Hepatocellular Carcinoma
|
|
|
- Dorthy Clark
- 5 years ago
- Views:
Transcription
1 Hepatocellular Carcinoma Derek Jonker, MD FRCPC Medical Oncologist, The Ottawa Hospital October 4, 2015 Conflict of Interest Disclosure Remuneration: none Research support: none beyond direct costs running trials. Indirect salary support: none 1

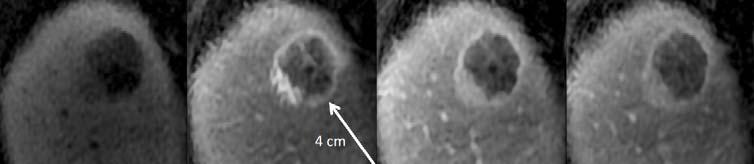
2 Case Study 52 year old 2001 Hematemesis; esophageal varices Banding U/S liver fatty liver, cirrhosis Hep B/C serology negative Dec 2012 U/S 5.9cm mass liver Jan 2013 MRI liver 6cm liver mass HCC Invasion of tumour into portal vein AFP 15,000 Case Study No contrast Arterial Venous/Delayed 2

3 Case Study March 2013 Biopsy liver hepatocellular ca Started sorafenib 400mg po bid Case Study AFP Sorafenib x24 months déc. 01, 12 janv. 01, 13 févr. 01, 13 mars 01, 13 avr. 01, 13 mai 01, 13 juin 01, 13 juil. 01, 13 août 01, 13 sept. 01, 13 oct. 01, 13 nov. 01, 13 déc. 01, 13 janv. 01, 14 févr. 01, 14 mars 01, 14 avr. 01, 14 mai 01, 14 juin 01, 14 juil. 01, 14 août 01, 14 sept. 01, 14 oct. 01, 14 nov. 01, 14 déc. 01, 14 janv. 01, 15 févr. 01, 15 mars 01, 15 avr. 01, 15 mai 01, 15 juin 01, 15 juil. 01, 15 août 01, 15 sept. 01, 15 Baseline 18 months later 3
, drop AFP Long control Jan 2015 two angry skin lesions on leg Bx keratoacanthoma Rising AFP Feb 2015 stop Rx Case Questions: What surveillance should")
4 Case Study Sorafenib 400mg po bid Diarrhea, high blood pressure. Dose reduction Unusually good response (PR), drop AFP Long control Jan 2015 two angry skin lesions on leg Bx keratoacanthoma Rising AFP Feb 2015 stop Rx Case Questions: What surveillance should cirrhotic patients have for HCC? How useful is AFP as a tumour marker? What is required to diagnose HCC? What scan to order? What is LiRADS? What are the treatment options for HCC? 4





5 Worldwide variation in HCC Worldwide 750,000 new cases annually 5th most common cancer, 3rd leading cancer death Hot spots: sub Saharan Africa, East Asia 9.2% of all cancers Case fatality ratio 96% in developing countries El Serag, et al. Gastroenterology 132(7): , 2007 Aflatoxin is produced by the Aspergillus fungus Grows on food such as corn, peanuts, pistachios in warm damp conditions Binds to DNA and can cause p53 mutation Synergistic with viral hepatitis, 60x risk if HBV infection 5
6 Hepatitis B Virus Responsible for 55% of HCC worldwide 400 million people infected Transmission 90% vertical transmission (maternal/newborn) in endemic areas In Canada is mostly sexual or parenteral Responsible for 85% of HCC in ethnic Chinese Men 3:1 HCC in Canada Lifetime probability of developing liver cancer is 0.8% for men, 0.3% for women Predominantly age >60 yrs 5-year overall survival 20% (only lung, esophagus and pancreas are worse) 6
7 Fastest increasing Incidence 2.4% per year for 10 years El Serag, et al. Gastroenterology 132(7): , 2007 Canadian Cancer Statistics Toronto, ON: Canadian Cancer Society;
8 HCC: Etiology Cirrhosis EtOH HCV 65% of HCC in Canada HBV Remaining 35%? NASH Rare: Hereditary hemochromatosis A-1 anti-trypsin Autoimmune hepatitis Porphyria Hepatitis C 170 million infected worldwide Vertical transmission In Canada immigrants, iv drug users, transfusion before ,000 infected in BC chronic infection leads to cirrhosis in 25% Interval infection to HCC 20+ years Curable 8

9 Harvoni : Ledipasvir + Sofosbuvir Randomized trials 12 week treatment, once daily 99% sustained virologic response Covered in most provinces E.g. EAP in Ontario $1000 per pill $84K Afdhal et al, NEJM 370(20): , 2014 Holkira Pak : Paritaprevir, ombiasvir, dasabuvir, ritonavir 3 pills per day % cure in genotype 1 Add ribavirin if genotype 1a or or 1b $56,000 for a 12 week course 9

10 Let me play the fool; With mirth and laughter let old wrinkles come, And let my liver rather heat with wine, than my heart cool with mortifying groans. Gratiano, Merchant of Venice Alcohol: Too much? Cirrhosis: Heavy for prolonged periods g per day OR X ½ bottle 5% x 341ml x3 = 51g HCC only if cirrhosis, no independent carcinogenic effect Synergistic effect if concomitant viral hepatits 13.5% x 750ml = 101g 10

11 Obesity Aside from immigration, the factor most responsible for the rise in HCC in Canada is obesity. Rise in obesity in NA has closely matched the rise in the incidence of HCC. Elevated BMI has a pronounced effect on relative risk of HCC in men. BMI>30 doubles your risk and BMI>35 quadruples the risk. This effect is not seen nearly as much in women Calle et al, NEJM 2003 Metabolic Syndrome in Canada, Statistics Canada [ 11
12 Obesity Metabolic Syndrome Non Alcoholic Fatty Liver Disease (NAFLD) Non Alcoholic Steatohepatitis (NASH) NASH cirrhosis Accumulation of fatty acids and glucose in the liver increases TNF a, NFK b, EGF, leptin NASH associated HCC now as frequent as HCV HCC NASH associated HCC New HCC: Evaluation for etiology History: iv drugs? Transfusion before 1992? EtOH? Prior hepatitis? Diabetic or metabolic syndrome Lab: anti-hcv Ab (prior infection) HBsAg (ongoing infection), HBsAb (prior infection/immunity) 12

13 Rare causes: work up Autoimmune hepatitis Female > male Associated autoimmune disorders: Celiac, IBD, Graves, Hashimoto s, GN, SLE sclerosing cholangitis, type I DM, RhA, Sjogren s Anti smooth muscle Ab, anti nuclear Ab Hereditary hemochromatosis Fasting transferrin saturation Evaluate further if >45% for males, >35% in women Ferritin only specific if >1000ng/mL Mutations: C282Y and H63D Other: MRI to measure iron, liver biopsy Alpha 1 antitrypsin deficiency Lung disease (emphysema) by age 50 Often unrecognized; 1/3000 of European descent; rare in Asians Genetic test SERPINA1 mutations Screening in cirrhotics? U/S every 6 months Further evaluation of any lesion > 1cm with either triphasic CT or dynamic contrast enhanced MRI AASLD guidelines, Canadian Consensus Guideline Meta-analysis [Aliment Pharmacol Ther Jul;30(1):37-47] Detect HCC at any stage Pooled sensitivity 94%, specificity 94% Detect HCC at early stage: sensitivity 63% higher sensitivity with U/S every 6 months (70%) than annual (50%); P =
14 AFP? Combining with U/S for screening does not improve detection Sensitivity 60% at level of 20ng/mL But, 20% of cirrhotics have level >20ng/mL 90% false positives Sensitivity 22% at level of 200ng/mL Useful as surrogate for response to treatment if >200 at baseline. AFP response better predictor of survival than ORR, ECOG PS, T-stage, or Childs-Pugh Riaz et al, JCO 2009 Diagnosis: Biopsy vs DI? Biopsy 2% risk of tumour seeding 10% false negative rate Non-invasive diagnostic standard: Li-RADs Liver Imaging Reporting and Data System 5 categories Li-RADS5-100% specific Forner et al Hepatology 2008» Sensitivity only 33% for lesions <2cm LiRAD4 only 80%(?) HCC follow or biopsy 14

15 Diagnosis of HCC Li-RADs By 4-phase CT or Dynamic contrast enhanced MRI Must record arterial and venous phases Threshold growth def: >100% (>6mos), >50% (<6mos), or new Capsule: noted in portal venous or delayed images What is Li-RADS5 Must have arterial enhancement Three additional factors: Growth Venous washout Capsule Li-RAD5 if 2cm+ and one of above 1-2cm and two of above 15





16 A B C 16
17 Child Pugh Classification 1 point 2 points 3 points INR < >2.3 Albumin (g/l) > <28 Bilirubin ( mol/l) < >50 Ascites (clinical) Absent Slight or diuretic controlled Score range 5 to 15 Childs A = 5 6 (ie maximum one risk) B = 7 9 C = (end stage liver disease) Moderate Encephalopathy None Mild Moderate HCC Management Solitary <2cm, Childs A 1-3 nodules <3cm (Milan Criteria) Larger or >3 nodules Childs-Pugh C PS >2 Fit Age <70 Comorbidities Age >70 Liver limited, Childs A/B Childs-Pugh A N+ or M+ Portal v inv TACE TACE Resect (or RFA) Transplant RFA TACE Sorafenib Palliation Adapted from the Barcelona-clinic liver cancer staging system 17
18 Milan criteria Score to predict risk of recurrence of HCC following liver transplant Criteria: single tumors 5 cm in diameter or no more than three tumors 3 cm in diameter 83% RFS at 26months 75% OS at 4 years Mazzaferro, NEJM 1996 Priority for Transplant: The MELD score Model for End Stage Liver Disease (MELD) system Score from 6 (less ill) to 40 (gravely ill) determines how urgently patient needs liver transplant within next 3 months MELD calculation: MELD = 3.78 ln[ min(1,bili/17.2)] ln[min(1,inr)] ln[min(1,cr/ 88.4)] MELD and mortality MELD score 3 month mortality Time on wait list? 40 71% Some transplant prioritization schemes also include 3 points for each 3 months % a patient is on the wait list % While you wait % TACE <10 1.9% More TACE 18
19 RFA (Radiofrequency Ablation) Heat 57 o C coagulative necrosis Percutaneous with local (conscious sedation), outpatient Criteria: Unresectable <3cm No extra-hepatic disease No vascular inv No adjacent loops bowel Childs A-B Post ablation zone is larger than initial lesion radiologist needs to know about ablation to interpret scan Post-ablation Nausea + pain post-op, resolve in 4 hrs flu-like symptoms x5d (fever, malaise) Bleeding 1%, seeding <1%, abscess 1%, diaphragmatic burn, Local control 80% Chemotherapy Typically low response rates Doxorubicin 0-15% Doxo/5FU/Methyl-CCNU 19% Doxo/bleo 16% Etoposide 13-18% Cisplatin 1% Absence of benefit in randomized trials 19

20 TACE: Arterial Chemoembolization HCC single blood supply hepatic artery Rest of liver protected Dual supply Chemotherapy agent Cisplatin (Not available) Doxorubicin 60-75mg/m2 Embolizing agent Lipiodol, gelfoam 55 vs 25% 2yOS HR % Childs A, 30% Childs B Average 3 sessions of TACE Llovet et al, Lancet 2 20
 upper gastrointestinal bleeding; 3% (0-22%) hepatic or splenic abscess, 1.3% (0-2.5%) treatment-related mortality 2.4% (0-9.5%) mainly due to acute liver failure.")
21 TACE: Toxicities Pain, fever, fatigue acute liver failure, 7.5% (range 0-49%) encephalopathy, 1.8% (0-16%) ascites, 8.3% (0-52%) acute renal failure, 1.8% (0-13%) upper gastrointestinal bleeding; 3% (0-22%) hepatic or splenic abscess, 1.3% (0-2.5%) treatment-related mortality 2.4% (0-9.5%) mainly due to acute liver failure. TACE: Doxo vs Drug Eluting-Beads? DC-BEADs bead loaded with doxorubicin Bead trapped in capillary, slowly releases doxo Lower systemic release of chemo Several small RCTs Less transaminitis, less abd pain No difference survival Cost driving choice of TACE Doxorubicin 100mg $420 DCBEADS $3000 Sacco et al, J Vasc Interven Radiol 2011 Golferi et al, BJC
22 TACE vs TEA? (Transarterial Ethanol Ablation) Lipiodol-ethanol mixture Ethanol causes arteriole endothelial damage Induces embolization Small comparative trials No difference in survival No concerns for anthracycline systemic toxicity (eg cardiac history) Very reasonable alternative Probably cheapest Sorafenib Sorafenib (Nexavar, Bayer HealthCare) Inhibits RAF, VEGRF, PDGR SHARP Trial Advanced HCC, Child-Pugh A, 92% ECOG 0-1 Sorafenib 400mg bid Placebo 22

 Weight loss (9 vs 1%) Diarrhea (39 vs 11% Alopecia (14")
 Hypertension (5 vs 2%) Abdominal pain (8 vs 3%) Rare: keratoacanthoma,")
23 SHARP Trial 97% Childs-Pugh A ORR 2 vs 1% mos 10.7 vs 7.9 months HR 0.69, p< yOS 44vs 33% Llovet et al, NEJM 20 Toxicity: Sorafenib toxicity Anorexia (14 vs 3%) Weight loss (9 vs 1%) Diarrhea (39 vs 11% Alopecia (14 vs 2%) Dry skin (8 vs 4%) Hand Foot reaction (21 vs 3%) Voice change (6 vs 1%) Hypertension (5 vs 2%) Abdominal pain (8 vs 3%) Rare: keratoacanthoma, SqCellCa Management Symptomatic (e.g. imodium), dose reduce (eg BID 200 QD) 23
 Not fundable PCODR Sorafenib as an adjuvant?")
24 Sorafenib for Childs-Pugh B? No RTC evidence N=297 consecutive patients, A+B Much worse outcome for CP-B Toxicity no different mos 10 vs 3.8 months (A vs B) Not fundable PCODR Sorafenib as an adjuvant? STORM trial evaluated post resection/ablation Sorafenib vs Placebo to maximum 4 years Results: No difference in RFS, OS More toxicity with sorafenib Bruix et al, ASCO
25 Special considerations Thrombocytopenia Some improvement with splenectomy or splenic embolization. Value? Variceal bleeding Non cardio-selective beta-blocker (eg propranolol) banding Ascites control Diuretics Pleurx catheter What s New? PD-1 cmet 25

26 Nivolumab and Immune Checkpoint Inhibition Nivolumab is a fully human IgG4 anti PD 1 monoclonal Ab that blocks interaction between PD 1 and PD L1/PD L2, restoring T cell immune activity directed against the tumour cell. Topailian et al, NEJM 2012 PD-1 / PD-L1 in HCC Upregulation of PD-1 and PD-L1 poor prognostic factors Phase I/II study HCC Inclusion: HCV, HBV and non-infected Child-Pugh A+B (no ascites or encephalopathy) Failed (68%) or refused sorafenib RD2DL: Nivolumab 10mg/kg q2 weeks ORR 19% (14% PR, CR 5%) 75% of these ongoing El-Koueiry, ASCO



27 Nivolumab in HCC El-Koueiry, ASCO 2015 El-Koueiry, ASCO 27


28 <br />MET as a Prognostic Factor Presented By Ghassan Abou-Alfa at 2015 ASCO Annual Meeting Presented By Ghassan Abou-Alfa at 2015 ASCO Annual Meeting 28

29 Phase III Cabozantinib vs Placebo NCT Presented By Ghassan Abou-Alfa at 2015 ASCO Annual Meeting High-cMET expressor subgroup 7.2 vs 3.8 months mos HR 0.38, p=0.01 Trivantinib Placebo 29
 Transplant RFA TACE Sorafenib Palliation Nivolumab,")
30 Phase III Tivantinib vs Placebo NCT Presented By Ghassan Abou-Alfa at 2015 ASCO Annual Meeting HCC Management Solitary <2cm, Childs A 1-3 nodules <3cm (Milan Criteria) Larger or >3 nodules Childs-Pugh C PS >2 Fit Age <70 Comorbidities Age >70 Liver limited, Childs A/B Childs-Pugh A N+ or M+ Portal vein inv TACE TACE Resect (or RFA) Transplant RFA TACE Sorafenib Palliation Nivolumab, Tivantinib, Cabozantinib Adapted from the Barcelona-clinic liver cancer staging system 30
31 Questions 31
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Tumor incidence varies significantly, depending on geographical location.
 Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC
: Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC") Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
End Stage Liver Disease & Disease Specific Indications for Liver Transplant. Susan Kang, RN, MSN, ANP-BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS?
 IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting?
 Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 )
") 蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 ) 1 Sorafenib Improves Survival in Hepatocellular Carcinoma: Results of a Phase III Randomized, -Controlled Trial Josep M. Llovet, Sergio Ricci, Vincenzo Mazzaferro, Philip
蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 ) 1 Sorafenib Improves Survival in Hepatocellular Carcinoma: Results of a Phase III Randomized, -Controlled Trial Josep M. Llovet, Sergio Ricci, Vincenzo Mazzaferro, Philip
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Hepatocellular Carcinoma (HCC)
") Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT
 HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT INTRODUCTION: Hepatocellular carcinoma (HCC): Fifth most common cancer worldwide Third most common cause of cancer mortality In Egypt: 2.3%
HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT INTRODUCTION: Hepatocellular carcinoma (HCC): Fifth most common cancer worldwide Third most common cause of cancer mortality In Egypt: 2.3%
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HCA
 UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Nexavar in advanced HCC: a paradigm shift in clinical practice
 Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
Study Objective and Design
 Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
3/22/2017. I will be discussing off label/investigational use of tivantinib for hepatocellular carcinoma.
 Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Surveillance for HCC Who, how Diagnosis of HCC Surveillance for HCC in Practice
 Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Hepatocellular carcinoma in Sri Lanka - where do we stand?
 SCIENTIFIC ARTICLE Hepatocellular carcinoma in Sri Lanka - where do we stand? R.C. Siriwardana 1, C.A.H. Liyanage 1, M.B. Gunethileke 2 1. Specialist Gastrointestinal and Hepatobilliary Surgeon, Senior
SCIENTIFIC ARTICLE Hepatocellular carcinoma in Sri Lanka - where do we stand? R.C. Siriwardana 1, C.A.H. Liyanage 1, M.B. Gunethileke 2 1. Specialist Gastrointestinal and Hepatobilliary Surgeon, Senior
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. Valle J et al. N Engl J Med 2010;362(14):
:") Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Screening for HCCwho,
 Screening for HCCwho, how and how often? Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital HCC Global Epidemiology
Screening for HCCwho, how and how often? Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital HCC Global Epidemiology
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Hepatocellular Carcinoma (HCC): Burden of Disease
: Burden of Disease") Hepatocellular Carcinoma (HCC): Burden of Disease Blaire E Burman, MD VM Hepatology Hepatocellular Carcinoma (HCC) Primary HCCs most often arise in the setting of chronic inflammation, liver damage, and
Hepatocellular Carcinoma (HCC): Burden of Disease Blaire E Burman, MD VM Hepatology Hepatocellular Carcinoma (HCC) Primary HCCs most often arise in the setting of chronic inflammation, liver damage, and
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval
 12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
Hepatocellular Carcinoma: Transplantation, Resection or Ablation?
 Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Hepatocellular Carcinoma
 Hepatocellular Carcinoma Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Louisville & Louisville VAMC 2010 Magnitude of the Problem 95% of
Hepatocellular Carcinoma Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Louisville & Louisville VAMC 2010 Magnitude of the Problem 95% of
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Professor Norbert Bräu
 Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Professor Norbert Bräu James J Peters VA Medical Center, New York, USA COMPETING INTEREST
Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Professor Norbert Bräu James J Peters VA Medical Center, New York, USA COMPETING INTEREST
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
SEQUENCING OF HCC TREATMENT. Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA
 SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
Latest Developments in the Treatment of Hepatocellular Carcinoma
 Latest Developments in the Treatment of Hepatocellular Carcinoma Roniel Cabrera, MD MS Associate Professor of Medicine Director of Hepatology and Medical Director of Liver Transplantation Division of Gastroenterology,
Latest Developments in the Treatment of Hepatocellular Carcinoma Roniel Cabrera, MD MS Associate Professor of Medicine Director of Hepatology and Medical Director of Liver Transplantation Division of Gastroenterology,
Outline. Updates in the Clinical Management of Hepatitis B and C. Who should be screened for HBV? Chronic Hepatitis B 10/7/2018
 Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Il treatment plan nella terapia sistemica dell epatocarcinoma
 Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Liver and Biliary Tract Cancers Critical Review
 Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC
 SATELLITE SYMPOSIUM Emerging Horizons in HCC: From Palliation to Cure RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC Professor Riccardo Lencioni, MD, FSIR, EBIR University of Pisa School of Medicine,
SATELLITE SYMPOSIUM Emerging Horizons in HCC: From Palliation to Cure RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC Professor Riccardo Lencioni, MD, FSIR, EBIR University of Pisa School of Medicine,
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Dr David Rowbotham NHS. The Leeds Teaching Hospitals. NHS Trust
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Il Tumore del Fegato Prospettive Future nel Trattamento dei Tumori Gastrointestinali
 Il Tumore del Fegato Prospettive Future nel Trattamento dei Tumori Gastrointestinali Lorenza Rimassa Medical Oncology Unit Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Disclosures
Il Tumore del Fegato Prospettive Future nel Trattamento dei Tumori Gastrointestinali Lorenza Rimassa Medical Oncology Unit Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Disclosures
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Riunione Monotematica A.I.S.F The future of liver diseases. HEPATIC NEOPLASMS The challenge for new drugs
 Riunione Monotematica A.I.S.F. 2016 The future of liver diseases Milan 13 th -15 th October 2016 Centro Congressi Fondazione Cariplo HEPATIC NEOPLASMS The challenge for new drugs Massimo Iavarone Gastroenterology
Riunione Monotematica A.I.S.F. 2016 The future of liver diseases Milan 13 th -15 th October 2016 Centro Congressi Fondazione Cariplo HEPATIC NEOPLASMS The challenge for new drugs Massimo Iavarone Gastroenterology
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Treatment of HCC in real life-chinese perspective
 Treatment of HCC in real life-chinese perspective George Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond), FAASLD (US) Chairman Humanity and Health Medical Group, Hong Kong SAR, CHINA
Treatment of HCC in real life-chinese perspective George Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond), FAASLD (US) Chairman Humanity and Health Medical Group, Hong Kong SAR, CHINA
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
Liver Cancer And Tumours
 Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present:
 and the International Coalition of Hepatology Education Providers (IC-HEP) present:") The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatocellular Carcinoma HCC: Age
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatocellular Carcinoma HCC: Age
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Hepatitis C Update on New Treatments
 Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Hepatocellular Carcinoma in Qatar
 Hepatocellular Carcinoma in Qatar K. I. Rasul 1, S. H. Al-Azawi 1, P. Chandra 2 1 NCCCR, 2 Medical Research Centre, Hamad Medical Corporation, Doha, Qatar Abstract Objective The main aim of this study
Hepatocellular Carcinoma in Qatar K. I. Rasul 1, S. H. Al-Azawi 1, P. Chandra 2 1 NCCCR, 2 Medical Research Centre, Hamad Medical Corporation, Doha, Qatar Abstract Objective The main aim of this study
Update EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma
 Update EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma Peter R. Galle PHC 2018 - www.aphc.info Disclosure of Conflict of Interest Peter R. Galle I have the following financial
Update EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma Peter R. Galle PHC 2018 - www.aphc.info Disclosure of Conflict of Interest Peter R. Galle I have the following financial
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Supplementary Digital Content
 Geissler et al: Sirolimus and Hepatocellular Carcinoma in Liver Transplantation Page 1 of 10 Supplementary Digital Content Supplementary Table 1. Surgical procedures used Total Transplant technique Piggy
Geissler et al: Sirolimus and Hepatocellular Carcinoma in Liver Transplantation Page 1 of 10 Supplementary Digital Content Supplementary Table 1. Surgical procedures used Total Transplant technique Piggy
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
Hepatocellular carcinoma
 Hepatocellular carcinoma Mary Ann Y. Huang, M.D., M.S., FAASLD Transplant hepatologist Peak Gastroenterology Associates Porter Adventist Hospital Denver, Colorado Background - Worldwide Hepatocellular
Hepatocellular carcinoma Mary Ann Y. Huang, M.D., M.S., FAASLD Transplant hepatologist Peak Gastroenterology Associates Porter Adventist Hospital Denver, Colorado Background - Worldwide Hepatocellular
Jose D Sollano, MD Professor of Medicine University of Santo Tomas Manila, Philippines. University of Santo Tomas
 Jose D Sollano, MD Professor of Medicine Manila, Philippines International Variation in Age-Standardized Liver Cancer Incidence Rates in Both Sexes, 2008 Global Age-Standardized Liver Cancer Incidence
Jose D Sollano, MD Professor of Medicine Manila, Philippines International Variation in Age-Standardized Liver Cancer Incidence Rates in Both Sexes, 2008 Global Age-Standardized Liver Cancer Incidence
Approach to Abnormal Liver Tests
 Approach to Abnormal Liver Tests Scott W. Biggins, MD, MAS Assistant Professor Division of Gastroenterology UCSF Scott.Biggins@ucsf.edu (Thanks to Hal Yee, MD) This Morning s Presentation Clinical vignettes
Approach to Abnormal Liver Tests Scott W. Biggins, MD, MAS Assistant Professor Division of Gastroenterology UCSF Scott.Biggins@ucsf.edu (Thanks to Hal Yee, MD) This Morning s Presentation Clinical vignettes
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία. Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018
 Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Hepatocellular Carcinoma: Epidemiology and Screening
 Hepatocellular Carcinoma: Epidemiology and Screening W. Ray Kim, MD Professor and Chief Gastroenterology and Hepatology Stanford University School of Medicine Case A 67 year old Filipino-American woman
Hepatocellular Carcinoma: Epidemiology and Screening W. Ray Kim, MD Professor and Chief Gastroenterology and Hepatology Stanford University School of Medicine Case A 67 year old Filipino-American woman
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O.
 Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
An Update on Hepatocellular Carcinoma. Ed Gane NZ Liver Transplant Unit
 An Update on Hepatocellular Carcinoma Ed Gane NZ Liver Transplant Unit Hepatocellular Carcinoma has a High Burden of Disease APSCVIR March 2018 Lung Liver Colon/Rectal Stomach Breast Cervix Uteri Esophagus
An Update on Hepatocellular Carcinoma Ed Gane NZ Liver Transplant Unit Hepatocellular Carcinoma has a High Burden of Disease APSCVIR March 2018 Lung Liver Colon/Rectal Stomach Breast Cervix Uteri Esophagus
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA*
 UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
New Insights: Systemic Therapy for Advanced Hepatocellular Carcinoma (HCC)
") New Insights: Systemic Therapy for Advanced Hepatocellular Carcinoma (HCC) Thomas W.T. Leung Associate Director and Honorary Consultant Comprehensive Oncology Centre Hong Kong Sanatorium and Hospital Hong
New Insights: Systemic Therapy for Advanced Hepatocellular Carcinoma (HCC) Thomas W.T. Leung Associate Director and Honorary Consultant Comprehensive Oncology Centre Hong Kong Sanatorium and Hospital Hong
Update on Hepatitis B and Hepatitis C
 Update on Hepatitis B and Hepatitis C Catherine Stedman Department of Gastroenterology, Christchurch Hospital and University of Otago, Christchurch Disclosures I have the following financial relationships
Update on Hepatitis B and Hepatitis C Catherine Stedman Department of Gastroenterology, Christchurch Hospital and University of Otago, Christchurch Disclosures I have the following financial relationships
Hepatocellular Carcinoma for NNN Cancer Webinar Series
 Hepatocellular Carcinoma for NNN Cancer Webinar Series Brian J McMahon, MD Liver Disease and Hepatitis Program Alaska Native Tribal Health Consortium * None Disclosures Outline of Talk * Epidemiology of
Hepatocellular Carcinoma for NNN Cancer Webinar Series Brian J McMahon, MD Liver Disease and Hepatitis Program Alaska Native Tribal Health Consortium * None Disclosures Outline of Talk * Epidemiology of
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Hepatocellular Carcinoma Surveillance
 Amit G. Singal, MD, MS Hepatocellular Carcinoma Surveillance Postgraduate Course: Challenges in Management of Common Liver Diseases 308 1 Patient Case 69 year-old otherwise healthy male with compensated
Amit G. Singal, MD, MS Hepatocellular Carcinoma Surveillance Postgraduate Course: Challenges in Management of Common Liver Diseases 308 1 Patient Case 69 year-old otherwise healthy male with compensated
Sorafenib for Egyptian patients with advanced hepatocellular carcinoma; single center experience
 Journal of the Egyptian National Cancer Institute (2014) 26, 9 13 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com Original article Sorafenib for
Journal of the Egyptian National Cancer Institute (2014) 26, 9 13 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com Original article Sorafenib for
Pamplona, junio de Futuro de la Hepatología: Cáncer Hepático. Bruno Sangro Clínica Universidad de Navarra. IDISNA. CIBERehd.
 Pamplona, junio de 2008 Futuro de la Hepatología: Cáncer Hepático Bruno Sangro Clínica Universidad de Navarra. IDISNA. CIBERehd. Pamplona, Spain Etiología del Cáncer Hepático HBV HCV Alcohol NAFLD Iron
Pamplona, junio de 2008 Futuro de la Hepatología: Cáncer Hepático Bruno Sangro Clínica Universidad de Navarra. IDISNA. CIBERehd. Pamplona, Spain Etiología del Cáncer Hepático HBV HCV Alcohol NAFLD Iron
9/10/2018. Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? DISCLOSURES
: What is New? DISCLOSURES") UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report