HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
|
|
|
- Anna Craig
- 5 years ago
- Views:
Transcription
1 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
2 AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened for HCV [1] HCV candidacy nearly universal [2] HIV coinfection creates unique considerations for pts with HCV, particularly potential drug interactions between HCV and HIV antivirals Even with potent HIV ARVs, pts with HIV/HCV coinfection are at increased risk for rapidly progressive liver disease [2] HIV ARV therapy is not a substitute for HCV treatment [2] 1. DHHS guidelines. October AASLD/IDSA. HCV guidance. September Slide credit: clinicaloptions.com
3 HBV Reactivation HBV reactivation reported in HCV mono-infected persons not on anti- HBV treatment Therefore all persons with prior HBV should be on anti-hbv therapy prior to HCV treatment
4 Pre-Treatment Questions HCV genotype/ subtype Stage of fibrosis Cirrhosis Y/N Decompensated Y/N Method Liver biopsy Transient elastography Fibrosure Prior HCV Treatment Response DAA usage Prior side effects Immunization status HIV HIV drug resistance Medication Child Bearing Potential Ribavirin
5 HCV DAAs Target Steps of HCV Life Cycle Inhibitor Class Suffix Examples Targeting HCV Protein Processing NS3/4A protease [1] -PREVIR Targeting HCV Replication NS5B polymerase [2] -BUVIR NS5A [3] -ASVIR Glecaprevir, grazoprevir, paritaprevir, simeprevir, voxilaprevir Nucleotide: sofosbuvir Nonnucleoside: dasabuvir Daclatasvir, elbasvir, ledipasvir, ombitasvir, pibrentasvir, velpatasvir 1. McCauley JA, et al. Curr Opin Pharmacol. 2016;30: Eltahla AA, et al. Viruses. 2015;7: Gitto S, et al. J Viral Hepat. 2017;24: Slide credit: clinicaloptions.com
6 AASLD/IDSA Recommendations for First-line HCV Treatment in HIV/HCV Coinfection Regimen by HCV GT 1, 4 2, 3 5, 6 Duration, Wks No Cirrhosis Compensated Cirrhosis egfr < 30 ml/min 8 GLE/PIB -- GLE/PIB 12 GZR/EBR,* SOF/LDV, SOF/VEL GLE/PIB, GZR/EBR,* SOF/LDV, SOF/VEL GZR/EBR 8 GLE/PIB -- GLE/PIB 12 SOF/VEL GLE/PIB, SOF/VEL -- 8 GLE/PIB -- GLE/PIB 12 SOF/LDV, SOF/VEL GLE/PIB, SOF/LDV, SOF/VEL *If GT1a with BL NS5A RASs for EBR, 12 wks not recommended; can increase duration to 16 wks with RBV (alternative). Some data to support 8 wks in GT1, but 8 wks not recommended in HIV/HCV coinfection. If decompensated cirrhosis, do not use HCV protease inhibitors. If BL Y93H RAS present in GT3, add RBV or consider SOF/VEL/VOX. If also cirrhotic, increase duration to 12 wks. -- AASLD/IDSA. HCV guidance. September Slide credit: clinicaloptions.com
7 Is HCV Treatment Different in the Setting of HIV/HCV Coinfection? Per AASLD/IDSA, treatment in HIV/HCV-coinfected pts should be the same as in HCV monoinfected pts, after consideration of potential drug drug interactions between DAAs and ARVs [1] Efficacy Across Separate Studies of GT1-6 HCV Infection With GLE/PIB, GZR/EBR, SOF/LDV, or SOF/VEL HCV Monoinfection [2-5] N = 146 to 624 SVR 95% to 99% HIV/HCV Coinfection [6-9] N = 75 to 218 SVR 95% to 98% Sustained HCV Virologic Response (%)* *Most data reported for these studies from treatment-naive pts with GT1/4 HCV infection receiving 12-wk regimens. References in slidenotes. Slide credit: clinicaloptions.com
8 Case Presentation-1 A 46y M with h/o IDU, now clean for many years Diagnosed in 2011 HIV On TDF/FTC and boosted atazanavir HCV GT 1a Treatment naïve Was not treated till now because he was afraid of side effects
9 Case Presentation-1, Contd HIV VL < 40, CD4-456 cells/cu mm HCV VL- 9 million copies/ml GT 1a HBV ve, surface antibody + Creatinine- 0.9, AST-51, ALT-60, Bilirubin-1.3
10 HIV/HCV Drug Drug Interactions ARV(s) GLE/PIB GZR/EBR SOF/LDV SOF/VEL SOF/VEL/VOX ATV + (RTV or COBI) X X * * X DRV + (RTV or COBI) X X * * * LPV + RTV X X * * X EFV X X * X X RPV * DTG * RAL EVG/COBI/FTC/TDF * X X * * EVG/COBI/FTC/TAF X 3TC/ABC TAF TDF * * * *Monitor for tenofovir toxicity if used with TDF. No clinically significant drug interaction per prescribing information; AASLD/IDSA and DHHS guideline recommend monitoring liver enzymes owing to lack of clinical safety data. DHHS guidelines. October Slide credit: clinicaloptions.com
11 Principles of Regimen Switching in Virologically Suppressed Pts Review ART history for prior intolerance or HIV virologic failure Review HIV resistance test results If prior HIV resistance uncertain, consider switch only if new regimen likely to maintain suppression of resistant virus In pts with HIV/HBV coinfection, continue ARVs active against HBV (even if not needed for HIV suppression) (TAF or TDF) plus (3TC or FTC) Switches usually maintain HIV suppression if no resistance to drugs in new regimen Check HIV-1 RNA during first 3 mos after switch to ensure suppression Boosted PI or INSTI monotherapy not recommended DHHS guidelines. October Slide credit: clinicaloptions.com
12 Does Switching ART Affect Likelihood of HCV Cure? Real-world, single-center, cohort study of HIV/HCV-coinfected pts treated with DAAs (N = 255) Change in ART No Change in ART n/n = 72/78 n/n = 174/ P = Pts Achieving SVR (%) Falade-Nwulia O, et al. Hepatology. 2017;66: Slide credit: clinicaloptions.com
13 Case-1 Continued Option #1 Pick HCV that does not interact with ARV LDV/SOF SOF/VEL Option #2 Switch ARV RAL RPV DTG Wait 4 wks to ensure pt is tolerating new ART and HIV-1 RNA remains suppressed prior to starting HCV treatment
14 Case-2 A 28 y F with well controlled HIV TDF/FTC/RPV Was treated with 12 weeks of SOF/LDV GT1a HCV VL rebounds at 4 weeks post treatment CD4-574, GT 1a, HCV resistance NS3: wild type NS5a: Y93H
15 AASLD/IDSA Recommendations for HCV Treatment of DAA-Experienced Pts HCV GT Duration, Wks 1 12 NS3 + PegIFN/RBV Experience GLE/PIB, SOF/LDV,* SOF/VEL Non-NS5A, SOF- Containing Experience GLE/PIB, SOF/VEL, SOF/VEL/VOX 2 12 GLE/PIB, SOF/VEL NS5A Experience SOF/VEL/VOX 3 12 SOF/VEL/VOX SOF/VEL/VOX SOF/VEL/VOX SOF/VEL/VOX SOF/VEL/VOX SOF/VEL/VOX *Not recommended if also cirrhotic. For genotype 1b only. For genotype 1a only. If also cirrhotic with prior NS5A failure, add RBV. AASLD/IDSA. HCV guidance. September Slide credit: clinicaloptions.com
16 Is Resistance Testing Needed When Retreating Pts Who Failed DAA-Containing Regimens? Regimen GLE/PIB RAS testing not recommended SOF/LDV SOF/VEL AASLD/IDSA RAS Testing Recommendations for Treatment-Experienced Pts Consider for pts with GT1a HCV; if significant resistance present, add RBV (and extend duration, if cirrhotic) or select a different regimen Recommended for pts with GT3 HCV; if Y93H mutation present, add RBV SOF/VEL/VOX RAS testing not recommended AASLD/IDSA. HCV guidance. September Slide credit: clinicaloptions.com
17 HIV/HCV Drug Drug Interactions ARV(s) SOF/VEL/VOX ATV + (RTV or COBI) X DRV + (RTV or COBI) * LPV + RTV X EFV X RPV DTG RAL EVG/COBI/FTC/TDF * EVG/COBI/FTC/TAF 3TC/ABC TAF No significant DDI TDF * *Monitor for tenofovir toxicity if used with TDF. No clinically significant drug interaction per prescribing information; AASLD/IDSA and DHHS guideline recommend monitoring liver enzymes owing to lack of clinical safety data. DHHS guidelines. October Slide credit: clinicaloptions.com
18 AASLD/IDSA Recommendations for LDV or VEL With Tenofovir Regimen Guidance for Coadministration With TDF [1] * Without COBI or RTV With COBI or RTV SOF/LDV Monitor [2] Monitor; consider TAF or ART switch SOF/VEL Monitor Monitor; consider TAF SOF/VEL/VOX Monitor Monitor (My approach: consider TAF) SOF/LDV, SOF/VEL, SOF/VEL/VOX Guidance for Coadministration With TAF [1] No significant interaction *If egfr < 60 ml/min, avoid TDF coadministration with SOF/LDV, SOF/VEL, or SOF/VEL/VOX. For combinations expected to increase tenofovir levels, baseline and ongoing assessment for tenofovir nephrotoxicity is recommended 1. AASLD/IDSA. HCV guidance. September Sofosbuvir/ledipasvir [package insert] Slide credit: clinicaloptions.com
19 GS-1992: SOF/LDF in HIV/HCV Coinfection After Switch to TAF-Based Regimens Randomized, open-label phase IIIb trial Wk 8 Wk 20 SVR12, % HIV-infected pts with HIV-1 RNA < 50 c/ml on stable ART, egfr 30 ml/min, GT1 HCV infection, no prior NS5A or NS5B DAA (N = 148) Switch to EVG/COBI/FTC/TAF (n = 74) Switch to RPV/FTC/TAF (n = 74) Start SOF/LDV Start SOF/LDV Switch to TAF-based regimen maintained HIV-1 RNA < 50 copies/ml in 95% of pts D/c before Wk 8 for lack of efficacy (n = 1), no resistance to ART Ramgopal M, et al. AASLD Abstract LB-12. ClinicalTrials.gov. NCT Slide credit: clinicaloptions.com
20 Case-3 A 48 y M with HCV, compensated cirrhosis HCV treatment naive HIV infection well controlled with single-tablet regimen of EFV/FTC/TDF HLA-B*5701 negative Past history of HBV infection with documented anti-hbs seroconversion ~ 9 yrs ago
21 Consider Potential for HBV Reactivation Test all pts initiating HCV DAA therapy for HBsAg, anti-hbc, and anti-hbs [1] HIV-infected pts with active HBV infection (HBsAg positive) should receive NRTIs with anti-hbv activity [2] (TAF or TDF) plus (3TC or FTC), or entecavir if TAF or TDF not feasible Initiate ART prior to DAA therapy owing to risk of HBV reactivation with DAAs In pts positive for anti-hbc ± anti-hbs, [1] no consensus Risk of HBV reactivation is very low, [3] but consider monitoring transaminases at Wks 4 and 8 Insufficient data to inform HBV DNA monitoring 1. AASLD/IDSA. HCV guidance. September DHHS guidelines. October Belperio PS, et al. Hepatology. 2017;66: Slide credit: clinicaloptions.com
22 AASLD/IDSA Recommendations for Treatment- Naive GT3 HCV Without Cirrhosis Regimen Duration Recommended GLE/PIB 8 SOF/VEL* 12 Alternative DCV + SOF 12
23 AASLD/IDSA Recommendations for Treatment- Naive GT3 HCV With Compensated Cirrhosis Regimen Recommended Duration, Wks GLE/PIB 12 SOF/VEL* 12 Alternative SOF/VEL/VOX 12 DCV + SOF ± weight-based RBV 24 *If Y93H, add RBV or use SOF/VEL/VOX as alternative. AASLD/IDSA. HCV guidance. September Slide credit: clinicaloptions.com
24 HIV/HCV Drug Drug Interactions ARV(s) GLE/PIB SOF/VEL SOF/VEL/VOX SOF + DCV ATV + (RTV or COBI) X * X Decrease DCV dose DRV + (RTV or COBI) X * * LPV + RTV X * X EFV X X X Increase DCV dose RPV DTG RAL EVG/COBI/FTC/TDF * * * Decrease DCV dose EVG/COBI/FTC/TAF Decrease DCV dose 3TC/ABC TAF TDF * * *Monitor for tenofovir toxicity if used with TDF. No clinically significant drug interaction per prescribing information; AASLD/IDSA and DHHS guideline recommend monitoring liver enzymes owing to lack of clinical safety data. DHHS guidelines. October Slide credit: clinicaloptions.com
25 Case-3, Contd ARV switched to DTG+ TDF/FTC Regimen change tolerated Pt started HCV treatment with GLE/PIB for 12 weeks Achieved cure/svr
26 Case-4 A 39y M with h/o IDU on EFV/TDF/FTC HIV VL < 50, CD4-744 cells Had h/o HCV previously treated with IFN/RBV treated successfully Was incarcerated for 2 years Now back into care Labs show ALT of 57 HCV PCR- 6 million
27 HCV Reinfection Risk After SVR in HIV/HCV-Coinfected Pts HCV Reinfection Rate (per 1000 Person-Yrs) Prospective cohort study of risk factors for HCV reinfection in HIV/HCV-coinfected pts achieving SVR (N = 257) First yr 1-3 yrs After 3 yrs 0 No Risk Factor Low-Risk MSM Young J, et al. Clin Infect Dis. 2017;64: High-Risk MSM Low-Frequency IDU High-Frequency IDU Slide credit: clinicaloptions.com
28 Case-5 A56 y male with HIV Abacavir, Lamivudine and Dolutegravir HIV VL < 20, CD4-357 HCV treatment naive GT 1a, HCV VL 6.5 million copies Never treated because his creatinine is 3.5
29 HCV Recommendations for CKD stage a 1,2,3 Recommended Daclatasvir (60 mg) b Daily fixed-dose combination of elbasvir (50 mg)/grazoprevir (100 mg) Daily fixed-dose combination of glecaprevir (300 mg)/pibrentasvir (120 mg) c Fixed-dose combination of ledipasvir (90 mg)/sofosbuvir (400 mg) Fixed-dose combination of sofosbuvir (400 mg)/velpatasvir (100 mg) Simeprevir (150 mg) Fixed-dose combination of sofosbuvir (400 mg)/velpatasvir (100 mg)/ voxilaprevir (100 mg) Sofosbuvir (400 mg) a Chronic kidney disease (CKD) stages: 1 = normal (egfr >90 ml/min); 2 = mild CKD (egfr ml/min); 3 = moderate CKD (egfr ml/min); 4 = severe CKD (egfr ml/min); 5 = end-stage CKD (egfr <15 ml/min) b Refer to the prescribing information and the section on HIV/HCV coinfection for patients on antiretroviral therapy. c This is a 3-tablet coformulation. Please refer to the prescribing information. AASLD/IDSA. HCV guidance. September 2017.
30 Patients With CKD Stage a 4 or 5 (egfr <30 ml/min or End-Stage Renal Disease) Recommended Genotype Duration Daily fixed-dose combination of elbasvir (50 mg)/grazoprevir (100 mg) 1a, 1b, 4 12 weeks Daily fixed-dose combination of glecaprevir (300 1, 2, 3, 4, 5, 6 8 to 16 weeks c mg)/pibrentasvir (120 mg) b a Chronic kidney disease (CKD) stages: 1 = normal (egfr >90 ml/min); 2 = mild CKD (egfr ml/min); 3 = moderate CKD (egfr ml/min); 4 = severe CKD (egfr ml/min); 5 = end-stage CKD (egfr <15 ml/min) b This is a 3-tablet coformulation. Please refer to the prescribing information. c Patients in this group should be treated as would patients without CKD. Duration of glecaprevir/pibrentasvir should be based on presence of cirrhosis and prior treatment experience (please refer to appropriate section). As such, strength of rating may be lower for certain subgroups. AASLD/IDSA. HCV guidance. September 2017.
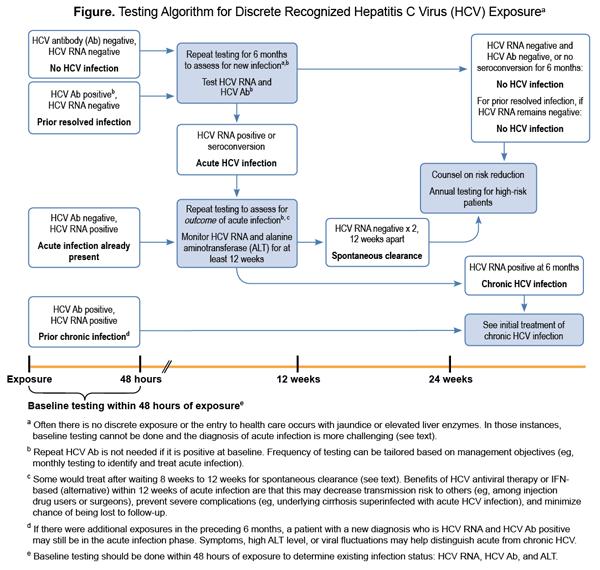
31 Case-6 A 24 y Man with HIV for 2 years doing well on TDF/FTC/EVG/c HIV VL < 20, CD4-645 cells/ cu mm On routine monitoring found to have elevated LFTs and now has HCV Ab positive Last HCV negative was negative 6 months ago
32
33 Treatment of Acute HCV Monitor for 6-12 months for possible spontaneous clearance Risk reduction counseling: alcohol, hepatotoxic medications etc Can start treatment sooner if clinician deems it necessary AASLD/IDSA. HCV guidance. September 2017.
34 HCV Care Continues Past Achievement of SVR Diagnosis Linkage to care Treatment Cure Persons at risk for infection: Counseling Harm reduction (injection and sex practices) Surveillance for reinfection Persons with advanced fibrosis (stage 3/4) Counseling Harm reduction (alcohol and obesity) Surveillance for HCC Characteristic No advanced fibrosis (Metavir stage F0-F2), no or low risk of HCV reinfection Advanced fibrosis (Metavir stage F3 or F4) Moderate to high risk of HCV reinfection Follow-up After SVR Standard medical care, as in someone without HCV Ultrasound surveillance for HCC every 6 mos ± AFP Harm reduction HCV RNA every 12 mos Falade-Nwulia O, et al. J Hepatol. 2017;66: AASLD/IDSA. HCV guidance. September Slide credit: clinicaloptions.com
35 Key Points Treatment regimens similar to HCV mono-infected Monitor for DDI Except for 1 exception treatment duration generally 12 weeks ART interruption for HCV treatment never allowed If significant DDI and ART cannot be changed Daclatasvir plus Sofosbuvir +/- Ribavirin acceptable

36
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
Antiviral treatment in Unique Populations
 Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World
 Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Hepatitis C Virus Management
 Hepatitis C Virus Management FORMATTED: 04/20/17 New York, New York: February 24, 2017 Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine University of California San Francisco San
Hepatitis C Virus Management FORMATTED: 04/20/17 New York, New York: February 24, 2017 Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine University of California San Francisco San
Disclosures. Hepatitis C: the 2016 Perspective. The Take Home. Glossary 12/9/16
 Disclosures Hepatitis C: the 2016 Perspective Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF I have received research grant support to UCSF related to HCV from the following:
Disclosures Hepatitis C: the 2016 Perspective Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF I have received research grant support to UCSF related to HCV from the following:
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Cases: Initial Treatment of Hepatitis C
 Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Hepatitis C: The New World of Treatment
 Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
1/16/2019. Goals of HCV Therapy. Objectives. Treating Hepatitis C and HIV Co Infection. Cure Defined as sustained virologic response (SVR)
") HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
Hepatitis C Guidance 2018 Update: AASLD-IDSA Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection
 Clinical Infectious Diseases IDSA FEATURES Hepatitis C Guidance 2018 Update: AASLD-IDSA Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection AASLD-IDSA HCV Guidance Panel a (See
Clinical Infectious Diseases IDSA FEATURES Hepatitis C Guidance 2018 Update: AASLD-IDSA Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection AASLD-IDSA HCV Guidance Panel a (See
Viral hepatitis in patients living with HIV: can we still speak of special population?
 Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
My HCV patient is co-infected with HIV: how to manage?
 EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
EASL «White Nights of Hepatology 2016» My HCV patient is co-infected with HIV: how to manage? A.V. Кravchenko MD, Professor Russia AIDS Federal Center Central Research Institute of Epidemiology St.-Petersburg,
Hepatitis C Virus: HIV/Hepatitis C Coinfection Wednesday, August 24, 2016
 Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
New York State HCV Provider Webinar Series
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Dost Sarpel, MD Division of Infectious Disease Viral Hepatology Milford Regional Medical Center Objectives Review the epidemiology
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Dost Sarpel, MD Division of Infectious Disease Viral Hepatology Milford Regional Medical Center Objectives Review the epidemiology
Harvoni (sofosbuvir/ledipasvir
 Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
Treatment of HCV in HIV/HCV Coinfection
 Treatment of HCV in HIV/HCV Coinfection Michael S. Saag, MD Associate Dean, Global Health Professor of Medicine Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Treatment of HCV in HIV/HCV Coinfection Michael S. Saag, MD Associate Dean, Global Health Professor of Medicine Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Treatment of Patients with HCV and HIV
 Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
New York State HCV Provider Webinar Series. Treatment of HCV/HIV Co-Infection
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Objectives Review the epidemiology of HCV and HIV/HCV co-infection Discuss the burden of HIV/HCV co-infection Discuss the treatment
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York
 Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Cases: Management of Hepatitis C in Prior Treatment Failure
 Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
Cases: Initial Hepatitis C Treatment, Including Coinfection
 Cases: Initial Hepatitis C Treatment, Including Coinfection Ricardo Franco MD Assistant Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama Learning Objectives After attending
Cases: Initial Hepatitis C Treatment, Including Coinfection Ricardo Franco MD Assistant Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama Learning Objectives After attending
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Potential Issues in Treating HIV/HCV co-infection with new HCV antivirals
 State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
State of the Art in Hepatitis C Virus Infection in HIV/HCV-Coinfected Patients FORMATTED: 11/17/15 David L. Wyles, MD Associate Professor of Medicine University of California San Diego San Diego, California
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
Treating Hepatitis C Virus (HCV) Infection
 Infection") Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
Sovaldi (sofosbuvir)
") Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Hepatitis C in HIV Coinfection. Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF
 Hepatitis C in HIV Coinfection Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Disclosures I have received research grant support to UCSF related to HCV from the following: Abbvie
Hepatitis C in HIV Coinfection Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Disclosures I have received research grant support to UCSF related to HCV from the following: Abbvie
Hepatitis C Medications Prior Authorization Criteria
 Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
Description of Antivirals for Hepatitis C. LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases
 Description of Antivirals for Hepatitis C LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases Dwayne-David@cherokee.org Objectives Compare the different classes of direct-acting antiviral
Description of Antivirals for Hepatitis C LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases Dwayne-David@cherokee.org Objectives Compare the different classes of direct-acting antiviral
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Hepatitis C in the HIV Co-infected Population: Where are we today?
 Hepatitis C in the HIV Co-infected Population: Where are we today? Sherilyn Brinkley MSN, CRNP Viral Hepatitis Center John G. Bartlett Specialty Practice 1 Disclosures Consulting and fees for non-cme/ce
Hepatitis C in the HIV Co-infected Population: Where are we today? Sherilyn Brinkley MSN, CRNP Viral Hepatitis Center John G. Bartlett Specialty Practice 1 Disclosures Consulting and fees for non-cme/ce
Initial Treatment of the Hepatitis C Virus-Infected Patient
 IDSA/AASLD www.hcvguidelines.org http://www.easl.eu/research/our-contributions/clinical-practice-guidelines/detail/easl-recommendations-ontreatment-of-hepatitis-c-216 Initial Treatment of the Hepatitis
IDSA/AASLD www.hcvguidelines.org http://www.easl.eu/research/our-contributions/clinical-practice-guidelines/detail/easl-recommendations-ontreatment-of-hepatitis-c-216 Initial Treatment of the Hepatitis
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Treating Hepatitis C in Patients with Advanced Renal Disease
 Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Current HCV Treatment by Genotype Ira M. Jacobson, MD
 Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
HCV/HIV Coinfection ANTON AND MARGARET FUISZ CHAIR IN MEDICINE. HIV and HCV Share Risk Factors PREVALENCE OF CO-INFECTION BY RISK FACTOR 60%
 HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
HCV/HIV Coinfection BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY HIV and HCV Share Risk Factors PREVALENCE
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Hepatitis C ew Medications, New Hope and New. V. Opportunities for Primary Care. Outline. HCV Disease Outcomes in the US 9/21/2016
 Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon
 HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
Outline. HCV Disease Outcomes in the US. Hepatitis C: The New Landscape 5/24/16. Advances in Internal Medicine May 24, I have no disclosures
 5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Current Management of Hepatitis C Virus Infection
 Current Management of Hepatitis C Virus Infection Kristen M. Marks, MD Assistant Professor Weill Cornell Medicine New York, New York FORMATTED: 10/13/16 Financial Relationships With Commercial Entities
Current Management of Hepatitis C Virus Infection Kristen M. Marks, MD Assistant Professor Weill Cornell Medicine New York, New York FORMATTED: 10/13/16 Financial Relationships With Commercial Entities
HIV/hepatitis co-infection. Christoph Boesecke Department of Medicine I University Hospital Bonn Germany
 HIV/hepatitis co-infection Christoph Boesecke Department of Medicine I University Hospital Bonn Germany Clinical Management and Treatment of HBV and HCV Co-infection in HIVpositive Persons Hepatitis B
HIV/hepatitis co-infection Christoph Boesecke Department of Medicine I University Hospital Bonn Germany Clinical Management and Treatment of HBV and HCV Co-infection in HIVpositive Persons Hepatitis B
Cases: Treatment of Hepatitis C in HIV/HCV Coinfection
 Cases: Treatment of Hepatitis C in HIV/HCV Coinfection David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Cases: Treatment of Hepatitis C in HIV/HCV Coinfection David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Contemporary Management of HIV-HCV Coinfection
 Contemporary Management of HIV-HCV Coinfection Elizabeth Sherman, PharmD, AAHIVP Faculty, South Florida - Southeast AIDS Education & Training Center HIV/AIDS Clinical Pharmacist, Memorial Healthcare System
Contemporary Management of HIV-HCV Coinfection Elizabeth Sherman, PharmD, AAHIVP Faculty, South Florida - Southeast AIDS Education & Training Center HIV/AIDS Clinical Pharmacist, Memorial Healthcare System
HCV Case Studies (and Special Populations)
") HCV Case Studies (and Special Populations) Case 1: Alfred 58 y/o man presents to clinic for primary care f/u. PMH: Hypertension, diabetes Medications: lisinopril, glipizide Allergies: NKDA Family History:
HCV Case Studies (and Special Populations) Case 1: Alfred 58 y/o man presents to clinic for primary care f/u. PMH: Hypertension, diabetes Medications: lisinopril, glipizide Allergies: NKDA Family History:
Hepatitis C: Newest Treatment Options and What To Do When We Cure It!
 Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
MEDICATIONS FOR THE TREATMENT OF CHRONIC HEPATITIS C
 MEDICATIONS FOR THE TREATMENT OF CHRONIC HEPATITIS C Annette Hewitt, ARNP, Liver Disease and Hepatitis Program Alaska Native Tribal Health Consortium CONFLICT OF INTEREST DISCLOSURE STATEMENT None. I will
MEDICATIONS FOR THE TREATMENT OF CHRONIC HEPATITIS C Annette Hewitt, ARNP, Liver Disease and Hepatitis Program Alaska Native Tribal Health Consortium CONFLICT OF INTEREST DISCLOSURE STATEMENT None. I will
Real World Management of HCV in HIV: Approach to Initial Therapy with focus on new DAAs
 Real World Management of HCV in HIV: Approach to Initial Therapy with focus on new DAAs Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Financial Relationships
Real World Management of HCV in HIV: Approach to Initial Therapy with focus on new DAAs Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Financial Relationships
Hepatitis C Update: A Growing Challenge With Evolving Management Solutions
 Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Disclosures. Lisa M. Chirch, MD, FIDSA has disclosed that she has served on advisory boards for Gilead Sciences and Melinta Therapeutics.
 HEPATITIS C IN 2017 Lisa M. Chirch, M.D. Associate Professor of Medicine University of Connecticut Health Center A Local Performance Site of the New England AETC Disclosures Lisa M. Chirch, MD, FIDSA has
HEPATITIS C IN 2017 Lisa M. Chirch, M.D. Associate Professor of Medicine University of Connecticut Health Center A Local Performance Site of the New England AETC Disclosures Lisa M. Chirch, MD, FIDSA has
A Practical Approach to HIV/HCV Co-infection
 A Practical Approach to HIV/HCV Co-infection Focus on Drug-Drug Interactions Amy Hirsch Shumaker, PharmD, BCPS HIV/Hepatitis C Clinical Pharmacy Specialist Louis Stokes Cleveland VA Medical Center Andrea
A Practical Approach to HIV/HCV Co-infection Focus on Drug-Drug Interactions Amy Hirsch Shumaker, PharmD, BCPS HIV/Hepatitis C Clinical Pharmacy Specialist Louis Stokes Cleveland VA Medical Center Andrea
New Hepatitis C Antivirals
 New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
Universal HCV treatment: Strategies for simplification
 Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos
 Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
P4C HIV TAC Collaborative Training: Hepatitis C Virus (HCV) Treatment Guidelines
 Treatment Guidelines") P4C HIV TAC Collaborative Training: Hepatitis C Virus (HCV) Treatment Guidelines Presenter: Stacey B. Trooskin, M.D., Ph.D Director of Viral Hepatitis Programs Philadelphia FIGHT Community Health Centers
P4C HIV TAC Collaborative Training: Hepatitis C Virus (HCV) Treatment Guidelines Presenter: Stacey B. Trooskin, M.D., Ph.D Director of Viral Hepatitis Programs Philadelphia FIGHT Community Health Centers
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
HCV Screening, Management, and Treatment Guidelines
 HCV ECHO WESTERN STATES HCV Screening, Management, and Treatment Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health
HCV ECHO WESTERN STATES HCV Screening, Management, and Treatment Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients. Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London
 Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health