DPT 772 Spine Notebook Matt Kubalski, SPT
|
|
|
- Kathlyn McDaniel
- 5 years ago
- Views:
Transcription

1 DPT 772 Spine Notebook Matt Kubalski, SPT
2 Table of Contents: IMPAIRMENTS/CLASSIFICATIONS PAGES Neck Pain with Mobility Deficit: Cervicalgia, Pain in thoracic spine - JOSPT 3-6 Neck Pain with Headache: Headache, cervicocranial syndrome JOSPT 7-10 Neck Pain with Movement Coordination Impairments: sprain and strain of C-spine - JOSPT Neck Pain with Radiating Pain: Spondylosis with radiculopathy, cervical disc disorder with radiculopathy - JOSPT Acute/subacute Low Back Pain with Mobility Deficits - JOSPT Acute/subacute/chronic Low Back Pain with Movement Coordination Impairments - JOSPT Acute Low Back Pain with Related (referred) Lower Extremity Pain - JOSPT Acute/subacute/chronic Low Back Pain with Radiating Pain - JOSPT Acute/subacute Low Back Pain with Related Cognitive or Affective Tendencies - JOSPT Chronic Low Back Pain with Related Generalized Pain JOSPT Derangement Syndrome MDT Dysfunction Syndrome MDT Postural Syndrome MDT Various Illustrations of stabilization, progressive loading and MDT exercises Kisner and Wise 58-65
3 Neck Pain with Mobility Deficit: Cervicalgia, Pain in thoracic spine Symptoms: Unilateral neck pain Neck motion limitations Onset of symptoms is often linked to a recent unguarded/awkward movement or position Associated (referred) UE pain may be present Impairments: Limited cervical ROM Neck pain reproduced at end ranges of AROM and PROM Restricted cervical and thoracic segmental mobility Neck and neck-related UE pain reproduced with provocation of the involved cervical or upper thoracic segments Key Concordant Signs: Familiar symptoms (unilateral neck pain, referred UE pain) reproduced with AROM or PROM and provocation of the involved segments Physical Exams to Rule In: Cervical AROM Cervical and thoracic segmental mobility Management for Each Stage of Healing: Cervical and thoracic mobilization/manipulation Stretching exercises Coordination, strengthening, and endurance exercises **See the table below for more details** Phases of Rehabilitation Intervention Kinesthetic awareness Proprioce ption training of safe movemen t and postures Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Cervical retraction: passive active assist in comfortable positions Awareness of what makes symptoms better vs. worse Learn neutral spine (or bias) Basic Training/Controlled motion Phase Moderate to minimum protection Active cervical control in various positions supine, prone, quadruped, sitting, standing Have patient practice moving into and out of cervical retraction to develop control Dynamic maintenance of pain-free position with activities Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine (cervical retraction) in all functional activities Return to normal ADLs, activities, work, function
4 Mobility/flexibilit y Move, stretch, manipulat e restricting tissues Muscle performance Stabilizati on training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Cervical and thoracic PA mobilizations grades 1 and 2 for pain control Gentle stretching of tight musculature/tissue in pain-free range Activation of deep neck flexor musculature using The Stabilizer biofeedback device: patient supine hold 10 seconds x 10 repetitions for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to 90, shoulder abduction to 90, and shoulder external rotation with arms at sides) Activation of cervical and thoracic extensors: patient prone, lift forehead off exercise mat and hold for 10 seconds x 10 repetitions for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off Cervical and thoracic mobilizations grade 3 to increase segmental mobility Gentle stretching of tight musculature/tissue and spinal movement into painful range Teach self-stretching exercises for cervical and thoracic spine (upper trapezius, scalenes, thoracic spine, suboccipital muscles) Muscle energy techniques to increase rotation for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to end range, shoulder ABD combined with ER to end range, diagonal PNF patterns) for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (elevate shoulder in full flexion, arms ABD to 90 and laterally rotated, elbows extended: horizontally ABD shoulders and ABB scapulae, UE diagonal PNF patterns) Cervical and thoracic mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities in painful/end range positions for cervical flexors progressing supine sitting stan ding with wall support standing with no support (reaching forward, outward, upward in functional patterns, pushing/puling and lifting activities) for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (reaching forward, outward, upward in functional patterns, pushing/pulling and lifting activities) Intermediate and advanced training transitional stabilization for the cervical and upper
5 table quadruped s tanding with wall support standing no support (arms at side: laterally rotate shoulders and adduct scapulae) Isometric exercises for cervical flexion, extension, rotation and sidebending. Dynamic cervical flexion thoracic regions (exercise ball roll out) Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, communit y, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use
6 common sense and follow good safety habits, review the HEP)
7 Neck Pain with Headache: Headache, cervicocranial syndrome Symptoms: Non-continuous, unilateral neck pain and associated (referred) headache Headache is precipitated or aggravated by neck movements or sustained positions Impairments: Headache reproduced with provocation of the involved upper cervical segments Limited cervical range of motion Restricted upper cervical segmental mobility Strength and endurance deficits of the deep neck flexor muscles Key Concordant Signs: Familiar symptoms (neck pain, headache) reproduced with provocation of the involved segments Physical Exams to Rule In: Cervical AROM Cervical segmental mobility (PA mobs) Cranial cervical flexion test Management for Each Stage of Healing: Cervical mobilization/manipulation Stretching exercises Coordination, strengthening, and endurance exercises **See the table below for more details** Phases of Rehabilitation Intervention Kinesthetic awareness Proprioce ption training of safe movemen t and postures Mobility/flexibilit y Move, stretch, manipulat e restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Cervical retraction: passive active assist active in comfortable positions Awareness of what makes symptoms better vs. worse Learn neutral spine (or bias) Cervical PA mobilizations grades 1 and 2 for pain control Gentle suboccipital release/traction Gentle stretching of tight musculature/tissue in pain-free range Basic Training/Controlled motion Phase Moderate to minimum protection Active cervical control in various positions supine, prone, quadruped, sitting, standing Have patient practice moving into and out of cervical retraction to develop control Dynamic maintenance of pain-free position with activities Cervical grade 3 to increase segmental mobility Suboccipital release/traction Gentle stretching of tight musculature/tissue and spinal movement into painful range Teach self-stretching exercises for cervical and thoracic spine (upper trapezius, Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine (cervical retraction) in all functional activities Return to normal ADLs, activities, work, function Cervical mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities in painful/end range positions
8 scalenes, thoracic spine, suboccipital muscles) Muscle performance Stabilizati on training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of deep neck flexor musculature using The Stabilizer biofeedback device: patient supine hold 10 seconds x 10 repetitions for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to 90, shoulder abduction to 90, and shoulder external rotation with arms at sides) Activation of cervical and thoracic extensors: patient prone, lift forehead off exercise mat and hold for 10 seconds x 10 repetitions for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (arms at side: laterally rotate shoulders and adduct scapulae) for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to end range, shoulder ABD combined with ER to end range, diagonal PNF patterns) for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (elevate shoulder in full flexion, arms ABD to 90 and laterally rotated, elbows extended: horizontally ABD shoulders and ABB scapulae, UE diagonal PNF patterns) Dynamic cervical flexion for cervical flexors progressing supine sitting stan ding with wall support standing with no support (reaching forward, outward, upward in functional patterns, pushing/puling and lifting activities) for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (reaching forward, outward, upward in functional patterns, pushing/pulling and lifting activities) Intermediate and advanced training transitional stabilization for the cervical and upper thoracic regions (exercise ball roll out)
9 Isometric exercises for cervical flexion, extension, rotation and sidebending. Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, communit y, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use
10 common sense and follow good safety habits, review the HEP)
11 Neck Pain with Movement Coordination Impairments: sprain and strain of C-spine Symptoms: Neck pain and associated (referred) UE pain Symptoms are often linked to a precipitating trauma/whiplash and may be present for an extended period of time Impairments: Strength, endurance, and coordination deficits of the deep neck flexor muscles Neck pain with mid-range motion that worsens with end range movements or positions Neck and neck-related UE pain reproduced with provocation of the involved cervical segment(s) Cervical instability may be present (note that muscle spasm adjacent to the involved cervical segment(s) may prohibit accurate testing) Key Concordant Signs: Familiar symptoms (neck pain, referred UE pain) reproduced with mid-range to end-range motion and provocation of the involved cervical segments Physical Exams to Rule In: Cranial cervical flexion test Deep neck flexor endurance Management for Each Stage of Healing: Coordination, strengthening, and endurance exercises Patient education and counseling Stretching exercises **See the table below for more details** Phases of Rehabilitation Intervention Kinesthetic awareness Proprioce ption training of safe movemen t and postures Mobility/flexibilit y Move, stretch, manipulat e restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Cervical retraction: passive active assist active in comfortable positions Awareness of what makes symptoms better vs. worse Learn neutral spine (or bias) Gentle suboccipital release/traction Gentle stretching of tight musculature/tissue in pain-free range Basic Training/Controlled motion Phase Moderate to minimum protection Active cervical control in various positions supine, prone, quadruped, sitting, standing Have patient practice moving into and out of cervical retraction to develop control Dynamic maintenance of pain-free position with activities Suboccipital release/traction Gentle stretching of tight musculature/tissue and spinal movement into painful range Teach self-stretching exercises for cervical and thoracic spine (upper trapezius, scalenes, thoracic Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine (cervical retraction) in all functional activities Return to normal ADLs, activities, work, function Continue to stretch tight tissue and perform exercises/activities in painful/end range positions
12 spine, suboccipital muscles) Muscle performance Stabilizati on training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of deep neck flexor musculature using The Stabilizer biofeedback device: patient supine hold 10 seconds x 10 repetitions for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to 90, shoulder abduction to 90, and shoulder external rotation with arms at sides) Possibly Extensors - Activation of cervical and thoracic extensors: patient prone, lift forehead off exercise mat and hold for 10 seconds x 10 repetitions Possibly Extensors - Stabilization exercises for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (arms at side: laterally rotate for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to end range, shoulder ABD combined with ER to end range, diagonal PNF patterns) Possibly Extensors - Stabilization exercises for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (elevate shoulder in full flexion, arms ABD to 90 and laterally rotated, elbows extended: horizontally ABD shoulders and ABB scapulae, UE diagonal PNF patterns) Dynamic cervical flexion for cervical flexors progressing supine sitting stan ding with wall support standing with no support (reaching forward, outward, upward in functional patterns, pushing/puling and lifting activities) Possibly Extensors - Stabilization exercises for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (reaching forward, outward, upward in functional patterns, pushing/pulling and lifting activities) Intermediate and advanced training transitional stabilization for the cervical and upper thoracic regions (exercise ball roll out)
13 shoulders and adduct scapulae) Isometric exercises for cervical flexion, extension, rotation and sidebending. Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, communit y, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use
14 common sense and follow good safety habits, review the HEP)
15 Neck Pain with Radiating Pain: Spondylosis with radiculopathy, cervical disc disorder with radiculopathy Symptoms: Neck pain with associated radiating (narrow band of lancinating) pain in the involved upper extremity Upper extremity paresthesias, numbness, and weakness may be present Impairments: Neck and neck-related radiating pain reproduced with: o 1. Cervical extension, sidebending, and rotation toward the involved side (Spurling s test) o 2. Upper limb tension testing Neck and neck-related radiating pain relieved with cervical distraction May have upper extremity sensory, strength, or reflex deficits associated with the involved nerve(s) Key Concordant Signs: Familiar symptoms (neck pain, upper extremity symptoms) reproduced with cervical extension, sidebending, and/or rotation Physical Exams to Rule In: Upper limb tension test Spurling s test Management for Each Stage of Healing: Distraction test Upper quarter and nerve mobilization procedures Traction Thoracic mobilization/manipulation **See the table below for more details** Phases of Rehabilitation Intervention Kinesthetic awareness Proprioce ption training of safe movemen t and postures Mobility/flexibilit y Move, stretch, manipulat e restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Cervical retraction: passive active assist active in comfortable positions Awareness of what makes symptoms better vs. worse Learn neutral spine (or bias) Thoracic mobilizations grades 1 and 2 Gentle suboccipital/cervical traction Gentle stretching of tight musculature/tissue in pain-free range Basic Training/Controlled motion Phase Moderate to minimum protection Active cervical control in various positions supine, prone, quadruped, sitting, standing Have patient practice moving into and out of cervical retraction to develop control Dynamic maintenance of pain-free position with activities Thoracic mobilizations grade 3 Suboccipital/cervical traction Gentle stretching of tight musculature/tissue and spinal movement into painful range Teach self-stretching exercises for cervical, Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine (cervical retraction) in all functional activities Return to normal ADLs, activities, work, function Thoracic mobilization grade 4 and manipulation Continue to stretch tight tissue and perform exercises/activities in painful/end range positions
16 Gentle nerve mobilization techniques thoracic spine and involved upper extremity (upper trapezius, scalenes, thoracic spine, suboccipital muscles, tight UE musculature) Progressive nerve mobilization techniques Progress nerve mobilization to end ranges Muscle performance Stabilizati on training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of deep neck flexor musculature using The Stabilizer biofeedback device: patient supine hold 10 seconds x 10 repetitions for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to 90, shoulder abduction to 90, and shoulder external rotation with arms at sides) Activation of cervical and thoracic extensors: patient prone, lift forehead off exercise mat and hold for 10 seconds x 10 repetitions for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (arms at side: laterally rotate shoulders and adduct scapulae) for cervical flexors progressing supine sitting stan ding with wall support standing with no support (shoulder flexion to end range, shoulder ABD combined with ER to end range, diagonal PNF patterns) for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (elevate shoulder in full flexion, arms ABD to 90 and laterally rotated, elbows extended: horizontally ABD shoulders and ABB scapulae, UE diagonal PNF patterns) Dynamic cervical flexion for cervical flexors progressing supine sitting stan ding with wall support standing with no support (reaching forward, outward, upward in functional patterns, pushing/puling and lifting activities) for cervical and thoracic extensors progressing prone forehead on treatment table and lift forehead off table quadruped s tanding with wall support standing no support (reaching forward, outward, upward in functional patterns, pushing/pulling and lifting activities) Intermediate and advanced training transitional stabilization for the cervical and upper thoracic regions (exercise ball roll out)
17 Isometric exercises for cervical flexion, extension, rotation and sidebending. Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, communit y, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use
18 common sense and follow good safety habits, review the HEP)
19 Acute/Subacute Low Back Pain with Mobility Deficits Symptoms: Acute/subacute low back, buttock, or thigh pain Unilateral pain Onset of symptoms is often linked to a recent unguarded/awkward movement or position May report sensation of back stiffness Impairments: Acute: Lumbar ROM limitations Restricted lower thoracic and lumbar segmental mobility Low back and low back-related LE symptoms are reproduced with provocation of the involved lower thoracic, lumbar, or sacroiliac segments Subacute: Symptoms reproduced with end-range spinal motions Symptoms reproduced with provocation of the involved lower thoracic, lumbar, or sacroiliac segments. Presence of 1 or more of the following: o Restricted thoracic ROM and associated segmental mobility o Restricted lumbar ROM and associated segmental mobility o Restricted lumbopelvic or hip ROM and associated accessory mobility Key Concordant Signs: Acute: Acute low back, buttock, or thigh pain (duration of 1 month or less) Subacute: Subacute, unilateral, low back, buttock, or thigh pain Physical Exams to Rule In: AROM for thoracic and lumbar spine and hip, PA mobs for segmental mobility Management for Each Stage of Healing: and symptom provocation, PROM hip motion Acute: Manual therapy procedures (thrust manipulation and other non-thrust mobilization techniques) to diminish pain and improve segmental spinal or lumbopelvic motion Therapeutic exercises to improve or maintain spinal mobility Patient education that encourages the patient to return to or pursue an active lifestyle Subacute: Manual therapy procedures to improve segmental spinal, lumbopelvic, and hip mobility Therapeutic exercises to improve or maintain spinal and hip mobility Focus on preventing recurring low back pain episodes through the use of (1) therapeutic exercises that address coexisting coordination impairments strength deficits, and endurance deficits, and (2) education that encourages the patient to pursue or maintain an active lifestyle **See the table below for more details**
20 Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Mobility/flexibility Move, stretch, manipulate restricting tissues Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) Lumbar and thoracic PA mobilizations grades 1 and 2 for pain control Gentle stretching of tight musculature/tissue in pain-free range in low back and hips Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Lumbar and thoracic mobilizations grade 3 to increase segmental mobility Gentle stretching of tight musculature/tissue and spinal movement into painful range for low back and hips Teach selfstretching exercises exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function Lumbar and thoracic mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities in painful/end range positions exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement
21 exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient
22 Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
23 Acute/Subacute/Chronic Low Back Pain with Movement Coordination Impairments Symptoms: Acute: Acute exacerbation of recurring low back pain that is commonly associated with referred LE pain Symptoms often include numerous episodes of low back and/or low backrelated lower extremity pain in recent years Subacute: Subacute, recurring low back pain that is commonly associated with referred LE pain Symptoms often include numerous episodes of low back and/or low back related LE pain in recent years Chronic: Chronic, recurring low back pain and associated (referred) LE pain Impairments: Acute: Low back and/or low back related LE pain at rest or produced with initial to mid range spinal movements Low back and/or low back related LE pain reproduced with provocation of the involved lumbar segment(s) Movement coordination impairments of the lumbopelvic region with low back flexion and extension movements Subacute: Lumbosacral pain with mid range motions that worsen with end range movements or positions Low back and low back related LE pain reproduced with provocation of the involved lumbar segment(s) Lumbar hypermobility with segmental mobility assessment may be present Mobility deficits of the thorax and/or lumbopelvic/hip regions Diminished trunk or pelvic region muscle strength and endurance Movement coordination impairments while performing self-care/home management activities Chronic: Presence of 1 or more of the following: o Low back and/or low back related LE pain that worsens with sustained end range movements or positions o Lumbar hypermobility with segmental motion assessment o Mobility deficits of the thorax and lumbopelvic/hip regions o Diminished trunk or pelvic region muscle strength and endurance o Movement coordination impairments while performing community/work related recreational or occupational activities Key Concordant Signs: Acute: Familiar symptoms (acute exacerbation of recurring low back pain and referred LE pain) reproduced with initial to mid-range spinal movements and provocation of the involved lumbar segment(s). Subacute: Familiar symptoms (subacute exacerbation of recurring low back pain and referred LE pain) reproduced with mid-range motions that worsen with end range movements or positions and provocation of the involved lumbar segment(s). Chronic: Familiar symptoms (chronic recurring low back pain and referred LE pain) reproduced with sustained end range movements or positions.
24 Physical Exams to Rule In: AROM of thoracic and lumbar spine and hip, PA mobs for segmental mobility and symptom provocation, observation for aberrant motion, trunk and pelvic region muscle strength and endurance tests, prone instability test, PROM hip motions Management for Each Stage of Healing: Acute: Neuromuscular re-education to promote dynamic (muscular) stability to maintain the involved lumbosacral structures in less symptomatic, mid-range positions. Consider the use of temporary external devices to provide passive restraint to maintain the involved lumbosacral structures in less symptomatic, mid-range positions Self-care/home management training pertaining to (1) postures and motions that maintain the involved spinal structures in neutral, symptom-alleviating positions, and (2) recommendations to pursue or maintain an active lifestyle Subacute: Neuromuscular re-education to promote dynamic (muscular) stability to maintain the involved lumbosacral structures in less symptomatic, mid-range positions during self-care related functional activities. Manual therapy procedures and therapeutic exercises to address identified thoracic spine, ribs, lumbopelvic, or hip mobility deficits. Therapeutic exercises to address trunk and pelvic-region muscle strength and endurance deficits Self-care/home management training in maintaining the involved structures in mid-range, less symptom-producing positions Initiate community/work reintegration training in pain management strategies while returning to community/work activities. Chronic: Neuromuscular re-education to promote dynamic (muscular) stability to maintain the involved lumbosacral structures in less symptomatic, mid-range positions during household, occupational or recreational activities. The rest is the same as subacute. **See the table below for more details**
25 Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Mobility/flexibility Move, stretch, manipulate restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) Lumbar and thoracic PA mobilizations grades 1 and 2 for pain control Gentle stretching of tight musculature/tissue in pain-free range in low back and hips Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Lumbar and thoracic mobilizations grade 3 to increase segmental mobility Gentle stretching of tight musculature/tissue and spinal movement into painful range for low back and hips Teach selfstretching exercises Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function Lumbar and thoracic mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities in painful/end range positions Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance)
26 bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient
27 Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
28 Acute Low Back Pain with Related (referred) Lower Extremity Pain Symptoms: Acute low back pain that is commonly associated with referred buttock, thigh, or leg pain Symptoms are often worsened with flexion activities and sitting Impairments: Low back and LE pain that can be centralized and diminished with specific postures and/or repeated movements Reduced lumbar lordosis Limited lumbar extension mobility Lateral trunk shift may be present Clinical findings consistent with subacute or chronic low back pain with movement coordination impairments classification criteria Key Concordant Signs: Familiar symptoms (acute low back pain, referred buttock, thigh, or leg pain) reproduced with flexion activities and sitting Physical Exams to Rule In: AROM of trunk, repeated motions of trunk and postures looking for centralized/diminished symptoms, observation for lateral trunk shift, PA mobs for lumbar spine for segmental mobility and symptom provocation, trunk muscle power and endurance tests Management for Each Stage of Healing: Therapeutic exercises, manual therapy, or traction procedures that promote centralization and improve lumbar extension mobility Patient education in positions that promote centralization Progress to interventions consistent with the Subacute or Chronic Low Back Pain with Movement Coordination Impairments intervention strategies **See the table below for details** Phases of Rehabilitation Intervention Kinesthetic awareness Propriocepti on training of safe movement and postures Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movemen ts) makes symptoms better vs. worse Learn neutral spine (or bias) Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function
29 Mobility/flexibility Move, stretch, manipulate restricting tissues Lumbar PA mobilizations grades 1 and 2 for pain control Gentle stretching of tight musculature/tissue in pain-free range in low back and hips Gentle hip side glides if lateral shift is present Repeated motions/stretching in the direction that diminishes symptoms in painfree range Lumbar and mobilizations grade 3 to increase segmental mobility Gentle stretching of tight musculature/tissu e and spinal movement into painful range for low back and hips Repeated motions/stretchin g in direction that diminishes symptoms Teach selfstretching exercises Hip side glides if lateral shift present Lumbar mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities/repea ter motions in painful/end range positions Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions exercises TA: patient supine bent leg fallout with TA activation exercises trunk extensors/multifidus : quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifid us starting quadruped than progressing to prone. Quadruped progression: flex (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement for trunk extensors/multifidus starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE
30 one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient
31 Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, pushups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
32 Acute/Subacute/Chronic Low Back Pain with Radiating Pain Symptoms: Acute: Acute low back pain with associated radiating (narrow band of lancinating) pain in the involved LE LE paresthesias, numbness, and weakness may be reported Subacute: Subacute, recurring, mid-back and/or low back pain with associated radiating pain in the involved LE LE paresthesias, numbness, and weakness may be reported Chronic: Chronic, recurring, mid- and/or low back pain with associated radiating pain in the involved lower extremity LE paresthesias, numbness, and weakness may be reported Impairments: Acute: LE radicular symptoms that are present at rest or produced with initial to midrange spinal mobility, lower limb tension tests/straight leg raising, and/or slump tests Signs of nerve root involvement may be present It is common for the symptoms and impairments of body function in patients who have acute low back pain with radiating pain to also be present in patients who have acute low back pain with related (referred) lower extremity pain Subacute: Mid-back, low back, and back-related radiating pain or paresthesia that are reproduced with mid-range and worsen with end range: o Lower limb tension testing/straight leg raising tests, and/or.. o Slump tests o May have LE sensory, strength, or reflex deficits associated with the involved nerve(s) Chronic: Mid-back, low back, or LE pain or paresthesias that are reproduced with sustained end-range lower-limb tension tests and/or slump tests Signs of nerve root involvement may be present Key Concordant Signs: Acute: Familiar symptoms of acute low back pain with associated radiating pain the involved LE, as well as LE paresthesias, numbness, and weakness. Symptoms reproduced with initial to mid-range spinal mobility, lower-limb tension/straight leg raising and or slump tests. Signs of nerve root involvement may be present. Subacute: Familiar symptoms of subacute, recurring mid-back and/or low back pain with associated radiating pain and potential sensory, strength or reflex deficits in the involved LE. Symptoms reproduced with mid-range and worsen with end range lower-limb tension/straight leg raising and/or slump tests. Chronic: Familiar symptoms of chronic, recurring mid-back and/or low back pain with associated radiating pain and potential sensory, strength or reflex deficits in the involved LE. Symptoms reproduced with sustained end range lower-limb tension/straight leg raising and/or slump tests. Physical Exams to Rule In: Trunk AROM with repeated movements, lower limb tension tests, straight leg raise, slump test, myotomes, dermatomes, reflexes Management for Each Acute: Stage of Healing: Patient education in positions that reduce strain or compression to the involved nerve root(s) or nerves Manual or mechanical traction
33 Manual therapy to mobilize the articulations and soft tissues adjacent to the involved nerve root(s) or nerves that exhibit mobility deficits Nerve mobility exercises in the pain-free, non symptom-producing ranges to improve the mobility of central (dural) and peripheral neural elements Subacute: Manual therapy to mobilize the articulations and soft tissues adjacent to the involved nerve root(s) or nerves that exhibit mobility deficits Manual or mechanical traction Nerve mobility and slump exercises in the mid- to end ranges to improve the mobility of central (dural) and peripheral neural elements Chronic Manual therapy and therapeutic exercises to address thoracolumbar and lowerquarter nerve mobility deficits Patient education pain management strategies **See below for more details** Phases of Rehabilitation Intervention Kinesthetic awareness Propriocepti on training of safe movement and postures Mobility/flexibility Move, stretch, manipulate restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movemen ts) makes symptoms better vs. worse Learn neutral spine (or bias) Lumbar PA mobilizations grades 1 and 2 for pain control Gentle passive stretching of tight musculature/tissue in pain-free range of LE Gentle repeated AROM of trunk in direction that Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Lumbar PA mobilizations grade 3 for segmental mobility Active stretching of tight musculature/tissu e and spinal movement into painful range for LE Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function Lumbar mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities/repea ter motions in painful/end range positions Continue LE nerve mobilization techniques
34 Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power diminishes symptoms Gentle LE nerve mobilization techniques for sciatic and/or femoral nerves Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions exercises TA: patient supine bent leg fallout with TA activation exercises trunk extensors/multifidus : quadruped unilateral arm raise or unilateral leg extension Repeated AROM of trunk in direction that diminishes symptoms Teach selfstretching exercises for LE LE nerve mobilization techniques for sciatic and/or femoral nerves exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifid us starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE for sciatic and/or femoral nerves (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement for trunk extensors/multifidus starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface
35 lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, pushups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal
36 Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
37 Acute/Subacute Low Back Pain with Related Cognitive or Affective Tendencies Symptoms: Acute or subacute low back and/or low back-related LE pain Impairments: One or more of the following: o Two positive responses to Primary Care Evaluation of Mental Disorders screen and affect consistent with an individual who is depressed o High scores on the Fear-Avoidance Beliefs Questionnaire and behavioral processes consistent with an individual who has excessive anxiety or fear o High scores on the pain Catastrophizing Scale and cognitive process consistent with rumination, pessimism, or helplessness Key Concordant Signs: Familiar symptoms of acute or subacute low back and/or low back-related LE pain along with presence of depression, fear-avoidance beliefs, and/or pain catastrophizing Physical Exams to Rule In: Trunk AROM, PA mobs for segmental mobility and symptom provocation, observation of aberrant motion, trunk muscle power and endurance tests, Management for Each Stage of Healing: PROM hip motions. Patient education and counseling to address specific classification exhibited by the patient (ie, depression, fear-avoidance, pain catastrophizing) **See the table below for details** Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function
38 Mobility/flexibility Move, stretch, manipulate restricting tissues Lumbar PA mobilizations grades 1 and 2 for pain control Gentle passive stretching of tight musculature/tissue in pain-free range of low back and hips Lumbar PA mobilizations grade 3 for segmental mobility Active stretching of tight musculature/tissue and spinal movement into painful range for low back and hips Lumbar mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities in painful/end range positions for low back and hips Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table
39 Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid
40 adaptations, load position, ergonomic changes to work and home postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
41 Chronic Low Back Pain with Related Generalized Pain Symptoms: Low back and/or low back-related LE pain with symptom duration for longer than 3 months Generalized pain not consistent with other impairment-based classification criteria presented in these clinical guidelines Impairments: One or more of the following: o Two positive responses to Primary Care Evaluation of Mental Disorders screen and affect consistent with an individual who is depressed o High scores on the Fear-Avoidance Beliefs Questionnaire and behavioral processes consistent with an individual who has excessive anxiety or fear o High scores on the pain Catastrophizing Scale and cognitive process consistent with rumination, pessimism, or helplessness Key Concordant Signs: Familiar symptoms of low back and/or low back-related LE pain lasting longer than 3 months and generalized pain not consistent with other impairment based classification criteria along with a presence of depression, fear-avoidance beliefs, and/or pain catastrophizing. Physical Exams to Rule In: Trunk AROM, PA mobs for segmental mobility and symptom provocation, observation of aberrant motion, trunk muscle power and endurance tests, PROM hip motions. Management for Each Stage of Healing: Patient education and counseling to address specific classification exhibited by the patient (ie, depression, fear-avoidance, pain catastrophizing) Low-intensity, prolonged (aerobic) exercise activities **See the table below** Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function
42 Mobility/flexibility Move, stretch, manipulate restricting tissues Lumbar PA mobilizations grades 1 and 2 for pain control Gentle passive stretching of tight musculature/tissue in pain-free range of low back and hips Lumbar PA mobilizations grade 3 for segmental mobility Active stretching of tight musculature/tissue and spinal movement into painful range for low back and hips Lumbar mobilizations and manipulation grades IV and thrust to increase segmental mobility Continue to stretch tight tissue and perform exercises/activities in painful/end range positions for low back and hips Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table
43 Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid
44 adaptations, load position, ergonomic changes to work and home postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
45 McKenzie - Derangement Symptoms: Constant or intermittent pain in low back and referred buttock or LE symptoms Can be acute, subacute, or chronic with either a gradual or sudden onset. Variable symptoms with rapid changes. Centralization of symptoms only in this classification of MDT Impairments: Neurological: motor or sensory deficits, abnormal reflexes and dural signs Trunk range of motion loss obstructed in either flexion or extension Restrictions in joint segmental mobility Possible trunk lateral shift Pain during movement and end range pain. Key Concordant Signs: Familiar symptoms of constant or intermittent low back pain and referred buttock/le symptoms that are reproduced during either trunk flexion or extension and are centralized with the opposite movement Physical Exams to Rule In: AROM of trunk, PA mobs for segmental mobility, neurological screen, repeated test movements, sustained postures, slump test, straight leg raise, lower limb tension tests Management for Each See the table below for details Stage of Healing: Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Mobility/flexibility Move, stretch, manipulate restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) Posterior Derangement- Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Lying prone with arms relaxed at side lying prone in extension, elbows propped up underneath body extension in lying, Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities Posterior Derangement- Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Lying prone with arms relaxed at side lying prone in extension, elbows propped up underneath body Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function Posterior Derangement- Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Lying prone with arms relaxed at side lying prone in extension, elbows propped up underneath body
46 patient props themselves up actively until elbows are fully extended extension in lying with selfoverpressure, lock elbows fully while exhaling and letting abdomen sag extension in standing varying degrees of extension in lying with clinician overpressure progressing towards end range extension passive extension mobilizations Posterior Derangement w/ lateral component Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Extension in lying (EIL) with hips off center away from pain EIL with hips off center with lateral overpressure by clinician side glide in standing (SGIS) rotation mobilization in extension rotation mobilization in flexion Anterior Derangement Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Flexion in lying (FIL) Flexion in sitting flexion in standing flexion in step standing flexion in extension in lying, patient props themselves up actively until elbows are fully extended extensio n in lying with selfoverpressure, lock elbows fully while exhaling and letting abdomen sag extension in standing varying degrees of extension in lying with clinician overpressure progressing towards end range extension passive extension mobilizations Posterior Derangement w/ lateral component Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Extension in lying (EIL) with hips off center away from pain EIL with hips off center with lateral overpressure by clinician side glide in standing (SGIS) rotation mobilization in extension rotation mobilization in flexion Anterior Derangement Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Flexion in lying (FIL) Flexion in sitting flexion in standing flexion in extension in lying, patient props themselves up actively until elbows are fully extended extensio n in lying with selfoverpressure, lock elbows fully while exhaling and letting abdomen sag extension in standing varying degrees of extension in lying with clinician overpressure progressing towards end range extension passive extension mobilizations Posterior Derangement w/ lateral component Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Extension in lying (EIL) with hips off center away from pain EIL with hips off center with lateral overpressure by clinician side glide in standing (SGIS) rotation mobilization in extension rotation mobilization in flexion Anterior Derangement Progression of forces: (type of progression dependent on patient tolerance and symptom presentation. Starting point different for each patient) Flexion in lying (FIL) Flexion in sitting flexion in standing flexion in
47 lying with clinician overpressure step standing flexion in lying with clinician overpressure step standing flexion in lying with clinician overpressure Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidus starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidus starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface,
48 curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from
49 prolonged postures, avoid spinal postures at end range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
50 McKenzie - Dysfunction Symptoms: Intermittent low back pain. May have referred buttock and LE symptoms if there is an adherent nerve root. Pain caused by presence of adaptively shortened tissue and pain occurs when these tissues are stretched Chronic condition with a gradual onset unless ANR was caused by a trauma or injury Symptoms are consistent with no rapid changes Impairments: Trunk range of motion loss in either flexion or extension restricted Pain at end range movements of flexion or extension or in prolonged positions Positive dural signs with ANR Restrictions in joint segmental mobility Key Concordant Signs: Familiar symptoms of intermittent low back pain at end range flexion or extension during prolonged positions Familiar symptoms of LE pain and numbness, tingling, paresthesias for ANR Physical Exams to Rule In: AROM of trunk to end range, PA mobs for segmental mobility, sustained postures. For ANR: neurological screen, slump test, straight leg raise, lower limb tension tests, flexion in standing and flexion in lying. Management for Each See the table below for details Stage of Healing: Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Mobility/flexibility Move, stretch, manipulate restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) Flexion Dysfunction: Flexion in lying (FIL) Flexion in sitting flexion in standing flexion in step standing and possibly flexion in lying with clinician overpressure Extension Dysfunction: Lying prone with arms relaxed at side lying Basic Training/Controlled motion Phase Moderate to minimum protection Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Flexion Dysfunction: Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function Flexion Dysfunction: Flexion in lying (FIL) Flexion in sitting flexion in standing flexion in step standing and possibly flexion in lying with clinician overpressure Extension Dysfunction: Lying prone with arms relaxed at side Flexion Dysfunction: Flexion in lying (FIL) Flexion in sitting flexion in standing flexion in step standing and possibly flexion in lying with clinician overpressure Extension Dysfunction: Lying prone with arms relaxed at side
51 prone in extension, elbows propped up underneath body extension in lying, patient props themselves up actively until elbows are fully extended extension in lying with selfoverpressure, lock elbows fully while exhaling and letting abdomen sag extension in standing and possibly varying degrees of extension in lying with clinician overpressure progressing towards end range extension and possibly passive extension mobilizations Side Gliding Dysfunction: Progressive side bending into direction of restriction to improve ROM ANR Dysfunction: Flexion in lying extension in lying flexion in step standing flexion in standing *** Progressive movement in direction of restriction (flexion, extension, side gliding, ANR). Improve motion gradually and assess symptoms during and after motion. Exercises performed 10 times every 2-3 waking hours. Move into ROM where symptoms are reproduced*** lying prone in extension, elbows propped up underneath body extension in lying, patient props themselves up actively until elbows are fully extended extensio n in lying with selfoverpressure, lock elbows fully while exhaling and letting abdomen sag extension in standing and possibly varying degrees of extension in lying with clinician overpressure progressing towards end range extension and possibly passive extension mobilizations Side Gliding Dysfunction: Progressive side bending into direction of restriction to improve ROM ANR Dysfunction: Flexion in lying extension in lying flexion in step standing flexion in standing *** Progressive movement in direction of restriction (flexion, extension, side gliding, ANR). Improve motion gradually and assess symptoms during and after motion. Exercises performed 10 times every 2-3 waking hours. Move into ROM where symptoms are reproduced*** lying prone in extension, elbows propped up underneath body extension in lying, patient props themselves up actively until elbows are fully extended extensio n in lying with selfoverpressure, lock elbows fully while exhaling and letting abdomen sag extension in standing and possibly varying degrees of extension in lying with clinician overpressure progressing towards end range extension and possibly passive extension mobilizations Side Gliding Dysfunction: Progressive side bending into direction of restriction to improve ROM ANR Dysfunction: Flexion in lying extension in lying flexion in step standing flexion in standing *** Progressive movement in direction of restriction (flexion, extension, side gliding, ANR). Improve motion gradually and assess symptoms during and after motion. Exercises performed 10 times every 2-3 waking hours. Move into ROM where symptoms are reproduced***
52 Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidus starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidus starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, quadratus
53 lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end
54 range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)
55 McKenzie - Postural Symptoms: Acute, intermittent, localized low back pain during sustained end-range positioning Condition is a gradual onset Impairments: Lumbar pain experienced during prolonged static loading at end range (Physical examination normal with no reproduction of symptoms in response to single or repeated movements. Normal range of motion) Poor static posture (standing or seated) Key Concordant Signs: Familiar symptoms of localized low back pain that are reproduced during sustained static end-range positioning Physical Exams to Rule In: Observation of posture, static loading at end range positions Management for Each Stage of Healing: See the table below for details Phases of Rehabilitation Intervention Kinesthetic awareness Proprioceptio n training of safe movement and postures Mobility/flexibility Move, stretch, manipulate restricting tissues Early Training/Protection Phase Maximum to moderate protection of injured area, pathologically involved tissues, or painful region Pelvic tilt: passive active assist active. Teach the patient to move his or her pelvis in an anterior and posterior pelvic tilt in a comfortable range Awareness of what (postures/movements ) makes symptoms better vs. worse Learn neutral spine (or bias) ***Mobility and flexibility should be WNL in examination for postural syndrome. Continue to give postural education and stretch any tissues that you find restricted in examination*** Basic Training/Controlled motion Phase Moderate to minimum protection Active spinal control in various positions supine, prone, quadruped, sitting, standing Dynamic maintenance of pain-free position with activities ***Mobility and flexibility should be WNL in examination for postural syndrome. Continue to give postural education and stretch any tissues that you find restricted in examination*** Intermediate to Advanced Training/Return to Function Phase Minimum to no protection Habitual use of neutral spine in all functional activities Return to normal ADLs, activities, work, function ***Mobility and flexibility should be WNL in examination for postural syndrome. Continue to give postural education and stretch any tissues that you find restricted in examination***
56 Muscle performance training (deep muscles for segmental stability, global muscles for general stability) Muscle endurance Strength and power Activation of TA and multifidus using The Stabilizer biofeedback device: hold 10 seconds x 10 repetitions TA: patient supine bent leg fallout with TA activation trunk extensors/multifidus: quadruped unilateral arm raise or unilateral leg extension exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Intermediate training: curl-ups, curl-downs, diagonal curl-up, double knee to chest, pelvic lifts, bilateral straight leg raising/lowering, thoracic elevation, leg lifts, superman, quadratus lumborum side plank exercises (lift bent leg to 90 hip flexion, slide heel, lift straight leg to 45 ) with patient supine for TA progressing: opposite LE on mat; bent leg fall out opposite LE on table holding opposite 90 of hip flexion with UE hold 90 of hip flexion (no UE assistance) bilateral LE movement exercises for trunk extensors/multifidu s starting quadruped than progressing to prone. Quadruped progression: flex one UE extend one LE by sliding along table Extend one LE and lift off table flex one UE and extend contralateral LE. Prone progression: extend one LE extend both LE lift head, arms and LE off table Advanced functional training: curl-ups on unstable surface, trunk flexion sitting or standing on stable/unstable surface w/ added UE loading in PNF patterns, trunk extension sitting or standing on stable/unstable surface w/ added UE loading in PNF
57 patterns, quadratus lumborum side plank progression Cardiopulmonary Endurance Aerobic training Only if tolerated with maximum protection in position of comfort. Select type of aerobic training appropriate for the patient Low to moderate intensity with moderate to minimal protection. Select type of aerobic training appropriate for the patient Use activities that emphasize spinal bias High-intensity (target heart rate), multiple times per week. Select type of aerobic training appropriate for the patient Functional Activities Body mechanics Skill in home, community, work, recreation, sport activities Safe postures for recumbent, sitting and standing Stable-spine techniques while rolling over, moving supine to sit, sit to stand Preparation for functional activities while maintaining stable spine: basic exercise techniques (modified bridging exercises, push-ups with trunk stabilization, wall slides, partial lunges, partial squats and steps, walking against resistance, quadruped forward/backward shifting, squatting and reaching, shifting weight and turning) Patient education on body mechanics and environmental adaptations, load position, ergonomic changes to work and home Intermediate to advanced exercise techniques for functional training while maintaining stable spine (repetitive lifting, repetitive reaching, repetitive pushing and pulling, rotation or turning, transitional movements, transfer of training Endurance and strengthening activities that replicate return to desired activities of patient Patient education and practice for prevention (avoid postures that brings on pain, taking breaks from prolonged postures, avoid spinal postures at end
58 range positions such as hyper extension, use common sense and follow good safety habits, review the HEP)


59


60

61
62

63

64

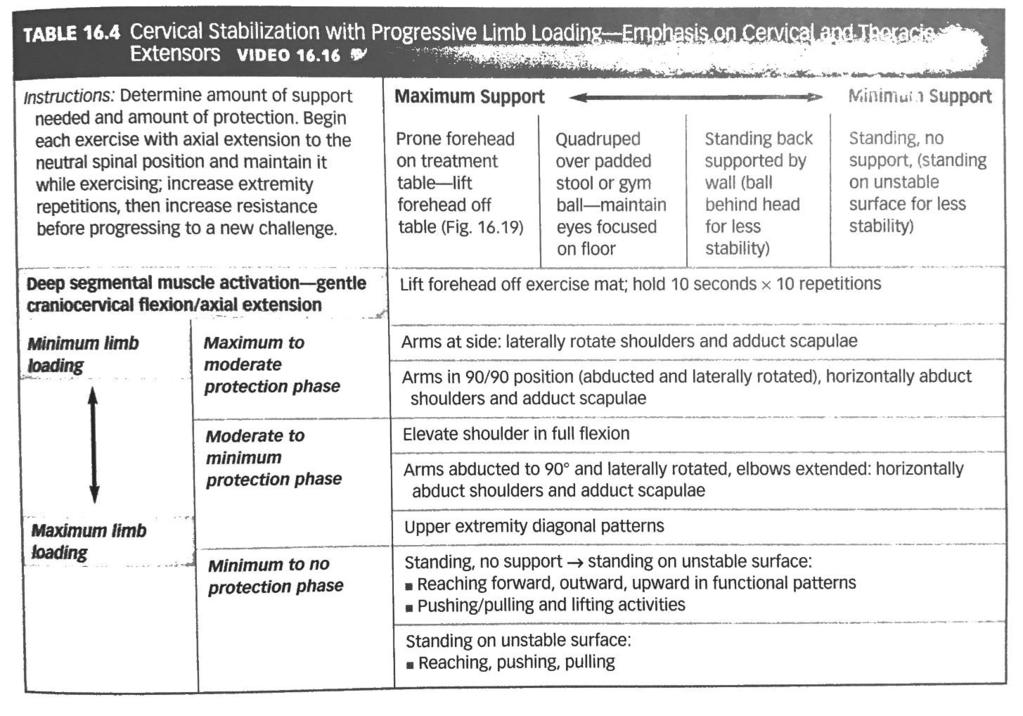
65
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Snow Angels on Foam Roll
 Thoracic Mobilization on Foam Roll Lie on your back with a foam roller positioned horizontally across your mid back, and arms crossed in front of your body. Bend your knees so your feet are resting flat
Thoracic Mobilization on Foam Roll Lie on your back with a foam roller positioned horizontally across your mid back, and arms crossed in front of your body. Bend your knees so your feet are resting flat
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Labral Repair with a Microfracture
 Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Deep Inferior Epigastric Perforator Breast Flap Reconstruction Protocol:
 Deep Inferior Epigastric Perforator Breast Flap Reconstruction Protocol: DAY 5-WEEK 2: Continue home exercise program per written patient handout. Continue appropriate incision care management per MD Maintain
Deep Inferior Epigastric Perforator Breast Flap Reconstruction Protocol: DAY 5-WEEK 2: Continue home exercise program per written patient handout. Continue appropriate incision care management per MD Maintain
Hip Arthroscopy. Labral Repair/Debridement with Femoroplasty
 Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
GENERAL EXERCISES MID-BACK BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES MID-BACK BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to
GENERAL EXERCISES MID-BACK BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to
Lumbar Stenosis Rehabilitation Using the Resistance Chair
 PRODUCTS HELPING PEOPLE HELP THEMSELVES! Lumbar Stenosis Rehabilitation Using the Resistance Chair a. Description Lumbar spinal stenosis is a term used to describe a narrowing of the spinal canal. The
PRODUCTS HELPING PEOPLE HELP THEMSELVES! Lumbar Stenosis Rehabilitation Using the Resistance Chair a. Description Lumbar spinal stenosis is a term used to describe a narrowing of the spinal canal. The
Rotator Cuff Repair Therapy Protocol
 Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Bart Eastwood D.O. 825 Davis st Blacksburg, VA 24060 540-951-6000 All information contained in this protocol is to be used as general guidelines only. Specific variations may be appropriate for each patient
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Internal Rotation (turning toes/knee toward other leg) 30 degree limit. limit
 30 degree limit. limit") Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals Precautions:
: Goals Precautions:") Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK
 ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
Do the same as above, but turn your head TOWARDS the side that you re holding on to the chair.
 Stretch 4-6 times per day and hold each stretch for a minimum of 30 seconds. Perform the stretch gently without bouncing. Discuss any problems with your Chiropractor. Sit upright with your head and shoulder
Stretch 4-6 times per day and hold each stretch for a minimum of 30 seconds. Perform the stretch gently without bouncing. Discuss any problems with your Chiropractor. Sit upright with your head and shoulder
Initial Exercises (Weeks 1-3)
") Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Somatic Adaptation in Cerebral Palsy LINKING ASSESSMENT WITH TREATMENT: AN NDT PERSPECTIVE. By W. Michael Magrun, M.S., OTR/L
 Somatic Adaptation in Cerebral Palsy LINKING ASSESSMENT WITH TREATMENT: AN NDT PERSPECTIVE By W. Michael Magrun, M.S., OTR/L INTRODUCTION Somatic adaptation is one of the primary functions of the central
Somatic Adaptation in Cerebral Palsy LINKING ASSESSMENT WITH TREATMENT: AN NDT PERSPECTIVE By W. Michael Magrun, M.S., OTR/L INTRODUCTION Somatic adaptation is one of the primary functions of the central
CERVICAL CENTRALIZATION
 CERVICAL CENTRALIZATION Flex with Rotation Sit up straight. Drop the chin down towards the chest. Glide the neck back. Rotate the head to the. Perform this exercise as needed to decrease pain. Hold seconds
CERVICAL CENTRALIZATION Flex with Rotation Sit up straight. Drop the chin down towards the chest. Glide the neck back. Rotate the head to the. Perform this exercise as needed to decrease pain. Hold seconds
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Home Exercise Program
 YOUR HOME PROGRAM Home Exercise Program Created by Dr. Furr MD Nov 30th, 1999 Total 21 LOWER TRUNK ROTATIONS - LTR Lying on your back with your knees bent, gently move your knees side-to-side. PRAYER STRETCH
YOUR HOME PROGRAM Home Exercise Program Created by Dr. Furr MD Nov 30th, 1999 Total 21 LOWER TRUNK ROTATIONS - LTR Lying on your back with your knees bent, gently move your knees side-to-side. PRAYER STRETCH
Summary Chart 1 2 months
 NEWBORN Physiological flexion provides stability for posture & random movements Neck righting Labyrinthine righting beginning in prone & supine Primary standing reaction Movements limited by available
NEWBORN Physiological flexion provides stability for posture & random movements Neck righting Labyrinthine righting beginning in prone & supine Primary standing reaction Movements limited by available
Microfracture. This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient.
 This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for two months (8-9 weeks). Allow to place
This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for two months (8-9 weeks). Allow to place
copyrighted material by PRO-ED, Inc.
 Contents Preparation for Functional Sitting Partial Pull to Sit.......................................................... 2 Pull to Sit................................................................ 3
Contents Preparation for Functional Sitting Partial Pull to Sit.......................................................... 2 Pull to Sit................................................................ 3
Shoulder Impingement Rehabilitation Recommendations
 Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Shoulder Impingement Rehabilitation Recommendations The following protocol can be utilized for conservative care of shoulder impingement as well as post- operative subacromial decompression (SAD) surgery.
Overhead Athlete Rehabilitation Guidelines
 Overhead Athlete Rehabilitation Guidelines This document is designed to be used as a guideline in the rehabilitation of the athlete playing overhead sports, mainly baseball and softball, but also including
Overhead Athlete Rehabilitation Guidelines This document is designed to be used as a guideline in the rehabilitation of the athlete playing overhead sports, mainly baseball and softball, but also including
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection
 The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
The SUPPORT Trial: SUbacromial impingement syndrome and Pain: a randomised controlled trial Of exercise and injection SUPPORT Physiotherapy Intervention Training Manual Authors: Sue Jackson (SJ) Julie
FIT IN LINE EXAMPLE REPORT (15/03/11) THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT
 THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT") THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT FIT IN LINE EXAMPLE REPORT (15/03/11) A 12 part assessment tool to screen your athletic performance in 4 key components: Flexibility, Balance, Strength & Core
THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT FIT IN LINE EXAMPLE REPORT (15/03/11) A 12 part assessment tool to screen your athletic performance in 4 key components: Flexibility, Balance, Strength & Core
Total Shoulder Rehab Protocol Dr. Payne
 Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Total Shoulder Rehab Protocol Dr. Payne Phase I Immediate Post Surgical Phase (0-4 weeks): Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase passive range of motion (PROM)
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS
 Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
Ms. Ruth A. Delaney, MB BCh BAO, MMedSc, MRCS Consultant Orthopaedic Surgeon, Shoulder Specialist. +353 1 5262335 ruthdelaney@sportssurgeryclinic.com Modified from the protocol developed at Boston Shoulder
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
Anterior Stabilization of the Shoulder: Latarjet Protocol
 Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Robert K. Fullick, MD 6400 Fannin Street, Suite 1700 Houston, Texas 77030 Ph.: 713-486-7543 / Fx.: 713-486-5549 Anterior Stabilization of the Shoulder: Latarjet Protocol The intent of this protocol is
Balance BALANCE BEAM - TANDEM WALK WOBBLE BOARD. Place a half foam roll on the ground in a forward-back direction with the rounded side up.
 The following is a list of the most common exercises in our clinic to be used as a reference for our patients. If one of your prescribed exercises is not listed, please inform us if you have any questions.
The following is a list of the most common exercises in our clinic to be used as a reference for our patients. If one of your prescribed exercises is not listed, please inform us if you have any questions.
2017 COS ANNUAL MEETING AND EXHIBITION HOME EXERCISES
 UPPER BODY Push Up From a push up position. Lower whole body down to floor. Press up to return to start position. Maintain abdominal hollow and neutral spinal alignment throughout movement. Note: Perform
UPPER BODY Push Up From a push up position. Lower whole body down to floor. Press up to return to start position. Maintain abdominal hollow and neutral spinal alignment throughout movement. Note: Perform
GENERAL EXERCISES KNEE BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES KNEE BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to be
GENERAL EXERCISES KNEE BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only are not to be
Bradley C. Carofino, M.D. Shoulder Specialist 230 Clearfield Avenue, Suite 124 Virginia Beach, Virginia Phone
 Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Subpectoral Bicep Tenodesis Protocol (Spreadsheet) Weeks 1-2 Modalities Treatment Restrictions Goals No active elbow flexion (6weeks) Full PROM shoulder and elbow PROM: Shoulder, elbow, forearm No active
Home Exercise Program Progression and Components of the LTP Intervention. HEP Activities at Every Session Vital signs monitoring
 Home Exercise Program Progression and Components of the LTP Intervention HEP Activities at Every Session Vital signs monitoring Blood pressure, heart rate, Borg Rate of Perceived Exertion (RPE) and oxygen
Home Exercise Program Progression and Components of the LTP Intervention HEP Activities at Every Session Vital signs monitoring Blood pressure, heart rate, Borg Rate of Perceived Exertion (RPE) and oxygen
Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme
 Chapter FOUR Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme Chris Higgs Cathy Chapple Daniel Pinto J. Haxby Abbott 99 n n 100 General Guidelines Knee Exercise
Chapter FOUR Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme Chris Higgs Cathy Chapple Daniel Pinto J. Haxby Abbott 99 n n 100 General Guidelines Knee Exercise
BACK SPASM. Explanation. Causes. Symptoms
 BACK SPASM Explanation A back spasm occurs when the muscles of the back involuntarily contract due to injury in the musculature of the back or inflammation in the structural spine region within the discs
BACK SPASM Explanation A back spasm occurs when the muscles of the back involuntarily contract due to injury in the musculature of the back or inflammation in the structural spine region within the discs
Dynamic slings and optimal 3D function
 Dynamic slings and optimal 3D function Abstract Trish Wisbey-Roth Olympic/Specialist Sports Physiotherapist (FACP), Masters of Sport Physiotherapy (AIS/UC) Active Rehabilitation Consultant Layered over
Dynamic slings and optimal 3D function Abstract Trish Wisbey-Roth Olympic/Specialist Sports Physiotherapist (FACP), Masters of Sport Physiotherapy (AIS/UC) Active Rehabilitation Consultant Layered over
GOLFERS TEN PROGRAM 1. SELF STRETCHING OF THE SHOULDER CAPSULE
 GOLFERS TEN PROGRAM 1. SELF STRETCHING OF THE SHOULDER CAPSULE POSTERIOR CAPSULAR STRETCH Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your elbow.
GOLFERS TEN PROGRAM 1. SELF STRETCHING OF THE SHOULDER CAPSULE POSTERIOR CAPSULAR STRETCH Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your elbow.
Presented by Maureen Hagan BScPT (Physiotherapist), BA PE ACE, Can-Fit-Pro Certified 2006 IDEA Fitness Instructor & 1998 Program Director of the Year
, BA PE ACE, Can-Fit-Pro Certified 2006 IDEA Fitness Instructor & 1998 Program Director of the Year") Presented by Maureen Hagan BScPT (Physiotherapist), BA PE ACE, Can-Fit-Pro Certified 2006 IDEA Fitness Instructor & 1998 Program Director of the Year 1. Overview the most common age-related risk factors
Presented by Maureen Hagan BScPT (Physiotherapist), BA PE ACE, Can-Fit-Pro Certified 2006 IDEA Fitness Instructor & 1998 Program Director of the Year 1. Overview the most common age-related risk factors
IFAST Assessment. Name: Date: Sport: Review Health Risk Assessment on initial consult form. List Client Goals (what brings you here?
 IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
The Golfers Ten Program. 1. Self Stretching of the Shoulder Capsule
 The Golfers Ten Program 1. Self Stretching of the Shoulder Capsule A. Posterior capsular stretch Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your
The Golfers Ten Program 1. Self Stretching of the Shoulder Capsule A. Posterior capsular stretch Bring your arm across your chest toward the opposite shoulder. With the opposite arm grasp your arm at your
Lab Workbook. ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone
 ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
ANATOMY Manual Muscle Testing Lower Trapezius Patient: prone Lab Workbook Fixation: place on hand below the scapula on the opposite side Test: adduction and depression of the scapula with lateral rotation
Lumbar/Core Strength and Stability Exercises
 Athletic Medicine Lumbar/Core Strength and Stability Exercises Introduction Low back pain can be the result of many different things. Pain can be triggered by some combination of overuse, muscle strain,
Athletic Medicine Lumbar/Core Strength and Stability Exercises Introduction Low back pain can be the result of many different things. Pain can be triggered by some combination of overuse, muscle strain,
Flexibility. STRETCH: Kneeling gastrocnemius. STRETCH: Standing gastrocnemius. STRETCH: Standing soleus. Adopt a press up position
 STRETCH: Kneeling gastrocnemius Adopt a press up position Rest one knee on mat with the opposite leg straight Maintain a neutral spine position Push through arms to lever ankle into increased dorsiflexion
STRETCH: Kneeling gastrocnemius Adopt a press up position Rest one knee on mat with the opposite leg straight Maintain a neutral spine position Push through arms to lever ankle into increased dorsiflexion
Pilates for Chronic Low Back Pain
 Pilates for Chronic Low Back Pain Julianne Bettencourt March 23, 2015 Course Year: 2014 Integrated Fitness, Visalia, CA Abstract Low back pain is an injury that affects thousands of people every day and
Pilates for Chronic Low Back Pain Julianne Bettencourt March 23, 2015 Course Year: 2014 Integrated Fitness, Visalia, CA Abstract Low back pain is an injury that affects thousands of people every day and
PART ONE. Belly Dance Fitness Technique
 PART ONE Belly Dance Fitness Technique OVERVIEW Understanding belly dance movement The gentle, symmetrical, rhythmic undulations that we practice in Belly dance can help to revitalize almost every part
PART ONE Belly Dance Fitness Technique OVERVIEW Understanding belly dance movement The gentle, symmetrical, rhythmic undulations that we practice in Belly dance can help to revitalize almost every part
Evaluating the Athlete Questionnaire
 Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
UPPER BACK PAIN. Contents What causes Upper Back Pain?... 3
 Contents What causes Upper Back Pain?............. 3 What treatment can I receive?.............. 5 YOUR GUIDE TO UPPER BACK PAIN An IPRS Guide to provide you with exercises and advice to ease your condition
Contents What causes Upper Back Pain?............. 3 What treatment can I receive?.............. 5 YOUR GUIDE TO UPPER BACK PAIN An IPRS Guide to provide you with exercises and advice to ease your condition
Knee Conditioning Program
 Knee Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Knee Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
BeBalanced! total body training
 BeBalanced! von Manuela Böhme made in switzerland 1 sponsored by As a therapy and training device, the AIREX Balance-pad Elite covers a large spectrum of possible applications. Thanks to its destabilising
BeBalanced! von Manuela Böhme made in switzerland 1 sponsored by As a therapy and training device, the AIREX Balance-pad Elite covers a large spectrum of possible applications. Thanks to its destabilising
The theory and practice of getting fitter and stronger
 The theory and practice of getting fitter and stronger David Docherty, PhD, Professor Emeritus School of Exercise Science, Physical and Health Education University of Victoria All the presentations are
The theory and practice of getting fitter and stronger David Docherty, PhD, Professor Emeritus School of Exercise Science, Physical and Health Education University of Victoria All the presentations are
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR
 REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR ANTERIOR SHOULDER RECONSTRUCTION WITH BANKART REPAIR The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Biceps Tenotomy Protocol
 Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Biceps Tenotomy Protocol A biceps tenotomy procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum. A biceps tenotomy is typically done when there is
Abductor Repair (Gluteus Medius/Minimus Repair)
") (Gluteus Medius/Minimus Repair) This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for 8
(Gluteus Medius/Minimus Repair) This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for 8
Theodore B. Shybut, M.D.
 Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Theodore B. Shybut, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Non-operative Shoulder Rehabilitation Protocol Basic shoulder program for: o Scapular Dyskinesis (proximally
Biceps Tenodesis Protocol
 Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
Biceps Tenodesis Protocol A biceps tenodesis procedure involves cutting of the long head of the biceps just prior to its insertion on the superior labrum and then anchoring the tendon along its anatomical
SPINE CARE. A helpful guide with exercises and expert tips
 SPINE CARE A helpful guide with exercises and expert tips Summit Orthopedics provides comprehensive bone, joint, and muscle care to the Twin Cities and Greater Minnesota. SPINE ANATOMY The vertebrae of
SPINE CARE A helpful guide with exercises and expert tips Summit Orthopedics provides comprehensive bone, joint, and muscle care to the Twin Cities and Greater Minnesota. SPINE ANATOMY The vertebrae of
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)
 Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)") Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
ATHLETIC CONDITIONING ON THE ARC BARREL
 ATHLETIC CONDITIONING ON THE ARC BARREL page 1 INTRODUCTION The STOTT PILATES Athletic Conditioning stream serves as a bridge between STOTT PILATES standard repertoire and the CORE Athletic Conditioning
ATHLETIC CONDITIONING ON THE ARC BARREL page 1 INTRODUCTION The STOTT PILATES Athletic Conditioning stream serves as a bridge between STOTT PILATES standard repertoire and the CORE Athletic Conditioning
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ACUTE PROXIMAL HAMSTRING TENDON REPAIR BENJAMIN J. DAVIS, MD
 Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Warm-Up and Stretching Exercises
 Warm-Up and Stretching Exercises Most athletes (swimmers included) use a combination of controlled movement exercises and specific joint/muscle stretching to improve performance potential. The proposed
Warm-Up and Stretching Exercises Most athletes (swimmers included) use a combination of controlled movement exercises and specific joint/muscle stretching to improve performance potential. The proposed
Sciatica. 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) Website: philip-bayliss.com
 Website: philip-bayliss.com") 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Sciatica Nagging, burning pain radiating down the back of the leg, or dull throbbing pain in the buttocks
43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Sciatica Nagging, burning pain radiating down the back of the leg, or dull throbbing pain in the buttocks
Thoracic Home Exercise Program
 Home Exercise Program 1. Bridging Laying on your back, knees bent with feet flat on the floor, arms along side resting on the floor, tighten your abdominals to stabilize your low back. Raise your buttocks
Home Exercise Program 1. Bridging Laying on your back, knees bent with feet flat on the floor, arms along side resting on the floor, tighten your abdominals to stabilize your low back. Raise your buttocks
Physical Sense Activation Programme
 Flexion extension exercises for neck and upper back Sitting on stool Arms hanging by side Bend neck and upper back Breathe out Extend your neck and upper back Lift chest to ceiling Squeeze shoulder blades
Flexion extension exercises for neck and upper back Sitting on stool Arms hanging by side Bend neck and upper back Breathe out Extend your neck and upper back Lift chest to ceiling Squeeze shoulder blades
VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL
 VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL Lumbar and Thoracic Spine Lumbar AROM Assessment -Patient Positioning: Standing, appropriately undressed so that the lumbar and thoracic
VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL Lumbar and Thoracic Spine Lumbar AROM Assessment -Patient Positioning: Standing, appropriately undressed so that the lumbar and thoracic
Neck Rehabilitation programme for Rugby players.
 Neck Rehabilitation programme for Rugby players. The programme consists of two parts, first the Therapeutic Exercise Programme to improve biomechanical function and secondly the Rehabilitation programme
Neck Rehabilitation programme for Rugby players. The programme consists of two parts, first the Therapeutic Exercise Programme to improve biomechanical function and secondly the Rehabilitation programme
REMEMBER GOOD POSTURE DURING ALL YOUR EXERCISES, AVOID SLOUCHING AS YOUR CURRENT PROGRAM BECOMES EASY SLOWLY INCREASE:
 REMEMBER GOOD POSTURE DURING ALL YOUR EXERCISES, AVOID SLOUCHING Apr 06, 2017 AS YOUR CURRENT PROGRAM BECOMES EASY SLOWLY INCREASE: # OF LAPS YOU ARE WALKING # OF REPITITIONS # OF SECONDS YOU HOLD A STRETCH
REMEMBER GOOD POSTURE DURING ALL YOUR EXERCISES, AVOID SLOUCHING Apr 06, 2017 AS YOUR CURRENT PROGRAM BECOMES EASY SLOWLY INCREASE: # OF LAPS YOU ARE WALKING # OF REPITITIONS # OF SECONDS YOU HOLD A STRETCH
Evaluating Movement Posture Disorganization
 Evaluating Movement Posture Disorganization A Criteria-Based Reference Format for Observing & Analyzing Motor Behavior in Children with Learning Disabilities By W. Michael Magrun, MS, OTR 3 R D E D I T
Evaluating Movement Posture Disorganization A Criteria-Based Reference Format for Observing & Analyzing Motor Behavior in Children with Learning Disabilities By W. Michael Magrun, MS, OTR 3 R D E D I T
Prater Chiropractic Wellness Center 903 W. South St. Kalamazoo, MI PH: (269)
") Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning
Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following a well-structured conditioning
Low Back Pain Home Exercises
 Low Back Pain Home Exercises General Instructions The low back exercise program is a series of stretching exercises and strengthening exercises prescribed by your physician for your medical condition.
Low Back Pain Home Exercises General Instructions The low back exercise program is a series of stretching exercises and strengthening exercises prescribed by your physician for your medical condition.
This Manual is copyright under the Berne Convention. In terms of the Copyright Act 98 of 1978 no part of this leaflet may be reproduced or
 Basic Ball Exercise Manual Train your Core This Manual is copyright under the Berne Convention. In terms of the Copyright Act 98 of 1978 no part of this leaflet may be reproduced or transmitted in any
Basic Ball Exercise Manual Train your Core This Manual is copyright under the Berne Convention. In terms of the Copyright Act 98 of 1978 no part of this leaflet may be reproduced or transmitted in any
Exercises to restore range of movement: Rotation
 Exercises to restore range of movement: Rotation Start position: Sitting upright with your back supported in a chair. Position your head so it is evenly balanced, looking forward. Avoid allowing your head
Exercises to restore range of movement: Rotation Start position: Sitting upright with your back supported in a chair. Position your head so it is evenly balanced, looking forward. Avoid allowing your head
Rehabilitation, Core Stability & Personal Training using the Swiss Ball
 s EDUCATION WORKSHOPS Rehabilitation, Core Stability & Personal Training using the Swiss Ball with B.App.Sc (Physio), Dip.Ed (P.E.) CONTENTS Topic Page 1. Introduction 2. Core Stability Basics 3 3. Core
s EDUCATION WORKSHOPS Rehabilitation, Core Stability & Personal Training using the Swiss Ball with B.App.Sc (Physio), Dip.Ed (P.E.) CONTENTS Topic Page 1. Introduction 2. Core Stability Basics 3 3. Core
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT
 REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
REHABILITATION GUIDELINES FOR ARTHROSCOPIC CAPSULAR SHIFT The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference to the average, but individual
Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate
 Bicep Tenodesis D. WATTS, M.D. Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate PHASE I PASSIVE RANG OF MOTION PHASE (STARTS APPROXIMATELY POST OP WEEKS 1-2) Minimize
Bicep Tenodesis D. WATTS, M.D. Progression to the next phase based on Clinic Criteria and or Time Frames as Appropriate PHASE I PASSIVE RANG OF MOTION PHASE (STARTS APPROXIMATELY POST OP WEEKS 1-2) Minimize
JOHN M. REDMOND, M.D.
 Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
PHASE I (Begin PT 3-5 days post-op) DOS:
 DOS:") REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
REHABILITATION GUIDELINES FOR POSTERIOR SHOULDER RECONSTRUCTION +/- LABRAL REPAIRS The rehabilitation guidelines are presented in a criterion based progression. General time frames are given for reference
Exercise for Reducing Neck Pain and Enhancing Dynamic Stability.
 Exercise for Reducing Neck Pain and Enhancing Dynamic Stability www.fisiokinesiterapia.biz Presentation Outline Compare/Contrast Lumbar Exercise Literature to Cervical Spine Discuss Neck Musculature and
Exercise for Reducing Neck Pain and Enhancing Dynamic Stability www.fisiokinesiterapia.biz Presentation Outline Compare/Contrast Lumbar Exercise Literature to Cervical Spine Discuss Neck Musculature and
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) Acetabuloplasty
 Fax: (860) Acetabuloplasty") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com This protocol
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com This protocol
Postural Correction for Neck and Back
 Dr. Bradley Gueldner Dr. Dana Gueldner Dr. Morgan Gueldner 101-32630 George Ferguson Way. Abbotsford, British Columbia. V2T 4V6. Tel: 604.852.1820 Purpose of Program: Postural Correction for Neck and Back
Dr. Bradley Gueldner Dr. Dana Gueldner Dr. Morgan Gueldner 101-32630 George Ferguson Way. Abbotsford, British Columbia. V2T 4V6. Tel: 604.852.1820 Purpose of Program: Postural Correction for Neck and Back
General Back Exercises
 Touch of Life Chiropractic 130-F Montauk Hwy., East Moriches, NY 11940 631-874-2797 General Back Exercises Muscular stretching can be a very important part of the healing process for tightened muscles
Touch of Life Chiropractic 130-F Montauk Hwy., East Moriches, NY 11940 631-874-2797 General Back Exercises Muscular stretching can be a very important part of the healing process for tightened muscles
LOW BACK. Performance Physical Therapy & Fitness
 LOW BACK On back, feet resting on ball, pull knees to chest until stretch is felt in low back. Pause, then return to start position. Repeat 15-20 times LOWER TRUNK ROTATION On back, feet resting on ball,
LOW BACK On back, feet resting on ball, pull knees to chest until stretch is felt in low back. Pause, then return to start position. Repeat 15-20 times LOWER TRUNK ROTATION On back, feet resting on ball,
Back Health and Safety
 Back Health and Safety Your back is at work every minute of every day, whether you are awake or asleep, active or quiet. Over time the effects of poor posture, bad body mechanics, physical deconditioning
Back Health and Safety Your back is at work every minute of every day, whether you are awake or asleep, active or quiet. Over time the effects of poor posture, bad body mechanics, physical deconditioning
Foundation Mobility (50 min)
") Foundation Mobility (50 min) Protection (10 min) Exercise Reps Duration (s) Wrist Abduction 12 ea 60 Wrist Adduction 12 ea 60 Wrist Pronation and Supination 10 ea 60 Wrist Pronation and Supination (Reverse
Foundation Mobility (50 min) Protection (10 min) Exercise Reps Duration (s) Wrist Abduction 12 ea 60 Wrist Adduction 12 ea 60 Wrist Pronation and Supination 10 ea 60 Wrist Pronation and Supination (Reverse
Standing Shoulder Internal Rotation with Anchored Resistance. Shoulder External Rotation Reactive Isometrics
 Standing Shoulder Row with Anchored Resistance Begin standing upright, holding both ends of a resistance band that is anchored in front of you at chest height, with your palms facing inward. Pull your
Standing Shoulder Row with Anchored Resistance Begin standing upright, holding both ends of a resistance band that is anchored in front of you at chest height, with your palms facing inward. Pull your
Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A Case Report.
 Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A. Kara Delie, SPT Kristine Erickson, PT, MS, NCS 1 Abstract: Title: Dynamic Neural Mobilization as an
Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A. Kara Delie, SPT Kristine Erickson, PT, MS, NCS 1 Abstract: Title: Dynamic Neural Mobilization as an
REPETITIVE STRESS SYNDROME AND ITS EFFECTS ON THE LOWER PELVIS
 REPETITIVE STRESS SYNDROME AND ITS EFFECTS ON THE LOWER PELVIS Kim Turney Body Arts and Science International Comprehensive Global Feb 2018 London, UK ABSTRACT In many lines of work people are subjected
REPETITIVE STRESS SYNDROME AND ITS EFFECTS ON THE LOWER PELVIS Kim Turney Body Arts and Science International Comprehensive Global Feb 2018 London, UK ABSTRACT In many lines of work people are subjected
Knee Conditioning Program
 Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
10 Minutes per Day Low Back Pain Prevention Guide
 10 Minutes per Day Low Back Pain Prevention Guide Did you know that an estimated $50 billion dollars is spent annually on back pain related issues? Low back pain (LBP) is one of the most prevalent medical
10 Minutes per Day Low Back Pain Prevention Guide Did you know that an estimated $50 billion dollars is spent annually on back pain related issues? Low back pain (LBP) is one of the most prevalent medical
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
BENJAMIN G. DOMB, MD
 Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Exercises to Correct Muscular Imbalances. presented by: Darrell Barnes, LAT, ATC, CSCS
 Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries)
") Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Limited Goals Program (Examples Include: Cuff Tear Arthropathy, Massive Irrepairable Rotator Cuff Tear, Selected Revision Surgeries) All information contained in this protocol is to be used as general
Movement System Diagnoses. Movement System Impairment Syndromes of the Lumbar Spine. MSI Syndrome - Assumptions. Return From Forward Bending
 Movement System Diagnoses Kinesiopathologic Pathokinesiologic Movement System Impairment Syndromes of the Lumbar Spine Shirley Sahrmann, PT, PhD, FAPTA Washington University St. Louis School of Medicine
Movement System Diagnoses Kinesiopathologic Pathokinesiologic Movement System Impairment Syndromes of the Lumbar Spine Shirley Sahrmann, PT, PhD, FAPTA Washington University St. Louis School of Medicine
Mobility sequencing!
 Mobility sequencing When practicing joint mobility drills we have the opportunity to improve our movement. The muscles associated with the joint being mobilised as well as the joint itself will improve
Mobility sequencing When practicing joint mobility drills we have the opportunity to improve our movement. The muscles associated with the joint being mobilised as well as the joint itself will improve
Presentation Overview 8/8/12. Muscle Imbalances Revealed Assessment & Exercise for Personal Training
 Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
AQUATIC ARSENAL. Shoulders & More By Melanie Sparks
 AQUATIC ARSENAL Shoulders & More By Melanie Sparks According to Livestron.com website, The shoulder is the most mobile and flexible joint in the human body. The truth is, we all use our shoulders a lot
AQUATIC ARSENAL Shoulders & More By Melanie Sparks According to Livestron.com website, The shoulder is the most mobile and flexible joint in the human body. The truth is, we all use our shoulders a lot