The Schiowitz Approach
|
|
|
- Moses McKenzie
- 5 years ago
- Views:
Transcription
1 The Schiowitz Approach American Academy of Osteopathy Annual Convocation March 23 rd, :00-3:30 PM & 4:00 5:30 PM Dennis J. Dowling, D.O., M.A., F.A.A.O.

2
3
4 F.P.R. Developed by Stanley Schiowitz, D.O., F.A.A.O. NYCOM

5
6 Stanley Schiowitz, D.O., F.A.A.O. Graduated from high school at age 15 St. John s University started PCOM at age 18 Graduated at age 22 in 1944 Internship/Apprenticeship with his mentor, M.W. Levy, D.O Private Practice in Brooklyn DME Interboro Hospital Chair of NYCOM OPP Department Director of Medical Education Director of Family Practice Associate Dean for Clinical Rotations Dean NYCOM Dean Emeritus

7

8 Someday, someone will explain to me what the hell I am doing.

9 I.O. INSTANT OSTEOPATHY How Long? A few seconds
10 Basic Rules of F.P.R. Diagnose Put region/joint into Neutral (flatten curves) places joint into idling position Monitor continuously Add facilitating force (usually compression or torsion) reduces proprioceptive noise Add freedoms in all three planes (Flexion/Extension, Sidebending, rotation) reduces muscle spindle activity allows reduction of gamma gain If compression doesn t work, try traction. If it doesn t work going to the right, go to the left. Simple philosophy.
11 Basic Rules of F.P.R. Hold position for five seconds Determine alteration of tissue tension Return to Neutral Reassess Barriers can then be challenged ( wiggle jiggle ) Reassess Any mechanical dysfunction in the body can affect any other part of the body and therefore can affect any system of the body (and vice versa). When treating a patient, never treat them for a diagnosed medical condition. Treat the musculoskeletal change, and if the patient feels better then you are both lucky. Maybe it will help, maybe it won t.

12 Basic Rules of F.P.R. Hold position for five seconds Determine alteration of tissue tension Return to Neutral Reassess Barriers can then be challenged ( wiggle jiggle ) Reassess But, Stan, you never wrote about challenging the barriers. What gives? PASSIVE INDIRECT & DIRECT
13 Still Technique I don t treat the way I teach, I get down to smaller and smaller motions. Facilitated Positional Release
14 Still Technique TWIN TECHNIQUES with DIFFERENT FATHERS Facilitated Positional Release




15 Did Stan Schiowitz know that his FPR was the third iteration of the Still Technique? No, he didn t He knew that it was the second.

16 F.P.R. J Am Osteopath Assoc Feb;90(2):145-6, Still Technique J Am Osteopath Assoc Oct;96(10):
: 1. Always do a complete H&P 2. Always do a rudimentary structural exam 3.")
17 Contraindications Localized pathological tissue conditions Infection Cellulitis Osteomyelitis Cysts Tumors Fracture Increase or significant alteration of symptoms Inability to tolerate position Learned from Moe Levy, D.O. (his mentor): 1. Always do a complete H&P 2. Always do a rudimentary structural exam 3. Always use OMT whenever you can.
18 A form of Myofascial Release Counterstrain & Functional techniques are positional techniques Facilitated Positional Release and Still technique rely on both the positional component and a facilitating force They both start INDIRECT and then become DIRECT They are both very TIME EFFICIENT It is important to learn efficiency in time and effort.
19 Type of Technique Passive - the patient does nothing Indirect - Treatment is directed primarily away from the barriers (Direct - barriers can be challenged afterwards) (Occasionally we ask the patient to do something [i.e. isometrics])
20 For FPR it is especially useful to use pillows Assists in the curves
21 It is important to learn efficiency in time and effort. Three Ds of Osteopathy Diagnosis Diagnosis Diagnosis When talking about restriction in motion, somatic dysfunction, osteopathic lesion, the great majority of limitation is created in the accessory (slide) motion of an articulation/segment.


22 DIAGNOSIS speedbumps Suspect that there is a Flexion dysfunction when there is a sudden increase (bump) in an anterior posterior curve The simpler you make it, the easier your life will be.
 in an anterior posterior curve. accessory and coupled motion are not the same.")

23 DIAGNOSIS potholes POTHOLES Suspect that there is an Extension dysfunction when there is a sudden decrease (dip) in an anterior posterior curve. accessory and coupled motion are not the same. Don t think of it as I have a flexion lesion, think of it as a translation problem. If you think that way, then you ll know what to do. Go with the flow but remember what your motion is and go with that.

24
25
26 Real segmental motion is very small.
27
28 TEST RELATIVE FLEXION
29 TEST RELATIVE EXTENSION
30 CERVICAL

31 Patient Supine Doctor at the head of the table A Pillow can be used on the doctor s lap
32 CERVICAL MOTION TESTING
33

34 PILLAR

35
36

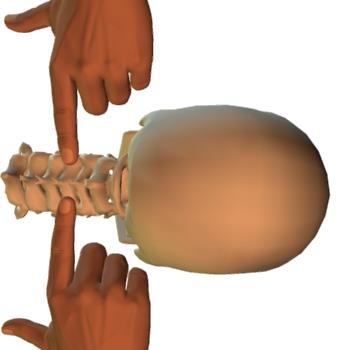
37 SPINOUS PROCESS FACET/PILLAR TRANSVERSE PROCESS
38
39
40
41 EXTENSION
42
43 FLEXION
44
45 Increased resistance: extension = FLEXION dysfunction flexion = EXTENSION dysfunction
46 RIGHT TRANSLATION creates LEFT SIDEBENDING
47 RIGHT SIDEBENDING LEFT TRANSLATION creates
48 Increased resistance in sidebending: left = RIGHT (ease) dysfunction right = LEFT (ease) dysfunction
49 ROTATION
50 Lifting the left side creates RIGHT ROTATION
51 Lifting the left side creates RIGHT ROTATION
52 Lifting the right side creates LEFT ROTATION
53 Lifting the right side LEFT ROTATION creates
54 FPR CERVICAL
55 CERVICAL Soft Tissue Treatment FINDINGS Posterior cervical muscle hypertonicity (soft tissue texture abnormalities). When practicing Osteopathy, you want to treat the hard stuff and the hard stuff doesn t have a name. Just treat what you find.
56 Cervical Segmental Somatic Dysfunction FINDINGS C3 ES L R L and C7 FS L R L PATIENT POSITION Supine, with the patient's head beyond the end of the table, resting on a pillow on the physician's lap.
57 O-A Dysfunction. (Example ESLRR) FINDINGS OA ES L R R PATIENT POSITION Supine, with the patient's head beyond the end of the table, resting on a pillow on the physician's lap Can motion be introduced, that is what is important.
58 THORACIC
59 THORACIC MOTION TESTING
60
61 Real segmental motion is very small.
62
63 TEST RELATIVE FLEXION
64 TEST RELATIVE EXTENSION

65 THORACIC Thoracic Spine, Seated FINDINGS T6 FS L R L. PATIENT POSITION The patient is seated on the end of the table. When you put a spinal segment into neutral it opens the facets and the articulation moves freely.

66 Alternative Thoracic Spine (Extension dysfunctions), Prone FINDINGS T6 ES L R L. PATIENT POSITION Resultant vector When treating the key is the angle of the vector force.

67 Treatment of an S or C shaped scoliosis of the thoracolumbar spine: S or C shaped scoliosis of the thoracolumbar spine FINDINGS T1-9 NS L R R and T10-L5 NS R R L T1-L5 NS L R R.
68 FIRST RIB

69 FIRST RIB FINDINGS First rib elevated on left. PATIENT POSITION The patient is Supine
70 CLAVICLE

71 STERNOCLAVICULAR/ACROMIOCLAVICULAR DYSFUNCTIONS Shoulder restrictions Left anteriorly rotated clavicle with the lateral clavicle anterior and inferior PATIENT POSITION The patient is seated
72 RIBS

73 FPR RIBS - SEATED FINDINGS Soft tissue and/or dysfunctions of the ribs. PATIENT POSITION The patient is seated
74 FPR RIBS & THORACIC - SIDELYING FINDINGS Soft tissue and/or dysfunctions of the thoracic and ribs. PATIENT POSITION The patient is sidelying with the side to be treated up


75 MIDDLE RIBS SERRATUS POSTERIOR RHOMBOIDS PVM
76 LUMBAR

77 FPR LUMBAR- SIDELYING FINDINGS Right Soft tissue and/or dysfunctions of the lumbar. PATIENT POSITION The patient is sidelying with the side to be treated up When treating muscles the muscles will tell you which way to go.

78 QUADRATUS LUMBORUM LATISSIMUS DORSI



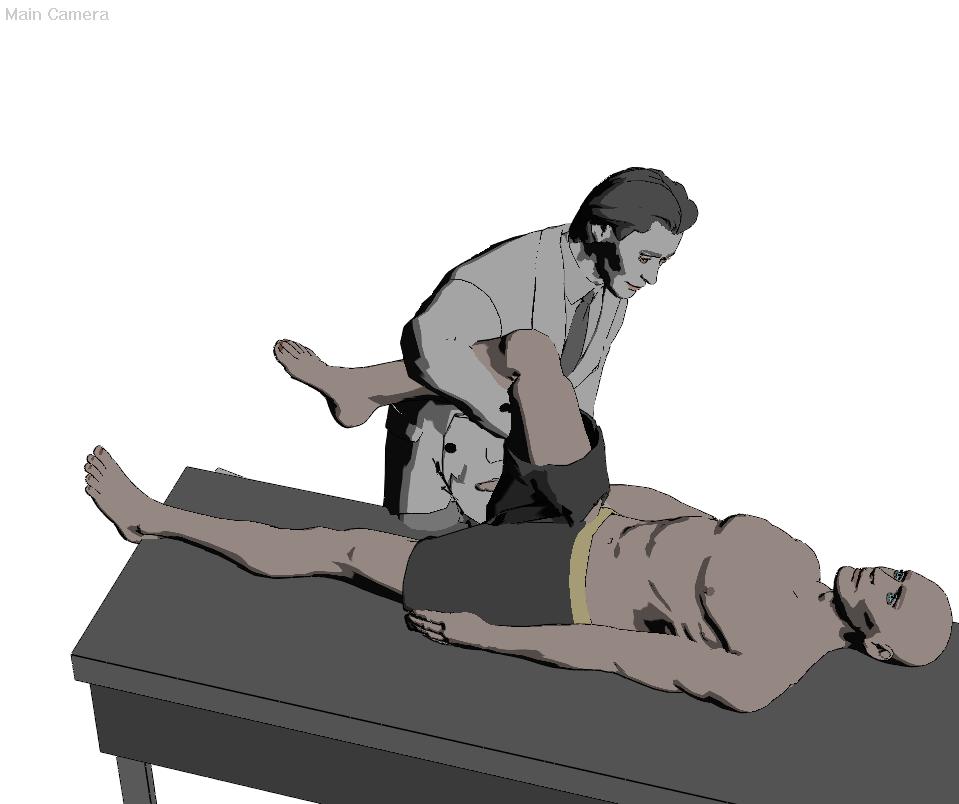
79 LUMBAR Soft Tissue Treatment FINDINGS Hypertonic right paravertebral lumbar muscles. POSITION The patient is prone, close to the right edge of the table, with a sufficient number of pillows beneath the abdomen to cause flattening of the lumbar lordosis 1 Patient prone with pillow beneath abdomen 2 Patient s lower half is sidebent towards the side to be treated 3 The opposite leg is further adducted and crossed at the ankle
80 LUMBAR Extension Somatic Dysfunction FINDINGS L3 ES R R R. POSITION The patient is prone, close to the left edge of the table, with a sufficient number of pillows beneath the abdomen to cause flattening of the lumbar lordosis THE LUMBAR VERTEBRA OF THE SOMATIC DYSFUNCTION RELATIVELY ROTATES TOWARD THE SAME SIDE
81 LUMBAR Flexion Somatic Dysfunction FINDINGS L4 FS R R R. POSITION The patient is prone, close to the left edge of the table, with a sufficient number of pillows beneath the abdomen to cause flattening of the lumbar lordosis. THE ADDUCTION CAUSES INTERNAL ROTATION WHICH LOCKS THE FEMORAL HEAD INTO THE ACETABULUM OF THE PELVIS THE LUMBAR VERTEBRA OF THE SOMATIC DYSFUNCTION RELATIVELY ROTATES TOWARD THE SAME SIDE
82
83 LUMBAR Discogenic Pain Syndrome Treatment FINDINGS Right lumbar disk herniation or bulge with right radiculitis. POSITION The patient is prone, close to the left edge of the table, with a sufficient number of pillows beneath the abdomen to cause flattening of the lumbar lordosis THE PHYSICIAN PUSHES THE PATIENT S FOOT TOWARDS THE FLOOR THE PHYSICIAN RAISES HIS OUTER KNEE AND PUTS LATERAL PRESSUREON THE PATIENT S POSTERIOR KNEE I don t treat herniated discs of the lumbar spine. I do treat (essentially) lateral stenosis. I don t want you to say; oh he taught me to pop a disc back, no I didn t.
84 SACRUM & PELVIS
85

86 SACRUM & PELVIS DIAGNOSIS RIGHT ANTERIOR PELVIC ROTATION FINDINGS RIGHT + STANDING FLEXION TEST RIGHT ASIS LOW RIGHT PSIS HIGH The patient is supine

87 SACRUM & PELVIS DIAGNOSIS RIGHT POSTERIOR PELVIC ROTATION FINDINGS RIGHT + STANDING FLEXION TEST RIGHT ASIS HIGH RIGHT PSIS LOW The patient is supine
88 Treat what you find, try to avoid naming it because the bad ones (somatic dysfunction) have no name.
89 SACRUM DIAGNOSIS LEFT SACRAL RESTRICTION FINDINGS LEFT + SEATED FLEXION TEST LEFT SACRAL RESTRICTION The patient is prone The Physician's cephalad hand thenar and hypothenar region is on the ILA of the sacrum on the same side as the dysfunction. The index &/or the pads of the index and middle fingers are medial to the PSIS on the same side The Physician's other hand grasps the patient s lower leg above the ankle on the same side.
90 SACRUM DIAGNOSIS LEFT SACRAL RESTRICTION FINDINGS LEFT + SEATED FLEXION TEST LEFT SACRAL RESTRICTION The patient is prone The Physician's cephalad hand maintains pressure on the sacrum with a slight anterior and cephalad force. The Physician's hand on the patient s lower leg introduces slight abduction of the hip by deviating the leg laterally and external rotation of the hip until motion is felt by the hand on the sacrum. Slight compression is introduced up to the pelvis and sacrum.
91 FPR SACRUM The Physician's cephalad hand maintains pressure on the sacrum with a slight anterior and cephalad force. The Physician's hand on the patient s lower leg introduces internal rotation of the hip until motion is felt by the hand on the sacrum. Traction is introduced. The Patient is instructed to inhale deeply. The physician increases the cephalad pressure on the ILA and can even introduce a slight cephalad/anterior thrust. The patient exhales and the dysfunction is reassessed

92 ALTERNATIVE PROINE SACRAL TECHNIQUE DIAGNOSIS RIGHT SACRAL RESTRICTION FINDINGS RIGHT + SEATED FLEXION TEST RIGHT SACRAL RESTRICTION The patient is prone

93 You have motion, you re through. The name of the game is motion.

94 FPR SIDELYING SACRUM
95 E/M Office Visit Codes New pt Established pt nurse evaluated/treated without doctor face-to-face involvement nurse evaluation or easy low complexity mod complexity high complexity
96 Modifier 25 The -25 modifier is used when additional E/M services are provided on the same day as a procedure is provided Modifier -25 Significant, separately identifiable E/M Service by the Same Physician on the Same Day of the Procedure or Other Service E/M services required above and beyond the other service provided, or beyond the usual pre- and post-operative care associated with the procedure performed. Different diagnoses are not required.
97 OMT Procedural Codes CPT for OMT Procedure CODES OMT; one to two regions involved OMT; three to four regions involved OMT; five to six regions involved OMT; seven to eight regions involved OMT; nine to ten regions involved They can include any 10 body regions combinations: cranial, cervical, thoracic, lumbar, sacral, innominate, upper extremity, lower extremity, rib cage, visceral
98 Osteopathic Diagnostic Codes Osteopathic ICD-10 Diagnostic Codes (10 Regions) Listed as: Segmental somatic dysfunctions or Non-allopathic dysfunction M99.00 Head region Occipito-cervical region M99.01 Cervical region Cervicothoracic region M99.02 Thoracic region Thoracolumbar region M99.03 Lumbar region Lumbosacral region M99.04 Sacral region Sacrococcygeal and Sacroiliac regions M99.05 Pelvic region Pelvic and Pubic regions M99.06 Lower extremities Hip, Knee, Ankle & Foot M99.07 Upper extremities Shoulder, Elbow, Wrist & Hand M99.08 Rib cage Costovertebral, Costochondral, and Sternochondral regions M99.09 Abdominal & other (Visceral) Abdominal, Pelvic, etc.
DIAGNOSIS ANTERIOR PELVIC ROTATION DIAGNOSIS DIAGNOSIS. Direct techniques to treat sacrum and pelvis somatic dysfunction (HVLA, MET)
") American Academy of Osteopathy Convocation PHYSICIAN STUDENT Thursday, March 18, 2010 Friday, March 19, 2010 2:30 4:00 PM 8:00 9:30 AM 4:30 6:00 PM 10:00 11:30 AM Direct techniques to treat sacrum and
American Academy of Osteopathy Convocation PHYSICIAN STUDENT Thursday, March 18, 2010 Friday, March 19, 2010 2:30 4:00 PM 8:00 9:30 AM 4:30 6:00 PM 10:00 11:30 AM Direct techniques to treat sacrum and
OMT Without An OMT Table. Ann L. Habenicht DO, FAAO, FACOFP, CS AAO Convocation- Student Program March12, 2015
 OMT Without An OMT Table Ann L. Habenicht DO, FAAO, FACOFP, CS AAO Convocation- Student Program March12, 2015 BASIC STUFF WE HAVE TO WADE THROUGH TO MAKE SURE WE RE ALL ON THE SAME PAGE A.T. Still To find
OMT Without An OMT Table Ann L. Habenicht DO, FAAO, FACOFP, CS AAO Convocation- Student Program March12, 2015 BASIC STUFF WE HAVE TO WADE THROUGH TO MAKE SURE WE RE ALL ON THE SAME PAGE A.T. Still To find
OMT Without An OMT Table Workshop. Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP
 OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
Lumbar. Physician. Technique: Continue this. back pain is. bent. under the contralatera. Copyright
 Lumbar myofascial releasee Lumbar spine Brief description: Low back pain is a common problem and lumbar myofascial releasee can be useful as part of a comprehensiv ve treatment of low back pain. By usingg
Lumbar myofascial releasee Lumbar spine Brief description: Low back pain is a common problem and lumbar myofascial releasee can be useful as part of a comprehensiv ve treatment of low back pain. By usingg
Manual Manipulative Medicine: A Structural Examination for Lower Back Pain. Friday, October 2, :30 AM - 12:00 PM W116.
 Manual Manipulative Medicine: A Structural Examination for Lower Back Pain Friday, October 2, 2015 10:30 AM - 12:00 PM W116. Level: Beginner No Financial Disclosures Amir Mahajer, DO Ronald Tolchin, DO
Manual Manipulative Medicine: A Structural Examination for Lower Back Pain Friday, October 2, 2015 10:30 AM - 12:00 PM W116. Level: Beginner No Financial Disclosures Amir Mahajer, DO Ronald Tolchin, DO
OMT for Chronic Low Back Pain: OSTEOPATHIC Trial Protocol. Learning Objectives. Chronic Low Back Pain 8/5/2016
 OMT for Chronic Low Back Pain: OSTEOPATHIC Trial Protocol David C. Mason, DO, MBA, FACOFP Chair Family Medicine and Osteopathic Manipulative Medicine Texas College of Osteopathic Medicine Learning Objectives
OMT for Chronic Low Back Pain: OSTEOPATHIC Trial Protocol David C. Mason, DO, MBA, FACOFP Chair Family Medicine and Osteopathic Manipulative Medicine Texas College of Osteopathic Medicine Learning Objectives
OMT Without The Table Saroj Misra, DO, FACOFP and Marissa Rogers, DO
 OMT Without The Table Saroj Misra, DO, FACOFP and Marissa Rogers, DO Why bother? May not always have the table present Patient may not be able to lay prone or supine Some techniques may be easier to accomplish
OMT Without The Table Saroj Misra, DO, FACOFP and Marissa Rogers, DO Why bother? May not always have the table present Patient may not be able to lay prone or supine Some techniques may be easier to accomplish
Authorized Osteopathic Thesaurus December, 2003 Terms
 s 100-199 USE (s) Elevated Rib Inhalation Rib Dysfunction Item number: 100 Broader (s) Related (s) End Feel Tissue Texture Abnormality Movement Barrier Item number: 101 Perceived quality of motion as an
s 100-199 USE (s) Elevated Rib Inhalation Rib Dysfunction Item number: 100 Broader (s) Related (s) End Feel Tissue Texture Abnormality Movement Barrier Item number: 101 Perceived quality of motion as an
Rotational Forces. : Their impact; our treatments
 Rotational Forces : Their impact; our treatments Lee Stang, LMT, LMBT, BCTMB NCBTMB Provider: 450217-06 bridgestohealthseminars.com bthseminars@gmail.com 860.985.5834 Facebook.com/BridgesToHealthSeminars
Rotational Forces : Their impact; our treatments Lee Stang, LMT, LMBT, BCTMB NCBTMB Provider: 450217-06 bridgestohealthseminars.com bthseminars@gmail.com 860.985.5834 Facebook.com/BridgesToHealthSeminars
OMT for the Pregnant Patient
 OMT for the Pregnant Patient Presented by: Kristie Petree, DO Assistant Professor of Neuromusculoskeletal Medicine and Osteopathic Manipulative Medicine Georgia Campus Philadelphia College of Osteopathic
OMT for the Pregnant Patient Presented by: Kristie Petree, DO Assistant Professor of Neuromusculoskeletal Medicine and Osteopathic Manipulative Medicine Georgia Campus Philadelphia College of Osteopathic
OMT for the child with ENT problems
 SEATED INNOMINATE AND PELVIC BOWL BALANCED LIGAMENTOUS TENSION 1. The physician is seated behind the child with both hands, each contacting an innominate and the sacrum. The fingers contact the ASIS bilaterally
SEATED INNOMINATE AND PELVIC BOWL BALANCED LIGAMENTOUS TENSION 1. The physician is seated behind the child with both hands, each contacting an innominate and the sacrum. The fingers contact the ASIS bilaterally
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
OMT Boot Camp. OMT Applications for Systemic Somatic Dysfunctions of the Spine. Natalie Nevins, DO, MSHPE
 ACOFP 54 th Annual Convention & Scientific Seminars OMT Boot Camp OMT Applications for Systemic Somatic Dysfunctions of the Spine Natalie Nevins, DO, MSHPE Lumbar, Innominate, Sacrum Diagnosis and Treatment
ACOFP 54 th Annual Convention & Scientific Seminars OMT Boot Camp OMT Applications for Systemic Somatic Dysfunctions of the Spine Natalie Nevins, DO, MSHPE Lumbar, Innominate, Sacrum Diagnosis and Treatment
OMT FOR CONCUSSIONS KIMBERLY WOLF, D.O. FEBRUARY 17, 2017
 OMT FOR CONCUSSIONS KIMBERLY WOLF, D.O. FEBRUARY 17, 2017 POTENTIAL SEQUENCE Address lymphatics including all transition zones/diaphragms Address somatic dysfunction in spine Focus on upper cervical spine
OMT FOR CONCUSSIONS KIMBERLY WOLF, D.O. FEBRUARY 17, 2017 POTENTIAL SEQUENCE Address lymphatics including all transition zones/diaphragms Address somatic dysfunction in spine Focus on upper cervical spine
KELLEY JOY, DO CLINICAL ASSOCIATE PROFESSOR OSTEOPATHIC MANIPULATIVE MEDICINE KCU JOPLIN CAMPUS
 STILL TECHNIQUE FOR COMMON COUNTERSTRAIN TENDER POINTS KELLEY JOY, DO CLINICAL ASSOCIATE PROFESSOR OSTEOPATHIC MANIPULATIVE MEDICINE KCU JOPLIN CAMPUS COUNTERSTRAIN HISTORY Lawrence Larry Jones, DO 1955
STILL TECHNIQUE FOR COMMON COUNTERSTRAIN TENDER POINTS KELLEY JOY, DO CLINICAL ASSOCIATE PROFESSOR OSTEOPATHIC MANIPULATIVE MEDICINE KCU JOPLIN CAMPUS COUNTERSTRAIN HISTORY Lawrence Larry Jones, DO 1955
Information within the handout. Brief Introduction Anatomy & Biomechanics Assessment & Diagnosis Treatment through Muscle Energy
 Manual Medicine Diagnosis and Treatment for Somatic Dysfunction of the Pelvis Through Muscle Energy Greenman s Priciples of Manual Medicine (5 th Ed.)- Lisa DeStefano,DO Speaker disclosure I declare I
Manual Medicine Diagnosis and Treatment for Somatic Dysfunction of the Pelvis Through Muscle Energy Greenman s Priciples of Manual Medicine (5 th Ed.)- Lisa DeStefano,DO Speaker disclosure I declare I
What is the most frequently sprained ligament with inversion ankle sprains? 1/30/2014
 What is the most frequently sprained ligament with inversion ankle sprains? A. Anterior Talofibular B. Anterior Tibiofibular C. Calcaniofibular D. Posterior Talofibular E. Deltoid Lateral ligaments of
What is the most frequently sprained ligament with inversion ankle sprains? A. Anterior Talofibular B. Anterior Tibiofibular C. Calcaniofibular D. Posterior Talofibular E. Deltoid Lateral ligaments of
VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL
 VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL Lumbar and Thoracic Spine Lumbar AROM Assessment -Patient Positioning: Standing, appropriately undressed so that the lumbar and thoracic
VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL Lumbar and Thoracic Spine Lumbar AROM Assessment -Patient Positioning: Standing, appropriately undressed so that the lumbar and thoracic
The Use of Seated Facet Release in Children
 The Use of Seated Facet Release in Children Karen M. Steele, DO, FAAO Professor Emerita, West Virginia School of Osteopathic Medicine Former AAO President Outline of lab Pedigree Basic Principles Diagnosis
The Use of Seated Facet Release in Children Karen M. Steele, DO, FAAO Professor Emerita, West Virginia School of Osteopathic Medicine Former AAO President Outline of lab Pedigree Basic Principles Diagnosis
Sacral Dysfunction: Bilateral Flexed Sacrum & Bilateral Extended Sacrum
 Sacral Dysfunction: Bilateral Flexed Sacrum & Bilateral Extended Sacrum Cherise Russo D.O. Northwestern Orthopaedic Institute, LLC Clinical Instructor, Northwestern University School of Medicine April
Sacral Dysfunction: Bilateral Flexed Sacrum & Bilateral Extended Sacrum Cherise Russo D.O. Northwestern Orthopaedic Institute, LLC Clinical Instructor, Northwestern University School of Medicine April
National Boards Part 4 Technique. Exam Format 5 stations (1 doctor and 1 patient). 2 setups per station (5 minutes) cervical
. 2 setups per station (5 minutes) cervical") 1 National Boards Part 4 Technique Exam Format 5 stations (1 doctor and 1 patient). 2 setups per station (5 minutes) cervical thoracic lumbar pelvic extremity Expect examiner interaction Graded on a Scantron
1 National Boards Part 4 Technique Exam Format 5 stations (1 doctor and 1 patient). 2 setups per station (5 minutes) cervical thoracic lumbar pelvic extremity Expect examiner interaction Graded on a Scantron
Possible diagnoses. and extension OA ES L RR. deep. equal. with flexion OA ES R RL. the leftt. equal. deep. equal. equal. for flexion.
 Cervical Diagnosis Occipitoatlantal (OA) joint Possible diagnoses Diagnosis OA FS L RR OA FS R RL OA ES L RR OA ES R RL Sulci findings Left sulcus is shallow and right sulcus is deep Right sulcus is shallow
Cervical Diagnosis Occipitoatlantal (OA) joint Possible diagnoses Diagnosis OA FS L RR OA FS R RL OA ES L RR OA ES R RL Sulci findings Left sulcus is shallow and right sulcus is deep Right sulcus is shallow
Seated & Standing OMT
 Copyright 2018, Kansas City University of Medicine & Biosciences (KCUMB). This presentation is intended for KCUMB educational use only. No part of this presentation may be distributed or reproduced without
Copyright 2018, Kansas City University of Medicine & Biosciences (KCUMB). This presentation is intended for KCUMB educational use only. No part of this presentation may be distributed or reproduced without
Subluxation and Muscle Patterns for the Lower Thoracics Marc Heller, DC
 Subluxation and Muscle Patterns for the Lower Thoracics Marc Heller, DC An extremely common subluxation pattern is a lack of extension, with restricted lateral bending and rotation to one side in the lower
Subluxation and Muscle Patterns for the Lower Thoracics Marc Heller, DC An extremely common subluxation pattern is a lack of extension, with restricted lateral bending and rotation to one side in the lower
3 Movements of the Trunk. Flexion Rotation Extension
 3 Movements of the Trunk Flexion Rotation Extension 1 TRUNK FLEXION 2 TRUNK FLEXION: Rectus Abdominalis O: Crest of Pubis & ligaments covering front of symphysis pubis. I: By «3 portions into cartilages
3 Movements of the Trunk Flexion Rotation Extension 1 TRUNK FLEXION 2 TRUNK FLEXION: Rectus Abdominalis O: Crest of Pubis & ligaments covering front of symphysis pubis. I: By «3 portions into cartilages
Michael L. Kuchera, DO, FAAO March 2014 AAO Convocation. Cervical Fingertip HVLA Workshop Colorado Springs, Colorado
 Cervical Spine HVLA at Your Fingertips Hands-On Workshop Michael L. Kuchera, DO, FAAO, FNAOME Professor & Chairperson, Marian University - College of Osteopathic Medicine Precise Facet Activation at Your
Cervical Spine HVLA at Your Fingertips Hands-On Workshop Michael L. Kuchera, DO, FAAO, FNAOME Professor & Chairperson, Marian University - College of Osteopathic Medicine Precise Facet Activation at Your
West Virginia Osteopathic Medical Association Annual CME Conference. Josephine Shen, DO, MAOM November 3, 2018
 West Virginia Osteopathic Medical Association Annual CME Conference Josephine Shen, DO, MAOM November 3, 2018 Anterior Cervical Fascia Lift Rib Ligamentous Articular Strain Twelfth Rib/Arcuate Ligament/Diaphragm
West Virginia Osteopathic Medical Association Annual CME Conference Josephine Shen, DO, MAOM November 3, 2018 Anterior Cervical Fascia Lift Rib Ligamentous Articular Strain Twelfth Rib/Arcuate Ligament/Diaphragm
Total Body Balancing An integrative approach to optimum treatment and balance Kerry D Ambrogio D.O.M., A.P., P.T., D.O.-M.T.P.
 Total Body Balancing An integrative approach to optimum treatment and balance Kerry D Ambrogio D.O.M., A.P., P.T., D.O.-M.T.P. Each day as a practitioner I am faced with the challenge of trying to understand,
Total Body Balancing An integrative approach to optimum treatment and balance Kerry D Ambrogio D.O.M., A.P., P.T., D.O.-M.T.P. Each day as a practitioner I am faced with the challenge of trying to understand,
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT
 Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT PREPARATION PHASE Individual examination, mechanical testing and tri-planar assessment. Frontal Plane Tests: Adduction Lift
Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT PREPARATION PHASE Individual examination, mechanical testing and tri-planar assessment. Frontal Plane Tests: Adduction Lift
Solving Today s Pain and Injury Puzzle with Erik Dalton An Online Workshop for ABMP Members Session 4 Handout
 Solving Today s Pain and Injury Puzzle with Erik Dalton An Online Workshop for ABMP Members Session 4 Handout Please Note: Erik Dalton teaches his Myoskeletal Alignment Techniques with the expectation
Solving Today s Pain and Injury Puzzle with Erik Dalton An Online Workshop for ABMP Members Session 4 Handout Please Note: Erik Dalton teaches his Myoskeletal Alignment Techniques with the expectation
The Swimmer s Shoulder: An Osteopathic Approach
 The Swimmer s Shoulder: An Osteopathic Approach Mary Solomon, D.O. Rainbow Babies and Children s Hospital Cleveland, OH 440-914-7865 1 I have no relevant relationships/affiliations with any proprietary
The Swimmer s Shoulder: An Osteopathic Approach Mary Solomon, D.O. Rainbow Babies and Children s Hospital Cleveland, OH 440-914-7865 1 I have no relevant relationships/affiliations with any proprietary
Pilates instructor final mat exam - ANSWERS
 Balanced Body - Mat EXAM Pilates instructor final mat exam - ANSWERS Name Date Training Location Examiner Total Points - 60 Passing Grade - 42 1) Which of the following are considered Balanced Body Pilates
Balanced Body - Mat EXAM Pilates instructor final mat exam - ANSWERS Name Date Training Location Examiner Total Points - 60 Passing Grade - 42 1) Which of the following are considered Balanced Body Pilates
A B C. Breathing Concentration Control Centring Precision Flow
 Session Two A B C Breathing Concentration Control Centring Precision Flow Will be based on your group of participants. Ensure that your lesson plan content links to objectives What is the reason for prep?
Session Two A B C Breathing Concentration Control Centring Precision Flow Will be based on your group of participants. Ensure that your lesson plan content links to objectives What is the reason for prep?
ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 4 of 10 Instructor: Paul Sherman, DC
 Online Continuing Education Courses www.onlinece.com www.chirocredit.com ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 4 of 10 Instructor: Paul Sherman, DC Important Notice: This download
Online Continuing Education Courses www.onlinece.com www.chirocredit.com ChiroCredit.com / OnlineCE.com presents Documentation 101 Part 4 of 10 Instructor: Paul Sherman, DC Important Notice: This download
Evidence-Based Examination of the Hip Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs
 Evidence-Based Examination of the Hip Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Hip (1 hour CEU time) Skilled Process
Evidence-Based Examination of the Hip Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Hip (1 hour CEU time) Skilled Process
For more information call , or visit
 Target Coding ICD-10 List for Chiropractic HEADACHE G43: Migraine G43.0: Migraine without aura (common migraine) G43.009: Migraine without aura, not intractable, without status migrainosus (migraine without
Target Coding ICD-10 List for Chiropractic HEADACHE G43: Migraine G43.0: Migraine without aura (common migraine) G43.009: Migraine without aura, not intractable, without status migrainosus (migraine without
Jennifer Lorine, DO. Practical Application of OMT in the Office: The Counterstrain Edition. Disclosures. Objectives
 Practical Application of OMT in the Office: The Counterstrain Edition August 4, 2018 POFPS Disclosures Dr. Lorine has provided no disclosures. Objectives For the audience to have a better understanding
Practical Application of OMT in the Office: The Counterstrain Edition August 4, 2018 POFPS Disclosures Dr. Lorine has provided no disclosures. Objectives For the audience to have a better understanding
Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives
 1 2 Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives List the muscular and ligamentous attachments of the thoracic and lumbar spine Describe how the muscles affect the spine and upper extremity
1 2 Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives List the muscular and ligamentous attachments of the thoracic and lumbar spine Describe how the muscles affect the spine and upper extremity
THE OSTEOPATHIC WORKSHOP: NECK PAIN
 THE OSTEOPATHIC WORKSHOP: NECK PAIN Trevine R. Albert, D.O. M.S. Family Medicine Neuromusculoskeletal Medicine PGY-3 2018 FSACOFP Convention DISCLOSURES There are no actual or potential personal, financial
THE OSTEOPATHIC WORKSHOP: NECK PAIN Trevine R. Albert, D.O. M.S. Family Medicine Neuromusculoskeletal Medicine PGY-3 2018 FSACOFP Convention DISCLOSURES There are no actual or potential personal, financial
Examination of the lumbosacral spine. Dr Lucy Holtzhausen Rotorua GP CME June 2015
 Examination of the lumbosacral spine Dr Lucy Holtzhausen Rotorua GP CME June 2015 Diagnostic Algorithm Presenting symptoms Diagnostic decisions Diagnostic triage LOW BACK PAIN Mechanical NON-SPECIFIC LBP
Examination of the lumbosacral spine Dr Lucy Holtzhausen Rotorua GP CME June 2015 Diagnostic Algorithm Presenting symptoms Diagnostic decisions Diagnostic triage LOW BACK PAIN Mechanical NON-SPECIFIC LBP
Chiropractic ICD-10 Common Codes List
 Chiropractic ICD-10 Common Codes List This is a preliminary list of Common ICD-10 Codes for chiropractic diagnoses. This is a common code list to be used as a guide for coding and is not intended to represent
Chiropractic ICD-10 Common Codes List This is a preliminary list of Common ICD-10 Codes for chiropractic diagnoses. This is a common code list to be used as a guide for coding and is not intended to represent
External Obliques Abdominal muscles that attaches at the lower ribs, pelvis, and abdominal fascia.
 The Core The core is where most of the body s power is derived. It provides the foundation for all movements of the arms and legs. The core must be strong, have dynamic flexibility, and function synergistically
The Core The core is where most of the body s power is derived. It provides the foundation for all movements of the arms and legs. The core must be strong, have dynamic flexibility, and function synergistically
Chiropractic Glossary
 Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs Chapter Five: Movement Examination of the Lumbar Spine Time) (45 minutes
Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs Chapter Five: Movement Examination of the Lumbar Spine Time) (45 minutes
 www.fisiokinesiterapia.biz Laboratory Manual Evidence based Examination & Selected Interventions for Patients with Lumbo Pelvic Spine & Hip Disorders www.evidenceinmotion.com Evidence based Examination
www.fisiokinesiterapia.biz Laboratory Manual Evidence based Examination & Selected Interventions for Patients with Lumbo Pelvic Spine & Hip Disorders www.evidenceinmotion.com Evidence based Examination
IFAST Assessment. Name: Date: Sport: Review Health Risk Assessment on initial consult form. List Client Goals (what brings you here?
 IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
MOTION PALPATION GUIDE
 MOTION PALPATION GUIDE C1 What s happening C1 is moving anterior and superior on the occipital condyles causing a Superior atlas. What you feel - The t.p. s will move, bilaterally in the anterior direction,
MOTION PALPATION GUIDE C1 What s happening C1 is moving anterior and superior on the occipital condyles causing a Superior atlas. What you feel - The t.p. s will move, bilaterally in the anterior direction,
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
Chiro-Tech IV Midterm Questions
 hiro-tech IV Midterm Questions 1. What is NOT a factor in shaping the Lumbar lordosis?. Wedge shaped L-S IV.. L5 vertebral body is wedge-shaped.. The size of the Sacrum.. Inclination of the vertebrae above
hiro-tech IV Midterm Questions 1. What is NOT a factor in shaping the Lumbar lordosis?. Wedge shaped L-S IV.. L5 vertebral body is wedge-shaped.. The size of the Sacrum.. Inclination of the vertebrae above
the back book Your Guide to a Healthy Back
 the back book Your Guide to a Healthy Back anatomy Your spine s job is to: Support your upper body and neck Increase flexibility of your spine Protect your spinal cord There are 6 primary components of
the back book Your Guide to a Healthy Back anatomy Your spine s job is to: Support your upper body and neck Increase flexibility of your spine Protect your spinal cord There are 6 primary components of
Anatomy - Reconnect with your Spine Muscles by NFPT Idea World 2016 : Session 449 Friday July 15th 9:40-11:30am Beverly Hosford, MA
 Anatomy - Reconnect with your Spine Muscles by NFPT Idea World 2016 : Session 449 Friday July 15th 9:40-11:30am Beverly Hosford, MA Posture Core Anatomy Awareness Action 1. Anatomy *Know the muscle attachments.
Anatomy - Reconnect with your Spine Muscles by NFPT Idea World 2016 : Session 449 Friday July 15th 9:40-11:30am Beverly Hosford, MA Posture Core Anatomy Awareness Action 1. Anatomy *Know the muscle attachments.
R. C. Walsh, Jr., DO, Col, TXANG Chief, Aerospace Medicine 136 AW/GMU
 R. C. Walsh, Jr., DO, Col, TXANG Chief, Aerospace Medicine 136 AW/GMU Objectives List the indications for OMM in the military patient Identify the appropriate OMT techniques that can be used in an austere
R. C. Walsh, Jr., DO, Col, TXANG Chief, Aerospace Medicine 136 AW/GMU Objectives List the indications for OMM in the military patient Identify the appropriate OMT techniques that can be used in an austere
MUSCLE ENERGY FOR CERVICAL SPINE. Dr. Gabrielle Koczab, DO Medical director Bedford Primary Care Core Teaching Faculty UH Regional Hospitals
 MUSCLE ENERGY FOR CERVICAL SPINE Dr. Gabrielle Koczab, DO Medical director Bedford Primary Care Core Teaching Faculty UH Regional Hospitals LEARNING OBJECTIVES 1. List conditions in which muscle energy
MUSCLE ENERGY FOR CERVICAL SPINE Dr. Gabrielle Koczab, DO Medical director Bedford Primary Care Core Teaching Faculty UH Regional Hospitals LEARNING OBJECTIVES 1. List conditions in which muscle energy
The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University
 The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University The Trunk and Spinal Column Vertebral column 24 articulating vertebrae 31 pairs of spinal nerves Abdominal muscles some
The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University The Trunk and Spinal Column Vertebral column 24 articulating vertebrae 31 pairs of spinal nerves Abdominal muscles some
OSTEOPATHIC PRINCIPLES AND PRACTICE: OMT IN 2018
 OSTEOPATHIC PRINCIPLES AND PRACTICE: OMT IN 2018 Walter B. Flesner III, D.O. Medical Director, ICPR, Cape Coral Florida. Past President, Florida Osteopathic Medical Association 1996-1997. Jon P. Burdzy,
OSTEOPATHIC PRINCIPLES AND PRACTICE: OMT IN 2018 Walter B. Flesner III, D.O. Medical Director, ICPR, Cape Coral Florida. Past President, Florida Osteopathic Medical Association 1996-1997. Jon P. Burdzy,
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK
 ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
Structure and Function of the Vertebral Column
 Structure and Function of the Vertebral Column Posture Vertebral Alignment Does it really matter? Yes it does! Postural Curves The vertebral column has a series of counterbalancing curves posterior anterior
Structure and Function of the Vertebral Column Posture Vertebral Alignment Does it really matter? Yes it does! Postural Curves The vertebral column has a series of counterbalancing curves posterior anterior
32b Passive Stretches: Guided Full Body
 32b Passive Stretches: Guided Full Body 32b Passive Stretches: Guided Full Body! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:" 25 minutes "Lecture:" 15
32b Passive Stretches: Guided Full Body 32b Passive Stretches: Guided Full Body! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:" 25 minutes "Lecture:" 15
TRAINING THE CORE BEGIN WITH ONE SET OF ALL 17 EXERCISES FOR A TOTAL OF 250 REPS. NEXT, MOVE TO TWO SETS FOR A TOTAL OF 500 REPS.
 TRAINING THE CORE 1. LATERAL SIT UPS.X 20 (10 EACH SIDE) 2. HYPEREXTENSIONS.X 10 3. LEG HUGS...X 15 4. RUSSIAN TWIST X 20 (10 EACH SIDE) 5. HIP CURLS..X 14 (7 EACH LEG) 6. JACK KNIFES..X 10 7. REVERSE
TRAINING THE CORE 1. LATERAL SIT UPS.X 20 (10 EACH SIDE) 2. HYPEREXTENSIONS.X 10 3. LEG HUGS...X 15 4. RUSSIAN TWIST X 20 (10 EACH SIDE) 5. HIP CURLS..X 14 (7 EACH LEG) 6. JACK KNIFES..X 10 7. REVERSE
OMT FOR THE PERFORMING ARTIST
 OMT FOR THE PERFORMING ARTIST Sajid A. Surve, DO Associate Professor, UNTHSC-TCOM Co-Director, UNT Texas Center for Performing Arts Health http://tcpah.unt.edu Occupation History for the Performer Pertinent
OMT FOR THE PERFORMING ARTIST Sajid A. Surve, DO Associate Professor, UNTHSC-TCOM Co-Director, UNT Texas Center for Performing Arts Health http://tcpah.unt.edu Occupation History for the Performer Pertinent
Algorithm #1 Lumbo-Pelvic Region Examination
 Red Screen for Potentially Serious Conditions (i.e., Red Flags) including Neurologic when indicated Positive Findings Algorithm #1 Lumbo-Pelvic Region Clinical Prediction Rule Screening: Duration of symptoms
Red Screen for Potentially Serious Conditions (i.e., Red Flags) including Neurologic when indicated Positive Findings Algorithm #1 Lumbo-Pelvic Region Clinical Prediction Rule Screening: Duration of symptoms
WELCOME TO KCUMB-COM ACOP
 WELCOME TO KCUMB-COM ACOP WELCOME TO THE CITY OF FOUNTAINS! Osteopathic Approach to the Pediatric Patient Objectives At the end of the workshop the attendee will be able to: Discuss the musculoskeletal
WELCOME TO KCUMB-COM ACOP WELCOME TO THE CITY OF FOUNTAINS! Osteopathic Approach to the Pediatric Patient Objectives At the end of the workshop the attendee will be able to: Discuss the musculoskeletal
Functional Movement Screen (Cook, 2001)
") Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
2017 COS ANNUAL MEETING AND EXHIBITION HOME EXERCISES
 UPPER BODY Push Up From a push up position. Lower whole body down to floor. Press up to return to start position. Maintain abdominal hollow and neutral spinal alignment throughout movement. Note: Perform
UPPER BODY Push Up From a push up position. Lower whole body down to floor. Press up to return to start position. Maintain abdominal hollow and neutral spinal alignment throughout movement. Note: Perform
Osteoporosis Protocol
 PRODUCTS HELPING PEOPLE HELP THEMSELVES! Osteoporosis Protocol Rehabilitation using the Resistance Chair General Information Osteoporosis is a condition where bones gradually decrease in mass or density
PRODUCTS HELPING PEOPLE HELP THEMSELVES! Osteoporosis Protocol Rehabilitation using the Resistance Chair General Information Osteoporosis is a condition where bones gradually decrease in mass or density
Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual
 Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual 2nd Edition Isabelle M. Bohman, M.S., P.T., NDT Coordinator Instructor TM Published by Clinician s View Albuquerque, NM 505-880-0058
Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual 2nd Edition Isabelle M. Bohman, M.S., P.T., NDT Coordinator Instructor TM Published by Clinician s View Albuquerque, NM 505-880-0058
Institute of Holistic Healthcare. Certificate in Orthopaedic Manipulative Therapy PROSPECTUS
 Institute of Holistic Healthcare Certificate in Orthopaedic Manipulative Therapy PROSPECTUS 2019 Contents Contents... 1 Aims:... 2 Objectives:... 2 Format of the Program:... 3 Program... 3 Continuing Professional
Institute of Holistic Healthcare Certificate in Orthopaedic Manipulative Therapy PROSPECTUS 2019 Contents Contents... 1 Aims:... 2 Objectives:... 2 Format of the Program:... 3 Program... 3 Continuing Professional
Gonstead Technique Study Sheet Fall 2006
 Patient Lower Cervical Adjustments (C2-C7) PR Right index, distallateral Right posterior inferior spinous process P-A, R-L through pts opposite eye, *** along plane line of PL Left index, distallateral
Patient Lower Cervical Adjustments (C2-C7) PR Right index, distallateral Right posterior inferior spinous process P-A, R-L through pts opposite eye, *** along plane line of PL Left index, distallateral
Please note. The following notes are 2017 Donna Farhi and Laura Stuart. They are for your personal study only, not for distribution or commercial use.
 Please note The following notes are 2017 Donna Farhi and Laura Stuart. They are for your personal study only, not for distribution or commercial use. Farhi & Stuart Model for Joint Function Form Closure
Please note The following notes are 2017 Donna Farhi and Laura Stuart. They are for your personal study only, not for distribution or commercial use. Farhi & Stuart Model for Joint Function Form Closure
The theory and practice of getting fitter and stronger
 The theory and practice of getting fitter and stronger David Docherty, PhD, Professor Emeritus School of Exercise Science, Physical and Health Education University of Victoria All the presentations are
The theory and practice of getting fitter and stronger David Docherty, PhD, Professor Emeritus School of Exercise Science, Physical and Health Education University of Victoria All the presentations are
Payment Policy. Chiropractic Care. Policy Specific Section: September 10, 2012 November 10, 2012
 Payment Policy Chiropractic Care Type: Payment Policy Policy Specific Section: Payment Original Policy Date: Effective Date: September 10, 2012 November 10, 2012 Description Chiropractic is a branch of
Payment Policy Chiropractic Care Type: Payment Policy Policy Specific Section: Payment Original Policy Date: Effective Date: September 10, 2012 November 10, 2012 Description Chiropractic is a branch of
PTA 210 PTA Techniques
 PTA 210 PTA Techniques Patient Positioning and Draping INTRO Patient Positioning Must be considered before, during and after treatment AND when the patient is to be at rest for a prolonged period of time
PTA 210 PTA Techniques Patient Positioning and Draping INTRO Patient Positioning Must be considered before, during and after treatment AND when the patient is to be at rest for a prolonged period of time
OMT in the Acute Care Setting. David C. Mason, DO, MBA, FACOFP Chair Department of Family Medicine and Osteopathic Manipulative Medicine UNTHSC-TCOM
 OMT in the Acute Care Setting David C. Mason, DO, MBA, FACOFP Chair Department of Family Medicine and Osteopathic Manipulative Medicine UNTHSC-TCOM Learning Objectives Discuss likely patient presentations
OMT in the Acute Care Setting David C. Mason, DO, MBA, FACOFP Chair Department of Family Medicine and Osteopathic Manipulative Medicine UNTHSC-TCOM Learning Objectives Discuss likely patient presentations
Functional Movement Test. Deep Squat
 Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
Functional Movement Test Put simply, the FMS is a ranking and grading system that documents movement patterns that are key to normal function. By screening these patterns, the FMS readily identifies functional
Richard L Van Buskirk, DO, PhD, FAAO
 Richard L Van Buskirk, DO, PhD, FAAO I approach the osteopathic concept as if the body is a biomechanical, electrochemical machine: If a part is not working quite right then the body will find a compensating
Richard L Van Buskirk, DO, PhD, FAAO I approach the osteopathic concept as if the body is a biomechanical, electrochemical machine: If a part is not working quite right then the body will find a compensating
General Principles of Stretching. To be effective, stretching must be done slowly, gently and frequently.
 General Principles of Stretching To be effective, stretching must be done slowly, gently and frequently. Slowly means that while the exercise is being done the muscle being stretched must be moved slowly
General Principles of Stretching To be effective, stretching must be done slowly, gently and frequently. Slowly means that while the exercise is being done the muscle being stretched must be moved slowly
WEEKEND 1 CERVICAL SPINE
 Virginia Orthopedic Manual Physical Therapy Institute - Technique Manual WEEKEND 1 CERVICAL SPINE Cervical Active Range of Motion Testing Rotation CT Flexion Mid Cervical Flexion Extension Side-Bending
Virginia Orthopedic Manual Physical Therapy Institute - Technique Manual WEEKEND 1 CERVICAL SPINE Cervical Active Range of Motion Testing Rotation CT Flexion Mid Cervical Flexion Extension Side-Bending
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Osteoporosis Exercise:
 Osteoporosis Exercise: Balance, Posture and Functional Exercises Osteoporosis Exercise: Weight-Bearing and Muscle Strengthening Exercises Introduction You can help improve and maintain your balance, posture
Osteoporosis Exercise: Balance, Posture and Functional Exercises Osteoporosis Exercise: Weight-Bearing and Muscle Strengthening Exercises Introduction You can help improve and maintain your balance, posture
TRAINING LAB SKELETAL REMAINS: IDENTIFYING BONES NAME
 TRAINING LAB SKELETAL REMAINS: IDENTIFYING BONES NAME Background: Skeletal remains are important pieces of evidence. The flesh, muscle, and organs of a victim rapidly decompose; however, the victim s skeleton
TRAINING LAB SKELETAL REMAINS: IDENTIFYING BONES NAME Background: Skeletal remains are important pieces of evidence. The flesh, muscle, and organs of a victim rapidly decompose; however, the victim s skeleton
Body Organizations Flashcards
 1. What are the two main regions of the body? 2. What three structures are in the Axial Region? 1. Axial Region (Goes down midline of the body) 2. Appendicular Region (limbs) 3. Axial Region (Goes down
1. What are the two main regions of the body? 2. What three structures are in the Axial Region? 1. Axial Region (Goes down midline of the body) 2. Appendicular Region (limbs) 3. Axial Region (Goes down
Exercises to restore range of movement: Rotation
 Exercises to restore range of movement: Rotation Start position: Sitting upright with your back supported in a chair. Position your head so it is evenly balanced, looking forward. Avoid allowing your head
Exercises to restore range of movement: Rotation Start position: Sitting upright with your back supported in a chair. Position your head so it is evenly balanced, looking forward. Avoid allowing your head
Cervico-Thoracic Management Exercise and Manual Therapy. Deep Neck Flexor Training. Deep Neck Flexor Training. FPTA Spring 2011 Eric Chaconas 1
 Cervico-Thoracic Management Exercise and Manual Therapy Eric Chaconas PT, DPT, CSCS, FAAOMPT Deep Neck Flexor Training Evidence of dysfunction in the longus coli and longus capitus. Chronic Neck Pain Idiopathic
Cervico-Thoracic Management Exercise and Manual Therapy Eric Chaconas PT, DPT, CSCS, FAAOMPT Deep Neck Flexor Training Evidence of dysfunction in the longus coli and longus capitus. Chronic Neck Pain Idiopathic
Static Back. Instructions: Purpose: Hold this ecise for 05 min. prepared for Pain Free Posture MN
 1 Static Back Hold this ecise for 05 min. 1. Lie on your back with your legs up over a block or chair 2. Place your arms out to the sides at 45 degrees from your body with palms up 3. Relax your upper
1 Static Back Hold this ecise for 05 min. 1. Lie on your back with your legs up over a block or chair 2. Place your arms out to the sides at 45 degrees from your body with palms up 3. Relax your upper
5 minutes: Attendance and Breath of Arrival. 50 minutes: Problem-Solving: Back
 Low Back Pain 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem-Solving: Back Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of
Low Back Pain 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem-Solving: Back Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of
The Back. Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa
 The Back Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa The spine has to meet 2 functions Strength Mobility Stability of the vertebral column is provided by: Deep intrinsic muscles of the back Ligaments
The Back Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa The spine has to meet 2 functions Strength Mobility Stability of the vertebral column is provided by: Deep intrinsic muscles of the back Ligaments
Balanced Body Movement Principles. How the Body Works and How to Train It Module 2: Trunk Integration. Copyright 2017, Balanced Body Education LLC.
 Balanced Body Movement Principles How the Body Works and How to Train It Module 2: Trunk Integration Trunk Integration Module 2: Key Principles Breathing Core work Transverse Abdominis, Multifidi, Pelvic
Balanced Body Movement Principles How the Body Works and How to Train It Module 2: Trunk Integration Trunk Integration Module 2: Key Principles Breathing Core work Transverse Abdominis, Multifidi, Pelvic
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Myoskeletal Alignment for Low Back, Hip, and Leg Pain DVDs
 Myoskeletal Alignment for Low Back, Hip, and Leg Pain DVDs Use these handy time markers to locate the specific treatment techniques on the Level 4 Dynamic Body 6 DVD set as demonstrated by Erik Dalton
Myoskeletal Alignment for Low Back, Hip, and Leg Pain DVDs Use these handy time markers to locate the specific treatment techniques on the Level 4 Dynamic Body 6 DVD set as demonstrated by Erik Dalton
The vault bones Frontal Parietals Occiput Temporals Sphenoid Ethmoid
 The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
The hip: Built for endurance and mobility
 The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
An Osteopathic Approach to Upper Extremity Pain Syndromes. Laura Griffin, D.O. FAAO American Academy of Osteopathy OMED 2014
 An Osteopathic Approach to Upper Extremity Pain Syndromes Laura Griffin, D.O. FAAO American Academy of Osteopathy OMED 2014 Outline Differential diagnosis for upper extremity pain Clinical presentations
An Osteopathic Approach to Upper Extremity Pain Syndromes Laura Griffin, D.O. FAAO American Academy of Osteopathy OMED 2014 Outline Differential diagnosis for upper extremity pain Clinical presentations
SCIATICA. Contents YOUR GUIDE TO. An IPRS Guide to provide you with exercises and advice to ease your condition. What is sciatica?...
 Contents What is sciatica?................................................3 What causes sciatica?............................................3 YOUR GUIDE TO SCIATICA An IPRS Guide to provide you with exercises
Contents What is sciatica?................................................3 What causes sciatica?............................................3 YOUR GUIDE TO SCIATICA An IPRS Guide to provide you with exercises
Physical Sense Activation Programme
 Flexion extension exercises for neck and upper back Sitting on stool Arms hanging by side Bend neck and upper back Breathe out Extend your neck and upper back Lift chest to ceiling Squeeze shoulder blades
Flexion extension exercises for neck and upper back Sitting on stool Arms hanging by side Bend neck and upper back Breathe out Extend your neck and upper back Lift chest to ceiling Squeeze shoulder blades
PART ONE. Belly Dance Fitness Technique
 PART ONE Belly Dance Fitness Technique OVERVIEW Understanding belly dance movement The gentle, symmetrical, rhythmic undulations that we practice in Belly dance can help to revitalize almost every part
PART ONE Belly Dance Fitness Technique OVERVIEW Understanding belly dance movement The gentle, symmetrical, rhythmic undulations that we practice in Belly dance can help to revitalize almost every part
 Back to Basics Technique Compendium www.fisiokinesiterapia.biz Pelvic torsion: Frontal plane Pelvic torsion: Sagittal plane Pelvic Torsion: Principal Contacts lumbar apex short lever long lever medium
Back to Basics Technique Compendium www.fisiokinesiterapia.biz Pelvic torsion: Frontal plane Pelvic torsion: Sagittal plane Pelvic Torsion: Principal Contacts lumbar apex short lever long lever medium
Contraindicated and High-Risk Exercises
 Contraindicated and High-Risk Exercises Young sub Kwon, Ph.D. ACSM RCEP, NSCA CSCS,*D Exercise Physiology Laboratory The University of New Mexico Albuquerque, NM, USA Introduction Any activity selected
Contraindicated and High-Risk Exercises Young sub Kwon, Ph.D. ACSM RCEP, NSCA CSCS,*D Exercise Physiology Laboratory The University of New Mexico Albuquerque, NM, USA Introduction Any activity selected