Sleep disordered breathing (SDB)
|
|
|
- Margaret Reed
- 5 years ago
- Views:
Transcription
 Scope of SDB Obstructive sleep apnoea (OSA) Central sleep apnoea (CSA)")
1 Update on Sleep Medicine II Sleep-disordered breathing Dirk Pevernagie Sleep Medicine Centre, Kempenhaeghe Foundation, Nl Dpt. Internal Medicine, Ghent University, Be ESRS Congress Tallinn Sleep disordered breathing (SDB) Scope of SDB Obstructive sleep apnoea (OSA) Central sleep apnoea (CSA) Hypoventilation (daytime hypercapnia) SDB in children 1
2 OSA current concept and definition Functional disorder characterized by repetitive obstructions of the upper airway (UA) during sleep Causing sleep disruption that the patient may or may not perceive Often causing or aggravating functional complaints and affecting comorbid conditions, e.g. arterial hypertension, disturbed glucose metabolism, etc. Treatment aims at stabilizing the UA during sleep OSA Update Update: What s new? Huge annual scientific output # hits on OSA in PubMed > 7500 yet limited data and often conflicting results Capita selecta on OSA: Pathophysiology Comorbidities Treatment Implications for clinical practice 2
3 Pathophysiology Pathophysiology Passive narrowing of the UA during sleep is the cause of increased resistance to inspiratory flow The pattern of inspiratory effort during obstruction is typically incremental, to overcome the increased resistance The crescendo effort is usually futile and an arousal is required to undo the obstruction Classical model: the balance of forces theory 3

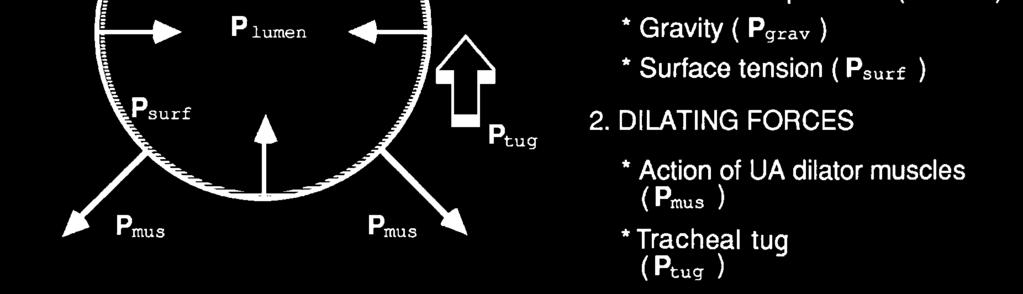
4 Pathophysiology classical paradigm Pathophysiology classical paradigm Isono et al. JAP 97, 82,

5 Pathophysiology classical paradigm 4 UA CSA (cm²) Pcrit Normal OSA pt AIRWAY PRESSURE (cm H 2 O) Isono et al. JAP 97, 82, 1319 Pcrit is a measure of the anatomic characteristics of the UA Pathophysiology new paradigm 5
6 Pathophysiology new paradigm Apneic [58] and non apneic [17] subjects (M+F) Determination of AHI and: Pcrit (anatomic factor) Arousal threshold Loop gain (respiratory control instability) Genioglossus Muscle responsiveness non anatomic factors Pathophysiologic traits were quantified ( PALM score) and varied substantially among subjects Eckert et al. AJRCCM 13, 188, 996 Pathophysiology new paradigm Eckert et al. AJRCCM 13, 188, 996 6
7 Pathophysiology new paradigm Loop gain = 4.2 / 1.4 = 3 Eckert et al. AJRCCM 13, 188, 996 Pathophysiology new paradigm Eckert et al. AJRCCM 13, 188, 996 7
 2b -2 to +2 37% Moderately collapsible UA one or more non-anatomic factors are important overall severe OSA (wide range) 3 <-2 hpa 19% Slightly collapsibel UA all have one or")

8 Pathophysiology The PALM scale PALM # Pcrit % Pts Features Treatment targets 1 >+2 23% Higly collapsible UA severe OSA 2a -2 to +2 21% Moderately collapsible UA only anatomically driven overall severe OSA (wide range) 2b -2 to +2 37% Moderately collapsible UA one or more non-anatomic factors are important overall severe OSA (wide range) 3 <-2 hpa 19% Slightly collapsibel UA all have one or more nonanatomic factors mild to moderate OSA (wide range) Anatomic intervention (CPAP) Anatomic intervention (CPAP, MRA,...) Anatomic plus nonanatomic interventions (e.g. oxygen supplement, sedatives) Combination of targeted therapies, plausibly with nonanatomic interventions Eckert et al. AJRCCM 13, 188, 996 Pathophysiology Phenotyping Editorial by S. Parathasarathy Physiologic phenotyping of OSA may lead to personalized treatment 8
9 Comorbidities of OSA Comorbidities of OSA what is known? Moderate to severe OSA is associated with: Arterial hypertension (AHT) *** new studies *** Cardiovascular morbidity and mortality Impaired glucose metabolism, dyslipidemia Systemic inflammation and oxidative stress New evidence on cancer 9
10 Comorbidities of OSA AHT Prearousal Arousal Shepard J. MCNA 85, 69, 1243 Timeline: Comorbidities of OSA AHT 90 s: trials with deficient study design Stradling et al. Sleep 97: Sleep apnea and hypertension what a mess! 00 s: adequate RCT s: significant decrease in 24 h BP Pepperell et al. Lancet 2002 Becker et al. Circulation s: Cohort studies and meta analyses O Connor et al. SHHS. AJRCCM 2009 Cano Pumarega et al. Vitoria Sleep cohort. AJRCCM 2011 Montesi et al. Meta analysis on CPAP. J Clin Sleep Med

11 OSA AHT: carefully conducted studies Pepperell et al. Lancet 2002 Becker et al. Circulation 2003 OSA AHT: current state of knowledge About half of OSA patients have AHT About a third of AHT patients have OSA About 80% of pts with resistant AHT have OSA; OSA may be the leading cause in about 2/3 CPAP decreases MAP by about 2 mmhg Some parameters may predict the antihypertensive effect of CPAP therapy New evidence on incident and resistant AHT 11
, 50% AHT, randomized to CPAP vs no treatment for 4 years")
12 OSA: new onset AHT in prospective cohorts Barbé et al. JAMA 2012 Vol 307, Marin et al. JAMA 2012 Vol 307, Spanish Sleep & Breathing Network OSA: new onset AHT in prospective cohorts Barbé: 725 OSA (AHI > 20; ESS < 10), 50% AHT, randomized to CPAP vs no treatment for 4 years Outcome: incidence of new AHT or CV events: (n/100 person years) CPAP = 11.0 untreated = 9.2 (NS) No difference in both groups when stratified for AHI (OSA severity) Post hoc analysis: better results in CPAP adherent patients 12
13 OSA: new onset AHT in prospective cohorts Marin: follow up of 1889 non hypertensive subjects (OSA + CPAP, OSA CPAP, non OSA) for > 10 years Outcome: incidence of new AHT: 705 cases Non-OSA Ineligible Declined Poor adherence Adherent I/100 p-y adjusted HR Compared with non OSA, OSA was associated with increased adjusted risk of incident AHT CPAP therapy was associated with a lower risk of AHT OSA: new onset AHT in prospective cohorts Comment: However, the potential bias related to group assignment based on adherence to therapy, which is inherent in observational study design, precludes definitive causal conclusions regarding the affect of CPAP therapy on the risk for hypertension in OSA. 13
 Martinez Garcia: 194 OSA (AHI ± 40) and RAHT were randomly")
 and DBP but not SBP were significantly lower in CPAP treatment arm, which had also more dippers (35.")
14 OSA: Impact of CPAP on resistant AHT Martinez-Garcia et al. JAMA 2013 Vol 310, OSA: Effect of CPAP on resistant AHT (RAHT) Martinez Garcia: 194 OSA (AHI ± 40) and RAHT were randomly assigned to CPAP (n = 98) or no CPAP (n = 96) for 3 months Outcome: decrease of BP parameters; BP dipping (ITT) MBP (3.1mm Hg) and DBP but not SBP were significantly lower in CPAP treatment arm, which had also more dippers (35.9 vs 21,6%) Hours of CPAP use correlated with decrease of BP So, favourable effects of CPAP were demonstrated 14
15 OSA: Effect of CPAP on resistant AHT (RAHT) Bakker: meta analysis of 8 RCTs including 968 OSA pts without major comorbidities; CPAP vs non therapeutic control conditions SBP was reduced by 2.3 mm Hg and DBP by 1.8 mm Hg in CPAP vs control. Various parameters affected the outcome of CPAP treatment. Conclusions: OSA pts with uncontrolled hypertension are likely to gain the largest benefit from PAP in terms of a substantial reduction in BP, even after controlling for disease severity. OSA, AHT and CPAP: summary Additional evidence for (1) risk of new onset AHT in OSA; (2) beneficial effect of CPAP therapy on BP Predictors of improvement of BP with CPAP therapy: 1. good adherence 2. young age 3. baseline BP (biggest effects in pts with higher end BP) 4. daytime sleepiness (larger falls in sleepier patients) 5. severity of OSA Yet effect of CPAP << effect of AHT drugs 15


16 OSA and cancer Almendros et al. ERJ 2012, 39, 215 OSA and cancer Almendros: conventional murine melanoma model ; 6 h/day CIH (60 events/h 1 ; 20 s of 5% O 2 40 s of room air) Growth of tumour D8, 11, 14 Animals D14 T growth in CIH mice >> control mice Hypothesis: CIH may stimulate angiogenesis and thus T growth 16
17 OSA and cancer Nieto: 22 yr follow up > 1500 people of Wisconsin cohort 50/112 deaths from cancer; total and cancer mortality ~ SDB Predictors: AHI and HO I baseline* Significant association mortality indices of SDB severity (after adjustment) HO I better predictor than AHI This population based epidemiologic study suggests a dose response relation between SDB and cancer mortality *Pts on CPAP were included; after exclusion association became stronger OSA and cancer Campos Rodriguez: retrospective study (N=4910 ; 4.5 yrs) 261 pts (5.3%) had diagnosis of cancer Predictors: AHI and HO I baseline* only HO I seems to have predictive power *Pts on CPAP were included; after exclusion association was not changed 17
18 Conclusions: OSA and cancer These three studies provide prleiminary evidence for the role of CIH in cancer incidence / progression Limitations: severe hypoxia model in mice; retrospective analysis (Spain); prospective study not designed to analyze cancer outcomes (US); small number of events AHI instead of ODI or HO I used as primary predictor These hypothesis generating studies need confirmation by large scale and long term prospective trials using correct predictor (ODI) and outcome (type of cancer) measures Treatment of OSA 18
19 Treatment of OSA overview Continuous positive airway pressure (CPAP) Mandibular advancement devices (MAD) Upper airway surgery Maxillo mandibular surgery Body position training Body weight reduction Hypoglossal Nerve Stimulation (HNS) CPAP vs MAD American Journal of Respiratory and Critical Care Medicine Vol 187 (8) ,
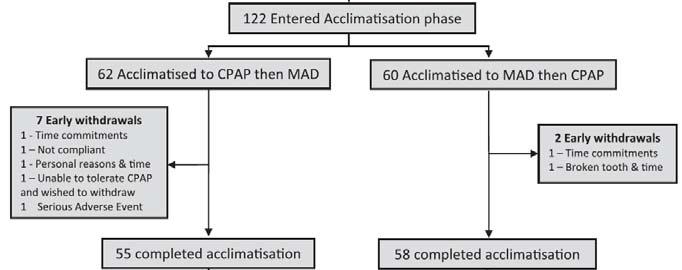
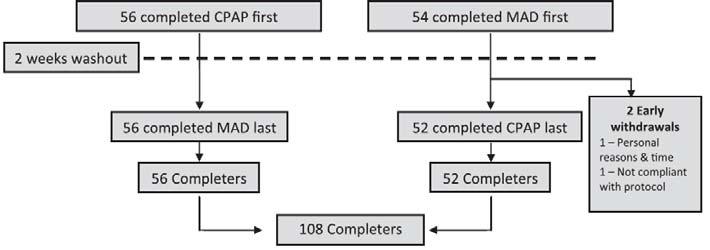
20 Study design: CPAP vs MAD CPAP (ResMed S8) vs MAD (Somnodent): effects on health outcomes in real life treatment conditions CV function, EDS, driving simulator, QoL Working hypothesis: suboptimal efficacy with MAD is counterbalanced by better compliance relative to CPAP ergo, similar overall alleviation of OSA ergo, similar effectiveness of both treatments Methods: CPAP vs MAD RCT, crossover, open label 1 month of optimal OSA treatment with CPAP vs optimal OSA treatment with MAD Optimal = highest compliance and best efficacy with each treatment in standard clinical practice Intention to treat protocol Sample size calculation was based on a BP outcome; noninferiority of MAD/CPAP for the 24MAP (margin of 1.6 mm Hg): 108 completers 20

21 CPAP vs MAD CPAP vs MAD 21

22 CPAP vs MAD CPAP vs MAD 22
 Obj/subj compliance CPAP: 4.68±2 / 5.1±2 (P<0.")
23 CPAP vs MAD 82% AHI>=15/h 81% M Overweight to obese 50% ESS > 10 38% on AHD CPAP vs MAD CPAP: 10.5±2 hpa (range 4 18 hpa) MAD: 8.09±2.6 mm (range mm) Obj/subj compliance CPAP: 4.68±2 / 5.1±2 (P<0.001) Treatment preference: 51% MAD; 23% CPAP; 21% either; 5% neither 23
24 CPAP vs MAD PSG outcomes: CV Outcomes: CPAP vs MAD Overall, BP was not lowered No differences CPAP/MAD: 24MAP ( 0.2 [ 0.7 to 1.1] mm Hg) Other BP measures In subgroup of pts with initial hypertension, a consistent treatment related 24h BP decrease (2 4 mm Hg) was found; neither treatment was superior Their was a trivial decrease of arterial stiffness (1 2%) No striking differences in neurobehavioural outcomes were found 24
25 Discussion: CPAP vs MAD Largest and most complete RCT so far comparing CPAP/MAD Innovative design, esp. acclimatization phase Focus group: moderate to severe OSA Confirmation of what is already known: CPAP is better in terms of AHI reduction MAD is superior regarding self reported compliance and patient s preference New: QoL is equivalent or better with MAD CPAP vs MAD Discussion: strenghts The current study controls for weaknesses of previous trials: exclusion of severe OSA (3 trials) small sample sizes (<50 pts) (5 trials) high dropout rates (>20%) (2 trials) nonadjustable MAD (1 trial) suboptimal compliance with CPAP (<4 h) (1 trial) including acclimatization in the treatment period Power of the study Randomisation to avoid treatment expectation bias 25
26 CPAP vs MAD Discussion: limitations 20% (actually 25%) not eligible for MAD treatment No objective measures of MAD compliance (results adjusted) Some pts did not use CPAP or MAD during PSG evaluation Noninferiority cannot be claimed: No effect from both treatment options on primary outcome BP Most pts were normotensive CPAP vs MAD Discussion: limitations Noninferiority studies are appropriate when one treatment option would be clearly preferrable to another with similar effectiveness; this is not the case in CPAP vs MAD choice personal preference is highly variable MAD must be custom made It was NOT mathematically assessed to what extent suboptimal efficacy with MAD is counterbalanced by better compliance relative to CPAP Therefore, CPAP remains treatment of first choicec 26
 for HGNS was implanted in 126 OSA pts, non adherent to CPAP, (multi center [22] single group cohort) Aim: to assess clinical safety and effectiveness @1 yr Primary outcomes: AHI, ODI and surgical")
27 HGN stimulation HGN stimulation Rationale and design: CPAP is effective for treatment of moderate to severe OSA, but insufficient compliance is an issue In this single cohort study, a device (Inspire MS) for HGNS was implanted in 126 OSA pts, non adherent to CPAP, (multi center [22] single group cohort) Aim: to assess clinical safety and yr Primary outcomes: AHI, ODI and surgical criterion for treatment success (reduction of AHI > 50% and < 20) Secondary outcomes: ESS and FOSQ 27
 Neuromuscular disease (incl.")
28 HGN stimulation Exclusion criteria: BMI > 32 kg/m² AHI < 20 or > 50/h (also >25% CSA or non supine AHI < 10/h) ENT: pronounced anatomic abnormalities or highly collapsible airway (concentric DISE) Neuromuscular disease (incl. HGN palsy) Cardiovascular and lung disease Active psychiatric disease / other sleep disorders HGN stimulation PSG PSG Control: RCT withdrawal study in 46 pt 1 week stop of treatment after 12 months Reassessment of primary outcomes PSG 28
29 HGN stimulation Results: N = 126, 83% men, 55 yrs, BMI 28 kg/m², 38% AHT, 17% UPPP AHI: 32 15/h (P<.001) ODI: 30 14/h (P<.001) 43 (32%) failure, 83 (68%) had AHI <20/h, 67 (53%) <10/h and 37 (29%) < 5/h ESS: 12 7 (P<.001) FOSQ:17 17 (P<.001) SAE: re intervention in 2, other complications in 33 Other AE: 23 temporary tongue weakness and 26 sore tongue RCT withdrawal AHI ODI Continued 9 8 Withdrawn P <.001 <.001 HGN stimulation Conclusions: In this uncontrolled cohort study, HGNS led to significant improvements in objective and subjective measures of the severity of OSA. Remaining issues: Limited eligibility (BMI < 32 kg/m²; AHI < 50/h) Definition of therapeutic success (in only 30% AHI score < 5/h is reached Better identification of responders Long term effects of HGNS? 29
30 Implications for clinical practice Implications for clinical practice The study of pathophysiology may be important to assess the phenotype of OSA (yet, noninvasive methods will be needed) Pts with severe OSA may be at risk for incident AHT; those with resistant AHT may benefit from CPAP, but adherence to treatment is important Further news on OSA cancer relationship is awaited It has not been proven that treatment with MAD is non inferior to CPAP regarding blood pressure and other outcomes Although HGNS improves severity of OSA, a cure is obtained in only a minority of patients Exclusion criteria limit applicability of MAD and HGNS AHI is losing importance in favour of ODI and HO I 30
Upper Airway Stimulation for Obstructive Sleep Apnea
 Upper Airway Stimulation for Obstructive Sleep Apnea Background, Mechanism and Clinical Data Overview Seth Hollen RPSGT 21 May 2016 1 Conflicts of Interest Therapy Support Specialist, Inspire Medical Systems
Upper Airway Stimulation for Obstructive Sleep Apnea Background, Mechanism and Clinical Data Overview Seth Hollen RPSGT 21 May 2016 1 Conflicts of Interest Therapy Support Specialist, Inspire Medical Systems
Sleep apnea as a risk factor for cardiovascular disease
 Sleep apnea as a risk factor for cardiovascular disease Malcolm Kohler Chair Respiratory Medicine, Clinical Director, Department of Pulmonology, University Hospital Zurich Incidence of fatal cardiovascular
Sleep apnea as a risk factor for cardiovascular disease Malcolm Kohler Chair Respiratory Medicine, Clinical Director, Department of Pulmonology, University Hospital Zurich Incidence of fatal cardiovascular
Mandibular Advancement Device vs CPAP in the Treatment of Obstructive Sleep Apnea: Are they Equally Effective in Short Term Health Outcomes?
 NoSnores Mandibular Advancement Device (mouthguard) for Snoring & Sleep Apnea CLINICAL REFERENCES J Clin Sleep Med. 2013 Sep;9(9):971-2. doi: 10.5664/jcsm.3008. Mandibular Advancement Device vs CPAP in
NoSnores Mandibular Advancement Device (mouthguard) for Snoring & Sleep Apnea CLINICAL REFERENCES J Clin Sleep Med. 2013 Sep;9(9):971-2. doi: 10.5664/jcsm.3008. Mandibular Advancement Device vs CPAP in
Sleep Apnea in Women: How Is It Different?
 Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
RESEARCH PACKET DENTAL SLEEP MEDICINE
 RESEARCH PACKET DENTAL SLEEP MEDICINE American Academy of Dental Sleep Medicine Dental Sleep Medicine Research Packet Page 1 Table of Contents Research: Oral Appliance Therapy vs. Continuous Positive Airway
RESEARCH PACKET DENTAL SLEEP MEDICINE American Academy of Dental Sleep Medicine Dental Sleep Medicine Research Packet Page 1 Table of Contents Research: Oral Appliance Therapy vs. Continuous Positive Airway
Precision Sleep Medicine
 Precision Sleep Medicine Picking Winners Improves Outcomes and Avoids Side-Effects North American Dental Sleep Medicine Conference February 17-18, 2017 Clearwater Beach, FL John E. Remmers, MD Conflict
Precision Sleep Medicine Picking Winners Improves Outcomes and Avoids Side-Effects North American Dental Sleep Medicine Conference February 17-18, 2017 Clearwater Beach, FL John E. Remmers, MD Conflict
Obstructive Sleep Apnea:
 Obstructive Sleep Apnea: A Physiological Approach Robert L. Owens, MD February 2018 Outline Cause(s) of OSA Can we measure the causes in an individual? Is that useful? 1 Thoracic pressure swings ( LV a
Obstructive Sleep Apnea: A Physiological Approach Robert L. Owens, MD February 2018 Outline Cause(s) of OSA Can we measure the causes in an individual? Is that useful? 1 Thoracic pressure swings ( LV a
Sleep Apnea Treatment Options, A Year After ASV
 Sleep Apnea Treatment Options, A Year After ASV Nancy Collop, MD, FAASM Emory University Associated Professional Sleep Societies, LLC 1 Conflict of Interest Disclosures for Speakers x 1. I do not have
Sleep Apnea Treatment Options, A Year After ASV Nancy Collop, MD, FAASM Emory University Associated Professional Sleep Societies, LLC 1 Conflict of Interest Disclosures for Speakers x 1. I do not have
Upper Airway Muscle Stimulation for Obstructive Sleep Apnea
 Upper Airway Muscle Stimulation for Obstructive Sleep Apnea M. Safwan Badr, MD, MBA Chair, Department of Medicine, Wayne State University School of Medicine. Staff Physician, John D. Dingell VA Medical
Upper Airway Muscle Stimulation for Obstructive Sleep Apnea M. Safwan Badr, MD, MBA Chair, Department of Medicine, Wayne State University School of Medicine. Staff Physician, John D. Dingell VA Medical
Obstructive sleep apnea and hypertension: why treatment does not consistently improve blood pressure?
 Martino F. Pengo MD, PhD 7 & 8 décembre 2018, Berlin Obstructive sleep apnea and hypertension: why treatment does not consistently improve blood pressure? Sleep Disorder Center Department of Cardiovascular,
Martino F. Pengo MD, PhD 7 & 8 décembre 2018, Berlin Obstructive sleep apnea and hypertension: why treatment does not consistently improve blood pressure? Sleep Disorder Center Department of Cardiovascular,
Sleep-disordered breathing in the elderly: is it distinct from that in the younger or middle-aged populations?
 Editorial Sleep-disordered breathing in the elderly: is it distinct from that in the younger or middle-aged populations? Hiroki Kitakata, Takashi Kohno, Keiichi Fukuda Division of Cardiology, Department
Editorial Sleep-disordered breathing in the elderly: is it distinct from that in the younger or middle-aged populations? Hiroki Kitakata, Takashi Kohno, Keiichi Fukuda Division of Cardiology, Department
11/13/2017. Jeremy Tabak MD, FAASM Medical Director Baptist Hospital Sleep Lab Medical Director Baptist Sleep Lab at Galloway
 Jeremy Tabak MD, FAASM Medical Director Baptist Hospital Sleep Lab Medical Director Baptist Sleep Lab at Galloway HypnoLaus study: OSA effect on mortality US Preventive Services Task Force recommendations
Jeremy Tabak MD, FAASM Medical Director Baptist Hospital Sleep Lab Medical Director Baptist Sleep Lab at Galloway HypnoLaus study: OSA effect on mortality US Preventive Services Task Force recommendations
Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea
 Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea Sigma Theta Tau International 28th International Nursing Research Congress 27-31 July 2017
Emerging Nursing Roles in Collaborative Management of Sleep Disordered Breathing and Obstructive Sleep Apnoea Sigma Theta Tau International 28th International Nursing Research Congress 27-31 July 2017
Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows
 Unhappy Bedfellows") Question Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows 1 ResMed 2012 07 2 ResMed 2012 07 Open Airway 3 ResMed 2012 07 Flow Limitation Snore 4 ResMed 2012 07 Apnoea 5 ResMed 2012
Question Heart Failure and Sleep Disordered Breathing (SDB) Unhappy Bedfellows 1 ResMed 2012 07 2 ResMed 2012 07 Open Airway 3 ResMed 2012 07 Flow Limitation Snore 4 ResMed 2012 07 Apnoea 5 ResMed 2012
How We Breathe During Sleep Affects Health, Wellness and Longevity
 How We Breathe During Sleep Affects Health, Wellness and Longevity Susan Redline, MD, MPH Peter C. Farrell Professor of Sleep Medicine Program Director- Sleep Medicine Epidemiology Harvard Medical School
How We Breathe During Sleep Affects Health, Wellness and Longevity Susan Redline, MD, MPH Peter C. Farrell Professor of Sleep Medicine Program Director- Sleep Medicine Epidemiology Harvard Medical School
Co-Morbidities Associated with OSA
 Co-Morbidities Associated with OSA Dr VK Vijayan MD (Med), PhD (Med), DSc, FCCP, FICC, FAPSR, FAMS Advisor to Director General, ICMR Bhopal Memorial Hospital and Research Centre & National Institute for
Co-Morbidities Associated with OSA Dr VK Vijayan MD (Med), PhD (Med), DSc, FCCP, FICC, FAPSR, FAMS Advisor to Director General, ICMR Bhopal Memorial Hospital and Research Centre & National Institute for
Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK
 Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK Sleep Disordered Breathing in CHF Erratic breathing during sleep known for years e.g.
Sleep Disordered Breathing: Beware Snoring! Dr T A McDonagh Consultant Cardiologist Royal Brompton Hospital London. UK Sleep Disordered Breathing in CHF Erratic breathing during sleep known for years e.g.
Obstructive Sleep Apnea and cardiovascular risk Ferran Barbé, MD
 Obstructive Sleep Apnea and cardiovascular risk Ferran Barbé, MD Institut de Recerca Biomedica. IRBLleida CIBERES. Instituto de Salud Carlos III. Madrid. Obstructive Sleep Apnea (OSA) Obstructive Sleep
Obstructive Sleep Apnea and cardiovascular risk Ferran Barbé, MD Institut de Recerca Biomedica. IRBLleida CIBERES. Instituto de Salud Carlos III. Madrid. Obstructive Sleep Apnea (OSA) Obstructive Sleep
BTS sleep Course. Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith)
") BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
Management of OSA. saurabh maji
 Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
Oral Appliances and their Clinical Indications in OSA
 Oral Appliances and their Clinical Indications in OSA Disclosures Andrew Chan, MB BS, PhD, FRACP, FCCP Staff Specialist, Department of Respiratory and Sleep Medicine, Royal North Shore Hospital, University
Oral Appliances and their Clinical Indications in OSA Disclosures Andrew Chan, MB BS, PhD, FRACP, FCCP Staff Specialist, Department of Respiratory and Sleep Medicine, Royal North Shore Hospital, University
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea
 Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
PVDOMICS. Sleep Core. Cleveland Clinic Cleveland, Ohio
 PVDOMICS Sleep Core Rawan Nawabit, Research Coordinator and Polysomnologist Joan Aylor, Research Coordinator Dr. Reena Mehra, Co-Investigator, Sleep Core Lead Cleveland Clinic Cleveland, Ohio 1 Obstructive
PVDOMICS Sleep Core Rawan Nawabit, Research Coordinator and Polysomnologist Joan Aylor, Research Coordinator Dr. Reena Mehra, Co-Investigator, Sleep Core Lead Cleveland Clinic Cleveland, Ohio 1 Obstructive
Chronic NIV in heart failure patients: ASV, NIV and CPAP
 Chronic NIV in heart failure patients: ASV, NIV and CPAP João C. Winck, Marta Drummond, Miguel Gonçalves and Tiago Pinto Sleep disordered breathing (SDB), including OSA and central sleep apnoea (CSA),
Chronic NIV in heart failure patients: ASV, NIV and CPAP João C. Winck, Marta Drummond, Miguel Gonçalves and Tiago Pinto Sleep disordered breathing (SDB), including OSA and central sleep apnoea (CSA),
Sleep Medicine. Paul Fredrickson, MD Director. Mayo Sleep Center Jacksonville, Florida.
 Sleep Medicine Paul Fredrickson, MD Director Mayo Sleep Center Jacksonville, Florida Fredrickson.Paul@mayo.edu DISCLOSURES No relevant conflicts to report. Obstructive Sleep Apnea The most common sleep
Sleep Medicine Paul Fredrickson, MD Director Mayo Sleep Center Jacksonville, Florida Fredrickson.Paul@mayo.edu DISCLOSURES No relevant conflicts to report. Obstructive Sleep Apnea The most common sleep
OSA and Hypertension Scope of the Problem
 OSA and Hypertension Scope of the Problem Dr Ahmad Izuanuddin Ismail Senior Lecturer & Respiratory Physician Faculty of Medicine, Universiti Teknologi MARA izuanuddin@salam.uitm.edu.my http://respiratoryuitm.com
OSA and Hypertension Scope of the Problem Dr Ahmad Izuanuddin Ismail Senior Lecturer & Respiratory Physician Faculty of Medicine, Universiti Teknologi MARA izuanuddin@salam.uitm.edu.my http://respiratoryuitm.com
Oral Appliances and their Clinical Applications
 Oral Appliances and their Clinical Applications Peter Cistulli MBBS, PhD, MBA, FRACP Professor of Respiratory Medicine & Head of Discipline of Sleep Medicine University of Sydney Director, Centre for Sleep
Oral Appliances and their Clinical Applications Peter Cistulli MBBS, PhD, MBA, FRACP Professor of Respiratory Medicine & Head of Discipline of Sleep Medicine University of Sydney Director, Centre for Sleep
Shyamala Pradeepan. Staff Specialist- Department of Respiratory and Sleep Medicine. John Hunter Hospital. Conjoint lecturer University of New Castle.
 Shyamala Pradeepan Staff Specialist- Department of Respiratory and Sleep Medicine. John Hunter Hospital. Conjoint lecturer University of New Castle. What is sleep apnoea?? Repetitive upper airway narrowing
Shyamala Pradeepan Staff Specialist- Department of Respiratory and Sleep Medicine. John Hunter Hospital. Conjoint lecturer University of New Castle. What is sleep apnoea?? Repetitive upper airway narrowing
Circadian Variations Influential in Circulatory & Vascular Phenomena
 SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
Sleep and the Heart. Physiologic Changes in Cardiovascular Parameters during Sleep
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart. Rami N. Khayat, MD
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep Apnea: Vascular and Metabolic Complications
 Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea induced Endothelial Dysfunction: could it be reversible?
 Orofacial Pain and Oral Medicine Course: OFPM #723 Motor/Sleep Disorders and Oral Physiology in OFPOM Lecture #3a Dr. Glenn Clark Professor of Diagnostic Sciences Assistant Dean of Distance Education Director
Orofacial Pain and Oral Medicine Course: OFPM #723 Motor/Sleep Disorders and Oral Physiology in OFPOM Lecture #3a Dr. Glenn Clark Professor of Diagnostic Sciences Assistant Dean of Distance Education Director
Advances in the Evaluation and Management of Adult OSA
 Advances in the Evaluation and Management of Adult OSA Michelle Cao, DO Clinical Associate Professor Pulmonary, Critical Care, and Sleep Medicine Stanford University Conflict of Interest Disclosure I declare
Advances in the Evaluation and Management of Adult OSA Michelle Cao, DO Clinical Associate Professor Pulmonary, Critical Care, and Sleep Medicine Stanford University Conflict of Interest Disclosure I declare
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
Sleep and the Heart. Sleep Stages. Sleep and the Heart: non REM 8/31/2016
 Sleep and the Heart Overview of sleep Hypertension Arrhythmias Ischemic events CHF Pulmonary Hypertension Cardiac Meds and Sleep Sleep Stages Non-REM sleep(75-80%) Stage 1(5%) Stage 2(50%) Stage 3-4*(15-20%)
Sleep and the Heart Overview of sleep Hypertension Arrhythmias Ischemic events CHF Pulmonary Hypertension Cardiac Meds and Sleep Sleep Stages Non-REM sleep(75-80%) Stage 1(5%) Stage 2(50%) Stage 3-4*(15-20%)
Neuromuscular Stimulation for Sleep Apnea. Overview 1/24/2013. Disclosures. Midline Glossectomy. Palate + Hypopharyngeal Surgery: BMI
 Neuromuscular Stimulation for Sleep Apnea Disclosures The following personal financial relationships with commercial interests relevant to this presentation: Eric J. Kezirian, MD, MPH Director, Division
Neuromuscular Stimulation for Sleep Apnea Disclosures The following personal financial relationships with commercial interests relevant to this presentation: Eric J. Kezirian, MD, MPH Director, Division
Simple diagnostic tools for the Screening of Sleep Apnea in subjects with high risk of cardiovascular disease
 Cardiovascular diseases remain the number one cause of death worldwide Simple diagnostic tools for the Screening of Sleep Apnea in subjects with high risk of cardiovascular disease Shaoguang Huang MD Department
Cardiovascular diseases remain the number one cause of death worldwide Simple diagnostic tools for the Screening of Sleep Apnea in subjects with high risk of cardiovascular disease Shaoguang Huang MD Department
In-Patient Sleep Testing/Management Boaz Markewitz, MD
 In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
The value of stratified economic analysis in cohort-level models: A case study on interventions for obstructive sleep apnea
 The value of stratified economic analysis in cohort-level models: A case study on interventions for obstructive sleep apnea BERNICE TSOI AND KAREN LEE CADTH Disclosure No actual or potential conflict of
The value of stratified economic analysis in cohort-level models: A case study on interventions for obstructive sleep apnea BERNICE TSOI AND KAREN LEE CADTH Disclosure No actual or potential conflict of
Management Issues in Hypoglossal Stimulation for OSA. A Sleep Medicine view of surgery
 Management Issues in Hypoglossal Stimulation for OSA Kingman P Strohl M.D. Professor of Medicine, Physiology & Biophysicis, and Oncology Center for sleep Disorders Reseach Case Western Reserve University,
Management Issues in Hypoglossal Stimulation for OSA Kingman P Strohl M.D. Professor of Medicine, Physiology & Biophysicis, and Oncology Center for sleep Disorders Reseach Case Western Reserve University,
Obstructive Sleep Apnoea
 Obstructive Sleep Apnoea Adam Whittle Respiratory Medicine Bristol Royal Infirmary Sleep Service 1990: Bristol respiratory sleep service Drs Catterall & Kendrick, Bristol General ATW since 2001 2008: NICE
Obstructive Sleep Apnoea Adam Whittle Respiratory Medicine Bristol Royal Infirmary Sleep Service 1990: Bristol respiratory sleep service Drs Catterall & Kendrick, Bristol General ATW since 2001 2008: NICE
Management of OSA in the Acute Care Environment. Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018
 Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
18/06/2009 NZ Respiratory & Sleep Institute
 Sleep Disorders in Primary Care - a personal view 18/06/2009 Andrew G Veale NZ Respiratory & Sleep Institute Abnormal Sleep Disorders of the initiation & maintenance of sleep (DIMS) Insomnia 1 o or 2 o
Sleep Disorders in Primary Care - a personal view 18/06/2009 Andrew G Veale NZ Respiratory & Sleep Institute Abnormal Sleep Disorders of the initiation & maintenance of sleep (DIMS) Insomnia 1 o or 2 o
Snoring and Its Outcomes
 Disclosures None Snoring and Its Outcomes Jolie Chang, MD Otolaryngology, Head and Neck Surgery University of California, San Francisco February 14, 2014 Otolaryngology Head Outline Snoring and OSA Acoustics
Disclosures None Snoring and Its Outcomes Jolie Chang, MD Otolaryngology, Head and Neck Surgery University of California, San Francisco February 14, 2014 Otolaryngology Head Outline Snoring and OSA Acoustics
11/19/2012 ก! " Varies 5-86% in men 2-57% in women. Thailand 26.4% (Neruntarut et al, Sleep Breath (2011) 15: )
 15: )") Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
A Deadly Combination: Central Sleep Apnea & Heart Failure
 A Deadly Combination: Central Sleep Apnea & Heart Failure Sanjaya Gupta, MD FACC FHRS Ohio State University Symposium May 10 th, 2018 Disclosures Boston Scientific: fellowship support, speaking honoraria
A Deadly Combination: Central Sleep Apnea & Heart Failure Sanjaya Gupta, MD FACC FHRS Ohio State University Symposium May 10 th, 2018 Disclosures Boston Scientific: fellowship support, speaking honoraria
Step (2) Looked for correlations between baseline surrogates and postoperative AHI.
 Looked for correlations between baseline surrogates and postoperative AHI.") Development of the PSG PLUS PHYIOLOGY model Step (1) Picked possible surrogates of the physiological traits (See Table 1 in the main text). Step (2) Looked for correlations between baseline surrogates
Development of the PSG PLUS PHYIOLOGY model Step (1) Picked possible surrogates of the physiological traits (See Table 1 in the main text). Step (2) Looked for correlations between baseline surrogates
Inspire Therapy for Sleep Apnea
 Inspire Therapy for Sleep Apnea Patient Guide Giving You the FREEDOM TO SLEEP Like Everyone Else Take Comfort. Inspire therapy can help. Inspire therapy is a breakthrough implantable treatment option for
Inspire Therapy for Sleep Apnea Patient Guide Giving You the FREEDOM TO SLEEP Like Everyone Else Take Comfort. Inspire therapy can help. Inspire therapy is a breakthrough implantable treatment option for
Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty: A Single University Experience
 771395AORXXX10.1177/0003489418771395Annals of Otology, Rhinology & LaryngologyHuntley et al research-article2018 Original Article Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty:
771395AORXXX10.1177/0003489418771395Annals of Otology, Rhinology & LaryngologyHuntley et al research-article2018 Original Article Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty:
Obstructive Sleep Apnea
 Obstructive Sleep Apnea Definition: Repetitive episodes of upper airway obstruction (complete or partial) that occur during sleep and are associated with arousals or desaturations +/or daytime sleepiness.
Obstructive Sleep Apnea Definition: Repetitive episodes of upper airway obstruction (complete or partial) that occur during sleep and are associated with arousals or desaturations +/or daytime sleepiness.
CPAP. Why is CPAP the treatment of choice for obstructive sleep apnea? CPAP: Treatment of Choice for OSA
 CPAP: Treatment of Choice for OSA Atul Malhotra Amalhotra@ucsd.edu Pulmonary, Critical Care and Sleep Disclosure: Nothing to disclose San Francisco 2014 CPAP Among CPAP adherent patients, outcomes are
CPAP: Treatment of Choice for OSA Atul Malhotra Amalhotra@ucsd.edu Pulmonary, Critical Care and Sleep Disclosure: Nothing to disclose San Francisco 2014 CPAP Among CPAP adherent patients, outcomes are
Inspire Therapy for Sleep Apnea
 Inspire Therapy for Sleep Apnea Patient Guide Giving You the FREEDOM TO SLEEP Like Everyone Else Take Comfort. Inspire therapy can help. Inspire therapy is a breakthrough implantable treatment option for
Inspire Therapy for Sleep Apnea Patient Guide Giving You the FREEDOM TO SLEEP Like Everyone Else Take Comfort. Inspire therapy can help. Inspire therapy is a breakthrough implantable treatment option for
Sleep Apnea: Diagnosis & Treatment
 Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Sleep Disordered Breathing
 Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Prefabricated Oral Appliances for Obstructive Sleep Apnea
 Medical Policy Manual Allied Health, Policy No. 36 Prefabricated Oral Appliances for Obstructive Sleep Apnea Next Review: May 2019 Last Review: April 2018 Effective: May 1, 2018 IMPORTANT REMINDER Medical
Medical Policy Manual Allied Health, Policy No. 36 Prefabricated Oral Appliances for Obstructive Sleep Apnea Next Review: May 2019 Last Review: April 2018 Effective: May 1, 2018 IMPORTANT REMINDER Medical
GOALS. Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) FINANCIAL DISCLOSURE 2/1/2017
 FINANCIAL DISCLOSURE 2/1/2017") Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) 19th Annual Topics in Cardiovascular Care Steven Khov, DO, FAAP Pulmonary Associates of Lancaster, Ltd February 3, 2017 skhov2@lghealth.org
Obstructive Sleep Apnea and Cardiovascular Disease (OVERVIEW) 19th Annual Topics in Cardiovascular Care Steven Khov, DO, FAAP Pulmonary Associates of Lancaster, Ltd February 3, 2017 skhov2@lghealth.org
Inspire Therapy for Obstructive Sleep Apnea. Clinical Data Update
 Inspire Therapy for Obstructive Sleep Apnea For OSA patients unable to tolerate or get consistent benefit from CPAP Clinical Data Update Summary of published long-term 3-year outcomes data Treatment Goals
Inspire Therapy for Obstructive Sleep Apnea For OSA patients unable to tolerate or get consistent benefit from CPAP Clinical Data Update Summary of published long-term 3-year outcomes data Treatment Goals
Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing. Alan S Maisel MD
 Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing Alan S Maisel MD Triumvirate of Health-public awareness 1.8% Sleep Physical Fitness Nutrition 91.3% 99.9% Sleep is important to
Apnea-Hypopnea- Index The new old biomarker for Sleep-Disordered Breathing Alan S Maisel MD Triumvirate of Health-public awareness 1.8% Sleep Physical Fitness Nutrition 91.3% 99.9% Sleep is important to
Is CPAP helpful in severe Asthma?
 Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
OBESITY HYPOVENTILATION SYNDROME: CPAP vs NIV. J. F. Masa San Pedro de Alcántara Hospital Cáceres. Spain
 OBESITY HYPOVENTILATION SYNDROME: CPAP vs NIV J. F. Masa San Pedro de Alcántara Hospital Cáceres. Spain Hypoventilation mechanisms OHS NIV action CPAP action Mechanical load Leptin resistance Breathing
OBESITY HYPOVENTILATION SYNDROME: CPAP vs NIV J. F. Masa San Pedro de Alcántara Hospital Cáceres. Spain Hypoventilation mechanisms OHS NIV action CPAP action Mechanical load Leptin resistance Breathing
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of hypoglossal nerve stimulation for moderate to severe obstructive sleep apnoea
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of hypoglossal nerve stimulation for moderate to severe obstructive sleep apnoea
General Outline. General Outline. Pathogenesis of Metabolic Dysfunction in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia
 Pathogenesis of Metabolic in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia Naresh M. Punjabi, MD, PhD Associate Professor of Medicine and Epidemiology Johns Hopkins University,
Pathogenesis of Metabolic in Sleep Apnea: The Role of Sleep Fragmentation and Intermittent Hypoxemia Naresh M. Punjabi, MD, PhD Associate Professor of Medicine and Epidemiology Johns Hopkins University,
Σύνδρομο σπνικής άπνοιας. Ποιός o ρόλος ηοσ ζηη γένεζη και ανηιμεηώπιζη ηων αρρσθμιών;
 Σύνδρομο σπνικής άπνοιας. Ποιός o ρόλος ηοσ ζηη γένεζη και ανηιμεηώπιζη ηων αρρσθμιών; E.N. Σημανηηράκης MD, FESC Επίκ. Καθηγηηής Καρδιολογίας Πανεπιζηημιακό Νοζοκομείο Ηρακλείοσ Epidemiology 4% 2% 24%
Σύνδρομο σπνικής άπνοιας. Ποιός o ρόλος ηοσ ζηη γένεζη και ανηιμεηώπιζη ηων αρρσθμιών; E.N. Σημανηηράκης MD, FESC Επίκ. Καθηγηηής Καρδιολογίας Πανεπιζηημιακό Νοζοκομείο Ηρακλείοσ Epidemiology 4% 2% 24%
Year in Review. Outline of Lecture
 Year in Review Allan I. Pack, M.B.Ch.B., Ph.D. John Miclot Professor of Medicine Director, Center for Sleep and Circadian Neurobiology University of Pennsylvania Perelman School of Medicine Philadelphia,
Year in Review Allan I. Pack, M.B.Ch.B., Ph.D. John Miclot Professor of Medicine Director, Center for Sleep and Circadian Neurobiology University of Pennsylvania Perelman School of Medicine Philadelphia,
Geriatric OSA: Should We Treat It?
 Geriatric OSA: Should We Treat It? Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu Sleepsurgery.ucsf.edu
Geriatric OSA: Should We Treat It? Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu Sleepsurgery.ucsf.edu
Inspire. therapy for sleep apnea. Giving you the freedom to sleep like everyone else
 Inspire therapy for sleep apnea Giving you the freedom to sleep like everyone else Take Comfort. Take Action. Inspire therapy can help. Here are some reasons people like you have chosen Inspire therapy
Inspire therapy for sleep apnea Giving you the freedom to sleep like everyone else Take Comfort. Take Action. Inspire therapy can help. Here are some reasons people like you have chosen Inspire therapy
Treatment of sleep apnea in heart failure patients after SERVE-HF results
 Treatment of sleep apnea in heart failure patients after SERVE-HF results Martin R Cowie Professor of Cardiology National Heart & Lung Institute Imperial College London (Royal Brompton Hospital Campus)
Treatment of sleep apnea in heart failure patients after SERVE-HF results Martin R Cowie Professor of Cardiology National Heart & Lung Institute Imperial College London (Royal Brompton Hospital Campus)
Central Sleep Apnoea during CPAP therapy First insights from a big data analysis. April 2018
 Central Sleep Apnoea during CPAP therapy First insights from a big data analysis April 2018 Agenda Lexicon Introduction to Big Data The findings of the Trajectories of Emergent Central Sleep Apnea during
Central Sleep Apnoea during CPAP therapy First insights from a big data analysis April 2018 Agenda Lexicon Introduction to Big Data The findings of the Trajectories of Emergent Central Sleep Apnea during
MCOEM Spring Chapter Meeting April 5, Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD
 MCOEM Spring Chapter Meeting April 5, 2014 Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD Case Presentation History of Present Illness 57 year old man with ihh/
MCOEM Spring Chapter Meeting April 5, 2014 Sleep Apnea An Overview with Emphasis on Cardiovascular Correlations Jacques Conaway, MD Case Presentation History of Present Illness 57 year old man with ihh/
Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease
 1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
(Young et al., 1993) AHI 15 AHI >5. (Peppard et al., 2013) - 10% 17%
 AHI 15 AHI >5. (Peppard et al., 2013) - 10% 17%") InSpiro ICSD3 3. 4. 5. 6. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd edition. Darien IL American Academy of Sleep Medicine 2014 1 3. 4. Pickwick American Academy
InSpiro ICSD3 3. 4. 5. 6. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd edition. Darien IL American Academy of Sleep Medicine 2014 1 3. 4. Pickwick American Academy
UCSD Pulmonary and Critical Care
 Sleep Apnea Phenotyping Atul Malhotra, MD amalhotra@ucsd.edu UCSD Pulmonary and Critical Care Director of Sleep Medicine NAMDRC 2014 Dr. Malhotra has declared no conflicts of interest related to the content
Sleep Apnea Phenotyping Atul Malhotra, MD amalhotra@ucsd.edu UCSD Pulmonary and Critical Care Director of Sleep Medicine NAMDRC 2014 Dr. Malhotra has declared no conflicts of interest related to the content
Increased Tongue Space. Option 1: Short Hook Single Point Midline Adjustment. turns the dsm world upside down! DDS TO MD COMMUNICATION
 Insider MAGAZINE DENTAL SLEEP MEDICINE MARCH 2016 Issue 10 the new dreamtap Greater Adjustment Range Increased Tongue Space Custom-formed Soft Liners Superior Retention Option 1: Short Hook Single Point
Insider MAGAZINE DENTAL SLEEP MEDICINE MARCH 2016 Issue 10 the new dreamtap Greater Adjustment Range Increased Tongue Space Custom-formed Soft Liners Superior Retention Option 1: Short Hook Single Point
The Effect of Sleep Disordered Breathing on Cardiovascular Disease
 The Effect of Sleep Disordered Breathing on Cardiovascular Disease Juan G. Flores MD Pulmonary, Critical Care and Sleep Medicine Dupage Medical Group Director of Edward Sleep Lab Disclaimers or Conflicts
The Effect of Sleep Disordered Breathing on Cardiovascular Disease Juan G. Flores MD Pulmonary, Critical Care and Sleep Medicine Dupage Medical Group Director of Edward Sleep Lab Disclaimers or Conflicts
Inspire Therapy for Sleep Apnea
 Inspire Therapy for Sleep Apnea Take Heart. If you have OSA, you re not alone. More than 18 million Americans are estimated to have Obstructive Sleep Apnea (OSA). OSA occurs when the tongue and other soft
Inspire Therapy for Sleep Apnea Take Heart. If you have OSA, you re not alone. More than 18 million Americans are estimated to have Obstructive Sleep Apnea (OSA). OSA occurs when the tongue and other soft
Patients preference of established and emerging treatment options for obstructive sleep apnoea
 Original Article Patients preference of established and emerging treatment options for obstructive sleep apnoea Tessa Campbell 1,2, Martino F. Pengo 1,3, Joerg Steier 1,4 1 Lane Fox Respiratory Unit/Sleep
Original Article Patients preference of established and emerging treatment options for obstructive sleep apnoea Tessa Campbell 1,2, Martino F. Pengo 1,3, Joerg Steier 1,4 1 Lane Fox Respiratory Unit/Sleep
The Sleep-Stroke Connection: An Under-recognized Entity. Simin Khavandgar MD UPMC Neurology Department
 The Sleep-Stroke Connection: An Under-recognized Entity Simin Khavandgar MD UPMC Neurology Department Sleep Disordered Breathing (SDB) Obstructive Sleep Apnea (OSA): -Transient cessation of airflow, duration
The Sleep-Stroke Connection: An Under-recognized Entity Simin Khavandgar MD UPMC Neurology Department Sleep Disordered Breathing (SDB) Obstructive Sleep Apnea (OSA): -Transient cessation of airflow, duration
Sleep Apnea and Heart Failure
 Sleep Apnea and Heart Failure Micha T. Maeder, MD Cardiology Division Kantonsspital St. Gallen Switzerland micha.maeder@kssg.ch Sleep Disordered Breathing (SDB) in HFrEF 700 HFrEF patients (LVEF
Sleep Apnea and Heart Failure Micha T. Maeder, MD Cardiology Division Kantonsspital St. Gallen Switzerland micha.maeder@kssg.ch Sleep Disordered Breathing (SDB) in HFrEF 700 HFrEF patients (LVEF
Clinical Trials in OSA
 24th ANNUAL ADVANCES IN SLEEP APNEA AND SNORING February 16-17, 2018 Grand Hyatt on Union Square San Francisco, California Clinical Trials in OSA Samuel T. Kuna, MD Department of Medicine Center for Sleep
24th ANNUAL ADVANCES IN SLEEP APNEA AND SNORING February 16-17, 2018 Grand Hyatt on Union Square San Francisco, California Clinical Trials in OSA Samuel T. Kuna, MD Department of Medicine Center for Sleep
High Flow Nasal Cannula in Children During Sleep. Brian McGinley M.D. Associate Professor of Pediatrics University of Utah
 High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
Commissioning Policy Individual Funding Request
 Commissioning Policy Individual Funding Request Continuous Positive Airway Pressure (CPAP) Treatment of Obstructive Sleep Apnoea/Hypopnoea Syndrome (OSAHS) Criteria Based Access Policy Date Adopted: 13
Commissioning Policy Individual Funding Request Continuous Positive Airway Pressure (CPAP) Treatment of Obstructive Sleep Apnoea/Hypopnoea Syndrome (OSAHS) Criteria Based Access Policy Date Adopted: 13
Pediatric Sleep-Disordered Breathing
 Pediatric Sleep-Disordered Breathing OSA in infants and young children is generally characterized by partial, persistent obstruction of the upper airway Continuum Benign primary snoring Upper-airway resistance
Pediatric Sleep-Disordered Breathing OSA in infants and young children is generally characterized by partial, persistent obstruction of the upper airway Continuum Benign primary snoring Upper-airway resistance
What is SDB? Obstructive sleep apnea-hypopnea syndrome (OSAHS)
") Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Have a Good Sleep? Estimated 70 million Americans have clinically significant sleep problems Chronic insomnias report decreased quality of life, memory and attention problems, decreased physical health
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Edoardo Gronda UO cardiologia e Ricerca Dipartimento Cardiovascolare IRCCS MultiMedica
 Convegno Pneumologia 2016 Milano 16-18 giugno 2016 Centro Congressi Palazzo delle Stelline Edoardo Gronda UO cardiologia e Ricerca Dipartimento Cardiovascolare IRCCS MultiMedica Central apnea 10 second
Convegno Pneumologia 2016 Milano 16-18 giugno 2016 Centro Congressi Palazzo delle Stelline Edoardo Gronda UO cardiologia e Ricerca Dipartimento Cardiovascolare IRCCS MultiMedica Central apnea 10 second
Is the population appropriate? Population: Groups that will be covered: Are there any specific subgroups that have not been mentioned?
 Sleep Disordered Breathing scope: stakeholder subgroup discussions Date: Thursday 12 April 2018 Group: 2 Population: Groups that will be covered: Adults (18 and older) with obstructive sleep apnoea/hypopnoea
Sleep Disordered Breathing scope: stakeholder subgroup discussions Date: Thursday 12 April 2018 Group: 2 Population: Groups that will be covered: Adults (18 and older) with obstructive sleep apnoea/hypopnoea
Can we do it? Yes we can! Managing Obstructive Sleep Apnea in Primary Care. Dr Andrea Loewen MD, FRCPC, DABIM (Sleep)
") Can we do it? Yes we can! Managing Obstructive Sleep Apnea in Primary Care Dr Andrea Loewen MD, FRCPC, DABIM (Sleep) Financial disclosures No conflict of interest Objectives When and how to order home
Can we do it? Yes we can! Managing Obstructive Sleep Apnea in Primary Care Dr Andrea Loewen MD, FRCPC, DABIM (Sleep) Financial disclosures No conflict of interest Objectives When and how to order home
Perioperative Management of Obstructive Sleep Apnea
 Perioperative Management of Obstructive Sleep Apnea Charles W. Atwood Jr, MD, FCCP, FAASM Associate Professor of Medicine Director, Sleep Medicine Program, VA Pittsburgh Healthcare System; Sleep Medicine
Perioperative Management of Obstructive Sleep Apnea Charles W. Atwood Jr, MD, FCCP, FAASM Associate Professor of Medicine Director, Sleep Medicine Program, VA Pittsburgh Healthcare System; Sleep Medicine
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Surgical Treatment of Snoring and Obstructive Sleep Apnea Syndrome Page 1 of 29 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Surgical Treatment of Snoring and
Surgical Treatment of Snoring and Obstructive Sleep Apnea Syndrome Page 1 of 29 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Surgical Treatment of Snoring and
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosres: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosres: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OSA and COPD: What happens when the two OVERLAP?
 2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
UP TO 25% SLEEP DISORDERED BREATHING AND STROKE OSA. Prevalence 11/12/2015. Young et al. NEJM 1993
 SLEEP DISORDERED BREATHING AND STROKE Daniel Shade, Jr., MD FCCP, ABSM, D Medical Director, AHN Sleep Medicine OSA Prevalence Young et al. NEJM 1993 Middle aged cohort (30-60years) Diagnosed by PSG, in
SLEEP DISORDERED BREATHING AND STROKE Daniel Shade, Jr., MD FCCP, ABSM, D Medical Director, AHN Sleep Medicine OSA Prevalence Young et al. NEJM 1993 Middle aged cohort (30-60years) Diagnosed by PSG, in
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #277: Sleep Apnea: Severity Assessment at Initial Diagnosis National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Quality ID #277: Sleep Apnea: Severity Assessment at Initial Diagnosis National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Methodological aspects of non-inferiority and equivalence trials
 Methodological aspects of non-inferiority and equivalence trials Department of Clinical Epidemiology Leiden University Medical Center Capita Selecta 09-12-2014 1 Why RCTs Early 1900: Evidence based on
Methodological aspects of non-inferiority and equivalence trials Department of Clinical Epidemiology Leiden University Medical Center Capita Selecta 09-12-2014 1 Why RCTs Early 1900: Evidence based on
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
DECLARATION OF CONFLICT OF INTEREST Obstructive sleep apnoea How to identify? Walter McNicholas MD Newman Professor in Medicine, St. Vincent s University Hospital, University College Dublin, Ireland. Potential
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea
 Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;