Learning Objectives: continued
|
|
|
- Abigayle Phelps
- 5 years ago
- Views:
Transcription

1
2 Learning Objectives: Describe the importance of a comprehensive assessment of a critically ill patient Describe how to assess the efficacy of breathing, work of breathing and adequacy of ventilation Discuss the principles of pulse oximetry Discuss the principles of blood gas analysis(abg,vbg,mixed Venous) continued
3 Continued Learning Objectives: Discuss the principles of ETCo2 Discuss the monitoring priorities of a mechanically ventilated patient Discuss the monitoring priorities of an intubated patient(ett,tt) Discuss the monitoring priorities of a patient with a chest drainage system
4 Sources for MONITORING RESPIRATORY FUNCTION History Taking : * Biographic Data * Current Health * ROS Physical Examination & Periodic Assessment Diagnostic Evaluations & Lab Tests
5
6
7 SIGNS & SYMPTOMS Dyspnea Respiratory pattern changes Coughing Sputum production Abnormal sounds (wheezing,crackle,rattle, stridor,gargling,snoring,friction rub) Asymmetrical chest movements Chest pain(non-cardiac/cardiac) Cyanosis Clubbing


8 DYSPNEA Onset Duration Timing Constant vs. Episodic Relieved by body position or medication Other manifestations(chest Pain,Cough,Nausea,Sputum,Weakness) Specific aggravating or alleviating factors(exertion/activity,stress/anxiety, Positin, Allergens, Medications)
9 Cough Onset Duration Timing Relieved by medications,fluids,rest? Is cough dry,hacking,wheezy? Other Manifestations(Chest Pain,fever,Dyspnea,Sputum) Specific aggravating or alleviating factors(fever,position,allergies,medication)
10 SPUTUM Duration Sudden vs Gradual onset Amount Appearance(Bloody,Purulent,Frothy, ) Color Anticoagulant or Immunosuppresive drugs use?
11 Abnormal Sounds Crackle(rale): atelectasis Wheeze: bronchospasm Rhonchus: partial obstruction of Bronchus Rattle: sputum retention, pulmonary edema Stridor: laryngeal or tracheal obstruction Friction rub: Pleurisy Snoring: obstruction in URT(nose and mouth) Gargling: fluid in upper airway
12 WHEEZING Onset (Sudden vs Gradual) Duration Timing Severity Relieved by medications,removal of allergens, Other Manifestations(Chest Pain,Cough) Specific aggravating or alleviating factors (Exertion/Activity,Stress/Anxiety,Allergies/Irritants,Medications)
13 STRIDOR Difficulty Swallowing Early Morning Headache Excessive Sleepiness Risk of Aspiration Heart Failure Voice Change
14 NONCARDIAC CHEST PAIN Location Duration Timing Radiation Previous Episodes Client Description (Burning,Sharp,Aching) Specific Aggravating or Alleviating Factors (Excertion,Movement,Breathing,Coughing)
15 CYANOSIS Location : * Perippheral * Central Severity

16

17 PHYSICAL EXAMINATION Inspection Palpation Percussion Auscultation
18 MONITORING IN PATIENT WHO HAS ARTIFICIAL AIRWAY

19
20 NURSE MUST NOTICE TO: 1) Monitor tube placement(be in right place) 2) Monitor airway patency 3) Monitor secretions viscosity 4) Monitor artificial airway fixation 5) Monitor cuff pressure how? 6) Monitor oral cavity BRUSHED? 7) Monitor S&S of complications
21 Breathing Sounds Normal: * Tubular(Bronchial) * Bronchovesicular * Vesicular Abnormal: * Crackle * Wheezing * Friction rub * Ronchous
22
23 OXYGENATION & VENTILATION MONITORING is necessary to assess ADEQUACY of LUNG VENTILATION & TISSUE OXYGENATION
24 DIAGNOSTIC TESTS
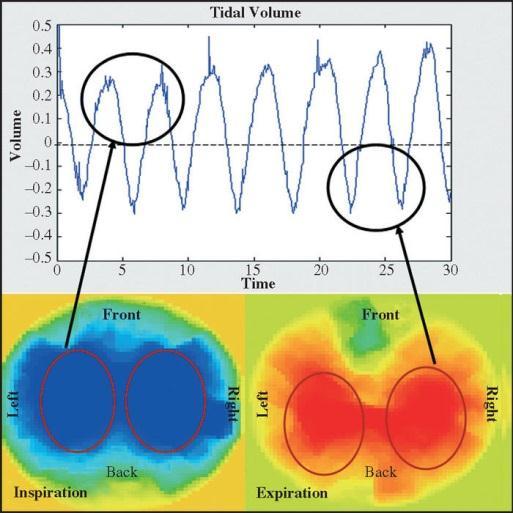
25 Functional Assessment: Pulmonary Function Test(PFT) Electrical Impedance Tomography/EIT (Pneumotachometry, Lab Tests( ABG analysis, α1 Anti-Tripsin, pleural fluid analysis, sputum examination, ) Pulse Oximetry SvO2 Monitoring(PA Cath, Transbronchial) Capnography(EtCO2 Monitoring) Respiratory Waveform Analysis

26 PULMONARY FUNCTION TEST (PFT)

27 PFT
28 Pulmonary Function Test
29



30 Pulse Oximetry

31
32 Normal Blood Gas Values Arterial Mixed Venous PH PaO mmhg SaO2 95 % PaCO mmhg HCO meq/lit BE -2 to +2 PH PaO mmhg SaO % PaCO mmhg HCO meq/lit BE -2 to +2
![Acid - Base Disorders Disorder ph [H + ] Primary disturbance Metabolic acidosis Metabolic alkalosis Respiratory](/docs-images/93/112718465/images/33-0.jpg "acidosis Respiratory alkalosis Secondary response [HCO 3- ] pco 2 [HCO 3- ] pco 2 pco 2 [HCO 3- ] pco 2 [HCO 3-")
33 Acid - Base Disorders Disorder ph [H + ] Primary disturbance Metabolic acidosis Metabolic alkalosis Respiratory acidosis Respiratory alkalosis Secondary response [HCO 3- ] pco 2 [HCO 3- ] pco 2 pco 2 [HCO 3- ] pco 2 [HCO 3- ]


34
35 Colorimetric ETco2(ETco2)


36

37
38

39
40

41 Electrical Impedance Tomography (EIT,Pneumotachometry)
42
43 ANATOMICAL ASSESSMENT



44

45
46

47


48

49

50
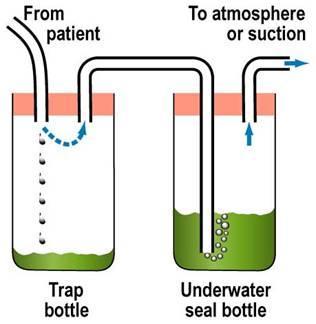
51 CHEST TUBE & CHEST DRAINAGE SYSTEM

52

53

54

55
56
57 Chest drainage system should be monitored for: Drainage System Patency Proper connecting between tube & drainage system Keeping drainage system closed Functioning the system(water seal, fluid Oscillation) Drained secretions(amount,color,quality, ) Complication signs & symptoms Condition of insertion site( skin & wound, dressing)

58


59

60
61 Triggering Cycling Limitation Ventilator Patient Volume Pressure Time Volume Pressure
62 Volume Cycled Pressure Cycled Time Cycled
63 Volume-Cycled CMV / ACV SIMV Pressure-Cycled PCV PSV(VAPSV) APRV Dual Control PRVC


64 PAV Proportional Assist Ventilation ASV Adaptive Support Ventilation(PS / PC)
65 Other Ventilatory ILV(DLV) Modalities IRV(PCIRV) HFV : * HFPPV * HFJV * HFO

66 CPAP PEEP BiPAP
67 Volume Time PPV (Alarms) Flow Pressure
 Condition * Patency *")

68 Parameters should be monitored during PPV: Patient s Airway(ETT/TT) Condition * Patency * Fixation & Length of the tube * Cuff Pressure * Secretions * Oral cavity * Ventilator Circuit * Complications
 Airway Pressures (")
 I : E Ratio Compliance(Static,Dynamic)")
69 Ventilatory parameters should be monitored during PPV: Respiratory Pattern ( Rate,Depth,Rhythm ) Airway Pressures ( PIP,Pplat,Pmean,PEEP,AutoPEEP ) Vt & MV ( Exp. Vt, Minute Ventilation ) I : E Ratio Compliance(Static,Dynamic) Airway Resistance Scalars & Loops
70 Minute Ventilation: ml/kg(ibw) /min or Male: MV = 4 BSA (based on Height& Weight) Female: MV = 3.5 BSA (based on Height& Weight)

71 Resistance Resistance= Airway Pressure(Paw) / Flow (R=P/F) Normal range: CmH2O/lit.sec With ETT: 5-6 CmH2O/lit.sec

72
73

74
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
The Goal of the Respiratory Assessment. Two Parts of the Respiratory Assessment
 The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
Therapist Written RRT Examination Detailed Content Outline
 I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
NEO 111 Melanie Jorgenson, RN, BSN
 NEO 111 Melanie Jorgenson, RN, BSN Inspection: performing deliberate, purposeful observations in a systematic manner Palpation: using the sense of touch Percussion: striking one object against another
NEO 111 Melanie Jorgenson, RN, BSN Inspection: performing deliberate, purposeful observations in a systematic manner Palpation: using the sense of touch Percussion: striking one object against another
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Northwest Community EMS System Continuing Education Class Credit Questions Respiratory Assessment January 2012
 Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
August 2013 CE. Site code # E-1213
 August 2013 CE Site code # 107200E-1213 Caring for the Patient with CHF or COPD Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
August 2013 CE Site code # 107200E-1213 Caring for the Patient with CHF or COPD Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
Oxygen Therapy. 7. Partial Initiation of therapy
 Oxygen Therapy 1. Nasal Initiation of therapy Cannula 2. Alteration of therapy 3. Change of equipment 4. Simple Mask Initiation of therapy 5. Alteration of therapy 6. Change of equipment 7. Partial Initiation
Oxygen Therapy 1. Nasal Initiation of therapy Cannula 2. Alteration of therapy 3. Change of equipment 4. Simple Mask Initiation of therapy 5. Alteration of therapy 6. Change of equipment 7. Partial Initiation
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Chapter 24. Kyphoscoliosis. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 24 Kyphoscoliosis 1 A Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary
Chapter 24 Kyphoscoliosis 1 A Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
SESSION 3 OXYGEN THERAPY
 SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
COMMISSION ON ACCREDITATION FOR RESPIRATORY CARE TMC DETAILED CONTENT OUTLINE COMPARISON
 A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Respiratory Management of Facioscapulohumeral Muscular Dystrophy. Nicholas S. Hill, MD Tufts Medical Center Boston, MA
 Respiratory Management of Facioscapulohumeral Muscular Dystrophy Nicholas S. Hill, MD Tufts Medical Center Boston, MA Respiratory Involvement in FSHD Very variable time of onset rate of progression Muscles
Respiratory Management of Facioscapulohumeral Muscular Dystrophy Nicholas S. Hill, MD Tufts Medical Center Boston, MA Respiratory Involvement in FSHD Very variable time of onset rate of progression Muscles
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
And Then There is Failure
 Heart Failure And Then There is Failure Heart Failure Brenda Phipps BSN Nurse Educator Minneapolis VA Tina Wright MSN Clinical Nurse Leader Minneapolis VA Symptoms SOB, use of accessory muscles Crackles,
Heart Failure And Then There is Failure Heart Failure Brenda Phipps BSN Nurse Educator Minneapolis VA Tina Wright MSN Clinical Nurse Leader Minneapolis VA Symptoms SOB, use of accessory muscles Crackles,
NUR 201. I believe. - we are continually learning building on previously learned concepts.
 NUR 201 I believe - we are responsible for preparing and learning. - we learn best by interacting & discussing collegially. - we must respect everyone. - we are continually learning building on previously
NUR 201 I believe - we are responsible for preparing and learning. - we learn best by interacting & discussing collegially. - we must respect everyone. - we are continually learning building on previously
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Problem Based Learning Session. Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days.
 Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Problem Based Learning Session Mr Robinson is a 67 year old man. He visits the GP as he has had a cough and fever for 5 days. The GP takes a history from him and examines his chest. Over the left base
Chapter 21. Flail Chest. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
Arterial Blood Gases Interpretation Definition Values respiratory metabolic
 Arterial Blood Gases Interpretation Definition A blood gas test measures the amount of oxygen and carbon dioxide in the blood. It is also useful in determining the ph level of the blood. The test is commonly
Arterial Blood Gases Interpretation Definition A blood gas test measures the amount of oxygen and carbon dioxide in the blood. It is also useful in determining the ph level of the blood. The test is commonly
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
Blood Gases / Acid-Base
 Blood Gases / Acid-Base Neonatal Ventilation Workshop June 2010 Dr. Julian Eason Consultant Neonatologist Why are blood gases performed? Diagnostic assessment of oxygenation capacity of lungs Therapeutic
Blood Gases / Acid-Base Neonatal Ventilation Workshop June 2010 Dr. Julian Eason Consultant Neonatologist Why are blood gases performed? Diagnostic assessment of oxygenation capacity of lungs Therapeutic
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
AIRWAY & HEART ANOTOMY
 Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
Objectives I CAN T BREATH Respiratory Emergencies Review of anatomical structures related to heart & lungs Differentiate differences between adult and pediatric airways Identify the need for airway assistance
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR
 CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 5 Respiratory Disorders. TEXT ASSIGNMENT Paragraphs 5-1 through 5-17. LESSON OBJECTIVES After completing this lesson, you should be able to: 5-1. Identify the characteristics,
LESSON ASSIGNMENT LESSON 5 Respiratory Disorders. TEXT ASSIGNMENT Paragraphs 5-1 through 5-17. LESSON OBJECTIVES After completing this lesson, you should be able to: 5-1. Identify the characteristics,
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
F: Respiratory Care. College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 59
 F: Respiratory Care College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 59 Competency: F-1 Airway Management F-1-1 F-1-2 F-1-3 F-1-4 F-1-5 Demonstrate knowledge and ability
F: Respiratory Care College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 59 Competency: F-1 Airway Management F-1-1 F-1-2 F-1-3 F-1-4 F-1-5 Demonstrate knowledge and ability
CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center
 FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
H: Respiratory Care. Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79
 H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care
 Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
Anatomy and Physiology
 Anatomy and Physiology Respiratory Diagnostic Procedures 2004 Delmar Learning, a Division of Thomson Learning, Inc. Bell Work Complete cost of smoking exercise. We will go over this together! (Don t worry)!
Anatomy and Physiology Respiratory Diagnostic Procedures 2004 Delmar Learning, a Division of Thomson Learning, Inc. Bell Work Complete cost of smoking exercise. We will go over this together! (Don t worry)!
Altered Respiratory Function Lecture 3. Nicole Tinny, RN, MSN Lake Sumter State College
 Altered Respiratory Function Lecture 3 Nicole Tinny, RN, MSN Lake Sumter State College Rhinitis Inflammation of nasal mucosa Due to infection or allergens Allergic rhinitis (hayfever) Rebound rhinitis
Altered Respiratory Function Lecture 3 Nicole Tinny, RN, MSN Lake Sumter State College Rhinitis Inflammation of nasal mucosa Due to infection or allergens Allergic rhinitis (hayfever) Rebound rhinitis
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL
 PROTOCOL") AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Ventilating the paediatric patient. Lizzie Barrett Nurse Educator November 2016
 Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
St. Dominic Jackson Memorial Hospital. Pulmonary Services. Therapist Driven Protocol. Assess and Treat Aerosol Therapy
 St. Dominic Jackson Memorial Hospital Pulmonary Services Therapist Driven Protocol Assess and Treat Aerosol Therapy Purpose The purpose of the Therapist Driven Protocol (TDP) aerosol therapy is to create
St. Dominic Jackson Memorial Hospital Pulmonary Services Therapist Driven Protocol Assess and Treat Aerosol Therapy Purpose The purpose of the Therapist Driven Protocol (TDP) aerosol therapy is to create
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Definitions. Definitions. Weaning. Weaning. Disconnection (Discontinuation) Weaning
 Weaning") Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
Getting Strarted using the Nursing Care Plans Templates
 Getting Strarted using the Nursing Care Plans Templates Using available Nursing Care Plan Templates. These templates are delivered as is and there is nothing which prevents you to use and modify these
Getting Strarted using the Nursing Care Plans Templates Using available Nursing Care Plan Templates. These templates are delivered as is and there is nothing which prevents you to use and modify these
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days
 1 week b) 24 days") Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
d) Always ensure patient comfort. Be considerate and warm the diaphragm of your stethoscope with your hand before auscultation.
 Always ensure patient comfort. Be considerate and warm the diaphragm of your stethoscope with your hand before auscultation.") Auscultation Auscultation is perhaps the most important and effective clinical technique you will ever learn for evaluating a patient s respiratory function. Before you begin, there are certain things
Auscultation Auscultation is perhaps the most important and effective clinical technique you will ever learn for evaluating a patient s respiratory function. Before you begin, there are certain things
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
ACVECC Small Animal Benchmark, May 2012
 ACVECC Small Animal Benchmark, May 2012 A 25 kg, 9 y MC Labrador Retriever presents with a 2-day history of cough and tachypnea. Physical exam revealed T 101.7 F, HR 120 BPM, pulses strong and synchronous,
ACVECC Small Animal Benchmark, May 2012 A 25 kg, 9 y MC Labrador Retriever presents with a 2-day history of cough and tachypnea. Physical exam revealed T 101.7 F, HR 120 BPM, pulses strong and synchronous,
High-Acuity Nursing. Global edition. Global edition. Kathleen Dorman Wagner Melanie G. Hardin-Pierce
 High-Acuity Nursing For these Global Editions, the editorial team at Pearson has collaborated with educators across the world to address a wide range of subjects and requirements, equipping students with
High-Acuity Nursing For these Global Editions, the editorial team at Pearson has collaborated with educators across the world to address a wide range of subjects and requirements, equipping students with
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
How it Works. CO 2 is the smoke from the flames of metabolism 10/21/18. -Ray Fowler, MD. Metabolism creates ETC0 2 for excretion
 CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
RESPIRATORY ASSESSMENT JENNY CASEY RESPIRATORY SERVICES LEAD ACE
 RESPIRATORY ASSESSMENT JENNY CASEY RESPIRATORY SERVICES LEAD ACE What does respiratory assessment involve? Subjective Assessment Objective Assessment Inspection, palpation, percussion and auscultation
RESPIRATORY ASSESSMENT JENNY CASEY RESPIRATORY SERVICES LEAD ACE What does respiratory assessment involve? Subjective Assessment Objective Assessment Inspection, palpation, percussion and auscultation
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP
 with BiPAP Device/Nasal CPAP") I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
BIOE221. Session 5. Examination of Thorax- Respiratory system. Bioscience Department. Endeavour College of Natural Health endeavour.edu.
 BIOE221 Session 5 Examination of Thorax- Respiratory system Bioscience Department Session Objectives Understand the structure of the thorax and the organs contained in this cavity Understand the importance
BIOE221 Session 5 Examination of Thorax- Respiratory system Bioscience Department Session Objectives Understand the structure of the thorax and the organs contained in this cavity Understand the importance
Cardiovascular and Respiratory Disorders
 Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Cardiovascular and Respiratory Disorders Blood Pressure Normal blood pressure is 120/80 mmhg (millimeters of mercury) Hypertension is when the resting blood pressure is too high Systolic BP is 140 mmhg
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Physiological Causes of Abnormal ABG s
 Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Airway Clearance Devices
 Print Page 1 of 11 Wisconsin.gov home state agencies subject directory department of health services Search Welcome» August 2, 2018 5:18 PM Program Name: BadgerCare Plus and Medicaid Handbook Area: Durable
Print Page 1 of 11 Wisconsin.gov home state agencies subject directory department of health services Search Welcome» August 2, 2018 5:18 PM Program Name: BadgerCare Plus and Medicaid Handbook Area: Durable
For more information about how to cite these materials visit
 Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed.
 Chapter 5 Monitoring the Emergency Patient NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1. Monitoring
Chapter 5 Monitoring the Emergency Patient NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1. Monitoring
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory