Deprescribing with Confidence Dr Sanjay Suman MD FRCP
|
|
|
- Kathlyn Holland
- 5 years ago
- Views:
Transcription

1 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent

2 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas 2010;246-50
3 What is Deprescribing? Process Required for the safe and effective cessation of inappropriate medication Taking into account Patient s physical functioning co-morbidities preferences lifestyle DTB 52:2014


4 Context Polypharmacy Causative factors Adverse outcomes Medication Review Deprescribing / Rational prescribing

 2016")



5 Context Increasing prevalence of multimorbidity NICE Guidance (ng 56) 2016 >50% of 85 years + 3 Long Term conditions Melzer D et al. Age Ageing 2014;ageing.afu113 Year Lifestyle Diseases commonest in the list of multimorbidities


6 Dementia Public Health England Dementia: Applying All Our Health Updated 23 January 2018



7 Multimorbidity: NICE Guidance (ng 56) 2016 Treatment Burden -Multiple appointments -Polypharmacy Maybe due to Focus on Primary Prevention Single health condition guidelines Based on Trials that recruit individuals Without multimorbidity Who take fewer medications

8 Case Study 85 years old Male PMH Hypertension, OA, T2DM, CKD Complaints Dizziness Diarrhoea Weight loss Episodic confusion Medications Ramipril 5 mg od Atorvastatin 10 mg od Doxazosin 2 mg od Metformin 1 gm bd Gliclazide 80 mg bd Tramadol 25mg PRN
9 Polypharmacy Historical Definition: Prescription 4 / 5 drugs No. of medications Yrs 28.9% 7.4% 80 Yrs 51.8% 18.6% Prevalence of Polypharmacy in a Scottish Primary care Population Payne et al. Eur J Cl Pharmacol 2004;
10 Polypharmacy Current Take on understanding the issue Appropriate Inappropriate Established co-morbidities Risk outweighs benefit Shared Goals Drug class duplication Effective & tolerated Co-prescribing drugs with potential interactions Spinewine A et al. Lancet 2007;370(9582): Hanlon JT et al. JAGS. 2001;49: Fisk D et al. Arch Intern Med. 2003;163: Steinman et al. JAGS. 2006;54: Omission of medications that are -effective -well tolerated -for established indications highly inappropriate

11 Multiple Prescribers / Silo prescribing Single Health Condition: narrow focus


12 Prescribing Cascade Adverse effects of a medication Treated with prescription of another drug Any new symptom maybe adverse drug effect: STOP, THINK

13 Adverse Drug Events (ADE s) Adverse Drug Reactions (ADR s) Noxious Unintended Undesired effects Medication Errors Prescribing Dispensing Administering


14 ADE s: Contributing Factors Drug Related Complex regimes Narrow therapeutic index drugs 60% Patient Related Living alone Cognitive impairment Physical frailty Poor vision/ Dexterity Poor compliance Clinician Related Inappropriate prescribing Failure to: -adjust Dose -monitor - analyse risk V benefit NPS MEDICINEWISE Sep 2013 Based on data: Roughead EE et al 2004; 13:83-7
15 ADE s: Impact Account for 6.5 % of hospital admissions 1 50% of Hospital Admissions due to Adverse Drug Effects are preventable Case fatality for those admitted to hospital: 4.7%² 70% of these are in individuals > 70 years old and on 5 medications Cost to NHS 466 million / annum³ ¹Medicines optimisation: ²Wu et al JR Soc Med. 2010;103(6): ³Pirmohamed et al BMJ 2004; 329: Scottish Government Polypharmacy Model of Care Group. Polypharmacy Guidance, Realistic Prescribing 3rd Edition, Scottish Governmen
16 ADE s: Polypharmacy contributes strongly Drug-Drug interactions Errors in dispensing Non- adherence Risk of overdose Fermer RE, Arenson JK. BMJ 2006; 333:143-5

17

18 Age related changes risk of ADR s ADR s Pharmacokinetics How the body handles drugs Pharmacodynamics How the drug affects the body
19 Effect of ageing on Pharmacokinetics Physiological Change Effect Drugs most affected Absorption ph & motility absorption Iron, Calcium Distribution body fat Body water Elimination half life Serum level Benzodiazepines Morphine Digoxin, Lithium, Theophylline Metabolism hepatic mass, blood flow first pass metabolism Serum level Propranolol, GTN, Lisinopril, Oxycodone, Atorvastatin Renal excretion GFR Serum level Digoxin, Lithium, Gentamicin, ACEi How the body handles drugs

20 Prevalence (%) Prevalence of CKD with age CKD stage Stage 4 Stage 3 Stage 2 Stage Prevalence of CKD by age group How the body handles drugs Anderson S et al. J Am Soc Nephrol. 2009;20:
21 Ageing enhances susceptibility to ADR s Impairment Drug class Adverse outcome Cholinergic activity Drugs acting on *CNS Delirium Cognitive impairment Falls Baroreceptor reflex Vasodilators Postural hypotension Falls How the drug affects the body *CNS: Central Nervous System




22 Common ADR s in frail individuals Falls Hypoglycaemia ADR s Delirium Dehydration Electrolyte imbalance Acute Kidney Injury
 Benzodiazepines Anti-epileptics Postural Hypotension Diuretics Alpha-blockers Beta blockers Ace-inhibitors Nitrates Parkinson s disease")
23 High risk medications: Falls Sedation/Drowsiness Antidepressants Antipsychotics Hypnotics Antihistamines Opiates Impaired Postural Stability Hypnotics (Z drugs) Benzodiazepines Anti-epileptics Postural Hypotension Diuretics Alpha-blockers Beta blockers Ace-inhibitors Nitrates Parkinson s disease medications



24 Baroreceptor reflex maintains BP Vasoconstriction + Heart rate Blood Pressure Restored Postural Hypotension X X Age related Impaired baroreceptor reflex enhances the ADR s of cardiovascular drugs Vasodilators β blockers
25 Orthostatic Hypotension (OH) OH Definition A drop of 20 mmhg in systolic or 10 mmhg in diastolic after 3 minutes of standing Important Causes Medications Autonomic failure Fluid depletion
26 Management of OH Stop the offending medication Alpha blockers (Doxazosin, Tamsulosin) Diuretics ACE-inhibitors Nitrates General Measures Fluid intake ( L) Increase salt intake (2-10g) if not contraindicated Adopt strategic getting up strategy Lie propped up at night with a head up tilt degrees (pillow height cm) Full length Gr 2-3 compression hosiery, Lower Limbs Pharmacological (usually initiated by specialists) Fludrocortisone microgram / d Midodrine mg tds ESC 2009, Eur Heart J 2009; 30:


27 ADR s: Cognition Benzodiazepine exposure is associated with increased risk of Alzheimer s Greater the length of exposure, stronger the risk
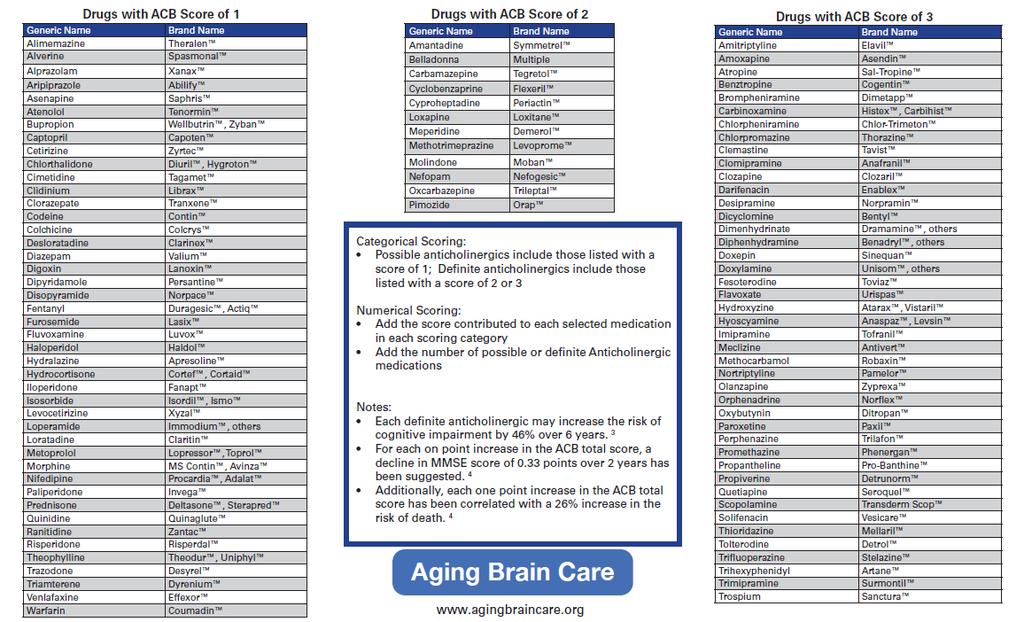

28 Estimating the anticholinergic burden
")
29 Lists commonly used drugs with anticholinergic properties Grades each drug with a score 1= Possible anticholinergic 2= Definite anticholinergic 3= Definite anticholinergic Each 1 point score risk of Cognitive impairment by 46% (over 6 years) Death by 26%


30 Benzodiazepines and hypnotics safety Kripke DF, Langer RD, Kline LE. BMJ Open. 2012;2:e


31 Benzodiazepines and hypnotics safety Which policies were effective?

32 Opiate potency compared to morphine Highly addictive 1/3 rd of opiate related deaths in US linked to prescribed opiates Common side effects in elderly include falls, constipation, delirium

33 Incident rate ratio Hypoglycaemia risk in elderly Diabetics with Renal impairment 1,2 In elderly people (>70 years) hypoglycaemia occurs more frequently in subjects with CKD stages With CKD Without CKD 1. Haneda M, Morikawa A. Nephrol Dial Transplant. 2009; 24: Adapted from Moen M et al. Clin J Am Soc Nephrol. 2009; 4:

34 CKD Cautions with Diabetes treatment
35 HbA1C Targets according to functional & cognitive status Functional/Cognitive Status HbA1C (%) HbA1C (mmol/mol) Functionally independent Functionally dependent Frail Up-to Dementia Up-to
36 Case Study Mr D, 85 years PMH Hypertension, OA, T2DM, CKD Complaints Dizziness Diarrhoea Weight loss Episodic confusion Medications Ramipril 5 mg od Atorvastatin 10 mg od Doxazosin 2 mg od Metformin 1 gm bd Gliclazide 80 mg bd Tramadol 50mg PRN Examination Weight 48 Kg, BMI 17 BP Lying 110 / 70, standing 80 /60 HR 60 regular, Gait: unsteady Recent Blood tests HbA1C 43, egfr40
37 Case Study Mr D, 85 years old 2 Falls in last 3 months What will you do next? o Stop Doxazosin o Stop Gliclazide o Reduce Metformin dose o Reduce Ramipril dose o All of the above Medications Ramipril 5 mg od Atorvastatin 10 mg od Doxazosin 2 mg od Metformin 1 gm bd Gliclazide 80 mg bd Tramadol 50mg PRN Examination Weight 48 Kg, BMI 17 BP Lying 110 / 70, standing 80 /60 HR 60 regular, Gait: unsteady Recent Blood tests HbA1C 43, egfr40

38 I feel a lot better since I ran out of those pills you gave me
39 Types and Levels of Medication Review Level 3 Clinical Medication Review Level 2 Treatment review Increasing Frailty severity status Multimorbidity Numbers of medications Suspected ADR s Falls Delirium End of Life Level 1 Prescription Review




40 Medication Review Process leading to Deprescribing Assess Monitor Define goal Stop Reduce Replace Drugs: critical analysis Risk Vs benefit for each drug

41 How often should medication review take place? Opportunistically 6 monthly if on 4 drugs Annually for all >75 years old General Practice Contract Requirement 2017/18 MARCH 2017


42 Practice Based Clinical Pharmacists Important Role in managing long term health conditions Inappropriate polypharmacy reduction Medicine Reconciliation

43 Tools for Polypharmacy reduction Beer s Criteria List 53 potentially inappropriate medications Endorsed by American Geriatrics Society 2012 STOPP / START Criteria Validated and relevant for UK population Endorsed by British Geriatrics Society Guidelines.co.uk/NiceMedOpt
44 Case 2: Mrs J, 81 requests appointment (3 rd in 4 months) PMH: Hypertension, Hypothyroidism Present History Previous 2 GP contacts for constipation still a problem + tired all the times, mobility Consent obtained from Patient for picture to be used for educational presentation Medications Co-Codamol 2 tabs qds Atenolol 50 mg od Simvastatin 40 mg od Levothyroxine 100 mcg od Laxido & Senna not helping
45 Case 2: Mrs J, 81 requests appointment (3 rd in 4 months) What will you do next o Try another laxative o Stop Co-Codamol o Check Thyroid Function o Reassure and follow up PMH: Hypertension, Hypothyroidism Present History Previous 2 GP contacts for constipation still a problem + tired all the times, mobility Medications Co-Codamol 2 tabs qds Atenolol 50 mg od Simvastatin 40 mg od Levothyroxine 100 mcg od Laxido & Senna not helping


46 Case 2: Mrs J has not been taking her Thyroxine as prescribed Constipation Tiredness Reduced Mobility TSH 65 mu/l Coarse facial features Receding hairline Loss of outer 1/3 rd of eyebrows
47 Prescribing for elderly: Considerations Any new symptom maybe adverse drug effect: STOP, THINK Non pharmacological measures remain underutilised Start low, go slow but use enough Life expectancy, functional and cognitive status play a role in shared decision making Quality of life matters most to people
48 Prescribing for elderly: Considerations Focus on common medications NSAID Proton Pump Inhibitors Opiates Hypnotics Benzodiazepines Antipsychotics (for behavioural and psychological symptoms in Dementia) Diuretics for leg oedema Antihypertensives Oral Hypoglycaemic agents Are any medications not being prescribed that need to be? Examples: Osteoporosis Anticoagulation in Atrial fibrillation

49 Prescribing for elderly: Considerations

50 Holistic Approach Guideline Medicine Care & Support Planning Single LTC Standardised Care Multimorbidity Frailty Personalised Care
51 Assessment for frailty / individuals approaching end of life Individualised Management plan Personal goals optimisation plans Advance care plan Psychological Social Comprehensive Geriatric Assessment Functional Medical Multimorbidity: NICE Guidance (ng 56) 2016
52 Conclusions Inappropriate prescribing runs risk of adverse effects particularly for frail elderly Establish local systems for regular medication reviews leading to rational prescribing for elderly / people with multimorbidity and frailty

53 Resources for further reading Thank you for listening
Frailty & Polypharmacy
 Frailty & Polypharmacy Elderly with LUTS Recognition and Management Dr Sanjay Suman MD FRCP Clinical Director Elderly Care Medway Maritime Hospital Kent Declaration of interests Honoraria and Advisory
Frailty & Polypharmacy Elderly with LUTS Recognition and Management Dr Sanjay Suman MD FRCP Clinical Director Elderly Care Medway Maritime Hospital Kent Declaration of interests Honoraria and Advisory
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Optimising prescribing in primary care in the face of multimorbidity and polypharmacy
 University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
University of Dundee School of Medicine Optimising prescribing in primary care in the face of multimorbidity and polypharmacy Bruce Guthrie Professor of Primary Care Medicine, University of Dundee NICE
Polypharmacy. A CPPE distance learning programme
 A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
A CPPE distance learning programme DLP 177 January 2016 Contents About CPPE distance learning programmes About this learning programme Glossary of key terms v vii ix Contents Section 1 The problem with
Pharmacology in the Elderly
 Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Pharmacology in the Elderly James Hardy Geriatrician, Royal North Shore Hospital A recent consultation Aspirin Clopidogrel Warfarin Coloxyl with senna Clearlax Methotrexate Paracetamol Pantoprazole Cholecalciferol
Polypharmacy. Polypharmacy. Suboptimal Prescribing in Older Adults. Kenneth Schmader, MD Professor of Medicine-Geriatrics
 Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Falls Assessment and Medication
 Falls Assessment and Medication Professor T.Masud President-Elect British Geriatrics Society Nottingham University Hospitals NHS Trust, UK Visiting Professor University of Southern Denmark Mrs GH is a
Falls Assessment and Medication Professor T.Masud President-Elect British Geriatrics Society Nottingham University Hospitals NHS Trust, UK Visiting Professor University of Southern Denmark Mrs GH is a
Taking the harm out of Polypharmacy Step by step. Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian
 Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Taking the harm out of Polypharmacy Step by step Karen Reid and Claire Stein Lead Integrated Care Pharmacist NHS Lothian Presentation: Polypharmacy Overview of the 2015 guidelines The Seven Steps Application
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Cover images courtesy of jk1991 at FreeDigitalPhotos.net Infographics courtesy of SIMPATHY consortium
 If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format: Scottish Government
If using any content from this document, please acknowledge the Scottish Government Polypharmacy Model of Care Group, 2018. When referencing this document, please use the following format: Scottish Government
Wednesday September 20 th CMT Regional Study Day. Dr Colin Mason, Consultant DME, Addenbrooke s Hospital
 Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Polypharmacy: Guidance for Prescribing in Frail Adults
 Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Rational prescribing in the older adult. Assoc Prof Craig Whitehead
 Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Rational prescribing in the older adult Assoc Prof Craig Whitehead Introduction Physioloical ageing and frailty Medication risks in older adults Drug Burden Anticholinergic and sedative drug burden Cascade
Frailty: what s it all about?
 Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
Frailty: what s it all about? What is frailty? 1. an inevitable consequence of aging 2. A state due to multiple long term conditions 3. A condition in which the person becomes fragile 4. A state associated
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients
 A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients") There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Prescribing in the Elderly. Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry
 Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Prescribing in the Elderly Dr Alison Macrae and Dr Debbie Vest GPST2 Drs in Psychiatry 24 th September 2014 Objectives Understand the significance of polypharmacy in the elderly Become familiar with the
Bulletin Independent prescribing information for NHS Wales
 Bulletin Independent prescribing information for NHS Wales July 2016 Optimising medicines use in care homes There are currently over 22 000 resident places in older adult care homes in Wales. 1 An ageing
Bulletin Independent prescribing information for NHS Wales July 2016 Optimising medicines use in care homes There are currently over 22 000 resident places in older adult care homes in Wales. 1 An ageing
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Intelligent Polypharmacy. Professor Colin P Bradley Department of General Practice University College Cork
 Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016
 Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Maximizing Medication Safety UNIVERSITY OF HAWAII AUGUST 31, 2016 Adverse Drug Events (ADE s) RISK FACTORS FOR Adverse Drug Events (ADEs) 6 or more concurrent chronic conditions 12 or more doses of drugs/day
Tackling inappropriate polypharmacy in NHS Scotland
 Tackling inappropriate polypharmacy in NHS Scotland Francesca Aaen Lead Care Homes Pharmacist - NHS Lanarkshire Heather Harrison - Senior Prescribing Advisor/ Chronic Pain Primary Care Service Development
Tackling inappropriate polypharmacy in NHS Scotland Francesca Aaen Lead Care Homes Pharmacist - NHS Lanarkshire Heather Harrison - Senior Prescribing Advisor/ Chronic Pain Primary Care Service Development
Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody
 Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody The presentation will begin at 12.00pm. Attendees will be muted during the presentation to avoid interference.
Welcome to the Routine frailty identification in the GP contract webinar presented by Dawn Moody The presentation will begin at 12.00pm. Attendees will be muted during the presentation to avoid interference.
Medication Assessment and Quality Parameters. Norma J. Owens, PharmD, FCCP Professor of Pharmacy University of Rhode Island
 Medication Assessment and Quality Parameters Norma J. Owens, PharmD, FCCP Professor of Pharmacy University of Rhode Island Financial Disclosure None of the planners, speakers, and/or members of the CME
Medication Assessment and Quality Parameters Norma J. Owens, PharmD, FCCP Professor of Pharmacy University of Rhode Island Financial Disclosure None of the planners, speakers, and/or members of the CME
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
Optimising Safe & Appropriate Medicines Use and Deprescribing. Katie Smith, Director, East Anglia Medicines Information Service February 2014
 Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
Optimising Safe & Appropriate Medicines Use and Deprescribing Katie Smith, Director, East Anglia Medicines Information Service February 2014 Background Objectives How & why the OSAMU document was developed
< = > less is more. De-diagnosing De-prescribing Non-testing
 < = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
< = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
Falls most commonly seen in RACFs are due to tripping, slipping and stumbling (21.6%). Falling down stairs is relatively uncommon in
. Falling down stairs is relatively uncommon in") This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Reviewing Medicines in at risk patients care homes
 Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Medicines optimisation for older people with disabilities
 Medicines optimisation for older people with disabilities Riddhika Joshi Care of older people and stroke pharmacist Objectives Medicines Optimisation Examples Identifying patients PREVENT Targeting patients
Medicines optimisation for older people with disabilities Riddhika Joshi Care of older people and stroke pharmacist Objectives Medicines Optimisation Examples Identifying patients PREVENT Targeting patients
Interdisciplinary detection of potential drug related problems in older people
 Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
The older person with co morbidities. Eugene Hughes General Practitioner Isle of Wight
 The older person with co morbidities Eugene Hughes General Practitioner Isle of Wight Eugene Hughes Age 60 BMI 26.5 BP 125/70 Alcohol intake moderate (?) TC 5.6 Regular exercise Non smoker Stress free
The older person with co morbidities Eugene Hughes General Practitioner Isle of Wight Eugene Hughes Age 60 BMI 26.5 BP 125/70 Alcohol intake moderate (?) TC 5.6 Regular exercise Non smoker Stress free
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
HA CONVENTION Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward
 Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
Effectiveness of Pharmacist-led Frail Elderly Medication Service in Acute Geriatric Ward HA CONVENTION 2017 Candis Chang Pharmacist Department of Pharmacy Ruttonjee and Tang Shiu Kin Hospitals Background
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
23/11/2018. Tools to stratify patients for clinical pharmacy interventions
 Tools to stratify patients for clinical pharmacy interventions Professor Mike Scott Director of the Regional Medicines Optimisation Innovation Centre (MOIC) 47 th ESCP Symposium, Belfast 24 th October
Tools to stratify patients for clinical pharmacy interventions Professor Mike Scott Director of the Regional Medicines Optimisation Innovation Centre (MOIC) 47 th ESCP Symposium, Belfast 24 th October
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS
 CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
CHAPTER 2. GERIATRICS, SELF-ASSESSMENT QUESTIONS 1. The following is an accurate description of the aging population: A. The number of older adults will reach 17 million in 2030 B. The ratio of women to
National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL or FAX
 National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL 01-4730589 or 1850-727-727 FAX 01-4730596 www.nmic.ie PRESCRIBING IN THE ELDERLY INTRODUCTION According to the most recent census
National Medicines Information Centre ST. JAMES S HOSPITAL DUBLIN 8 TEL 01-4730589 or 1850-727-727 FAX 01-4730596 www.nmic.ie PRESCRIBING IN THE ELDERLY INTRODUCTION According to the most recent census
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Disclosures. Use caution in the elderly: review of safe and effective medication use in older patients. Institute of Medicine. Learning Objectives
 Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Use caution in the elderly: review of safe and effective medication use in older patients Disclosures I have no disclosures or conflicts of interest related to this presentation John T. Holmes, PharmD,
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Medicines Optimisation the opportunities and challenges. Christina Short Medicines Optimisation Project Manager
 Medicines Optimisation the opportunities and challenges Christina Short Medicines Optimisation Project Manager The remit:- Clinical Pharmacy input into the Locality Model Proposal: To contract a senior
Medicines Optimisation the opportunities and challenges Christina Short Medicines Optimisation Project Manager The remit:- Clinical Pharmacy input into the Locality Model Proposal: To contract a senior
Prescribing appropriately. May 2016
 Prescribing appropriately May 2016 Prescribing process Prescribing process Patient problem Core knowledge Decision to prescribe Medicines Choice Modification Habit Formulation Dose Frequency Preferred
Prescribing appropriately May 2016 Prescribing process Prescribing process Patient problem Core knowledge Decision to prescribe Medicines Choice Modification Habit Formulation Dose Frequency Preferred
Geri-PARDY! (2015 Beers Criteria) Pharmacology Edition
 Pharmacology Edition") Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Geri-PARDY! Pharmacology Edition (2015 Beers Criteria) Aurelio Muyot, MD, AGSF, FACP Assistant Professor College of Osteopathic Medicine Touro University Nevada Objectives Review the 2015 Beers Criteria
Rational Pharmacotherapy for LUTS in Older People. Dr William Gibson MBChB MRCP
 Rational Pharmacotherapy for LUTS in Older People Dr William Gibson MBChB MRCP Frailty Frailty = state of increased vulnerability resulting from agingassociated decline in reserve and function NOT synonymous
Rational Pharmacotherapy for LUTS in Older People Dr William Gibson MBChB MRCP Frailty Frailty = state of increased vulnerability resulting from agingassociated decline in reserve and function NOT synonymous
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Medication Use in Older Adults
 Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Medication Use in Older Adults F. Michael Gloth, III, MD, AGSF, FACP, CMD Clinical Professor Department of Geriatrics, Florida State University College of Medicine Associate Professor of Medicine Division
Prevention of Medication-Related Falls Through Appropriate Medication Use. Clay Sprouse, MEd., CPhT Piedmont Technical College
 Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
Prevention of Medication-Related Falls Through Appropriate Medication Use Clay Sprouse, MEd., CPhT Piedmont Technical College Disclosure I have no relevant financial or nonfinancial relationships to disclose
DEPRESCRIBING. Phil St John CSIM Workshop
 DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
DEPRESCRIBING Phil St John CSIM Workshop Conflict of Interest Disclosure Consultant for: none Speaker for: none Received grant/research support from: CIHR, MHRC, Riverview Foundation Received honoraria
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Safe Prescribing in Dementia
 Safe Prescribing in Dementia Dr Daniel Harwood Consultant Psychiatrist and Clinical Director, London Strategic Clinical Network Gurdeep Kaur Major Rapid Access Team Senior Pharmacist, Camden CNWL NHS Trust
Safe Prescribing in Dementia Dr Daniel Harwood Consultant Psychiatrist and Clinical Director, London Strategic Clinical Network Gurdeep Kaur Major Rapid Access Team Senior Pharmacist, Camden CNWL NHS Trust
A Primer on Safe Prescribing to the Elderly. Dr. John Puxty
 A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
A Primer on Safe Prescribing to the Elderly Dr. John Puxty Learning Objectives Describe an approach to safe prescribing for older patients. Appreciate the significance and causes of Polypharmacy. Identify
Managing falls in the elderly: real world approach DR PRISCILLA NG
 Managing falls in the elderly: real world approach DR PRISCILLA NG A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level. FALL:
Managing falls in the elderly: real world approach DR PRISCILLA NG A fall is defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level. FALL:
Pitfalls in Pharmacotherapy of Geriatrics
 Pitfalls in Pharmacotherapy of Geriatrics DR Ali M. Alyami (M Pharm., PhD) Case Study An 85 year old female with a history of atrial fibrillation, stroke, dementia, and hypertension, who is receiving chronic
Pitfalls in Pharmacotherapy of Geriatrics DR Ali M. Alyami (M Pharm., PhD) Case Study An 85 year old female with a history of atrial fibrillation, stroke, dementia, and hypertension, who is receiving chronic
Falls Injury Prevention in Residential Care
 in Residential Care Guide to Best Practice Prepared by Mandy Harden and John Ward, HNE Health, Nov, 2010. Epidemiology About one-third of all hip fractures occur in aged care facilities Many people with
in Residential Care Guide to Best Practice Prepared by Mandy Harden and John Ward, HNE Health, Nov, 2010. Epidemiology About one-third of all hip fractures occur in aged care facilities Many people with
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS
 ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
Briefing Document on Medication use and Falls
 Briefing Document on Medication use and Falls This document is intended as a briefing document and is not to be regarded as a document offering definitive legal advice in relation to the subject matter.
Briefing Document on Medication use and Falls This document is intended as a briefing document and is not to be regarded as a document offering definitive legal advice in relation to the subject matter.
POLYPHARMACY. A practical approach to deprescribing in care homes. Care Home Pharmacy Team. Herts Valleys Clinical Commissioning Group
 POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
POLYPHARMACY A practical approach to deprescribing in care homes. Care Home Pharmacy Team Herts Valleys Clinical Commissioning Group Neeta Gulhane Specialist Pharmaceutical Advisor Care Homes The Care
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Deprescribing: A Practical Guide
 Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Deprescribing: A Practical Guide The information in this booklet should be used as a pragmatic decision aid, in conjunction with other relevant patient specific data. Useful resource links http://www.derbyshiremedicinesmanagement.nhs.uk/assets/clinical_guidelines/clinical_guidelines_fr
Managing Polypharmacy: Thinking outside the box
 Managing Polypharmacy: Thinking outside the box Martin Wilson Consultant Physician Care of the Elderly NHS Highland Clare Morrison Lead Pharmacist (North) Senior Quality Clinical Lead NHS Highland Disclosure
Managing Polypharmacy: Thinking outside the box Martin Wilson Consultant Physician Care of the Elderly NHS Highland Clare Morrison Lead Pharmacist (North) Senior Quality Clinical Lead NHS Highland Disclosure
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
Module 3.2. Management of hypertension at primary health care
 Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Back to Basics: The Basics of Medication Monitoring
 DIAMOND PHARMACY SERVICES Back to Basics: The Basics of Medication Monitoring Presented by: Dr. Deborah Milito, Pharm. D., CGP. Director of Clinical and Consultant Services Skilled Division Annual Educational
DIAMOND PHARMACY SERVICES Back to Basics: The Basics of Medication Monitoring Presented by: Dr. Deborah Milito, Pharm. D., CGP. Director of Clinical and Consultant Services Skilled Division Annual Educational
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies. Falls can be classified into four main groups:
 What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
The role of medication in falls risk
 The role of medication in falls risk Patrick A. Ball, Foundation Professor of Rural Pharmacy, Charles Sturt University, Wagga Wagga Lecture outline The aged are not created equal Insidious nature of onset
The role of medication in falls risk Patrick A. Ball, Foundation Professor of Rural Pharmacy, Charles Sturt University, Wagga Wagga Lecture outline The aged are not created equal Insidious nature of onset
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH. Barry Goldlist October 31, 2014
 HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
HYPERTENSION IN THE ELDERLY A BALANCED APPROACH Barry Goldlist October 31, 2014 DISCLOSURE I have not accepted any money for myself from any pharmaceutical company in the 21 st century I have accepted
Polypharmacy. in the Elderly. Lesley Charles, MBChB, CCFP
 Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
Polypharmacy in the Elderly Lesley Charles, MBChB, CCFP Associate Professor and Program Director Division of Care of the Elderly Department of Family Medicine, University of Alberta March 06, 2016 1 Faculty/Presenter
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
POLICY DOCUMENT. Pharmacy MMG/MPG. Approved By and Date Medicines Management roup March March 2016
 POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Prescribing Drugs to the Elderly
 Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Answers to your questions from University of Toronto experts Prescribing Drugs to the Elderly Can drugs do more harm than good? M.A. is a 90-year-old man living at home. He has dementia and due to wandering
Living well with frailty. JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England
 Living well with frailty JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England A LTC rarely travels alone Kent Whole Population Dataset: Interim Report 2014 The burden
Living well with frailty JOHN YOUNG National Clinical Director for the Frail Elderly & Integration, NHS England A LTC rarely travels alone Kent Whole Population Dataset: Interim Report 2014 The burden
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
High blood pressure (Hypertension)
") High blood pressure (Hypertension) Information for patients from the Department of Renal (Kidney) Medicine This leaflet is not meant to replace the information discussed between you and your doctor, but
High blood pressure (Hypertension) Information for patients from the Department of Renal (Kidney) Medicine This leaflet is not meant to replace the information discussed between you and your doctor, but
A Step Forward: Promoting Independence through Falls Prevention
 A Step Forward: Promoting Independence through Falls Prevention 2014 Geriatric Update Meharry Consortium Geriatric Education Center A Step Forward: Promoting Independence through Falls Prevention Moderator:
A Step Forward: Promoting Independence through Falls Prevention 2014 Geriatric Update Meharry Consortium Geriatric Education Center A Step Forward: Promoting Independence through Falls Prevention Moderator: