Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia
|
|
|
- Hugo Powers
- 5 years ago
- Views:
Transcription
1 Assessment at the bedside or in the clinic using the history, examination and laboratory tests to distinguish between different types of dementia AP Passmore
2 Content Common dementia syndromes (older people) Clinical features Assessments Proposed diagnostic criteria for AD Use of CSF Case histories

3 Few points At bedside delirium? better to delay clinical assessment for dementia ensure assessment by or follow up at memory service Can assess clinically, check bloods and perform neuroimaging Later presentation very difficult (primary diagnosis) Age factor
4 Common causes of dementia Alzheimer s Disease (AD) Vascular dementia AD + CVD Lewy body dementia Parkinson s disease dementia Fronto-temporal lobar degeneration *
5 Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Longitudinal follow up, first 141 autopsies 50 with dementia AD + Infarcts AD VaD 12 AD + PD/DLB Other 30 80% have AD pathology Schneider, Neurology 2007; 61:
6 Clinical criteria exist for all main dementia subtypes All criteria require a diagnosis of dementia and include the caveats that there should not be a symptom pattern more in keeping with another of the dementias and that cognitive impairments should not be better explained by a psychiatric illness. Neuropsychiatric symptoms should be sought Often features such as hallucinations and delusions will not be volunteered unless specific enquiries are made.
7 Diagnostic Criteria for AD Probable AD: A plus one or more supportive features B, C, D, or E Core diagnostic criteria A. Presence of an early and significant episodic memory impairment that includes the following features: 1. Gradual and progressive change in memory function reported by patients or informants over more than 6 months 2. Objective evidence of significantly impaired episodic memory on testing: this generally consists of recall deficit that does not improve significantly or does not normalise with cueing or recognition testing and after effective encoding of information has been previously controlled 3. The episodic memory impairment can be isolated or associated with other cognitive changes at the onset of AD or as AD advances Dubois et al. Lancet Neurol 2007;6:734 46
8 The diagnosis of dementia due to Alzheimer s disease: Recommendations from the NIA - Alzheimer s Association workgroups on diagnostic guidelines for Alzheimer s disease The diagnosis of probable AD dementia should not be applied when there is evidence of substantial concomitant cerebrovascular disease, defined by a history of a stroke temporally related to the onset or worsening of cognitive impairment; or the presence of multiple or extensive infarcts or severe white matter hyperintensity burden McKhann et al. Alzheimer s & Dementia 2011;7:
9 NINDS AIREN Criteria for Vascular Dementia Dementia Cerebrovascular disease: Focal CNS signs Evidence of CVD by brain imaging A relationship between the two manifested by one or more of the following: Dementia onset within 3 months of stroke Abrupt deterioration in cognition or fluctuating stepwise course Neurology 1994;43:250-60
10 Classification and Causes of Sporadic Vascular Cognitive Impairment Post-stroke dementia Vascular dementia multi-infarct dementia (cortical vascular dementia) subcortical ischaemic vascular dementia strategic infarct dementia hypoperfusion dementia haemorrhagic dementia dementia caused by specific arteriopathies Mixed AD and vascular dementia Vascular mild cognitive impairment O Brien et al., Lancet Neurology 2003;2:89-98
11 Hachinski Ischaemic Score Item Score value Correlates of VaD (OR) Abrupt onset 2 Stepwise deterioration Fluctuating course Nocturnal confusion 1 Relative preservation of personality 1 Depression 1 Somatic complaints 1 Emotional incontinence 1 History of hypertension History of strokes Evidence of associated atherosclerosis 1 Focal neurological symptoms Focal neurological signs 2
12
13 Diagnostic Criteria for Dementia with Lewy Bodies Central: Dementia Core clinical features: fluctuating attention, recurrent visual hallucinations, Parkinsonism Suggestive features: REM sleep behaviour disorder, severe neuroleptic sensitivity, low dopamine transporter uptake in the basal ganglia on functional neuroimaging Additional supportive features: repeated falls and syncope, transient unexplained loss of consciousness, severe autonomic dysfunction, hallucinations in other modalities, systematized delusions, depression, relative preservation of medial temporal lobe structures on structural neuroimaging, reduced occipital activity on functional neuroimaging, prominent slow wave activity on electroencephalogram, and low uptake myocardial scintigraphy McKeith et al. Neurology ;65:

14 CVD + AD
15 Can past history help?



16 Overlap between AD and VaD AD Female Genetics VaD Male Genetics Stroke/TIA Hypertension Hypertension Hypercholesterolemia Cholinergic deficits Hypercholesterolemia Age Definite AD AF AF Definite VaD Age Probable AD Possible AD Mixed Possible VaD Probable VaD Homocysteine Diabetes Amyloid Plaques Neurofibrillary Tangles Diabetes Homocysteine Kalaria RN, Ballard C. Alzheimer Dis Assoc Disord. 1999;13:S
17 Diagnosis The common mistake is to label what is AD w/ CVD as VaD
18 Parkinson s disease dementia Early symptoms Sensitivity to dopaminergic treatment Hallucinations
19 Proforma essential History patient and informant Cognitive checklist Neuropsychiatric symptoms Depression Activities of daily living (Bristol ADL) PMH Family history Medication (cholinergic burden) Head injury
20 Cognitive assessment Proforma MMSE (orientation, registration and recall, attention, language, visual construction) ACE III (attention, memory, verbal fluency, language, visuospatial) General examination important CVS CNS
21 Investigations Full blood picture ESR/CRP Clinical chemistry profile (U&E, calcium, glucose) Thyroid function B 12 and folate Neuroimaging (next talk)
22 Diagnostic Criteria for AD Supportive features B. Presence of medial temporal lobe atrophy Volume loss of hippocampi, entorhinal cortex, amygdala evidenced on MRI with qualitative ratings using visual scoring (referenced to well characterised population with age norms) or quantitative volumetry of regions of interest (referenced to well characterised population with age norms) C. Abnormal cerebrospinal fluid biomarker Low amyloid β1 42 concentrations, increased total tau concentrations, or increased phospho-tau concentrations, or combinations of the three Other well validated markers to be discovered in the future Dubois et al. Lancet Neurol 2007;6:734 46
23 Diagnostic Criteria for AD Supportive Features D. Specific pattern on functional neuroimaging with PET Reduced glucose metabolism in bilateral temporal parietal regions Other well validated ligands, including those that foreseeably will emerge such as Pittsburg compound B or FDDNP E. Proven AD autosomal dominant mutation within the immediate family Dubois et al. Lancet Neurol 2007;6:734 46
24 CSF Studies
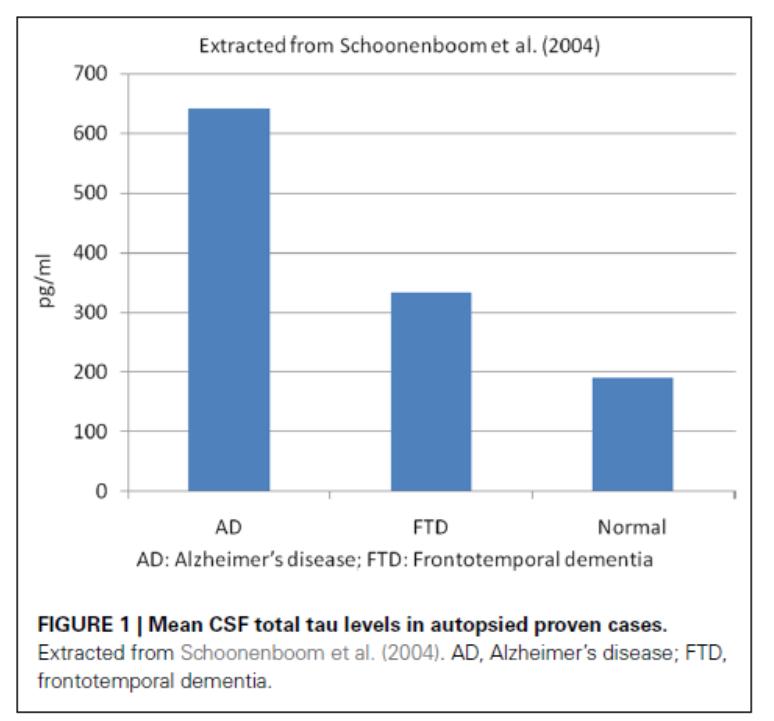
25 AD Diagnosis Low CSF Aβ42 and high t-tau or p-tau proteins have shown high accuracy for AD diagnosis (Galasko et al 1998; Andreasen et al 2001; Schoonenboom et al 2004) Studies that compared AD patients with normal control subjects have demonstrated that low Aβ42 had % sensitivity and 47 81% specificity for AD diagnosis High CSF t-tau levels had 70% sensitivity and 92% specificity and p-tau showed 77% sensitivity and 87% specificity However, p-tau appears to be better than t-tau in the diagnosis of AD, and it has shown a positive predictive value of 90%, especially p-tau phosphorylated at threonine 181 (ptau181; Hampel et al 2004a; Mitchell 2009).

26 Differential Diagnosis
27 Differential Diagnosis
28 Assessment of CSF Aβ42 as an aid to discriminating AD from other dementias and mild cognitive impairment: meta-analysis of 50 studies. CSF Aβ42 concentrations were significantly lower in AD compared to: MCI (SMD: -0.68, 95% CI: [-0.80, -0.56], P<0.001) FTD (SMD: -1.09, 95% CI: [-1.41, -0.76], P<0.001) PDD (SMD: -0.75, 95% CI: [-1.39, -0.10], P=0.023) VaD (SMD: -0.95, 95% CI: [-1.30, -0.61], P<0.001) Compared to DLB, Aβ42 concentrations are moderately lower in AD (SMD: -0.27, 95% CI: -0.51, -0.03, P=0.028) Results from this meta-analysis hinted that CSF Aβ42 is a good biomarker for discriminating Alzheimer's disease from other dementias and MCI. Tang et al. J Neurol Sci. 2014;345(1-2):26-36
29 Lumbar puncture is a routine procedure, but may not be readily acceptable to all patients. Despite being associated with side effects such as headache, it is generally well tolerated. CSF studies perhaps afford the most promising use of biomarkers for prediction, diagnosis and disease progression CSF studies probably do not add significantly to diagnostic certainty when the patient meets current clinical criteria for probable AD CSF studies may provide confirmation whether the underlying cause of MCI is likely due to AD
30 Case 1 73 year old man with 2 year history of short term memory problems. Gradual onset and more noticeable to self and family Needs persuaded to go out and play bowls. Memory loss causes some frustration/agitation, no other behavioural issues Reluctant to make telephone calls, some difficulty with finances and simple household maintenance tasks. Driving is fine, can manage his medication PMH: hypertension and ischaemic heart disease. No head injury Medication: aspirin 75mg, amlodipine 5mg, perindopril 5mg No family history of cognitive problems Cognition: ACE III 73/100. deficits in memory, attention and visuospatial testing Physical examination nothing of note Bloods normal
31 Diagnosis? 1. Mild cognitive impairment 2. Depression 3. Alzheimer s disease dementia 4. Vascular dementia 5. Alzheimer s disease + cerebrovascular disease dementia 6. Lewy body dementia
32 Case 2 76 year old lady. 18 month history of problems with short term memory. Noticeable to herself and family. Family notice a difficulty with organisational ability. Symptoms can vary. Mood can be a bit down at times but denies depression. No other cognitive or behavioural symptoms. Difficulties with finances and use of TV controls. PMH: hypertension, diabetes mellitus, ischaemic heart disease, CKD Medications: metformin 1g bd, clopidogrel 75mg, bisoprolol 5mg, perindopril 5mg No family history of cognitive problems Cognition: ACE III 76/100. Deficits in attention mostly and in language Physical examination: gait a little unsteady, symmetrical brisk reflexes Bloods: haemoglobin 110, egfr 45, BS 8.6,
33 Diagnosis? 1. Mild cognitive impairment 2. Depression 3. Alzheimer s disease dementia 4. Vascular dementia 5. Alzheimer s disease + CVD 6. Lewy body dementia
34 Case 3 78 year old man with complaints of short term memory loss for 8 months. Some restless legs, symptoms can vary. No apathy Some difficulty with managing medicines. Not keen on driving. Needs some help with finances Some frustration with memory problems. Daughter mentions he sets an extra place for dinner as he has seen his wife (she died 16 months before) in the house at times. Mood variable PMH: has fallen 3 or 4 times over past 6 months, no syncope. Hypertension, peripheral vascular disease No family history of cognitive problems Medication: amlodipine 5mg, clopidogrel 75mg, quinine sulphate 300mg, zopiclone 7.5mg Cognition: ACE III 75/100. Deficits in attention and memory mostly and a little in language Physical examination: a little slow to respond to questions, gait a little unsteady, no postural BP drop Bloods: normal
35 Diagnosis? 1. Mild cognitive impairment 2. Depression 3. Alzheimer s disease dementia 4. Vascular dementia 5. Alzheimer s disease + CVD 6. Lewy body dementia
36 Thank you for your attention
37
38 Global Function Cognitive Function Caregiver Burden Activities of Daily Living Behavioural Disturbances
39 Suggested Diagnostic Work-up for Dementia Diagnostic interview both patient and a reliable informant Office-based clinical assessment comprehensive physical examination brief neurologic and mental status evaluation brief quantified cognitive function evaluation (MMSE) Office-based clinical assessment (cont d) laboratory evaluation (CBC, chemistries, thyroid, vitamin B 12 ) optional imaging studies (CT head scan, MRI) Neuropsychological testing if diagnosis is unclear AAGP, AA, AGS consensus statement, 1997

40
41 Ideal Biomarker for AD Should detect a fundamental feature of neuropathology and be validated in neuropathologically confirmed cases Should have a diagnostic sensitivity of more than 80% for detecting AD and a specificity of more than 80% for distinguishing other dementias Should be reliable, reproducible, noninvasive, simple to perform, and inexpensive It would be especially useful if the biomarker could capture the beneficial effect of disease-modifying therapy predict conversion from MCI to AD correspond closely to available clinical detection methods and thus provide an opportunity for early intervention or prevention. Neurobiol Aging. 1998; 19:
42 AD diagnosis and progression Aβ42/tau ratio is used to improve the diagnosis of AD Meta-analysis showed that Aβ42/tau ratio had a sensitivity of 71% and specificity of 83% for AD (Hampel et al 2004) A recent study showed that the signature of AD, based on the CSF Aβ42/p-tau181 ratio cut offs, was present in 90% of the AD patients compared to 36% in the normal control group (De Meyer et al 2010) Although these CSF biomarkers seem to be useful to diagnose AD, they are not sensitive enough to assess disease progression
43 The diagnosis of dementia due to Alzheimer s disease: Recommendations from the National Institute on Aging-Alzheimer s Association workgroups on diagnostic guidelines for Alzheimer s disease The core clinical criteria for AD dementia will continue to be the cornerstone of the diagnosis in clinical practice, but biomarker evidence is expected to enhance the pathophysiological specificity of the diagnosis of AD dementia. Much work lies ahead for validating the biomarker diagnosis of AD dementia McKhann et al. Alzheimer s & Dementia 2011;7:
44 World Alzheimer Report 2011
45 Neuropsychiatric Inventory (Cummings et al., Neurology 1994;44: ) Behavioural Apathy Aberrant motor behaviour Appetite disturbance Irritability Agitation / aggression Sleep disturbance Psychological Depression Anxiety Delusions Disinhibition Hallucinations Elation
46 History Cognitive impairments central to the diagnosis of dementia can be categorised into five main domains: memory; executive function; language; visuospatial abilities; personality and behaviour As dementia, of any cause progresses, cognitive impairments broaden, involving more domains, and deepen, causing increased functional impairment It can thus be difficult to distinguish dementias of different aetiologies in the later stages In the early stages however the pattern of prominent symptoms can help identify the most likely underlying disease process
47 CSF Little doubt that CSF AB and tau are markers of AD No cut offs defined Global studies to standardize assays
48 Cochrane Database Syst Rev Jun 10;(6):CD doi: / CD pub4. Plasma and cerebrospinal fluid amyloid beta for the diagnosis of Alzheimer's disease dementia and other dementias in people with mild cognitive impairment (MCI). Ritchie C1, Smailagic N, Noel-Storr AH, Takwoingi Y, Flicker L, Mason SE, McShane R. The proposed diagnostic criteria for prodromal dementia and MCI due to Alzheimer's disease, although still being debated, would be fulfilled where there is both core clinical and cognitive criteria and a single biomarker abnormality. From our review, the measure of abnormally low CSF Aß levels has very little diagnostic benefit with likelihood ratios suggesting only marginal clinical utility. The quality of reports was also poor, and thresholds and length of follow-up were inconsistent. We conclude that when applied to a population of patients with MCI, CSF Aß levels cannot be recommended as an accurate test for Alzheimer's disease
Introduction, use of imaging and current guidelines. John O Brien Professor of Old Age Psychiatry University of Cambridge
 Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Introduction, use of imaging and current guidelines John O Brien Professor of Old Age Psychiatry University of Cambridge Why do we undertake brain imaging in AD and other dementias? Exclude other causes
Dementia Update. October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada
 Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Dementia Update October 1, 2013 Dylan Wint, M.D. Cleveland Clinic Lou Ruvo Center for Brain Health Las Vegas, Nevada Outline New concepts in Alzheimer disease Biomarkers and in vivo diagnosis Future trends
Brain imaging for the diagnosis of people with suspected dementia
 Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
Why do we undertake brain imaging in dementia? Brain imaging for the diagnosis of people with suspected dementia Not just because guidelines tell us to! Exclude other causes for dementia Help confirm diagnosis
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Dementia Diagnosis Guidelines Primary Care
 Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia Diagnosis Guidelines Primary Care Dementia Diagnosis Primary Care Guidelines Introduction Dementia is a long term condition, which primarily affects people over the age of 65 (late on-set dementia)
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia
 86 Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia Pai-Yi Chiu 1,3, Chung-Hsiang Liu 2, and Chon-Haw Tsai 2 Abstract- Background: Neuropsychiatric profile
86 Neuropsychiatric Manifestations in Vascular Cognitive Impairment Patients with and without Dementia Pai-Yi Chiu 1,3, Chung-Hsiang Liu 2, and Chon-Haw Tsai 2 Abstract- Background: Neuropsychiatric profile
Regulatory Challenges across Dementia Subtypes European View
 Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Regulatory Challenges across Dementia Subtypes European View Population definition including Early disease at risk Endpoints in POC studies Endpoints in pivotal trials 1 Disclaimer No CoI The opinions
Mild Cognitive Impairment (MCI)
") October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
October 19, 2018 Mild Cognitive Impairment (MCI) Yonas E. Geda, MD, MSc Professor of Neurology and Psychiatry Consultant, Departments of Psychiatry & Psychology, and Neurology Mayo Clinic College of Medicine
Dementia: How to explain the diagnosis to patients and relatives
 GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
GPHot Topics (April 2017): Dementia: How to explain the diagnosis to patients and relatives mohammad somauroo Consultant Physician with specialist interest in Community Geriatrics Royal Liverpool and Broadgreen
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
DISCLOSURES. Objectives. THE EPIDEMIC of 21 st Century. Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia NONE TO REPORT
 Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Clinical Assessment of Cognition: New & Emerging Tools for Diagnosing Dementia DISCLOSURES NONE TO REPORT Freddi Segal Gidan, PA, PhD USC Keck School of Medicine Rancho/USC California Alzheimers Disease
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status. Case 1 4/7/11. Which of the following evaluations is your next step?
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University of California San Francisco
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
UNIVERSITY OF WESTERN ONTARIO
 UNIVERSITY OF WESTERN ONTARIO Vladimir Hachinski, CM, MD, FRCPC, DSc Department of Clinical Neurological Sciences University of Western Ontario London, Ontario, Canada Vladimir.hachinski@lhsc.on.ca ALZHEIMER
UNIVERSITY OF WESTERN ONTARIO Vladimir Hachinski, CM, MD, FRCPC, DSc Department of Clinical Neurological Sciences University of Western Ontario London, Ontario, Canada Vladimir.hachinski@lhsc.on.ca ALZHEIMER
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Part 2: Early detection, assessment and treatment in relation to the new guidelines. Christopher Patterson McMaster University
 Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Part 2: Early detection, assessment and treatment in relation to the new guidelines Christopher Patterson McMaster University C. Patterson MD, FRCPC Division of Geriatric Medicine, McMaster University
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia
 Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Patterns of Cognitive Impairment in Dementia Lindsay R. Clark, PhD Assistant professor (CHS) Department of Medicine - Division of Geriatrics & Gerontology UW-Madison School of Medicine & Public Health
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic Guidelines? The Debate Continues
 Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Comments to this discussion are invited on the Alzforum Webinar page. Who Should Use the New Diagnostic s? The Debate Continues Ever since new criteria came out for a research diagnosis of prodromal/preclinical
Dementia and Healthy Ageing : is the pathology any different?
 Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
Dementia and Healthy Ageing : is the pathology any different? Professor David Mann, Professor of Neuropathology, University of Manchester, Hope Hospital, Salford DEMENTIA Loss of connectivity within association
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Moving Targets: An Update on Diagnosing Dementia in the Clinic
 Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Moving Targets: An Update on Diagnosing Dementia in the Clinic Eric McDade DO Department of Neurology School of Medicine Alzheimer Disease Research Center Disclosures No relevant financial disclosures
Silent Cerebral Strokes: Clinical Outcomes and Management
 Silent Cerebral Strokes: Clinical Outcomes and Management Nagaendran Kandiah Senior Consultant Neurologist, National Neuroscience Institute, Singapore Clinician Scientist, National Medical Research Council,
Silent Cerebral Strokes: Clinical Outcomes and Management Nagaendran Kandiah Senior Consultant Neurologist, National Neuroscience Institute, Singapore Clinician Scientist, National Medical Research Council,
UDS version 3 Summary of major changes to UDS form packets
 UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
UDS version 3 Summary of major changes to UDS form packets from version 2 to VERSION 3 february 18 final Form A1: Subject demographics Updated question on principal referral source to add additional options
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Significant cognitive improvement with cholinesterase inhibition in AD with cerebral amyloid angiopathy
 Paterson, Abdi 1 Significant cognitive improvement with cholinesterase inhibition in AD with cerebral amyloid angiopathy Ross W Paterson MRCP 1 *, Zeinab Abdi MRCP 1 *, Amanda Haines RMN 1, Jonathan M
Paterson, Abdi 1 Significant cognitive improvement with cholinesterase inhibition in AD with cerebral amyloid angiopathy Ross W Paterson MRCP 1 *, Zeinab Abdi MRCP 1 *, Amanda Haines RMN 1, Jonathan M
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist
 New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist Andrew E Budson, 1,2 Paul R Solomon 2,3 1 Center for Translational Cognitive Neuroscience, VA
New diagnostic criteria for Alzheimer s disease and mild cognitive impairment for the practical neurologist Andrew E Budson, 1,2 Paul R Solomon 2,3 1 Center for Translational Cognitive Neuroscience, VA
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
A Case of Vascular MCI
 A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis Initial Evaluation 78 y.o. Rt. Handed
A Case of Vascular MCI Charles DeCarli, MD Victor and Genevieve Orsi Chair in Alzheimer s Research Director Alzheimer s Disease Center University of California at Davis Initial Evaluation 78 y.o. Rt. Handed
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Alzheimer's Disease An update on diagnostic criteria & Neuropsychiatric symptoms. l The diagnosis of AD l Neuropsychiatric symptoms l Place of the ICT
 Alzheimer's Disease An update on diagnostic criteria & Neuropsychiatric symptoms State of the art lecture March 4-2012 Philippe H Robert, Philippe Nice - France Robert The diagnosis of AD Neuropsychiatric
Alzheimer's Disease An update on diagnostic criteria & Neuropsychiatric symptoms State of the art lecture March 4-2012 Philippe H Robert, Philippe Nice - France Robert The diagnosis of AD Neuropsychiatric
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia
 Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Carol Manning, PhD, ABPP-CN Director, Memory Disorders Clinic University of Virginia Case Study Mr. S. is a 74 year old man who has smoked for 20 years. He is overweight, has high cholesterol and high
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
review of existing studies on ASL in dementia Marion Smits, MD PhD
 review of existing studies on ASL in dementia Marion Smits, MD PhD Associate Professor of Neuroradiology Department of Radiology, Erasmus MC, Rotterdam (NL) Alzheimer Centre South-West Netherlands, Rotterdam
review of existing studies on ASL in dementia Marion Smits, MD PhD Associate Professor of Neuroradiology Department of Radiology, Erasmus MC, Rotterdam (NL) Alzheimer Centre South-West Netherlands, Rotterdam
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE
 CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
CHAPTER 5 NEUROPSYCHOLOGICAL PROFILE OF ALZHEIMER S DISEASE 5.1 GENERAL BACKGROUND Neuropsychological assessment plays a crucial role in the assessment of cognitive decline in older age. In India, there
September 26 28, 2013 Westin Tampa Harbour Island. Co-sponsored by
 September 26 28, 2013 Westin Tampa Harbour Island Co-sponsored by From Brains at Risk to Cognitive Dysfunction: The Role of Vascular Pathology Ralph Sacco, MD, MS, FAHA, FAAN Miller School of Medicine
September 26 28, 2013 Westin Tampa Harbour Island Co-sponsored by From Brains at Risk to Cognitive Dysfunction: The Role of Vascular Pathology Ralph Sacco, MD, MS, FAHA, FAAN Miller School of Medicine
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Neuro degenerative PET image from FDG, amyloid to Tau
 Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Neuro degenerative PET image from FDG, amyloid to Tau Kun Ju Lin ( ) MD, Ph.D Department of Nuclear Medicine and Molecular Imaging Center, Chang Gung Memorial Hospital ( ) Department of Medical Imaging
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Diagnosis and management of Dementia
 Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Diagnosis and management of Dementia Dr. Jahnavi Kedare Associate Professor Dept. of Psychiatry, T. N. Medical College B. Y. L. Nair Hospital, Mumbai Prevalence of Dementia Lower than developed countries
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Introduction to Dementia: Diagnosis & Evaluation. Created in March 2005 Duration: about 15 minutes
 Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
Introduction to Dementia: Diagnosis & Evaluation Created in March 2005 Duration: about 15 minutes Axel Juan, MD The Geriatrics Institute axel.juan@med.va.gov 305-575-3388 Credits Principal medical contributor:
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS
 FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
FRONTOTEMPORAL DEGENERATION: OVERVIEW, TRENDS AND DEVELOPMENTS Norman L. Foster, M.D. Director, Center for Alzheimer s Care, Imaging and Research Chief, Division of Cognitive Neurology, Department of Neurology
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies
 A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
A Fresh View of Cognitive Disorders in Older Adults: New Classification and Screening Strategies Lynda Mackin, PhD, AGPCNP-BC, CNS University of California San Francisco School of Nursing 1 Alzheimer s
Dementia UK & Admiral Nurses
 Dementia UK & Admiral Nurses Susan Drayton Admiral Nurse www.dementiauk.org 356 Holloway road. London N7 6PA 020 7697 4174 info@dementiauk.org @DementiaUK www.dementiauk.org 356 Holloway Road. London N7
Dementia UK & Admiral Nurses Susan Drayton Admiral Nurse www.dementiauk.org 356 Holloway road. London N7 6PA 020 7697 4174 info@dementiauk.org @DementiaUK www.dementiauk.org 356 Holloway Road. London N7
Neuroimaging for dementia diagnosis. Guidance from the London Dementia Clinical Network
 Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
Neuroimaging for dementia diagnosis Guidance from the London Dementia Clinical Network Authors Dr Stephen Orleans-Foli Consultant Psychiatrist, West London Mental Health NHS Trust Dr Jeremy Isaacs Consultant
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
CAREGIVER SUMMIT. The PD You Can't See: Dealing with Non-Motor Symptoms. Kaitlyn Roland, PhD. Sponsored by:
 CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
CSF Aβ1-42 predicts cognitive impairment in de novo PD patients
 CSF Aβ1-42 predicts cognitive impairment in de novo PD patients Mark Terrelonge MPH *1, Karen Marder MD MPH 1, Daniel Weintraub MD 2, Roy Alcalay MD MS 1 1 Columbia University Department of Neurology 2
CSF Aβ1-42 predicts cognitive impairment in de novo PD patients Mark Terrelonge MPH *1, Karen Marder MD MPH 1, Daniel Weintraub MD 2, Roy Alcalay MD MS 1 1 Columbia University Department of Neurology 2
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 diagnosis and assessment bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
diagnosis and assessment bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Prof Tim Anderson. Neurologist University of Otago Christchurch
 Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
Prof Tim Anderson Neurologist University of Otago Christchurch Tim Anderson Christchurch Insidious cognitive loss From subjective memory complaints (SMC) to dementia Case 1. AR. 64 yrs Male GP referral
University of Bristol - Explore Bristol Research
 Skrobot, O. A., O'Brien, J., Black, S., Chen, C., DeCarli, C., Erkinjuntti, T.,... Kehoe, P. G. (2016). The vascular impairment of cognition classification consensus study. Alzheimer's and Dementia. DOI:
Skrobot, O. A., O'Brien, J., Black, S., Chen, C., DeCarli, C., Erkinjuntti, T.,... Kehoe, P. G. (2016). The vascular impairment of cognition classification consensus study. Alzheimer's and Dementia. DOI:
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
FTD basics! Etienne de Villers-Sidani, MD!
 FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
FTD basics! Etienne de Villers-Sidani, MD! Frontotemporal lobar degeneration (FTLD) comprises 3 clinical syndromes! Frontotemporal dementia (behavioral variant FTD)! Semantic dementia (temporal variant
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Probable Early-onset Alzheimer s Disease Diagnosed by Comprehensive Evaluation and Neuroimage Studies
 Case Report Taiwanese Journal of Psychiatry (Taipei) Vol. 25 No. 1 2011 45 Probable Early-onset Alzheimer s Disease Diagnosed by Comprehensive Evaluation and Neuroimage Studies Sin-Yi Chen, M.D. 1, Yuan-Han
Case Report Taiwanese Journal of Psychiatry (Taipei) Vol. 25 No. 1 2011 45 Probable Early-onset Alzheimer s Disease Diagnosed by Comprehensive Evaluation and Neuroimage Studies Sin-Yi Chen, M.D. 1, Yuan-Han
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Dementia and Delirium
 Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Dementia and Delirium LPT Gondar Mental Health Group www.le.ac.uk Dementia and Delirium WTINP Chapter 4.6 Introduction - areas to be covered Delirium Definition and causes Clinical features Management
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Next patient please Dementia Clare Hawley 2018
 Next patient please Dementia Clare Hawley 2018 I have no conflict of interest to declare Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory Angina Hon Clinical
Next patient please Dementia Clare Hawley 2018 I have no conflict of interest to declare Dr Clare Hawley Associate Specialist Cardiology Chesterfield Royal Hospital GPwSI Refractory Angina Hon Clinical
Dementia and Delirium:
 Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive
Dementia and Delirium: A Neurologist s Approach to Altered Mental Status S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017