Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
|
|
|
- Stewart Francis
- 5 years ago
- Views:
Transcription

1 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital
2 Objectives Review pertinent pharmacotherapy common to the critically ill patients Discuss new developments in the pharmacotherapy of critically ill patients Identify relationship between respiratory therapists and pharmacist in the care of critically ill patients


3 What s New? Daily Awakenings ECMO Delirium Vasopressor Selection Tranexamic Acid Sleep Cycles Role of Nutrition Support Intensive Insulin Therapy Choice of Fluid Resuscitation Agent Early Goal Directed Therapy Tidal Volumes Relative Adrenal Insufficiency
4 2 Key Publications Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit Crit Care Med 2013; 41: Update from 2002 guidelines Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Crit Care Med 2013; 41: Update from 2008 guidelines
5 Pain, Agitation, Delirium Guidelines All encompassing for ICU patients Greatly effects both of our jobs As those with experience know it is an art not necessarily a science
6 Pain Incidence Not readily addressed in 2002 guidelines ICU patients routinely experience pain at rest & with care Procedural pain common Specified 2 patient populations Cardiac surgery pain is common & poorly treated More pain in female patients undergoing cardiac surgery Assessment Use vital signs to cue further assessment Utilize valid scoring systems Behavioral Pain Scale (BPS) Critical-Care Pain Observation Tool (CPOT) Crit Care Med 2013; 41:
7 Behavioral Pain Scale Baseline score should be 3 (but studies show it may be 4) Scoring increases during painful procedures (6 7) Anesth Analg 2005;101:
8 Critical-Care Pain Observation Tool
9 Pain Treat It Use preemptive analgesia when possible Prior to painful procedures Intravenous opioids First line for non-neuropathic pain All are effective if titrated appropriately Crit Care Med 2013; 41:
10 Opioid Pharmacology Opiate Onset (IV) Elimination Half-Life Intermittent Dosing Fentanyl IV 1-2 m 2-4 h mcg/kg q h Infusion Rates mcg/kg/hr Comments Less BP Accumulates in fat Chest wall rigidity Hydromorphone IV 5-15 m 2-3 h mg q 1-2 h mg/h Accumulates in renal & liver failure Morphine IV 5-10m 3-4 h 2 4 mg q 1 2 h 2 30 mg/h Accumulates in renal & liver failure Histamine release Methadone IV 1-3d h IV: mg q 6 12h N/A Unpredictable! Remifentanil IV 1-3 m 3-10 m N/A Load 1.5 mcg/kg then mcg/kg/hr Watch dosing in obese pts Crit Care Med 2013; 41:
11 Non-Opioid Pharmacology Opiate Onset (IV) Elimination Half-Life Dosing Comments Ketamine (IV) s 2 3 h mg/kg then mg/kg/h Emergency reactions Hallucinations Acetaminophen PO: m IV: 5 10 m 2 4 h 2 h mg q6h max 4 g/d 1000 mg q 6h max 4 g/d Caution in liver failure Ketorolac IV 10 m 2 9 h mg iv q 6h x max of 5 days Caution in renal failure & bleeding risk Gabapentin (PO) 25 min 1 3 h Start 100 mg q8h & titrate to mg q6h (up to 1200 mg/d) May cause sedation & ataxia Crit Care Med 2013; 41:

12 Sedation Don t just sedate people Attempt to identify underlying cause of anxiety & agitation Pain Delirium Hypoxemia Hypoglycemia Hypotension Alcohol or drug withdrawal Crit Care Med 2013; 41:
13 Sedation Depth: Light = good Assessments Use Richmond Agitation-Sedation Scale (RASS) or Sedation- Agitation Scale (SAS) Objective measuring techniques (Bispectral Index, etc.) Not recommended as primary method of assessment Adjunctive assessments in paralyzed pts or when subjective assessment is unobtainable Use EEG monitoring for seizing pts Crit Care Med 2013; 41:
14 Sedation Pharmacology Agent Onset (IV) Elimination Half-Life Intermittent or loading doses Infusion Rates Midazolam 2 5 m 3 11 h mg/kg mg/kg/h Adverse Effects Respiratory depression Hypotension Lorazepam m 8 15 h mg/kg load mg/kg q 2 6 h prn Diazepam 2 5 m h 5 10 mg load mg/kg q h prn mg/kg/h N/A Respiratory depression Hypotension Respiratory depression Hypotension Propofol 1 2 m Short term: 3 12h Long term: h 1 mg/kg 5 50 mcg/kg/min (or up to 100) Dexmedetomidine 5 10 m h 1 mcg/kg over 10 min mcg/kg/h Lots Hypotension, TG, Acidosis; Pancreatitis.. Bradycardia, hypotension, hypertension with loading dose Crit Care Med 2013; 41:
15 Benzodiazepines Anxiolytic, amnestic, sedating, hypnotic, anticonvulsant effects Highly lipid soluble: diazepam & midazolam Quicker onset Larger volume of distribution Can hang around forever in certain patients Elderly Liver dysfunction Renal dysfunction Crit Care Med 2013; 41:
16 Propofol Sedative, hypnotic, anxiolytic, amnestic, antiemetic, & anticonvulsant effects Quick on, quick off BUT Long term use = saturation of peripheral tissues & prolonged effect Dose dependent hypotension Propofol infusion syndrome Worsening metabolic acidosis, TG, BP, & arrythmias Generally associated with prolonged duration of higher dose (> 70 mcg/kg/min) Crit Care Med 2013; 41:
17 Dexmedetomidine Selective alpha-2 agonist Sedative, analgesic/opioid sparing, & sympatholytic properties Pts are more easily arousal & minimal respiratory depression Often requires higher dosages than general approved dose Crit Care Med 2013; 41:
 to improve clinical outcomes in mechanically ventilated adult ICU patients Class +2B recommendation Crit Care Med 2013;")
18 Sedation Choice We suggest that sedation strategies using nonbenzodiazepine sedatives (either propofol or dexmedetomidine) may be preferred over sedation with benzodiazepines (either midazolam or lorazepam) to improve clinical outcomes in mechanically ventilated adult ICU patients Class +2B recommendation Crit Care Med 2013; 41:
19 Carson et al. Crit Care Med 2006; 34: SEDCOM. JAMA 2009; 301: Data Lorazepam vs. Propofol (Carson et al) Compared duration of ventilation Pts expected to require > 48 hrs ventilation Daily awakenings N=132 pts Lower ventilator days in propofol vs. lorazepam group (5.8 vs. 8.4, p = 0.04) SEDCOM: Dexmedetomidine vs. Midazolam Primary endpoint = % time within RASS -2 to +1 Pts expected to require > 24 hrs ventilation N = 366 pts No difference in time within RASS goal BUT
20 SEDCOM Secondary Objectives Decrease in time to extubation with dexmedetomidine group (1.9 day difference) Dexmedetomidine: 3.7 days [95% CI )] vs. Midazolam: 5.6 days [95% CI ]; p = 0.01 Prevalence of delirium in dexmedetomidine (54%) decreased by 22% vs. midazolam (76/6%) p< JAMA 2009; 301:
21 Cost Analysis for Dexmedetomidine Nested pharmacoeconomic evaluation of SEDCOM Prices used: 200 mcg vial of dexmedetomidine = $58; 5 mg vial of midazolam = $1.50 Median total intensive care unit cost savings of $9679 (CI, $ $17,045) with dexmedetomidine compared with midazolam Primary cost drivers Reduced cost of ICU stay (median savings $6584) Reduced costs of mechanical ventilation (median savings $2958) Crit Care Med 2010; 38;

22 Sedation Conclusions Guidelines exist Most of us don t follow them Data are there but likely need more Change is hard
23 Delirium Syndrome characterized by acute onset of cerebral dysfunction with a change or fluctuation in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness Does not require hallucination or delusions Pts can fluctuate between 2 types Hyperactive: agitated Hypoactive: calm and lethargic Crit Care Med 2013; 41:
24 Delirium Symptoms Disturbed level of consciousness (reduced clarity of awareness of surroundings) Memory deficit Disorientation Language disturbance Perceptual disturbance like hallucinations or delusions Fear Anxiety Anger Depression Apathy Euphoria Crit Care Med 2013; 41:
25 Delirium So What? May affect up to 80% of mechanically ventilated adult ICU pts Costs $ 4 to 16 billion annually in US alone Associated with increase in mortality, prolonged ICU & hospital length of stay We still really don t understand why and how it happens Not great data on how to treat it Crit Care Med 2013; 41:
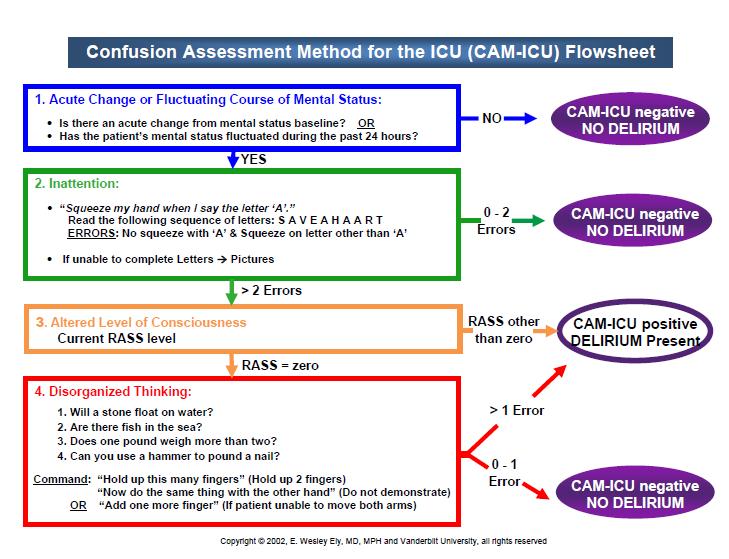
26 Delirium Assessment Most important thing identify it early before it gets too bad Confusion Assessment Method for the ICU (CAM-ICU) Scoring Needs to part of standard ICU assessments Crit Care Med 2013; 41:
27
28 Delirium Prophylaxis No great data exist to recommend pharmacologic agents to prevent delirium Non pharmacologic recommendations Early mobilization & aggressive mobilization Crit Care Med 2013; 41:
29 Delirium Treatment Vitamin H : no published evidence that treatment with haloperidol reduces the duration of delirium in adult ICU patients Atypical antipsychotics may be of use Small study suggests quetiapine may reduce duration of delirium Crit Care Med 2013; 41:
30 Sleep It s a Good Thing We recommend promoting sleep in adult ICU patients Crit Care Med 2013; 41:



31 Current Events ww.cnn.com
32 Normal Circadian Rhythm Wake Inhibition of melatonin release orexin, acetylcholine, serotonin, norepinephrine, dopamine, histamine, adenosine Sleep Diurnal secretion of melatonin adenosine Kamdar BB, et al. J Intensive Care Med. 2012;27(2):
33 Normal Sleep Architecture Normal sleep cycle lasts approximately 90 minutes Continuous cycling between Non-Rapid Eye Movement (NREM) and Rapid Eye Movement (REM) sleep stages Kamdar BB, et al. J Intensive Care Med. 2012;27(2):
34 Normal Sleep Architecture Sleep Stage Description of Sleep Percentage of Total Sleep Stage I (N1) Light 2-5% Stage II (N2) Light 45-55% Slow wave sleep (SWS) Deep sleep 15-20% REM Deep sleep 20-25% Kamdar BB, et al. J Intensive Care Med. 2012;27(2):
")



35 Sleep Disturbances in the Intensive Care Unit (ICU) Noise Critical illness Light Medications Vital signs Mechanical ventilation Laboratory monitoring Gabor JY, et al. Am J RespirCrit Care Med 2003;167:
36 Patient Perception of Sleep Quality in the ICU Freeman NS, et al. Am J Respir Crit Care Med. 1999;159:
37 Consequences of Sleep Deprivation Fatigue, anxiety, impaired cognition and concentration Potential risk factor for development of delirium Increased activation of the hypothalamic-pituitaryadrenal axis Tachycardia, hypertension, increased cortisol Alterations in nitrogen balance, protein catabolism Increased insulin resistance Immune system dysfunction Boyko Y, et al. Acta Anaesthesiol Scand.2012;56(8):950-8.
38 Mechanical Ventilation and Sleep Quality Same alteration of sleep architecture in mechanicallyventilated patients Pressure support vs. pressure assist control Less central apneas improved sleep quality Weaning should occur during daytime hours Non-invasive ventilation Limited studies Cooper AB, et al. Chest 2000;117: Cabello B, et al. Crit Care Med. 2008;36(6): Alexopoulou C, et al. Intensive Care Med. 2013;39: Roche-Camp F, et al. Crit Care Med 2013; 41:
39 Comparison of Sleep and Sedation Similarities Altered sensorium and mentation Muscle hypotonia Temperature dysregulation Disconjugate eye movements Differences with Sleep Spontaneous Rhythmic Essential Reversible with stimuli respiratory rate Kondili E, et al. Intensive Care Med. 2012;38(10):
40 Propofol and Sleep Quality Study Design Inclusion Exclusion Outcomes Randomized, crossover Medical ICU (single center) Mechanical ventilation (assisted modes) > 48 hours, hemodynamic stability, no concomitant sedation or analgesia Glasgow coma scale < 11, APACHE II > 15, presence of delirium, neurologic disease, sleep apnea, sepsis, detectable plasma levels of sedative drugs Sleep architecture using PSG Kondili E, et al. Intensive Care Med. 2012;38(10):
41 Overnight Intervention (20:00 to 07:00) N = 13 Night 1 Night 2 No propofol Propofol mg/kg bolus followed by infusion titrated to Ramsey scale of 3 Kondili E, et al. Intensive Care Med. 2012;38(10):
42 Baseline Characteristics Characteristic Result Male sex, % 50 Age (years), median 73 Admission APACHE II, median 23 Mechanical ventilation (days), median 18 Mechanical ventilation mode, % Pressure support ventilation 84 Continuous positive pressure airway pressure 8 Proportional assist ventilation + 8 Propofol infusion dose, (mcg/kg/min) median 15 Kondili E, et al. Intensive Care Med. 2012;38(10):
43 Sleep Architecture Results Endpoint, median (IQR) No Propofol Propofol p value TST (min) Sleep efficiency (% TST) SWS (% TST) 0 (0-0) 0 (0-5.8) 0.75 REM (% TST) 1.4 (0-13) 0 (0-0) 0.04 Kondili E, et al. Intensive Care Med. 2012;38(10):
44 Influence of Medications on Sleep Quality Medication Sleep latency TST N1, N2 SWS REM Benzodiazepines Propofol - Dexmeditomidine Dopamine antagonists - - Opioid agonists - - Corticosteroids - - Vasopressors Kamdar BB, et al. J Intensive Care Med. 2012;27(2): Hardin KA. Chest.2009;136(1):
45 Treatment of Sleep No great pharmacologic options Utilize non-pharmacologic techniques Ultimately get em out of the unit


46 The Men & Women Keeping Us All Together

47 Conclusions Guidelines exist Change is hard Try to minimize sedation as much as possible Utilize analgesia as first option for treatment Watch for delirium Be mindful of effects of sleep deprivation on patients
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Update on the Management and Monitoring of Deep Analgesia and Sedation in the Intensive Care Unit
 AACN Advanced Critical Care Volume 24, Number 2, pp.101 107 2013, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Update on the Management and Monitoring
AACN Advanced Critical Care Volume 24, Number 2, pp.101 107 2013, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Update on the Management and Monitoring
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Sedative-Hypnotics. Sedative Agents (General Considerations)
") Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES
 WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Sedation For Cardiac Procedures A Review of
 Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOL USE OF PROPOFOL (DIPRIVAN) FOR VENTILATOR MANAGEMENT
 FOR VENTILATOR MANAGEMENT") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOL I. PURPOSE: To provide guidelines for the administration of Propofol, which is an anesthetic agent, indicated for the continuous intravenous
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOL I. PURPOSE: To provide guidelines for the administration of Propofol, which is an anesthetic agent, indicated for the continuous intravenous
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
 Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
SEDATION / ANALGESIA for Brain Failure Patient INASNACC
 SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD
 SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment
 Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Chapter 004 Procedural Sedation and Analgesia
 Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Approach to agitated patient in ICU
 Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Sleep in ICU. Yuliya Boyko, Poul Jennum, Helle Oerding, Palle Toft
 Sleep in ICU Yuliya Boyko, Poul Jennum, Helle Oerding, Palle Toft Background: Why is sleep is important? Modulation of the immune system Regenerative processes Neurophysiological organisation Memory consolidation
Sleep in ICU Yuliya Boyko, Poul Jennum, Helle Oerding, Palle Toft Background: Why is sleep is important? Modulation of the immune system Regenerative processes Neurophysiological organisation Memory consolidation
The Difficult to Sedate ICU Patient
 The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium
 Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline
 Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Sedation and Analgesia in the Critically Ill
 12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Sedation and analgesia in pediatric mechanical ventilation: are we doing it optimally?
 Sedation and analgesia in pediatric mechanical ventilation: are we doing it optimally? Dick Tibboel; Erwin Ista; Nienke Vet; Monique van Dijk Erasmus MC Sophia Children s Hospital Rotterdam, The Netherlands
Sedation and analgesia in pediatric mechanical ventilation: are we doing it optimally? Dick Tibboel; Erwin Ista; Nienke Vet; Monique van Dijk Erasmus MC Sophia Children s Hospital Rotterdam, The Netherlands
Vanderbilt University Medical Center Multidisciplinary Surgical Critical Care
 Vanderbilt University Medical Center Multidisciplinary Surgical Critical Care PROTOCOLIZING AND MONITORING SEDATION, ANALGESIA AND DELIRIUM IN THE CRITICALLY ILL Introduction Critically ill patients are
Vanderbilt University Medical Center Multidisciplinary Surgical Critical Care PROTOCOLIZING AND MONITORING SEDATION, ANALGESIA AND DELIRIUM IN THE CRITICALLY ILL Introduction Critically ill patients are
1
 Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
7/6/ ANNUAL MEETING BRINGING THE ABC(DEF) S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES
 S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES") ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
Pathway to Pain Control
 Pathway to Pain Control Assessing, Preventing, and Managing Pain in the Intensive Care Unit Caitlin S. Brown, PharmD Brianne M. Ritchie, PharmD, MBA, BCCCP, BCPS Pharmacy Grand Rounds November 21, 2017
Pathway to Pain Control Assessing, Preventing, and Managing Pain in the Intensive Care Unit Caitlin S. Brown, PharmD Brianne M. Ritchie, PharmD, MBA, BCCCP, BCPS Pharmacy Grand Rounds November 21, 2017
Preventing Postoperative Cognitive Decline in the Elderly
 Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Preventing Postoperative Cognitive Decline in the Elderly Alex Bekker, M.D., Ph.D Professor and Chair Department of Anesthesiology Rutgers New Jersey Medical School "My brain, that's my second favorite
Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients
 Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients 1 Determine transfer risks as per BC Ambulance Risk Stratification Tool 2 Determine required sedation level accordingly: RASS Level
Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients 1 Determine transfer risks as per BC Ambulance Risk Stratification Tool 2 Determine required sedation level accordingly: RASS Level
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids