3/6/2019 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING FINANCIAL DISCLOSURES LEARNING OBJECTIVES
|
|
|
- Melina Bishop
- 5 years ago
- Views:
Transcription


1 DIAGNOSIS OF DEMENTIA IN THE OUTPATIENT SETTING MILTA LITTLE, DO, CMD DUKE UNIVERSITY SCHOOL OF MEDICINE FINANCIAL DISCLOSURES Dr. Little has no relevant financial disclosures to report Dr. Little will not be discussing any off label or unapproved medications LEARNING OBJECTIVES By the end of the session, participants will be able to Define and distinguish dementia and mild cognitive impairment Describe the impact dementia has on the patient and caregiver Identify the most common types of dementing illnesses Successfully perform brief cognitive screens that can be used in daily clinical practice 1




2 BACKGROUND 1 in 3 elderly individuals develop some form of dementia 5.7 million Americans are currently living with Alzheimer s and this number is expected to rise to 14 million by the year 2050 Between 2000 and 2015, deaths from heart dz declined by 11% but deaths due to dementia have increased by 123%!! Dementia is the only cause of death in the top 10 causes of death in America that cannot be prevented, cured, or slowed Nearly ½ of patients with dementia suffer from depression Nearly ½ of caregivers also suffer from depression This year (2018), dementia has lead to an expenditure of $277 billion in healthcare and caregiving costs ALZHEIMER S ASSOCIATION 2018 ALZHEIMER S DISEASE FACTS AND FIGURES REPORT BACKGROUND: DEFINITION OF DEMENTIA Memory impairment plus a decline in one or more cognitive domains learning ability, social function, visuo-spatial function, language, complex attention, executive functioning Significant decline from previous abilities +Impairment in daily functioning Decline is progressive, disabling Caused by damage to the brain ARE THERE NORMAL CHANGES IN MEMORY WITH AGE? Yes!! Slower recall of information, such as names Increased effort needed to learn new tasks Greater difficulty multi-tasking Easier distractibility Slower processing But, dementia is NOT NORMAL in the older adult 2
 Memory impairment significant enough to be noticeable to family and/or")

 3 STAGES IN THE DEVELOPMENT AND PROGRESSION")
3 BACKGROUND NOT ALL DEMENTIA IS ALZHEIMER S DISEASE MILD COGNITIVE IMPAIRMENT (MCI) Memory impairment significant enough to be noticeable to family and/or individual, but not significant enough to interfere with daily activities Occurs in 10-20% of adults >65 Established risk factor for the development of Alzheimer s Disease 30% of those w/ MCI progress to Alzheimer s each year (70% of people with MCI don t progress) 3 STAGES IN THE DEVELOPMENT AND PROGRESSION OF DEMENTIA 3


4 WHAT ARE THE IMPLICATIONS FOR HEALTH CARE PROVIDERS? Dementia dx changes in our approach with the patient: Do caregivers need to be present during office visits or called to be updated after visits? Should written and verbal instructions be provided? Is there a pattern to repeat hospitalizations, ER visits, etc, that may need to be addressed is the pt receiving enough oversight at home? Are there signs of caregiver burnout that we can assist with? What is the overall life expectancy and how does seeing the big picture change our management? NOW ON TO MAKING THE DIAGNOSIS DIAGNOSIS Goals: Rule out reversible causes! Distinguish between the various types of dementing illnesses Build a comprehensive treatment plan (bio-psycho-social care) tailored to the individual 4
 **At the present time, there is no single diagnostic test for detecting mild cognitive impairment, Alzheimer s")
 2. Saint Louis University Mental Status Examination (SLUMS) 3. Montreal Cognitive Assessment (MoCA) 4. Mini-Cog Test 5.")
5 DIAGNOSIS Complete medical history Physical and neurological examinations Memory Test Saint Louis University Mental Status Examination (SLUMs) or Rapid Cognitive Screen (RCS) Neuroimaging Laboratory tests Neuropsychological assessment (optional) **At the present time, there is no single diagnostic test for detecting mild cognitive impairment, Alzheimer s Disease or other types of dementia REVERSIBLE CAUSES OF MCI/DEMENTIA DETECTING MCI Which of the following dementia screening tools can also be used to screen for MCI? 1. Mini Mental Status Examination (MMSE) 2. Saint Louis University Mental Status Examination (SLUMS) 3. Montreal Cognitive Assessment (MoCA) 4. Mini-Cog Test 5. Rapid Cognitive Screen (RCS) 6. All of the Above 5
 67% 93% 64% 94% What are we measuring in each SLUMS item? Q1-Q3: Attention, Immediate Recall, and Orientation. Q4 & Q7: Delayed Recall with Interference.")

6 MOCA AND TRAILS A/B SLUMS SLUMS: SAINT LOUIS UNIVERSITY MENTAL STATUS EXAM Sensitivity to detect MCI according to area under the curve (AUC) analysis * Education Less than HS More than HS Instrument MMSE SLUMS MMSE SLUMS AUC (Sensitivity) 67% 93% 64% 94% What are we measuring in each SLUMS item? Q1-Q3: Attention, Immediate Recall, and Orientation. Q4 & Q7: Delayed Recall with Interference. Q5: Numeric Calculation and Registration. Q6: Immediate Recall with Interference (time constraint). Q8: Registration and Digit Span. Q9: Visual Spatial and Executive Function. Q10: Visual Spatial. Q11: Executive Function plus Extrapolation. *Tariq SH, Tumosa N, Chibnall JT, Perry MH, Morley J. Comparison of the Saint Louis University mental Status Examination and themini-mental State Examination for Detecting Dementia and Mild Neurocognitive Disorder- A Pilot Study. Am J Geriatr Psychiatry. 2006; 14(11):

7 SLUMS: SAINT LOUIS UNIVERSITY MENTAL STATUS EXAM CRUZ, JAMDA 2010 Cognitive Impairment Screening Instruments ability in detecting Dementia Authors Instrument Sensitivity, % Specificity % Comparison to Class of MMSE evidence * Tangalos et al. MMSE II Kokmen et al. STMS Y III Solomon et al. 7-Minute Screen Y III Buschke et al. MIS Y I Borson et al. Mini-Cog Y III Cahn et al. CDT I Nasreddine et al. MoCA Y I Tariq et al. SLUMS** 100/98 98/100 Y II **This study has different values according to education, first set of numbers represent the sensitivity and specificity for less than high school and the second set represent high school or higher education. This table was adapted from the American Academy of Neurology. Classification of evidence, see next slide. MINI-COG 1. Instruct the patient to listen carefully and repeat: APPLE WATCH PENNY 2. Administer the Clock Drawing Test 3. Ask the patient to repeat the three words Score: 0 Positive for cognitive impairment 1-2 Abnormal CDT then positive for cognitive impairment 1-2 Normal CDT then negative for cognitive impairment 3 Negative screen for dementia (no need to score CDT) Benefit: QUICK! Drawback: Low sensitivity RAPID COGNITIVE SCREEN 7
8 RAPID COGNITIVE SCREEN VS MINICOG DEMENTIA MCI AUC (95% CI) RCS 0.98 ( ) Mini-Cog 0.92 ( ) Dementia MCI Malmstrom TK1, et al. J Nutr Health Aging Aug;19(7): TIME TO DRAW A CLOCK! Clock drawings by patients with AD. van der Flier W M, ScheltensP J Neurol Neurosurg Psychiatry 2005;76:v45-v by BMJ Publishing Group Ltd 8

9 CLOCK DRAWINGS BY PATIENTS WITH UNILATERAL NEGLECT 3 REASONS TO DO A RAPID COGNITIVE SCREEN (RCS) It s fast It s free no copyright It detects mild cognitive impairment (MCI) WHY IS AN EARLY DIAGNOSIS IMPERATIVE? Early diagnosis of dementia is important because: It can identify any potentially reversible or treatable causes and these can be corrected before permanent damage to brain is done It can facilitate planning for patients and families Includes naming POA, getting finances in order, discussion of medical preferences Can address critical safety issues such as driving and living alone before a crisis occurs It can explain why the patient acts and thinks different and allow families to place blame on the disease process and not the patient themselves 9
 Vascular dementia Lewy body dementia Other Parkinsonian dementias Dementia of Diabetes Alzheimer s")
10 MAIN TYPES OF DEMENTIA ALZHEIMER S DISEASE, VASCULAR DISEASE, LEWY BODY DEMENTIA, PARKINSON S DISEASE WITH DEMENTIA, FRONTOTEMPORAL DEMENTIA, HIPPOCAMPAL SCLEROSIS OF AGING, PRIMARY TAUOPATHY COMMON DEMENTIAS IN OLDER PERSONS Hippocampal sclerosis of aging Primary age-related tauopathy(part) Vascular dementia Lewy body dementia Other Parkinsonian dementias Dementia of Diabetes Alzheimer s disease Nelson PT1, et al. Brain May;134(Pt 5): ALZHEIMER S DISEASE What causes Alzheimer s Disease? Not fully understood yet Develops as a result of complex series of events that take place in the brain over many years Genetic, environmental and lifestyle factors contribute Caused by: Accumulation of plaques and tangles Neurotransmitter deficits Inflammation Early-onset form is rare (1-2%) and occurs before the age of 60 Late-onset form develops after the age of 60 10










11 ALZHEIMER S DISEASE History: Named in 1901 by German psychiatrist Alois Alzheimer Pathophysiology: Caused by plaques and tangles Plaques occur outside of nerve cells and are made of an abnormal protein fragment called amyloid beta Neurofibrillary tangles occur inside nerve cells and are made of tau protein This abnormal protein accumulation also leads to increased inflammation and cellular death, causing more damage ALZHEIMER S DISEASE 11



12 ALZHEIMER S DISEASE ALZHEIMER S DISEASE ALZHEIMER S DISEASE: STAGES Gradual onset with progressive decline Motor symptoms are rare early in disease course but develop later on 12





13 ALZHEIMER S DISEASE: STAGING VASCULAR DEMENTIA Caused by poor blood flow strokes, diabetes, high blood pressure, high cholesterol, atrial fibrillation Sudden onset and stepwise progression Abrupt changes in cognitive ability Future damage can be prevented or slowed by aggressive control of chronic medical conditions VASCULAR DEMENTIA Symptoms tend to correlate with where in the brain the stroke or blood vessel narrowing occurs Head imaging reveals ischemic small vessel disease or previous infarcts 13



14 VASCULAR DEMENTIA Multi-infarct dementia vascular dementia LEWY BODY DEMENTIA Caused by abnormal protein deposits Lewy Bodies On the same spectrum as Parkinson s Disease More common in men Symptoms: visual hallucinations, fluctuating attention, motor dysfunction, abnormal movements during sleep Widely under-diagnosed Symptoms are dependent on where in the brain the Lewy Bodies deposit 14







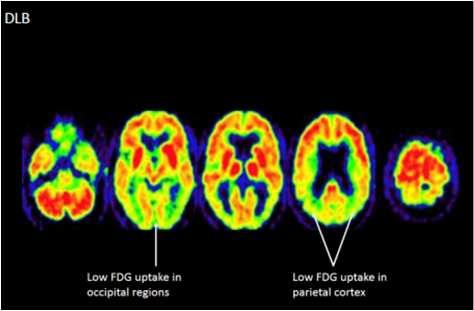
15 LEWY BODY DEMENTIA GORE R, VARDY E, O BRIEN J. DELIRIUM AND DEMENTIA WITH LEWY BODIES: DISTINCT DIAGNOSES OR PART OF THE SAME SPECTRUM? J NEUROLNEUROSURG PSYCHIATRY 2015;86:50-9. LEWY BODY DEMENTIA 15


16 PARKINSON S DISEASE WITH DEMENTIA Parkinson s Disease is a chronic, progressive neurological condition Symptoms: tremors, muscle stiffness, masked faces, and slow, shuffling gait Most people with Parkinson s will eventually develop dementia Memory loss is accompanied by depression, anxiety, and hallucinations Often have marked impairment in visual-spatial functioning, causing earlier concern with driving PARKINSON S DISEASE WITH DEMENTIA Parkinson s disease with dementia is very similar to Lewy Body Dementia and the two can be hard to tell apart at later stages Timing differentiates: Lewy Body memory impairment precedes or accompanies motor symptoms Parkinson s disease with dementia Motor symptoms precede memory impairment by >1 year, but usually by many years FRONTOTEMPORAL DEMENTIA (FTD) AKA Pick s Disease Results from progressive degeneration of frontal and temporal lobes Affects personality, causing a decline in social skills and inability to understand/read another s emotions Can affect language and motor skills Behavior and personality changes manifest long before memory loss Occurs at a younger age and is more common than Alzheimer s in people <60 16

 Medications only work in a small")
 Rivastigmine(Exelon) Galantamine(Razadyne)")
17 NOW A QUICK WORD ON TREATMENT TREATMENT Goal of treatment is to enhance quality of life and maximize functional performance by improving cognition, mood, and behavior TREATMENT There are no proven cures or disease-slowing treatments Goal is to maximize cognitive abilitiesfor as long as possible (improve symptoms) Medications only work in a small subset of patients and on average improve memory test scores by 1-2 points There are 4 FDA approved medications: Donepezil (Aricept) Rivastigmine(Exelon) Galantamine(Razadyne) Memantine(Namenda) 17



18 TREATMENT SOAPBOX Disclaimer: I am biased against anti-dementia medications in most cases If they worked, there would be no dementia Medications are aimed at only one pathway causing dementia, but we know it is more complicated than one pathway The public is mislead into thinking that these are must-have cures and are effective for all TREATMENT 257 studies included in review Cholinesterase inhibitors (ChEIs) produce small improvements in cognitive function in pts w/ mild to moderate Alzheimer s and Lewy Body dementia, but clinical significance is unclear No improvement w/ vascular dementia Efficacy wanes over time w/ minimal benefit after 1yr of tx No evidence for benefit in advanced dz or in those >85 y/o Adverse effects are significant and occur in a dose-dependent manner 2-5x increase in side effects, particularly weight loss, syncope, and debility Those >85 have 2x the risk of side effects seen in younger pts TREATMENT Memantine (Namenda) is FDA approved for treating moderate to severe dementia It is often used in combination with donepezil because the studies for monotherapy are not impressive Even though it is not as beneficial for cognition, there are several positive studies that show improvements in behavior 18

 Organized group therapy program for those w/ mild to moderate dementia Uses a structured")
19 SO IF MEDICATIONS DON T REALLY WORK, WHAT TREATMENTS CAN WE OFFER? EXERCISE AND DEMENTIA Exercise has been shown to improve quality of life for all stages of Dementia and Alzheimer s It likely works better than our best medications in improving symptoms and behavioral issues Can reduce risk of stroke and improve high blood pressure, diabetes, and cholesterol, all of which are risk factors for vascular dementia Improved physical fitness can allow for longer independence Reduces risk of falls Improves mood Improves sleep COGNITIVE STIMULATION THERAPY (CST) Organized group therapy program for those w/ mild to moderate dementia Uses a structured approach to focus on: Reminiscence Orientation Mental stimulation Not only enhances cognitive function, but has been shown to improve quality of life for both patient and caregiver Typically structured as a 14 session course which meets 2x/weekly Can take place in nursing home, adult day centers, assisted living, or home 19



20 SAFE RETURN IDENTIFICATION GUNS AND DEMENTIA DON T MIX 20




21 COMPLICATING FACTORS Infections: UTI Pneumonia Change in environment Hospitalizations Move to higher level of care Change in routine CAREGIVER SUPPORT Assess for caregiver burden/burnout What resources may be available? Alzheimer s Association Private duty nursing Respite care Explore feelings regarding when placement outside of the home may be needed ADVANCE DIRECTIVES Advance Directive: Legal document containing preferences for health care decisions should one become unable to make decisions/incapacitated due to illness (dementia) or injury Living will: One form of advance directive that discusses specific preferences such as feeding tube placement, ventilator usage, CPR preferences, etc Durable power of attorney (DPOA): Individual named to make decisions should one become incapacitated 21

22 THANKS! 22
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Latest Methods to Early Detection for Alzheimer's: Cognitive Assessments and Diagnostic Tools in Practice
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/alzheimers-disease-towards-earlier-detection/latest-methods-earlydetection-alzheimers-cognitive-assessments-and-diagnostic-tools-practice/8321/
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Overview. Case #1 4/20/2012. Neuropsychological assessment of older adults: what, when and why?
 Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Neuropsychological assessment of older adults: what, when and why? Benjamin Mast, Ph.D. Associate Professor & Vice Chair, Psychological & Brain Sciences Associate Clinical Professor, Family & Geriatric
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Understanding Dementia
 Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Understanding Dementia Dr. Dallas Seitz MD FRCPC Assistant Professor, Department of Psychiatry, Queen s University, Kingston, Ontario, Canada What s Next Information about Dementia, Elder Care and Supports
Significance A Busy Clinician's Guide to Seniors with Memory Loss
 Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
Significance A Busy Clinician's Guide to Seniors with Memory Loss Victoria Braund MD FACP CMD Division of Geriatrics. NorthShore University HealthSystem Alzheimer's disease is the sixth leading cause of
New life Collage of nursing Karachi
 New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Cognitive Screening in Risk Assessment. Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University.
 Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
Cognitive Screening in Risk Assessment Geoffrey Tremont, Ph.D. Rhode Island Hospital & Alpert Medical School of Brown University Outline of Talk Definition of Dementia and MCI Incidence and Prevalence
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Sorting Out the Three D s:
 Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
Sorting Out the Three D s: Delirium, Depression & Dementia Teepa Snow, Positive Approach, LLC to be reused only with permission. Dementia Delirium Depression What s What? What s What For Each D Onset Hx
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Identification of Cognitive Impairment in HIV patients. Belinda Vicioso MD FACP, AGSF Jose Garcia Professor of Medicine UTSW
 Identification of Cognitive Impairment in HIV patients Belinda Vicioso MD FACP, AGSF Jose Garcia Professor of Medicine UTSW New emphasis on cognition Why? Common in our patient population Often overlooked
Identification of Cognitive Impairment in HIV patients Belinda Vicioso MD FACP, AGSF Jose Garcia Professor of Medicine UTSW New emphasis on cognition Why? Common in our patient population Often overlooked
Dementia and cognitive decline
 Dementia and cognitive decline Expert Briefing Su Ray and Dr Susan Davidson Research Department Together, we can help everyone to love later life 01 Brain basics Normal ageing, cognitive impairment and
Dementia and cognitive decline Expert Briefing Su Ray and Dr Susan Davidson Research Department Together, we can help everyone to love later life 01 Brain basics Normal ageing, cognitive impairment and
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
Dementia Awareness Handout
 Dementia Awareness Handout This handout is designed to be used as a brief aid to remind you of the contents of your dementia awareness session. Definition of dementia The term dementia is used to describe
Dementia Awareness Handout This handout is designed to be used as a brief aid to remind you of the contents of your dementia awareness session. Definition of dementia The term dementia is used to describe
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Imaging of Alzheimer s Disease: State of the Art
 July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
July 2015 Imaging of Alzheimer s Disease: State of the Art Neir Eshel, Harvard Medical School Year IV Outline Our patient Definition of dementia Alzheimer s disease Epidemiology Diagnosis Stages of progression
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. There are over 200 subtypes of dementia, but the five most
Memory Loss, Dementia and Alzheimer's Disease: The Basics
 Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Memory Loss, Dementia and Alzheimer's Disease: The Basics What is memory loss? What is age-related memory loss? Typical changes Typical age-related changes involve: Making a bad decision once in a while
Cognitive Assessment 4/29/2015. Learning Objectives To be able to:
 Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Clinical Provider Practice Tool
 Clinical Provider Practice Tool Cognitive Impairment Identification Annual Exam Mini Screen Tools Mini-Cog or GPCOG AND Family Questionniare (if family available) Normal Follow up in 1 year IF Mini-Cog
Clinical Provider Practice Tool Cognitive Impairment Identification Annual Exam Mini Screen Tools Mini-Cog or GPCOG AND Family Questionniare (if family available) Normal Follow up in 1 year IF Mini-Cog
Dementia UK & Admiral Nurses
 Dementia UK & Admiral Nurses Susan Drayton Admiral Nurse www.dementiauk.org 356 Holloway road. London N7 6PA 020 7697 4174 info@dementiauk.org @DementiaUK www.dementiauk.org 356 Holloway Road. London N7
Dementia UK & Admiral Nurses Susan Drayton Admiral Nurse www.dementiauk.org 356 Holloway road. London N7 6PA 020 7697 4174 info@dementiauk.org @DementiaUK www.dementiauk.org 356 Holloway Road. London N7
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
What is dementia? What is dementia?
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. It has been identified that there are over 200 subtypes of
EARLY DEMENTIA. University of Hawaii Geriatric Medicine Department
 EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
EARLY DEMENTIA University of Hawaii Geriatric Medicine Department INTRODUCTION Dementia is very prevalent Screening and early diagnosis is important Evaluation Dementia Management DEMENTIA IS VERY PREVALENT
Alzheimer s Disease. Fact Sheet. Fact Sheet. Fact Sheet. What Causes AD?
 2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
2 Alzheimer s Disease Dementia is a brain disorder that seriously affects a person s ability to carry out daily activities. The most common form of dementia among older people is Alzheimer s disease (AD),
10 Facts We All Need to Know About Dementia (MNCD) in Old Age
 in Old Age") 10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
10 Facts We All Need to Know About Dementia (MNCD) in Old Age DUNCAN ROBERTSON FRCP (LOND & EDIN) FRCPC MEDICAL ADVISOR TO ADVANCING DEMENTIA DIAGNOSIS AND MANAGEMENT IN ALBERTA AND PRIMARY HEALTH CARE
What About Dementia? Module 8, Part B (With Dr Allison Lamont)
") What About Dementia? Module 8, Part B (With Dr Allison Lamont) Slide 1 Module 8 Part B will address the question What about dementia? Several surveys of older people both in the UK and USA have shown that
What About Dementia? Module 8, Part B (With Dr Allison Lamont) Slide 1 Module 8 Part B will address the question What about dementia? Several surveys of older people both in the UK and USA have shown that
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia. Memory Evaluation Center Neurology
 Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Dementia Memory Evaluation Center Neurology Topics Overview of dementia Stages Medications Advanced planning What is Dementia? Dementia = significant global decline in cognitive function not due to medicine
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia
 Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Mild cognitive impairment A view on grey areas of a grey area diagnosis
 Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
Mild cognitive impairment A view on grey areas of a grey area diagnosis Dr Sergi Costafreda Senior Lecturer Division of Psychiatry, UCL Islington Memory Service, C&I NHS FT s.costafreda@ucl.ac.uk London
Drug Update. Treatments for Cognitive Impairment in the Older Adult. William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle
 Drug Update Treatments for Cognitive Impairment in the Older Adult William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle Current Drug Treatments for Alzheimer s Disease Cholinesterase Inhibitors:
Drug Update Treatments for Cognitive Impairment in the Older Adult William Solan, M.D. Karen Sanders, Ph.D. Northwest Hospital Seattle Current Drug Treatments for Alzheimer s Disease Cholinesterase Inhibitors:
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Memory Matters: Learning Objectives: Synapses, Age, and Health. Neuronal Synapses DISCLOSURE DECLARATION. Cognition and Normal Aging
 Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
Standard Deviations from Mean Memory Matters: Preventing and Treating Late-Life, Cognitive Decline Daniel L. Murman, MD, MS Director, Behavioral and Geriatric Neurology Program Professor & Vice Chair,
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Case Presentation. Cognition: changes with Normal Aging? Synonyms
 Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Evaluation and Treatment of Dementia
 Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Evaluation and Treatment of Dementia Jeffrey M. Burns, MD Edward H. Hashinger Professor of Neurology Co-Director, KU Alzheimer s Disease Center Director, Clinical and Translational Science Unit Disclosures
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Decline in Mental Capacity
 Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
Decline in Mental Capacity Elder Law: Issues, Answers and Opportunities ALI-ABA, February 23-24, 2006 Robert B. Fleming 1 FLEMING & CURTI, P.L.C. 330 N. Granada Ave. Tucson, Arizona 85701 www.elder-law.com
Dementia is not normal aging!
 The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
The Future of Alzheimer s Disease Treatment Adam L. Boxer, MD, PhD Director, Alzheimer s Disease Clinical Trials Program Memory and Aging Center Assistant Professor of Neurology University of California,
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
UNDERSTANDING CAPACITY & DECISION-MAKING VIDEO TRANSCRIPT
 I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
I m Paul Bourque, President and CEO of the Investment Funds Institute of Canada. IFIC is preparing materials to assist advisors and firms in managing effective and productive relationships with their aging
Capacity and Older Adults. Kenneth I. Shulman
 Capacity and Older Adults Kenneth I. Shulman Increased Requests for Contemporaneous Assessments of Testamentary Capacity Increase in challenges to testamentary capacity Demographics/Economics Prevalence
Capacity and Older Adults Kenneth I. Shulman Increased Requests for Contemporaneous Assessments of Testamentary Capacity Increase in challenges to testamentary capacity Demographics/Economics Prevalence
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Dementia Diagnosis Guidelines Primary Care
 Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Evaluations. Alzheimer s Disease A Public Health Response. Viewer Call-In. July 19, Guest Speakers. Thanks to our Sponsors:
 Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
Alzheimer s Disease A Public Health Response July 19, 2007 1 2 Guest Speakers Thanks to our Sponsors: Earl A. Zimmerman, M.D. Bender Endowed Chair of Neurology and Director of the Alzheimer s Center at
What is dementia? Symptoms of dementia. Memory problems
 What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
What is dementia? What is dementia? What is dementia? Dementia is an umbrella term for a range of progressive conditions that affect the brain. The brain is made up of nerve cells (neurones) that communicate
The current state of healthcare for Normal Aging, Mild Cognitive Impairment, & Alzheimer s Disease
 The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
The current state of healthcare for Normal Aging, g, Mild Cognitive Impairment, & Alzheimer s Disease William Rodman Shankle, MS MD FACP Director, Alzheimer s Program, Hoag Neurosciences Institute Neurologist,
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
Mental Health Disorders Civil Commitment UNC School of Government
 Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask. Presented By: Tuesday, March 22, 2011 at 1:00 PM ET
 PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Alzheimer's Disease Brain Failure, Stopping the Momentum. Katherine E. Galluzzi, DO, CMD, FACOFP dist.
 AOA/ACOFP 113th Annual Convention and Scientific Seminar Las Vegas, Nevada Alzheimer's Disease Brain Failure, Stopping the Momentum Katherine E. Galluzzi, DO, CMD, FACOFP dist. Monday, October 27, 2008
AOA/ACOFP 113th Annual Convention and Scientific Seminar Las Vegas, Nevada Alzheimer's Disease Brain Failure, Stopping the Momentum Katherine E. Galluzzi, DO, CMD, FACOFP dist. Monday, October 27, 2008
East End Neuropsychiatric Associates 2539 Middle Country Rd Suite 4 Centereach, NY (631) What is Vascular Dementia?
 What is Vascular Dementia?") Dementia is diagnosed when both memory and another cognitive function are each affected severely enough to interfere with a person's ability to carry out routine daily activities. The Journal of the American
Dementia is diagnosed when both memory and another cognitive function are each affected severely enough to interfere with a person's ability to carry out routine daily activities. The Journal of the American
Diagnosing & Dealing with Dementia
 Diagnosing & Dealing with Dementia Robert G. Arias, PhD. I have no financial disclosures or conflicts of interest to report. Robert G. Arias, PhD. 1 Today We Will Learn About: Diagnosing dementia Characteristics
Diagnosing & Dealing with Dementia Robert G. Arias, PhD. I have no financial disclosures or conflicts of interest to report. Robert G. Arias, PhD. 1 Today We Will Learn About: Diagnosing dementia Characteristics
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness.
 Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Mental Health Counseling for mood, aging, and coping with life transitions and chronic illness. Silver Linings for Seniors Silver Linings for Seniors, Inc. offers on-site confidential Mental Health Counseling
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Understanding dementia
 Dementia handbook for carers Essex Understanding dementia About this handbook 1 What is dementia 3 Summary of dementia symptoms 6 Medication and treatment 7 About this handbook This handbook aims to summarise
Dementia handbook for carers Essex Understanding dementia About this handbook 1 What is dementia 3 Summary of dementia symptoms 6 Medication and treatment 7 About this handbook This handbook aims to summarise
UNDERSTANDING ALZHEIMER S AND DEMENTIA
 UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
UNDERSTANDING ALZHEIMER S AND DEMENTIA Geri T., living with Alzheimer's, and her husband and care partner, Jim T. THE IMPACT OF ALZHEIMER S AND DEMENTIA Currently, an estimated 50 million people worldwide
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease
 Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
Understanding Symptoms, Causes, and Risks for Alzheimer s Disease Gene E. Alexander, Ph.D., Professor of Psychology, Neuroscience, and Physiological Sciences; Director, Brain Imaging, Behavior & Aging
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
ALZHEIMER S DISEASE OVERVIEW. Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health
 ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
ALZHEIMER S DISEASE OVERVIEW Jeffrey Cummings, MD, ScD Cleveland Clinic Lou Ruvo Center for Brain Health Prevalence AD: DEMOGRAPHY AND CLINICAL FEATURES Risk and protective factors Clinical features and
FACTORS AFFECTING CAPACITY
 FACTORS AFFECTING CAPACITY Psychosocial Factors Affecting Capacity Psychosocial factors include one s surroundings, way of life & things that affect relationships between the adult and their environment.
FACTORS AFFECTING CAPACITY Psychosocial Factors Affecting Capacity Psychosocial factors include one s surroundings, way of life & things that affect relationships between the adult and their environment.
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University
 Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Mild Cognitive Impairment
 Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Mild Cognitive Impairment Victor W. Henderson, MD, MS Departments of Health Research & Policy (Epidemiology) and of Neurology & Neurological Sciences Stanford University Director, Stanford Alzheimer s
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Cognitive Evaluation in Primary Care. Scott T. Larson, MD Clinical Assistant Professor University of Iowa
 Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
Cognitive Evaluation in Primary Care Scott T. Larson, MD Clinical Assistant Professor University of Iowa scott-larson@uiowa.edu Objectives Understand the subtypes of dementia, and the DSM-5 categorization
What is Neuropsychology?
 Alzheimer s Disease Neurological Bases and Informed Behavioral Interventions Peter T. Keenan Clinical Neuropsychologist Marshfield Clinic Minocqua Center What is Neuropsychology? Science of the relationship
Alzheimer s Disease Neurological Bases and Informed Behavioral Interventions Peter T. Keenan Clinical Neuropsychologist Marshfield Clinic Minocqua Center What is Neuropsychology? Science of the relationship
Alzheimer s Disease without Dementia
 Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Alzheimer s Disease without Dementia Dr Emer MacSweeney CEO & Consultant Neuroradiologist Re:Cognition Health London Osteopathic Society 13 September 2016 Early diagnosis of Alzheimer s Disease How and
Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives, friends
 ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
ASSESSING COMPETENCE Michael A Hill MD UNC Psychiatry 2008 Information Gathering Obtaining history is the most critical first step Patient-provided history may not be reliable Need info from relatives,
Falls: Cognitive Motor Perspectives
 Falls: Cognitive Motor Perspectives Joe Verghese, MBBS, MS. Integrated Divisions of Cognitive & Motor Aging (Neurology) & Geriatrics (Medicine) Albert Einstein College of Medicine, Bronx, NY joe.verghese@einstein.yu.edu
Falls: Cognitive Motor Perspectives Joe Verghese, MBBS, MS. Integrated Divisions of Cognitive & Motor Aging (Neurology) & Geriatrics (Medicine) Albert Einstein College of Medicine, Bronx, NY joe.verghese@einstein.yu.edu