At the end of this session, participants will be able to:
|
|
|
- Jordan Ramsey
- 6 years ago
- Views:
Transcription


1 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University of Florida College of Medicine/Jacksonville Objectives At the end of this session, participants will be able to: Compare contagiousness of children of different ages with pulmonary TB, and apply this to planning investigations Discuss importance and indications for source case investigation Plan evaluation for contacts of patients with various forms of TB disease Discuss infection control guidelines for a child hospitalized with TB disease 1
2 Key Terms Case A particular patient with TB disease. All TB cases are reportable. Contact (AKA: Exposed person) Someone who has been exposed to M. tuberculosis by sharing air space with a person with infectious TB. Index case The first case or patient who comes to attention as indicator of a potential public health problem. Source case The case or person who was the original source of infection for secondary cases or contacts; can be, but is not necessarily, the index case. Case 2
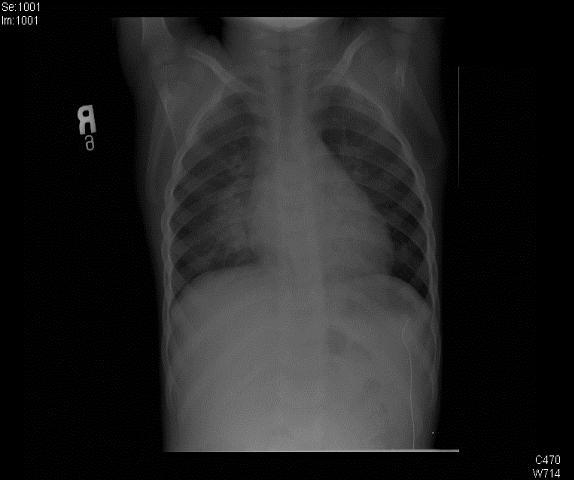
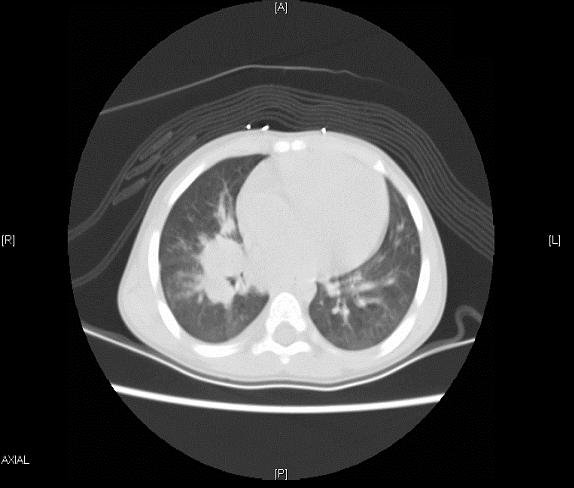
3 Index Case 2 y/o AA male presented to ER with 8 day history of fever and cough. He was diagnosed with pneumonia and was prescribed amoxicillin. After 5 days, his fever was not better, so he was admitted to the hospital for IV antibiotics. He was started on ceftriaxone, and then vancomycin was added. However, fever persisted. PMH: no significant illness, no surgeries or hospitalizations Index Case Family/Social history: lives with mother and 2 older siblings. Has attended a Daycare Center since the age of 7 months. No travel history, no history of contacts with adults with HIV, IVDU, homeless, incarcerated. Physical exam was normal, with the exception of Tmax of 41 degrees. 3
4 4
5 Index Case TST was placed and read as 10 mm of induration Gastric aspirates x 3 were sent Patient was started on INH, Rif, and PZA, and fever resolved after 3 days. He was discharged home to continue meds under DOT. Gastric aspirate cultures were negative Case 2y/o AA male with a clinical case of pulmonary TB. What would you do next? a. Obtain biopsy of hilar lymph nodes to confirm TB. b. Since patient is responding to anti-tb therapy, just complete 6 months of therapy c. Plan and conduct a contact investigation d. Plan and conduct a source-case investigation 5
6 Source-Case Investigations Source-case Investigations Seeks the source of recent M.tuberculosis infection TB in children <5 years of age typically indicates recent transmission. Young children usually do not transmit TB to others. The source-case is usually an adult/adolescent care-giver. A source-case investigation should be considered for children <5 y/o (especially <2) with TB. 6
7 Importance of Source-case Investigations Public health measure Identify the individual who infected the child, who is probably transmitting TB to others Diagnostic measure Isolating the organism from the source case provides likely drug susceptibility of the child s organism Yield is higher than yield of diagnostic microbiology in children Source-case Investigation for Child with LTBI Search for source of infection for child with LTBI is not likely to be productive and cost-efficient Recommended only with infected children <2 years of age, and only if data are monitored to determine the value of the investigation Relative recent transmission! 7
8 Procedures for Source-Case Investigation Same procedure as standard contact investigation Patient or guardians best informants (associates) Focus on associates who have symptoms of TB disease Should begin with closest associates, and expand if appropriate Back to our case Source case investigation was conducted All household tested negative (TST) Investigation was expanded to the Daycare Center (DCC) 3 DCC staff had +TST, but negative CXR One DCC worker had neg TST, but history of chronic cough, and was eventually diagnosed with Pulmonary TB (cavitary, smear positive) This was the source case! What next? 8

9 Contact Investigations A Crucial Prevention Strategy On average, 10 contacts are identified for each person with infectious TB in the U.S. 20% 30% of all contacts have LTBI 1% of contacts have TB disease Of contacts who will ultimately have TB disease, approximately 50% develop disease in the first year after exposure 5 Benefits of Contact Investigations Finding and treating additional TB disease cases (potentially interrupting further transmission) Finding and treating persons with LTBI to avert future cases 9
10 Importance of Contact Investigation How are pediatric cases discovered? Active Contact investigation: 25-80% Screening of high risk groups: 3-35% Passive Symptomatic children: 15-45% Contact Investigation Responsibilities Health departments are responsible for conducting contact investigations Contact investigations are complicated activities that require Many interdependent decisions Time-consuming interventions 10
11 Decisions to Initiate a Contact Investigation Public health officials must decide which Contact investigations should be assigned a higher priority Contacts to evaluate first Decision to investigate an index patient depends on presence of factors used to predict likelihood of transmission Factors that Predict Likely Transmission of TB Anatomical site of the disease Positive sputum bacteriology Radiographic findings (cavitation) Behaviors/procedures that increase aerosolization of respiratory secretions Age HIV status Administration of effective treatment 11
12 Characteristics of the Index Patient Associated with Increased Risk of TB Transmission Pulmonary, laryngeal, or pleural TB Acid-fast bacilli (AFB) positive sputum smear Cavitation on CXR Adolescent or adult patient No or ineffective treatment of TB disease Determining the Infectious Period Sets time frame for testing contacts most likely to be at risk for infection Information to assist with determining infectious period Approximate dates TB symptoms were noticed Bacteriologic results Extent of disease Start is 3 months before TB diagnosis (recommended) Earlier start should be used in certain circumstances (e.g., patient aware of illness for longer period of time) 12
13 Assigning Priorities to Contacts Priorities based on likelihood of infection and hazards to the contact if infected Factors for Assigning Contact Priorities Characteristics of the index/source patient Characteristics of contacts Age Immune status Other medical conditions Exposure Patient has pulmonary, laryngeal, or pleural TB with cavitary lesion on chest radiograph or is AFB sputum smear positive Household contact High Contact <5 years of age High Contact with medical risk factor (HIV or other medical risk High factor) Contact with exposure during medical procedure High (bronchoscopy, sputum induction, or autopsy) Contact in a congregate setting High Contact exceeds duration/environment limits (limits per unit High time established by the health department for high-priority contacts) Contact is 5 years and 15 years of age Contact exceeds duration/environment limits (limits per unit time established by the health department for medium-priority contacts) Any contact not classified as high or medium priority is assigned a low priority. Medium Medium 13
14 Back to our case A full scale Contact Investigation was conducted 52 children exposed within the previous 3 months were identified and tested (ROS, Physical exam, TST and CXR) 24 children had + TST 5 children were diagnosed with Pulmonary TB (1 with meningitis) 18 children had LTBI 28 children had TST and - CXR <5y/o started on window prophylaxis 2 more children had +TST after 10 weeks (re-test) Day Care Settings: High Priority for Contact Investigation Children < 5 years of age Prolonged exposure Close contact Depending on the size of the daycare center Crowding Poor ventilation 14
15 General Population vs Day Care Setting On average, 10 contacts are identified for each person with infectious TB in the U.S. 52 exposed children identified 20% 30% of all contacts have LTBI 38% of children had LTBI 1% of contacts have TB disease, half of them in the first year after exposure 12% of children developed TB disease All of them developed it within 6 months Evaluation of contacts Testing for TB Infection All high or medium priority contacts who do not have a documented previous positive TST/IGRA or previous TB disease should receive a TST or IGRA at the initial encounter TST interpretation 5 mm induration is positive for any contact If TST/IGRA negative Repeat same test in 8-10 weeks (window period) If second TST is positive after initial negative Contact is classified as recently infected 15

16 Evaluation of contacts Medical Evaluation All contacts with positive TST/IGRA or who report any symptoms consistent with TB disease should undergo further examination and testing for TB disease History & Physical CXR Other tests as indicated Window-Period Prophylaxis Decision to treat contacts with a negative TST/IGRA should take the following factors into consideration The frequency, duration, and intensity of exposure Risk factors for TB disease Age of the contacts Medical conditions 16
17 Management of Contacts Younger than 5 years of age Evaluation TST CXR Review of symptoms and physical exam (PE) Primary prophylaxis ( window ) If TST, CXR, and PE are neg, start INH until repeat TST in 8-10 weeks If repeat TST is neg, stop INH If repeat TST is pos, treat as LTBI Prophylactic Treatment Prophylactic treatment (after TB disease is excluded) of presumed M. tuberculosis infection recommended for persons With HIV infection Taking immunosuppressive therapy for organ transplant Taking anti-tumor necrosis factor alpha (TNF-α) agents Since LTBI cannot be excluded, these contacts should be treated with 9 months of INH 17
18 A story that never ends Seven months later, a high school student with no risk factors was diagnosed with Pulmonary TB (cavitary, smear positive). Where did he get it from? Grandson of a friend of the CCC source case, with occasional contact with her before her diagnosis Had not been identified as a contact in the previous investigation MTB isolate was genotypically identical to source case. A story that never ends Contact investigation conducted at the High School Initial: 197contacts identified (same classrooms, sports teammates, bus-riders) 1 st TST: 16+ (8%) 2 nd TST: 18+ /103 (17%) Expanded: 206 additional contacts TST: 8+ (4%) None with TB disease 18
19 Determining When to Expand a Contact Investigation Consideration of the following factors recommended Extent of recent transmission Unexpectedly large rate of infection or TB disease in high-priority contacts Evidence of second-generation transmission TB disease in any contacts who had been assigned low priority Infection in any contacts aged <5 years Contacts with change in skin test status from negative to positive A story that never ends It keeps going, and going One month later, a 7 m/o old male, cousin of the high school student, was diagnosed with Pulmonary TB He was identified as a contact, and had been evaluated by PCP Asymptomatic, TST negative No CXR, no further intervention A month later, presented with fever, wheezing and productive cough CXR with right hilar adenopathy and RUL infiltrate Gastric aspirates smear and cx - POSITIVE 19
20 And it keeps going, and going This baby attended a small Child Care Center Because of extensive disease, significant cough, and + smear, and anxiety, a Contact Investigation was conducted at the CCC 4 workers 8 infants All evaluations were negative Why not contact investigations in young children? Transmission Airborne infection Inhalation of droplet nuclei produced by an adult or adolescent with pulmonary or laryngeal TB Infectiousness correlates with the number of organisms expelled 20
21 Why not contact investigations in young children? Very low yield! Most children with TB are not contagious because compared to adults they are less likely to Have a productive cough Generate force to aerosolize the organisms Have large numbers of organisms Children with extrapulmonary TB are not infectious unless disease of larynx or open abscesses/lesions When to consider contact investigations in children Transmission of TB from children can occur, but usually due to exceptional circumstances Adult-type disease: cavitary, extensive upper lobe disease Procedures creating aerosolization of bacilli Bronchoscopy Induced sputum By the way, gastric aspirates are NOT associated with transmission! 21

22 Infection Control Recommendations for Preventing M. tuberculosis Transmission in Health-Care Settings 22

23 Fundamentals of Infection Control Administrative Controls Environmental Controls Respiratory Protection Fundamentals of Infection Control Administrative controls: reduce risk of exposure via effective IC program Assign responsibility for IC in the facility Conduct annual facility risk assessment by examining Institute IC plan to ensure TB suspects found, isolated, evaluated, treated Ensure recommended laboratory services are available For HCWs, implement effective work practices and test as classification indicates Ensure equipment is properly cleaned, disinfected, and sterilized Educate, train, and counsel HCWs, patients, visitors about TB 23
24 Fundamentals of Infection Control Environmental controls: prevent spread and reduce concentration of droplet nuclei Primary controls: ventilation technologies Natural ventilation vs mechanical ventilation Use of AII room Secondary controls: HEPA filters and ultraviolet germicidal irradiation (UVGI) Fundamentals of Infection Control Environmental Controls Characteristics of AII room: Single-patient room with private bathroom Negative pressure relative to hallway Air sent outdoors or through HEPA filter Six or more air changes per hour (in some settings 12 or more air changes per hour are recommended) Visitors should use N95 respirator 24


25 Fundamentals of Infection Control Respiratory protection controls: further reduce risk of exposure in special areas and circumstances Consists of using personal protective equipment in areas with increased risk of exposure Should be used by persons Entering rooms of suspected/confirmed TB patients Around cough- or aerosol-producing procedures In settings where administrative and environmental controls will not prevent the inhalation of infectious droplet nuclei Respirator for Health-Care Workers HCW N95 Respirator Designed to filter out droplet nuclei from being inhaled by the health-care worker and other individuals. Should properly fit different face sizes and features. Should NOT be worn by the patient. 25

26 Surgical Mask for Persons with Infectious TB Disease Patient Surgical mask Designed to stop droplet nuclei from being spread (exhaled) by the patient. Should NOT be worn by the health-care worker. Risk Factors for Infectiousness Presence of productive cough Cavitation or extensive upper lobe disease Positive AFB smear of sputum Involvement of larynx Failure to cover mouth/nose with cough Cough-inducing or aerosol=generating procedures (bronchoscopy, sputum production, aerosolized medications) 26
27 Isolation of the Hospitalized Adult Patient with TB or suspected TB Airborne infection isolation HCW and visitors wear at least N95 mask Discontinuation of isolation Suspected TB Another diagnosis excludes TB or 3 negative AFB sputum smear results Confirmed TB Effective therapy and Clinical improvement and 3 negative AFB sputum smear results Isolation of the Hospitalized Pediatric Patient with TB or suspected TB Children with TB, especially <10 y/o, are rarely infectious Nosocomial transmission in pediatric setting rare Adults accompanying children into the hospital may be the source case and potentially infectious Emphasis on infection control should be on these adults Isolate children until infectiousness excluded in patient and adults accompanying patient CXR is critical component of evaluation Until evaluation is complete, limit visitation or visitors should wear masks in common areas 27
28 TB among Adult Visitors of Children with Suspected TB at a Children s Hospital Adult caretakers accompanying admitted children Screening for TB prior to admission CXR as part of screening Isolation if child potentially contagious or of delay in obtaining accompanying adults CXR 59 children enrolled 8 required isolation 105 adults screened 15% had abnormal CXR compatible with TB Infect Control and Hosp Epidemiol 2002; 23: Management of the Newborn whose Mother has LTBI Mother has reactive TST or IGRA and normal CXR If mother is asymptomatic, no separation Mother should be treated for LTBI after the initial postpartum period Newborn needs no further evaluation Other household members should be evaluated for TB infection or disease This should not delay newborn s discharge from the hospital Mother can breastfeed the infant 28
29 Management of the Newborn whose Mother has Suspected TB Mother has clinical signs/symptoms or abnormal CXR c/w TB disease Evaluate mother ASAP (e.g. sputum for AFB, etc) Separate mother and infant until evaluation complete If TB suspected/confirmed, separate them until mother receiving adequate therapy she wears a mask, and she understands and follows infection-control measures Mother can breastfeed the infant after at least 2 weeks of adequate treatment AND when considered not contagious Management of the Newborn whose Mother has Suspected TB Mother has clinical signs/symptoms or abnormal CXR c/w TB disease If mother has TB disease, evaluate infant for congenital TB If excluded, begin INH Repeat TST when infant is 3-4 mo old If negative, discontinue INH If positive, re-evaluate for TB disease If no disease, complete 9 mo of INH Once INH started for infant, separation no longer necessary unless there is suspicion for MDR TB 29
30 Management of the Newborn whose Mother has Suspected TB Mother has clinical signs/symptoms or abnormal CXR c/w TB disease If mother has TB disease, and MDR is suspected/proven Separate mother and infant until mother considered no longer contagious Consider BCG vaccination for infant (if HIV negative) if separation from mother is not possible Management of the Newborn whose Mother has Suspected TB Mother has abnormal CXR findings but no evidence of TB disease Separation not necessary Mother should receive LTBI treatment Household should be investigated for TB 30
31 Prevention of Transmission in the Community Child care Children with TB can attend child care if they are receiving appropriate therapy If source case child care worker, other children in center should be evaluated Child with TB not contagious unless adult-type disease School Children can attend school if receiving appropriate therapy School contacts of children with adult-type disease should be investigated by Health Department Take-Home Messages The diagnosis of TB in a child is a sentinel event representing recent transmission of TB in the community A source case investigation should be considered when a young child is diagnosed with TB Do not forget non-family care-givers Contact investigations are an essential component of TB prevention Daycare centers represent a high priority for contact investigation Young children are rarely contagious, but the source-case is Use window prophylaxis in young children 31

32 Main References American Academy of Pediatrics. Tuberculosis. In: Pickering, Baker, Kimberlin, Long, ed. Red Book: 2012 Report of the Committee on Infectious Diseases. Elk Grove Village, IL: American Academy of Pediatrics; Centers for Disease Control and Prevention. Guidelines for the Investigation of Contacts of Persons with Infectious Tuberculosis: Recommendations from the National Tuberculosis Controllers Association and CDC. MMWR 2005; 54 (No. RR 15) Centers for Disease Control and Prevention. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, MMWR 2005; 54 (No. RR-17). 32
Investigation of Contacts of Persons with Infectious Tuberculosis, 2005
 1 Investigation of Contacts of Persons with Infectious Tuberculosis, 2005 Daniel P. Dohony, MPH Division of Tuberculosis Elimination Centers for Disease Control and Prevention and Philadelphia TB Control
1 Investigation of Contacts of Persons with Infectious Tuberculosis, 2005 Daniel P. Dohony, MPH Division of Tuberculosis Elimination Centers for Disease Control and Prevention and Philadelphia TB Control
TB CONTROL IN HEALTHCARE FACILITIES: A PRACTICAL GUIDE FOR PREVENTION
 TB CONTROL IN HEALTHCARE FACILITIES: A PRACTICAL GUIDE FOR PREVENTION HOW TB IS SPREAD GENERATION OF TB DROPLET NUCLEI One cough produces 500 droplets Average TB patient generates 75,000 droplets/day (before
TB CONTROL IN HEALTHCARE FACILITIES: A PRACTICAL GUIDE FOR PREVENTION HOW TB IS SPREAD GENERATION OF TB DROPLET NUCLEI One cough produces 500 droplets Average TB patient generates 75,000 droplets/day (before
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Rebecca O. Sanchez, BSN., RN., MPH. has the following disclosures to make:
 INFECTION CONTROL PRACTICES Rebecca O. Sanchez, RN, BSN, MPH Texas Department of State Health Services Texas Center for Infectious Disease Rebecca O. Sanchez, BSN., RN., MPH. has the following disclosures
INFECTION CONTROL PRACTICES Rebecca O. Sanchez, RN, BSN, MPH Texas Department of State Health Services Texas Center for Infectious Disease Rebecca O. Sanchez, BSN., RN., MPH. has the following disclosures
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
The Air We Share: Principles and Practices of TB Infection Control
 The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Contact Investigation in the Correctional Setting Jessica Quintero, BAAS March 24, 2011 Jessica Quintero, BAAS has the following disclosures to make: No
TB in Corrections Phoenix, Arizona March 24, 2011 Contact Investigation in the Correctional Setting Jessica Quintero, BAAS March 24, 2011 Jessica Quintero, BAAS has the following disclosures to make: No
Chapter 7 Tuberculosis Infection Control
 Chapter 7 Tuberculosis Infection Control Table of Contents Chapter Objectives.... 187 Introduction.... 189 Infectiousness.... 190 TB Infection Control Measures... 194 TB Infection Control Program................................................
Chapter 7 Tuberculosis Infection Control Table of Contents Chapter Objectives.... 187 Introduction.... 189 Infectiousness.... 190 TB Infection Control Measures... 194 TB Infection Control Program................................................
TB Contact Investigation
 Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
Ann Raftery, RN, PHN, MS Curry International TB Center Overview Contact investigation as a core TB control and elimination activity Components of TB Contact Investigation TB Control Priority Strategies.
TB Program Management San Antonio, Texas November 5-7, 2008
 TB Program Management San Antonio, Texas November 5-7, 2008 Infection Control Lynelle Phillips, RN, MPH November 7, 2008 Infection Control Lynelle Phillips, RN MPH Nurse Consultant Heartland National TB
TB Program Management San Antonio, Texas November 5-7, 2008 Infection Control Lynelle Phillips, RN, MPH November 7, 2008 Infection Control Lynelle Phillips, RN MPH Nurse Consultant Heartland National TB
TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks
 1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
2018 Tuberculosis Clinical Intensive: Infection Prevention & Control. > No disclosures
 2018 Tuberculosis Clinical Intensive: Infection Prevention & Control > No disclosures 1 Objectives By the end of today s session, hopefully you will be able to: > Recognize potential TB exposures in healthcare
2018 Tuberculosis Clinical Intensive: Infection Prevention & Control > No disclosures 1 Objectives By the end of today s session, hopefully you will be able to: > Recognize potential TB exposures in healthcare
What s New in TB Infection Control?
 What s New in TB Infection Control? Mark Lobato, MD Division of TB Elimination CDC / USPHS March 24, 2010 Providence, RI Keeping the scourge at bay Early disease prevention Modern cough etiquette When
What s New in TB Infection Control? Mark Lobato, MD Division of TB Elimination CDC / USPHS March 24, 2010 Providence, RI Keeping the scourge at bay Early disease prevention Modern cough etiquette When
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Contact Investigation Basics
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 TB Contact Investigation Basics Carrie Storrs, RN April 28, 2010 Contact Investigation Carrie Storrs TB Program Illinois Department of Public
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 TB Contact Investigation Basics Carrie Storrs, RN April 28, 2010 Contact Investigation Carrie Storrs TB Program Illinois Department of Public
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program
 Transmission in Ambulatory Surgery Centers. Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program") Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
Preventing Tuberculosis (TB) Transmission in Ambulatory Surgery Centers Heidi Behm, RN, MPH TB Controller HIV/STD/TB Program Topics of Discussion TB Overview Epidemiology of TB in Oregon Annual Facility
TB Infection Control in Healthcare Settings
 TB Infection Control in Healthcare Settings Wendi K. Drummond DO, MPH Medical Director, Infection Prevention Assistant Professor of Medicine National Jewish Health April 6, 2018 Objectives Understand
TB Infection Control in Healthcare Settings Wendi K. Drummond DO, MPH Medical Director, Infection Prevention Assistant Professor of Medicine National Jewish Health April 6, 2018 Objectives Understand
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE May 8-11, 2018 TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE May 8-11, 2018 TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the
TB Infection Control: Fears and Facts Lisa V. Adams, MD Elizabeth A. Talbot, MD Dartmouth Medical School June 2011
 TB Infection Control: Fears and Facts Lisa V. Adams, MD Elizabeth A. Talbot, MD Dartmouth Medical School June 2011 Outline Background Warm-up with easy myth busting Challenge round myth busting Your participation
TB Infection Control: Fears and Facts Lisa V. Adams, MD Elizabeth A. Talbot, MD Dartmouth Medical School June 2011 Outline Background Warm-up with easy myth busting Challenge round myth busting Your participation
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
TB Infection Control. Carol Staton, RN, BSN March 17, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 TB Infection Control Carol Staton, RN, BSN March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Carol Staton, RN, BSN has the following disclosures
TB Infection Control Carol Staton, RN, BSN March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Carol Staton, RN, BSN has the following disclosures
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Issues in TB Infection Control. Stopping transmission of TB. The Issue: Transmission of TB. TB Infection Control
 Curry International TB Center Issues in TB Infection Control Lisa Chen, MD CITC TB Intensive, Oct. 2017 Stopping transmission of TB TB Infection Control A combination of measures aimed at minimizing the
Curry International TB Center Issues in TB Infection Control Lisa Chen, MD CITC TB Intensive, Oct. 2017 Stopping transmission of TB TB Infection Control A combination of measures aimed at minimizing the
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Transmission, Pathogenesis & Infection Control
 TB Transmission, Pathogenesis & Infection Control Bradley Allen, MD, PhD, FACP, FIDSA. 2014 MFMER slide-1 Disclosures Medical Consultant, TB Control Program Indiana State Department of Health Past clinical
TB Transmission, Pathogenesis & Infection Control Bradley Allen, MD, PhD, FACP, FIDSA. 2014 MFMER slide-1 Disclosures Medical Consultant, TB Control Program Indiana State Department of Health Past clinical
TB Nurse Case Management San Antonio, Texas March 7 9, TB Infection Control Robert Petrossian March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 TB Infection Control Robert Petrossian March 8, 2012 Robert Petrossian has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 TB Infection Control Robert Petrossian March 8, 2012 Robert Petrossian has the following disclosures to make: No conflict of interests No relevant
Pediatric TB Basics and Evaluation and Management of Exposed Neonates
 Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
ICM VI-09 DEFINITION REFERENCES
 TITLE/DESCRIPTION: MANAGEMENT OF SELECTED AIRBORNE AND DROPLET INFECTIOUS DISEASE EXPOSURES IN HEALTHCARE WORKERS INDEX NUMBER: EFFECTIVE DATE: APPLIES TO: ISSUING AUTHORITY: 01/01/2009 01/01/2013 All
TITLE/DESCRIPTION: MANAGEMENT OF SELECTED AIRBORNE AND DROPLET INFECTIOUS DISEASE EXPOSURES IN HEALTHCARE WORKERS INDEX NUMBER: EFFECTIVE DATE: APPLIES TO: ISSUING AUTHORITY: 01/01/2009 01/01/2013 All
"GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES"
 MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow"
MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN INSTITUTIONAL FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow"
POLICY FOR THE PREVENTION AND CONTROL OF TUBERCULOSIS
 POLICY FOR THE PREVENTION AND CONTROL OF TUBERCULOSIS Policy No: 7.20 Approval Date: Review Date: Lead Director: Under Review Under Review Under Review Page 1 of 7 Polic y_for_the_prevention_and_control_of_tuberculosis
POLICY FOR THE PREVENTION AND CONTROL OF TUBERCULOSIS Policy No: 7.20 Approval Date: Review Date: Lead Director: Under Review Under Review Under Review Page 1 of 7 Polic y_for_the_prevention_and_control_of_tuberculosis
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
"GUARDING AGAINST TUBERCULOSIS IN HEALTHCARE FACILITIES"
 MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN HEALTHCARE FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow" Outline
MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS IN HEALTHCARE FACILITIES" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow" Outline
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Improving Tuberculosis Infection Control
 Improving Tuberculosis Infection Control the implementation of HIV/TB collaborative activities in selected African countries Addis Ababa, Nov 13-14, 2008 Nthabiseng Ntlama Deputy TB Program Manager Outline
Improving Tuberculosis Infection Control the implementation of HIV/TB collaborative activities in selected African countries Addis Ababa, Nov 13-14, 2008 Nthabiseng Ntlama Deputy TB Program Manager Outline
Tuberculosis 6/7/2018. Objectives. What is Tuberculosis?
 Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Tuberculosis Understanding, Investigating, Eliminating Jeff Maupin, RN Tuberculosis Control Nurse Sedgwick County Division of Health Objectives At the conclusion of this presentation, you will be able
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Core Curriculum on Tuberculosis: What the Clinician Should Know
 Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
Core Curriculum on Tuberculosis: What the Clinician Should Know Sixth Edition 2013 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Division of Tuberculosis Elimination 1 Chapters
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
TB Infection Control. Delvina Mimi Ford, BSN, RN, CCRN-K, has the following disclosures to make:
 TB Infection Control Delvina Mimi Ford, BSN, RN, CCRN-K September 7, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Delvina Mimi Ford, BSN, RN, CCRN-K,
TB Infection Control Delvina Mimi Ford, BSN, RN, CCRN-K September 7, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Delvina Mimi Ford, BSN, RN, CCRN-K,
TB Infection Control
 TB Infection Control Delvina Mimi Ford, BSN, RN, CCRN K March 7, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Delvina Mimi Ford, BSN, RN, CCRN K has the
TB Infection Control Delvina Mimi Ford, BSN, RN, CCRN K March 7, 2017 TB Nurse Case Management March 7 9, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Delvina Mimi Ford, BSN, RN, CCRN K has the
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
"GUARDING AGAINST TUBERCULOSIS AS A FIRST RESPONDER"
 MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS AS A FIRST RESPONDER" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow" Outline
MAJOR PROGRAM POINTS "GUARDING AGAINST TUBERCULOSIS AS A FIRST RESPONDER" Training For THE CDC "TUBERCULOSIS PREVENTION GUIDELINES" "Quality Safety and Health Products, for Today...and Tomorrow" Outline
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of
 TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
TUBERCULOSIS IN HEALTHCARE SETTINGS Diana M. Nilsen, MD, FCCP Director of Medical Affairs, Bureau of Tuberculosis Control New York City Department of Health and Mental Hygiene TODAY S PRESENTATION Epidemiology
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Guidelines for Preventing the Transmission of M. tuberculosis in Health-Care Settings, Division of Tuberculosis Elimination
 Guidelines for Preventing the Transmission of M. tuberculosis in Health-Care Settings, 2005 Division of Tuberculosis Elimination September 2006 Purpose of 2005 Guidelines Update and replace 1994 Mycobacterium
Guidelines for Preventing the Transmission of M. tuberculosis in Health-Care Settings, 2005 Division of Tuberculosis Elimination September 2006 Purpose of 2005 Guidelines Update and replace 1994 Mycobacterium
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Disclosure. Objectives
 Breaking the Chain of TB Airborne Isolation Regina McDade EdD, MPH, BSN, RN TB Clinical Care Coordinator Jackson Health System Department of Infection Prevention and Control David Ashkin, M.D. FCCP Medical
Breaking the Chain of TB Airborne Isolation Regina McDade EdD, MPH, BSN, RN TB Clinical Care Coordinator Jackson Health System Department of Infection Prevention and Control David Ashkin, M.D. FCCP Medical
Contact Investigation San Antonio, Texas January 14-15, 2013
 Contact Investigation San Antonio, Texas January 14-15, 2013 Assigning Priorities to Contacts Patrick Moonan, PhD, MPH January 14, 2013 Patrick Moonan, PhD, MPH has the following disclosures to make: No
Contact Investigation San Antonio, Texas January 14-15, 2013 Assigning Priorities to Contacts Patrick Moonan, PhD, MPH January 14, 2013 Patrick Moonan, PhD, MPH has the following disclosures to make: No
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Minutes required for removal efficiency ACH 99% 99.9% <1 1
 List Major Errata in Order Importance from the Guidelines for Preventing the Transmission Mycobacterium tuberculosis in Health-care Settings, 2005 http://www.cdc.gov/mmwr/pdf/rr/rr5417.pdf. Major Errata
List Major Errata in Order Importance from the Guidelines for Preventing the Transmission Mycobacterium tuberculosis in Health-care Settings, 2005 http://www.cdc.gov/mmwr/pdf/rr/rr5417.pdf. Major Errata
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
결핵노출접촉자감염관리 서울아산병원감염내과 김성한
 결핵노출접촉자감염관리 서울아산병원감염내과 김성한 TB incidence (2012) TB incidence South Korea 108 China 73 Taiwan 68 Portucal 26 Japan 19 Spain 14 US 3.6 * unit- per 100,000 population Adapted from WHO Adapted from WHO Emerg
결핵노출접촉자감염관리 서울아산병원감염내과 김성한 TB incidence (2012) TB incidence South Korea 108 China 73 Taiwan 68 Portucal 26 Japan 19 Spain 14 US 3.6 * unit- per 100,000 population Adapted from WHO Adapted from WHO Emerg
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Who is at Risk of TB?
 Who is at Risk of TB? Lisa Armitige, MD, PhD September 20, 2017 Screening for Tuberculosis Infection September 20, 2017 Harlingen, TX EXCELLENCE EXPERTISE INNOVATION Lisa Armitige, MD, PhD has the following
Who is at Risk of TB? Lisa Armitige, MD, PhD September 20, 2017 Screening for Tuberculosis Infection September 20, 2017 Harlingen, TX EXCELLENCE EXPERTISE INNOVATION Lisa Armitige, MD, PhD has the following
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
When Can Isolation Be Discontinued?
 When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
When Can Isolation Be Discontinued? - It Depends on the Patient and the Setting. Masae Kawamura M.D. and Barbara Seaworth M.D. Texas: (800) TEX-LUNG New Jersey: 973-972-3270? HNTC Consultation Line California:
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
Contact Investigation Overview
 Contact Investigation Overview Jan Dougan, RN May 4, 2017 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Jan Dougan, RN has the following disclosures to make: No conflict
Contact Investigation Overview Jan Dougan, RN May 4, 2017 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Jan Dougan, RN has the following disclosures to make: No conflict
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 12 PURPOSE To provide guidelines for the prevention and the treatment of tuberculosis (TB) in the N.C. Department of Correction. POLICY The N. C. Department of Correction will abide by this Tuberculosis
PAGE 1 of 12 PURPOSE To provide guidelines for the prevention and the treatment of tuberculosis (TB) in the N.C. Department of Correction. POLICY The N. C. Department of Correction will abide by this Tuberculosis
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...