5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
|
|
|
- Derick Norman
- 5 years ago
- Views:
Transcription

1 1
2 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year
3 International Liaison Committee on Resuscitation (ILCOR) American Academy of Paediatrics American Heart Association
4 5-10% of all newborns require some degree of active resuscitation 1-10% of all newborns require assisted ventilation
5
6
7
8 Early application of nasal CPAP: Less intubation Shorter ventilation Less postnatal cortisone administration Intubation and administration of surfactant in the first 30 minutes after birth Immediate intubation in ELBW without prenatal betamethasone prophylaxis
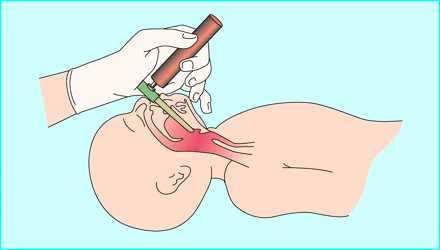
9 Present in 12% of deliveries Suction of the mouth, nose and pharynx after delivery of the head not recommended any longer! Don t stimulate the infant!! Endotracheal suction only for depressed infants (apnoea, bradycardia, hypotony)
10 Defect or hole in the diaphragma that allows the abdominal contents to move into the chest cavity. Treatment is usually surgical
11
12 Anticipated COMMUNICATIONwith obstetricians for risk deliveries At least 1 person solely for care of the infant 1 experienced person must be immediately available
13 At least 2 experienced people 1 person for ventilation, 1 person for circulation A team of3 peopleis desirable (one leader)
14 Question Answer Reaction Number of fetuses? > 1 More staff Gestation? preterm ventilation Drugs? Yes ventilation Amniotic fluid colour? Bleeding? Meconium stained Placental bleeding Suction, intubation Fluids 14
15
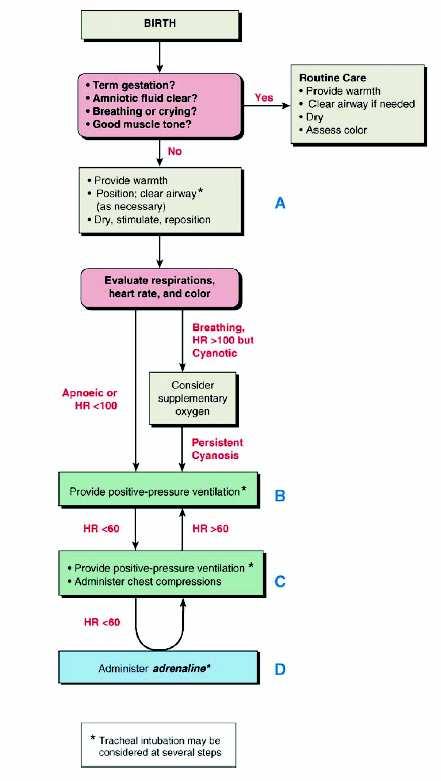
16 Initial evaluation by visual inspection (vitality, meconium, preterm, respiration, colour of skin, ect.) Further assessment based only on: Respiration Heart rate Colour
17 1. Respiration: Gasping or apnoea 2. Heart rate: Stethoscope or umbilical pulsations > 100/min 3. Colour: Central cyanosis Pallor 4.??
18 One of the most important measures reducing neonatal mortality Warm, Draft-free place Heat source (radiant warmer/mother) Rapidly dry the skin and remove wet linen Use of plastic wrapping in preterm infants < 1500g 2 randomised and 3 observational studies
19
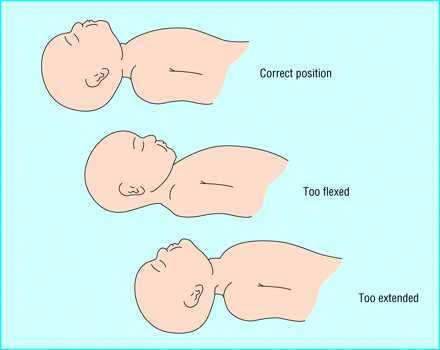
20 Supine or lying on the side Head in a neutral position Correct overextension or flexion (towel under the shoulders)
21 21
22 Vigorous infants don t need suction Before ventilation clear the airway! First mouth, then nose Avoid pharyngeal stimulation in the first minutes after birth Apnoea Bradycardia
23 Drying and suctioning is enough stimulation (20-30 seconds) Secondary stimulation by rubbing the back of flicking the soles If these efforts are not succesful, assume secondary apnoea and ventilate!
24 Increasing evidence that room air is as effective as 100% oxygenin resuscitation of newborn infants Meta-analysis: 100%-O2 vs. room air (Cochrane 2004): Less mortality in the room air-group No detrimental effects 100% Oxygen must be available! The goal is to achieve a normoxaemia! Administer oxygen in the case of persistent, central cyanosis
25 Indications: When after 30 seconds of stimulation the baby presents: Apnoea Gasping respirations Bradycardia < 100/min Persistent cyanosis despite 100% oxygen Most newborns can be ventilated adequately with bag and mask
26 26


27



28 Neopuff TM Ventilation using Neopuff TM
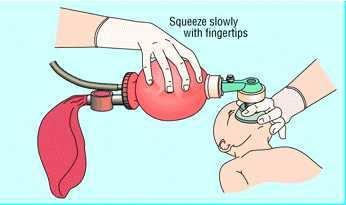
29 Higher pressure and longer inflation time during first breaths Chest expansion and increase in the heart rate are the most reliable signs of adequate ventilation Use a rate of 30-60/min (30-40) Avoid a hypocapnia Utilization of PEEP?
30 Bags should be notlarger than 750 ml Pressure-release valve set at cm H2O Round masks seal better in small preterm infants
31 If the ventilation is not adequate: Check the seal between mask and face Clear airway obstructions Decompress the stomach with a 8F gastric tube
32 Indications: Despite adequate technique, bag-mask ventilation remains ineffective Chest compressions are performed Endotracheal administration of medicaments Special circumstances Meconium aspiration Congenital malformations Extreme immaturity
33 33
34 Intubate orally Calculate the depth of the tube: Weight in kilograms + 6 cm Use a straight blade: Size 0 for preterm infants Size 1 for term infants
35 Check the right position of the tube: Symmetrical chest motion Symmetric breath sounds (axillae) Fog of moisture during exhalation Absence of gastric inflation CO2 measurement in exhaled air
36 Bradycardia is usually the result of hypoxemia! Ventilation is the key therapeutic measure! Chest compressions diminish the effectiveness of ventilation Don t initiate until adequate ventilation is established!
37 General indication: Heart rate < 60/min despite adequate ventilation with for 30 seconds
38 2 thumb-encircling technique seems to be more effective Compress 1/3 of the anterior-posterior diameter of the chest The compression should be shorter than the relaxation

39


40

41


42
43 Avoid simultaneous delivery of compression and ventilation! 3 compressions and then 1 breath 90 compressions and 30 breaths in a minute One second for the inspiration One second for 3 compressions
44 Epinephrine Naloxone Volume expanders Bicarbonate
45 The tracheal route is the most rapidly accessible (epinephrine) Umbilical vein Just under the skin level (blood returns) For all medicaments and volume expanders An intraosseous access can be an alternative
46 Hypoglycaemia in animals with asphyxia is associated with: Higher mortality Larger necrotic area in the brain Clinical studies: Worse neurological outcome in patients with asphyxia and hypoglycaemia In any case of resuscitation try to achieve a normal blood glucose level!
47 No controlled studies in newborn infants Worse neurological outcome in paediatric patients receiving high doses Indications: Bradycardia < 60/min despite 30 seconds of adequate ventilation and chest compressions
48 1 ml = 1 mg (1:1000) Dilute in 10 ml (1ml = 100 µg) (1:10000) Administer µg/kg (0,1-0,3 ml) i.v. Up to 100 µg/kg (1 ml) e.t. Repeat every 3-5 minutes No high doses i.v!
49 Suspect hypovolaemia when the infant doesn't respond to resuscitation No difference between crystalloids and albumine-containing solutions (3 randomised studies in newborn infants with arterial hypotension) Isotonic crystalloid solution (less expensive, less risk) O-neg red blood cells for haemorrhage 10 ml/kg in 5-10 minutes
50 Naloxon can theoretically increase the neurological damage due to asphyxia! Dose: 0.1 mg/kg i.v., s.c., i.m. Short half life!! Contraindicated in recent narcotic abuse of the mother!!
51 Drying (stimulation) always Suctioning secretions if not vital Oxygen if cyanosis is persistent
52 Apnoea HR < 100/min B : Breathing (ventilation) Bag and mask ventilation If ineffective, check the technique Consider endotracheal intubation
53 HR < 60/min C : Circulation Endotracheal intubation as soon as possible Chest compressions
54 HR < 60/min D : Drugs Epinephrine Repeat every 3-5 min, if necessary
55 Neonatal resuscitation Assess Measure Time A: Vital baby? Drying 30s Aspirate B: Apnoea/HF<100 Ventilation 30s C: HR<60 Intubation 30s Chest compressions D: HR<60 Epinephrine every 5 min
56

57 Holand 25ga Japan 21ga Canada 22 ga: parents' request 23-24ga: depending on the birth of newborn 25ga: resuscitation always with the exception of newborns with congenital lethal
58 Local protocols should dictate the procedures Protocols must be regularly reviewed and modified as necessary
59 In patients with borderline survival In patients with high rates of morbidity When the burden to the child is high
60 Ethically equivalent Initiation of resuscitation doesn'tmandate continued support Partial support can worsen the outcome Discontinue after 10 minutes of failed resuscitation
61 In situation in which a very high mortality and an unacceptable prognosis for the few survivors is expected: GA < 23 weeks Birth weight < 400g Proved trisomy 13 or 18 Anencephalia

62 QUESTIONS? 62
63 THANK YOU!! 63
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
 NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني
 Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Neonatal Resuscitation
 Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Table 1: The major changes in AHA / AAP neonatal resuscitation guidelines2010 compared to previous recommendations in 2005
 Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
NRP Raising the Bar for Providers and Instructors
 NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context
 Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal Resuscitation in What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011
 Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
These signs should lead to the administration of high concentrations of
 Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Hypoxic-ischemic encephalopathy (HIE); (cont.) Clinical manifestations; *Intrauterine; growth restriction and increased vascular resistances may be the st manifestation of fetal hypoxia. *During labor;
Resuscitation efforts for Mom & Baby
 Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Steven Ringer MD PhD April 5, 2011
 Steven Ringer MD PhD April 5, 2011 Disclaimer Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter
Steven Ringer MD PhD April 5, 2011 Disclaimer Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE Management, Monitoring & Documentation of a Clinically Significant Cardiopulmonary Event (CSCPE) (NUR47) DATE: REVIEWED: PAGES: 9/09 9/17 1 of 6 PS1094
SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE Management, Monitoring & Documentation of a Clinically Significant Cardiopulmonary Event (CSCPE) (NUR47) DATE: REVIEWED: PAGES: 9/09 9/17 1 of 6 PS1094
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Pediatric Advanced Life Support Overview Judy Haluka BS, RCIS, EMT-P
 Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Protocol for performing chest clearance techniques by nursing staff
 Protocol for performing chest clearance techniques by nursing staff Rationale The main indications for performing chest clearance techniques (CCT) are to assist in the removal of thick, tenacious secretions
Protocol for performing chest clearance techniques by nursing staff Rationale The main indications for performing chest clearance techniques (CCT) are to assist in the removal of thick, tenacious secretions
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
ISPUB.COM. The Use of LMA in Newborn Resuscitation. R Vadhera INTRODUCTION VENTILATION
 ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA
 GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
GUIDELINE PHYSIOLOGY OF BIRTH ASPHYXIA The newborn is not an adult, nor a child. In people of all ages, death can occur from a failure of breathing and / or circulation. The interventions required to aid
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
ILCOR ADVISORY STATEMENT: RESUSCITATION OF THE NEWLY BORN INFANT. An Advisory Statement From the Pediatric Working Group of the
 ILCOR ADVISORY STATEMENT: RESUSCITATION OF THE NEWLY BORN INFANT An Advisory Statement From the Pediatric Working Group of the International Liaison Committee on Resuscitation John Kattwinkel, MD* ; Susan
ILCOR ADVISORY STATEMENT: RESUSCITATION OF THE NEWLY BORN INFANT An Advisory Statement From the Pediatric Working Group of the International Liaison Committee on Resuscitation John Kattwinkel, MD* ; Susan
United States Department of Transportation National Highway Traffic Safety Administration Paramedic: National Standard Curriculum 1
 Neonatology: 1 UNIT TERMINAL OBJECTIVE 6-1.1 At the completion of this unit, the paramedic student will be able to integrate pathophysiological principles and assessment findings to formulate a field impression
Neonatology: 1 UNIT TERMINAL OBJECTIVE 6-1.1 At the completion of this unit, the paramedic student will be able to integrate pathophysiological principles and assessment findings to formulate a field impression
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
CHEST PHYSIOTHERAPY IN NICU PURPOSE POLICY STATEMENTS SITE APPLICABILITY PRACTICE LEVEL/COMPETENCIES. The role of chest physiotherapy in the NICU
 PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
New Zealand Data Sheet. Poractant alfa (Phospholipid fraction of porcine lung) 80 mg/ml
 80 mg/ml") CUROSURF New Zealand Data Sheet Poractant alfa (Phospholipid fraction of porcine lung) 80 mg/ml Presentation Sterile suspension in single-dose vials for intratracheal or intrabronchial administration.
CUROSURF New Zealand Data Sheet Poractant alfa (Phospholipid fraction of porcine lung) 80 mg/ml Presentation Sterile suspension in single-dose vials for intratracheal or intrabronchial administration.
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Scope This guideline is aimed at all Health care professionals involved in the care of infants within the Neonatal Service.
 Management of Newborn Infants born through Meconium-stained liquor University Hospitals of Leicester NHS NHS Trust March 2018 March 2021 Scope This guideline is aimed at all Health care professionals involved
Management of Newborn Infants born through Meconium-stained liquor University Hospitals of Leicester NHS NHS Trust March 2018 March 2021 Scope This guideline is aimed at all Health care professionals involved
Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management. Neonatology. Topics. EMT Paramedic / Critical Refresher Session # 22
 EMT Paramedic / Critical Refresher Session # 22 Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management 1 Neonatology 2 Topics Newborns & Neonates High Risk Newborn Patients APGAR Scoring
EMT Paramedic / Critical Refresher Session # 22 Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management 1 Neonatology 2 Topics Newborns & Neonates High Risk Newborn Patients APGAR Scoring
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
Overview. Chapter 37. Advanced Airway Techniques. Sellick Maneuver 9/11/2012
 Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
PUMANI bcpap GUIDELINES FOR CLINICIANS. An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use
 An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use What is bcpap? bcpap stands for bubble Continuous Positive Airway Pressure. Sometimes called Continuous Distending Pressure,
An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use What is bcpap? bcpap stands for bubble Continuous Positive Airway Pressure. Sometimes called Continuous Distending Pressure,
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Procedure No: Procedure Approved for Use By: WCCSS Divisional Quality Meeting. Date: May 2017
 Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Standard Operating Procedure (SOP): Standard operating procedure for Neonatal Difficult Airway Kit and Intubation Pathway Procedure No: 1 Document replaced: Version 1 Version: 2.0 Procedure Written By:
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Chapter 5 PEDIATRIC RESUSCITATION
 Chapter 5 PEDIATRIC RESUSCITATION Lisa D. Heyden, MD This chapter discusses the 2010 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation and focuses on the resuscitation of pediatric
Chapter 5 PEDIATRIC RESUSCITATION Lisa D. Heyden, MD This chapter discusses the 2010 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation and focuses on the resuscitation of pediatric
Birth Resuscitation. Jon Palmer, VMD, DACVIM New Bolton Center University on Pennsylvania USA
 Birth Resuscitation Jon Palmer, VMD, DACVIM New Bolton Center University on Pennsylvania USA Resuscitation Fetal Resuscitation Intranatal Resuscitation EXIT Procedures Birth Resuscitation Birth Transition
Birth Resuscitation Jon Palmer, VMD, DACVIM New Bolton Center University on Pennsylvania USA Resuscitation Fetal Resuscitation Intranatal Resuscitation EXIT Procedures Birth Resuscitation Birth Transition
Learning Station Competency Checklists
 Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
** SURFACTANT THERAPY**
 ** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
It is important to point out and frequently remind learners that they are expected to complete ALL aspects of a normal assessment.
 Background The purpose of this document is to provide guidelines for faculty on various aspects of patient simulators to be emphasized to learners during orientation. We recommend that every learner be
Background The purpose of this document is to provide guidelines for faculty on various aspects of patient simulators to be emphasized to learners during orientation. We recommend that every learner be
Pedi-Cap CO 2 detector
 Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
Pedi-Cap CO 2 detector Presentation redeveloped for this program by Rosemarie Boland from an original presentation by Johnston, Adams & Stewart, (2006) Background Clinical methods of endotracheal tube
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
And Then There Were Two. Renae Buehner RNC, BSN Avera McKennan Labor and Delivery Unit Supervisor, Lead OB Flight RN
 And Then There Were Two Renae Buehner RNC, BSN Avera McKennan Labor and Delivery Unit Supervisor, Lead OB Flight RN Disclosures I have none She s coming in hot Assisting the maternal patient in a safe
And Then There Were Two Renae Buehner RNC, BSN Avera McKennan Labor and Delivery Unit Supervisor, Lead OB Flight RN Disclosures I have none She s coming in hot Assisting the maternal patient in a safe
EQUIPMENT: Nitrous Oxygen Delivery System:
 Policy: Nitrous Oxide Use in the Intrapartum and Immediate Postpartum Period for Obstetrical Patients in the Family Birth Place Approvers: CEO. CNO, Medical Staff President, Anesthesia Chair, OB Medical
Policy: Nitrous Oxide Use in the Intrapartum and Immediate Postpartum Period for Obstetrical Patients in the Family Birth Place Approvers: CEO. CNO, Medical Staff President, Anesthesia Chair, OB Medical
Pretest. Comprehensive Advanced Life Support: Provider Course
 Pretest Comprehensive Advanced Life Support: Provider Course Please, use the answer sheet provided to record your answers and bring the completed answer sheet to class. Answer sheets will be collected
Pretest Comprehensive Advanced Life Support: Provider Course Please, use the answer sheet provided to record your answers and bring the completed answer sheet to class. Answer sheets will be collected
Non Invasive Ventilation In Preterm Infants. Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid
 Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Orotracheal Intubation
 T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
A retrospective review of tracheal suction at birth in neonates with meconium aspiration syndrome
 A retrospective review of tracheal suction at birth in neonates with meconium aspiration syndrome D. Manickam MBBS, DCH, MRCP, MIAC, Paediatric Department, Penang General Hospital, 10450 Pulau Pinang Summary
A retrospective review of tracheal suction at birth in neonates with meconium aspiration syndrome D. Manickam MBBS, DCH, MRCP, MIAC, Paediatric Department, Penang General Hospital, 10450 Pulau Pinang Summary
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
RESUSCITATION AT BIRTH
 ` 1 VITED ARTICLE RESUSCITATION AT BIRTH R Joseph ABSTRACT Birth asphyxia is frequent and often severe, occurring in about 10% and 1% respectively of all births; in a third it is unexpected. Delivery rooms
` 1 VITED ARTICLE RESUSCITATION AT BIRTH R Joseph ABSTRACT Birth asphyxia is frequent and often severe, occurring in about 10% and 1% respectively of all births; in a third it is unexpected. Delivery rooms
Scope This guideline is aimed at all healthcare professionals involved in the care of infants within the neonatal service.
 UHL Neonatal Guideline: CPAP Nursing Care University Hospitals of Leicester NHS NHS Trust Nov 2018 Nov 2021 Scope This guideline is aimed at all healthcare professionals involved in the care of infants
UHL Neonatal Guideline: CPAP Nursing Care University Hospitals of Leicester NHS NHS Trust Nov 2018 Nov 2021 Scope This guideline is aimed at all healthcare professionals involved in the care of infants
Birth Asphyxia - Summary of the previous meeting and protocol overview
 Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Admission/Discharge Form for Infants Born in Please DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
A SYNOPSIS BY ILCOR PEDIATRIC TASK FORCE. Pediatric Basic Life Support, Pediatric Advanced Life Support and Neonatal Resuscitation 2015
 Vol. 2 - No.4 October - December 2015 83 Vol. 2 - No.4 October - December 2015 84 There is new evidence that when treating pediatric septic shock in specific settings, the use of restricted volume of isotonic
Vol. 2 - No.4 October - December 2015 83 Vol. 2 - No.4 October - December 2015 84 There is new evidence that when treating pediatric septic shock in specific settings, the use of restricted volume of isotonic
Newborn Life Support. NLS guidance.
 Kelly Harvey, ANNP NWNODN, previously Wythenshawe Hospital has shared this presentation with the understanding that it is for personal use following your attendance at the 8th Annual Senior Neonatal Nursing
Kelly Harvey, ANNP NWNODN, previously Wythenshawe Hospital has shared this presentation with the understanding that it is for personal use following your attendance at the 8th Annual Senior Neonatal Nursing
Module 2: Facilitator instructions for Airway & Breathing Skills Station
 Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) NICU POCKET GUIDE
 NICU POCKET GUIDE") Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Vital Signs and Oxygen Administration
 Vital Signs and Oxygen Administration By Dr. Mohsen Dashti Patient Care and Management (202) May-9-2010 Vital Signs and Oxygen Administration What are the vital signs? Why do we need to know them? How
Vital Signs and Oxygen Administration By Dr. Mohsen Dashti Patient Care and Management (202) May-9-2010 Vital Signs and Oxygen Administration What are the vital signs? Why do we need to know them? How
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation