Pediatric Infections: Treatment of Resistant Pathogens. Focus : MRSA and DRSP Infections, Including Pneumonia. Blaise L. Congeni M.D.
|
|
|
- Gerald Nichols
- 6 years ago
- Views:
Transcription
1 Pediatric Infections: Treatment of Resistant Pathogens Focus : MRSA and DRSP Infections, Including Pneumonia Blaise L. Congeni M.D.
2 Patient 1-LP 8 yo with 8 days of fever and 6 days of cough. She had consistently demonstrated fever of about 102. Because of worsening cough and persistent fever the patient was given ceftriaxone and then cefdinir. Because of failure to improve the pt. was admitted.

3

4

5

6
7 Patient HPI 16 y/o male, with PMH of exerciseinduced asthma, ADHD, and Asperger syndrome, presents with 4 day hx of SOB. Associated with pressure-like pain in chest and back, worsening with inspiration. Denies fevers, sick contacts, change in asthma sx. ROS positive for nonproductive cough, decreased appetite and possible 5# wt loss over 2-3 weeks PTA
8 Exam and Labs Vitals: 36.2 P66 R18 BP117/40 100% 2L Exam: In NAD, Resp are easy and nonlabored, No rales or rhonchi, no wheezes, S1S2 RRR, no murmurs noted, nailbeds are pink, no pain to palpation of chest Labs: WBC 5.2 with normal diff, ESR 22 CRP 2.74 CXR: WNL O2 was weaned, pt did well
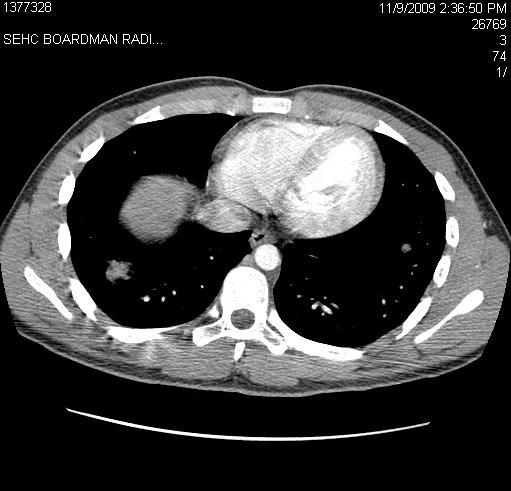
9 Chest CT
10 5 days later Pt is seen by PCP for new onset fever with Tmax 102, left hip/thigh pain, frontal pressure HA that is nonradiating and not associated with N/V, photophobia. Elevated liver enzymes on lab, so a CT of abdomen and pelvis were ordered.

11

12 Case of Severe CAP 30 y/o female presents to ER at 0400 with acute fever, cough, dyspnea; recent viral syndrome Severely hypoxic Requires immediate intubation Treated with 3 rd Gen Ceph +

13 Case of Severe CAP Gram stain of ET aspirate reveals GPC in clusters Vancomycin added Patient has multiorgan dysfunction; expires at 1600 CO- MRSA isolated PVL +
14 Community Acquired Pneumonia Akron Children s Guidelines Early, appropriate antibiotic therapy/optimizes clinical outcomes 2. Customized, effective DX & RX strategies must be based on best available evidence 3. Minimizing diagnostic and therapeutic variability is an important goal of guidelines 4. The target population for theses guidelines are: a) Non neonates (>30 of age) b) Immunocompetent c) Immunizations up to date 5. Mycoplasma should be suspected in moderately ill school aged/adolescent patients Draft: many thanks to committee, esp MF and JB
15 No Toxic Appearing (DX) Yes=(Severe Sepsis) Recommended O Optional Θ Not Recommended CXR CBC SpO2 APR* BCX* Rapid Viral Θ Θ O Θ Θ O F/U radiographs not routinely recommended O Suspected Bacterial Pathogen Especially if a. failed b. disease progression Early influenza RX independent of negative rapid result If rapid positive, consider limiting ABX use Suspected mycoplasma (school aged or adolescent) consider Macrolide Toxic Appearing (TX) No 1. Amoxicillin consider Macrolide APR=Acute Phase Reactants PCX=Blood Cx PPE=Parapneumonic Effusion Yes 1. Ceftriaxone MG/KG/day -Consider Azithromycin for school age/adolescent -Consider Vancomycin if: a. 3-6 months b. pneumatocele c. suspected influenza d. sputum/cx suspected staph e. Parapneumonic effusion
16 2010 Antibiogram ORGANISM ANTIBIOTIC Total Streptococcus Pneumoniae Total= 99 Penicillin Ceftriaxone Erythromycin Clindamycin Tetracycline Ofloxacin Vancomycin Sensitive % Intermediate % Resistant % % 80.6% 47.9% 59.6% 62.2% 92.9% 100.0% % 17.3% 0.0% 0.0% 2.0% 6.1% 0.0% % 2.0% 52.1% 40.4% 35.7% 1.0% 0.0%
17 Therapy of S. pneumo Focus: CAP and DRSP Use third generation ceph if local epidemiology documents high-level pen resistance, or life-threatening dis. For oral therapy, amox PK/PD, tolerability more favorable than pen. To cover possibility of RRSP, (MIC-2), use 90 mg/kg/d (3 doses). No oral ceph provides comparable activity to HD amox.
18 Therapy of S. pneumo Focus: CAP and DRSP Significant macrolide resistance is seen in currently available macrolides. For patients with non-serious allergic reactions to amoxicillin, treatment is not well defined, and should be individualized. For more serious allergies treatment options include linezolid, a macrolide, (up to 40% R), or clindamycin.
19 Therapy of S. pneumo Focus: IV amp v ceftriaxone. Ceftriaxone and cefotaxime are substantially more active in vitro than Pne G. Ceftriaxone has been documented to be effective in adults with ceftriaxone R strains. Although no prospective studies exist, iv amp appears as effective as IV ceftriaxone for strains with MICs up to 2 µg/ml.
20

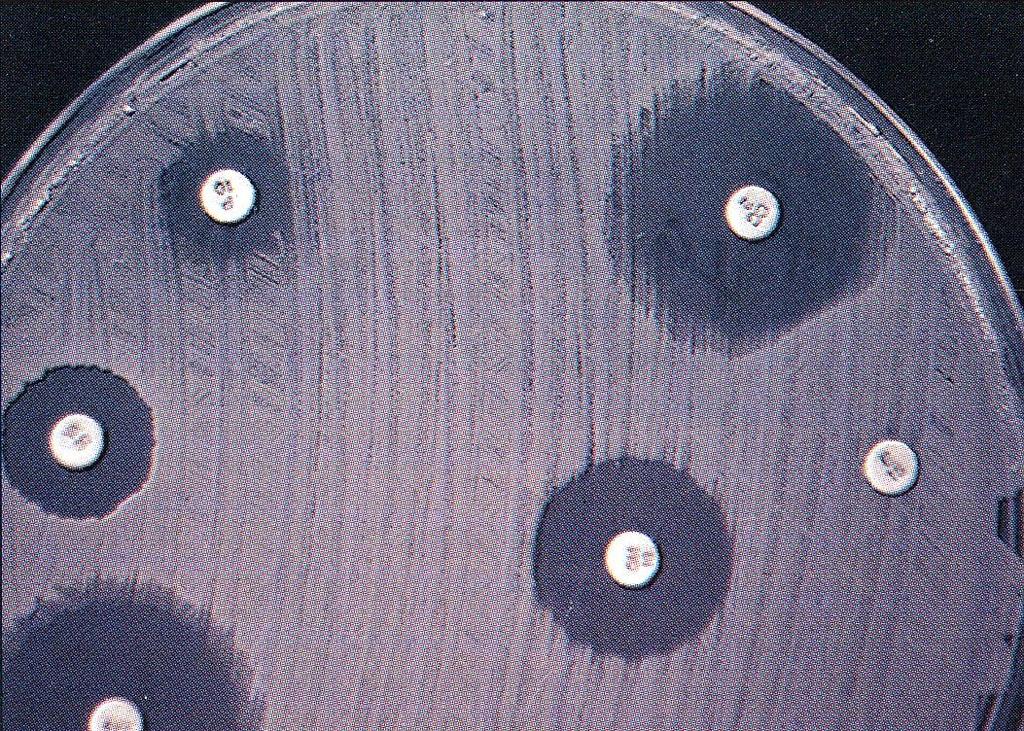
21 E test: Utilization of antibiotic concentration gradient

22 MIC= MICs of Vancomycin for S. aureus <0.25 0% 20% 40% 60% 80% 100% 1/1/11-6/21/11 6/ /31/10 6/2009-6/2010* *Vancomycin MIC reported from automated instrument only; no E-test confirmation

23
24


25
26


27
28 Mechanisms of Resistance MRSA Penicillin Binding Proteins Catalyze synthesis of cell wall Site of lactam action inhibit cell wall PBP-2 meca gene synthesizes an altered PBP-2a Lower binding of lactam
29 meca Gene Part of mobile genetic element A genetic element that has the ability to move from one site on a chromosome to another. Staphylococcal cassette chromosome (SCCmec) May harbor other virulence genes or other antibiotic resistance genes
30 CA-MRSA Empiric Treatment Assess disease severity and host Consider resistance issues Obtain cultures
31 TMP/SMX Few studies (Ann Intern Med 1992;117:390-8) Side effects Hypersensitivity rxns Bone marrow suppression No GABHS coverage Resistance potential, but remains low
32 Tetracycline Doxycycline or minocycline Age restriction Resistance in 3% of isolates Some data on use in skin and soft tissue infections No indication for serious disease
33 Clindamycin Resistance S. aureus Clindamycin resistance varies by region 5-25% Macrolide and lincosamide resistance closely related 23S rrna Risk of induced clinda resistance in Erythro resistant strains
34 MLS B Resistance via erm gene No MLS resistance (no erm) ERYTH S; CLINDA - S Constitutive MLS resistance (erm present) ERYTH R; CLINDA - R Possible Inducible resistance ERYTH R; CLINDA S (erm-repressed) ERYTH R; CLINDA S (mef)
35 D Test
36 CA-MRSA Empiric Treatment Life threatening (e.g. endocarditis, septicemia, toxic shock) lactam antibiotic (e.g. Nafcillin) and Non lactam reliably active against CA- MRSA (Vancomycin) May require additional agents for broader spectrum
37 CA-MRSA Empiric Treatment Moderate localized infections (e.g. osteomyelitis, cellulitis +/- abscess) Incision and drainage when appropriate Consider: Clindamycin Vancomycin Doxycycline ( 8 yrs) TMP/SMX
38 CA-MRSA Empiric Treatment Mild (e.g. simple skin infection) Topical therapy - mupirocin Clindamycin TMP/SMX lactam await culture and clinical response
39 Vancomycin Dosing and Monitoring Adults IV Vanco, mg/kg/dose Q 8-12 hrs. (abw) Not to exceed 2 grams/dose In seriously ill patients with suspected MRSA, consider a loading dose of mg/kg. Consider prolonged infusion, 2 ; antihistamine use Trough levels after the 3 rd dose most accurate way to guide dosing. For most pts with SSTI-1 gram Q 12 hrs. Trough levels rec. for morbidly obese, fluctuating volume of distribution, renal dysfunction. CID 2011:52. pg
40 Vancomycin Dosing and Monitoring Pediatrics IV Vancomycin 15 mg/kg/dose Q 6 hrs. is recommended in children with serious or invasive disease. Consider other issues (NSAIDs, dehydration, use of concomitant antivirals or antimicrobics), and consider modifying dose and additional levels and monitoring renal status. Double Consider Rule also called Law of Unintended Consequences) The efficacy of targeting trough concentrations of µg/ml requires additional study, but should be considered. CID 2011:52 pg 1-38.
41 Linezolid vs Vancomycin in the Management of Nosocomial Pneumonia Phase IV double-blind, RCT 1225 patients enrolled; 448 with MRSA Linezolid 600 mg Q12 vs Vancomcin 15mg/kg Q12 (adjusted for renal function and levels); 7-14 days Linezolid Vancomycin Clinical response (per protocol) 95/165 (57.5%) 81/174 (46.5%) p=0.042 Adverse events 5.2% (anemia) 7.2% anemia * No difference in mortality Kunkle M et al. Abstract LB-49. Annual meeting Infectious Diseases Society America. Vancouver Oct 24, 2010.
42 Outcomes in MSSA Bacteremia Nafcillin vs Vancomycin Prospective Observational Study With 6 Months Follow-up Nafcillin (n=18) Vancomycin (n=70) Persistent >3 but 7 Days 0 Persistent >7 Days 0 Relapse 0 Bacteriologic Failure Chang et al. Medicine (Baltimore). 2003;82:
43 Percent Influence of Vancomycin MIC on Outcome in S aureus Infection MIC Failure Success Moise-Broder et al. Clin Infect Dis. 2004;38:
44 Susceptibility Testing Vancomycin MIC 2 µg/ml indicates susceptibility Vancomycin MIC >2 µg/ml an alternative to vanc should be used, confirm and further characterize. 4-8=VISA; 16=VRSA. Best parameter to predict efficacy of vanc is AUC/MIC (area under curve/minimum inhibitory concentration), determined by measuring trough concentrations

45
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
DELL CHILDREN S MEDICAL CENTER EVIDENCE-BASED OUTCOMES CENTER. Community Acquired Pneumonia
 DELL CHILDREN S MEDICAL CENTER Community Acquired Pneumonia LEGAL DISCLAIMER: The information provided by Dell Children s Medical Center of Texas (DCMCT), including but not limited to Clinical Pathways
DELL CHILDREN S MEDICAL CENTER Community Acquired Pneumonia LEGAL DISCLAIMER: The information provided by Dell Children s Medical Center of Texas (DCMCT), including but not limited to Clinical Pathways
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Staphylococcal Bacteremia
 Staphylococcal Bacteremia Henry F. Chambers, M.D. Professor of Medicine, UCSF Chief of Infectious Diseases San Francisco General Hospital Case 1 38 y/o man, new CHF, alcoholic cardiomyopathy, Hct = 13
Staphylococcal Bacteremia Henry F. Chambers, M.D. Professor of Medicine, UCSF Chief of Infectious Diseases San Francisco General Hospital Case 1 38 y/o man, new CHF, alcoholic cardiomyopathy, Hct = 13
Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center
 CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
ESPID New Bone and Joint Infection Guidelines
 ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Aspiration pneumonia in older people
 Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management
Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates
 Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates Xuzhuang Shen Beijing Children's Hospital, Capital Medical University,
Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates Xuzhuang Shen Beijing Children's Hospital, Capital Medical University,
Choosing an appropriate antimicrobial agent. 3) the spectrum of potential pathogens
 the spectrum of potential pathogens") Choosing an appropriate antimicrobial agent Consider: 1) the host 2) the site of infection 3) the spectrum of potential pathogens 4) the likelihood that these pathogens are resistant to antimicrobial agents
Choosing an appropriate antimicrobial agent Consider: 1) the host 2) the site of infection 3) the spectrum of potential pathogens 4) the likelihood that these pathogens are resistant to antimicrobial agents
Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship
 Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians
Community Acquired Pneumonia Pediatric Ages 3 month to 18 years Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Guideline for management of children & adolescents with pleural empyema
 CHILD AND ADOLESCENT HEALTH SERVICE PRINCESS MARGARET HOSPITAL FOR CHILDREN Guideline for management of children & adolescents with pleural empyema This guideline provides an evidence-based framework for
CHILD AND ADOLESCENT HEALTH SERVICE PRINCESS MARGARET HOSPITAL FOR CHILDREN Guideline for management of children & adolescents with pleural empyema This guideline provides an evidence-based framework for
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine June 10-12, 2011
 The 48 th Annual Pediatrics for the Practitioner Symposium June 11, 2011 James H. Brien, DO James H. Brien, DO has no relevant financial relationships with commercial interests to disclose. Case #1 4½-month-old
The 48 th Annual Pediatrics for the Practitioner Symposium June 11, 2011 James H. Brien, DO James H. Brien, DO has no relevant financial relationships with commercial interests to disclose. Case #1 4½-month-old
Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,.
 Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,. 12-10-2017 Group B streptococci are uniformly sensitive to penicillin
Group B streptococcal infection;. Bacteremia without a focus occurs in 80-85%,. July has been recognised as Group B Strep Awareness Month,. 12-10-2017 Group B streptococci are uniformly sensitive to penicillin
Invasive Staphylococcal Infections
 Invasive Staphylococcal Infections Henry F. Chambers, M.D. Professor of Medicine, UCSF San Francisco General Hospital Disclosures AstraZeneca advisory board Cubist research grant, advisory panel Genentech
Invasive Staphylococcal Infections Henry F. Chambers, M.D. Professor of Medicine, UCSF San Francisco General Hospital Disclosures AstraZeneca advisory board Cubist research grant, advisory panel Genentech
Daptomycin in Clinical Practice. Paolo Grossi
 Clinica delle Malattie Infettive e Tropicali Università degli Studi dell Insubria Ospedale di Circolo e Fondazione Macchi, Varese Second Opinion Infettivologica Centro Nazionale Trapianti, ISS, Roma Daptomycin
Clinica delle Malattie Infettive e Tropicali Università degli Studi dell Insubria Ospedale di Circolo e Fondazione Macchi, Varese Second Opinion Infettivologica Centro Nazionale Trapianti, ISS, Roma Daptomycin
The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA
 The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA Franklin D. Lowy, MD Columbia University College of Physicians & Surgeons New York, NY Topics to Be Covered Background Some
The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA Franklin D. Lowy, MD Columbia University College of Physicians & Surgeons New York, NY Topics to Be Covered Background Some
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF -- William Osler, M.D.
 Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Objectives. Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection
 that drive empiric antimicrobial selection") Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Macrolides & Ketolides. Objectives. Protein Synthesis
 Macrolides & Ketolides Elizabeth D. Hermsen, Pharm.D. Infectious Diseases Research Fellow University of Minnesota College of Pharmacy bjectives Participant should be able to explain macrolide/ketolide
Macrolides & Ketolides Elizabeth D. Hermsen, Pharm.D. Infectious Diseases Research Fellow University of Minnesota College of Pharmacy bjectives Participant should be able to explain macrolide/ketolide
Management of Common Respiratory Disorders in Children. Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children. Disclosures. Roadmap 6/10/2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Infectious Diseases Society of America Emerging Infections Network. Comments for Query: Osteomyelitis in Children
 Infectious Diseases Society of America Emerging Infections Network Comments for Query: Osteomyelitis in Children Choice of antimicrobial At our institution, we typically start with clindamycin (unless
Infectious Diseases Society of America Emerging Infections Network Comments for Query: Osteomyelitis in Children Choice of antimicrobial At our institution, we typically start with clindamycin (unless
Management of severe staphylococcal infections
 Management of severe staphylococcal infections Dilip Nathwani BSAC April 7 th 2009 Ninewells Hospital & Medical School Dundee DD1 9SY Objectives Mortality related to MSSA and MRSA infections Glycopeptides
Management of severe staphylococcal infections Dilip Nathwani BSAC April 7 th 2009 Ninewells Hospital & Medical School Dundee DD1 9SY Objectives Mortality related to MSSA and MRSA infections Glycopeptides
Development of C sporins. Beta-lactam antibiotics - Cephalosporins. Second generation C sporins. Targets - PBP s
 Beta-lactam antibiotics - Cephalosporins Development of C sporins Targets - PBP s Activity - Cidal - growing organisms (like the penicillins) Principles of action - Affinity for PBP s Permeability properties
Beta-lactam antibiotics - Cephalosporins Development of C sporins Targets - PBP s Activity - Cidal - growing organisms (like the penicillins) Principles of action - Affinity for PBP s Permeability properties
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Department of Pediatrics, University of California San Diego School of Medicine and Rady Children's Hospital of San Diego, San Diego, California; 2
 IDSA GUIDELINES Executive Summary: The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society
IDSA GUIDELINES Executive Summary: The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society
Department of Pediatrics, University of California San Diego School of Medicine and Rady Children's Hospital of San Diego, San Diego, California; 2
 IDSA GUIDELINES Executive Summary: The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society
IDSA GUIDELINES Executive Summary: The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
Department of Pediatrics, University of California San Diego School of Medicine and Rady Children's Hospital of San Diego, San Diego, California; 2
 IDSA GUIDELINES The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious
IDSA GUIDELINES The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious
Department of Pediatrics, University of California San Diego School of Medicine and Rady Children's Hospital of San Diego, San Diego, California; 2
 Clinical Infectious Diseases Advance Access published August 30, 31, 2011 IDSA GUIDELINES The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice
Clinical Infectious Diseases Advance Access published August 30, 31, 2011 IDSA GUIDELINES The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice
I have no disclosures
 Disclosures Streptococcal Pharyngitis: Update and Current Guidelines Richard A. Jacobs, MD, PhD Emeritus Professor of Medicine Division of Infectious Diseases I have no disclosures CID 2012:55;e 86-102
Disclosures Streptococcal Pharyngitis: Update and Current Guidelines Richard A. Jacobs, MD, PhD Emeritus Professor of Medicine Division of Infectious Diseases I have no disclosures CID 2012:55;e 86-102
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
CLINICAL USE OF GLYCOPEPTIDES. Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel
 CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
Pneumonia in Older Adults: An Update
 Pneumonia in Older Adults: An Update - 2010 Suzanne F. Bradley, M.D. Professor of Internal Medicine Geriatrics & Infectious Diseases University of Michigan Medical School GRECC - VA Ann Arbor HCS ID Hospitalizations
Pneumonia in Older Adults: An Update - 2010 Suzanne F. Bradley, M.D. Professor of Internal Medicine Geriatrics & Infectious Diseases University of Michigan Medical School GRECC - VA Ann Arbor HCS ID Hospitalizations
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
PNEUMONIA. Patient Case: Chief Complaint: I have been short of breath and have been coughing up rust-colored phlegm for the past 3 days.
 PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
MCH-Immunization Conference. September 2012
 MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Skin and Soft Tissue Infections (SSTI): More than a skin deep review. Vicky Parente, MD Sea Pines Conference July 12th, 2018
: More than a skin deep review. Vicky Parente, MD Sea Pines Conference July 12th, 2018") Skin and Soft Tissue Infections (SSTI): More than a skin deep review Vicky Parente, MD Sea Pines Conference July 12th, 2018 Objectives To review the anatomy and classification of SSTIs To understand the
Skin and Soft Tissue Infections (SSTI): More than a skin deep review Vicky Parente, MD Sea Pines Conference July 12th, 2018 Objectives To review the anatomy and classification of SSTIs To understand the
-> Education -> Excellence
 Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship
 Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Community Acquired Pneumonia - Pediatric Clinical Practice Guideline MedStar Health Antibiotic Stewardship These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF
 Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH)
") Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
BONE & JOINT INFECTIONS
 BONE & JOINT INFECTIONS Henry F. Chambers, MD Disclosures AstraZeneca advisory board Cubist research grant, advisory panel Genentech advisory board Merck stock Pfizer advisory board Theravance advisory
BONE & JOINT INFECTIONS Henry F. Chambers, MD Disclosures AstraZeneca advisory board Cubist research grant, advisory panel Genentech advisory board Merck stock Pfizer advisory board Theravance advisory
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
- Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including
: important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including") KHOA DICH VU HO HAP - Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including wheezing, coryza, bronchopneumonia. -
KHOA DICH VU HO HAP - Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including wheezing, coryza, bronchopneumonia. -
ภก.วส นต กาต บ. Use of vancomycin is appropriate or acceptable. FDA Labeled Indication
 Quality improvement for DUE: Vancomycin, Linezolid and Daptomycin Vancomycin ภก.วส นต กาต บ Vancomycin. In: DRUGDEX System [Internet database]. Greenwood Village, Colo: Thomson Healthcare. Updated periodically.
Quality improvement for DUE: Vancomycin, Linezolid and Daptomycin Vancomycin ภก.วส นต กาต บ Vancomycin. In: DRUGDEX System [Internet database]. Greenwood Village, Colo: Thomson Healthcare. Updated periodically.
ESCMID Online Lecture Library. by author
 Hospital Universitario Virgen Macarena, Seville New drugs against MRSA and VRE L. Eduardo López Cortés Seville, 8th July Tedizolid Oxazolidinone Ceftaroline // Ceftobiprole 5 th gen cephalosporin Overview
Hospital Universitario Virgen Macarena, Seville New drugs against MRSA and VRE L. Eduardo López Cortés Seville, 8th July Tedizolid Oxazolidinone Ceftaroline // Ceftobiprole 5 th gen cephalosporin Overview
Community-Acquired Pneumonia. Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital. Nothing to disclose.
 Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Pneumonia: The Forgotten Killer
 Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
SEPTIC ARTHRITIS Native Joint BONE & JOINT INFECTIONS. Case. What is the most appropriate initial therapy for this patient? Henry F.
 BONE & JOINT INFECTIONS SEPTIC ARTHRITIS Native Joint Henry F. Chambers, MD Curr Rheumatol Rep 15:332, 2013; Best Prac Res Clin Rheumatol 25:407, 2011 Case 38 y/o type 2 diabetic women, single, sexually
BONE & JOINT INFECTIONS SEPTIC ARTHRITIS Native Joint Henry F. Chambers, MD Curr Rheumatol Rep 15:332, 2013; Best Prac Res Clin Rheumatol 25:407, 2011 Case 38 y/o type 2 diabetic women, single, sexually
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Bone and Joint Infections Oh, My
 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
More Than the Sniffles: Update on the Treatment of Pediatric Respiratory Infections
 More Than the Sniffles: Update on the Treatment of Pediatric Respiratory Infections Amy Crawford, Pharm.D. R.Ph NDPhA 2014 Annual Convention April 5 th, 2014 Conflict of Interest No relevant financial
More Than the Sniffles: Update on the Treatment of Pediatric Respiratory Infections Amy Crawford, Pharm.D. R.Ph NDPhA 2014 Annual Convention April 5 th, 2014 Conflict of Interest No relevant financial
Acute Bacterial Sinusitis: The latest treatment recommendations. Objectives Having completed the learning activities, the participant will be able to:
 Acute Bacterial Sinusitis: The latest treatment recommendations Presented by: Monica Tombasco, MS, MSNA, FNP-BC, CRNA Senior Lecturer Fitzgerald Health Education Associates, Inc., North Andover, MA Emergency
Acute Bacterial Sinusitis: The latest treatment recommendations Presented by: Monica Tombasco, MS, MSNA, FNP-BC, CRNA Senior Lecturer Fitzgerald Health Education Associates, Inc., North Andover, MA Emergency
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP /15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain,
 Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Endocardite infectieuse
 Endocardite infectieuse 1. Raccourcir le traitement: jusqu où? 2. Proposer un traitement ambulatoire: à partir de quand? Endocardite infectieuse A B 90 P = 0.014 20 P = 0.0005 % infective endocarditis
Endocardite infectieuse 1. Raccourcir le traitement: jusqu où? 2. Proposer un traitement ambulatoire: à partir de quand? Endocardite infectieuse A B 90 P = 0.014 20 P = 0.0005 % infective endocarditis
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
IH Pharmacy Live Rounds
 IH Pharmacy Live Rounds Effect of Vancomycin plus Rifampicin in the Treatment of Nosocomial Methicillin-resistant Staphylococcus aureus Pneumonia Sandra Katalinic, Pharmacy Resident Kelowna General Hospital
IH Pharmacy Live Rounds Effect of Vancomycin plus Rifampicin in the Treatment of Nosocomial Methicillin-resistant Staphylococcus aureus Pneumonia Sandra Katalinic, Pharmacy Resident Kelowna General Hospital
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Invasive Bacterial Disease
 Invasive Bacterial Disease All Streptococcus pneumoniae Electronic Disease Surveillance System Division of Surveillance and Disease Control Infectious Disease Epidemiology Program : 304-558-5358 or 800-423-1271
Invasive Bacterial Disease All Streptococcus pneumoniae Electronic Disease Surveillance System Division of Surveillance and Disease Control Infectious Disease Epidemiology Program : 304-558-5358 or 800-423-1271
[Pediatric comments provided in blue]
![[Pediatric comments provided in blue]](/thumbs/77/76528727.jpg "[Pediatric comments provided in blue]") Infectious Diseases Society of America Emerging Infections Network Comments for Query: S. aureus Community-Acquired Pneumonia 2008 [Pediatric comments provided in blue] S. aureus colonization / Diagnosis
Infectious Diseases Society of America Emerging Infections Network Comments for Query: S. aureus Community-Acquired Pneumonia 2008 [Pediatric comments provided in blue] S. aureus colonization / Diagnosis
Alabama Medicaid Pharmacist
 Alabama Medicaid Pharmacist Published Quarterly by Health Information Designs, LLC, Winter 015 edition A Service of Alabama Medicaid PDL Update Effective January 5, 015, the Alabama Medicaid Agency will
Alabama Medicaid Pharmacist Published Quarterly by Health Information Designs, LLC, Winter 015 edition A Service of Alabama Medicaid PDL Update Effective January 5, 015, the Alabama Medicaid Agency will
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Vancomycin: Class: Antibiotic.
 Vancomycin: Class: Antibiotic. Indications: Treatment of patients with infections caused by staphylococcal species and streptococcal Species. Available dosage form in the hospital: 1G VIAL, 500MG VIAL.
Vancomycin: Class: Antibiotic. Indications: Treatment of patients with infections caused by staphylococcal species and streptococcal Species. Available dosage form in the hospital: 1G VIAL, 500MG VIAL.
VANCOMYCIN DOSING AND MONITORING GUIDELINES
 VANCOMYCIN DOSING AND MONITORING GUIDELINES NB Provincial Health Authorities Anti-Infective Stewardship Committee Approved: May 2017 GENERAL COMMENTS Vancomycin is a glycopeptide antibiotic with bactericidal
VANCOMYCIN DOSING AND MONITORING GUIDELINES NB Provincial Health Authorities Anti-Infective Stewardship Committee Approved: May 2017 GENERAL COMMENTS Vancomycin is a glycopeptide antibiotic with bactericidal
Update on Rhinosinusitis 2013 AAP Guidelines Review
 Update on Rhinosinusitis 2013 AAP Guidelines Review Carla M. Giannoni, MD Surgeon, Otolaryngology Texas Children's Hospital Professor, Surgery and Pediatrics, Baylor College of Medicine CDC: Acute Rhinosinusitis
Update on Rhinosinusitis 2013 AAP Guidelines Review Carla M. Giannoni, MD Surgeon, Otolaryngology Texas Children's Hospital Professor, Surgery and Pediatrics, Baylor College of Medicine CDC: Acute Rhinosinusitis
WORKSHOP. The Multiple Facets of CAP. Community acquired pneumonia (CAP) continues. Jennifer s Situation
 continues. Jennifer s Situation") Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Practical Pointers pointers For for Your your Practice practice The Multiple Facets of CAP Dr. George Fox, MD, MSc, FRCPC, FCCP Community acquired pneumonia (CAP) continues to be a significant health burden
Renal Unit. Catheter Related Bacteraemia Guidelines
 Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Getting Smart About: Upper Respiratory Infections
 Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Continuous Infusion of Antibiotics In The ICU: What Is Proven? Professor of Medicine Vice-Chairman, Department of Medicine SUNY at Stony Brook
 Continuous Infusion of Antibiotics In The ICU: What Is Proven? Michael S. Niederman, M.D. Chairman, Department of Medicine Winthrop-University Hospital Mineola, NY Professor of Medicine Vice-Chairman,
Continuous Infusion of Antibiotics In The ICU: What Is Proven? Michael S. Niederman, M.D. Chairman, Department of Medicine Winthrop-University Hospital Mineola, NY Professor of Medicine Vice-Chairman,
Sep Oct Nov Dec Total
 LB PAGE 2 LB PAGE 3 Sep Oct Nov Dec 2007 2007 2007 2007 Total Repeat Information Total Repeats 35 15 17 9 76 Repeat Rate 6.01% 0.17% 1.12% 0.39% 2.07% Repeat Chemistry 25 0 2 0 27 Repeat Extraction 1 0
LB PAGE 2 LB PAGE 3 Sep Oct Nov Dec 2007 2007 2007 2007 Total Repeat Information Total Repeats 35 15 17 9 76 Repeat Rate 6.01% 0.17% 1.12% 0.39% 2.07% Repeat Chemistry 25 0 2 0 27 Repeat Extraction 1 0
prophylaxis for endocarditis in patients at high risk prophylaxis for major surgical procedures
 1 Glycopeptides appropriate uses serious infections due to beta-lactam- resistant gram-positive microorganisms infections due to gram-positive microorganisms in patients with serious allergy to beta-lactam
1 Glycopeptides appropriate uses serious infections due to beta-lactam- resistant gram-positive microorganisms infections due to gram-positive microorganisms in patients with serious allergy to beta-lactam