Government of Afghanistan Ministry of Counter Narcotics AFGHANISTAN
|
|
|
- Constance Goodwin
- 5 years ago
- Views:
Transcription

1 Government of Afghanistan Ministry of Counter Narcotics AFGHANISTAN Drug Use Survey 25
2 Acknowledgements The following individuals contributed to this national assessment of drug abuse in Afghanistan and to the preparation of the present survey report: Drug Demand Reduction Section of the Ministry of Counter-Narcotics Mohammad Zafar (Head) Mohammad Raza (Deputy Head) David Macdonald (Consultant) UNODC (Afghanistan) Doris Buddenburg (Representative) Jehanzeb Khan (International Project Coordinator) Mohammad Naim (National Project Coordinator) Sayed Hassan (Senior Programme Officer) Friba Aabidi (National Project Officer) Mohammad Aqa Stanikzai (National Project Officer) Patrick Halewood (Consultant) Hakan Demirbuken (Regional Illicit Crop Monitoring Expert, ICMP) Nazir Ahmad Shah (National Project Coordinator, ICMP) Ziuddin Zaki (Data Analyst, ICMP) Shamsullah Rahman (Database Developer) Nooria Khairandish (Data Entry Clerk) Zuhra Saddiqe (Data Entry Clerk) Zia Ulhaq (Data Entry Clerk) Mohammad Alam Ghaleb (Regional Coordinator, Nangarhar Zone) Fazal Mohammad Fazli (Regional Coordinator, Kandarhar Zone) Lutfurahman Lutfi (Regional Coordinator, Balkh Zone) Mohammad Alem Yaqubi (Regional Coordinator, Badakhshan Zone) Altaf Hussain Joya (Regional Coordinator, Herat Zone) The field interviews were conducted by field workers of the Drug Dependency Treatment Center of the Mental Health Hospital and the Gesellschaft fuer Technische Zusammenarbeit (GTZ),Demand Reduction Action Teams (DRATs) comprising staff of the Ministries of Public Health and Education, and UNODC field surveyors. The implementation of UNODC s Afghanistan Drug Use Survey 25 was made possible by financial contributions from the Governments of Canada, Italy and Japan. UNODC Country Office for Afghanistan House 49/51, Lane 4, Street 15 Wazir Akbarkhan Kabul, Afghanistan Tel: +93 () ,+93 () Fax: / fo.afghanistan@unodc.org
3 DRUG ABUSE FACT SHEET... 1 EXECUTIVE SUMMARY... 2 GLOSSARY INTRODUCTION AND BACKGROUND TO THE REPORT SURVEY METHODOLOGY... 7 Estimation of the number of drug users... 8 Profile of drug users RESULTS... 1 Opium use Heroin use Hashish use Pharmaceutical use Alcohol use Use of other drugs Trends in drug use in Afghanistan Urban and rural patterns of drug use Drug use among females Child drug use Drug use among ex-combatants... 5 Drug use among returned refugees Injecting drug use Drug treatment facilities and services in Afghanistan... 54
4
5 FACT SHEET - AFGHANISTAN DRUG USE SURVEY 25 Estimated number of drug users 92, as percent of total population (23,85,) 3.8% Estimated number of adult male drug users 74, as percent of total adult male population (6,62,) 12.1% Estimated number of adult female drug users 12, as percent of total adult female population (5,825,) 2.1% Estimated number of child drug users 6, as percent of total child population (11,963,).7% Estimated number of opium users 15, as percent of total population.6% Estimated number of heroin users 5, as percent of total population.2% Estimated number of hashish users 52, as percent of total population 2.2% Estimated number of pharmaceutical drug users 18, as percent of total population.8% Estimated number of alcohol users 16, as percent of total population.7% Estimated number of other drug users 1 2, as percent of total population.9% Note: Estimates of drug use are based on results from 148 key informant and 1393 drug user interviews 1. Other drugs include preparations made from the cannabis plant and opium poppy capsule, as well as solvents
6 Executive summary The Afghanistan Drug Use Survey 25 was carried out from April to August 25 in 32 provincial capitals, 3 district centres and 152 villages in Afghanistan.The number of interviews was based on the estimated population in each location. A total of 148 key informants and 1393 drug users were interviewed in provincial capitals, district centres and villages. People identified as having knowledge of drug use in their communities, such as community leaders, health care workers, police officers and teachers, were selected as key informants. They were asked a series of questions regarding their estimates of the number and demographics of drug users, the types of drugs used and drug use trends in the areas in which they were living. Key informants and other sources introduced the interviewers to problem drug users in their communities. The drug users were asked the same questions, and also further questions regarding their own drug use history. The number of drug users in Afghanistan is estimated at nearly 1,, people, with few areas in the country where drug use does not occur. This figure represents 3.8% of the total population, and includes over 86, adults (7% of the population aged 15-64). There are strong indications that the estimates presented in this survey of numbers of drug users are lower than the true figures, particularly the number of women and child drug users, since Afghans are likely for cultural reasons to underestimate the level of drug use in their communities. According to key informants and experienced drug demand reduction workers, the number of drug users in Afghanistan is increasing. This survey estimates that the number of drug users in Kabul in 25 had doubled since 23. The level of polydrug use is also rising. The amount and type of drugs consumed and the frequency of use indicate that many people in Afghanistan are dependent on a range of drugs. At least 2, people (1.7% of the population aged 15-64), mostly men, are regular users of opiates in the form of either opium or heroin, accounting for between 5% and 1% of Afghanistan s opium harvest. An estimated 18, people use pharmaceutical drugs illicitly, including 6, women and 3, children under 15 years of age. Injecting drug use occurs in the heroin and pharmaceutical drug user communities (14% and 16% of each community, respectively), and to a lesser degree among opium users, and needle-sharing is common. Drug demand reduction workers consider injecting drug use to be increasing. An on-going seroprevalence assessment of blood-borne infections among Kabul IDU has detected measurable prevalences of HIV, syphilis, and hepatitis B and C. There is a higher rate of drug use among returned refugees than among other members of Afghan society. Approximately two per cent of Afghans have spent time in Iran as refugees, yet returnees account for nearly one third of heroin users and almost the same proportion of opium users in Afghanistan. Less than half of those Afghans that fled to Iran have returned. Current drug treatment services and facilities cannot meet demand. There are no more than 1 places available in residential treatment facilities in the entire country, and many areas identified as having a large number of drug users have no treatment facilities at all. Such programmes, even when operating at maximum efficiency, can treat less than.25% of drug users in Afghanistan each year. 2 2
7 Afghanistan: Estimated Drug Users by zone UZBEKISTAN TURKMENISTAN Jawzjan Balkh Kunduz Faryab NORTH Sari Pul Samangan Baghlan Hirat Badghis Ghor Bamyan Wardak Parwan Logar WEST Uruzgan Ghazni Farah SOUTH Paktika Zabul IRAN Nimroz Hilmand Kandahar Note: The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. TAJIKISTAN NORTH EAST Takhar Badakhshan Nuristan Laghman Kapisa Kunar EAST Kabul Nangarhar Paktya Khost CENTRAL Drug Users per Zone PAKISTAN Estimated Users <1, 1,-2, >2, km Geographic Projection, Datum: WGS 84 International boundary Provincial boundary UN zone boundary "
8 Glossary Demand reduction: A broad term applied to a range of policies and programmes which seek to reduce desire and preparedness to obtain and use illegal drugs. Demand for drugs may be reduced through prevention and education programmes to dissuade users or potential users from experimenting with illegal drugs and/or continuing to use them; treatment programmes aimed primarily towards facilitating abstinence and reducing the frequency of use or amount consumed; and broad social policies to minimize factors contributing to drug use, such as unemployment, homelessness and truancy. Dependence: As applied to alcohol and other drugs: a need for repeated doses of a given drug, giving the user a continued sense of wellbeing or preventing withdrawal symptoms. Detoxification: The process by which a person who is dependent on a psychoactive substance ceases use in such a way as to minimize withdrawal symptoms and risk of harm. Traditionally, detoxification has been provided on an in-patient basis, either in a specialist treatment facility or on the wards of a general or psychiatric hospital. Drug: A term of varied usage. In the various United Nations Conventions and the Declaration on the Guiding Principles of Drug Demand Reduction, the term refers to substances subject to international control. In common usage, it often refers specifically to psychoactive drugs, and also, within that category, to illicit drugs. Drug use: Current international drug control treaties do not define drug use, but instead employ a variety of terms, including abuse, misuse and illicit use. For the purposes of this report, the term drug use means the use of any substance under international control for purposes other than medical use, including use without a doctor s prescription, in excess, or for an unjustified period of time. Hashish: In Afghanistan, hashish refers to cannabis resin obtained from the flowering tops of the cannabis plant. Heroin: A drug obtained through acetylation of morphine. The most common type of heroin in Afghanistan is so-called brown heroin and is not suitable for injection, though it can be converted easily into an injectable form. Home treatment: Home-based detoxification, usually involving home visits by medical staff and informal support provided by family and/or friends. IV: An abbreviation for intravenous injection route, i.e., the injection of a substance into a vein in any part of the body. Regular injecting drug users may damage the veins in their arms and consequently inject veins in other parts of their body instead. Opium: The coagulated juice from the unripe capsule of the poppy plant (Papaver somniferum). Contains approximately 1 per cent morphine. Outreach programme: A community-based activity with the overall aim of facilitating improvement in health and reducing drug-related risk or harm to individuals and groups. Peer pressure: This term is applied to drug use to embody the idea of pressure exerted on an individual to conform to the behavioural norms of his or her peers, which may include the illegal consumption of drugs. Such individuals are seen to be easily influenced and passive in the face of such pressure. Pharmaceutical drug: A pharmaceutical drug (pharmaceutical) is a substance manufactured by the pharmaceutical industry or prepared in a pharmacy for medical purposes, or any preparation derived from such substances. The most common pharmaceuticals encountered during this survey were anxiolytic and hypnosedative drugs such as Diazepam, and painkillers such as Pentacozine. Poly-drug use: The use of more than one psychoactive drug either simultaneously or at different times. The term is often used to distinguish persons with a more varied pattern of drug use from those who use only one kind of drug. Relapse: A return to drug use after a period of abstinence. Residential treatment: Treatment programmes which require participants to live in a hostel, home or hospital unit. Self-treatment: Home-based detoxification carried out by a drug user with minimal outside support. Snowballing: A method of recruitment of illicit drug users for research purposes. The method involves the recruitment of a small number of illicit drug users for the purpose of establishing contact with a number of other drug users of their acquaintance. 4 4
9 1. Introduction and background to the report The Drug Use Survey 25, conducted jointly by UNODC and the Ministry of Counter- Narcotics (MCN) of the Islamic Republic of Afghanistan, aims to provide the first nationwide profile of drug use in the country. For the survey, 148 key informants were asked questions regarding the number of drug users in their communities, the drug types that were used and trends in the level of drug use. In addition, 1393 drug users were asked the same questions and also interviewed regarding their own drug use history. The answers given by these two groups provide the core of this report. It is anticipated that the report will provide accurate baseline information enabling relevant government agencies and NGOs to develop rational and realistic strategies for drug demand reduction interventions in Afghanistan. Illicit drug use has long been recognised as a major problem in Afghan communities both within Afghanistan and in neighbouring countries. A report produced by UNODC (formerly UNDCP) in 1995 noted that levels of urban drug use, particularly heroin, were increasing 1, and as early as 1998, high levels (2% to 3%) of opium addiction were reported among the local population in areas of Badakhshan province 2. In response to the reported escalation of drug use in Afghan communities, in 1998 UNODC launched the first of five studies on problem drug use within those communities. The first report 3 set out an initial assessment of the problem within Afghanistan and in Afghan refugee communities in Pakistan, particularly in Peshawar and Quetta. It identified the prevalence of poly-drug use, including the use of 2 different combinations of drugs, and also the health-related, economic, social and legal problems associated with drug use within Afghan communities. It further identified IV use among heroin users and the potential for misuse of pharmaceutical drugs. The report noted that the most commonly used illicit drug was hashish; that alcohol use outside of Kabul and Mazar-e-Sharif was restricted; and that a number of young people had applied to a drug treatment centre for treatment of solvent abuse. Subsequent studies focused on specific groups of drug users or specific areas in Afghanistan. Afghan women living in refugee camps and street heroin users in Pakistan were the subjects of more detailed reports 4 5. A report on the former group noted a high prevalence of poly-drug use among female refugees (76% 6 ), particularly the use of opium and pharmaceutical drugs alone or in combination with other drugs (62%). The report indicated low levels of heroin use among women (four per cent), and suggested the relatively high price of heroin and a ready supply of other, cheaper drugs as possible factors influencing the decision by women not to use heroin. The report on street heroin users interviewed 15 male users in Peshawar and Quetta. The average rate of IV use among those populations was 1.3%, though a further 5% of heroin users had injected in the past. At least 43% of IV users shared needles. The fourth report 7 focused on drug use in rural areas southeast of Kabul. The study area covered parts of the Logar, Kabul, Nangarhar and Paktya provinces. The report estimated that 4% to 6% of adults used opium;.1% to.14% heroin; 7% to 11% hashish; and 1.4% to 2% pharmaceutical drugs. It also showed that the distribution of drug users varied widely between districts, and that nearly 4% of drug users first used drugs in either Pakistan or Iran. 1 Ulrich Kohler (1995), Report of a drug demand reduction assessment and strategy formulation mission to Afghanistan, UNDCP, Islamabad, quoted in UNDCP (1999), Community Drug Profile #1 - Problem Drug Use in Afghan Communities: An Initial Assessment, UNDCP Programme, Islamabad. 2 ORA International Central Asia (1998), Taking up the Challenge: ORA Annual Report 1997/98, ORA, quoted as above. 3 UNDCP (1999), Community Drug Profile #1 - Problem Drug Use in Afghan Communities: An Initial Assessment, UNDCP Programme, Islamabad. 4 UNDCP (1999), Community Drug Profile #2 Opium and Other Problem Drug Use in a Group of Afghan Refugee Women, UNDCP Programme, Islamabad. 5 UNDCP (2), Community Drug Profile #3 A Comparative Study of Afghan Street Heroin Addicts in Peshawar and Quetta, UNDCP Programme, Islamabad. 6 The original report indicated a figure of 92%, but included tobacco use. The present report did not consider tobacco use. 7 UNDCP (21), Community Drug Profile #4 An Assessment of Problem Drug Use in Rural Afghanistan: the GAI Target Districts, UNDCP Programme, Islamabad. 5 5
10 The final UNODC survey 1, carried out in 23, was designed to assess problem drug use in Kabul itself. The survey interviewed 1 key informants and 2 drug users (25% of the latter were female) in Kabul and estimated the following levels of drug use 2 : opium.4%; heroin.3%; hashish 1%; pharmaceuticals.6%; and alcohol.3%. As in earlier reports, drug users were asked where they first started using drugs, and again it was found that a high percentage (4% of opium users and 5% of heroin users) had first started using drugs in either Iran or Pakistan. The report also examined reasons why individuals began using drugs and the problems associated with drug use, and also identified problems in accurately assessing levels of drug use in Afghanistan, particularly among women. All of the reports found that, whilst the level of drug use in Afghanistan is difficult to estimate, even conservative estimates indicate that drug use is a major problem in Afghanistan and among Afghan communities overseas. They also established that the level of drug use appears to be increasing, particularly heroin use, and that treatment services are not able to meet demand. There have been a number of other studies on drug use in Afghanistan. Such studies often examine use of a specific drug in a particular location 3. Whilst these studies have a narrow focus, many of their findings can be applied at the national level, such as the health and social problems experienced by drug users and the level of debt in which many families find themselves as a result of drug use. During the 25 Annual Opium Poppy Survey 1,9 village headmen were asked to provide an estimate on the number of opium and heroin addicted people in their communities. The survey 4 reported that opium addiction affects.5% of the rural population (approximately 1% of population aged 15-64), and heroin addiction.3% of the rural population. The report further noted that, on average, opium addiction rates were seven times higher in opium poppy growing villages than in other villages. This survey was designed to give indicative figures of the level of opiate addiction in rural Afghanistan. The survey did not conduct interviews in urban centers or in district centres. 1 UNDCP (23), Community Drug Profile #5 An Assessment of Problem Drug Use in Kabul City, UNDCP Programme, Islamabad 2 Lowest estimates, based on an estimate of the population of Kabul at 2.5 million at the time of the survey. 3 For example: Theuss et al, (25) Addiction in the Border Regions of Badakshan, Afghanistan: Range, Trajectory and Impacts. 4 UNODC (25), Afghanistan Opium Poppy Survey, November 25, p
11 2. Survey Methodology A total of 148 key informants and 1393 drug users were interviewed in all 32 provincial capitals, 3 district centres (1% of all district centres) and 152 villages (.5% of all villages) in Afghanistan 1. District centres and villages were chosen at random from the AIMS Geocodes and Settlements Database for Afghanistan 2, the number of interviews being based on the estimated population in each location. Interviews were conducted with both male (125) and female (155) key informants, and likewise with male (1228) and female (122) drug users 3. Approximately 15 people in Kabul and other provincial centres were trained in interview skills, ethnography applied to working with drug users, and survey methodology. The survey began in June 25 and was completed by September of the same year. The surveyors first task was to identify key informants in each of the selected communities. Key informants were chosen on the basis of their familiarity with the local drug user population. Female informants were employed primarily as health care workers or teachers, or were not employed outside of the home; male informants were employed in a broader range of jobs, but were often police officers, community leaders or self-employed (Table 2.1). Employment category Female 33 4* Male Not recorded * including two judges 1=Healthcare workers, doctors, pharmacists, social workers 2=Police 3=Government employees 4=Religious/ community leaders 5=Labourers/ farmers/ self-employed/ tradesmen/ shopkeepers/ students/ housewives/ unemployed 6=Teachers Table 2.1 Employment categories of key informants Over 7% of key informants had lived in their respective communities for more than 1 years, almost 6% having never lived anywhere else. Most informants were aged between 31 and 5, almost all were married and many (4%) had completed high school. Female informants tended to be younger (on average 37 years old) and better educated than their male counterparts, who were older (on average 42 years old) and more likely to have been educated at a madrasa (religious school). Most key informants reported that they were familiar with drug use with respect to at least one of the six categories of drugs that they were asked about (Table 2.2), and more than 9% were personally acquainted with one or more drug users. Drug use within the community (percentage of key informants) Drug type Yes No Don't know Opium Heroin Hashish Pharmaceuticals Alcohol Other drugs Table 2.2: Key informants awareness of drug use 1 See Annex A Gender of interviewee was not always recorded. 7 7
12 The majority of those key informants that reported that they were not acquainted with any drug users were from one of six villages where no drug users were identified, which suggested that those villages were drug-free. The high percentage of key informants who were unaware of any pharmaceutical use may be attributable to the method of use of such drugs, which are commonly consumed in tablet form, and to the fact that pharmaceuticals are generally not consumed when others are present. Each key informant was asked a series of 72 questions regarding their perceptions of drug use in their immediate community. These questions covered not only the types of drugs consumed and the number of drug users, but also the reasons for drug use, problems experienced as a result of drug use and whether more or fewer people were using drugs than in the past 1. Key informants were then asked to introduce the surveyors to a number of drug users in the areas in which they were living. On the basis of initial interviews with drug users, further users were identified and questioned. A total of 1393 drug users were identified and interviewed in this way. Drug users were asked the same questions as key informants, but were also asked a further 74 questions regarding their own pattern of drug use 2. These questions included the history of their drug use, the amount and types of drugs that they consumed, family drug use, details of problems that they had experienced as a result of drug use and information on any treatment that they had undergone. Drug Use Exists in Community (% of Drug Users) Drug Type Yes No Don't Know Opium Heroin Hashish Pharmaceuticals Alcohol Other Drugs Table 2.3: Drug users awareness of drug use Drug users reported lesser knowledge of drug use in their communities than key informants. This was noted in previous surveys 3 and attributed to the fact that the drug user questionnaire was much longer than that given to the informants. Users were more likely to lose concentration, possibly owing inter alia to cold or fatigue, and give vague or misleading answers. It is unlikely that users experienced cold during the survey, since it was carried out during the summer, but other such factors may have come into play. Estimation of the number of drug users Estimates of the number of drug users were calculated using the reports of both key informants and drug users. A simple average of the estimates provided by key informants and drug users was used to minimize the likelihood of over- or underestimation 4. Where an informant or user had given a clearly unlikely estimate, then the answer given by that individual would not be used in determining the final estimate for the location in question, for example, if 5 users and 4 informants all estimated the number of opium users in their 1 See Annex A2 for complete questionnaire. 2 See Annex A3 for complete questionnaire. 3 UNDCP (23), Community Drug Profile #5 An Assessment of Problem Drug Use in Kabul City, UNDCP Programme, Islamabad, p See Annex A4. 8 8
13 community at between 1 and 15, but a single informant estimated there to be no opium users, or perhaps 5 users. There was a very high correlation between the estimates provided by key informants and drug users (r=.9); informants generally estimated numbers of drug users at 2% to 3% higher than drug users themselves 1. The high correlation between key informants and drug users estimates was found in communities irrespective of total population and drug using population. In order to calculate a national estimate of the number of drug users, it was necessary to take into account the sampling method used only.5% of villages and 1% of district centres were sampled 2 and to adjust figures to allow for the level of poly-drug use. It is important to note that the sampling method used was designed to provide an accurate estimate of drug use at the national or regional level at best. Parts of the present report, give estimates of drug users at the provincial level. These estimates must be used with caution, and should be interpreted as indicative only. No estimate of error can be given at the provincial level, as the sample size was too small to give accurate provincial estimates. Profile of drug users The profiles of drug users set out in Section 3 are predominantly based on analysis of the additional questions posed to drug users. Key informants provided useful information on problems experienced by users as a result of drug use and reasons why users cease drug use. Any analysis of these answers must take into account, however, that drug users themselves are likely to give more accurate answers to these questions. 1 See Annex A4 for details. 2 See Annex A5 for details. 9 9
14 3. Results There are a number of important issues that should be borne in mind when interpreting the findings of this report. Past studies have shown that informants may for cultural reasons underestimate levels of drug use. The stigma commonly associated with drug use may be perceived by informants as reflecting on themselves or their communities; even among drug users there appears to be a reluctance to provide accurate estimates of community drug use or to discuss personal drug use openly. Whilst the surveyors were well trained in techniques to overcome these problems, the estimated numbers of drug users reported in this survey should be treated as minimum estimates. A further problem, identified in previous work, in accurately estimating levels of drug use among women is the difficulty in identifying female drug users who are willing to be interviewed. Due to the nationwide coverage of this survey, interviews were often carried out in areas with poor security. Female surveyors, required to interview female key informants and drug users, were unable to travel to some areas. This was not only the case in isolated, rural areas, but also in a number of urban areas where female surveyors were unable to contact a reasonable sample of female drug users. In discussions with staff at drug treatment centres and other experienced drug demand reduction workers, it was noted that drug use patterns among women are of a less public nature than those among men. Most pharmaceutical and opium use by women occurs in the home, and women typically eat opium rather than smoking it, which makes their drug use less visible to other members of the community. This suggests that those key informants and drug users interviewed may have had less knowledge of drug use among females than of that among males in their respective communities, and that their estimates of drug use among females are lower than the true figures. Since drug use among children is also less visible outside of the family home, this survey probably underestimates the true level of child drug use. Before estimating the total number of illicit drug users in Afghanistan, it was necessary to consider poly-drug use. Drug users were asked a series of questions regarding the combination, if any, of drugs that they were using from among six categories, namely opium, heroin, hashish, pharmaceutical drugs, alcohol and other drugs. Number of illicit drug types used Drug users interviewed (%) 1 only 53% 2 only 27% 3 only 13% 4 only 5% 5 only 2% All 6 1% Table 3.1: Poly-drug use, based on individual patterns of use among drug users. The answers given indicated that poly-drug use was common, particularly among men, and that nearly half of all adult drug users used more than one drug type (Table 3.1). Of 63 possible combinations of two or more drugs from among the six drug categories, male drug users reported using 54 combinations, whilst female drug users reported 21 combinations 1. Since no children (under 15 years of age) were interviewed during the survey, it is not possible to estimate the level of poly-drug use among child users separately from that among adults. The estimate of the total number of drug users was reduced by approximately 3% to account for those that had been included in the estimates of numbers of poly-drug users (Table 3.2) 2. 1 See Annex B1. 2 See Annex A5 for details. 1 1
15 9% confidence interval Drug type Male Female Child 1 Total Lower Upper Opium 132,27 16,528 4,134 15, 11, 155, Heroin 45,81 3, , 35, 51, Hashish 511,224 8,83 2,778 52, 43, 665, Pharmaceuticals 91,875 57,444 29,626 18, 125, 2, Alcohol 143,794 18, , 155, 2, Other drugs 93,135 64,18 46,284 2, 13, 23, Total 1,18,35 168,138 84,74 1,26, 98, 1,5, Total, adjusted for poly-drug use 739, 121, 6, 92, 71, 1,9, Table 3.2: Estimated number of drug users in Afghanistan in The use of illicit drugs is ubiquitous in Afghanistan. The total number of drug users is estimated at 1.27 million people, on the basis of estimates provided by key informants and drug users. If this figure is adjusted to allow for poly-drug use, i.e., cases in which a user may have been counted twice or more, the estimated number of illicit drug users in Afghanistan is at least 92,. This figure represents 3.8% of the total population 2. 1 Children under 15 years of age. 2 Based on an estimated national population of 23.9 million

16 Opium use It is estimated that there are at least 152, opium users in Afghanistan, approximately 86% (132,) of who are adult males, 11% (16,) adult females, and 3% (4,) children. These figures are based on estimates given by both male and female key informants and drug users. Had only those responses given by female interviewees been used, the final estimate of the number of female opium users would have been almost three times higher i.e. more than 45, women. Geographically, the highest concentrations of opium users outside of Kabul city are found in provinces along Afghanistan s northern border (Figure 3.4). Although opium is used in areas along Afghanistan s border with Pakistan, it is noticeable that levels in those areas are significantly lower than elsewhere in the country. This is even more noteworthy when considering that, in 25, the Hilmand and Kandarhar provinces accounted for almost 4% of Afghanistan s total opium production 1, and that Nangarhar province has traditionally produced a significant quantity of opium 2. The distribution of male and female opium users does not vary significantly from province to province, although there were almost no reports of opium use among females across a broad swath of provinces stretching from Hilmand and Kandarhar through to the Bamyan and Wardak provinces. Figure 3.1: Estimated number of opium users, by province. The following profile of opium users is based on the answers given by 576 male and 71 female opium users. Approximately 4% of opium users interviewed lived in provincial centres and 6% in rural Afghanistan. Most users were between 3 and 4 years of age and had been using opium for an average of six years. Most opium users were married (75%), and almost 2% of female users were widowed (the corresponding figure for male users was 1%). Whilst 15% of male users were unemployed, nearly 65% of women were not in paid employment. Approximately 15% of opium users reported that they were ex-combatants. Typically, the family income of female opium users was approximately 2,8 Afghanis (AFA) per month, of which those users spent a monthly sum of roughly AFA1,6 on opium, whilst 1 UNODC (25), Afghanistan Opium Poppy Survey, November UNODC (24), Afghanistan Opium Poppy Survey, November
17 the average income of male opium users was AFA3,4 per month, of which approximately AFA2,5 was spent on opium each month 1. Roughly 6% of female opium users obtained their opium exclusively from drug dealers, although a further 3% purchased some of their opium from drug dealers; 13% reported that they had obtained opium from their own poppy fields. Approximately 35% of male opium users obtained their opium exclusively from drug dealers. Whilst 2% reported that they obtained opium from their own poppy fields, only 4% reported private cultivation as their sole source. It is estimated that 1% of households in Afghanistan are directly involved in the cultivation of opium poppy 2. It is not possible to establish whether poppy farming leads to a higher rate of opium use, or whether opium users grow poppy for their own use, but this survey shows that a greater percentage of opium users than non-users are involved in poppy cultivation. Sixty per cent of female users who purchased opium depended solely on family members as a source of money. Approximately 35% of women used their income from employment to purchase opium. No women reported having to resort to crime to raise money. Ninety-four per cent of male users who purchased opium depended on earned income or money borrowed from family members to finance their purchases. A small number of opium users resorted to crime (three per cent) or begging (four per cent) to raise money. Interviewees tended to be descriptive rather than referring to approximate weights when asked how much opium they used each day, often describing the quantity used as equal to the size of a seed, such as a bean or a pea. In general, female users consumed less opium (1.2g per day) than male users (1.7g), and used opium less frequently, although roughly 9% of both groups consumed opium at least once per day. No attempt was made during this survey to measure the potency or quality of opium used in different areas, the variability of which may partly account for the variation in quantities used. Combined analysis of the data obtained for quantities of opium used and the estimates of the number of opium users indicate that at least 88 metric tonnes of opium are consumed within Afghanistan each year, accounting for just over 2% of opium production of Afghanistan in There is a general trend of increased opium consumption with length of use among male users (Figure 3.3), with men who had used opium for more than 1 years using 7% more opium than men who had used opium for less than 1 year. There is no clear trend among female opium users. The most common method of opium use among women was to eat the drug, whilst the numbers of male users who ate opium and those that smoked the drug were roughly equal (Figure 3.4). Less than two per cent of male opium users reported that they injected a preparation of the drug, and in no cases was injection reported as the sole method of drug use. Notably, all but one injecting opium user reported sharing needles with other injecting users. There appears to be no correlation between length of use and method of use, or between method of use and quantity used. 1 Estimates of amount spent on drugs each month should be considered indicative only. Often drug users are supported financially by other family members, and this level of support may not have been included in their overall expenditure 2 UNODC (25), Afghanistan Opium Poppy Survey, November Ibid
18 2.5 Average amount of opium consumed daily (g) < 1 year 1-3 years 4-6 years 7-9 years > 1 years FEMALE MALE Figure 3.3: Average amount of opium used daily compared to length of time using opium % of users FEMALE MALE eating smoking injecting Figure 3.4: Method of opium use. Very few male users gave a clear, single answer as to why they began using opium. The most common answers given were recreation and peer pressure (Figure 3.5). Significantly, 42% of male users reported that the medicinal effects of opium were among the reasons why they first took opium. Unlike male users, female users provided reasonably clear answers as to why they first began using opium. More than 85% reported that the medicinal effects of opium were among the reasons why they first took opium, and 7% reported those effects as the only reason
19 % of opium users FEMALE MALE as medicine curiosity easily available liked the effects other peer pressure recreation Figure 3.5: Reasons given for beginning to use opium. There was moderate correlation between user age and length of time using opium. All women interviewed were married or widowed; 93% had children; nearly 25% had seven or more children; and 7% gave the sole response as medicine when asked why they first began using opium. On that basis it was concluded that the majority of female users first began taking opium to treat medical conditions associated with childbirth. Most male opium users (92%) reported at least one problem associated with their use of opium, and the majority reported multiple problems (Figure 3.6). All female opium users reported at least one problem associated with their use of opium, and again the majority reported multiple problems % of opium users FEMALE MALE criminal behaviour financial health social relations stigma Figure 3.6: Problems associated with opium use. Except in the case of criminal behaviour, men and women experience the same problems as a result of drug use. It is ironic that health problems are most commonly reported, considering that the use of opium as a medicine is one of the most common reasons given for beginning to use the drug. Nearly 75% of female users reported that they were trying to resolve their problems: 13% were seeking treatment and 62% were trying to give up opium by other methods. The corresponding percentages among male users were more than 9%; 3%; and 6% respectively
20 5 4 % of opium users 3 2 FEMALE MALE 1 home jail self detoxification treatment centre Figure 3.7: Methods/location used to give up opium. Nearly 63% (n=361) of male opium users and 7% (n=49) of female opium users reported that they had tried to stop using opium in the past, citing different circumstances in which they had stopped. Just over 4% (n=164) of this group of male and female opium users had stopped at home with some help from health workers. Some of these users had also been taken to a medical clinic by their family for help rather than being helped at home, with a few physically restricted to the home by family members. A further 22% (n=11) of women and 25% (n=9) of men stopped at home by themselves without any medical assistance, going through a process of self-detoxification unaided. Around 2% (n=72) of men who had stopped and 12% (n=9) of women had received specialist help from a drug treatment centre, either residential or community-based. Just under 5% of men had stopped opium use when they had been sent to prison % of opium users who had tried stopping A few days 1 w eek 1 month 1 year >1 year Figure 3.8: Period of abstinence from opium among users following stopping. A variety of reasons were given by male drug users as to why they resumed opium use following stopping (Figure 3.9). By far the most common reason for resuming use was physical or psychological pain, according to nearly 55% of respondents. Female opium users formed the overwhelming majority of those that reported physical or psychological pain as the reason for resuming opium use following stopping. Nearly 55% of all women who had sought treatment cited the same as their sole reason for resuming opium use. 1 Sample size of female users was very small (37)
21 FEMALE MALE easily and cheaply available lack of family support no treatment facility pain (physical or psychological) peer pressure unemployment other Table 3.9: Reasons given for resuming opium use following stopping. A comparison of the reasons given by opium users for first beginning to use opium and those given for resuming opium consumption following stopping reveals that female users commonly give a clear single answer: they begin using opium for its medicinal effects, and resume use as a result of pain after giving up. Male users rarely give clear single answers; peer pressure and recreation were more commonly identified as reasons for first using opium than any medicinal effect that the drug may have; and peer pressure was a common reason given for resuming opium use following treatment. 2 % of all opium users FEMALE MALE brother or sister father mother spouse child under 5 child over 5 other Figure 3.1: Use of opium by family members of users. The pattern of opium use among users family members varied between male and female users. Slightly less than 18% of male opium users reported that a close family member also used opium, in most cases one or more brothers. Nearly one third of female opium users reported that a close family member also used opium, in most cases their husband. Women were also more likely than men to have a mother or children who used opium. More than 78% of male opium users reported poly-drug use, compared with approximately 55% of female users. By far the most common combination of drugs used by males reported by 56% of male users was that of opium and hashish, in combination with or without other drugs. While 28% of men said that they took only opium, 27% reported that they used heroin in combination with opium. The most common drug type used by female users in combination with opium was pharmaceutical drugs (3%). Of the 2% of women who 17 17




22 reported that they used heroin in combination with opium, all lived in urban areas, particularly Kabul. This report estimates significantly higher figures of opium use, particularly in Kabul, than past surveys 1. Earlier reports predicted that opium use in Afghanistan may increase as a result of easy availability and relatively cheap prices, and the present report can confirm that those predictions indeed appear to be coming true. It should be noted that this report does not confirm previous estimates of opium use in Badakshan. This is possibly due to the sampling methodology applied in this study. Opium use in Badakshan appears to be common only in certain areas (particularly the Ishkashim, Shugnan, Wakhan and Zebak districts). One of the consequences of selecting a small number of villages at random was that only one of the surveyed villages was in an area of high opium use, whereas five were in areas where opium use is not considered common. Figure 3.11: Surveyed villages (Drug Use Survey 25) in Badakshan and areas previously identified as having high levels of opium use. 1 Theuss et al, (25) Addiction in the Border Regions of Badakshan, Afghanistan: Range, Trajectory and Impacts
23 Heroin use According to estimates provided by key informants and drug users, there are some 49,5 heroin users in Afghanistan. More than 92% (46,) of heroin users are men, 7% (3,5) are women, and less than 1% (fewer than 3) are children. These results are based on the estimates given both by male and by female interviewees. Had only the estimates provided by women been used, the final estimate of the number of female heroin users would have been nearly 2% higher, i.e. approximately 1, women. Figure 3.12: Estimated number of heroin users, by province. The distribution of heroin users in Afghanistan follows a similar pattern to that of opium users, with most rural users living in provinces along Afghanistan s northern border and urban users concentrated in Kabul. Whilst female users were concentrated particularly in Kabul, there were reported to be no female heroin users in 22 of the total 32 provinces. The stigma associated with drug use, in particular with heroin use among females, must be considered here. It is possible that informants failed to report cases of heroin use by females in those provinces because they were either unwilling to do so or were unaware of such cases. There appears to be little correlation between the location of heroin production facilities 1 and the distribution of heroin users. The following profile of heroin users is based on the answers given by 259 men and 19 women who reported that they were using heroin. Of the men, 137 lived in provincial centres, whilst the remainder (122) lived in rural areas; only one woman lived in a rural area. Whilst the responses given by women will be discussed, it is not possible to draw up an accurate profile of female users owing to the very low number of female heroin users interviewed. The responses given by a single rural female heroin user cannot of course be representative of all rural female heroin users. The average age of those interviewed was 32 years for male heroin users and 38 years for female heroin users. The former had been using heroin for an approximate average of 4 years and the latter for an average of 4.8 years. Some 7% of heroin users were married, whilst the remainder were single or, rarely (less than 1% percent), widowed or divorced. 1 UNODC, 25, p
24 Almost 5% of male and 8% of female users had never attended school; 1% of male users had completed high school, as compared to % of female users. Just over 25% of heroin users were unemployed, although the corresponding figure for female users was higher at 8%. Most users (approximately 7%) worked in the private sector or as farmers. Some 16% of male heroin users reported that they were ex-combatants. Most heroin users (7%) had lived in their communities for more than 1 years. Typically, male heroin users earned approximately AFA3,4 per month and spent around AFA2,4 on heroin monthly. Eighty-five per cent of users depended on earned income or money borrowed from family members to purchase heroin. Some male heroin users resorted to crime (ten per cent) or begging (nearly nine per cent) to raise money. Approximately 35% of heroin users obtained the drug exclusively from drug dealers, and all users reported that they obtained all or most of their heroin from drug dealers or friends. Each male user consumed an average of 1.4 g of heroin per day, whilst women consumed.9 g. More than 9% of male and female users consumed heroin at least once a day, and nearly two thirds of male users consumed heroin more than once a day. As in the case of Opium there is a general trend of increased heroin consumption with length of use among male users (Figure 3.13), with men who had used opium for more than 1 years using 1% more opium than men who had used opium for less than 1 year. There is no clear trend among female opium users. No users were asked questions relating to the grade or quality of the heroin that they used. Average amount of heroin consumed daily (g) < 1 year 1-3 years 4-6 years 7-9 years > 1 years Figure 3.13 Average amount of heroin used daily compared to length of time using heroin. 2 2
25 1 9 8 % of heroin users eating injecting smoking Figure 3.14: Method of heroin use. Smoking was the most popular method of heroin use by both male and female users (Figure 3.14). Almost 14% of male users injected heroin, whereas no female users reported using the injection method. Unlike in the case of opium use, few people reported using multiple methods to take heroin. Nearly 7% of men who injected heroin reported sharing needles with other users. Very few users gave a clear single answer as to why they began using heroin, although women tended to give fewer reasons than men. The most common answers given by female users were as medicine and liked the effects, whilst men selected peer pressure and recreation (Figure 3.15). A small number of men also reported work pressure as a reason for beginning to use heroin. Unlike opium users, few heroin users first used the drug for any medicinal effects it may have. Recreational use of heroin and peer pressure were significant reasons for first use by both men and women. 4 3 % of heroin users 2 1 FEMALE MALE as medicine curiosity easily available liked the effects peer pressure recreation other Figure 3.15: Reasons given for beginning to use heroin. All heroin users reported at least one problem associated with their use of heroin, with over 98% reporting multiple problems (Figure 3.16)
26 % of heroin users criminal behaviour financial health social relations stigma FEMALE MALE Figure 3.16: Problems associated with heroin use Approximately 85% of male users and 9% of female users reported financial problems. Ninety-eight per cent of heroin users reported multiple problems associated with their drug use; eighty per cent reported that they were trying to resolve their problems; twenty per cent of women and thirty per cent of men were seeking treatment. Remarkably, health problems were reported by half as many women as men, and by half as many female heroin users as female opium users. Nearly 8% of female heroin users and 7% of male users reported that they had tried to stop using heroin in the past (Figure 3.17), although only 2% of them had tried multiple methods. With the exception of jail, male and female treatment patterns are very similar. 7 6 % of heroin users FEMALE MALE 1 home jail self detoxification treatment centre Figure 3.17: Methods used to give up heroin
27 5 % of users who had tried to stop A few days 1 w eek 1 month 1 year >1 year Figure 3.18: Period of abstinence from heroin following treatment. This analysis of periods of abstinence was based on answers provided by heroin users who had tried only one method of treatment (14). No women reported being treated in jail. Homebased treatment was the least successful method in treating heroin use, whilst treatment at treatment centres and to a lesser degree self-detoxification were most successful. As in the case of opium users, heroin users gave a variety of reasons as to why they resumed heroin use following treatment (Figure 3.19). By far the most common reason for resuming use was physical or psychological pain, as given by over 8% of male respondents and all female respondents, thus revealing close similarity between the responses given by heroin and opium users to this question. % of heroin users who had undergone treatment easily and cheaply available lack of family support no treatment facilities pain (physical or psychological) peer pressure unemployment other Table 3.19: Reasons given for resuming heroin use following treatment. Approximately 1% of heroin users reported that a close family member also used heroin, although the corresponding figure among female users only is higher at 3%. The majority of those that reported other family members as using heroin (56%) were men with a brother or 23 23
28 brothers who also used heroin. Only one man reported multiple close family members as using heroin, namely his mother, wife and brother(s). Just over 8% of male heroin users reported poly-drug use, whilst the corresponding figure among female users was lower at 7%. Almost 53% of male users used hashish in combination with heroin, whilst 52% used opium in combination with heroin. Fifty-six per cent of female users used heroin in combination with opium


29 Hashish use According to the responses of key informants and drug users interviewed for this survey, there are 52, hashish users in Afghanistan. Hashish use is almost exclusively a male activity. Slightly more than 98% of hashish users are men; 1.5% women; and the remainder children. Had only the estimates given by female hashish users (n=14) and key informants (n=142) been used to calculate the estimated number of female hashish users in Afghanistan, that number would be approximately 4, women rather than 8,. Figure 3.2: Estimated number of hashish users, by province. According to both male and female key informants and drug users, there are no female hashish users in 25 of Afghanistan s 32 1 provinces. Unlike in the case of the distribution of male opiate users, male hashish users are not concentrated in any particular area in Afghanistan, with the exception of urban users, who are found predominantly in Kabul city. The following profile of hashish users is based on the answers given by 774 men and 14 women who reported that they had used hashish in the past or were using hashish at the time of the survey. Of those users, 287 lived in provincial centres and 51 in rural areas. The average age of hashish users was 34 years, and the average length of time for which respondents had been using hashish was approximately 7 years. Around 75% of hashish users were married, whilst the remainder were single or, rarely (less than one per cent), widowed or divorced. Almost 55% of users had never attended school, although 1% had completed high school. Just over 15% of hashish users were unemployed. Most users (around 75%) worked in the private sector or as farmers. Some 15% of male hashish users reported that they were ex-combatants. Typically, male hashish users earned approximately AFA3,4 per month and spent an approximately monthly sum of AFA1,4 on hashish. Roughly 7% of users relied on their income from employment to purchase hashish. Some hashish users resorted to crime (four per cent) or begging (four per cent) to raise money. Approximately 4% of hashish users obtained their hashish exclusively from drug dealers. All hashish users reported that they obtained all or most of their hashish from drug dealers or friends. Around 15% of users reported that they produced hashish from their own crops. 1 This survey used the 32-province model. Thirty-four provinces are now officially recognized
30 Each hashish user consumed an average of 2.3 g of hashish per day, generally smoking the drug, although 3% said that they ate it. Ninety-three per cent of users consumed hashish at least once a day, and more than two thirds of users consumed hashish more than once a day. There are low correlations between the number of years a user has consumed hashish and user age (r=.13) or the quantity of hashish consumed (r=.8). It is estimated that between 4 and 55 metric tonnes of hashish are consumed in Afghanistan each year. No reliable estimate of Afghanistan s hashish production is available. Very few users gave a clear single answer as to why they began using hashish. The most common answers given were recreation and peer pressure. A small number of men also cited medicinal effects and family influence as reasons for beginning to use hashish % of hashish users as medicine curiosity easily available liked the effects peer pressure recreation other Figure 3.21: Reasons given for beginning to use hashish. Despite the fact that almost 8% of respondents reported using hashish for recreation, a high percentage of users (96%) reported at least one problem associated with their use of hashish, with 85% reporting multiple problems (Figure 3.22) criminal behaviour financial health social relations stigma Figure 3.23: Problems associated with hashish use
31 Approximately 78% of users reported financial problems and 75% reported health problems as a result of using hashish. Seventy-five per cent reported that they were trying to resolve their problems; twenty five per cent were seeking treatment. Almost 6% of hashish users reported that they had tried to stop using hashish in the past, although only 15% reported using multiple methods (Figure 3.24). 4 3 % of hashish users 2 1 home jail self detoxification treatment Figure 3.24: Methods used to give up hashish. 5 % of users who had tried to stop A few days 1 w eek 1 month 1 year >1 year Figure 3.25: Period of abstinence from hashish following treatment. This analysis of periods of abstinence was based on answers provided by hashish users who had tried only one method of treatment. No women reported being treated in jail. Home-based treatment was the least successful method in treating hashish use, whilst treatment at treatment centres was the most successful
32 % of hashish users who had sought treatment easily and cheaply available unemployment lack of f amily support no treatment facility pain (physical or psychological) peer pressure other Figure 3.26: Reasons given for resuming hashish use following treatment. A variety of reasons were given by drug users as to why they resumed hashish use following treatment (Figure 3.26). By far the most common reason for resuming use, given by over 6% of respondents, was physical or psychological pain. As in the case of all other drugs, the majority of male users cited peer pressure as a reason for their return to hashish use. Approximately 2% of hashish users reported that a close family member also used hashish. In all cases the family member in question was male (Figure 3.27) % of hashish users 1 5 brother father other Figure 3.27: Hashish users with family members who also use hashish. Poly-drug use is common among hashish users. Slightly less than 6% of men reported taking another drug in combination with hashish, particularly opium and alcohol
33 Pharmaceutical use (illicit use of pharmaceutical drugs) Pharmaceutical drugs (pharmaceuticals) include a wide variety of anxiolytic drugs, painkillers and hypnosedatives. Specifically, respondents mentioned Atarex, Diazepam, Dolantine, Librium, Mandrax, Pentacozine, and Sosegan. It is estimated that there are 18, pharmaceutical drug users in Afghanistan, of whom approximately 5% (9,) are male, 3% (6,) are female and 2% (3,) are children. Pharmaceuticals are the drugs most commonly used by women and children. Had only those estimates by female pharmaceutical users and female key informants been used to calculate the number of female pharmaceutical users in Afghanistan, the figure would be in the region of 18, women, i.e. twice the estimated number of male pharmaceutical users. Figure 3.28: Estimated numbers of pharmaceutical drug users, by province. Whilst pharmaceutical use is widespread across Afghanistan, Kabul and surrounding provinces are home to the highest concentration of drug users. A lower but nonetheless significant concentration of pharmaceutical users is found in the Balkh and Samangan provinces. Those concentrations are accounted for by both male and female users in urban and rural environments. It is suggested that pharmaceutical use is related to access to health care facilities. Anecdotal evidence suggests that many people first take pharmaceutical drugs under medical supervision and subsequently continue to take the same drugs without paying regular visits to doctors and without prescription, even when such use is no longer justified on medical grounds. The following profile of pharmaceutical users is based on the answers given by 231 men and 55 women who reported that they had used pharmaceuticals in the past or were doing so at the time of the survey. Of the total number of users, 118 lived in provincial centres and 168 in rural areas. The average age of female pharmaceutical users was 37 years, and the average length of time for which they had been using pharmaceuticals was 4 years. The corresponding statistics for male users were 34 years of age and 3 years, respectively. Approximately 75% of male pharmaceutical users were married and the remainder single or, rarely (less than 3%), widowed or divorced. Slightly more than 25% of female pharmaceutical users were widows. Almost 8% of female users and 5% of male users had never attended school, although 1% had completed high school. Slightly more than 25% of all 29 29
34 pharmaceutical users were unemployed. Most users (approximately 66%) worked in the private sector or as farmers. Some 15% of male pharmaceutical users reported that they were ex-combatants. Typically, pharmaceutical users earned approximately AFA3,3 per month, of which they spent approximately AFA1,2 on pharmaceuticals. Roughly 65% of users relied on their income from employment to purchase pharmaceuticals. Some pharmaceutical users resorted to crime (three per cent) or begging (three per cent) to raise money. Almost all pharmaceutical users obtained a proportion of their drugs from pharmacies (Figure 3.29). 1 % of pharmaceutical users bazaar family and friends other users pharmacy Figure 3.29: Source of pharmaceuticals. Whilst many drug users provided details of the quantities of pharmaceuticals that they used (i.e., number of tablets), they did not provide details of the type or doses of those drugs. It was recorded that 85% of users took pharmaceutical drugs on a daily basis. Nearly 2% of male pharmaceutical users reported injecting pharmaceuticals, and 55% of injecting users shared needles with other injecting drug users. No women reported injecting pharmaceuticals. The answer most commonly given for beginning to use pharmaceuticals was as medicine (Figure 3.3). 1 9 % of pharmaceutical users FEMALE MALE as medicine curiosity easily available liked the effects peer pressure recreation other Figure 3.3: Reasons given for beginning to use pharmaceuticals. 3 3
35 Men often gave multiple answers as to why they began using pharmaceuticals, but unlike other drug users did not consider peer pressure to be a significant factor. Nearly one third of men began using pharmaceutical drugs partly for recreation or because they liked the effects. Almost 96% of pharmaceutical users reported at least one problem associated with their use of pharmaceuticals, and 85% reported multiple problems (Figure 3.31). 9 8 % of pharmaceutical users FEMALE MALE criminal behaviour financial health social relations stigma Figure 3.31: Problems associated with pharmaceutical use. Approximately 72% of users reported financial problems, and 78% reported health problems. As in the case of other drug types, a high percentage of users reported first beginning to use a drug because of its supposed medicinal effects, but the same users subsequently reported health problems as a result of using the drug. Some 75% of users reported that they were trying to resolve their problems; 22% were seeking treatment. Nearly 55% of pharmaceutical users reported that they had tried to stop using pharmaceuticals in the past, though few reported using multiple methods (Figure 3.32). 5 % of pharmaceutical users FEMALE MALE home jail self detoxification treatment centre Figure 3.32: Methods used to give up pharmaceuticals
36 5 % of users who had tried to stop A few days 1 w eek 1 month 1 year >1 year Figure 3.33: Period of abstinence from pharmaceuticals following treatment. This analysis of periods of abstinence was based on answers given by pharmaceutical users who had tried only one method of treatment. No women reported stopping pharmaceutical drug use in jail. Home-based treatment was the least successful method in treating pharmaceutical use; treatment centres were the most successful FEMALE MALE easily and cheaply available unemployment lack of f amily support no t reat ment facility pain (physical or psychological) peer pressure ot her Figure 3.34: Reasons given for resuming use of pharmaceutical drugs following treatment. A variety of reasons were given by drug users as to why they resumed use of pharmaceuticals following treatment (Figure 3.34). By the far the most common reason given by almost 9% of respondents was physical or psychological pain. Whilst peer pressure was cited as an influence by male pharmaceutical users, it was not considered as important by male pharmaceutical users as by male users of other drugs. Approximately 18% of pharmaceutical users reported that a close family member also used pharmaceutical drugs. Considering the level of child pharmaceutical use estimated in this report, it was unexpected that only one pharmaceutical user should have reported a child in his family that also used drugs of this type. The family member most commonly identified as using pharmaceuticals was parent, mothers and fathers being equally represented in male and female drug user responses
37 15 % of pharmaceutical users 1 5 FEMALE MALE all family brother or sister child <5 yrs parent spouse other Figure 3.35: Users family members who also use pharmaceutical drugs. Poly-drug use was reported by just over 8% of male pharmaceutical drug users. The most common combination of drugs used was that of opium and hashish, reported by nearly 5% of male users. As in the case of female drug users in general, the level of poly-drug use among female pharmaceutical users (49%) was lower than that among male users. It is important to note that the survey did not ask users about poly-drug use as applicable to the combined use of different types of pharmaceuticals only. The few responses that clearly indicated the types of pharmaceuticals used also indicated that more than one type of pharmaceutical drug were often used]

38 Alcohol use It is estimated that there are 16, alcohol users in Afghanistan. Of that total, 14, (88%) are men, 2, (12%) are women and fewer than 1, are children. These results are based on all key informant and drug user responses. Unlike in the case of the other drugs studied so far in this report, had only those responses given by women been used to calculate the level of use among females, the estimated number of female users would be lower by around 2%, i.e. approximately 16, women. Figure 3.36: Estimated number of alcohol users, by province. Kabul city and nearby towns and villages account for 7% of alcohol users in Afghanistan. While alcohol users were concentrated to a lesser degree in northern Afghanistan, in a number of provinces particularly in southern provinces such as Kandarhar, Uruzgan and Zabul alcohol use was reported as negligible among men and non-existent among women. The following profile of alcohol users is based on the answers given by 262 men and 4 women who reported that they consumed alcohol. Of that total, 142 lived in provincial centres and 224 in rural areas. The average age of alcohol users was approximately 32 years, and the average length of time for which they had been consuming alcohol was 5 years. Some 75% of alcohol users were married; the remainder were single. Almost 33% of users had never attended school, whereas nearly 25% had completed high school. Slightly more than 17% of all alcohol users were unemployed. Nearly 5% of users worked in the private sector, and 13% of male users reported that they were ex-combatants. Typically, alcohol users earned approximately AFA4, per month, of which they spent around AFA3, on alcohol. Some 75% of users relied on their income from employment to purchase alcohol; 22% borrowed money from family members. Very few alcohol users resorted to crime (3%) or begging (1.5%) to raise money, and all of that number were poly-drug users. Almost 8% of users purchased some of their alcohol from drug dealers; 5% purchased some of their alcohol from shops. It is not known whether those drug dealers who sell alcohol also sell other drugs. Alcohol users commonly gave vague and/or contradictory answers when asked about their consumption of alcohol, typically reporting that they consumed one to three glasses per week 34 34
39 yet at the same time describing their intake as twice daily. The few clear answers given indicate that 7% of users consume alcohol only once a day or less frequently, generally one or two glasses on each occasion. When questioned regarding the type of alcohol consumed, the answers were more clear (Figure 3.37). 7 6 % of alcohol users beer home-brew vodka other Table 3.37: Type of alcohol consumed in Afghanistan. Nearly 3% of users reported consuming one type of alcohol only, typically vodka in urban areas and home-made alcoholic beverages in rural areas. The most common reasons given for beginning to consume alcohol were recreation, peer pressure and liked the effects (Figure 3.38) % of alcohol users as medicine curiosity easily available liked the effects peer pressure recreation other Figure 3.38: Reasons given for beginning to consume alcohol. Typically, alcohol users gave multiple answers as to why they began consuming alcohol, and, as in the case of many other drugs, peer pressure played an important role among men. Nearly 86% of alcohol users reported at least one problem associated with their consumption of alcohol; 8% reported multiple problems (Figure 3.39)
40 8 7 6 % of alcohol users criminal behaviour financial health social relations stigma Figure 3.39: Problems associated with alcohol consumption. Whilst only 54% of users reported health problems associated with their consumption of alcohol as compared to the higher corresponding percentages established for other drug categories, the proportion of users who reported social relationships and stigma as problems (64% and 56%, respectively) did not vary significantly from that of users of other drugs such as opiates. More than half of those users who reported problems associated with their consumption of alcohol said that they were trying to resolve those problems; 17% were seeking treatment. Slightly more than 4% of alcohol users reported that they had tried to give up alcohol in the past, although only 25% reported using multiple methods (Figure 3.4). 8 % of alcohol users who had sought treatment home jail self detoxification treatment centre Figure 3.4: Methods used to give up alcohol
41 6 % of users who had tried to stop A few days 1 w eek 1 month 1 year >1 year Figure 3.41: Period of abstinence from alcohol following treatment. This analysis of periods of abstinence was based on responses given by alcohol users who had tried only one method of treatment. Home-based treatment and self-detoxification were the most successful methods, although sample sizes were small (only 15 users tried selfdetoxification). % of users who had treid to stop using alcohol easily available lack of family support no treatment facility pain (physical or psychological) peer pressur unemployment other Figure 3.42: Reasons given for resuming alcohol consumption following treatment. A variety of reasons were given by drug users as to why they resumed alcohol consumption following treatment (Figure 3.42). By far the most common reason for resuming consumption was peer pressure, as reported by nearly 7% of respondents, which exceeds the percentage of users who gave peer pressure as a reason for beginning to consume alcohol. Approximately 16% of alcohol users reported that a close family member also used alcohol, in almost all cases a male family member, particularly brother(s) (13%) or father (2%). Poly-drug use was reported by slightly less than 8% of male alcohol users. Alcohol was predominantly combined with hashish as reported by nearly 65% of male users and also with opium, as reported by 5% of users. No female alcohol user reported using other drugs


42 Use of other drugs Other drugs most commonly reported were cough medicines; volatile liquids commonly petrol and glues, which are inhaled and/or consumed; various preparations derived from the cannabis plant and opium poppy capsules, such as barsh, bhangawa and majun; and a variety of locally sourced drugs, including preparations made from dried scorpions, snakes and wasps. It is estimated that there are 2, users of such drugs in Afghanistan, of whom 9, (45%) are men, 65, (33%) are women and 45, (22%) are children. These results are based on all key informant and drug user responses. Had only those responses given by female respondents been used to calculate the level of use of other drugs among females, the number of female users would be in the region of 17,. Figure 3.43: Estimated number of users of other drugs, by province. The use of other drugs was concentrated in Kabul and surrounding provinces, and in northern and western provinces. The following profile of users of other drugs is based on the answers given by 147 men and 25 women who said that they used other drugs; 56 lived in provincial centres and 119 in rural areas. The average age of users of other drugs was 34 years and the average length of time for which they had been using such drugs was 4.5 years. Approximately 76% of users of other drugs were married; the remainder were single (17%) or divorced (7%). Almost 5% of users had never attended school, although the corresponding figure among female users was 9%. Slightly less than 2% of users were unemployed. Nearly 45% worked in the private sector, and 3% were farmers. Around 13% of male users reported that they were excombatants. Typically, users of other drugs earned around AFA3, per month, of which they spent approximately AFA85 on such drugs. Almost 75% of those drug users who gave clear answers as to which other drugs they used said that they consumed cough syrup, whilst 2 per cent reported using solvents. Approximately 7% of users relied on their income from employment to purchase drugs; 45 per cent borrowed money from family members. Very few drug users resorted to crime (three per cent) or begging (three per cent) to raise money, and all of these were poly-drug users. Almost 93% of users purchased drugs from their local market; 4% reported that they obtained at least a proportion of their drugs from other users. Less than two per cent of users 38 38
43 reported purchasing drugs from drug dealers or pharmacies. Other users commonly gave vague answers when asked about their consumption of drugs. Common answers were whenever I cough or a few times a month. Even when users gave more specific answers, they tended not to specify the type or indicate the potency of the drugs that they were referring to. User responses indicate that some 75% of users consume such drugs at least once a day. The most common answer given for beginning to use other drugs was as medicine (Figure 3.44), as reported by 85% of drug users. The overwhelming majority of women gave this as their sole reason for beginning use % of other drug users as medicine curiosity easily available liked the effects peer pressure recreation other Figure 3.44: Reasons given for beginning to use other drugs. Nearly 84% of users of other drugs reported at least one problem associated with their use of drugs; 55% reported multiple problems (Figure 3.45) % of other drug users criminal behaviour financial health social relations stigma Figure 3.45: Problems associated with use of other drugs. More than 78% of users reported financial problems associated with their use of drugs, and almost 73% reported health problems. The proportion of those who reported social relationships and stigma as problems (35% and 24%, respectively) was significantly lower than that of users of drugs in other categories. More than 6% of those who reported problems associated with their use of other drugs said that they were trying to resolve those problems; 2% were seeking treatment
44 Slightly more than 43% of users of other drugs reported that they had tried to stop using drugs in the past; one third reported using multiple methods (Figure 3.46). % of all other drug users who had sought treatment home jail self detoxification treatment center Figure 3.46: Methods used to give up other drugs. 5 % of users who had tried to stop A few days 1 w eek 1 month 1 year >1 year Figure 3.47: Period of abstinence from other drugs following treatment. This analysis of periods of abstinence was based on answers given by users of other drugs who had tried only one method of treatment. Home-based treatment and self-detoxification were the most successful methods, although sample sizes were small (eight had tried selfdetoxification and six had been treated in treatment centres). 4 4
45 easily and cheaply available lack of family support no treatment facility pain (physical or psychological) peer pressure unemployment other Figure 3.48: Reasons given for resuming use of other drugs following treatment. As in the case of all drug types, male users gave a variety of reasons as to why they resumed use of other drugs following treatment (Figure 3.48). By far the most common reason for resuming use was pain relief, as reported by 95% of respondents and given by all female users as the only reason. Almost 42% of users of other drugs reported that a close family member also used drugs, and often entire families used the same drug. This proportion was the highest among all drug categories. 2 % of other drug users all family brother or sister child <5 years parent spouse Figure 3.49: Users family members who also use other drugs. Poly-drug use was reported by 95% of users of other drugs, although poly-drug use among females was slightly lower at 8%. Men combined other drugs predominantly with hashish, as reported by 67% of male users, whilst 44% of women reported using other drugs in combination with opium
46 Trends in drug use in Afghanistan Although there have been no previous nationwide estimates of drug use in Afghanistan, with respect to the number of drug users in Kabul city the results of this survey can be compared to a survey conducted by UNODC in 23 1, which used a similar methodology to estimate that number (Table 3.3) Change Opium 1,8 24, +22% Heroin 7, 16,5 +235% Hashish 24, 63,5 +265% Pharmaceuticals 14,3 12, -16% Alcohol 6,6 81, +12% Table 3.3: Lowest estimated number of drug users in 23 and 25 in Kabul city, and per cent difference (change) shown as percentage. Note: Estimates for 25 include children under 15 years of age. Except in the case of pharmaceuticals, the percentage change in the number of drug users from 23 to 25 concurs with estimates provided by drug treatment workers in Kabul. Earlier in this report it was noted that pharmaceutical use among women is likely to be a significant underestimate. This may explain the decrease in the estimated number of pharmaceutical drug users between 23 and 25. The percentage changes seen in Kabul city cannot be applied to other areas in Afghanistan, since regional variations were identified in key informants responses during this survey. Key informants were asked whether the number of drug users in their communities had increased or decreased, but drug users themselves were not asked that question. The majority of informants considered numbers to be increasing in all drug categories (Table 3.4). Number of key Decrease Increase informants Opium 951 8% 92% Heroin 487 6% 94% Hashish 115 7% 93% Pharmaceuticals 387 8% 92% Alcohol 479 3% 97% Other drugs 33 11% 89% Table 3.4: Trends in drug use as reported by key informants. There were some regional differences in perceptions among key informants as to the extent of change in drug use levels. Opium use in the Jawzjan and Sari Pul provinces in northern Afghanistan and in Paktika province in southern Afghanistan was considered by the majority of key informants living in those provinces to be decreasing; heroin use was also thought to be decreasing in Paktika; and pharmaceutical use was believed to be decreasing in Samangan province. There were no provinces where the majority of key informants considered hashish, alcohol or other drug use to be decreasing. In some villages within individual provinces, drug use was considered by all key informants to have decreased, and in provincial centres the majority of informants reported that drug use was decreasing in some districts. 1 UNDCP (23), Community Drug Profile #5 An Assessment of Problem Drug Use in Kabul City, UNDCP Programme, Islamabad, p
47 Urban and rural patterns of drug use It is estimated that 188, drug users live in urban areas in Afghanistan, 87% of whom are men, 1%1 per cent women, and 2% children under 15 years of age. A further 732, drug users live in rural areas, of whom 78% are men, 14% women, and 8% children. When considering these figures in conjunction with estimated urban and rural populations (Table 3.7), it becomes clear that men account for the overwhelming majority of the drug user community in Afghanistan. This is true of all categories of drugs, particularly heroin and alcohol in the case of urban male users and opium and hashish in the case of rural male users. Use of alcohol among urban women and use of pharmaceuticals and other drugs among their rural counterparts reflect most closely the overall percentage of female drug users in Afghanistan. Urban Rural Drug type Male Female Child Male Female Child National total Opium 27,36 5, ,172 1,682,3, ,869 Heroin 19,698 1, ,13 1, ,536 Hashish 82,93 2, ,294 5,948 2, ,84 Pharmaceuticals 9,418 6,14 1,585 82,458 51,34 28,42 178,945 Alcohol 79,94 9, ,854 9, ,376 Other drugs 6,826 4,15 1,688 86,31 6,3 44,597 23,437 Total 225,846 29,227 4, , ,911 79,255 1,27,247 Total, adjusted for poly-drug use 164, 21, 3, 575, 1, 57, 92, Table 3.5: Estimated number of urban and rural drug users. Urban Rural Drug Type Male Female Child Male Female Child Total Opium 18% 4% <1% 69% 7% 2% 1% Heroin 4% 4% <1% 53% 3% 1% 1% Hashish 16% <1% <1% 82% 1% 1% 1% Pharmaceuticals 5% 3% 1% 46% 29% 16% 1% Alcohol 49% 6% 1% 39% 6% <1% 1% Other Drugs 3% 2% 1% 42% 29% 22% 1% Table 3.6: Urban and rural drug users as percentage of users of each drug type. Population (million) % of national population Urban Rural Male Female Male Female Total % 1.5% 4.% 38.% 1% Table 3.7: Estimated population of Afghanistan in 25. In addition to differences in urban and rural patterns of drug use, substantial variation is found in drug use from province to province (Tables 3.8 and 3.9)
48 Province Opium Heroin Hashish Ph Alcohol Other Badakhshan <5 <5 5 <5 5 <5 Badghis <5 <5 <5 <5 <5 <5 Baghlan <5 <5 5 <5 <5 <5 Balkh <5 Bamyan <5 <5 <5 <5 <5 <5 Farah <5 <5 <5 <5 <5 <5 Faryab <5 15 <5 Ghazni <5 <5 5 <5 <5 <5 Ghor <5 <5 5 <5 5 <5 Herat 5 <5 1 <5 <5 <5 Hilmand <5 <5 <5 Jawzjan <5 <5 <5 <5 5 <5 Kabul Kandarhar <5 <5 <5 Kapisa <5 <5 <5 5 <5 <5 Khost <5 <5 <5 <5 <5 <5 Kunar <5 <5 5 <5 <5 <5 Kunduz <5 <5 5 <5 <5 <5 Laghman <5 <5 <5 <5 <5 <5 Logar <5 <5 <5 <5 <5 <5 Nangarhar <5 <5 5 <5 5 <5 Nimroz <5 <5 <5 <5 <5 5 Nuristan <5 <5 <5 <5 <5 <5 Paktika <5 <5 <5 <5 <5 <5 Paktya < <5 5 Parwan <5 Samangan <5 <5 <5 <5 <5 <5 Sari Pul <5 <5 <5 <5 <5 <5 Takhar <5 <5 <5 <5 <5 <5 Uruzgan <5 <5 5 <5 <5 <5 Wardak <5 <5 <5 <5 <5 <5 Zabul <5 <5 <5 <5 <5 <5 Table 3.8. Indicative number of drug users in urban areas, by province. In terms of absolute numbers, the overwhelming majority of urban drug users live in Kabul (Figure 3.5). Drug users are also concentrated in the cities of Chaharikar in Parwan province, Gardez in Paktya province, Maymana in Fayab province, Lashkar Gah in Hilmand province and Mazar-i-Sharif in Balkh province. The greatest number of rural drug users are found in rural areas of Kabul province. Users are also concentrated in a band of provinces stretching from northwest Kabul to Balkh province, and in a cluster of provinces in northwest Afghanistan, particularly along the country s borders with Iran and Turkmenistan
49 Province Opium Heroin Hashish Ph Alcohol Other Badakhshan 35 <5 9 <5 15 <5 Badghis Baghlan Balkh Bamyan 15 <5 55 <5 <5 <5 Farah 2 < Faryab Ghazni 35 <5 115 <5 <5 <5 Ghor Herat <5 Hilmand <5 <5 <5 Jawzjan 8 <5 1 1 <5 5 Kabul Kandarhar <5 5 Kapisa Khost 5 < Kunar <5 <5 55 <5 <5 5 Kunduz Laghman 45 < <5 22 Logar <5 <5 <5 Nangarhar 5 < <5 <5 Nimroz <5 5 Nuristan <5 <5 <5 <5 <5 5 Paktika 5 <5 13 <5 <5 <5 Paktya <5 < <5 2 Parwan 15 < <5 18 Samangan Sari Pul 15 < <5 Takhar 1 <5 3 <5 5 <5 Uruzgan <5 <5 Wardak 15 < Zabul <5 1 <5 <5 <5 <5 Table 3.9: Indicative number of drug users in rural areas, by province
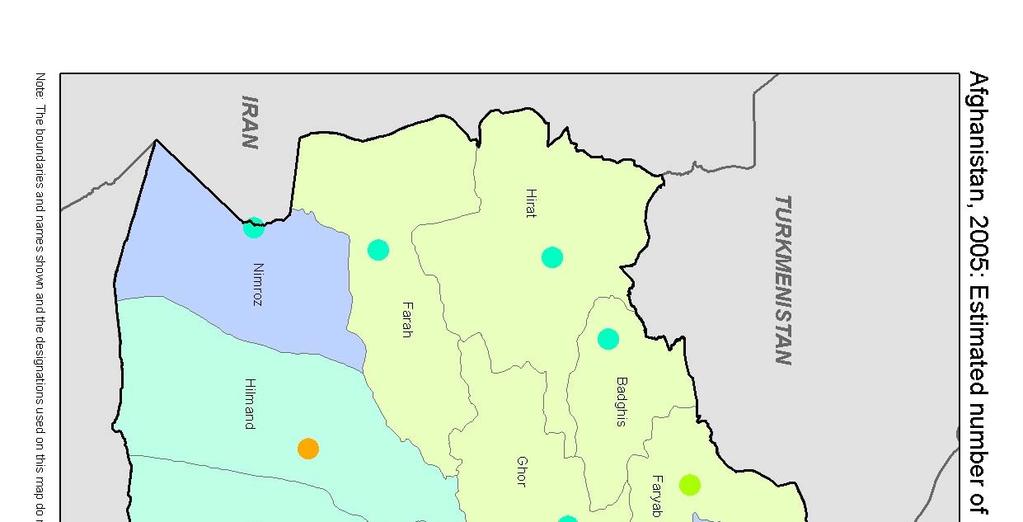
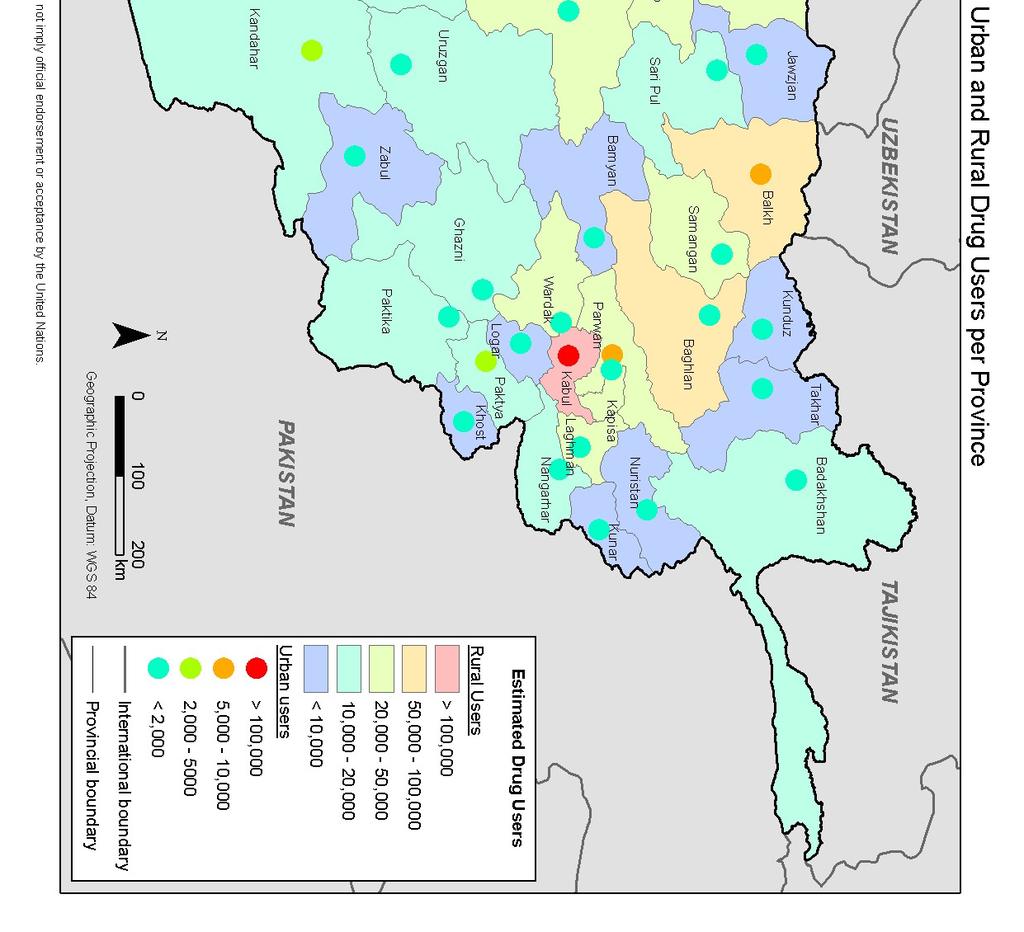
50
51 Drug use among females It is estimated that there are 12, adult female drug users in Afghanistan, which represents 2.1% of the female population. The drugs by far the most commonly used by women are pharmaceuticals (an estimated 6, users) and other drugs (65, users) such as cough syrups; poly-drug use is common, particularly the combined use of opium and pharmaceuticals. These figures are considered to be an underestimate of the true level of female drug use in Afghanistan for a number of reasons, most influential of which is the stigma associated with drug use in Afghanistan. This is thought to be the reason for underestimation overall, but appears to influence estimates by key informants and drug users of female drug use in particular.. As noted earlier in this report, patterns of female drug use reflect the fact that female users are able to conceal their use of drugs from the community inter alia by eating rather than smoking opium and consuming pharmaceuticals in tablet form rather than injecting them thus increasing the likelihood of underestimation. A further reason for underestimation is the difficulty in identifying female drug users; interviews alone may cause such users fear of exposure to family and community members. All interviews with women were carried out by female surveyors, and some areas could not be visited by women due to the poor security situation, particularly in southern Afghanistan. It was noted during the analysis of the survey results that men generally provided much lower estimates of female drug use in their communities than women, whilst male and female estimates of drug use among men did not vary significantly. Were only the responses of female key informants and drug users used to calculate the level of drug use among females in Afghanistan, the resulting estimates would be 45, opium users, 1, heroin users, 4, hashish users, 18, pharmaceutical users, 16, alcohol users, and 17, other drug users. Female informants estimate that 33, women in Afghanistan are poly-drug users. Few areas in Afghanistan were identified as having no female drug users (Figure 3.48). The majority of female drug users live in Kabul city and the surrounding rural areas of Kabul province. Most female opium users are found in Kabul, although significant numbers are also found in the northern provinces of Balkh, Faryab, Kunduz and Jawzjan, and smaller numbers in major poppy-growing provinces in western and southern Afghanistan, such as Hilmand, Hirat, Kandarhar and Nimroz. Outside of Kabul, and to a lesser degree in Balkh province, female heroin use is extremely rare; there was reported to be a small number of users located in Nimroz. Kabul and surrounding provinces such as Kapisa, Parwan and Paktya reported the highest levels of pharmaceutical use among women, and lower levels were estimated for Balkh, Jawzjan and Kunduz. Female alcohol and hashish use was rarely reported; Kabul city and province reported the highest levels. The greatest numbers of users of other drugs were reported in Kabul and Nimroz, and to a lesser degree in Kapisa. Quantities of drugs used and frequency of use were consistently lower among women than among men. Except in the case of heroin, the response most commonly given by female drug users to the question as to why they first took drugs was for the medicinal effect of the drug. Unlike male drug users, they rarely cited peer pressure, curiosity, or recreation as reasons for beginning to take drugs. Once women became regular drug users, the range of problems that they faced differed little from those experienced by men. Health and financial problems were common for all drug types, and problems in social relationships and stigma were also typically cited. Very few women reported criminal behaviour as a consequence of their use of drugs. In cases where women had tried to stop using drugs, physical or psychological pain was given by the overwhelming majority as their reason for resuming use. Whilst male drug users generally gave multiple reasons for resuming drug use following treatment, women were consistent in reporting pain as their reason, rarely citing easy availability, lack of treatment services or peer pressure

52 Figure 3.51: Female drug users in Afghanistan, by province

 or drugs classified in this survey as other drugs (45,).")

53 Child drug use It is estimated that 6, children under 15 years of age use drugs. However, since no children were interviewed during this survey, it is not possible to estimate that number accurately. The above figure is based on the assumption that the level of poly-drug use among children is the same as that among adults. Assuming that poly-drug use is rare among children, however, the number of child drug users is estimated at 85,, i.e., approximately one third higher. The majority of child drug users use either pharmaceuticals (3,) or drugs classified in this survey as other drugs (45,). Although absolute figures for child opiate use are low (approximately 5,), the level is still alarming. It is important to note that whilst estimates by drug users and key informants were used to calculate the number of child drug users, very few drug users reported a child drug user in their family. Some 12% of opium users mostly women and 6% of users of other drugs reported that a child in their family also used such drugs. It is clear from discussions with staff at treatment facilities that in nearly all cases children who use drugs have at least one parent that uses the same drug(s). Figure 3.52: Child drug users in Afghanistan, by province. As Figure 3.52 shows, the majority (85%) of child drug users live in Kabul city and surrounding rural areas. Smaller concentrations of child drug users are found in northern Afghanistan, particularly in the Balkh, Faryab and Jawzjan provinces. Child heroin use was not reported outside of Kabul, and hashish use was confined to Nimroz province. Pharmaceutical use was most common in Kabul and neighbouring Kapisa province, although above-average levels were also found in Jawzjan and Paktya provinces. Use of other drugs among children was most common in Nimroz, Kabul and Kapisa provinces
54 Drug use among ex-combatants Drug demand reduction workers in Kabul consider ex-combatants to be particularly susceptible to drug use. This perception, however, was not confirmed in this study. All drug users were asked whether they had been combatants during any of Afghanistan s conflicts since Table 3.1 shows the percentage of male drug users who responded affirmatively. Drug type per cent ex-combatants Opium 13.4 Heroin 16.1 Hashish 12.5 Pharmaceuticals 14.6 Alcohol 12.5 Other 13.1 Table 3.1: Percentage of drug users who are ex-combatants. An average 12.9% of male drug users were ex-combatants, although individual percentages ranged from 12.5% (hashish and alcohol users) to 16.1% (heroin users). A range of estimates is given for the number of ex-combatants in Afghanistan. The most common estimate of 1, 1 refers to the estimated number of men in private militias in 23. Such militias are the focus of disarmament activities by UNDP. The figure does not include men who fought in conflicts from 1979 onwards and may have disarmed before 23; no estimates of the number of such men could be found. No of illicit drug types used % of drug users interviewed 1 only 51 2 only 25 3 only 11 4 only 7 5 only 4 all 6 1 Table 3.11: Levels of poly-drug use among ex-combatants. The level of poly-drug use among ex-combatants did not differ significantly from that among the overall drug user population. There is no evidence from this survey to suggest that ex-combatants are more likely than other members of the community to be drug users. The pattern of drug use among excombatants does not differ from that among other drug users. 1 23, United Nations General Assembly: Disarmament, demobilization and reintegration. 5 5
55 Drug use among returned refugees Approximately 7.8 million Afghans have spent some time living as refugees in either Iran (1.7 million) or Pakistan (6.1 million). Of that number, some 8, have returned to Afghanistan from Iran and 3.5 million from Pakistan. On the basis of these figures it can be calculated that approximately.3% of the population of Afghanistan were formerly refugees in Iran, and 11.3% have lived as refugees in Pakistan. According to experienced demand reduction workers in Kabul, the level of drug use among returned refugees is much higher than that among the general population, and returnees began to use drugs while living as refugees. It would appear that, taken at face value, these statements are likely to be true, given levels of drug use in Iran and Pakistan. However, they should also be reflected in the number of drug users who themselves reported first using a drug while living as a refugee in either Iran or Pakistan. Of the 1393 drug users interviewed for this study, 18.6% (n=259) had spent time as refugees in Iran, and 17.2% (n=239) as refugees in Pakistan (Figures 3.53 and 3.54). These figures are far higher than corresponding percentages for non-drug users who have lived as refugees in either of those two countries. Percentages for men and women varied little. Much higher numbers of opium and heroin users had been refugees in Iran than in Pakistan. 6 5 % of drug users FEMALE MALE 1 refugee in Iran refugee in Pakistan never left this area other area of Afghanistan other countries no answer Figure 3.53: Responses to the question: Where did you live before your current location? Drug users were also asked where they had first used specific drugs (Figure 3.55). The responses given indicate that, except in the case of opium and heroin, few drug users first began using drugs in areas other than the location in which they were living at the time of the survey. A high proportion of opium and heroin users first began using those drugs in Iran (approximately 28% of users in both cases). The following may be concluded with regard to refugees only: Almost 85% of all opium users who had spent time as refugees in Iran (n=179) first used opium during that period, as compared to only 45% who began using the drug while refugees in Pakistan (n=7). Ninety per cent of all heroin users who had spent time as refugees in Iran (n=77) first used heroin during that period, as compared to only fifty per cent who began using the drug while refugees in Pakistan (n=38). Nearly 3% of all hashish users who had spent time as refugees in Iran (n=138) first used hashish during that period, as compared to 5% who began using the drug while refugees in Pakistan (n=168). Forty-one per cent of all pharmaceutical users who had spent time as refugees in Iran (n=61) or Pakistan (n=51) began using those drugs during that period. There were few cases in which users claimed to have begun using different drug types in different areas
56 6 % of drug users opium heroin hashish pharmaceuticals alcohol other refugee in iran refugee in pakistan never left this area other are in Afghanistan other countries Figure 3.54: Responses to the question: Where did you live before your current location? 9 8 % of drug users opium heroin hashish pharmaceuticals alcohol other Iran Pakistan this area of Afghanistan other area of Afghanistan other country Figure 3.55: Responses to the question: Where did you first use drugs? There is clear evidence to suggest that having been a refugee in either Iran or Pakistan leads to a higher likelihood of being a drug user. This is particularly true in the case of opiate use among those formerly refugees in Iran. Whilst such users represent approximately 2% of the general population, they account for almost 3% of opium and heroin users. The situation regarding those who lived as refugees in Pakistan is more complex. Despite the fact that this group accounts for a large proportion of drug users, particularly hashish users, few reported using drugs for the first time in Pakistan. It would appear that some aspect of having been a refugee in Pakistan leads to an increased level of drug use following return to Afghanistan. There is no evidence from this survey to indicate that levels of drug use were high among those who left Afghanistan to become refugees in Pakistan before they did so. Given that approximately 5% of those who left Afghanistan to live as refugees are yet to return, and that the Office of the United Nations High Commissioner for Refugees (UNHCR) expects the rate of return to increase in the coming years, it can be expected that the level of drug use in Afghanistan will drastically increase during that period. Current treatment services already fall severely short of demand, a situation that is expected to worsen whilst demand reduction activities are not expected to increase sufficiently to address that shortfall effectively
57 Injecting drug use among opium, heroin and pharmaceutical drug users in Afghanistan A total of 1393 drug users were questioned regarding their opium, heroin and pharmaceutical drug use, including the methods that they used to consume those drugs, whether they injected the drug, and whether they shared their needles with other drug users. The responses are shown in Table Number of users interviewed Number of IDU Number of IDU sharing needles Opium Heroin Pharmaceuticals Table 3.12: Summary of drug users responses to questions regarding injecting drug use (IDU). Women claimed not to have injected drugs. For a number of injecting drug users, the sex was not recorded, it is likely that they were males. Slightly more than 1% of opium 1 users, 14% of heroin users and 16% of pharmaceutical users reported injecting those drugs. Many injecting users also reported also using other methods: for example, all injecting opium users reported that they also smoked the drug. The level of needle-sharing varied across drug types. Among injecting drug users, 9% of opium users, 7% of heroin users and 25% of pharmaceutical users reported sharing needles with other drug users. The combination of these figures with nationwide estimates of numbers of opium, heroin and pharmaceutical drug users and levels of poly-drug use produces an estimate of 19, injecting drug users in Afghanistan. This figure includes 2, opium users, 7, heroin users and 18, pharmaceutical users. Assuming that the pattern of drug use among those interviewed accurately represents the overall pattern of drug use, an estimated 8, injecting drug users share needles in Afghanistan. An on-going seroprevalence study among injection drug users is being conducted through the Central Polyclinic in Kabul. Preliminary data indicates that measurable prevalence of HIV, syphilis, and hepatitis B and C exist among this group. Due to the cross-sectional nature of this study, the sample may not be representative of all IDU in Kabul. However, when final results are available, the information will provide some indication of existing infection in this environment with high rates of needle-sharing. 1 It was previously thought that it was not possible to produce from raw opium a material suitable for injection without chemical refinement. However, experienced drug demand reduction workers are aware of a simple process used in Afghanistan that does produce a solution suitable for injecting use
58 Drug treatment facilities and services in Afghanistan Although demand for drug treatment facilities in Afghanistan has increased over the last 25 years, the resources and facilities available for such treatment are limited. This survey found that no more than 1 places were available at residential treatment centres throughout the country. Resources currently allocated to drug treatment activities are such that these programmes treat fewer than.25% of drug users in Afghanistan each year. The Government of Afghanistan and national and international organizations are implementing projects to address this issue. The Drug Demand Reduction Directorate of the Ministry of Counter-Narcotics is responsible for the overall coordination of demand reduction activities in Afghanistan. At present, treatment facilities and services are offered by the following organizations: UNODC Drug Demand Reduction Action Teams (DRATs); Ministry of Counter-Narcotics (MCN); Gesellschaft für Technische Zusammenarbeit (GTZ); Colombo Plan Drug Advisory Programme; Mental Health Hospital of the Ministry of Public Health; Aga Khan Foundation; Khatiz Organization for Rehabilitation (KOR); Nejat Centre; Welfare Association for the Development of Afghanistan (WADAN); Shahmat Centre 54 54

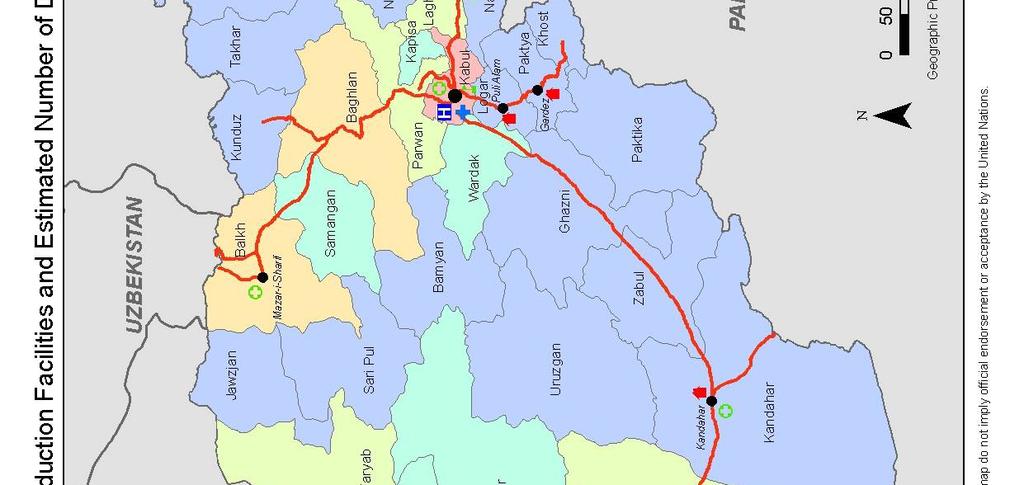

59 55 55
60 ANNEX A.1 Number and Location of Interviews UN Zone Province KIs DUs KIs DUs No of Villages KIs DUs Kabul Khost Logar Paktya Parwan Wardak Kapisa Kunar Laghman Nangarhar Nuristan Central West South North East North East Provincial Capital District Centre Villages Badakhshan Takhar Badghis Baghlan Balkh Bamyan Faryab Jawzjan Kunduz Samangan Sari Pul Ghazni Hilmand Kandarhar Paktika Uruzgan Zabul Farah Ghor Herat Nimroz Total Table A.1 Number of key informants (KIs) and drug users (DUs) interviewed
61 ANNEX A.2 Key Informants Questionnaire 57 57
62 58 58
63 59 59
64 ANNEX A.3 Drug Users Questionnaire 6 6
65 61 61
66 62 62
67 63 63
68 64 64
69 ANNEX A.4 Estimates of the number of drug users 65 65
70 ANNEX A.5 Estimation of the Number of Drug Users As all 32 province centers were visited by surveyors, no extrapolation is needed for urban figures given by drug users or key informants. For rural areas (districts and villages) drug user estimations were done at UN zone level for each drug type using: i = i i i i equation (1) Where DU i = Estimated number of drug users in zone i xi = Average number of users of drug i in sampled district centre Di = Total number of districts in zone i yi = Average number of users of drug i in sampled villages V = Total number of villages in zone i DU ( x * D) + ( y * V ) i The population of villages and district centers vary across each zone. Therefore a boot strap technique was used to calculate the total number of users for each drug category. This means, equation (1) was iterated 1, times and the average of all iterations was used to derive the final estimation figures. Adjustment for Poly-Drug Users By simply combining the total number of users of each drug type to arrive at an overall total number of drug users over represents the number of drug users, since an individual drug user may have been counted in the figures for more than one drug type (e.g. an opium user who also uses hashish and alcohol would be included three times in the combined total figure). Based on drug user s answers regarding their personal drug use patterns it was found that 54% of all drug users take only one drug type, and 27% of all drug users take a combination of 2 drug types. Table A.3 gives the percentage of all drug users that reported using combinations of 1 or more drug types. No. of illicit drug types used % of drug users interviewed 1 only 53% 2 only 27% 3 only 13% 4 only 5% 5 only 2% all 6 1% Table A.3 Polydrug use from drug users own patterns of use Using these percentages, the following formula was applied to the estimated total number of drug users, the estimated total number of male drug users, the estimated total number of female drug users and the estimated total number of child drug users: DU *.27 DU *.13 DU *.5 DU *.2 DU *.1 AT = DU * = DU*.727 equation (2) Where AT = adjusted estimate of drug users DU= total estimate of drug users While male and female drug users reported using different combinations of drug types, overall the percentages using one or more drug types were not significantly different
71 ANNEX B.1 Combinations of drugs used in Afghanistan (as reported by drug users). MALE USERS (n=1228) FEMALE USERS (n=122) Combinations Number of Number of % of users Combinations users users % of users Op Op He 51 4 He 8 7 Ha Ph Ph 43 4 Al 3 2 Al 53 4 Ot 5 4 Ot 11 1 Op+He 5 4 Op+He 23 2 Op+Ha 1 1 Op+Ha Op+Ph 8 7 He+Ha 25 2 Ph+Al 1 1 Op+Ph 2 2 Op+Ot 8 7 He+Ph 4 <1 He+Ot 2 2 Ha+Ph 18 1 Ha+Ot 1 1 Op+Al 7 1 Ph+Ot 4 3 He+Al 4 <1 Op+He+Ha 1 1 Ha+Al 37 3 OP+He+Ph 6 5 Ph+Al 3 <1 OP+Ha+Ph 3 2 Op+Ot 15 1 Op+Ph+Ot 2 2 He+Ot 5 <1 Ha+Ph+Ot 1 1 Ha+Ot 22 2 He+Ph+Ot 1 1 Ph+Ot 25 2 Op+He+Ha+Ph 1 1 Al+Ot 3 <1 Op+He+Ph+Ot 1 1 Op+He+Ha 38 3 OP+He+Ph 13 1 Op+He+Al 5 <1 Key Op+He+Ot 2 <1 Op = Opium OP+Ha+Ph 17 1 He = Heroin He+Ha+Ph 6 <1 Ha = Hashish Op+Ha+Al 52 4 Ph = Pharmaceutical drugs He+Ha+Al 1 <1 Al = Alcohol Op+Ha+Ot 6 <1 Ot = Other drugs Op+Ph+Al 1 <1 He+Ph+Al 1 <1 Ha+Ph+Al 6 <1 Op+Ph+Ot 2 <1 Ha+Ph+Ot 5 <1 He+Al+Ot 1 <1 Ha+Al+Ot 2 <1 Op+He+Ha+Ph 12 1 Op+He+Ha+Al 23 2 Op+He+Ha+Ot 4 <1 Op+He+Ph+Ot 2 <1 He+Ha+Ph+Al 7 1 Op+Ha+Ph+Al 2 <1 Op+Ha+Ph+Ot 6 <1 Op+Ha+Al+Ot 6 <1 He+Ha+Al+Ot 1 <1 Ha+Ph+Al+Ot 2 <1 Op+He+Ha+Ph+Al 12 1 Op+He+Ha+Ph+Ot 8 1 Op+He+Ha+Al+Ot 3 <1 Op+He+Ph+Al+Ot 1 <1 Op+Ha+Ph+Al+Ot 3 <1 He+Ha+Ph+Al+Ot 3 <1 Op+He+Ha+Ph+Al+Ot 9 1 Table B.1 Combinations of drugs used in Afghanistan (as reported by drug users)
 (1) 266-, Fax: +(43) (1)")
72 Vienna International Centre. PO Box 5, A 14 Vienna, Austria Tel: +(43) (1) 266-, Fax: +(43) (1) , Printed in Pakistan
MCN / UNODC Afghanistan Opium Price Monitoring April 2009
 April 20 Afghanistan Opium Price Monitoring Monthly Report Ministry of Counter Narcotics, Islamic Republic of Afghanistan, Kabul And United Nations Office on Drugs and Crime, Kabul 1 MCN / UNODC Afghanistan
April 20 Afghanistan Opium Price Monitoring Monthly Report Ministry of Counter Narcotics, Islamic Republic of Afghanistan, Kabul And United Nations Office on Drugs and Crime, Kabul 1 MCN / UNODC Afghanistan
Afghanistan. April Winter Rapid Assessment all regions. Phases 1 and 2
 Government of Afghanistan Ministry of Counter Narcotics Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Afghanistan Winter Rapid
Government of Afghanistan Ministry of Counter Narcotics Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Afghanistan Winter Rapid
ALTERNATIVE LIVELIHOODS DATABASE ANALYSIS REPORT
 Ministry of Counter Narcotics ALTERNATIVE LIVELIHOODS DATABASE ANALYSIS REPORT Alternative Livelihoods Investment and Opium Poppy Cultivation Trends 23-27 October 28 Contents Summary 4 1. Introduction
Ministry of Counter Narcotics ALTERNATIVE LIVELIHOODS DATABASE ANALYSIS REPORT Alternative Livelihoods Investment and Opium Poppy Cultivation Trends 23-27 October 28 Contents Summary 4 1. Introduction
The Paris Pact Initiative
 The Paris Pact Initiative A partnership to counter the trafficking and consumption of opiates originating in Afghanistan Drug Situation Analysis Report Islamic Republic of Afghanistan 2010 Report Abbreviations
The Paris Pact Initiative A partnership to counter the trafficking and consumption of opiates originating in Afghanistan Drug Situation Analysis Report Islamic Republic of Afghanistan 2010 Report Abbreviations
FACT SHEET AFGHANISTAN (ISLAMIC REPUBLIC OF)
") FACT SHEET AFGHANISTAN (ISLAMIC REPUBLIC OF) Borders: China: 76 km, Tajikistan: 1,206 km, Uzbekistan: 137 km, Turkmenistan: 744 km, I.R. of Iran: 936 km, Pakistan: 2,430 km (Durand line) Source: Annual
FACT SHEET AFGHANISTAN (ISLAMIC REPUBLIC OF) Borders: China: 76 km, Tajikistan: 1,206 km, Uzbekistan: 137 km, Turkmenistan: 744 km, I.R. of Iran: 936 km, Pakistan: 2,430 km (Durand line) Source: Annual
Afghanistan SEPTEMBER Survey of Commercial Cannabis Cultivation and Production 2011
 Government of Afghanistan Ministry of Counter Narcotics Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Survey of Commercial
Government of Afghanistan Ministry of Counter Narcotics Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Survey of Commercial
Press Conference 27 November Yury Fedotov, Executive Director, United Nations Office on Drugs and Crime (UNODC);
;") Press Conference PRESS CONFERENCE (near verbatim transcript) Yury Fedotov, Executive Director, United Nations Office on Drugs and Crime (UNODC); Jean-Luc Lemahieu, Country Representative for Afghanistan
Press Conference PRESS CONFERENCE (near verbatim transcript) Yury Fedotov, Executive Director, United Nations Office on Drugs and Crime (UNODC); Jean-Luc Lemahieu, Country Representative for Afghanistan
Afghanistan Opium Survey 2007
 Government of Afghanistan Ministry of Counter Narcotics Afghanistan Opium Survey 2007 Executive Summary August 2007 ABBREVIATIONS AEF ANP GPS ICMP MCN RAS UNODC Afghan Eradication Force Afghan National
Government of Afghanistan Ministry of Counter Narcotics Afghanistan Opium Survey 2007 Executive Summary August 2007 ABBREVIATIONS AEF ANP GPS ICMP MCN RAS UNODC Afghan Eradication Force Afghan National
GLOBAL POLIO ERADICATION INITIATIVE (GPEI) STATUS REPORT ANNEX 29 APRIL 2013
 STATUS REPORT ANNEX 29 APRIL 2013") GLOBAL POLIO ERADICATION INITIATIVE (GPEI) STATUS REPORT 29 APRIL 2013 ANNEX Table of Contents GPEI STRATEGIC PLAN 2010 2012 Milestones...1 GPEI STRATEGIC PLAN 2010 2012 Major Process Indicators...2 Afghanistan...2
GLOBAL POLIO ERADICATION INITIATIVE (GPEI) STATUS REPORT 29 APRIL 2013 ANNEX Table of Contents GPEI STRATEGIC PLAN 2010 2012 Milestones...1 GPEI STRATEGIC PLAN 2010 2012 Major Process Indicators...2 Afghanistan...2
CONCEPT NOTE Reducing Drug Demand and HIV in Afghanistan Time Frame: June 2010 July 2012
 Background CONCEPT NOTE Reducing Drug Demand and HIV in Afghanistan Time Frame: June 2010 July 2012 Drug abuse in Afghanistan was traditionally limited and customary bound. However due to internal and
Background CONCEPT NOTE Reducing Drug Demand and HIV in Afghanistan Time Frame: June 2010 July 2012 Drug abuse in Afghanistan was traditionally limited and customary bound. However due to internal and
The Drugs Scenario - Global, Regional and National
 The Drugs Scenario - Global, Regional and National 1. The growing demand for narcotic drugs and psychotropic substances in the world is being met by an increase in their production through a proliferation
The Drugs Scenario - Global, Regional and National 1. The growing demand for narcotic drugs and psychotropic substances in the world is being met by an increase in their production through a proliferation
Afghanistan Opium Survey 2011
 Islamic Republic of Afghanistan Ministry of Counter Narcotics Islamic Republic of Afghanistan Ministry of Counter Narcotics Banayee Bus Station, Jalalabad Main Road 9th District, Kabul, Afghanistan Tel.:
Islamic Republic of Afghanistan Ministry of Counter Narcotics Islamic Republic of Afghanistan Ministry of Counter Narcotics Banayee Bus Station, Jalalabad Main Road 9th District, Kabul, Afghanistan Tel.:
Government of Afghanistan. Counter Narcotics Directorate AFGHANISTAN. Opium Survey 2004
 Government of Afghanistan Counter Narcotics Directorate AFGHANISTAN Opium Survey 2004 November 2004 Abbreviations ICMP UNODC GPS CND UNODC Illicit Crop Monitoring Programme United Nations Office on Drugs
Government of Afghanistan Counter Narcotics Directorate AFGHANISTAN Opium Survey 2004 November 2004 Abbreviations ICMP UNODC GPS CND UNODC Illicit Crop Monitoring Programme United Nations Office on Drugs
AFGHAN OPIATE TRAFFICKING ALONG THE NORTHERN ROUTE
 AFGHAN OPIATE TRAFFICKING ALONG THE NORTHERN ROUTE Research I June 2018 II AFGHAN OPIATE TRAFFICKING ALONG THE NORTHERN ROUTE June 2018 III DISCLAIMERS This report has not been formally edited. The content
AFGHAN OPIATE TRAFFICKING ALONG THE NORTHERN ROUTE Research I June 2018 II AFGHAN OPIATE TRAFFICKING ALONG THE NORTHERN ROUTE June 2018 III DISCLAIMERS This report has not been formally edited. The content
World Drug Report 2017
 World Drug Report 2017 DEMAND Global trends in estimated number of drug users and people with drug user disorders, 2006-2015 Global trends in the estimated prevalence of drug use and prevalence of people
World Drug Report 2017 DEMAND Global trends in estimated number of drug users and people with drug user disorders, 2006-2015 Global trends in the estimated prevalence of drug use and prevalence of people
2007 WORLD DRUG REPORT
 2007 WORLD DRUG REPORT Preface Something new and significant is going on in the world drugs market. In last year's World Drug Report we made the argument that drug control is working and the world drug
2007 WORLD DRUG REPORT Preface Something new and significant is going on in the world drugs market. In last year's World Drug Report we made the argument that drug control is working and the world drug
Text of Anti Narcotics Policy 2010
 Text of Anti Narcotics Policy 2010 ISLAMABAD, Jul 14 (APP): The Federal Cabinet on Wednesday gave final approval to the Anti-Narcotics Policy 2010 that would follow its implementation. Following is the
Text of Anti Narcotics Policy 2010 ISLAMABAD, Jul 14 (APP): The Federal Cabinet on Wednesday gave final approval to the Anti-Narcotics Policy 2010 that would follow its implementation. Following is the
UNODC United Nations Office on Drugs and Crime. drugsmonitoring.unodc-roca.org
 UNODC ABOUT THE DRUGS MONITORING PLATFORM The Drugs Monitoring Platform is a unique global online tool for collecting, monitoring and sharing drug-related data. Initiated jointly by the Paris Pact Initiative,
UNODC ABOUT THE DRUGS MONITORING PLATFORM The Drugs Monitoring Platform is a unique global online tool for collecting, monitoring and sharing drug-related data. Initiated jointly by the Paris Pact Initiative,
NOVEMBER Afghanistan Opium Survey Cultivation and Production. Research. Islamic Republic of Afghanistan Ministry of Counter Narcotics
 Islamic Republic of Afghanistan Ministry of Counter Narcotics Afghanistan Opium Survey 2017 Cultivation and Production NOVEMBER 2017 Research MCN/NSD Narcotics Survey Directorate ACKNOWLEDGEMENTS The
Islamic Republic of Afghanistan Ministry of Counter Narcotics Afghanistan Opium Survey 2017 Cultivation and Production NOVEMBER 2017 Research MCN/NSD Narcotics Survey Directorate ACKNOWLEDGEMENTS The
AFGHANISTAN INTERPROVINCIAL OPIATE TRAFFICKING DYNAMICS
 ISLAMIC REPUBLIC OF AFGHANISTAN MINISTRY OF COUNTER NARCOTICS (MCN) AFGHANISTAN INTERPROVINCIAL OPIATE TRAFFICKING DYNAMICS November 2013 Acknowledgements The present study was prepared by the Research
ISLAMIC REPUBLIC OF AFGHANISTAN MINISTRY OF COUNTER NARCOTICS (MCN) AFGHANISTAN INTERPROVINCIAL OPIATE TRAFFICKING DYNAMICS November 2013 Acknowledgements The present study was prepared by the Research
AOTP UPDATE VOLUME 1. Acetic anhydride in the context of Afghan heroin
 AOTP UPDATE VOLUME 1 Acetic anhydride in the context of Afghan heroin Research 2018 AOTP About the AOTP Update Content About the Afghan Opiate Trade Project The opiates produced in Afghanistan continue
AOTP UPDATE VOLUME 1 Acetic anhydride in the context of Afghan heroin Research 2018 AOTP About the AOTP Update Content About the Afghan Opiate Trade Project The opiates produced in Afghanistan continue
KAZAKHSTAN. National Focal Point. Drug Abuse and Drug Dependence Treatment Situation. Territory : 2,717,300 km 2 Capital: Astana BASIC DATA
 KAZAKHSTAN Territory : 2,717,300 km 2 Capital: Astana Map No. 3771 Rev. 6 UNITED NATIONS January 2004 BASIC DATA Total population (millions) 2009 15.5* Population under age15 (as % of total) 2010 23.8*
KAZAKHSTAN Territory : 2,717,300 km 2 Capital: Astana Map No. 3771 Rev. 6 UNITED NATIONS January 2004 BASIC DATA Total population (millions) 2009 15.5* Population under age15 (as % of total) 2010 23.8*
FACT SHEET TAJIKISTAN (REPUBLIC OF)
") FACT SHEET TAJIKISTAN (REPUBLIC OF) Territory: 142,600 sq. km. Source: Tajikistan in Figures 2014, Agency on Statistics under the President of the Republic of Tajikistan, 2014 Borders: Afghanistan - 1,344
FACT SHEET TAJIKISTAN (REPUBLIC OF) Territory: 142,600 sq. km. Source: Tajikistan in Figures 2014, Agency on Statistics under the President of the Republic of Tajikistan, 2014 Borders: Afghanistan - 1,344
FACT SHEET 1 IRAN (ISLAMIC REPUBLIC OF)
") FACT SHEET 1 IRAN (ISLAMIC REPUBLIC OF) Territory: Borders: 1,648,195 sq. km. Azerbaijan (432 km/268 mi) and Armenia (35 km/22 mi) to the north-west; Turkmenistan (992 km/616 mi) to the north-east; Pakistan
FACT SHEET 1 IRAN (ISLAMIC REPUBLIC OF) Territory: Borders: 1,648,195 sq. km. Azerbaijan (432 km/268 mi) and Armenia (35 km/22 mi) to the north-west; Turkmenistan (992 km/616 mi) to the north-east; Pakistan
WORLD DRUG REPORT 2011
 WORLD DRUG REPORT 2011 EXECUTIVE SUMMARY Global developments in illicit drug consumption, production and trafficking Consumption Globally, UNODC estimates that, in 2009, between 149 and 272 million people,
WORLD DRUG REPORT 2011 EXECUTIVE SUMMARY Global developments in illicit drug consumption, production and trafficking Consumption Globally, UNODC estimates that, in 2009, between 149 and 272 million people,
OPIUM IN AFGHANISTAN. Prepared for: Connect Model United Nations 2012 United Nations Office on Drugs and Crime Director: Geena Lee INTRODUCTION
 UNITED NATIONS OFFICE ON DRUGS AND CRIME TOPIC A B ACKGROUNDER OPIUM IN AFGHANISTAN Prepared for: Connect Model United Nations 2012 United Nations Office on Drugs and Crime Director: Geena Lee INTRODUCTION
UNITED NATIONS OFFICE ON DRUGS AND CRIME TOPIC A B ACKGROUNDER OPIUM IN AFGHANISTAN Prepared for: Connect Model United Nations 2012 United Nations Office on Drugs and Crime Director: Geena Lee INTRODUCTION
Statistics on Drug Misuse: England, 2012
 Statistics on Drug Misuse: England, 2012 Copyright 2012, The Health and Social Care Information Centre. All Rights Reserved. Copyright 2012, The Health and Social Care Information Centre. All Rights Reserved.
Statistics on Drug Misuse: England, 2012 Copyright 2012, The Health and Social Care Information Centre. All Rights Reserved. Copyright 2012, The Health and Social Care Information Centre. All Rights Reserved.
Third Ministerial Conference of the Paris Pact Partners on Combating Illicit Traffic in Opiates Originating in Afghanistan. (Vienna, 16 February 2012)
") Third Ministerial Conference of the Paris Pact Partners on Combating Illicit Traffic in Opiates Originating in Afghanistan (Vienna, 16 February 2012) Vienna Declaration 1. The Paris Pact is one of the
Third Ministerial Conference of the Paris Pact Partners on Combating Illicit Traffic in Opiates Originating in Afghanistan (Vienna, 16 February 2012) Vienna Declaration 1. The Paris Pact is one of the
Social and Psychological Back-Ground of Drug Addicts Interviewed in Dublin
 Social and Psychological Back-Ground of Drug Addicts Interviewed in Dublin R. D. STEVENSON M.D., D.P.M. Consultant Psychiatrist St Brendan s Hospital, Lecturer in Psychiatry, R.C.S.I. A. CARNEY M.B., D.P.M.
Social and Psychological Back-Ground of Drug Addicts Interviewed in Dublin R. D. STEVENSON M.D., D.P.M. Consultant Psychiatrist St Brendan s Hospital, Lecturer in Psychiatry, R.C.S.I. A. CARNEY M.B., D.P.M.
Government of Afghanistan Ministry of Counter Narcotics. Afghanistan. Opium Winter Assessment
 Government of Afghanistan Ministry of Counter Narcotics Afghanistan Opium Winter Assessment January 2009 ABBREVIATIONS AGE Anti Government Elements GPS Global Positioning System ICMP Illicit Crop Monitoring
Government of Afghanistan Ministry of Counter Narcotics Afghanistan Opium Winter Assessment January 2009 ABBREVIATIONS AGE Anti Government Elements GPS Global Positioning System ICMP Illicit Crop Monitoring
Should Methadone and/or Buprenorphine be included in the WHO Model List of Essential Medicines? Reviewing evidence from Iranian experience.
 Should Methadone and/or Buprenorphine be included in the WHO Model List of Essential Medicines? Reviewing evidence from Iranian experience. MT Yasamy, MD * Essential drugs are those that satisfy the health
Should Methadone and/or Buprenorphine be included in the WHO Model List of Essential Medicines? Reviewing evidence from Iranian experience. MT Yasamy, MD * Essential drugs are those that satisfy the health
Drug Use Around the World
 Special Agents U.S. DRUG ENFORCEMENT AGENCY STAFFING AND BUDGETS 1975 2000 10000 5000 Total Employees 8000 6000 4000 3000 2000 4000 1975 1980 1985 1990 1995 2000 1000 1975 1980 1985 1990 1995 2000 Support
Special Agents U.S. DRUG ENFORCEMENT AGENCY STAFFING AND BUDGETS 1975 2000 10000 5000 Total Employees 8000 6000 4000 3000 2000 4000 1975 1980 1985 1990 1995 2000 1000 1975 1980 1985 1990 1995 2000 Support
MYANMAR. Emerging trends and concerns
 MYANMAR MYANMAR Emerging trends and concerns Myanmar remains a major source of methamphetamine pills and opiates in South-East Asia, most of which are manufactured in Shan State in the eastern part of
MYANMAR MYANMAR Emerging trends and concerns Myanmar remains a major source of methamphetamine pills and opiates in South-East Asia, most of which are manufactured in Shan State in the eastern part of
Drug Money: the illicit proceeds of opiates trafficked on the Balkan route. Executive summary
 Drug Money: the illicit proceeds of opiates trafficked on the Balkan route Executive summary 2015 Executive summary The cultivation, production and trafficking of illicit opiates accounted for almost
Drug Money: the illicit proceeds of opiates trafficked on the Balkan route Executive summary 2015 Executive summary The cultivation, production and trafficking of illicit opiates accounted for almost
United Nations International Drug Control Programme Country Office for Afghanistan
 United Nations International Drug Control Programme Country Office for Afghanistan Afghanistan Preliminary Findings for the Opium Ground Survey of Northern Provinces May 2002 Illicit Crop Monitoring Programme
United Nations International Drug Control Programme Country Office for Afghanistan Afghanistan Preliminary Findings for the Opium Ground Survey of Northern Provinces May 2002 Illicit Crop Monitoring Programme
Global drug trends and sustainable development
 Lau Global drug trends and sustainable development Chloé Carpentier Chief, Drug Research Section UNODC Göteborg, 15 November 2017 Global trends in estimated number of drug users and people with drug user
Lau Global drug trends and sustainable development Chloé Carpentier Chief, Drug Research Section UNODC Göteborg, 15 November 2017 Global trends in estimated number of drug users and people with drug user
Introduction Overview of the status quo
 Introduction Whenever we learn that a government has prohibited the use or sale of certain goods, there is one thing we can be sure of - sooner or later, people willing to break the law will take advantage
Introduction Whenever we learn that a government has prohibited the use or sale of certain goods, there is one thing we can be sure of - sooner or later, people willing to break the law will take advantage
FACT SHEET IRAN (ISLAMIC REPUBLIC OF)
") FACT SHEET IRAN (ISLAMIC REPUBLIC OF) Territory: Borders: 1,648,195 sq. km. Azerbaijan (432 km/268 mi) and Armenia (35 km/22 mi) to the north-west; Turkmenistan (992 km/616 mi) to the north-east; Pakistan
FACT SHEET IRAN (ISLAMIC REPUBLIC OF) Territory: Borders: 1,648,195 sq. km. Azerbaijan (432 km/268 mi) and Armenia (35 km/22 mi) to the north-west; Turkmenistan (992 km/616 mi) to the north-east; Pakistan
Statement of the Executive Director UNODC on International Day against Drug Abuse and Illicit Trafficking
 Statement of the Executive Director UNODC on International Day against Drug Abuse and Illicit Trafficking 26 June 2013 The International Day against Drug Abuse and Illicit Trafficking is a suitable day
Statement of the Executive Director UNODC on International Day against Drug Abuse and Illicit Trafficking 26 June 2013 The International Day against Drug Abuse and Illicit Trafficking is a suitable day
Understanding Afghanistan s Poppy Economy. Najmuddin Shaikh
 Understanding Afghanistan s Poppy Economy Najmuddin Shaikh The Afghanistan Essays This 2018 short-essay series by the Jinnah Institute (JI) reflects a range of Pakistani thought leadership on Afghanistan
Understanding Afghanistan s Poppy Economy Najmuddin Shaikh The Afghanistan Essays This 2018 short-essay series by the Jinnah Institute (JI) reflects a range of Pakistani thought leadership on Afghanistan
WORLD DRUG REPORT. Volume 2: Statistics
 WORLD DRUG REPORT Volume 2: Statistics 2004 WORLD DRUG REPORT Volume 2: Statistics The Office for Drug Control and Crime Prevention (UNODCCP) became the Office on Drugs and Crime (UNODC) on 1 October
WORLD DRUG REPORT Volume 2: Statistics 2004 WORLD DRUG REPORT Volume 2: Statistics The Office for Drug Control and Crime Prevention (UNODCCP) became the Office on Drugs and Crime (UNODC) on 1 October
1.1 Overview Evolution of the World Drug Problem
 1.1 Overview 1.1.1 Evolution of the World Drug Problem Vigilance is needed to respond to year-onyear expansion in some market sectors The long-term stabilization which occurred in drug markets continued
1.1 Overview 1.1.1 Evolution of the World Drug Problem Vigilance is needed to respond to year-onyear expansion in some market sectors The long-term stabilization which occurred in drug markets continued
Annex A: Estimating the number of people in problem debt while being treated for a mental health crisis
 Annex A: Estimating the number of people in problem debt while being treated for a mental health crisis A.1 Estimating the number of referrals to NHS crisis response teams in England per year Unfortunately
Annex A: Estimating the number of people in problem debt while being treated for a mental health crisis A.1 Estimating the number of referrals to NHS crisis response teams in England per year Unfortunately
Development of a Village Based Treatment Model for Afghanistan
 Development of a Village Based Treatment Model for Afghanistan Tay Bian How 1, Morales Brian 2, V. Thirumagal 3, Muhammad Ayub 4. 1 Asian Centre for Certification and Education of Addiction Professionals
Development of a Village Based Treatment Model for Afghanistan Tay Bian How 1, Morales Brian 2, V. Thirumagal 3, Muhammad Ayub 4. 1 Asian Centre for Certification and Education of Addiction Professionals
PRICES AND MARKET INTERACTIONS IN THE OPIUM ECONOMY
 PRICES AND MARKET INTERACTIONS IN THE OPIUM ECONOMY William A. Byrd and Olivier Jonglez 1 I. INTRODUCTION Given the enormous economic importance and development implications of drugs in Afghanistan, 2
PRICES AND MARKET INTERACTIONS IN THE OPIUM ECONOMY William A. Byrd and Olivier Jonglez 1 I. INTRODUCTION Given the enormous economic importance and development implications of drugs in Afghanistan, 2
Giving and Volunteering in Quebec
 Giving and Volunteering in Quebec Results from the 1997 National Survey of Giving, Volunteering and Participating Michelle Goulbourne Research Associate Canadian Centre for Philanthropy www.nsgvp.org Giving
Giving and Volunteering in Quebec Results from the 1997 National Survey of Giving, Volunteering and Participating Michelle Goulbourne Research Associate Canadian Centre for Philanthropy www.nsgvp.org Giving
NATIONAL COMMITTEE ON AIDS, DRUGS AND PROSTITUTE CONTROL OF VIETNAM
 NATIONAL COMMITTEE ON AIDS, DRUGS AND PROSTITUTE CONTROL OF VIETNAM CEREMONY FOR THE PUBLIC ANNOUNCEMENT OF THE STRATEGY ON PREVENTING, COMBATING AND CONTROLLING DRUG ABUSE IN VIETNAM TILL 2020 AND ORIENTATION
NATIONAL COMMITTEE ON AIDS, DRUGS AND PROSTITUTE CONTROL OF VIETNAM CEREMONY FOR THE PUBLIC ANNOUNCEMENT OF THE STRATEGY ON PREVENTING, COMBATING AND CONTROLLING DRUG ABUSE IN VIETNAM TILL 2020 AND ORIENTATION
: UNODC Cooperation on Drugs and Crime in the Islamic Republic of Iran
 History and Achievements 1999-2004: Beginning of UNODC Cooperation with the Islamic Republic of Iran The United Nations Office on Drugs and Crime in the Islamic Republic of Iran established a country office
History and Achievements 1999-2004: Beginning of UNODC Cooperation with the Islamic Republic of Iran The United Nations Office on Drugs and Crime in the Islamic Republic of Iran established a country office
COUNCIL OF THE EUROPEAN UNION. Brussels, 6 December /02 CORDROGUE 103
 COUNCIL OF THE EUROPEAN UNION Brussels, 6 December 2002 15349/02 CORDROGUE 103 NOTE From : Presidency To : European Council No. prev. doc. : 12451/3/02 CORDROGUE 80 REV 3 Subject : Note from the Council
COUNCIL OF THE EUROPEAN UNION Brussels, 6 December 2002 15349/02 CORDROGUE 103 NOTE From : Presidency To : European Council No. prev. doc. : 12451/3/02 CORDROGUE 80 REV 3 Subject : Note from the Council
Findings on FMD in Afghanistan and Pakistan
 Findings on FMD in Afghanistan and Pakistan Giancarlo Ferrari Project Coordinator GTFS/INT/907/ITA Controlling Trans-boundary Animal Diseases in Central Asian countries AGAH/EMPRES FAO Outline of the presentation
Findings on FMD in Afghanistan and Pakistan Giancarlo Ferrari Project Coordinator GTFS/INT/907/ITA Controlling Trans-boundary Animal Diseases in Central Asian countries AGAH/EMPRES FAO Outline of the presentation
OPIUM GLOBAL ILLICIT CULTIVATION OF OPIUM POPPY AND PRODUCTION OF OPIUM, CULTIVATION (1) IN HECTARES POTENTIAL PRODUCTION IN METRIC TONS
 IN HECTARES POTENTIAL PRODUCTION IN METRIC TONS") 3. PRODUCTION 3. Production: Opium/heroin 3.1 Opium/heroin OPIUM GLOBAL ILLICIT CULTIVATION OF OPIUM POPPY AND PRODUCTION OF OPIUM, 1990-2003 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
3. PRODUCTION 3. Production: Opium/heroin 3.1 Opium/heroin OPIUM GLOBAL ILLICIT CULTIVATION OF OPIUM POPPY AND PRODUCTION OF OPIUM, 1990-2003 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Holas, Jakub et al. Regionální kriminalita a její odraz v kvalitě života obyvatel Regional crime and its impact on quality of life Summary
 Holas, Jakub et al. Regionální kriminalita a její odraz v kvalitě života obyvatel Regional crime and its impact on quality of life ISBN 978-80-7338-160-8 Summary The aim of the project (whose results are
Holas, Jakub et al. Regionální kriminalita a její odraz v kvalitě života obyvatel Regional crime and its impact on quality of life ISBN 978-80-7338-160-8 Summary The aim of the project (whose results are
The science of the mind: investigating mental health Treating addiction
 The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
Summary Report - IBBS Balochistan - Quetta Round 1, ROUND 1 SUMMARY REPORT -BALOCHISTAN QUETTA
 ROUND 1, 5-6 SUMMARY REPORT - BALOCHISTAN NATIONAL AIDS CONTROL PROGRAM BALOCHISTAN AIDS CONTROL PROGRAM CANADA PAKISTAN HIV/AIDS SURVEILLANCE PROJECT May 6 5-6 ROUND 1 SUMMARY REPORT -BALOCHISTAN QUETTA
ROUND 1, 5-6 SUMMARY REPORT - BALOCHISTAN NATIONAL AIDS CONTROL PROGRAM BALOCHISTAN AIDS CONTROL PROGRAM CANADA PAKISTAN HIV/AIDS SURVEILLANCE PROJECT May 6 5-6 ROUND 1 SUMMARY REPORT -BALOCHISTAN QUETTA
Cover photograph: Rebirth NGO Camp, Islamic Republic of Iran, Alessandro Scotti
 November 2008 Work in Progress Preventing and Treating Opiates Addiction and HIV/AIDS Epidemics in Afghanistan and Neighbouring Countries Opium This document is part of the UNODC s Rainbow Strategy which
November 2008 Work in Progress Preventing and Treating Opiates Addiction and HIV/AIDS Epidemics in Afghanistan and Neighbouring Countries Opium This document is part of the UNODC s Rainbow Strategy which
What is harm reduction?
 What is harm reduction? The International Harm Reduction Association (IHRA) defines harm reduction as the policies, programmes and practices that aim to reduce the harms associated with the use of psychoactive
What is harm reduction? The International Harm Reduction Association (IHRA) defines harm reduction as the policies, programmes and practices that aim to reduce the harms associated with the use of psychoactive
Statistics on Drug Misuse: England, 2007
 Statistics on Drug Misuse: England, 2007 Summary For the first time, this annual statistical bulletin presents information on drug misuse among both adults and children. The topics covered include: Prevalence
Statistics on Drug Misuse: England, 2007 Summary For the first time, this annual statistical bulletin presents information on drug misuse among both adults and children. The topics covered include: Prevalence
Taking away the chaos The health needs of people who inject drugs in public places in Glasgow city centre
 Taking away the chaos The health needs of people who inject drugs in public places in Glasgow city centre Plain-language summary The health needs of people who inject drugs in public places in Glasgow
Taking away the chaos The health needs of people who inject drugs in public places in Glasgow city centre Plain-language summary The health needs of people who inject drugs in public places in Glasgow
Global market for synthetic stimulants expanding
 (d) Cross-cutting issues: new challenges, threats and realities in preventing and addressing the world drug problem in compliance with relevant international law, including the three drug control conventions;
(d) Cross-cutting issues: new challenges, threats and realities in preventing and addressing the world drug problem in compliance with relevant international law, including the three drug control conventions;
Statistics on Drug Misuse: England, 2008
 Statistics on Drug Misuse: England, 2008 Summary This annual statistical report presents information on drug misuse among both adults and children. It includes a focus on young adults. The topics covered
Statistics on Drug Misuse: England, 2008 Summary This annual statistical report presents information on drug misuse among both adults and children. It includes a focus on young adults. The topics covered
Opiate flows through Northern Afghanistan and Central Asia: a threat assessment
 Opiate flows through Northern Afghanistan and Central Asia: a threat assessment ACKNOWLEDGEMENTS... 2 GLOSSARY:... 3 INTRODUCTION... 4 KEY FINDINGS... 4 EXECUTIVE SUMMARY... 6 METHODOLOGY... 13 I. OPIATE
Opiate flows through Northern Afghanistan and Central Asia: a threat assessment ACKNOWLEDGEMENTS... 2 GLOSSARY:... 3 INTRODUCTION... 4 KEY FINDINGS... 4 EXECUTIVE SUMMARY... 6 METHODOLOGY... 13 I. OPIATE
Economic and Social Council COMMISSION ON NARCOTIC DRUGS ANNUAL REPORT QUESTIONNAIRE FOR 2015
 United Nations Economic and Social Council Distr.: Limited 29 December 2010 Original: English COMMISSION ON NARCOTIC DRUGS ANNUAL REPORT QUESTIONNAIRE FOR 2015 PART II COMPREHENSIVE APPROACH TO DRUG DEMAND
United Nations Economic and Social Council Distr.: Limited 29 December 2010 Original: English COMMISSION ON NARCOTIC DRUGS ANNUAL REPORT QUESTIONNAIRE FOR 2015 PART II COMPREHENSIVE APPROACH TO DRUG DEMAND
The International Relations of the Narcotics Trade through Afghanistan and Central Asia
 Meeting Summary: Russia and Eurasia Programme The International Relations of the Narcotics Trade through Afghanistan and Central Asia This event was held under the Chatham House Rule. 7 March 2012 The
Meeting Summary: Russia and Eurasia Programme The International Relations of the Narcotics Trade through Afghanistan and Central Asia This event was held under the Chatham House Rule. 7 March 2012 The
JSNA Substance Misuse
 JSNA Substance Misuse Introduction 9.1. Substance misuse causes less damage to health in absolute population terms than tobacco or alcohol. However, its association with crime and antisocial behaviour
JSNA Substance Misuse Introduction 9.1. Substance misuse causes less damage to health in absolute population terms than tobacco or alcohol. However, its association with crime and antisocial behaviour
ARTF RESULTS STORIES 2016
 ARTF RESULTS STORIES 2016 PROVIDING QUALITY HEALTH SERVICES IN AFGHANISTAN Afghanistan Reconstruction Trust Fund PROVIDING QUALITY HEALTH SERVICES IN AFGHANISTAN The System Enhancement for Health Action
ARTF RESULTS STORIES 2016 PROVIDING QUALITY HEALTH SERVICES IN AFGHANISTAN Afghanistan Reconstruction Trust Fund PROVIDING QUALITY HEALTH SERVICES IN AFGHANISTAN The System Enhancement for Health Action
Injecting Equipment Provision in Scotland Survey 2011/12
 Publication Report Injecting Equipment Provision in Scotland Survey 25 June 2013 An Official Statistics Publication for Scotland Contents Introduction... 2 Key points... 3 Results and Commentary... 4 1.
Publication Report Injecting Equipment Provision in Scotland Survey 25 June 2013 An Official Statistics Publication for Scotland Contents Introduction... 2 Key points... 3 Results and Commentary... 4 1.
Trends in treated problem cannabis use in the seven health board areas outside the Eastern Regional Health Authority, 1998 to 2002
 Drug Misuse Resear ch Divisio n Contents - Summary - Glossary of terms - Introduction - Methods - Analysis Trends in treated problem cannabis use in the seven health board areas outside the Eastern Regional
Drug Misuse Resear ch Divisio n Contents - Summary - Glossary of terms - Introduction - Methods - Analysis Trends in treated problem cannabis use in the seven health board areas outside the Eastern Regional
Developing a drug monitoring system for New Zealand: IDMS
 Developing a drug monitoring system for New Zealand: IDMS 2006-2016 NDEWS webinar "Examining Global Drug Early Warning Systems 26 th September 2017 Chris Wilkins SHORE & Whariki Research Centre College
Developing a drug monitoring system for New Zealand: IDMS 2006-2016 NDEWS webinar "Examining Global Drug Early Warning Systems 26 th September 2017 Chris Wilkins SHORE & Whariki Research Centre College
Stigmatization & Media
 Stigmatization of People with Addictive Disorders Stigmatization & Media According to the 2018 World Drug Report (1) of the UN Office on Drugs and Crime (UNODC), About 275 million people worldwide, which
Stigmatization of People with Addictive Disorders Stigmatization & Media According to the 2018 World Drug Report (1) of the UN Office on Drugs and Crime (UNODC), About 275 million people worldwide, which
EMBARGOED UNTIL 22 JUNE PM CEST (GMT+2)
") FACT SHEET ON STATISTICS AND TRENDS IN ILLICIT DRUGS Global estimates of drug use All illicit drug use Problem drug use** Annual prevalence (%)* 5.3 (3.3-7.3) 0.6 (0.3-0.9) Number of users (millions)*
FACT SHEET ON STATISTICS AND TRENDS IN ILLICIT DRUGS Global estimates of drug use All illicit drug use Problem drug use** Annual prevalence (%)* 5.3 (3.3-7.3) 0.6 (0.3-0.9) Number of users (millions)*
American Farm Bureau Federation Polling Presentation October 31, 2017
 American Farm Bureau Federation Polling Presentation October 31, 2017 Key Points One in three rural adults say there is a great deal of stigma associated with opioid abuse in their local community. Relatedly,
American Farm Bureau Federation Polling Presentation October 31, 2017 Key Points One in three rural adults say there is a great deal of stigma associated with opioid abuse in their local community. Relatedly,
World Drug Report 2018 Methodology Report. Research and Trend Analysis Branch UNODC, Vienna
 World Drug Report 2018 Methodology Report Research and Trend Analysis Branch UNODC, Vienna Table of Contents 1. Introduction... 1 Sources of information... 1 2. Data on drug use and health consequences
World Drug Report 2018 Methodology Report Research and Trend Analysis Branch UNODC, Vienna Table of Contents 1. Introduction... 1 Sources of information... 1 2. Data on drug use and health consequences
FACT SHEET BOSNIA AND HERZEGOVINA
 FACT SHEET BOSNIA AND HERZEGOVINA Territory: 51,209 sq km Borders: 1,459 km (Croatia 932 km, Serbia 312 km, Montenegro 215 km) Estimated population (thousands) 2012 2013 2014 2015 2016 Total 3,828 3,824
FACT SHEET BOSNIA AND HERZEGOVINA Territory: 51,209 sq km Borders: 1,459 km (Croatia 932 km, Serbia 312 km, Montenegro 215 km) Estimated population (thousands) 2012 2013 2014 2015 2016 Total 3,828 3,824
REGIONAL HIGHLIGHTS AFRICA AMERICAS. Central America and the Caribbean. INTERNATIONAL NARCOTICS CONTROL BOARD Report 2017
 REGIONAL HIGHLIGHTS AFRICA Increase in drug use: while Africa remains a key transit region for drug trafficking, the use of various types of drugs, including cocaine, opioids, amphetamine-type stimulants,
REGIONAL HIGHLIGHTS AFRICA Increase in drug use: while Africa remains a key transit region for drug trafficking, the use of various types of drugs, including cocaine, opioids, amphetamine-type stimulants,
Project for Alternative Livelihoods in Eastern Afghanistan (PAL)
") Project for Alternative Livelihoods in Eastern Afghanistan (PAL) 1 Understanding Rural Livelihoods and Addressing the Causes of Opium Poppy Cultivation in Eastern Afghanistan Abridged Version 1. Introduction
Project for Alternative Livelihoods in Eastern Afghanistan (PAL) 1 Understanding Rural Livelihoods and Addressing the Causes of Opium Poppy Cultivation in Eastern Afghanistan Abridged Version 1. Introduction
Table of Contents. 3. Programme Support IV. ONGOING AND PLANNED ASSISTANCE OF GLOBAL PROJECTS Drafted by A. Mancini, F.
 PROGRAMME IIN AFGHANIISTAN Aprri ill 2010 Table of Contents I. PROGRAMME SUMMARY... 3 II. OVERVIEW OF UNODC PROJECTS IN AFGHANISTAN... 5 III. ONGOING AND PLANNED ASSISTANCE OF NATIONAL AND REGIONAL PROJECTS...
PROGRAMME IIN AFGHANIISTAN Aprri ill 2010 Table of Contents I. PROGRAMME SUMMARY... 3 II. OVERVIEW OF UNODC PROJECTS IN AFGHANISTAN... 5 III. ONGOING AND PLANNED ASSISTANCE OF NATIONAL AND REGIONAL PROJECTS...
South Asian Cocktail The Predominant Drug Use Pattern in Nepal and its Association with Spread of HIV
 14 Original Article South Asian Cocktail The Predominant Drug Use Pattern in Nepal and its Association with Spread of HIV Ojha S P 1, Sigdel S 2, H-G M 3, Verthein U 4 1 Tribhuvan University Teaching Hospital,
14 Original Article South Asian Cocktail The Predominant Drug Use Pattern in Nepal and its Association with Spread of HIV Ojha S P 1, Sigdel S 2, H-G M 3, Verthein U 4 1 Tribhuvan University Teaching Hospital,
Annual Reports Questionnaire (ARQ) Part III: Extent, patterns and trends in drug use
 Part III: Extent, patterns and trends in drug use") Annual Reports Questionnaire (ARQ) Part III: Extent, patterns and trends in drug use Report of the Government of: Reporting Year: Completed on (date): Please return completed questionnaire to: arq@unodc.org
Annual Reports Questionnaire (ARQ) Part III: Extent, patterns and trends in drug use Report of the Government of: Reporting Year: Completed on (date): Please return completed questionnaire to: arq@unodc.org
The Role for Alternative Development Strategies in Opium Eradication
 The Role for Alternative Development Strategies in Opium Eradication Elimination of opium poppy cultivation, shifting cultivation and poverty are ranked as national priorities. Laos is presently the third
The Role for Alternative Development Strategies in Opium Eradication Elimination of opium poppy cultivation, shifting cultivation and poverty are ranked as national priorities. Laos is presently the third
Outcomes Monitoring System Iowa Project
 Outcomes Monitoring System Iowa Project Year Six Report Prepared By: Iowa Consortium for Substance Abuse Research and Evaluation University of Iowa, Iowa City, Iowa 52242-5000 With Funds Provided By: Iowa
Outcomes Monitoring System Iowa Project Year Six Report Prepared By: Iowa Consortium for Substance Abuse Research and Evaluation University of Iowa, Iowa City, Iowa 52242-5000 With Funds Provided By: Iowa
FACT SHEET SERBIA (REPUBLIC OF)
") FACT SHEET SERBIA (REPUBLIC OF) Territory: Borders: 88,509 sq. km 2,362 km (total) Hungary: 175 km, Romania: 548 km, Bulgaria: 361 km, FYR of Macedonia: 283 km, Albania: 114 km, Montenegro: 249 km, Bosnia
FACT SHEET SERBIA (REPUBLIC OF) Territory: Borders: 88,509 sq. km 2,362 km (total) Hungary: 175 km, Romania: 548 km, Bulgaria: 361 km, FYR of Macedonia: 283 km, Albania: 114 km, Montenegro: 249 km, Bosnia
Dark Sides of the J&K
 World Overview on Drugs Dark Sides of the J&K About 275 million people worldwide, which is roughly 5.6 per cent of the global population aged 15 64 years, used drugs at least once during 2016. Some 31
World Overview on Drugs Dark Sides of the J&K About 275 million people worldwide, which is roughly 5.6 per cent of the global population aged 15 64 years, used drugs at least once during 2016. Some 31
Youth Opioid Study: Attitudes and Usage Young Adults Ages 18 to 24 in the United States
 Youth Opioid Study: Attitudes and Usage Young Adults Ages 18 to 24 in the United States Conducted for: Presented on: April 30, 2015 Conducted by: www.qmarketresearch.com Page 1 Contents Background... 3
Youth Opioid Study: Attitudes and Usage Young Adults Ages 18 to 24 in the United States Conducted for: Presented on: April 30, 2015 Conducted by: www.qmarketresearch.com Page 1 Contents Background... 3
The transnational threat of Afghan opium. Executive summary
 Addiction, crime and insurgency The transnational threat of Afghan opium Executive summary Copyright United Nations Office on Drugs and Crime (UNODC), October 2009 Acknowledgements This report was prepared
Addiction, crime and insurgency The transnational threat of Afghan opium Executive summary Copyright United Nations Office on Drugs and Crime (UNODC), October 2009 Acknowledgements This report was prepared
Dr. dr. Diah Setia Utami, SpKJ, MARS Deputy of Rehabilitation Narcotic National Board of Republic of Indonesia
 Dr. dr. Diah Setia Utami, SpKJ, MARS Deputy of Rehabilitation Narcotic National Board of Republic of Indonesia Growing evidence in changing of usage, from natural plant substances to synthetic substances
Dr. dr. Diah Setia Utami, SpKJ, MARS Deputy of Rehabilitation Narcotic National Board of Republic of Indonesia Growing evidence in changing of usage, from natural plant substances to synthetic substances
Epidemiology of non medical use of prescription drugs. Kamran Niaz, Survey and Statistics Section, Policy Analysis and Research Branch
 Epidemiology of non medical use of prescription drugs Kamran Niaz, Survey and Statistics Section, Policy Analysis and Research Branch Monitoring of the drug use situation: Annual reports questionnaire
Epidemiology of non medical use of prescription drugs Kamran Niaz, Survey and Statistics Section, Policy Analysis and Research Branch Monitoring of the drug use situation: Annual reports questionnaire
IOM - Humanitarian Assistance Programme
 IOM - Humanitarian Assistance Programme Weekly Report Period: Week Starting Date Week Ending Date 08 August 2018 14 August 2018 Submission Date: 15 August 2018 Cumulative Highlights (Verified Data on the
IOM - Humanitarian Assistance Programme Weekly Report Period: Week Starting Date Week Ending Date 08 August 2018 14 August 2018 Submission Date: 15 August 2018 Cumulative Highlights (Verified Data on the
SOCIAL ATTITUDES TO HOMELESSNESS. A Student Survey of Cambridge Residents
 SOCIAL ATTITUDES TO HOMELESSNESS A Student Survey of Cambridge Residents March 2014 Attitudes to Homelessness: A Survey of Cambridge Residents Wednesday 19th February 2014 This report presents the findings
SOCIAL ATTITUDES TO HOMELESSNESS A Student Survey of Cambridge Residents March 2014 Attitudes to Homelessness: A Survey of Cambridge Residents Wednesday 19th February 2014 This report presents the findings
Intervention from the World Health Organization
 Thematic discussion on the implementation of the UNGASS outcome document Operational recommendations on Demand reduction and related measures, including prevention and treatment, as well as other health-related
Thematic discussion on the implementation of the UNGASS outcome document Operational recommendations on Demand reduction and related measures, including prevention and treatment, as well as other health-related
Using Rapid Assessment and Response Methodology: Waterloo Region's Experience Ontario Harm Reduction Distribution Program Conference
 Using Rapid Assessment and Response Methodology: Waterloo Region's Experience Ontario Harm Reduction Distribution Program Conference February 12, 2013 Before we begin Who has completed, or been involved
Using Rapid Assessment and Response Methodology: Waterloo Region's Experience Ontario Harm Reduction Distribution Program Conference February 12, 2013 Before we begin Who has completed, or been involved
SYNTHESIS REPORT. The Impact and Effectiveness of Various Counter Narcotics Media Campaigns
 SYNTHESIS REPORT The Impact and Effectiveness of Various Counter Narcotics Media Campaigns October 2008 CONTENTS SUMMARY 4 1. BACKGROUND 8 2. OBJECTIVES AND METHODOLOGY 8 3. ANALYSIS 9 3.1 Phase I: Assessment
SYNTHESIS REPORT The Impact and Effectiveness of Various Counter Narcotics Media Campaigns October 2008 CONTENTS SUMMARY 4 1. BACKGROUND 8 2. OBJECTIVES AND METHODOLOGY 8 3. ANALYSIS 9 3.1 Phase I: Assessment
Drug problems in Dublin
 Symposium Gerald Bury MRCPI, MRCGP Lecturer in General Practice, Royal College of Surgeons in Ireland, Department of General Practice, Dublin, Ireland Drug problems in Dublin Despite some evidence of a
Symposium Gerald Bury MRCPI, MRCGP Lecturer in General Practice, Royal College of Surgeons in Ireland, Department of General Practice, Dublin, Ireland Drug problems in Dublin Despite some evidence of a
Needle and Syringe Programs - 17 October 2013
 Needle and Syringe Programs - 17 October 2013 ANCD Position Paper: Needle and Syringe Programs MEDIA RELEASE 17 October 2013 The Australian National Council on Drugs (ANCD) has today released a position
Needle and Syringe Programs - 17 October 2013 ANCD Position Paper: Needle and Syringe Programs MEDIA RELEASE 17 October 2013 The Australian National Council on Drugs (ANCD) has today released a position
The data were expressed as descriptive frequencies and percentages.
 173 32 6 9 2 6 9 Drug and alcohol abuse among university students is a major cause for concern. Use of illegal substances may be associated with a deterioration in personal and social life, especially
173 32 6 9 2 6 9 Drug and alcohol abuse among university students is a major cause for concern. Use of illegal substances may be associated with a deterioration in personal and social life, especially
PH52. Audit tool for the implementation of. NICE public health guidance 52 Needle and syringe programmes
 PH52 Audit tool for the implementation of NICE public health guidance 52 Needle and syringe programmes Introduction This audit tool has been developed to help you audit implementation of, and compliance
PH52 Audit tool for the implementation of NICE public health guidance 52 Needle and syringe programmes Introduction This audit tool has been developed to help you audit implementation of, and compliance
LIMITED OPIUM YIELD ASSESSMENT SURVEYS. Technical report: Observations and findings
 SCIENTIFIC AND TECHNICAL NOTES SCITEC/19 December 23 LIMITED OPIUM YIELD ASSESSMENT SURVEYS Technical report: Observations and findings Guidance for future activities prepared by Laboratory and Scientific
SCIENTIFIC AND TECHNICAL NOTES SCITEC/19 December 23 LIMITED OPIUM YIELD ASSESSMENT SURVEYS Technical report: Observations and findings Guidance for future activities prepared by Laboratory and Scientific
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Drug Misuse: opiate detoxification of drug misusers in the community, hospital and prison. 1.1 Short title Drug misuse detoxification
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Drug Misuse: opiate detoxification of drug misusers in the community, hospital and prison. 1.1 Short title Drug misuse detoxification
Running Head: LEGALIZATION OF MARIJUANA 1 LEGALIZATION OF RECREATIONAL MARIJUANA IN CALIFORNIA
 Running Head: LEGALIZATION OF MARIJUANA 1 LEGALIZATION OF RECREATIONAL MARIJUANA IN CALIFORNIA By Name Course Tutor s Name Institution Date LEGALIZATION OF MARIJUANA 2 Legalization of Recreational Marijuana
Running Head: LEGALIZATION OF MARIJUANA 1 LEGALIZATION OF RECREATIONAL MARIJUANA IN CALIFORNIA By Name Course Tutor s Name Institution Date LEGALIZATION OF MARIJUANA 2 Legalization of Recreational Marijuana
POLICY, LEGISLATION, ECONOMIC ANALYSIS AND MEDIA COVERAGE. Last data available Indicator (sphere)
") POLICY, LEGISLATION, ECONOMIC ANALYSIS AND MEDIA COVERAGE Amendments in laws and legal regulations number 8 2 NDC Expenditures for activities against drugs and drug addictions in Bulgaria [1] BGN 1 102
POLICY, LEGISLATION, ECONOMIC ANALYSIS AND MEDIA COVERAGE Amendments in laws and legal regulations number 8 2 NDC Expenditures for activities against drugs and drug addictions in Bulgaria [1] BGN 1 102
MYANMAR SEX WORK & HIV MYANMAR SEX WORK & HIV
 e SEX WORK & HIV SEX WORK & HIV Myanmar, formerly known as Burma, has a population of 50 million people [1]. The estimated nation wide population of sex workers in 2007 was between 40,000 and 80,000 and
e SEX WORK & HIV SEX WORK & HIV Myanmar, formerly known as Burma, has a population of 50 million people [1]. The estimated nation wide population of sex workers in 2007 was between 40,000 and 80,000 and