Disclosures. Lisa M. Chirch, MD, FIDSA has disclosed that she has served on advisory boards for Gilead Sciences and Melinta Therapeutics.
|
|
|
- Brenda Malone
- 6 years ago
- Views:
Transcription

1 HEPATITIS C IN 2017 Lisa M. Chirch, M.D. Associate Professor of Medicine University of Connecticut Health Center A Local Performance Site of the New England AETC
2 Disclosures Lisa M. Chirch, MD, FIDSA has disclosed that she has served on advisory boards for Gilead Sciences and Melinta Therapeutics.
3 Learning Objectives Review the most recent epidemiology of chronic hepatitis C infection. Describe the initial assessment of patients with chronic hepatitis C. Review recent guideline recommendations for the treatment of chronic hepatitis C virus (HCV) infection. Evaluate new and emerging treatments for hepatitis C. Recognize adverse effects and important drug-drug interactions with available therapies for hepatitis C.

4 China, Pakistan, Nigeria, Egypt and India account for an estimated half of the up to 180 million hepatitis C infections worldwide; 3-4 million new infections annually. -Dr. Imad Waked, National Liver Institute, Cairo Hepatitis C Yellow Book Travelers' Health CDC.


5 Current landscape
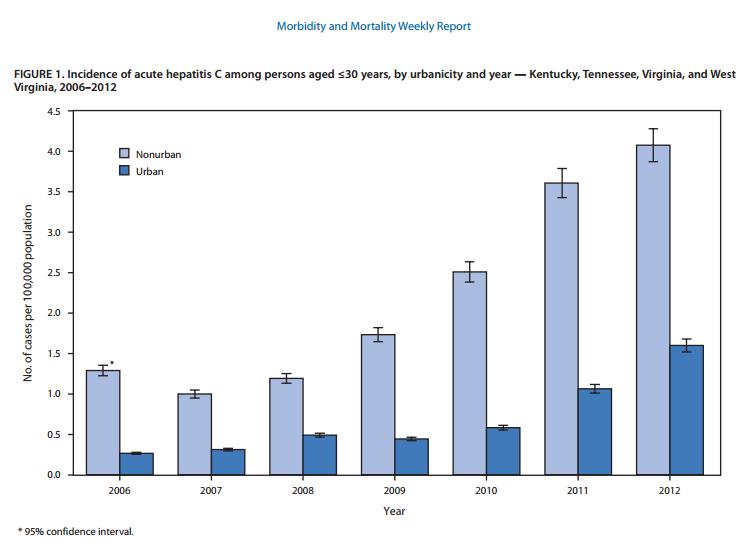
6 Magnitude of the U.S. Problem Nearly 4 million persons in United States infected Approximately 35,000 new cases yearly >15,000 deaths annually Acute infections on the rise since 2010 Young MSM, rural vs urban (MMWR 2015) <10% chronically infected patients are treated Leading cause of Chronic liver disease Cirrhosis Liver cancer Liver transplantation Sulkowski M.ID Week 2015

7 Lack of Awareness Silent Epidemic Virus Prevalence % Unaware of Status HBV 800, million About 65% HCV million About 75% HIV 1.1 million About 21%
8 Pts (%) Hepatitis C Virus (HCV) in the US: Gaps in Current Practice % % 43% 27% 20 17% 16% 9% 0 Chronic Diagnosed Access to HCV Infected and Outpatient Aware Care HCV RNA Confirmed Underwent Liver Biopsy Prescribed Achieved HCV Sustained Viral Treatment Response n = 3,500,000 1,743,000 1,514, , , , ,859 Yehia BR, et al. PLoS One. 2014;9:e
9

.")
10 Southeast Indiana had previously recorded only about five cases of HIV infection annually, yet by June 10, 2015, a total of 169 people had been newly diagnosed with HIV in about half a year. More than 80% of them were coinfected with hepatitis C virus (HCV). Needle exchange programs illegal in IN.
11 Indications for HCV screening? HIV IDU History of chronic HD, transfusion, blood product or organ transplant prior to 1992 Unexplained persistent elevation in ALT (?RNA) One-time testing without prior ascertainment of HCV risk for persons born during , a population with a disproportionately high prevalence of HCV infection and related disease. CDC 2012

12 Why Baby Boomers? Persons born between are 5 times more likely to be infected with HCV ~2 million chronically infected ~ 1/3 cirrhotic* Represent ~75% of all HCV-associated mortality ~ 1/3 lack health insurance High rates of alcohol consumption Low rates of Hepatitis A/B vaccination November *Sulkowski ID Week 2015

13 Testing sequence MMWR 2013
14 If 10 people are exposed to the hepatitis C virus, approximately how many will develop chronic infection?
 Cirrhosis 20% (17%) HCC, hepatocellular carcinoma *Nancy Reau.")
15 Hepatitis C Virus Infection Natural History Resolved 15% (15%) Acute HCV Chronic HCV 85% (85%) *11% decompensate - transplant/death Stable 80% (68%) Cirrhosis 20% (17%) HCC, hepatocellular carcinoma *Nancy Reau. ID Week 2015 Slowly progressive 75% (13%) *HCC 25% (4% annually)
16 Hepatitis C Virus Genotypes in the USA Type 2 17% Type 1 72% Type 3 10% All others 1% McHutchinson JG, et al. N Engl J Med. 1998;339:
17 Management of Chronic HCV Disease Severity AST/ALT Bilirubin Albumin Pro-time (INR) Platelet count Liver histology Transient Elastography Response to Therapy ALT HCV RNA HCV genotype Liver histology
18 Fibrosis Staging in Hepatitis: What You Need to Know Assess whether pt has advanced disease Metavir Stage 0-2 No fibrosis or portal fibrosis Metavir Stage 3-4 Advanced fibrosis or cirrhosis Determines: Treatment duration Use of ribavirin Follow-up after cure Monitor for progressive fibrosis Noninvasive strategies or biopsy APRI (AST platelet ratio index), FIB-4, FibroSure, Fibroscan

19 Sampling error??

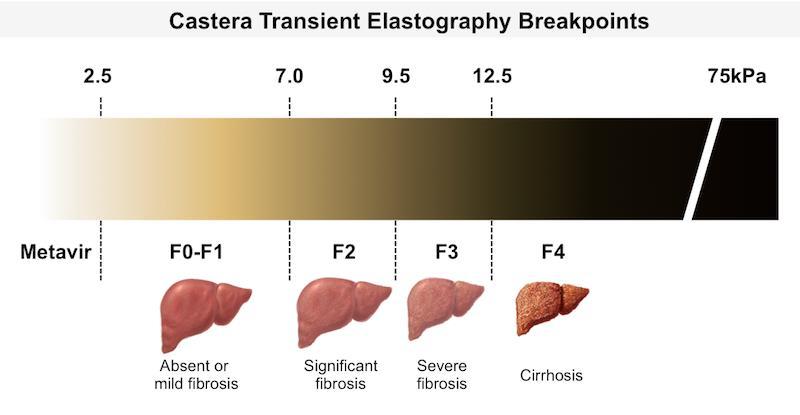
20 Fibroscan
21 HCV Treatment Goals Goals of treatment for chronic HCV Viral eradication (undetectable viral load) Delay progression of fibrosis Prevent decompensation, HCC, transplant, and death (+ quality of life??) Best indicator of successful treatment is sustained virologic response (SVR) Van der Meer AJ, et al. JAMA. 2012;308: ; Younossi Z, et al. Clin Gastroenterol Hepatol. 2014;12:
22 Sustained virologic response SVR: serum HCV RNA is undetectable based on a quantitative HCV RNA assay with lower limit of detection of 50 IU/mL or less at 12 weeks after treatment ends
23 All-Cause Mortality (%) Liver-Related Mortality or Liver Transplantation (%) Hepatocellular Carcinoma (%) Hepatitis C Virologic Cure Associated With Improved Outcomes All-Cause Mortality Liver-Related Mortality or 30 Liver Transplantation 30 P <.001 P < Hepatocellular Carcinoma P < Without SVR 10 Without SVR 10 Without SVR With SVR With SVR Yr Yr HR: 0.26 (95% CI: ; P <.001) With SVR Yr Virologic cure does not protect against reinfection van der Meer AJ, et al. JAMA. 2012;308:
24 Sustained Virologic Response (%) Treatment of Chronic HCV Peginterferon and Ribavirin PegIFN-2a/RBV PegIFN-2b/RBV Genotype Fried MW, et al. N Eng J Med. 2002;347: Manns MP, et al. Lancet 2001;358:
25 Incidence/Severity Time Course of Treatment-Associated Psychiatric Adverse Effects Depression Fatigue Influenza-like symptoms Months Dan A, et al. J Hepatol. 2006;44: Constant A, et al. J Clin Psychiatry. 2005;66:
26 Ribavirin Nucleoside analog Inhibits inosine monophosphate dehydrogenase Potentiates purine analogs, ie didanosine Immune modulator, shift from Th2 to Th1 response Teratogenic both men and women must use contraception during and for 6 months after treatment Dose-dependent hemolytic anemia Increased risk for lactic acidosis

27 FLAVIvirus Yellow Fever Dengue West Nile ZIKA

28 Summary of Approved Direct-Acting Antivirals Drug Abbreviation Class Grazoprevir GZR NS3/4A protease inhibitor Paritaprevir PTV NS3/4A protease inhibitor Simeprevir SMV NS3/4A protease inhibitor Daclatasvir DCV NS5A inhibitor Elbasvir EBR NS5A inhibitor Highly effective options for every genotype Ledipasvir LDV NS5A inhibitor Single-pill formulations or 2-pill combinations Ombitasvir OBV NS5A inhibitor Velpatasvir VEL NS5A inhibitor Sofosbuvir Dasabuvir SOF DSV NS5B nucleotide polymerase inhibitor NS5B nonnucleoside polymerase inhibitor Slide credit: clinicaloptions.com
29 Ledipasvir/Sofosbuvir FDA Approved, October 2014 One tablet daily for HCV GT1, 4, 5, 6 and HIV coinfection EXTREMELY well tolerated adverse events rare Fatigue and headache most common Patient No Population dosing in CrCl<30ml/min Recommendation (!!!) Treatment naïve, with or without cirrhosis 12 weeks Treatment experiences without cirrhosis Treatment experienced with cirrhosis Treatment naïve, without cirrhosis, baseline viral load < 6 million IU/ml Treatment naïve AND experienced with DECOMPENSATED cirrhosis (CP B or C) Transplant recipients 12 weeks 24 weeks Consider* 8 weeks 12 weeks + RIBAVIRIN 12 weeks + RIBAVIRIN
30 SVR12 (%) SVR12 by Treatment Regimen and Duration in Pts Without Cirrhosis Pooled data from multiple trials, HCV RNA < 6 M IU/mL in 8-wk arm With RAVs No RAVs n/n = /32 107/ / /509 8 Wks 12 Wks Zeuzem S, et al. AASLD Abstract 91.
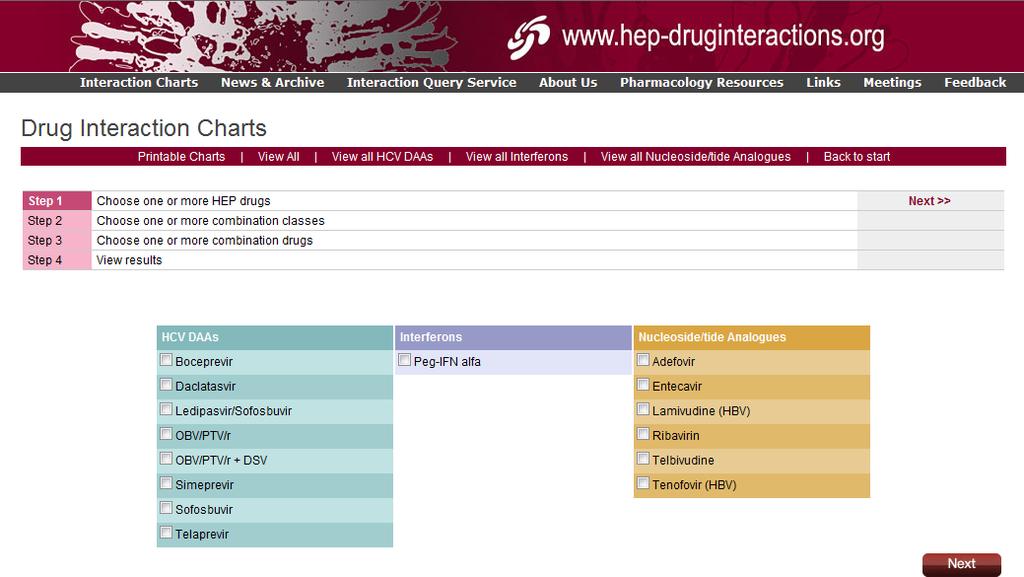
31 HEP ichart

32 Ledipasvir/Sofosbuvir Medications to Avoid Antiarrythmics, Anticonvulsants/Antimycobacterials Amiodarone, carbamazepine, phenytoin, phenobarbital, oxcarbazepine, rifampin, rifabutin HCV Products Simeprevir Coadministration not recommended. Coadministration not recommended. Herbal Supplements: St. John s wort (Hypericum perforatum) HMG-CoA Reductase Inhibitors: Rosuvastatin Harvoni PI, 2014, Coadministration not recommended. Northeast/ Caribbean AETC Coadministration not recommended.
33 Elbasvir/Grazoprevir NS5A inhibitor plus NS3/4A protease inhibitor Approved January 2016 for GT 1 and 4
 Placebo (n = 113) Open-label period Grazoprevir/Elbasvir (n = 113) 99% 98% Grazoprevir/elbasvir dosed orally 100 mg/50 mg once daily.")
34 C-SURFER: Grazoprevir/Elbasvir in Pts With GT1 HCV and Stage 4/5 CKD Treatment Wk 12 Follow-up Wk 4 Follow-up Wk 16 Randomized period SVR12* GT1 HCV infected pts with stage 4/5 CKD (n = 224) Grazoprevir/Elbasvir (n = 111) Placebo (n = 113) Open-label period Grazoprevir/Elbasvir (n = 113) 99% 98% Grazoprevir/elbasvir dosed orally 100 mg/50 mg once daily. This study also included a pharmacokinetic analysis (n = 11) in which pts were treated as in the randomized grazoprevir/elbasvir study group. 76% on dialysis 34% with diabetes 52% GT1a, 48% GT1b 6% cirrhosis *Modified full analysis set population. Roth D, et al. Lancet. 2015;386: Roth D, et al. Kidney Week Abstract SA-PO1100.
35 SVR12 (%) Adjust EBR/GZR Duration Based on Baseline NS5A RASs in GT1a n/n = 0 C-EDGE Treatment Naive: 12 Wks of Elbasvir/Grazoprevir /15 7 All No BL NS5A RASs / /19 BL NS5A RASs 129/13 1 GT1a GT1b If NS5A RASs in GT1a, treat with EBR/GZR + RBV for 16 wks (alternative) No baseline RAS testing needed in GT1b pts All Zeuzem Z, et al. Ann Intern Med. 2015;163:1-13. Kwo P, et al. J Hepatol. 2015;62(suppl 2):S674-S675. Slide credit: clinicaloptions.com

36 Sofosbuvir/ Velpatasvir NB5B plus NS5A
37 ASTRAL-1: SOF/VEL for 12 Wks in GT1, 2, 4, 5, 6 Pts With and Without Cirrhosis 19% cirrhosis, 32% treatment experienced [1] GT3 pts evaluated in separate study (ASTRAL-3) [2] GT2 pts also studied with SOF/VEL vs SOF + RBV in ASTRAL-2 with similar results [2] SVR12 (%) [1] n/n = 0 618/ / / / / 116 Overall GT1a GT1b GT2 GT4 GT5 GT6 34/ 35 41/ Feld JJ, et al. N Engl J Med. 2015;373: Foster GR, et al. N Engl J Med. 2015;373: Slide credit: clinicaloptions.com
38 HCC-Free Survival Genotype 3 Is Important Second most common genotype globally [1] 10% to 15% of HCV cases in the US Associated with more rapid progression of fibrosis and higher risk of HCC [2] Suboptimal responses to first-generation DAAs Genotype 1 Genotype 2 Genotype 3 Genotype 4 HCC-Free Survival by Genotype [2] P =.001 Genotype 4 Genotype 2 Genotype 1 Genotype Yrs Messina JP, et al. Hepatology. 2015;61: Nkontchou G, et al. J Viral Hepat. 2011;18:e516-e522.
39 Avoiding Future Failure... ASTRAL 3: SVR12 rate with SOF/VEL relative to presence/absence of NS5A RAVs: 97% SVR12 SO.for genotype 3, add RIBAVIRIN IF*: 1) Y93H RAV present OR 225/ (84%) had no baseline NS5A RAVs 43 (16%) had baseline NS5A RAVs 2) RX-experienced and cirrhotic 88% SVR12 38/43 Foster GR, et al. N Engl J Med. 2015;373: *
40 SVR12 (%) SVR12 (%) SURVEYOR 2, Part 4: 8 Wks GLE/PIB For Pts With GT 2, 4, 5, 6 HCV Without Cirrhosis 99% SVR12 rate with 8-wk regimen in DAA-naive pts with GT2 HCV noninferior to 95% historical control (SOF + RBV for 12 wks) ITT mitt n/n 0= / 20 All / 14 GT2 5 43/ 46 GT4 2/2 GT5 90 9/1 0 GT n/n 0= / / / 43 2/ / 9 All GT2 GT4 GT5 GT6 Relapse D/C No SVR12 data Hassanein TI, et al. AASLD Abstract LB-15. Slide credit: clinicaloptions.c
41 SVR12 by ITT (%) ENDURANCE-3: Glecaprevir/Pibrentasvir in GT3 HCV Without Cirrhosis Most pts had history of IDU (63% to 66%) n/n = 0 Failure, n (%) Breakthroug h Relapse AE-related d/c LTFU 1 (1) 5 (3) 0 2 (1) Noninferior / / (< 1) 3 (1) 1 (< 1) 4 (2)* Noninferior 111/ (1) 1 (1) 2 (2) 8-wk GLE/PIB 12-wk GLE/PIB 12-wk DCV + SOF No serious AEs deemed related to study drug No clinically relevant ALT increases, 1 isolated bilirubin increase (G/P 8 wks), 1 isolated neutrophil count decrease (G/P 12 wks) Foster GR, et al. EASL Abstract GS-007.

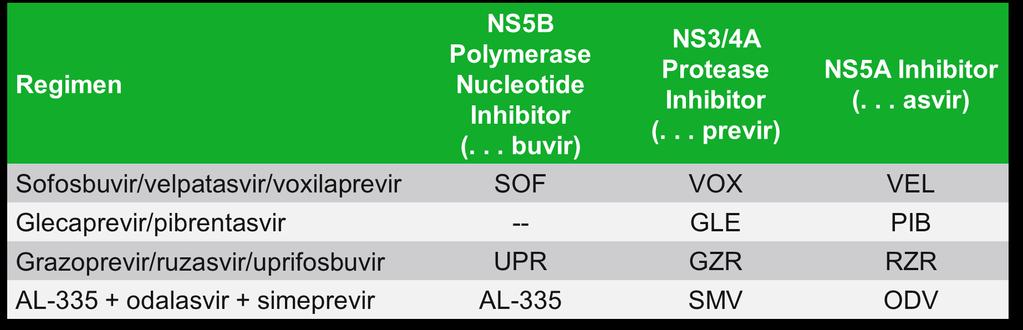
42 In the pipeline
43 To summarize Several highly effective regimens approved for GT1 Need for extended therapy and/or RBV in cirrhotics depending on regimen, GT1 subtype, and prior treatment status Data support 8 wks of LDV/SOF in GT1 treatmentnaive noncirrhotics with HCV RNA < 6 M IU/mL High-dose PPIs should be avoided with LDV and with VEL 8 week course of G/P comparable efficacy Genotype 3 remains problematic, but not for long??
44 Key Points All pts born should be screened for hepatitis C infection Know risk-based screening recommendations Virtually all pts with hepatitis C infection should be treated, regardless of genotype and fibrosis Prevents morbidity, progression of fibrosis, hepatocellular carcinoma Many pts can be treated in primary care setting Must refer pts with decompensation Current treatments include pangenotypic and ribavirin-free options > 95% rate of cure for most genotypes 8 to12 wks, ribavirin free, all oral, once daily
45 Just a few more things Hepatitis B reactivation HCC screening


46 HBV Reactivation Risk in HBV/HCV Coinfected Pts Receiving HCV DAAs Case reports of HBV reactivation in pts treated with several different DAA regimens 29 reports of HBV-R associated with DAA therapy Reactivation of HBV usually occurred 4 to 8 weeks after DAA initiation Decompensated liver failure developed in 3 patients, 2 died and 1 required liver transplantation FDA Black box warning
47 HBV Testing and Monitoring During HCV DAA Therapy: AASLD/IDSA Guidance Test all pts initiating HCV therapy for HBsAg, anti-hbc, and anti-hbs No HBV markers: VACCINATE (this is not new!) HBV markers present: HBV DNA detectable HBV DNA meets criteria for treatment in AASLD HBV guidelines Treat with HBV drug HBsAg positive AASLD/IDSA. HCV guidance. September HBV DNA low or undetectable Monitor for reactivation; treat if HBV DNA level meets AASLD HBV guideline treatment criteria HBsAg negative; Anti-HBc positive (± anti-hbs) Insufficient data to provide recommendations Slide credit: clinicaloptions.com
48 HCC Risk Persists After DAA Therapy in Pts With HCV-Related Cirrhosis Retrospective analysis of 344 HCV-infected pts with CP A or B cirrhosis treated with DAAs (SVR: 89%) Pts followed for wks after treatment completion No HCC at baseline, but previous HCC permitted Overall HCC incidence after DAA therapy: 7.6% In pts without previous HCC: 3.2% In pts with previous HCC: 29.0% More advanced liver disease and previous HCC significant risk factors for HCC after DAAs Factor No HCC (n = 318) HCC (n = 26) P Value CP class B, % Mean liver stiffness, kpa Liver stiffness, n.005 kpa < kpa > Mean platelets, x 1000/mm Previous HCC, n.0001 Yes No Buonfiglioli F, et al. EASL Abstract LBP506. Slide credit: clinicaloptions.com
49 HCC Screening Guidelines EASL-EORTC Guidelines 2012 [1] : Pts at high risk for developing HCC should be entered into surveillance programs. Surveillance should be performed by experienced personnel in all at-risk populations using abdominal ultrasound every 6 mos AASLD/IDSA HCV Guidance 2016 [2] : Surveillance for hepatocellular carcinoma with twice-yearly ultrasound examination is recommended for pts with advanced fibrosis (ie, Metavir stage F3 or F4) who achieve an SVR 1. EASL-EORTC. J Hepatol. 2012;56: AASLD/IDSA. HCV Guidance Slide credit: clinicaloptions.com
50 Enter the Nonspecialist: Will Evolving Hepatitis C Therapies Reduce the Need for Specialized Care? Graham R. Foster, FRCP, PhD - 10/8/2013 Enter the ID Pharmacist: Multidisciplinary approach to HCV care Improved adherence and SVR when pharmacists involved (Chastain C, CID 2015) Education/counseling; attention to DDIs and toxicities, cost evaluation A rapid expansion of patients and providers will mirror improving efficacies and gentler adverse event profiles the introduction of a single-tablet regimen for HCV therapy a development that will propel hepatitis C care to its future in nonspecialist providers offices. Information will be the key to overcoming preconceptions about adverse events and regimen complexities, finally allowing nonspecialists to take a central role in caring for HCV-infected patients.


51 Cost Considerations $$ Harvoni: 32K monthly Epclusa:28K monthly (wholesale acquisition cost) Zepatier: 18K 12 weeks Copay cards for some medications available Mavyret: 13K per 8 week course Medicaid restrictions in MANY states; federal and state discount programs in place hepatitis-c-drug-could-launch-the-drug-worlds-own-hunger-games
52 Summary HCV epidemiology and treatment landscape are rapidly evolving. Interferon free regimens are here for majority of patients, ribavirin may not be needed for most. Cost remains an issue Generalists and pharmacists will play an increasingly important role in HCV management going forward. Remember to screen for hepatitis B, and for HCC even when cure achieved.


53
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Updates in the Treatment of Hepatitis C
 Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Disclosures Updates in the Treatment of Hepatitis C Arslan Kahloon M.D Assistant Professor of Medicine University of Tennessee, Chattanooga I have no conflicts of interest or financial sponsorship to disclose
Outline. HCV Disease Outcomes in the US. Hepatitis C: The New Landscape 5/24/16. Advances in Internal Medicine May 24, I have no disclosures
 5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
5/24/16 Hepatitis C: The New Landscape Advances in Internal Medicine May 24, 2016 I have no disclosures Rena K. Fo, MD Professor of Clinical Medicine, UCSF Outline I. Current HCV outcomes in the US II.
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Cases: Initial Treatment of Hepatitis C
 Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Hepatitis C ew Medications, New Hope and New. V. Opportunities for Primary Care. Outline. HCV Disease Outcomes in the US 9/21/2016
 Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
HIV-HCV Co-Infection in Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School
 HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
HIV-HCV Co-Infection in 2018 Shobha Swaminathan, MD Associate Professor of Medicine Rutgers New Jersey Medical School AASLD/IDSA and DHHS Guidance: HIV/HCV Coinfection All pts with HIV should be screened
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
1/16/2019. Goals of HCV Therapy. Objectives. Treating Hepatitis C and HIV Co Infection. Cure Defined as sustained virologic response (SVR)
") HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
New Hepatitis C Antivirals
 New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
New Hepatitis C Antivirals Kris Stewart, BSP, MD, FRCPC Drug Therapy Conference College of Medicine, University of Saskatchewan September 23, 2016 Disclosures I have received research and program support
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
HCV Disease Outcomes in the US. Hepatitis C New Medications, New Hope and New Opportunities for Primary Care. Learning Objectives 10/13/17
 Hepatitis C New Medications, New Hope and New Opportunities for Primary Care Disclosures: Grant for quality improvement Gilead In this talk, 10 drugs will be discussed, 4 of which are manufactured by Gilead.
Hepatitis C New Medications, New Hope and New Opportunities for Primary Care Disclosures: Grant for quality improvement Gilead In this talk, 10 drugs will be discussed, 4 of which are manufactured by Gilead.
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner
 Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
HCV Screening, Management, and Treatment Guidelines
 HCV ECHO WESTERN STATES HCV Screening, Management, and Treatment Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health
HCV ECHO WESTERN STATES HCV Screening, Management, and Treatment Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Hepatitis C Update: A Growing Challenge With Evolving Management Solutions
 Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
On Target for Hepatitis C Elimination: Direct Acting Antiviral Agents in 2018
 On Target for Hepatitis C Elimination: Direct Acting Antiviral Agents in 2018 Trana Hussaini, PharmD Pharmacotherapy Specialist in Liver Transplantation, VGH Clinical Assistant Professor, Faculty of Pharmaceutical
On Target for Hepatitis C Elimination: Direct Acting Antiviral Agents in 2018 Trana Hussaini, PharmD Pharmacotherapy Specialist in Liver Transplantation, VGH Clinical Assistant Professor, Faculty of Pharmaceutical
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York
 Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon
 HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
New York State HCV Provider Webinar Series. Side Effects of Therapy and Drug-Drug Interactions
 New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
Hepatitis C: Newest Treatment Options and What To Do When We Cure It!
 Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Hepatitis C: Newest Treatment Options and What To Do When We Cure It! Richard Kalman, MD Division of Hepatology Department of Transplantation Einstein Medical Center Learning Objectives Scope of HCV How
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Hepatitis C: The New World of Treatment
 Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
New York State HCV Provider Webinar Series. Side Effects of Therapy and Drug-Drug Interactions
 New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
New York State HCV Provider Webinar Series Side Effects of Therapy and Drug-Drug Interactions Case Presentation Case 56 year-old lady with Genotype 1A Hepatitis C, Treatment-naive Noninvasive fibrosis
Hepatitis C Update on New Treatments
 Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
Case. 63 year old woman now with:
 Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18
 Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HCV Screening, Management and Guidelines
 HCV ECHO WESTERN STATES HCV Screening, Management and Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health Sciences Center
HCV ECHO WESTERN STATES HCV Screening, Management and Guidelines Paulina Deming, PharmD, PhC Associate Professor of Pharmacy-College of Pharmacy Project ECHO University of New Mexico Health Sciences Center
Sovaldi (sofosbuvir)
") Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Harvoni (sofosbuvir/ledipasvir
 Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
Description of Antivirals for Hepatitis C. LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases
 Description of Antivirals for Hepatitis C LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases Dwayne-David@cherokee.org Objectives Compare the different classes of direct-acting antiviral
Description of Antivirals for Hepatitis C LCDR Dwayne David, PharmD, BCPS, NCPS Cherokee Nation Infectious Diseases Dwayne-David@cherokee.org Objectives Compare the different classes of direct-acting antiviral
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Patients with compensated cirrhosis: how to treat and follow-up
 Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Contemporary Management of HIV-HCV Coinfection
 Contemporary Management of HIV-HCV Coinfection Elizabeth Sherman, PharmD, AAHIVP Faculty, South Florida - Southeast AIDS Education & Training Center HIV/AIDS Clinical Pharmacist, Memorial Healthcare System
Contemporary Management of HIV-HCV Coinfection Elizabeth Sherman, PharmD, AAHIVP Faculty, South Florida - Southeast AIDS Education & Training Center HIV/AIDS Clinical Pharmacist, Memorial Healthcare System
5/10/2016. Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients. HCV life-cycle and antiviral targets
 5/1/216 Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients David L. Wyles, MD Associate Professor of Medicine University of California San Diego La Jolla,
5/1/216 Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients David L. Wyles, MD Associate Professor of Medicine University of California San Diego La Jolla,
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Case 1: Chronic Hepatitis C
 Case 1: Chronic Hepatitis C Moderator Dawn Pease, MSN, RN, ANP-BC Seton Healthcare Family University Medical Center Brackenridge Brackenridge Specialty Clinics - Gastroenterology and Endocrinology Austin,
Case 1: Chronic Hepatitis C Moderator Dawn Pease, MSN, RN, ANP-BC Seton Healthcare Family University Medical Center Brackenridge Brackenridge Specialty Clinics - Gastroenterology and Endocrinology Austin,
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World
 Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Hepatitis C Genotype 1 (GT 1) Patients in the United States (US)
 Patients in the United States (US)") Hepatitis C Genotype 1 (GT 1) Patients in the United States (US) INDICATION is indicated with or without ribavirin for the treatment of patients with chronic hepatitis C virus (HCV) genotype 1, 4, 5, or
Hepatitis C Genotype 1 (GT 1) Patients in the United States (US) INDICATION is indicated with or without ribavirin for the treatment of patients with chronic hepatitis C virus (HCV) genotype 1, 4, 5, or
Program Disclosure. A maximum of 1.5 contact hours may be earned for successful completion of this activity.
 Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
Program Disclosure This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HIV and Hepatitis C Have we finally slayed the beast?
 HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
HIV and Hepatitis C Have we finally slayed the beast? Mark W. Sonderup Division of Hepatology Department of Medicine University of Cape Town & Groote Schuur Hospital Accelerated Fibrosis in HIV-HCV co-infected
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
Hepatitis C Elimination: Screening, Linkage and Treatment. Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas
 Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
10/4/2016. Management of Hepatitis C Virus Genotype 2 or 3 Infection
 Management of Hepatitis C Virus Genotype 2 or 3 Infection Kenneth E. Sherman, MD, PHD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati Cincinnati, Ohio FORMATTED:
Management of Hepatitis C Virus Genotype 2 or 3 Infection Kenneth E. Sherman, MD, PHD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati Cincinnati, Ohio FORMATTED:
Hepatits C Criteria Direct Acting Antiviral Medications
 Hepatits C Criteria Direct Acting Antiviral Medications Harvoni-Formulary PA required 1. Is the patient being treated for a funded condition by the Oregon Health Plan? 2. Does the member have a diagnosis
Hepatits C Criteria Direct Acting Antiviral Medications Harvoni-Formulary PA required 1. Is the patient being treated for a funded condition by the Oregon Health Plan? 2. Does the member have a diagnosis
Hepatitis C: a treatment revolution
 Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O.
 Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Epclusa (Sofosbuvir/Velpatasvir) for HIV/HCV
 for HIV/HCV") Mountain West AIDS Education and Training Center Epclusa (Sofosbuvir/Velpatasvir) for HIV/HCV John Scott, MD, MSc Associate Professor University of Washington Jul 28, 2016 This presentation is intended
Mountain West AIDS Education and Training Center Epclusa (Sofosbuvir/Velpatasvir) for HIV/HCV John Scott, MD, MSc Associate Professor University of Washington Jul 28, 2016 This presentation is intended
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Disclosures. Hepatitis C: the 2016 Perspective. The Take Home. Glossary 12/9/16
 Disclosures Hepatitis C: the 2016 Perspective Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF I have received research grant support to UCSF related to HCV from the following:
Disclosures Hepatitis C: the 2016 Perspective Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF I have received research grant support to UCSF related to HCV from the following: