KEY REFERENCES Laying the foundation for D of ABCDEF bundle
|
|
|
- Allan Ferguson
- 5 years ago
- Views:
Transcription
1
2 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286: (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27: (ICDSC) Dubois M. Intensive Care Med. 2001;27: (Risk Factors) Ely E. Intensive Care Med. 2001;27: (LOS and Risk Factors) Ely E. JAMA. 2004;291: (Delirium Mortality) Pisani M. Am J Respir Crit Care Med. 2009;180: (Delirium Mortality) Shehabi Y. Crit Care Med. 2010; 38: (Delirium Mortality) Schweickert W. Lancet. 2009;373: (Delirium Reduction) Needham D. Arch Phys Med Rehabil. 2010;91: (Delirium Reduction) Colombo R. Minerva Anestesiol. 2012;78: (Delirium Reduction) Gusmao-Flores D. Crit Care. 2012;16:R115 (Meta-Analysis of Tools) Balas M. Crit Care Med. 2013;42: (Delirium Reduction) Kamdar B. Crit Care Med. 2013;41: (Delirium Reduction)
3 Course Objectives Define delirium and manifestations Discuss the impact of delirium on patient outcomes Review tools to measure delirium Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), Intensive Care Delirium Screening Checklist (ICDSC) Identify strategies to build an ICU attentive to delirium Examine general principles, non-pharmacologic and pharmacologic interventions for the management of delirium


4 Creating a Standard Language

5 Barr J Crit Care Med. 2013;41:


6 Articles Published on Delirium Slide: E Wes Ely, MD Vanderbilt University
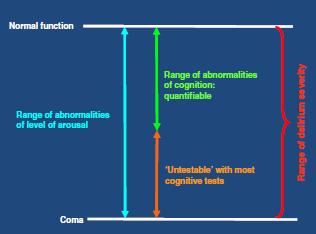
7 Delirium: Key Features (DSM-V) A. Disturbance in attention and awareness B. Disturbance in cognition: e.g., memory, disorientation, language, perception C. Develops over a short period of time and tends to fluctuate during the course of the day D. Disturbances are NOT better explained by a preexisting, established or evolving neurocognitive disorder and do NOT occur in the context of a severely reduced level of arousal such as coma E. There is evidence from the history and physical exam and/or labs that the disturbance is caused by a medical condition, substance intoxication or withdrawal, or medication/toxin side effect American Psychiatric Association. DSM-V. Washington DC; 2013.
 Emotional disturbances (e.g., fear, anger, depression, apathy) Sleep disturbances")
8 Associated but Nondiagnostic Symptoms of ICU Delirium Hallucinations, delusions Abnormal psychometric activity (e.g., agitation, lethargy) Emotional disturbances (e.g., fear, anger, depression, apathy) Sleep disturbances
 Peterson JF J Am Geriat Soc. 2006;54(3):479-484.")
9 Delirium: Motoric Subtypes Combative Agitated Restless Hyperactive Delirium (~1%) Alert and Calm Lethargic Sedated Stupor Hypoactive Delirium (35%) Peterson JF J Am Geriat Soc. 2006;54(3): Mixed Delirium (64%)


10 ICU Delirium: Pathophysiology Cavallazzi R Ann Intensive Care. 2012;2(1):49.
11 Delirium: Epidemiology and Short-Term Outcomes Prevalence 50% to 80% of mechanically ventilated patients 20% to 50% of lower severity patients Associated outcomes Prolonged hospitalization Increased mortality Increased cost Ely E JAMA. 2001;286: Dubois M. Intensive Care Med. 2001;27: Ely E JAMA. 2003;289: Ely E JAMA. 2004;291: Thomason JW. Crit Care. 2005;9:R Milbrandt EB Crit Care Med. 2004; 32:
12 Delirium: Long-Term Outcomes Mortality Each day of delirium in the ICU increases the hazard of 1-year mortality by 10% 1 Cognitive Impairment ICU delirium is an independent risk factor for long-term cognitive impairment 2,3 34% with scores similar to moderate TBI 24% with scores similar to mild Alzheimer disease 1 Pisani MA Am J Respir Crit Care Med. 2009;180: Girard T Crit Care Med.2010;38: Pandharipande PP N Engl J Med. 2013;369(14):
13 PAD Delirium Assessment Recommendations Routinely monitor for delirium in all adult ICU patients (+1B) Use either: Confusion Assessment Method for ICU (CAM-ICU) Intensive Care Delirium Screening Checklist (ICDSC) Barr J Crit Care Med. 2013;41: s
14 Assessment: Coma vs. Delirium Coma: defined by level of arousal SAS 1 or 2, RASS = -4 or -5 Only responsive to physical or noxious stimulus, if at all Unable to communicate Comatose patients should be reassessed over time to permit delirium scoring Scoring is optimal during a patient s maximal level of wakefulness Eligible for delirium when they arouse to verbal stimulus RASS -3: brief eye opening to voice, no contact SAS 3: awakens to verbal stimulus, but drifts off

15 Confusion Assessment Method (CAM, CAM-ICU) Inouye SK Ann Intern Med. 1990;113: Ely E JAMA. 2001;286:

16 CAM-ICU Flowsheet Pooled Test Characteristics: Sensitivity 80% Specificity 96% > 0.91 Figure: Gusmao-Flores D. Crit Care. 2012;16:R115-R125.
17 Intensive Care Delirium Screening Checklist (ICDSC) 1. Altered level of consciousness 2. Inattention 3. Disorientation 4. Hallucination, delusion, or psychosis 5. Psychomotor agitation or retardation 6. Inappropriate speech or mood 7. Sleep/wake cycle disturbances 8. Symptom fluctuation Score 1 point per domain present Delirium if > 4 Pooled Test Characteristics: Sensitivity 74% Specificity 82% > 0.80 Figure: Gusmao-Flores D. Crit Care. 2012;16:R115-R125
18 Screening: Implementation Strategies Case-based scenarios 1 Before-and-after case studies Strategy increased usage of the ICDSC by 70% and accuracy of assessment by 54% Spot-checking 2,3 Systematic comparison of users with expert raters Identifies areas for fine tuning education Get it into the water Incorporate delirium into hospital nursing orientation 1. Devlin JW Crit Care. 2008;12(1):R Pun BT Crit Care Med. 2005;33(6): Soja SL Intensive Care Med. 2008;34(7):
19 Rounding Presentations: Emphasizing Mind and Body Pain Pain controlled or uncontrolled on (current analgesics) Most recent pain score, source of pain (when known) Agitation and Delirium Target RASS/SAS for the day Current RASS/SAS Delirium status Current psychoactive medications Physical Activity Prior level of activity PT/OT consulted Target activity level for the day
20 UCSF RN rounding script
21 Anticipating Delirium: Risk Factors Baseline Vulnerability Underlying brain disease (dementia, stroke, Parkinson) Increased age Institutionalization Chronic disease (HIV, HTN, ETOH dependency, diabetes, etc.) Visual/hearing deficits Precipitants Medications Infection Dehydration Immobility/restraints Malnutrition Tubes/catheters Electrolyte imbalance Sleep deprivation
22 Limits of Evidence: Delirium Prevention Perform early mobilization of adult ICU patients whenever feasible to reduce the incidence and duration of delirium (+1B) No recommendation for Using pharmacologic delirium prevention protocol Using combined nonpharmacologic and pharmacologic delirium prevention protocol as no compelling data demonstrate that these reduce the incidence or duration of delirium (0,C) We do not suggest that either haloperidol or atypical antipsychotics be administered to prevent delirium in adult ICU patients (-2C) We provide no recommendation for the use of dexmedetomidine to prevent delirium in adult ICU patients, as there is no compelling evidence regarding its effectiveness in these patients (O,C) Barr J Crit Care Med. 2013;41:
23 Interventions for Delirium Early mobility and rehabilitation Sleep enhancement (via nonpharm and hygiene) Reducing unnecessary and deliriogenic medications Structured reorientation Adequate oxygenation American Geriatric Society 2014 Guidelines. J Am Geriat Soc. 2016;63(1): Inouye SK N Engl J Med. 1999;340(9): McNamara L. Am J Crit Care. 2008;17:576.
24 Interventions on Delirium Pain management Constipation relief Nutrition and fluid repletion Sensory assistive devices (vision and hearing) Cognitive stimulation/rehabilitation American Geriatric Society 2014 Guidelines. J Am Geriat Soc. 2016;63(1): Inouye SK N Engl J Med. 1999;340(9): McNamara L. Am J Crit Care. 2008;17:576.
25 Wake Up, Breathe, and Exercise Dual center, RCT of 104 sedated, MV patients Both (B) SATs + SBTs for ALL patients Intervention patients If unresponsive, passive range of motion If following commands, PT/OT coordinated with DIS Daily PT/OT until return to independence or hospital discharge Days from intubation to milestone Intervention (n=49) Control (n=54) P value Out of bed <0.001 Standing <0.001 Marching in place <0.001 Transferring to chair <0.001 Ambulating <0.001 Schweickert WD Lancet. 2009; 373:
26 Early Exercise Patient s functional performance improved Independent functional status at hospital discharge: intervention 59% vs. control 35% Shorter duration of MV Substantial reduction in duration of delirium 2 vs. 4 days Schweickert WD Lancet. 2009;373:
27 Delirium and Sleep in the ICU Sleep and delirium Sleep disruption is a manifestation of delirium Sleep deprivation yields delirium Sleep deprivation and fragmentation commonly occur Etiologies: Loss of night-day cues, constant environmental stimuli Pain, sedatives, MV, stress ICU sleep hygiene programs Decrease both incidence and duration of delirium in patients Nighttime sedation sleep promotion Alway AE Am J Crit Care. 2013;22(4): Van Rompaey B Crit Care. 2012;16(3):R73. Kamdar BB Anaesthesia. 2014;69(6): Patel J Anaesthesia. 2014;69(6):
28 ICU Environment, Sleep, and Delirium Daytime Interventions Blinds raised Less than 50% of the day napping Avoid caffeine after 3 PM Nighttime Interventions Before 10 PM Room lights dimmed Room curtain closed Warm bath Unnecessary alarms prevented Room temperature optimized Pain appropriately controlled Television off Result: No difference in perceived sleep quality, but Reductions in delirium/coma incidence (49% vs. 69%) Improved daily noise rating Kamdar BB Crit Care Med. 2014; 41(3):
29 Reorienting ICU Patients Before-after observations in 214 ICU patients Interventions: Night environment, music therapy, visual cues (clock) Reorientation with 5 W s and 1 H Who? Who are you? Who is the nurse/physician? What? What happened? Where? Where are you/we? Why? Why did it happen? How? How did it happen? And what is the illness progression? Result: Delirium incidence reduction Pre 35% vs. post 22% Colombo R Minerva Anestesiol. 2012;78:

30 Bundle Implementation Success: key findings from a meta-analysis 21 studies, all including process measures and 9 with clinical outcomes data
31 Bundle Implementation Success: key findings from a meta-analysis A variety of programs improved process measures e.g., 92% Delirium screening adherence Using more implementation strategies (6 or more) and integrating PAD guidelines or ABCDE bundle: Statistically lower mortality and shorter ICU LOS Delirium incidence static; delirium duration may be better metric Strategies targeting organizational changes in addition to provider behavior also associated with reduced mortality Trogrlić Z. Critical Care 2015; 19:157
32 Helpful Approach to Delirium Management Stop THINK Lastly medicate
33 Helpful Approach to Delirium Management Stop THINK Lastly medicate
34 Reducing Unnecessary Medications STOP: especially consider sedatives Is your patient on the minimal amount necessary? Review medications Doses adjusted for elderly, renal failure, liver failure Do you have a plan to reduce drug exposure? Spontaneous awakening trial Nurse empowerment to titrate drug to a team-determined target level of arousal
35 Delirium Risk Factor: Drug Exposure Measuring the probability of being delirious the next day Result: Drugs have the potential for contributing to delirium Lorazepam particularly susceptible Pandharipande PP Anesthesiology 2006;104:21-26.
36 Helpful Approach to Delirium Management Stop THINK Lastly medicate
37 What to THINK if positive for delirium Toxic Situations Congestive heart failure, shock, dehydration Deliriogenic medications (tight titration) New organ failure (liver, kidney, etc.) Hypoxemia Infection/sepsis (nosocomial), Immobilization Nonpharmacological interventions K+ or electrolyte problems
38 Helpful Approach to Delirium Management Stop THINK Lastly medicate
39 PAD Treatment of Delirium Recommendations There are no published data that treatment with haloperidol reduces the duration of delirium in adult ICU patients (no evidence). Atypical antipsychotics may reduce the duration of delirium in adult ICU patients (C). Barr J Crit Care Med. 2013;41:
40 Antipsychotics and Delirium Unknown efficacy for delirium prevention and management Studies are ongoing Indication: delirium with agitation and risk for self-harm Unresponsive to nonpharmacologic strategies Not proven to aid in delirium prevention/management Ensure agitation not from untreated pain or withdrawal Do no harm Measure QTc interval regularly Avoid when baseline prolongation of QTc or history of torsades Caution with concomitant meds known to prolong the QTc interval Discontinue antipsychotics within 48 hours of delirium resolution Barr J Crit Care Med. 2013;41:
41 Dexmedetomidine and Delirium Multicenter, double-blind RCTs studying dexmedetomidine with delirium as an endpoint. MENDS: dexmedetomidine vs. lorazepam 1 Dex: more combined delirium and coma-free days DEXCOM: dexmedetomidine vs. morphine 2 Dex: shorter duration of delirium SEDCOM: dexmedetomidine vs. midazolam 3 Dex: shorter duration of delirium 1 Pandharipande PP JAMA. 2007;298(22): Shehabi Y Anesthesiology. 2009;111(5): Riker RR JAMA. 2009;301(5):
42 Dexmedetomidine and Delirium In MV patients at risk for developing delirium, dexmedetomidine administered for sedation may be associated with a lower prevalence of delirium compared to benzodiazepine infusions (B). We suggest that sedation strategies using nonbenzodiazepine sedatives (either propofol or dexmedetomidine) may be preferred over sedation with benzodiazepines to improve clinical outcomes in MV patients (+2B). Barr J Crit Care Med. 2013;41:

43 Reducing ICU Delirium Treat pain first! Promote consciousness! Prevent delirium Wean MV Increase mobility Increase patient participation Promote patient recovery Reduce complications Improve patient outcomes* (Photo by Chris Hartlove for The New York Times) *Collinsworth AW J Intensive Care Med Oct 27 [Epub ahead of print].
44 Additional Slides
45
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium
 ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Putting the Pieces of the Puzzle Together: A Journey through ABCDEF
 Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care Kristy Colford- Have No Disclosures ZOOM in & ZOOM
Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care Kristy Colford- Have No Disclosures ZOOM in & ZOOM
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Juliana Barr, MD, FCCM
 Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
7/6/ ANNUAL MEETING BRINGING THE ABC(DEF) S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES
 S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES") ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
What you need to know about Delirium in ICU. Dr Valerie Page Watford General Hospital
 What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
Ohio/Minnesota Collaborative
 Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Ohio/Minnesota Collaborative Place picture here Delirium Prevention Virtual Learning Session February 24, 2016 Delirium collaboration Ohio and Minnesota HENs In December 2015, the Minnesota and Ohio HENS
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Delirium and Falls. Julia Poole CNC Aged Care RNSH
 Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Delirium and Falls Julia Poole CNC Aged Care RNSH Falls Risk Screening Tool Ontario STRATIFY NORTHERN SYDNEY CENTRAL COAST HEALTH Falls Risk Screening - Ontario STRATIFY Please read instructions for use
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Preventing Delirium in the IntensiveCareUnit
 Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
What are Appropriate End-points for Delirium Prevention/Treatment Studies
 What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
What are Appropriate End-points for Delirium Prevention/Treatment Studies Pratik Pandharipande, MD, MSCI Professor of Anesthesiology and Surgery Department of Anesthesiology Vanderbilt University School
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Occurrence of delirium is severely underestimated in the ICU during daily care
 Intensive Care Med (2009) 35:1276 1280 DOI 10.1007/s00134-009-1466-8 BRIEF REPORT Peter E. Spronk Bea Riekerk José Hofhuis Johannes H. Rommes Occurrence of delirium is severely underestimated in the ICU
Intensive Care Med (2009) 35:1276 1280 DOI 10.1007/s00134-009-1466-8 BRIEF REPORT Peter E. Spronk Bea Riekerk José Hofhuis Johannes H. Rommes Occurrence of delirium is severely underestimated in the ICU
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Delirium in the ICU Pamela L. Smithburger, PharmD, MS, BCPS, BCCCP, FCCP Associate Professor, University of School of Pharmacy
 Delirium in the ICU Pamela L. Smithburger, PharmD, MS, BCPS, BCCCP, FCCP Associate Professor, University of Pi@sburgh School of Pharmacy Pa2ent Case JJ is 75 Yo male admi@ed to the MICU on 12/10 with acute
Delirium in the ICU Pamela L. Smithburger, PharmD, MS, BCPS, BCCCP, FCCP Associate Professor, University of Pi@sburgh School of Pharmacy Pa2ent Case JJ is 75 Yo male admi@ed to the MICU on 12/10 with acute
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Confusion Assessment Method for the ICU (CAM-ICU)
") Confusion Assessment Method for the ICU (CAM-ICU) The Complete Training Manual Revised Edition: August 31, 2016 This is a training manual for physicians, nurses and other healthcare professionals who wish
Confusion Assessment Method for the ICU (CAM-ICU) The Complete Training Manual Revised Edition: August 31, 2016 This is a training manual for physicians, nurses and other healthcare professionals who wish
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment
 Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium: How We Can Make a Difference. Denise Kresevic RN, PhD, APN January 2017
 Delirium: How We Can Make a Difference Denise Kresevic RN, PhD, APN January 2017 Disclosure Dr. Kresevic has no actual or potential conflict of interest in relation to this presentation Any views or opinions
Delirium: How We Can Make a Difference Denise Kresevic RN, PhD, APN January 2017 Disclosure Dr. Kresevic has no actual or potential conflict of interest in relation to this presentation Any views or opinions
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,