SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
|
|
|
- Georgia Booth
- 5 years ago
- Views:
Transcription
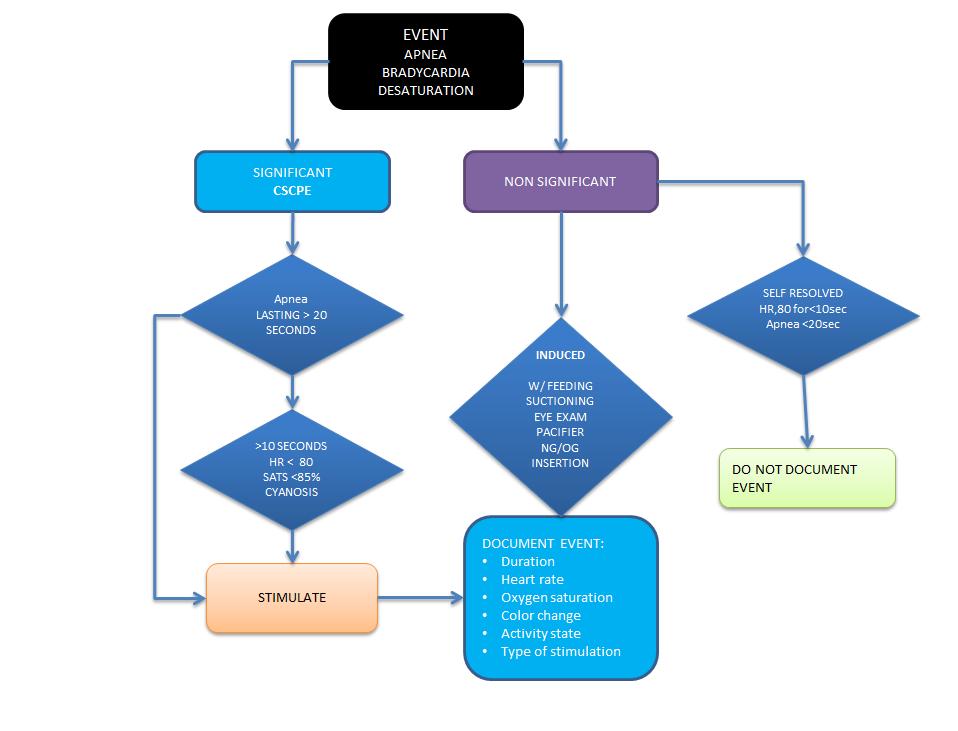
1 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE Management, Monitoring & Documentation of a Clinically Significant Cardiopulmonary Event (CSCPE) (NUR47) DATE: REVIEWED: PAGES: 9/09 9/17 1 of 6 PS1094 ISSUED FOR: RESPONSIBILITY: RN, LPN, MST Neonatal Nursing PURPOSE: DEFINITIONS: To provide a process for management, monitoring, treatment and documentation of clinically significant cardiopulmonary events in infants in the Neonatal Intensive Care Unit (NICU). Clinically Significant Cardiopulmonary Event (CSCPE): 1. An apneic event > = 20 seconds 2. An apneic event < 20 seconds accompanied by a bradycardia < 80 bpm for any duration 3. An apneic event < 20 seconds with desaturation <85% or accompanied by central cyanosis for any duration 4. A bradycardia < 80 bpm for > 10 seconds 5. Oxygen desaturation < 85% or central cyanosis for >10 seconds ( if no pulse oximeter was being used) Induced Significant Cardiopulmonary Event Events that occur during procedures such as, but are not limited to suctioning, eye exams, feedings, OG/NG insertions or events that are pacifier related. Events requiring vigorous stimulation document as CSCPE. Do not document self-resolved events with HR <80 for < 10 sec. for Apnea <20 sec. Apnea: A respiratory pause 20 seconds Bradycardia: Heart rate less than 80 bpm for more than 10 seconds. The lowest heart rate should be recorded. Desaturation: SpO 2 <85% for at least 10 seconds. The lowest SpO 2 should be recorded.
2 Periodic Breathing: A series of 3 or more respiratory pauses per minute longer than 3 seconds with intervals of respiration between pauses. This pattern of breathing is common in newborns and is usually not associated with significant bradycardia or desaturation. The term is only used when there is no significant bradycardia or desaturation. Stimulation: Gentle: Infant responds immediately to gentle strokes on body, repositioning or removal of pacifier Moderate: Infant responds to rubbing of the back, trunk or extremities, and/or flicking soles of the feet. Vigorous: Infant requires blow by oxygen, positive pressure ventilation or use of resuscitative drugs. PROCEDURE: Management of Infants with Apnea of Prematurity All infants less than 35 weeks 0 days gestation will be monitored on a cardiorespiratory monitor after birth until risk for developing apnea of prematurity is assessed. Infants > 35 weeks with history of duskiness should have pulse oximetry monitoring for minimum of 48 hours. Any changes to the procedure must be ordered by the physician. Pulse oximetry monitoring should continue until infant is consistently PO feeding > 75% of his/her feedings in 24 hours AND is free of CSCPE for a minimum of 7 days off caffeine therapy. If the infant has frequent episodes of CSCPE, a full clinical examination should be conducted including assessment of airway patency, thermal stability, blood pressure, glucose regulation and other potential causes of apnea.
3 While monitored, infants may be positioned prone, side-lying or supine, maintaining the infant s head in a neutral position. The cardiorespiratory monitor should be set with a 20-second apnea delay. Maintain the infant in a thermal neutral environment. Treatment options for CSCPE include medications, usually caffeine, nasal CPAP, Vapotherm or intubation. Responding to Monitor Alarms When the monitor alarms, the infant should initially be evaluated (observed) for respiratory movements, color, and heart rate. Assess the infant for hyperextension or flexion of the neck. This may cause or contribute to apnea/bradycardia. Reposition the head and neck if necessary. Maintain the head and neck in a neutral position. If the infant has a CSCPE appropriate tactile stimulation should be initiated. Positive pressure ventilation (PPV) should be administered if the infant does not respond to tactile stimulation and/or repositioning within 30 seconds. Do not continue to stimulate a baby who is not breathing within 30 seconds. Provide gentle ventilation for a few breaths with a ventilation bag (self-inflating or T-piece resuscitator) and face mask or until infant recovers effective respiration. Avoid vigorous manual ventilation as it may adversely affect the infant s CO2 level. The PPV should be set at the same oxygen level as the baby is otherwise requiring. Continue PPV if required until regular respiration, normal heart rate and color have returned.
4 Reassess respiratory effort, heart rate and oxygen saturation after 30 seconds of PPV if it is required for that length of time. Oxygen should be increased only if the baby does not improve after 30 seconds of PPV. DOCUMENTATION: Do Record On the Flowsheet: Any CSCPE and Induced CSCPE as defined above should be recorded under the CSCPE header in the Vital Signs Flowsheets. The duration of the episode should be from the time the monitor goes off and is confirmed by the nurse s assessment to be true until the episode resolves. Documentation should include duration, heart rate, oxygen saturation, color change, activity state and type of stimulation. DO NOT RECORD: Self-resolved events. Episodes of periodic breathing or respiratory pauses <20 seconds that are not associated with significant bradycardia or desaturation. Episodes related to monitor artifact. (events that were not witnessed should be checked in event review) Episodes of bradycardia that are self-resolved within 10 seconds and are not associated with a desaturation below 80% or respiratory pause. REFERENCE: 1. AAP, POLICY STATEMENT: Apnea, Sudden Infant Death Syndrome, and Home Monitoring. Committee on Fetus and Newborn. PEDIATRICS Vol. 111 No. 4 April 2003, pp Alvaro, R. MD. Apnea of Prematurity& Bradycardia (Cardiorespiratory Events): Management, Monitoring & Documentation Procedure, University of Manitoba, Neonatal Manual, Stokowski, L.A. A Primer on Apnea of the Prematurity. Advances in Neonatal Care:
5 June Volume 5 - Issue 3 - p Butler, T. Jeffrey, MD, Kimberly S. Firestone, BS, RRT, Jennifer L. Grow, MD, and Anand D. Kantak, MD. Standardizing Documentation and the Clinical Approach to Apnea of Prematurity Reduces Length of Stay, Improves Staff Satisfaction, and Decreases Hospital Cost. The Joint Commission Journal on Quality and Patient Safety 40.6(2014): Print. 5. Alere Neonatal Clinical Management Guidelines. 8th Edition. REVIEWING AUTHOR (S): Heike Bucken RNC-NCC,CLC, NICU Clinical Coordinator Kathy Duffy RRT, Respiratory Therapy Lisa Biach RNC-NCC,CBC, NICU Discharge Coordinator Heather Graber RNC-NCC, CBC NICU Clinical Manager
6
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia Main cause of perinatal and neonatal
MODULE VII. Delivery and Immediate Neonatal Care
 MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
MODULE VII Delivery and Immediate Neonatal Care NEONATAL ASPHYXIA About one million deaths per year In Latin America 12% of newborns suffer some degree of asphyxia A major cause of perinatal and neonatal
 NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
NEONATAL LIFE SUPPORT PROVIDER (NLSP) CERTIFICATION EXAMINATION 1. To determine if an infant requires resuscitation, you must rapidly assess gestation period, presence of meconium in amniotic fluid, breaths
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context
 Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
Addendum to the NRP Provider Textbook 6 th Edition Recommendations for specific modifications in the Canadian context A subcommittee of the Canadian Neonatal Resuscitation Program (NRP) Steering Committee
NRP Raising the Bar for Providers and Instructors
 NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
NRP 2011 Raising the Bar for Providers and Instructors What is the same? 1. Minimum course requirement is Lessons 1 through 4 and Lesson 9. The NRP Provider Card requires renewal every 2 years. Your facility
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني
 Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Lecture 6 PROFESSOR DR. NUMAN NAFIE HAMEED الاستاذ الدكتور نعمان نافع الحمداني Neonatal Resuscitation Program (NRP) 2010 MCQ? In neonatal resuscitation program, the preterm neonates need special preparations
Neonatal Resuscitation in What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011
 Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
Neonatal Resuscitation in 2011- What is new? How did we get here? Steven Ringer MD PhD Harvard Medical School May 25, 2011 Conflicts I have no actual or potential conflict of interest in relation to this
Resuscitation efforts for Mom & Baby
 Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Resuscitation efforts for Mom & Baby Beth Ann Clayton, CRNA, MS AmSol Obstetric Anesthesia CRNA Educator Obstetric Anesthesia Clinical Coordinator Mercy Health-Fairfield Hospital Assistant Professor, University
Table 1: The major changes in AHA / AAP neonatal resuscitation guidelines2010 compared to previous recommendations in 2005
 Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Steven Ringer MD PhD April 5, 2011
 Steven Ringer MD PhD April 5, 2011 Disclaimer Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter
Steven Ringer MD PhD April 5, 2011 Disclaimer Mead Johnson sponsors programs such as this to give healthcare professionals access to scientific and educational information provided by experts. The presenter
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Home Cardiorespiratory Monitoring. Description. Section: Durable Medical Equipment Effective Date: April 15, 2017
 Subject: Home Cardiorespiratory Monitoring Page: 1 of 9 Last Review Status/Date: March 2017 Home Cardiorespiratory Monitoring Description Home cardiorespiratory monitors track respiratory effort and heart
Subject: Home Cardiorespiratory Monitoring Page: 1 of 9 Last Review Status/Date: March 2017 Home Cardiorespiratory Monitoring Description Home cardiorespiratory monitors track respiratory effort and heart
Research in Medical Physics: Physiological Signals and Dynamics
 Research in Medical Physics: Physiological Signals and Dynamics Incidents of apnea or of sepsis create critical situations in a neonatal intensive care unit (NICU). Of the 4.2 million babies born annually
Research in Medical Physics: Physiological Signals and Dynamics Incidents of apnea or of sepsis create critical situations in a neonatal intensive care unit (NICU). Of the 4.2 million babies born annually
5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
 1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
Name and title of the investigators responsible for conducting the research: Dr Anna Lavizzari, Dr Mariarosa Colnaghi
 Protocol title: Heated, Humidified High-Flow Nasal Cannula vs Nasal CPAP for Respiratory Distress Syndrome of Prematurity. Protocol identifying number: Clinical Trials.gov NCT02570217 Name and title of
Protocol title: Heated, Humidified High-Flow Nasal Cannula vs Nasal CPAP for Respiratory Distress Syndrome of Prematurity. Protocol identifying number: Clinical Trials.gov NCT02570217 Name and title of
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE VENTILATION FOR THE Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: Director, Respiratory Care Services 126.685 (neo) 3/26/15
PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE VENTILATION FOR THE Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: Director, Respiratory Care Services 126.685 (neo) 3/26/15
Introduce the basics of the newborn resuscitation period Practice calculations for TPN orders Learn how to manage basic ventilator settings
 Introduce the basics of the newborn resuscitation period Practice calculations for TPN orders Learn how to manage basic ventilator settings Complex concepts you may be expected to know Not taught this
Introduce the basics of the newborn resuscitation period Practice calculations for TPN orders Learn how to manage basic ventilator settings Complex concepts you may be expected to know Not taught this
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Apnea in the Newborn
 Apnea in the Newborn Developed by - Lisa Fikac, RNC-NIC, MSN Original Author - Stacey Cashwell, MSN, RN Expiration Date - 1/27/17 This continuing education activity is provided by Cape Fear Valley Health
Apnea in the Newborn Developed by - Lisa Fikac, RNC-NIC, MSN Original Author - Stacey Cashwell, MSN, RN Expiration Date - 1/27/17 This continuing education activity is provided by Cape Fear Valley Health
What s new in neonatal resuscitation?
 What s new in neonatal resuscitation? Anup Katheria, M.D. Director, Neonatal Research Institute Sharp Mary Birch Hospital for Women & Newborns Disclosures I have no financial Disclosures. Overview Delivery
What s new in neonatal resuscitation? Anup Katheria, M.D. Director, Neonatal Research Institute Sharp Mary Birch Hospital for Women & Newborns Disclosures I have no financial Disclosures. Overview Delivery
Non-Invasive Monitoring
 Grey Nuns and Misericordia Community Hospital Approved by: Non-Invasive Monitoring Neonatal Policy & Procedures Manual : Assessment : Oct 2015 Date Effective Oct 2015 Gail Cameron Senior Director Operations,
Grey Nuns and Misericordia Community Hospital Approved by: Non-Invasive Monitoring Neonatal Policy & Procedures Manual : Assessment : Oct 2015 Date Effective Oct 2015 Gail Cameron Senior Director Operations,
Oxygen Delivery. Purpose. Policy Statement. Applicability
 Approved by: Oxygen Delivery Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual Policy
Approved by: Oxygen Delivery Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual Policy
NEONATOLOGY Healthy newborn. Neonatal sequelaes
 NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
NEONATOLOGY Healthy newborn. Neonatal sequelaes Ágnes Harmath M.D. Ph.D. senior lecturer 11. November 2016. Tasks of the neonatologist Prenatal diagnosed condition Inform parents, preparation of necessary
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Maria Tracey, Director-Perioperative and Elaine Warren, Directory-Surgery Level. III (Three)
") PAGE 1/6 MANAGEMENT OF ADULT SURGICAL CLIENTS WITH KNOWN OR SUSPECTED OBSTRUCTIVE SLEEP APNEA (OSA) Patient Care Issuing Authority Dr. James Flynn, Clinical Chief Surgical Services (Perioperative) Signed
PAGE 1/6 MANAGEMENT OF ADULT SURGICAL CLIENTS WITH KNOWN OR SUSPECTED OBSTRUCTIVE SLEEP APNEA (OSA) Patient Care Issuing Authority Dr. James Flynn, Clinical Chief Surgical Services (Perioperative) Signed
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Non Invasive Ventilation In Preterm Infants. Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid
 Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
AEROSURF Phase 2 Program Update Investor Conference Call
 AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
Emergency Department Guideline. Procedural Sedation and Analgesia Policy for the Registered Nurse
 Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
And Then There Were Two. Renae Buehner RNC, BSN Avera McKennan Labor and Delivery Unit Supervisor, Lead OB Flight RN
 And Then There Were Two Renae Buehner RNC, BSN Avera McKennan Labor and Delivery Unit Supervisor, Lead OB Flight RN Disclosures I have none She s coming in hot Assisting the maternal patient in a safe
And Then There Were Two Renae Buehner RNC, BSN Avera McKennan Labor and Delivery Unit Supervisor, Lead OB Flight RN Disclosures I have none She s coming in hot Assisting the maternal patient in a safe
Administrative Policies and Procedures. Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916
 Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Medically Fragile Children (Chapter 2)
") Medically Fragile Children (Chapter 2) Birth to three programs classify children with delays as those who have either established risk or are at risk Established risk infants are those with Genetic disorders
Medically Fragile Children (Chapter 2) Birth to three programs classify children with delays as those who have either established risk or are at risk Established risk infants are those with Genetic disorders
OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General
![OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General](/thumbs/85/91909911.jpg "OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General") OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Prophylactic Aminophylline for Prevention of Apnea at Higher-Risk Preterm Neonates
 Iran Red Crescent Med J. 2014 August; 16(8): e12559. Published online 2014 August 5. DOI: 10.5812/ircmj.12559 Research Article Prophylactic Aminophylline for Prevention of Apnea at Higher-Risk Preterm
Iran Red Crescent Med J. 2014 August; 16(8): e12559. Published online 2014 August 5. DOI: 10.5812/ircmj.12559 Research Article Prophylactic Aminophylline for Prevention of Apnea at Higher-Risk Preterm
10/13/2017. Newborn Care. Objectives. Cardiac Anatomy. Managing Transitional Physiology
 Newborn Care Managing Transitional Physiology Mary Coughlin MS, NNP, RNC-E President and Founder Caring Essentials Collaborative Boston, MA Objectives Upon completion of the learning session participants
Newborn Care Managing Transitional Physiology Mary Coughlin MS, NNP, RNC-E President and Founder Caring Essentials Collaborative Boston, MA Objectives Upon completion of the learning session participants
COMPARISON OF THE EFFICIENCY OF CAFFEINE VERSUS AMINOPHYLLINE FOR THE TREATMENT OF APNOEA OF PREMATURITY
 CASE STUDIES COMPARISON OF THE EFFICIENCY OF CAFFEINE VERSUS AMINOPHYLLINE FOR THE TREATMENT OF APNOEA OF PREMATURITY Gabriela Ildiko Zonda 1, Andreea Avasiloaiei 1, Mihaela Moscalu 2, Maria Stamatin 1
CASE STUDIES COMPARISON OF THE EFFICIENCY OF CAFFEINE VERSUS AMINOPHYLLINE FOR THE TREATMENT OF APNOEA OF PREMATURITY Gabriela Ildiko Zonda 1, Andreea Avasiloaiei 1, Mihaela Moscalu 2, Maria Stamatin 1
(C) The following criteria must be met for coverage of an apnea monitor:
 The following criteria must be met for coverage of an apnea monitor:") ACTION: Final DATE: 07/02/2018 10:05 AM 5160-10-09 Apnea monitors. TO BE RESCINDED (A) Definitions. (1) "Apnea monitors" are defined as cardiorespiratory monitoring devices capable of providing continuous
ACTION: Final DATE: 07/02/2018 10:05 AM 5160-10-09 Apnea monitors. TO BE RESCINDED (A) Definitions. (1) "Apnea monitors" are defined as cardiorespiratory monitoring devices capable of providing continuous
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
FANNP 28TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW OCTOBER 17-21, 2017
 Pulse Oximetry in the Delivery Room: Principles and Practice GS2 3 Jonathan P. Mintzer, MD, FAAP Assistant Professor of Pediatrics Stony Brook Children s Hospital, Division of Neonatal-Perinatal Medicine,
Pulse Oximetry in the Delivery Room: Principles and Practice GS2 3 Jonathan P. Mintzer, MD, FAAP Assistant Professor of Pediatrics Stony Brook Children s Hospital, Division of Neonatal-Perinatal Medicine,
1st Annual Clinical Simulation Conference
 1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
ACoRN Workbook 2010 Update
 ACoRN Neonatal Society Société néonatale ACoRN A Canadian non-profit Society Vancouver, British Columbia www.acornprogram.net ACoRN Workbook 2010 Update Name: ACoRN Acute Care of at-risk Newborns The ACoRN
ACoRN Neonatal Society Société néonatale ACoRN A Canadian non-profit Society Vancouver, British Columbia www.acornprogram.net ACoRN Workbook 2010 Update Name: ACoRN Acute Care of at-risk Newborns The ACoRN
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
Pediatric CPR. Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY
 Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
ACoRN Workbook 2012 Update
 ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
ACoRN Neonatal Society Société néonatale ACoRN www.acornprogram.net A Canadian non-profit Society Vancouver, British Columbia ACoRN Workbook 2012 Update Name: The ACoRN Process The Resuscitation Sequence
Dr. AM MAALIM KPA 2018
 Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
hour pneumogram and on the incidence of clinically important apnoea. Subjects and methods
 Archives of Disease in Childhood, 1986, 61, 891-895 Effect of caffeine of infancy on pneumogram and apnoea M ANWAR, H MONDESTIN, N MOJICA, R NOVO, M GRAFF, M HIATIT, AND T HEGYI Department of Pediatrics,
Archives of Disease in Childhood, 1986, 61, 891-895 Effect of caffeine of infancy on pneumogram and apnoea M ANWAR, H MONDESTIN, N MOJICA, R NOVO, M GRAFF, M HIATIT, AND T HEGYI Department of Pediatrics,
Procedural Sedation. Conscious Sedation AAP Sedation Guidelines: Disclosures. What does it mean for my practice? We have no disclosures
 2016 AAP Sedation Guidelines: What does it mean for my practice? Amber P. Rogers MD FAAP Assistant Professor of Section of Hospital Medicine and Anesthesiology Corrie E. Chumpitazi MD FAAP FACEP Assistant
2016 AAP Sedation Guidelines: What does it mean for my practice? Amber P. Rogers MD FAAP Assistant Professor of Section of Hospital Medicine and Anesthesiology Corrie E. Chumpitazi MD FAAP FACEP Assistant
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) NICU POCKET GUIDE
 NICU POCKET GUIDE") Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Carole Wegner RN, MSN And Lori Leiser CRT
 Airway Clearance Carole Wegner RN, MSN And Lori Leiser CRT Topics Suctioning and suctioning equipment Medications to facilitate t airway clearance Bronchial hygiene modalities Preparing for suctioning
Airway Clearance Carole Wegner RN, MSN And Lori Leiser CRT Topics Suctioning and suctioning equipment Medications to facilitate t airway clearance Bronchial hygiene modalities Preparing for suctioning
Neonatal Resuscitation
 Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Neonatal Resuscitation High Risk Deliveries A person trained in neonatal resuscitation is usually called to be present for the following deliveries: 1. Antepartum factors Maternal diabetes Pregnancy induced
Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; 10/09; 10/10 Manual of Administrative Policy Source Sedation Committee
 Code No. 711 Section Subject Moderate Sedation (formerly termed Conscious Sedation ) Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; Manual of Administrative Policy Source
Code No. 711 Section Subject Moderate Sedation (formerly termed Conscious Sedation ) Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; Manual of Administrative Policy Source
MASTER SYLLABUS
 MASTER SYLLABUS 2018-2019 A. Academic Division: Health Science B. Discipline: Respiratory Care C. Course Number and Title: RESP 2490 Practicum IV D. Course Coordinator: Tricia Winters, BBA, RRT, RCP Assistant
MASTER SYLLABUS 2018-2019 A. Academic Division: Health Science B. Discipline: Respiratory Care C. Course Number and Title: RESP 2490 Practicum IV D. Course Coordinator: Tricia Winters, BBA, RRT, RCP Assistant
Management of Upper Airway Obstruction in Pierre Robin Sequence
 Management of Upper Airway Obstruction in Pierre Robin Sequence South Wales Cleft Team Pierre Robin Sequence Triad of cleft palate, micrognathia and airway obstruction was described by St Hilaire in 1822,
Management of Upper Airway Obstruction in Pierre Robin Sequence South Wales Cleft Team Pierre Robin Sequence Triad of cleft palate, micrognathia and airway obstruction was described by St Hilaire in 1822,
SARASOTA MEMORIAL HOSPITAL
 SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE EXCHANGE TRANSFUSION OF THE INFANT Nursing Neonatal Services DATE: REVIEWED: PAGES: 2/88 2/18 1 of 8 RESPONSIBILITY: RN Neonatal Services
SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE EXCHANGE TRANSFUSION OF THE INFANT Nursing Neonatal Services DATE: REVIEWED: PAGES: 2/88 2/18 1 of 8 RESPONSIBILITY: RN Neonatal Services
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management
 yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
CHEST PHYSIOTHERAPY IN NICU PURPOSE POLICY STATEMENTS SITE APPLICABILITY PRACTICE LEVEL/COMPETENCIES. The role of chest physiotherapy in the NICU
 PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
Therapist Written RRT Examination Detailed Content Outline
 I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
Pulse Oximetry Test: Summary Report
 Test Condition : Overnight on Room Air Pulse Oximetry Test: Summary Report Patient Information Referring/Ordering Physician DME/HME Courier John Sample Insurance ID : 123456789B DOB : 1/1/1909 Gender :
Test Condition : Overnight on Room Air Pulse Oximetry Test: Summary Report Patient Information Referring/Ordering Physician DME/HME Courier John Sample Insurance ID : 123456789B DOB : 1/1/1909 Gender :
Application of tactile/kinesthetic stimulation in preterm infants: a systematic review
 Application of tactile/kinesthetic stimulation in preterm infants: a systematic review Euro Health Care and Fitness Summit 2015 Valencia, Spain Vanessa Pepino J Pediatr (Rio J). 2015; 91(3):213-223 About
Application of tactile/kinesthetic stimulation in preterm infants: a systematic review Euro Health Care and Fitness Summit 2015 Valencia, Spain Vanessa Pepino J Pediatr (Rio J). 2015; 91(3):213-223 About
Stabilization of the Newborn for Transport. Relevant Disclosure. Learning Objectives
 Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
Stabilization of the Newborn for Transport Arlen Foulks, DO FAAP FACOP Medical Director, CCMH Level II NICU Medical Director, NeoFlight Assistant Professor of Pediatrics Neonatal Perinatal Medicine Section,
QUICK REFERENCE GUIDE CAPNOGRAPHY DURING PROCEDURAL SEDATION
 QUICK REFERENCE GUIDE CAPNOGRAPHY DURING PROCEDURAL SEDATION Changes in capnography values and waveforms may help clinicians understand a patient s level of comfort, sedation, and respiratory function
QUICK REFERENCE GUIDE CAPNOGRAPHY DURING PROCEDURAL SEDATION Changes in capnography values and waveforms may help clinicians understand a patient s level of comfort, sedation, and respiratory function
Sonoma Valley Hospital Sonoma Valley Healthcare District Policy and Procedure Organizational. Page: 1
 Title: PAIN MANAGEMENT Sonoma Valley Hospital Organizational Number: PC-104 Page: 1 Effective Date: 3/96 Mary Kelly, R.N., M.P.A. 12/07 Approved By Date Revision Dates: 07/01, 02/02 Signature on file Signature
Title: PAIN MANAGEMENT Sonoma Valley Hospital Organizational Number: PC-104 Page: 1 Effective Date: 3/96 Mary Kelly, R.N., M.P.A. 12/07 Approved By Date Revision Dates: 07/01, 02/02 Signature on file Signature
Chapter 10. Objectives. Objectives 01/09/2013. Airway Management, Artificial Ventilation, and Oxygenation
 Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
DEEP SEDATION TEST QUESTIONS
 Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
ARTIFICIAL INTELLIGENCE FOR PREDICTION OF SEPSIS IN VERY LOW BIRTH WEIGHT INFANTS
 ARTIFICIAL INTELLIGENCE FOR PREDICTION OF SEPSIS IN VERY LOW BIRTH WEIGHT INFANTS Markus Leskinen MD PhD, Neonatologist Children s Hospital, University of Helsinki and Helsinki University Hospital The
ARTIFICIAL INTELLIGENCE FOR PREDICTION OF SEPSIS IN VERY LOW BIRTH WEIGHT INFANTS Markus Leskinen MD PhD, Neonatologist Children s Hospital, University of Helsinki and Helsinki University Hospital The
ISPUB.COM. The Use of LMA in Newborn Resuscitation. R Vadhera INTRODUCTION VENTILATION
 ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
ISPUB.COM The Internet Journal of Anesthesiology Volume 1 Number 4 The Use of LMA in Newborn Resuscitation R Vadhera Citation R Vadhera. The Use of LMA in Newborn Resuscitation. The Internet Journal of
Sleep and Neuromuscular Disease. Sharon De Cruz, MD Tisha Wang, MD
 Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
5/3/2012. Goals and Objectives HFNC. High-Flow Oxygen Therapy: Real Benefit or Just a Fad?
 High-Flow Oxygen Therapy: Real Benefit or Just a Fad? Timothy R. Myers MBA, RRT-NPS Director, Women s & Children s Respiratory Care & Procedural Services and Pediatric Heart Center Rainbow Babies & Children
High-Flow Oxygen Therapy: Real Benefit or Just a Fad? Timothy R. Myers MBA, RRT-NPS Director, Women s & Children s Respiratory Care & Procedural Services and Pediatric Heart Center Rainbow Babies & Children