CMS Reimbursement of CPAP, Oxygen, BPAP, HMV for Sleep Disordered Breathing Peter C Gay Professor of Medicine Mayo Clinic Rochester, MN
|
|
|
- Jonah Hudson
- 5 years ago
- Views:
Transcription

1 45th Annual New Mexico Thoracic Society Lung Disease Symposium CMS Reimbursement of CPAP, Oxygen, BPAP, HMV for Sleep Disordered Breathing Peter C Gay Professor of Medicine Mayo Clinic Rochester, MN

2 Conflicts? Nothing Current
")

3 Objectives You will: Know How to Prescribe PAP + O2 Have Perspective on Current NPPV (RAD) Rules Understand the Dramatic Shift and Difficulties in Current Rules Have Hope for the Future
4 Introduction PAP, PAP and Oxygen What are the differences in indications, and applications for: High level RADS Home Vents How did we get here and why do we need different widgets? Where do we need to get?
5 It s the Law LCD= L33718 Obstructive sleep apnea per Medicare: CPAP will be covered under Medicare in adult patients with OSA if either of the following criteria is met: 1)AHI 15, or 2)AHI 5 and 14 with documented symptoms of excessive daytime sleepiness, impaired cognition, mood disorders or insomnia, or documented hypertension, ischemic heart disease or history of stroke.

6 Oxygen for OSA 6
7 Home Oxygen for Treatment of Obstructive Sleep Apnea (OSA) Medicare does not reimburse for oxygen for OSA Frequently Asked Questions: Oxygen Use in Beneficiaries with Obstructive Sleep Apnea 3/cope23913.htmlprimary treatment of OSA.
8 Oxygen and PAP for OSA & COPD If a new Medicare beneficiary is already on PAP and O2, are both therapies eligible for reimbursement? For PAP: a. The original testing done to diagnose OSA may be used to qualify for Medicare coverage if the results meet or exceed Medicare AHI/RDI requirements; and, b. The 90-day compliance period is replaced with an in-person physician visit that documents (1) compliant use of the equipment and (2) benefit from therapy For Home Oxygen: For beneficiaries who start oxygen while enrolled in a Medicare managed care plan, the blood oxygen testing used by the plan for qualification may be used for qualification purposes by fee-forservice Medicare. 8
9 Oxygen and PAP for OSA & COPD A beneficiary with OSA and chronic, severe lung disease (i.e., COPD) has DAYTIME SpO2 is < 88% and the beneficiary s physician was prescribed home oxygen therapy. In this instance, would home oxygen be covered? Yes, home oxygen would be covered. This beneficiary meets the Oxygen LCD Group I criteria. Oximetry testing while the beneficiary is awake may be used for qualification of home oxygen. While awake OSA does not affect blood oxygen levels. 9
10 Oxygen and PAP for OSA & COPD Patients with OSA and chronic lung disease (e.g. COPD) has a PSG titration that lasted >2 hours and AHI <10/hr with SpO2 <88% for >5 min and oxygen is prescribed in conjunction with PAP. Is this covered? Yes, home oxygen would be covered. The question restates the titration PSG requirements described in the LCDs. A titration PSG meeting these requirements can be used for qualification of home oxygen.

11 Algorithm to Assist in Analyzing OSA/Home Oxygen Testing Scenarios
12 Local Coverage Determination (LCD) for Respiratory Assist Devices (L11504 ) CMS Criteria Categories I. Restrictive Thoracic Disorders II. Severe COPD III. Central Sleep Apnea IV. Hypoventilation Syndromes ssist+devices.pdf/39126d12-28d0-4bc1-8ab8-5f71db06de43 Google: CMS.GOV DME RAD
13 Case 1: History Pt is a 71-yo MWM retired farmer, nonsmoker, who developed a foot drop in 1995 and over the last 6-12 mos. progressive dyspnea, weakness, some choking, 30 lbs. wt. loss, and now uses a walker at home. He naps regularly during the day and regards himself as sleepy. He can lie on his back with the aid of several large pillows but now prefers a recliner and he has never snored.
14 Playing the Game Lab: Abnormal overnight oximetry ABGs= 70/57/7.41 FVC = 45% pred; PiMax = -50 cmh 2 O EMG = Motor neuron disease Diagnosis: ALS, hypersomnolence, nocturnal hypoxemia Must a formal sleep study be done?
15 I. Restrictive Thoracic Disorders A. Documentation in the pt s medical record of progressive neuromuscular disease (e.g., ALS) or a severe thoracic cage abnormality (e.g., post-thoracoplasty for TB), and B. 1. PaCO2, awake, breathing the pt's usual FIO2, is > 45 mmhg, or 2. Sleep oximetry demonstrates O2 saturation < 88% for 5 min, done while breathing the patient s usual FIO2, or 3. For a progressive neuromuscular disease (only), Maximal inspiratory pressure is < -60cm H 2 O or Forced vital capacity is < 50% predicted, and C. Chronic obstructive pulmonary disease does not contribute significantly to the patient s pulmonary limitation
16 Case 2: History Pt is 72-yo WWF, former smoker with severe COPD on home O2, hx. of PAF, hypertension, with 1 recent hospitalization. 3 weeks of progressive dyspnea, worsening cough but no fever or chills. No chest pain or known CAD She never snores but always feels unrested and fatigued. No history of depression or alcohol.
17 Playing the Game Pt admitted to step-down ICU and given NPPV, O2, optimal medications PFTs showed FEV1 of 15% pred ABG the day prior to dismissal: 60/75/7.38 on 2LPM NC-O2 Do you need a sleep study to prescribe home NPPV use?
18 II. Severe COPD: A)1. PaCO2 > 52 mm Hg, on pt s usual FIO2 and, 2. Sleep oximetry demonstrates oxygen saturation <88% for at least 5 minutes, done on O2 at 2 LPM or the pt s usual FIO2 (whichever is higher) and, B) OSA (and CPAP therapy) considered and ruled out- does not require a PSG If all of the above criteria for COPD pts are met, a EO470 device (no backup rate) is covered for first 3 months of therapy and thereafter pending successful reassessment
19 III. Central Sleep Apnea Central sleep apnea (CSA) is defined as: (1) An apnea hypopnea index >5; AND (2) Central apneas/hypopneas >50% of the total apneas/hypopneas; AND (3) Central apneas or hypopneas >5/Hr; AND (4) Symptoms of either excessive sleepiness or disrupted sleep. Complex sleep apnea (CompSA) is a form of central apnea specifically identified by the persistence or emergence of central apneas or hypopneas upon exposure to CPAP or an E0470 device when obstructive events have disappeared. These patients have predominately obstructive or mixed apneas during the diagnostic PSG occurring >5/hour. With use of a CPAP or E0470, they show a pattern of apneas and hypopneas that meets the definition of CSA described above. Revision Effective Date: 01/01/2006
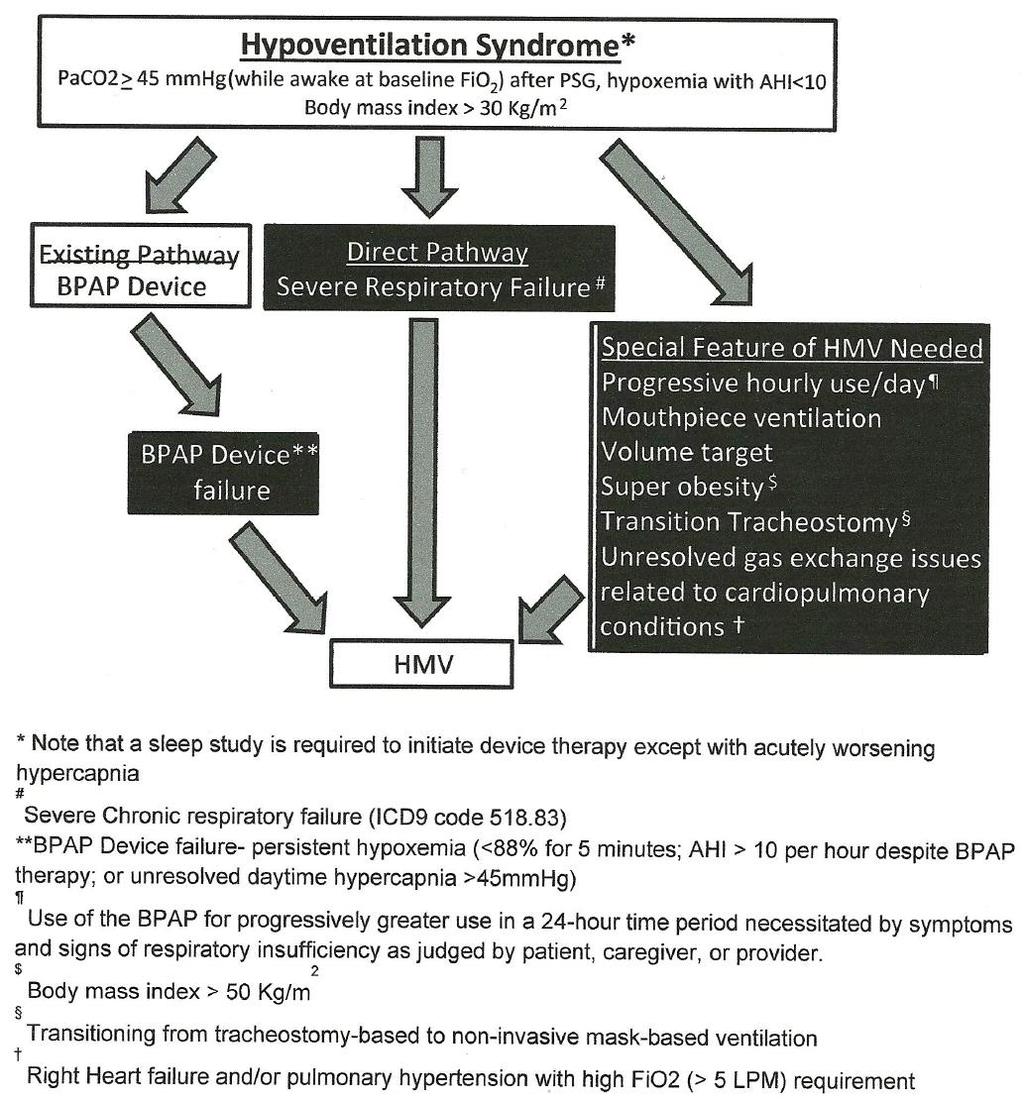
20 IV. Hypoventilation Syndrome An E0471 device is covered for a beneficiary with hypoventilation syndrome if both criteria A, B, and either criterion C or D are met: A. A covered E0470 device is being used. B. Spirometry shows an FEV1/FVC >70%. (Refer to SEVERE COPD (above) for device coverage for FEV1/FVC < 70%).
21 IV. Hypoventilation Syndrome C. An awake PaCO2, while breathing the beneficiary s prescribed FIO2, shows that the beneficiary s PaCO2 worsens greater than or equal to 7 mm HG compared to the ABG result performed to qualify the beneficiary for the E0470 device (criterion A under E0470). D. A facility-based PSG or HST demonstrates oxygen saturation <88% for >5 minutes of nocturnal recording time (minimum recording time of 2 hours) that is not caused by obstructive upper airway events i.e., AHI <5 while using an E0470 device. (Refer to the Positive Airway Pressure Devices LCD for information about E0470 coverage for obstructive sleep apnea.)
22 RADs vs Vents Frequent and Substantial Servicing vs Capped Rental CMS used term therapeutic ventilator without real definition, just as no true definition for a RAD with a backup rate. CMS final regulation 1/27/06 shifted payment for any RADs in frequent and substantial payment category to capped rental Capped rental payment continues 13 mos (mandated by Deficit Reduction Act). Frequent and substantial payment, continues for the time the beneficiary requires the device


23 E0450 LP- 6 PB 2800




24 Retired Ventilators PB-540 LP-10 PLV-100 T-Bird






25 E0463/4 Pulmonetics LTV Series Astral 150

26 Why Do Need So Many Widgets? We Need More Ventilation Scotty? What do you need to ventilate? When does a RAD fail? Is this one or another better? The Needed Aspects for Success More horsepower Special features Mouthpiece and other unique modes Battery backup Alarms and Better Monitoring
27 How Did We Get Here? The problem: Current reimbursement policy creates a disconnect between a patient s clinical status/needs and reimbursement because payment policies focus on devices rather than the clinical situation.
28 How Did We Get Here? FDA approved HMV (home mechanical ventilator) in 1977 focused upon ventilator dependent pediatric pts with a trach. BPAP (Bilevel positive airway pressure) were specifically addressed in the Federal Register and defined as respiratory assist devices or RADs in No distinction made in the Healthcare Common Procedure Coding System (HCPCS) whether or not a backup rate feature was employed. However, effective Jan 1, 1992, code E0453 with wording therapeutic ventilator; suitable for use 12 hours or less per day was added to the HCPCS.
29 How Did We Get Here? Reimbursement ruling was changed to ensure that all BPAPs, even when used as a ventilator with a backup rate, were nevertheless paid as a capped rental item (CR). As later clarified in 2006 in the Federal Register, Ventilators that are excluded from the FSS payment category are paid in accordance with section 1834(a)(7) of the Act under the CR category on a rental basis. This ruling clarified reimbursement policy for BPAPs vs. HMVs, but did not help identify the clinical situations appropriate for FSS or CR equipment
30 How Did We Get Here? Increased acceptance and use of NPPV for management of chronic respiratory failure especially after episode of acute respiratory failure New RCT evidence supporting decreased mortality using NIV with a backup rate for severe COPD with chronic hypercapnic respiratory failure- T Kohnlein et al Lancet 2014 J Lewarski AARC Times Jan 2017
31 How Did We Get Here? Restrictive capped rental RAD policy and barriers to more sophisticated modes especially backup rate feature Changing healthcare models with value-based care initiatives that penalize poor outcomes especially readmission Post-acute bundled payment spawns management teams encouraging NIV use with HMV for COPD protocols

32 The Real Problem
33 The Real Problem In 2015, Medicare expenditures for HMV NIV rose to $343 million 2009, NMD accounted for 56% of claims with chronic respiratory failure at 29% 2015, chronic respiratory failure rose to 85% of E0464 claims while NMD fell to 7%

34 New Vent Codes
35 NAMDRC Working Group Report on the Use of Noninvasive Home Mechanical Ventilation in Adult Patients with Chronic Hypercapnic RF THE AUTHORS- Charles Atwood, MD UPMC, Pittsburgh, PA Joshua Benditt, MD U Washington, Seattle, WA Kent Christopher, MD Denver, Colorado Gerry Criner, MD Temple U, Philadelphia, PA Peter Gay, MD Mayo Clinic, Rochester, MN Nick Hill, MD Tufts U, Boston, MA Sai Parthasarathy, MD U Arizona, Tucson, AZ Lisa Wolfe, MD Northwestern U, Chicago, IL
36 Restrictive Thoracic Disorders Suggested Change: a. An ABG PaCO2 done while awake is >45mm Hg, or b. Sleep oximetry demonstrates SpO2 > 88% for > 5 min of nocturnal recording time (minimum recording time of 30 minutes), or Comment: The change to delete and breathing the beneficiary s prescribed FI02 is discussed below under the Severe COPD section since the rationale is the same for both sections. Insisting upon a demonstration period of 2 hrs desaturation puts patients at undue risk as also discussed below.
37
38 Severe COPD Suggested Change: Patients with COPD must have GOLD Stage 3 or 4 airway obstruction and a PaCO2 done while awake is > 52 mmhg. Comment: Recent evidence, especially from the Kohnlein study, supports the hypercapnia requirement. Chronic CO2 retainers appear to be the group most likely to benefit. There should be no stipulation about the FIO2 with the ABG as the issue at hand is about ventilation and not oxygenation. Based on our comments below, we recommend deleting criterion B and covering both E0470 and E0471 if the remaining two criteria are met. Contingent upon such revisions, situations 1 and 2 currently used to justify coverage of an E0471 device should be removed in their entirety.
39 NAMDRC COPD Working Group Report Recommended Revised Algorithm for NIV via HMV in COPD SEVERE COPD ABG while awake breathing usual FiO 2 demonstrates PaCO 2 > 52 mmhg Prescribe BPAP Successfully achieve ven la on goals Con nue BPAP Failure on a BPAP Device Progressively increased hours of nocturnal and diurnal use/need for ba ery backup/volume targeted modes Enhanced alarm requirement Ini ate HMV
40 Central or Complex Sleep Apnea If all of the above criteria are met, either an E0601, E0470 or an E0471 device (based upon the judgment of the treating physician) will be covered for beneficiaries with documented CSA or CompSA for the first three months of therapy. Comment: The recent findings from the SERVE-HF trial 10 surprisingly identified the fact the patients with symptomatic CHF with reduced LV function in fact had a higher mortality with the previously preferred E071 device adaptive servo-ventilator. This limits alternative therapy for central apnea in these patients based on current American Academy of Sleep Medicine guidelines to oxygen and CPAP (E0601) which is not permitted presently.
41 Hypoventilation Syndrome Suggested Change: An initial PACO2 done while awake is > 45 mm Hg. Comment: As with the COPD discussion above, criteria should not force oxygen therapy on the patient when assessing hypercapnia Current Language: Spirometry shows an FEV1/FVC >70%. Suggested Change: Spirometry shows an FEV1/FVC > 70%. (Refer to SEVERE COPD (above) for information about device coverage for beneficiaries with FEV1/FVC <70%). This also includes patients with parenchymal lung disease leading to restriction AND hypercapnia that do not meet the criteria for the first category, Restrictive Thoracic Disease.
42
43 Home Mechanical Ventilation, Respiratory Failure and Coverage Criteria Recommendations On June 29, 2001, CMS issued a Decision Memo (CAG N) to the DME MACs regarding the role of Respiratory Assist Devices (RADs) and the need for a backup rate for patients with severe COPD. In part, the memo stated that noninvasive mechanical ventilation is distinguished from the invasive ventilation administered via a securely intubated airway, in a patient for whom interruption or failure of respiratory support leads to death.



44 LCD ID- L33800 Original ICD-9 LCD ID- L11504 LCD Title= Respiratory Assist Devices
45 LCD ID- L33800 Original ICD-9 LCD ID- L11504 LCD Title= Respiratory Assist Devices VENTILATOR WITH NOINVASIVE INTERFACES The Centers for Medicare & Medicaid Services (CMS) National Coverage Determinations Manual (Internet-Only Manual, Publ ) in Chapter 1, Part 4, Section stipulates that ventilators (E0450, E0460-E0464) are covered for the following conditions: Neuromuscular diseases, thoracic restrictive diseases, and chronic respiratory failure consequent to chronic obstructive pulmonary disease. Each of these disease categories are comprised of conditions that can vary from severe and life-threatening to less serious forms. These disease groups may appear to overlap conditions described in the Respiratory Assist Devices LCD but they are not overlapping. Choice of an appropriate device i.e., a ventilator versus a bi-level PAP device is made based upon the severity of the condition. CMS distinguished the use of respiratory product types in a National Coverage Analysis Decision Memo (CAG-00052N) in June 2001 saying that RAD is distinguished from ventilation in a patient for whom interruption or failure of respiratory support leads to death.
46 LCD ID- L33800 Original ICD-9 LCD ID- L11504 LCD Title= Respiratory Assist Devices VENTILATOR WITH NOINVASIVE INTERFACES The conditions described in the Respiratory Assistance Devices (RAD) local coverage determination are not life-threatening conditions where interruption of respiratory support would quickly lead to serious harm or death. These policies describe clinical conditions that require intermittent and relatively short durations of respiratory support. Thus, any type ventilator would not be eligible for reimbursement for any of the conditions described in the RAD LCD even though the ventilator equipment may have the capability of operating in a bi-level PAP (E0470, E0471) mode. Bi-level PAP devices (E0470, E0471) are considered as reasonable and necessary in those clinical scenarios. Claims for ventilators (E0450, E0460-E0464) used for the treatment of conditions described in the RAD LCD will be denied as not reasonable and necessary.
47 NAMDRC Working Group Report on the Use of Noninvasive Home Mechanical Ventilation in Adult Patients with Chronic Hypercapnic RF The purpose of this document is to review available evidence and provide expert consensus opinion regarding the use of home non-invasive mechanical ventilation in adults, attempting to describe different clinical scenarios that dictate the need for different levels of ventilator assistance and support.
48 Definitions: Respiratory Failure Respiratory Failure: Respiratory failure is the inability of the respiratory system to maintain gas exchange within normal limits. The degree of respiratory failure may range from mild to severe with the severity determining the urgency and extent of treatment. It is generally divided into 2 forms: Oxygenation failure inability to maintain PaO 2 of 60 mm Hg or greater on room air and, Ventilatory failure inability to maintain PaCO 2 of 50 mm Hg or below
49 Definitions: Respiratory Failure Definitions: Mechanical Ventilator andmechanical Ventilation Mechanical Ventilator: A mechanical ventilator is a device capable of delivering pressurized gas (either through a secured artificial airway or through a mask or mouthpiece) in a manner that repeatedly supplies a physiological tidal volume to the lungs sufficient to improve or fully sustain respiration. Mechanical Ventilation: Mechanical ventilation is the use of a mechanical ventilator on a patient in whom interruption or failure of this device can reasonably be expected to lead to eventual or rapid clinical deterioration leading to medical harm or even death.
50 Establishment of Distinct Categories of Mechanically Ventilated Patients 1. Create a distinct category for use of a mechanical ventilator 16 hours/day or greater 2. Create a distinct category for use of a mechanical ventilator greater than nocturnally alone or approximately > 8 hours, but<16 hrs/24 hrs. 3. Create a distinct category for use of a mechanical ventilator (bi level device, or RAD) just nocturnally or up to 8 hours /24 hrs.
51 Conclusions Evidence based outcome data supports use of backup rate and high IPAP in severe COPD HMV devices offer many advantages but expense is significantly greater with little scientific information available regarding clinical practice DME MAC determination essentially terminates non-invasive HMV use for all pts unless severe or life-threatening documentation
52 Conclusions The landscape will certainly drastically change for NPPV patients and possibly even for those with a tracheostomy when HMV treatment plans are sought NAMDRC BOD is presently crafting a response plan possibly including a legislative approach to appropriately address this immense barrier to proper patient care
THE WALTER O DONOHUE MEMORIAL LECTURE
 THE WALTER O DONOHUE MEMORIAL LECTURE TYPES OF HOME MECHANICAL VENTILATION: WHEN IS IT REALLY A VENTILATOR? PETER C. GAY, MD PROFESSOR OF MEDICINE MAYO MEDICAL SCHOOL ROCHESTER, MN PETER C. GAY, MD, is
THE WALTER O DONOHUE MEMORIAL LECTURE TYPES OF HOME MECHANICAL VENTILATION: WHEN IS IT REALLY A VENTILATOR? PETER C. GAY, MD PROFESSOR OF MEDICINE MAYO MEDICAL SCHOOL ROCHESTER, MN PETER C. GAY, MD, is
Policy Specific Section: October 1, 2010 January 21, 2013
 Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Respiratory Assist Device E0470:
 Respiratory Assist Device E0470: Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION IN SUPPLIER S FILE All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order obtained
Respiratory Assist Device E0470: Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION IN SUPPLIER S FILE All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order obtained
RESPIRATORY ASSIST DEVICE E0470
 JURISDICTIONS B &C Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the
JURISDICTIONS B &C Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the
RESPIRATORY ASSIST DEVICE E0471
 JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
RESPIRATORY ASSIST DEVICE E0471
 JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
Helpful hints for filing
 Helpful hints for filing Respiratory Assist Devices HCPCS Code E0470 E0471 Overview The following information describes the Durable Medical Equipment Medicare Administrative Contractors' (DME MACs) medical
Helpful hints for filing Respiratory Assist Devices HCPCS Code E0470 E0471 Overview The following information describes the Durable Medical Equipment Medicare Administrative Contractors' (DME MACs) medical
Medicare C/D Medical Coverage Policy. Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders
 Medicare C/D Medical Coverage Policy Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January,
Medicare C/D Medical Coverage Policy Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January,
New Government O2 Criteria and Expert Panel. Jennifer Despain, RPSGT, RST, AS
 New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
April 22, Dear Ms. Syrek Jensen:
 April 22, 2015 Ms. Tamara Syrek Jensen Director Coverage and Analysis Group Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244: Dear Ms. Syrek Jensen: On behalf of the
April 22, 2015 Ms. Tamara Syrek Jensen Director Coverage and Analysis Group Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, MD 21244: Dear Ms. Syrek Jensen: On behalf of the
Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment
 Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment Judith R. Fischer, MSLS, Editor, Ventilator-Assisted Living (fischer.judith@sbcglobal.net) Thanks to Josh Benditt, MD, University
Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment Judith R. Fischer, MSLS, Editor, Ventilator-Assisted Living (fischer.judith@sbcglobal.net) Thanks to Josh Benditt, MD, University
Cues for Coding & Coverage
 Cues for Coding & Coverage Last Updated: September, 2010 www.medgroup.com Table of Contents Introduction 1 Testing Specifications 1 Initial Coverage Criteria 2 Upgrades 4 Continued Coverage 5 RAD Replacements
Cues for Coding & Coverage Last Updated: September, 2010 www.medgroup.com Table of Contents Introduction 1 Testing Specifications 1 Initial Coverage Criteria 2 Upgrades 4 Continued Coverage 5 RAD Replacements
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Medics Home Health Services 1075 South Main St. Ste. 450 Madison, GA P F
 Medics Home Health Services 1075 South Main St. Ste. 450 Madison, GA 30650 706-342-9236 P 706-342-0079 F Medicare Coverage Criteria for DME WE HAVE THIS AVAILBIE IN DIGITAL FORM IF YOU D PREFER LET US
Medics Home Health Services 1075 South Main St. Ste. 450 Madison, GA 30650 706-342-9236 P 706-342-0079 F Medicare Coverage Criteria for DME WE HAVE THIS AVAILBIE IN DIGITAL FORM IF YOU D PREFER LET US
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Name of Policy: Noninvasive Positive Pressure Ventilation
 Name of Policy: Noninvasive Positive Pressure Ventilation Policy #: 203 Latest Review Date: April 2014 Category: Durable Medical Equipment Policy Grade: Effective July 31, 2013: Active Policy but no longer
Name of Policy: Noninvasive Positive Pressure Ventilation Policy #: 203 Latest Review Date: April 2014 Category: Durable Medical Equipment Policy Grade: Effective July 31, 2013: Active Policy but no longer
Medicare CPAP/BIPAP Coverage Criteria
 Medicare CPAP/BIPAP Coverage Criteria For any item to be covered by Medicare, it must 1) be eligible for a defined Medicare benefit category, 2) be reasonable and necessary for the diagnosis or treatment
Medicare CPAP/BIPAP Coverage Criteria For any item to be covered by Medicare, it must 1) be eligible for a defined Medicare benefit category, 2) be reasonable and necessary for the diagnosis or treatment
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea
 Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
NIPPV FOR THE HYPERCAPNIC COPD AND OBSESITY HYPOVENTILATION PATIENT
 NIPPV FOR THE HYPERCAPNIC COPD AND OBSESITY HYPOVENTILATION PATIENT Gaurav Singh, MD Stanford University Associate Professor Saturday, January 19, 2019 3:20 p.m. 4:00 p.m. Gaurav Singh, MD, completed all
NIPPV FOR THE HYPERCAPNIC COPD AND OBSESITY HYPOVENTILATION PATIENT Gaurav Singh, MD Stanford University Associate Professor Saturday, January 19, 2019 3:20 p.m. 4:00 p.m. Gaurav Singh, MD, completed all
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea
 Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO
11/20/2015. Beyond CPAP. No relevant financial conflicts of interest. Kristie R Ross, M.D. November 12, Describe advanced ventilation options
 Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
Itamar Medical 2016 Reimbursement Coding Guide
 Itamar Medical 2016 Reimbursement Coding Guide Continuous positive airway pressure (CPAP) and associated devices for Obstructive Sleep Apnea (OSA) DISCLAIMER: The information contained in this guide is
Itamar Medical 2016 Reimbursement Coding Guide Continuous positive airway pressure (CPAP) and associated devices for Obstructive Sleep Apnea (OSA) DISCLAIMER: The information contained in this guide is
Home Mechanical Ventilation:
 Home Mechanical Ventilation: A Global A Global View View Nicholas Hill MD Tufts Medical Center Boston MA Nicholas S Hill MD Tufts Medical Center Boston, MA Disclosures Research Grants MAB Breathe Technologies
Home Mechanical Ventilation: A Global A Global View View Nicholas Hill MD Tufts Medical Center Boston MA Nicholas S Hill MD Tufts Medical Center Boston, MA Disclosures Research Grants MAB Breathe Technologies
OSA and COPD: What happens when the two OVERLAP?
 2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
Reasons Providers Use Bilevel
 Reasons Providers Use Bilevel More comfort, improve therapy compliance Noncompliant OSA (NCOSA) 1 Scripts from lab referrals Central/Complex Sleep Apnea 2 For ventilations needs Restrictive Thoracic Disorders/Neuromuscular
Reasons Providers Use Bilevel More comfort, improve therapy compliance Noncompliant OSA (NCOSA) 1 Scripts from lab referrals Central/Complex Sleep Apnea 2 For ventilations needs Restrictive Thoracic Disorders/Neuromuscular
MEDICARE Quick Reference Guide. Reimbursement Guidelines for Referral Sources
 MEDICARE Quick Reference Guide Reimbursement Guidelines for Referral Sources What s inside? Face-to-Face Rules Patient Lifts/Lift Chairs/ Commodes Support Surfaces and Beds Mobility Equipment Non-invasive
MEDICARE Quick Reference Guide Reimbursement Guidelines for Referral Sources What s inside? Face-to-Face Rules Patient Lifts/Lift Chairs/ Commodes Support Surfaces and Beds Mobility Equipment Non-invasive
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
MEDICAL POLICY. SUBJECT: POSITIVE AIRWAY PRESSURE DEVICES: CPAP, BiPAP, APAP AND NONINVASIVE POSITIVE PRESSURE VENTILATORS
 MEDICAL POLICY SUBJECT: POSITIVE AIRWAY PRESSURE DEVICES: CPAP, BiPAP, APAP AND (DELETED: 07/16/09-04/28/11) PAGE: 1 OF: 10 If a product excludes coverage for a service, it is not covered, and medical
MEDICAL POLICY SUBJECT: POSITIVE AIRWAY PRESSURE DEVICES: CPAP, BiPAP, APAP AND (DELETED: 07/16/09-04/28/11) PAGE: 1 OF: 10 If a product excludes coverage for a service, it is not covered, and medical
Average volume-assured pressure support
 Focused review Average volume-assured pressure support Abdurahim Aloud MD Abstract Average volume-assured pressure support (AVAPS) is a relatively new mode of noninvasive positive pressure ventilation
Focused review Average volume-assured pressure support Abdurahim Aloud MD Abstract Average volume-assured pressure support (AVAPS) is a relatively new mode of noninvasive positive pressure ventilation
Challenging Cases in Pediatric Polysomnography. Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep
 Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
MEDICAL POLICY. SUBJECT: POSITIVE AIRWAY PRESSURE DEVICES: CPAP, BiPAP, APAP AND NONINVASIVE POSITIVE PRESSURE VENTILATORS
 MEDICAL POLICY SUBJECT: POSITIVE AIRWAY PRESSURE DEVICES: CPAP, BiPAP, APAP AND (DELETED: 07/16/09-04/28/11) PAGE: 1 OF: 9 If a product excludes coverage for a service, it is not covered, and medical policy
MEDICAL POLICY SUBJECT: POSITIVE AIRWAY PRESSURE DEVICES: CPAP, BiPAP, APAP AND (DELETED: 07/16/09-04/28/11) PAGE: 1 OF: 9 If a product excludes coverage for a service, it is not covered, and medical policy
Oxygen and Oxygen Equipment
 Oxygen and Oxygen Equipment Policy Number: Original Effective Date: MM.01.008 12/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 08/25/2017 Section: DME Place(s) of Service:
Oxygen and Oxygen Equipment Policy Number: Original Effective Date: MM.01.008 12/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 08/25/2017 Section: DME Place(s) of Service:
Corporate Medical Policy
 Corporate Medical Policy Noninvasive Respiratory Assist Devices File Name: Origination: Last CAP Review: Next CAP Review: Last Review: noninvasive_respiratory_assist_devices 12/2009 2/2017 2/2018 2/2017
Corporate Medical Policy Noninvasive Respiratory Assist Devices File Name: Origination: Last CAP Review: Next CAP Review: Last Review: noninvasive_respiratory_assist_devices 12/2009 2/2017 2/2018 2/2017
RESPIRATORY EQUIPMENT AND SUPPLIES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 RESPIRATORY EQUIPMENT AND SUPPLIES CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 RESPIRATORY EQUIPMENT AND SUPPLIES Table of Contents 36.1 Enrollment......................................................................
RESPIRATORY EQUIPMENT AND SUPPLIES CSHCN SERVICES PROGRAM PROVIDER MANUAL APRIL 2018 CSHCN PROVIDER PROCEDURES MANUAL APRIL 2018 RESPIRATORY EQUIPMENT AND SUPPLIES Table of Contents 36.1 Enrollment......................................................................
PEDIATRIC PAP TITRATION PROTOCOL
 PURPOSE In order to provide the highest quality care for our patients, our sleep disorders facility adheres to the AASM Standards of Accreditation. The accompanying policy and procedure on pediatric titrations
PURPOSE In order to provide the highest quality care for our patients, our sleep disorders facility adheres to the AASM Standards of Accreditation. The accompanying policy and procedure on pediatric titrations
2/13/2018 OBESITY HYPOVENTILATION SYNDROME
 OBESITY HYPOVENTILATION SYNDROME David Claman, MD UCSF Professor of Medicine Director, UCSF Sleep Disorders Center Disclosures: None. 1 COMPLICATIONS OF OSA Cardiovascular HTN, CHF, CVA, arrhythmia, Pulm
OBESITY HYPOVENTILATION SYNDROME David Claman, MD UCSF Professor of Medicine Director, UCSF Sleep Disorders Center Disclosures: None. 1 COMPLICATIONS OF OSA Cardiovascular HTN, CHF, CVA, arrhythmia, Pulm
CPAP. The CPAP will be covered
 CPAP CPAP Did your patient have a face to face visit with the physician prior to having a sleep study that documented (1) Sleep History and symptoms and/or (2) Epworth Scale and/or (3) Physical Examination?
CPAP CPAP Did your patient have a face to face visit with the physician prior to having a sleep study that documented (1) Sleep History and symptoms and/or (2) Epworth Scale and/or (3) Physical Examination?
Complex Sleep Apnea. Can we do better? David Weed D.O.,FCCP,FAASM. September 8, 2016
 Complex Sleep Apnea Can we do better? David Weed D.O.,FCCP,FAASM September 8, 2016 If you don t know where you are going, you ll end up somewhere else. Yogi Berra Objectives Discuss what syndromes comprise
Complex Sleep Apnea Can we do better? David Weed D.O.,FCCP,FAASM September 8, 2016 If you don t know where you are going, you ll end up somewhere else. Yogi Berra Objectives Discuss what syndromes comprise
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
DECISION AND ORDER. After due notice, a telephone hearing was held on. , Medical Director, also testified as a witness for the MHP.
 STATE OF MICHIGAN MICHIGAN ADMINISTRATIVE HEARING SYSTEM FOR THE DEPARTMENT OF HEALTH AND HUMAN SERVICES P.O. Box 30763, Lansing, MI 48909 (517) 373-0722; Fax: (517) 373-4147 IN THE MATTER OF:, MAHS Docket
STATE OF MICHIGAN MICHIGAN ADMINISTRATIVE HEARING SYSTEM FOR THE DEPARTMENT OF HEALTH AND HUMAN SERVICES P.O. Box 30763, Lansing, MI 48909 (517) 373-0722; Fax: (517) 373-4147 IN THE MATTER OF:, MAHS Docket
Medical Affairs Policy
 Medical Affairs Policy Service: Sleep Disorder Treatment: Positive Airway Pressure Devices and Oral Appliances (CPAP, BPAP, BiPAP, BiPAP ST, BiPAP with backup, BiPAP -Auto SV, VPAP, VPAP Adapt, VPAP adapt
Medical Affairs Policy Service: Sleep Disorder Treatment: Positive Airway Pressure Devices and Oral Appliances (CPAP, BPAP, BiPAP, BiPAP ST, BiPAP with backup, BiPAP -Auto SV, VPAP, VPAP Adapt, VPAP adapt
Mechanical Ventilation of the Patient with Neuromuscular Disease
 Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Chronic NIV in heart failure patients: ASV, NIV and CPAP
 Chronic NIV in heart failure patients: ASV, NIV and CPAP João C. Winck, Marta Drummond, Miguel Gonçalves and Tiago Pinto Sleep disordered breathing (SDB), including OSA and central sleep apnoea (CSA),
Chronic NIV in heart failure patients: ASV, NIV and CPAP João C. Winck, Marta Drummond, Miguel Gonçalves and Tiago Pinto Sleep disordered breathing (SDB), including OSA and central sleep apnoea (CSA),
Sleep & Respiratory. Qualifying Criteria Guidebook
 Sleep & Respiratory Qualifying Criteria Guidebook Sleep & Respiratory Qualifying Criteria Guidebook Respiratory Therapy Services & Equipment Respiratory Care Practitioners at HME are industry top performers
Sleep & Respiratory Qualifying Criteria Guidebook Sleep & Respiratory Qualifying Criteria Guidebook Respiratory Therapy Services & Equipment Respiratory Care Practitioners at HME are industry top performers
Sleep Apnea: Diagnosis and Treatment
 Coverage Summary Sleep Apnea: Diagnosis and Treatment Policy Number: S-003 Products: UnitedHealthcare Medicare Advantage Plans Original Approval Date: 08/23/2007 Approved by: UnitedHeatlhcare Medicare
Coverage Summary Sleep Apnea: Diagnosis and Treatment Policy Number: S-003 Products: UnitedHealthcare Medicare Advantage Plans Original Approval Date: 08/23/2007 Approved by: UnitedHeatlhcare Medicare
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea
 Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
Positive Airway Pressure and Oral Devices for the Treatment of Obstructive Sleep Apnea Policy Number: Original Effective Date: MM.01.009 11/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO;
Oxygen and Oxygen Equipment
 Oxygen and Oxygen Equipment Policy Number: Original Effective Date: MM.01.008 12/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 09/01/2013 Section: DME Place(s) of Service: Home I.
Oxygen and Oxygen Equipment Policy Number: Original Effective Date: MM.01.008 12/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 09/01/2013 Section: DME Place(s) of Service: Home I.
TOPIC: Continuing Coverage of CPAP Machines and Supplies for the Treatment of Obstructive Sleep Apnea
 These documents are not used to determine benefits or reimbursement. Please reference the appropriate certificate or contract for benefit information. BLUE CROSS BLUE SHIELD of MI MEDICAL POLICY Enterprise:
These documents are not used to determine benefits or reimbursement. Please reference the appropriate certificate or contract for benefit information. BLUE CROSS BLUE SHIELD of MI MEDICAL POLICY Enterprise:
Respiratory Equipment and Supplies
 Respiratory Equipment and Supplies Chapter.1 Enrollment..................................................................... -2.2 Benefits, Limitations, and Authorization Requirements...........................
Respiratory Equipment and Supplies Chapter.1 Enrollment..................................................................... -2.2 Benefits, Limitations, and Authorization Requirements...........................
Positive Airway Pressure (PAP) Devices Physician Frequently Asked Questions December 2008
 Devices Physician Frequently Asked Questions December 2008") Positive Airway Pressure (PAP) Devices Physician Frequently Asked Questions December 2008 Based on questions received from the clinical community, the following Frequently Asked Questions will address
Positive Airway Pressure (PAP) Devices Physician Frequently Asked Questions December 2008 Based on questions received from the clinical community, the following Frequently Asked Questions will address
Any device utilized for this procedure must have FDA approval specific to the indication, otherwise it will be considered investigational.
 Non-invasive Positive Pressure Ventilators (In-Home Use) DESCRIPTION A non-invasive positive pressure ventilator (NIPPV) provides ventilatory support through a non-invasive interface, such as a nasal mask,
Non-invasive Positive Pressure Ventilators (In-Home Use) DESCRIPTION A non-invasive positive pressure ventilator (NIPPV) provides ventilatory support through a non-invasive interface, such as a nasal mask,
Oxygen and Oxygen Equipment
 Oxygen and Oxygen Equipment I. Policy University Health Alliance (UHA) will reimburse for home oxygen and oxygen equipment when it is determined to be medically necessary and when it meets the medical
Oxygen and Oxygen Equipment I. Policy University Health Alliance (UHA) will reimburse for home oxygen and oxygen equipment when it is determined to be medically necessary and when it meets the medical
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acquired central hypoventilation syndrome, NPPV in children with, 475 Acute cardiogenic pulmonary edema, PAP therapy in, 394 395 Adaptive
Index Note: Page numbers of article titles are in boldface type. A Acquired central hypoventilation syndrome, NPPV in children with, 475 Acute cardiogenic pulmonary edema, PAP therapy in, 394 395 Adaptive
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
(HST) (95806, G0398, G0399)
 (95806, G0398, G0399)") 95800 Sleep study, unattended, simultaneous recording of, heart rate, oxygen saturation, respiratory analysis (e.g. by airflow or peripheral arterial tone), and sleep time 95801 Sleep study, unattended,
95800 Sleep study, unattended, simultaneous recording of, heart rate, oxygen saturation, respiratory analysis (e.g. by airflow or peripheral arterial tone), and sleep time 95801 Sleep study, unattended,
COMPLEX SLEEP APNEA IS IT A DISEASE? David Claman, MD UCSF Sleep Disorders Center
 COMPLEX SLEEP APNEA IS IT A DISEASE? David Claman, MD UCSF Sleep Disorders Center CENTRAL APNEA Central Apnea Index > 5 ( >50% of apnea are central) Mayo Clinic Proc 1990; 65:1255 APNEA AT SLEEP ONSET
COMPLEX SLEEP APNEA IS IT A DISEASE? David Claman, MD UCSF Sleep Disorders Center CENTRAL APNEA Central Apnea Index > 5 ( >50% of apnea are central) Mayo Clinic Proc 1990; 65:1255 APNEA AT SLEEP ONSET
Monitoring: gas exchange, poly(somno)graphy or device in-built software?
graphy or device in-built software?") Monitoring: gas exchange, poly(somno)graphy or device in-built software? Alessandro Amaddeo Noninvasive ventilation and Sleep Unit & Inserm U 955 Necker Hospital, Paris, France Inserm Institut national
Monitoring: gas exchange, poly(somno)graphy or device in-built software? Alessandro Amaddeo Noninvasive ventilation and Sleep Unit & Inserm U 955 Necker Hospital, Paris, France Inserm Institut national
Jurisdiction B, C and D Combined Council Questions Sorted by A-Team May, 2015
 A CMS Medicare Administrative Contractor http://www.ngsmedicare.com Jurisdiction B, C and D Combined Council Questions Sorted by A-Team May, 2015 Disclaimer: This Q&A document is not an official publication
A CMS Medicare Administrative Contractor http://www.ngsmedicare.com Jurisdiction B, C and D Combined Council Questions Sorted by A-Team May, 2015 Disclaimer: This Q&A document is not an official publication
CERT PAP Errors: The DME CERT Outreach and Education Task Force Responds
 CERT PAP Errors: The DME CERT Outreach and Education Task Force Responds DME CERT Outreach and Education Task Force National PAP Webinar, December 17, 2014 PAP CERT Errors Medical Records: Face-to-Face
CERT PAP Errors: The DME CERT Outreach and Education Task Force Responds DME CERT Outreach and Education Task Force National PAP Webinar, December 17, 2014 PAP CERT Errors Medical Records: Face-to-Face
Sleep 101. Kathleen Feeney RPSGT, RST, CSE Business Development Specialist
 Sleep 101 Kathleen Feeney RPSGT, RST, CSE Business Development Specialist 2016 Why is Sleep Important More than one-third of the population has trouble sleeping (Gallup) Obstructive Sleep Apnea Untreated
Sleep 101 Kathleen Feeney RPSGT, RST, CSE Business Development Specialist 2016 Why is Sleep Important More than one-third of the population has trouble sleeping (Gallup) Obstructive Sleep Apnea Untreated
Interdisciplinary Care of the Patient with Amyotrophic Lateral Sclerosis Respiratory Therapy Care
 Peggy Cox, RRT, RN Frazier Rehab Institute Pulmonary Rehab Interdisciplinary Care of the Patient with Amyotrophic Lateral Sclerosis Respiratory Therapy Care Disclosure I have the following relevant financial
Peggy Cox, RRT, RN Frazier Rehab Institute Pulmonary Rehab Interdisciplinary Care of the Patient with Amyotrophic Lateral Sclerosis Respiratory Therapy Care Disclosure I have the following relevant financial
A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation
 1 A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation The following 3 minute polysomnogram (PSG) tracing was recorded in a 74-year-old man with severe ischemic cardiomyopathy
1 A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation The following 3 minute polysomnogram (PSG) tracing was recorded in a 74-year-old man with severe ischemic cardiomyopathy
Polysomnography and Sleep Studies
 Polysomnography and Sleep Studies Policy Number: Original Effective Date: MM.02.016 09/14/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2014 Section: Medicine Place(s)
Polysomnography and Sleep Studies Policy Number: Original Effective Date: MM.02.016 09/14/2004 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2014 Section: Medicine Place(s)
How to write bipap settings
 How to write bipap settings 6-6-2013 Living On O2 for Life If you use a bipap machine, like I do, this post is for you. I've been using a bipap machine since 1993 which is a pretty long time. BiPAP 's
How to write bipap settings 6-6-2013 Living On O2 for Life If you use a bipap machine, like I do, this post is for you. I've been using a bipap machine since 1993 which is a pretty long time. BiPAP 's
Rebecca Mason. Respiratory Consultant RUH Bath
 NIV in motor neurone disease Rebecca Mason Respiratory Consultant RUH Bath NIV in motor neurone disease Why does MND affect the Respiratory System? Should NIV be offered to patients with MND? If so when?
NIV in motor neurone disease Rebecca Mason Respiratory Consultant RUH Bath NIV in motor neurone disease Why does MND affect the Respiratory System? Should NIV be offered to patients with MND? If so when?
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT
, RPSGT") BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center
 FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Approved By: CLINICAL MEDICAL POLICY Noninvasive Positive Pressure Intermittent Ventilation in the Home Setting MP-002-MD-WV Medical Management Provider Notice Date: 04/01/2018;
Policy Name: Policy Number: Approved By: CLINICAL MEDICAL POLICY Noninvasive Positive Pressure Intermittent Ventilation in the Home Setting MP-002-MD-WV Medical Management Provider Notice Date: 04/01/2018;
Do Not Cite. For Public Comment Period DRAFT MEASURE #3: Evaluation of Pulmonary Status Ordered MUSCULAR DYSTROPHY
 MEASURE #3: Evaluation of Pulmonary Status Ordered MUSCULAR DYSTROPHY Measure Description All patients diagnosed with a muscular dystrophy who had a pulmonary status evaluation* ordered. Measure Components
MEASURE #3: Evaluation of Pulmonary Status Ordered MUSCULAR DYSTROPHY Measure Description All patients diagnosed with a muscular dystrophy who had a pulmonary status evaluation* ordered. Measure Components
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Approved By: CLINICAL MEDICAL POLICY Noninvasive Positive Pressure Intermittent Ventilation in the Home Setting MP-002-MD-DE Medical Management Provider Notice Date: 04/15/2018;
Policy Name: Policy Number: Approved By: CLINICAL MEDICAL POLICY Noninvasive Positive Pressure Intermittent Ventilation in the Home Setting MP-002-MD-DE Medical Management Provider Notice Date: 04/15/2018;
About VirtuOx. Was marketed exclusively by Phillips Healthcare division, Respironics for 3 years
 About VirtuOx VirtuOx, Inc. assists physicians and Durable Medical Equipment (DME)( companies diagnose respiratory diseases and qualify patients for home respiratory equipment under the guidelines of CMS
About VirtuOx VirtuOx, Inc. assists physicians and Durable Medical Equipment (DME)( companies diagnose respiratory diseases and qualify patients for home respiratory equipment under the guidelines of CMS
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Airway Clearance Devices
 Print Page 1 of 11 Wisconsin.gov home state agencies subject directory department of health services Search Welcome» August 2, 2018 5:18 PM Program Name: BadgerCare Plus and Medicaid Handbook Area: Durable
Print Page 1 of 11 Wisconsin.gov home state agencies subject directory department of health services Search Welcome» August 2, 2018 5:18 PM Program Name: BadgerCare Plus and Medicaid Handbook Area: Durable
LCD for Positive Airway Pressure (PAP) Devices for the Treatment of Obstructive Sleep Apnea (L171)
 Devices for the Treatment of Obstructive Sleep Apnea (L171)") Page 1 of 20 LCD for Positive Airway Pressure (PAP) Devices for the Treatment of Obstructive Sleep Apnea (L171) Contractor Name Noridian Administrative Services Contractor Number 19003 Contractor Type
Page 1 of 20 LCD for Positive Airway Pressure (PAP) Devices for the Treatment of Obstructive Sleep Apnea (L171) Contractor Name Noridian Administrative Services Contractor Number 19003 Contractor Type
Oral Appliances for Obstructive Sleep Apnea Response to Comments
 Oral Appliances for Obstructive Sleep Apnea Response to Comments November 11, 2010 1. There are no randomized, controlled crossover trials that show efficacy of any prefabricated oral appliance. As the
Oral Appliances for Obstructive Sleep Apnea Response to Comments November 11, 2010 1. There are no randomized, controlled crossover trials that show efficacy of any prefabricated oral appliance. As the
Preventing Respiratory Complications of Muscular Dystrophy
 Preventing Respiratory Complications of Muscular Dystrophy Jonathan D. Finder, MD Professor of Pediatrics University of Pittsburgh School of Medicine Children s Hospital of Pittsburgh Introduction Respiratory
Preventing Respiratory Complications of Muscular Dystrophy Jonathan D. Finder, MD Professor of Pediatrics University of Pittsburgh School of Medicine Children s Hospital of Pittsburgh Introduction Respiratory
Non-Invasive Ventilation
 Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
Case 1. Level of difficulty: 2/5
 Case 1 Level of difficulty: 2/5 Summary Settings in the ventilator BULBAR ALS Ventilation 24h/24, Good tolerance PaO2 82; PaCO2 : 42, ph=7,42 (under ventilation) Mode: S/T Main parameters : Pressure Support
Case 1 Level of difficulty: 2/5 Summary Settings in the ventilator BULBAR ALS Ventilation 24h/24, Good tolerance PaO2 82; PaCO2 : 42, ph=7,42 (under ventilation) Mode: S/T Main parameters : Pressure Support
QUESTIONS FOR DELIBERATION
 New England Comparative Effectiveness Public Advisory Council Public Meeting Hartford, Connecticut Diagnosis and Treatment of Obstructive Sleep Apnea in Adults December 6, 2012 UPDATED: November 28, 2012
New England Comparative Effectiveness Public Advisory Council Public Meeting Hartford, Connecticut Diagnosis and Treatment of Obstructive Sleep Apnea in Adults December 6, 2012 UPDATED: November 28, 2012
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Coding for Sleep Disorders Jennifer Rose V. Molano, MD
 Practice Coding for Sleep Disorders Jennifer Rose V. Molano, MD Accurate coding is an important function of neurologic practice. This section of is part of an ongoing series that presents helpful coding
Practice Coding for Sleep Disorders Jennifer Rose V. Molano, MD Accurate coding is an important function of neurologic practice. This section of is part of an ongoing series that presents helpful coding
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด
 Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Understanding Breathing Muscle Weakness
 Understanding Breathing Muscle Weakness A N D R E A L. K L E I N P R E S I D E N T / F O U N D E R B R E A T H E W I T H M D w w w.facebook.com/ b r e a t h e w i t h m d h t t p : / / w w w. b r e a t
Understanding Breathing Muscle Weakness A N D R E A L. K L E I N P R E S I D E N T / F O U N D E R B R E A T H E W I T H M D w w w.facebook.com/ b r e a t h e w i t h m d h t t p : / / w w w. b r e a t
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
Respiratory Management of Facioscapulohumeral Muscular Dystrophy. Nicholas S. Hill, MD Tufts Medical Center Boston, MA
 Respiratory Management of Facioscapulohumeral Muscular Dystrophy Nicholas S. Hill, MD Tufts Medical Center Boston, MA Respiratory Involvement in FSHD Very variable time of onset rate of progression Muscles
Respiratory Management of Facioscapulohumeral Muscular Dystrophy Nicholas S. Hill, MD Tufts Medical Center Boston, MA Respiratory Involvement in FSHD Very variable time of onset rate of progression Muscles
In-Patient Sleep Testing/Management Boaz Markewitz, MD
 In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
Premier Health Plan considers Oral Appliances for Obstructive Sleep Apnea (OSA) medically necessary for the following indications:
 medically necessary for the following indications:") Premier Health Plan POLICY AND PROCEDURE MANUAL MP.063.PH - al Appliances for Obstructive Sleep Apnea This policy applies to the following lines of business: Premier Commercial Premier Employee Premier
Premier Health Plan POLICY AND PROCEDURE MANUAL MP.063.PH - al Appliances for Obstructive Sleep Apnea This policy applies to the following lines of business: Premier Commercial Premier Employee Premier
Auto Servo Ventilation Indications, Basics of Algorithm, and Titration
 Auto Servo Ventilation Indications, Basics of Algorithm, and Titration 1 ASV Learning Objectives Understand the indications for Auto Servo Ventilation Differentiate obstructive versus central hypopneas
Auto Servo Ventilation Indications, Basics of Algorithm, and Titration 1 ASV Learning Objectives Understand the indications for Auto Servo Ventilation Differentiate obstructive versus central hypopneas
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Enclosed on Page 5 is an authorization form to release your health information.
 Monitor Medical, Inc. "The CPAP Co." Ph: (877) 569-9436 Fax: (888) 773-2854 www.monitormedical.com Dear Medicare Beneficiary: Thank you for selecting Monitor Medical, Inc. to provide you with all of your
Monitor Medical, Inc. "The CPAP Co." Ph: (877) 569-9436 Fax: (888) 773-2854 www.monitormedical.com Dear Medicare Beneficiary: Thank you for selecting Monitor Medical, Inc. to provide you with all of your
All About Positive Airway Pressure (PAP) Therapy
 Therapy") All About Positive Airway Pressure (PAP) Therapy Nitipatana Chierakul Division of Respiratory Disease and Tuberculosis, Department of Medicine, Siriraj Medical School Siriraj Sleep Center: Fiscal-year
All About Positive Airway Pressure (PAP) Therapy Nitipatana Chierakul Division of Respiratory Disease and Tuberculosis, Department of Medicine, Siriraj Medical School Siriraj Sleep Center: Fiscal-year
High Flow Nasal Cannula in Children During Sleep. Brian McGinley M.D. Associate Professor of Pediatrics University of Utah
 High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
 Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting Lisa F. Wolfe MD Northwestern University Chicago, Illinois Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting Lisa F. Wolfe MD Northwestern University Chicago, Illinois Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting