2.4 mm Variable Angle LCP
Anatomic AC Joint TightRope Fixation
 Arthroscopic Anatomic Stabilization of Acute Acromioclavicular Joint Dislocation using the TightRope System Surgical Technique Anatomic AC Joint TightRope Fixation Background Disruption of the coracoclavicular
Arthroscopic Anatomic Stabilization of Acute Acromioclavicular Joint Dislocation using the TightRope System Surgical Technique Anatomic AC Joint TightRope Fixation Background Disruption of the coracoclavicular
COMPARATIVE STUDY OF FUNCTIONAL OUTCOME OF OPERATIVE AND NON-OPERATIVE TREATMENT IN MIDSHAFT CLAVICLE FRACTURES
 COMPARATIVE STUDY OF FUNCTIONAL OUTCOME OF OPERATIVE AND NON-OPERATIVE TREATMENT IN MIDSHAFT CLAVICLE FRACTURES R. Sahaya Jose 1 1Assistant Professor, Department of Orthopaedics, Sree Mookambika Institute
COMPARATIVE STUDY OF FUNCTIONAL OUTCOME OF OPERATIVE AND NON-OPERATIVE TREATMENT IN MIDSHAFT CLAVICLE FRACTURES R. Sahaya Jose 1 1Assistant Professor, Department of Orthopaedics, Sree Mookambika Institute
Design Team Vipul Nanavati, MD James M. Paci, MD Frederick W. Werner, MME Levi G. Sutton, MS
 Design Team Vipul Nanavati, MD James M. Paci, MD Frederick W. Werner, MME Levi G. Sutton, MS SUNY Upstate Medical University Scott Macfarlane Office of Technology Transfer 315-464-7613 Anatomically shaped
Design Team Vipul Nanavati, MD James M. Paci, MD Frederick W. Werner, MME Levi G. Sutton, MS SUNY Upstate Medical University Scott Macfarlane Office of Technology Transfer 315-464-7613 Anatomically shaped
Fractures of the tibia shaft treated with locked intramedullary nail Retrospective clinical and radiographic assesment
 ARS Medica Tomitana - 2013; 4(75): 197-201 DOI: 10.2478/arsm-2013-0035 Șerban Al., Botnaru V., Turcu R., Obadă B., Anderlik St. Fractures of the tibia shaft treated with locked intramedullary nail Retrospective
ARS Medica Tomitana - 2013; 4(75): 197-201 DOI: 10.2478/arsm-2013-0035 Șerban Al., Botnaru V., Turcu R., Obadă B., Anderlik St. Fractures of the tibia shaft treated with locked intramedullary nail Retrospective
Index. B Backslap technique depth assessment, 82, 83 diaphysis distal trocar, 82 83
 Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
A Patient s Guide to Adult Clavicle Fractures
 A Patient s Guide to Adult Clavicle Fractures 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 1 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Adult Clavicle Fractures 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 1 DISCLAIMER: The information in this booklet is compiled from a variety
Conventus CAGE PH Surgical Techniques
 Conventus CAGE PH Surgical Techniques Conventus Orthopaedics The Conventus CAGE PH (PH Cage) is a permanent implant comprised of an expandable scaffold, made from nitinol and titanium, which is deployed
Conventus CAGE PH Surgical Techniques Conventus Orthopaedics The Conventus CAGE PH (PH Cage) is a permanent implant comprised of an expandable scaffold, made from nitinol and titanium, which is deployed
Reconstruction of coracoclavicular and acromioclavicular ligaments under small incision for the treatment of old acromioclavicular joint dislocation.
 Research Article http://www.alliedacademies.org/journal-physical-therapy-sports-medicine/ Reconstruction of coracoclavicular and acromioclavicular ligaments under small incision for the treatment of old
Research Article http://www.alliedacademies.org/journal-physical-therapy-sports-medicine/ Reconstruction of coracoclavicular and acromioclavicular ligaments under small incision for the treatment of old
Common Orthopaedic Injuries in Children
 Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
LCP Distal Humerus Plates
 The anatomic fixation system for the distal humerus with angular stability Surgical technique LCP Locking Compression Plate Contents Indications and contraindications 2 Implants 3 Instruments 5 Preparation
The anatomic fixation system for the distal humerus with angular stability Surgical technique LCP Locking Compression Plate Contents Indications and contraindications 2 Implants 3 Instruments 5 Preparation
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
2.4 mm Variable Angle LCP Volar Extra-Articular Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology.
 Technique Guide 2.4 mm Variable Angle LCP Volar Extra-Articular Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology. Table of Contents Introduction 2.4
Technique Guide 2.4 mm Variable Angle LCP Volar Extra-Articular Distal Radius System. For fragment-specific fracture fixation with variable angle locking technology. Table of Contents Introduction 2.4
Acu-Loc Wrist Spanning Plate System. Surgical Technique
 Acu-Loc Wrist Spanning Plate System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches
Acu-Loc Wrist Spanning Plate System Surgical Technique Acumed is a global leader of innovative orthopaedic and medical solutions. We are dedicated to developing products, service methods, and approaches
Transcapsular Buttonholing of the Proximal Ulna as a Cause for Irreducible Pediatric Anterior Elbow Dislocation.
 Transcapsular Buttonholing of the Proximal Ulna as a Cause for Irreducible Pediatric Anterior Elbow Dislocation. Nick N. Patel, Emory University Robert W. Bruce, Emory University Journal Title: Case report
Transcapsular Buttonholing of the Proximal Ulna as a Cause for Irreducible Pediatric Anterior Elbow Dislocation. Nick N. Patel, Emory University Robert W. Bruce, Emory University Journal Title: Case report
Fractures of the Hand in Children Which are simple? And Which have pitfalls??
 Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
Fractures of the Hand in Children Which are simple? And Which have pitfalls?? Kaye E Wilkins DVM, MD Professor of Orthopedics and Pediatrics Departments of Orthopedics and Pediatrics University of Texas
LCP Proximal Radius Plates 2.4. Plates for radial head rim and for radial head neck address individual fracture patterns of the proximal radius.
 Technique Guide LCP Proximal Radius Plates 2.4. Plates for radial head rim and for radial head neck address individual fracture patterns of the proximal radius. Table of Contents Introduction LCP Proximal
Technique Guide LCP Proximal Radius Plates 2.4. Plates for radial head rim and for radial head neck address individual fracture patterns of the proximal radius. Table of Contents Introduction LCP Proximal
LCP Metaphyseal Plates. For extra-articular fractures.
 LCP Metaphyseal Plates. For extra-articular fractures. Surgical Technique This publication is not intended for distribution in the USA. Instruments and implants approved by the AO Foundation. Image intensifier
LCP Metaphyseal Plates. For extra-articular fractures. Surgical Technique This publication is not intended for distribution in the USA. Instruments and implants approved by the AO Foundation. Image intensifier
EVOS MINI with IM Nailing
 Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
Technique Guide. PHILOS and PHILOS Long. The anatomic fixation system for the proximal humerus.
 Technique Guide PHILOS and PHILOS Long. The anatomic fixation system for the proximal humerus. Table of Contents Introduction PHILOS and PHILOS Long 2 AO Principles 4 Indications 5 Surgical Technique
Technique Guide PHILOS and PHILOS Long. The anatomic fixation system for the proximal humerus. Table of Contents Introduction PHILOS and PHILOS Long 2 AO Principles 4 Indications 5 Surgical Technique
Surgical Technique. Intramedullary locked Nailing With Screws for Humerus Fractures Solid/Cannulated. Humeral Interlocking Nail.
 Screws for Humerus Fractures Surgical Technique Humeral Interlocking Nail Approved by Humerus Nail Kit Code 08050001 Contents Introduction Implant design Indications Pre-operative planning Patient positioning
Screws for Humerus Fractures Surgical Technique Humeral Interlocking Nail Approved by Humerus Nail Kit Code 08050001 Contents Introduction Implant design Indications Pre-operative planning Patient positioning
Terrible Triad: Tricks for Dealing with the Unstable Elbow
 Terrible Triad: Tricks for Dealing with the Unstable Elbow Mark A. Mighell, MD Kaitlyn N. Christmas, BS Disclosure Paid Consultation Research Support Speakers Bureau Paid Consultation Speakers Bureau The
Terrible Triad: Tricks for Dealing with the Unstable Elbow Mark A. Mighell, MD Kaitlyn N. Christmas, BS Disclosure Paid Consultation Research Support Speakers Bureau Paid Consultation Speakers Bureau The
LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia.
 LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia. LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia.
LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia. LISS DF and LISS PLT. Less Invasive Stabilization Systems for Distal Femur and Proximal Lateral Tibia.
Fracture and Dislocation of Metacarpal Bones, Metacarpophalangeal Joints, Phalanges, and Interphalangeal Joints ( 1-Jan-1985 )
") In: Textbook of Small Animal Orthopaedics, C. D. Newton and D. M. Nunamaker (Eds.) Publisher: International Veterinary Information Service (www.ivis.org), Ithaca, New York, USA. Fracture and Dislocation
In: Textbook of Small Animal Orthopaedics, C. D. Newton and D. M. Nunamaker (Eds.) Publisher: International Veterinary Information Service (www.ivis.org), Ithaca, New York, USA. Fracture and Dislocation
Technique Guide. TomoFix Osteotomy System. A comprehensive plating system for stable fixation of osteotomies around the knee.
 Technique Guide TomoFix Osteotomy System. A comprehensive plating system for stable fixation of osteotomies around the knee. Table of Contents Introduction TomoFix Osteotomy System 2 AO Principles 4 Indications
Technique Guide TomoFix Osteotomy System. A comprehensive plating system for stable fixation of osteotomies around the knee. Table of Contents Introduction TomoFix Osteotomy System 2 AO Principles 4 Indications
recovery. Many methods of treatment for fractures of the clavicle had been IJMDS January 2016; 5(1) 991
 991") Original article A clinical study on role of different types of plates in surgical management of middle one third clavicle fracture in adults Garg V 1, Agarwal A 2 ABSTRACT Background: Fractures of the
Original article A clinical study on role of different types of plates in surgical management of middle one third clavicle fracture in adults Garg V 1, Agarwal A 2 ABSTRACT Background: Fractures of the
)394( COPYRIGHT 2017 BY THE ARCHIVES OF BONE AND JOINT SURGERY
394( COPYRIGHT 2017 BY THE ARCHIVES OF BONE AND JOINT SURGERY") )94( COPRIGHT 207 B THE ARCHIVES OF BONE AND JOINT SURGER RESEARCH ARTICLE Functional Results of Unstable (Type 2) Distal Clavicle Fractures Treated with Superior Anterior Locking Plate Rajesh Govindasamy,
)94( COPRIGHT 207 B THE ARCHIVES OF BONE AND JOINT SURGER RESEARCH ARTICLE Functional Results of Unstable (Type 2) Distal Clavicle Fractures Treated with Superior Anterior Locking Plate Rajesh Govindasamy,
Competence of the Deltoid Ligament in Bimalleolar Ankle Fractures After Medial Malleolar Fixation *
 Competence of the Deltoid Ligament in Bimalleolar Ankle Fractures After Medial Malleolar Fixation * BY PAUL TORNETTA, III, M.D. Investigation performed at Kings County Hospital, New York, N.Y. Abstract
Competence of the Deltoid Ligament in Bimalleolar Ankle Fractures After Medial Malleolar Fixation * BY PAUL TORNETTA, III, M.D. Investigation performed at Kings County Hospital, New York, N.Y. Abstract
Technique Guide. LCP Proximal Femoral Hook Plate 4.5/5.0. Part of the LCP Periarticular Plating System.
 Technique Guide LCP Proximal Femoral Hook Plate 4.5/5.0. Part of the LCP Periarticular Plating System. Table of Contents Introduction Features and Benefits 2 AO ASIF Principles 4 Indications 5 Surgical
Technique Guide LCP Proximal Femoral Hook Plate 4.5/5.0. Part of the LCP Periarticular Plating System. Table of Contents Introduction Features and Benefits 2 AO ASIF Principles 4 Indications 5 Surgical
The Orthopaedic Cable System TECHNIQUE GUIDE
 The Orthopaedic Cable System TECHNIQUE GUIDE Original Instruments and Implants of the Association for the Study of Internal Fixation AO ASIF Table of Contents INTRODUCTION Indications.....................................
The Orthopaedic Cable System TECHNIQUE GUIDE Original Instruments and Implants of the Association for the Study of Internal Fixation AO ASIF Table of Contents INTRODUCTION Indications.....................................
NEW INSTRUMENTS FOR INTERNAL FIXATION OF FRACTURES USING MINIMALLY INVASIVE TECHNIQUES
 NEW INSTRUMENTS FOR INTERNAL FIXATION OF FRACTURES USING MINIMALLY INVASIVE TECHNIQUES Dr.eng. Comşa Stanca, sing. Gheorghiu Doina, eng. Ciobota Dan National Institute of Research & Development for fine
NEW INSTRUMENTS FOR INTERNAL FIXATION OF FRACTURES USING MINIMALLY INVASIVE TECHNIQUES Dr.eng. Comşa Stanca, sing. Gheorghiu Doina, eng. Ciobota Dan National Institute of Research & Development for fine
Wright Medical Technology, Inc Cherry Road Memphis, TN
 Wright Medical Technology, Inc. 1023 Cherry Road Memphis, TN 38117 800 238 7117 901 867 9971 www.wmt.com Wright Medical EMEA Atlas Arena, Australia Building Hoogoorddreef 7 1101 BA Amsterdam the Netherlands
Wright Medical Technology, Inc. 1023 Cherry Road Memphis, TN 38117 800 238 7117 901 867 9971 www.wmt.com Wright Medical EMEA Atlas Arena, Australia Building Hoogoorddreef 7 1101 BA Amsterdam the Netherlands
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Disclosure Statement. Acromioclavicular (AC) Joint
 Joint") Michael D. Loeb. M.D. Texas Orthopedics, Sports Medicine, and Rehabilitation Associates, P.A. Austin, Texas Disclosure Statement NO INTERESTS PERTAINING TO INFORMATION GIVEN IN THIS PRESENTATION Acromioclavicular
Michael D. Loeb. M.D. Texas Orthopedics, Sports Medicine, and Rehabilitation Associates, P.A. Austin, Texas Disclosure Statement NO INTERESTS PERTAINING TO INFORMATION GIVEN IN THIS PRESENTATION Acromioclavicular
Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture Dislocation of the Elbow in an Adult
 Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Introduction Basics MIS Screw 2 System Characteristics 2 Indication 2
 Clinical Advisor M. Walther. M.D., Ph.D. Professor of Orthopedic Surgery Head of Department Centre for Foot and Ankle Surgery Schön Klinik München Harlaching FIFA Medical Centre Table of Contents Introduction
Clinical Advisor M. Walther. M.D., Ph.D. Professor of Orthopedic Surgery Head of Department Centre for Foot and Ankle Surgery Schön Klinik München Harlaching FIFA Medical Centre Table of Contents Introduction
Knee Surgical Technique
 Knee Surgical Technique COMPASS Universal Hinge by Jimmy Tucker, M.D. Orthopaedic Surgeon Director, Arkansas Sports Medicine, P.A. Little Rock, Arkansas Table of contents Design features 3 Indications
Knee Surgical Technique COMPASS Universal Hinge by Jimmy Tucker, M.D. Orthopaedic Surgeon Director, Arkansas Sports Medicine, P.A. Little Rock, Arkansas Table of contents Design features 3 Indications
The NBX Non-Bridging External Fixator A Non-Bridging External Fixator/Locking Plate capturing a series of.062mm K-wires and 3mm half-pins that are
 The NBX Non-Bridging External Fixator A Non-Bridging External Fixator/Locking Plate capturing a series of.062mm K-wires and 3mm half-pins that are inserted in a multiplanar and multi-directional fashion
The NBX Non-Bridging External Fixator A Non-Bridging External Fixator/Locking Plate capturing a series of.062mm K-wires and 3mm half-pins that are inserted in a multiplanar and multi-directional fashion
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Comparison between Intramedullary Nailing and Percutaneous K-Wire Fixation for Fractures in the Distal Third of the Metacarpal Bone
 Comparison between Nailing and K-Wire Fixation for Fractures in the Distal Third of the Metacarpal Bone Original Article Sung Jun Moon 1, Jae-Won Yang 2, Si Young Roh 1, Dong Chul Lee 1, Jin Soo Kim 1
Comparison between Nailing and K-Wire Fixation for Fractures in the Distal Third of the Metacarpal Bone Original Article Sung Jun Moon 1, Jae-Won Yang 2, Si Young Roh 1, Dong Chul Lee 1, Jin Soo Kim 1
Practical Reduction Techniques: Diaphyseal Reduction. Philip Wolinsky University of California at Davis Medical Center
 OTA Specialty Day 2016 Practical Reduction Techniques: Diaphyseal Reduction Philip Wolinsky University of California at Davis Medical Center 8:55 am 9:55 am Tips and Tricks: Practical Reduction Techniques
OTA Specialty Day 2016 Practical Reduction Techniques: Diaphyseal Reduction Philip Wolinsky University of California at Davis Medical Center 8:55 am 9:55 am Tips and Tricks: Practical Reduction Techniques
Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4)
") AO Manual of ESIN in children s fractures Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4) Title AO Manual of ESIN in children Subtitle Elastic stable intramedullary nailing (ESIN) Author
AO Manual of ESIN in children s fractures Chapter 4: Forearm 4.3 Forearm shaft fractures, transverse (12-D/4) Title AO Manual of ESIN in children Subtitle Elastic stable intramedullary nailing (ESIN) Author
Physeal injuries of the ankle joint constitute 11% of all
 ORIGINAL ARTICLE Outcome of Physeal and Epiphyseal Injuries of the Distal Tibia With Intra-Articular Involvement Savvas P. Nenopoulos, MD, Vasilios A. Papavasiliou, MD, and Athanasios V. Papavasiliou,
ORIGINAL ARTICLE Outcome of Physeal and Epiphyseal Injuries of the Distal Tibia With Intra-Articular Involvement Savvas P. Nenopoulos, MD, Vasilios A. Papavasiliou, MD, and Athanasios V. Papavasiliou,
Double Engine Orthopedic Bone Nail System Universal Humeral Nail
 Double Engine Orthopedic Bone Nail System ----------- Universal Humeral Nail Surgical Technique Manual Note: The surgical procedures should be performed under the guidance of qualified skilled orthopedic
Double Engine Orthopedic Bone Nail System ----------- Universal Humeral Nail Surgical Technique Manual Note: The surgical procedures should be performed under the guidance of qualified skilled orthopedic
COMPLICATIONS OF BRACHYMETATARSIA REPAIR WITH CALLUS DISTRACTION
 C H A P T E R 4 1 COMPLICATIONS OF BRACHYMETATARSIA REPAIR WITH CALLUS DISTRACTION Michelle L. Butterworth, DPM INTRODUCTION Brachymetatarsia represents one of the best and most useful indications for
C H A P T E R 4 1 COMPLICATIONS OF BRACHYMETATARSIA REPAIR WITH CALLUS DISTRACTION Michelle L. Butterworth, DPM INTRODUCTION Brachymetatarsia represents one of the best and most useful indications for
Surgical Technique. Targeter Systems Overview
 Surgical Technique Targeter Systems Overview PERI-LOC Locked Plating System Targeter Systems Overview Table of contents Product overview... 2 Introduction... 2 Indications... 2 Design features and benefits...
Surgical Technique Targeter Systems Overview PERI-LOC Locked Plating System Targeter Systems Overview Table of contents Product overview... 2 Introduction... 2 Indications... 2 Design features and benefits...
VA-LCP Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle.
 VA-LCP Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Surgical Technique This publication is not intended for distribution
VA-LCP Anterior Clavicle Plate. The anatomically precontoured fixation system with angular stability for clavicle shaft and lateral clavicle. Surgical Technique This publication is not intended for distribution
Surgical Technique. Clavicle Locking Plate
 Surgical Technique Clavicle Locking Plate PERI-LOC Locked Plating System Clavicle Locking Plate Surgical Technique Table of Contents Introduction...2 Indications...3 Plate Features...3 Patient Positioning...4
Surgical Technique Clavicle Locking Plate PERI-LOC Locked Plating System Clavicle Locking Plate Surgical Technique Table of Contents Introduction...2 Indications...3 Plate Features...3 Patient Positioning...4
Biceps Tendon Rupture
 Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about Biceps Tendon Rupture must be made in conjunction with your Physician or a
Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about Biceps Tendon Rupture must be made in conjunction with your Physician or a
Medial circumflex artery Lateral circumflex artery
 Femoral Head Fractures: A Critical But Frequently Missed Injury Susanna C. Spence MD Manickam Kumaravel MBBS University of Texas Health Science Center at Houston Background Femoral head fractures: A complication
Femoral Head Fractures: A Critical But Frequently Missed Injury Susanna C. Spence MD Manickam Kumaravel MBBS University of Texas Health Science Center at Houston Background Femoral head fractures: A complication
PediLoc 3.5mm and 4.5mm Contour Femur Plate Surgical Technique
 PediLoc 3.5mm and 4.5mm Contour Femur Plate Surgical Technique Surgical Technique Contour Femur Plate The technique description herein is made available to the healthcare professional to illustrate the
PediLoc 3.5mm and 4.5mm Contour Femur Plate Surgical Technique Surgical Technique Contour Femur Plate The technique description herein is made available to the healthcare professional to illustrate the