Clinical Studies and Recent Real-World Data with Sofosbuvir/Ledipasvir
|
|
|
- Carmel Young
- 5 years ago
- Views:
Transcription

1 Clinical Studies and Recent Real-World Data with Sofosbuvir/Ledipasvir Kalliopi Zachou Assistant Professor of Medicine University of Thessaly
2 Disclosures Speaker s bureau and advisory: Gilead Bristol





3 History of HCV therapy
 DIRECT ACTING ANTIVIRALS")
4 HOST TARGETING ANTIVIRALS (HTAs) DIRECT ACTING ANTIVIRALS (DAAs)
 Receptor binding and")

5 Manns MP, et al. Nat Rev Drug Discov HCV Life Cycle and Targets for Direct-Acting Antivirals (DAAs) Receptor binding and endocytosis Transport and release Fusion and uncoating (+) RNA Virion assembly Translation NS3/4 and polyprotein protease processing inhibitors Membranous web NS5B polymerase RNA inhibitors replication Nucleos(t)ide Non-nucleoside NS5A inhibitors replication and assembly
6 Updated February 24, 2016 J Hepatol2015 vol. 63 :

7 Nucleotide analog-based regimen Nucleotide-free triple comb Nucleotide-free double comb Pawlotsky Gastroenterology 2015
8 Greek guidelines for treatment of CHC
 Ledipasvir (LDV) Picomolar potency against HCV GT 1a and 1b Effective against NS5B RAV S282T Once-daily, oral, 90 mg LDV NS5A inhibitor Sofosbuvir")
9 Lawitz E, et al. EASL 2011, poster 1219; Cheng G, et al. EASL 2012, poster 1172; HARVONI (ledipasvir/sofosbuvir), Gilead Sciences International Ltd. SmPC,. Ledipasvir/Sofosbuvir: A Single Tablet Regimen (STR) Ledipasvir (LDV) Picomolar potency against HCV GT 1a and 1b Effective against NS5B RAV S282T Once-daily, oral, 90 mg LDV NS5A inhibitor Sofosbuvir (SOF) Potent antiviral activity against HCV GT 1 6 Effective against NS5A RAVs High barrier to resistance Once-daily, oral, 400-mg tablet SOF - NS5B nucleotide polymerase inhibitor Ledipasvir/Sofosbuvir STR Once-daily, oral fixed-dose (90/400 mg) combination tablet, RBV-free Limited DDIs, no food effect >2000 patients treated in clinical trials LDV NS5A inhibitor SOF - NS5B nucleotide polymerase inhibitor FDA Approval 10 October 2014 European Approval 18 November 2014
10

11 LDV/SOF Clinical Development Program ELECTR ON LONESTAR ERADICA TE HCV/HIV Coinfection ELECTRON- 2 ION-3 ION-2 ION-4 HCV/HIV Coinfection LONEST AR-3 French ANRS HCV/HIV Coinfection SYNERGY Egypt GT 4 SOLAR- 1 French GT 4,5 Russia GT 1, Cirrhotic Subjects Enrolled Korea/ Taiwan GT 1 Australia TAP IVDU SOLAR- 2 Japan GT 1 Nosoco mial HCV Bleeding Disorders ION-1 SIRIUS Retreatment GT 1 GT 1, incl. PI failures GT 4 GT 1/4 Immediate Post-liver Transplant GT 1/3 GT 4/5 Specific populations Post-renal Transplant Brain Imaging Study Sickle Cell Anaemia GT 1/3/6

12

13 LDV/SOF: phase 3 ION-1 ION-2 ION-3 N = 865 Treatment naïve 16% cirrhotic N = 440 Treatment experienced 20% cirrhotic; 1952 total patients (224 cirrhotics) N = 647 Treatment naïve Non-cirrhotic Wk 0 Wk 8 Wk 12 Wk 24 LDV/SOF + RBV ION-1 ION-2 LDV/SOF LDV/SOF + RBV ION-3 LDV/SOF LDV/SOF + RBV LDV/SOF Afdhal N, et al. N Engl J Med 2014 Afdhal N, et al. N Engl J Med 2014 Kowdley K, et al. N Engl J Med 2014
14 LDV/SOF Phase 3 (ION-1, ION-2, ION-3) Afdhal N, et al. N Engl J Med 2014 Afdhal N, et al. N Engl J Med 2014 Kowdley K, et al. N Engl J Med 2014 Overall Demographics Total N=1952 n (%) Mean age, y (range) 53 (18 80) Age > 65 yrs, n (%) 152 (8) Male, n (%) 1175 (60) Female 777 (40) Black, n (%) 308 (16) Hispanic, n (%) 181 (9) Mean BMI, kg/m 2 (range) 27 (18 56) BMI > 30, n (%) 501 (26) IL28B non-cc, n (%) 1469 (75) GT 1a, n (%) 1443 (74) Cirrhosis, n (%) 224 (12) Prior PI+PEG+RBV failures 231 (12)
15 LDV/SOF: phase 3 endpoints ION-1 ION-3 Primary endpoint: SVR 12 Secondary endpoints: SVR 4, SVR 24 Safety and tolerability Relapse Viral resistance to LDV and SOF during and after treatment ION-2 Primary endpoint: SVR 12 Secondary endpoints: SVR 4, SVR 24 Safety and tolerability Relapse Viral resistance to LDV and SOF during and after treatment Primary endpoint: SVR 12 Secondary endpoints: Non-inferiority of 8 weeks of LDV/SOF to the other treatment groups SVR 4, SVR 24 Safety and tolerability Relapse Viral resistance to LDV and SOF during and after treatment Afdhal N, et al. N Engl J Med 2014 Afdhal N, et al. N Engl J Med 2014 Kowdley K, et al. N Engl J Med 2014
16 SVR12 (%) SVR 12 (%) ION Phase 3 Program (ION-1, ION-2, ION-3) Results: efficacy summary (ITT Analysis) LDV/SOF LDV/SOF+RBV / 213* 211/ / / / / Weeks 24 Weeks 8 Weeks 12 Weeks 12 Weeks 24 Weeks ION-1 ION-3 60 ION-2 GT 1 treatment-naïve GT 1 treatment-naïve GT 1 treatment-experienced including cirrhotics non-cirrhotic including cirrhotics and PI failures 97% (1886/1951) overall SVR rate 20 Similar efficacy was observed between the RBV-free and RBV-containing treatment arms 3% (65/1951) did not achieve SVR 0 1.8% (36) relapsed LDV/SOF LDV/SOF 1.4% (27) were either lost to follow up or withdrew consent 8 Weeks 12 Weeks 0.1% (2) virologic breakthrough (both due to non-adherence) 208/ 216 Efficacy in Subjects with Baseline HCV RNA < 6 Million IU/mL / % 96% 107/ / / 111 *excluding one subject with genotype 4 infection Error bars represent 95% confidence intervals. Afdhal N, et al. N Engl J Med 2014 Afdhal N, et al. N Engl J Med 2014 Kowdley K, et al. N Engl J Med 2014


17 SVR12 (%) Results: SVR12 by presence of cirrhosis (ITT) ION-1/ -2 ION-1: treatment naive ION-2: treatment experienced Absence of Cirrhosis Cirrhosis Absence of Cirrhosis Cirrhosis 179/ / / / / / / / 36 83/ 87 19/ 22 89/ 89 18/ 22 22/ 22 22/ 22 LDV/SOF LDV/SOF + RBV LDV/SOF LDV/SOF + RBV LDV/SOF LDV/SOF + RBV LDV/SOF LDV/SOF + RBV 12 Weeks 24 Weeks 12 Weeks 24 Weeks Sulkowski M, IAC 2014, LBPE16
18 Pooled Safety ION Phase 3 Program (ION-1, ION-2, ION-3) n (%) LDV/SOF (N=1080) LDV/SOF+RBV (N=872) Adverse Event 800 (74%) 745 (85%) Treatment Related AEs 484 (45%) 617 (71%) Grade 3 AE 46 ( 4%) 45 ( 5%) SAE 34 (3%) 17 (2%) Treatment-Related SAE 4 (<1%) 1 (<1%) AEs Leading to Study Drug Modification/Interruption 6 (1%) 118 (14%) Treatment DC due to AE 6 (1%) 7 (1%) Death 0 0 The most common adverse reactions ( 10%) were fatigue and headache in subjects treated with 8, 12, or 24 weeks of LDV/SOF. Sulkowski M, IAC 2014, LBPE16
19 ION Phase 3 Program (ION-1, ION-2, ION-3) Pooled Summary of Adverse Events n (%) LDV/SOF 8 Weeks (N = 215) LDV/SOF 12 Weeks (N = 539) LDV/SOF 24 Weeks (N = 326) LDV/SOF+ RBV 8 Weeks (N = 216) LDV/SOF+ RBV 12 Weeks (N = 328) LDV/SOF+ RBV 24 Weeks (N = 328) Fatigue 45 ( 21%) 116 ( 22%) 79 ( 24%) 75 ( 35%) 124 ( 38%) 132 ( 40%) Headache 30 ( 14%) 113 ( 21%) 79 ( 24%) 54 ( 25%) 75 ( 23%) 99 ( 30%) Nausea 15 ( 7%) 61 ( 11%) 36 ( 11%) 38 ( 18%) 57 ( 17%) 57 ( 17%) Insomnia 11 ( 5%) 41 ( 8%) 30 ( 9%) 26 ( 12%) 63 ( 19%) 66 ( 20%) Diarrhoea 15 ( 7%) 40 ( 7%) 33 ( 10%) 13 ( 6%) 23 ( 7%) 31 ( 10%) Irritability 3 ( 1%) 22 ( 4%) 21 ( 6%) 29 ( 13%) 30 ( 9%) 36 ( 11%) Rash 3 ( 1%) 23 ( 4%) 21 ( 6%) 19 ( 9%) 32 ( 10%) 43 ( 13%) Arthralgia 9 ( 4%) 32 ( 6%) 27 ( 8%) 11 ( 5%) 27 ( 8%) 28 ( 9%) Cough 3 ( 1%) 18 ( 3%) 21 ( 6%) 12 ( 6%) 37 ( 11%) 41 ( 13%) Pruritus 2 ( 1%) 21 ( 4%) 10 ( 3%) 16 ( 7%) 32 ( 10%) 30 ( 9%) Sulkowski M, IAC 2014, LBPE16
 Patients with")
20 Conclusions ION Phase 3 Program (ION-1, ION-2, ION-3) Afdhal N, et al. N Engl J Med 2014 Afdhal N, et al. N Engl J Med 2014 Kowdley K, et al. N Engl J Med 2014 ION-1 ION-2 ION-3 LDV/SOF for 12 w achieved an SVR12 rate of 99% in treatment-naive GT 1 patients without cirrhosis (addition of RBV did not increase SVR12 rates) Patients with compensated cirrhosis achieved SVR12 of 94% with 12 or 24 w of treatment with LDV/SOF LDV/SOF for 8 or 12 weeks resulted in high SVR12 rates in GT 1 treatment-naïve patients without cirrhosis LDV/SOF for 12 w resulted in SVR12 of 94% in GT 1 patients who had failed PegIFN+RBV±PI (addition of RBV did not increase SVR12 rates) Patients who were treatment experienced and were non-cirrhotic had SVR12 rate of 95% with LDV/SOF for 12 weeks Patients who were treatment experienced and were cirrhotic had SVR12 rate of 100% with LDV/SOF for 24 weeks Host and viral factors traditionally associated with lower SVR rates did not affect SVR12 rates Baseline NS5A polymorphisms did not impact SVR rate LDV/SOF STR was well tolerated Addition of RBV contributed to a higher incidence of SAEs and laboratory abnormalities
21 Greek guidelines for treatment of CHC EASL (cirrhosis) 12 wk with RBV, or 24wk without RBV, or 24wk with RBV (if negative predictors of response)
22 The clinical data to support the use of Harvoni in patients infected with HCV genotype 3 are limited. The relative efficacy of a 12 week regimen consisting of ledipasvir/sofosbuvir + ribavirin, compared to a 24 week regimen of sofosbuvir + ribavirin has not been investigated. A conservative 24 weeks of therapy is advised in all treatment-experienced genotype 3 patients and those treatment-naïve genotype 3 patients with cirrhosis (Harvoni SmPC, Dec 2015).
 N=25 N=26")

 89 73 16/26")
23 SVR 12 % ELECTRON-2 (LDV/SOF±RBV) N=25 N=26 N=50 LDV/SOF LDV/SOF+RBV LDV/SOF+RBV Cirrhotics 4/25 (16%) 6/26 (23%) 22/50 (44%) /26 41/50 16/22
24 Greek guidelines for treatment of CHC Η εγκεκριμένη διάρκεια θεραπείας με Harvoni + RBV στο γονότυπο 3 είναι 24 εβδομάδες
25
 9 (43) Country of Origin Egypt, n (%) 6 (29) United States, n (%) 5 (24) Ethiopia, n (%) 4")
 7 (33) 19/20 * 95% SVR12 with LDV/SOF for GT 4 HCV No subject discontinued due to an")
26 SVR12, % NIAID SYNERGY Wk 0 Wk 12 Wk 24 N=21 LDV/SOF SVR12 Demographics Age 55 ± 10 Male, n (%) 14 (67) Black, n (%) 9 (43) Country of Origin Egypt, n (%) 6 (29) United States, n (%) 5 (24) Ethiopia, n (%) 4 (19) Cameroon, n (%) 3 (14) HCV RNA > 800,000 IU/mL, n (%) 13 (62) Treatment Experienced, n (%) 8 (38) Cirrhotic, n (%) 7 (33) 19/20 * 95% SVR12 with LDV/SOF for GT 4 HCV No subject discontinued due to an AE
 50 (30 62) Male, n (%) 11 (50) 17 (77) White, n (%) 19 (86) 17 (77) Cirrhosis, n (%) 1 (5) 9 (41) IL28B non-cc, n (%) 15 (68) 21 (95) Mean HCV RNA, log 10 IU/mL")
 GT 4a, n (%) 13 (59) 12 (55) GT 4d, n (%) 5 (23) 5 (23) GT 4b, 4f, 4m, 4o, 4r, n (%) 4 (18) 5 (23) 21/22 TN 20/22 TE 31/34 No 10/10 Yes Treatment Status Cirrhosis No")
27 SVR12 (%) LDV/SOF in GT 4 Patients Multicenter study in GT 4 patients in France Week N=44 LDV/SOF SVR12 Naïve n=22 Experienced n=22 Mean age, years (range) 52 (21 69) 50 (30 62) Male, n (%) 11 (50) 17 (77) White, n (%) 19 (86) 17 (77) Cirrhosis, n (%) 1 (5) 9 (41) IL28B non-cc, n (%) 15 (68) 21 (95) Mean HCV RNA, log 10 IU/mL (range) 6.0 ( ) 6.3 ( ) GT 4a, n (%) 13 (59) 12 (55) GT 4d, n (%) 5 (23) 5 (23) GT 4b, 4f, 4m, 4o, 4r, n (%) 4 (18) 5 (23) 21/22 TN 20/22 TE 31/34 No 10/10 Yes Treatment Status Cirrhosis No subjects D/C study due to AEs LDV/SOF for 12 weeks was highly effective and well tolerated, without the need for RBV Abergel, EASL, 2015, O056
28 Greek guidelines for treatment of CHC EASL (cirrhosis) 12 wk with RBV, or 24wk without RBV, or 24wk with RBV (if negative predictors of response)
29 LDV NS5A inhibitor SOF - NS5B nucleotide polymerase inhibitor Failure to prior treatment with DAAs HCV/HIV co-infection Advanced cirrhosis/ post transplant Patients with hemoglobulinopathies
 Wk 0 Wk 12 Wk 24 N=77 LDV/SOF + RBV Placebo N=78 Placebo LDV/SOF + RBV 74/77 75/77 LDV/SOF+RBV 12 Weeks LDV/SOF 24 Weeks TE cirrhotics")
30 LDV/SOF in cirrhotic patients Gen 1 who previously failed PI- Based triple therapy (SIRIUS) Double-blind, placebo-controlled study in cirrhotic GT1 subjects who failed both PegIFN+RBV and PI+PegIFN+RBV regimens in France (null or partial responders) Wk 0 Wk 12 Wk 24 N=77 LDV/SOF + RBV Placebo N=78 Placebo LDV/SOF + RBV 74/77 75/77 LDV/SOF+RBV 12 Weeks LDV/SOF 24 Weeks TE cirrhotics had a similar response to LDV/SOF+RBV for 12 weeks and LDV/SOF for 24 weeks Bourliere et al, Lancet Inf Dis 2015
31 SIRIUS: Retreatment of Cirrhotic Subjects Who Failed Both PegIFN+RBV and PI+PegIFN+RBV Results: Adverse Events 15% Placebo 12 Wk LDV/SOF + RBV 12 Wk LDV/SOF 24 Wk Preferred term, n (%) Placebo 12 Wk n=77 Second 12 Wk n=76 Most AEs mild or moderate in severity Overall Period n=77 First 12 Wk n=78 Overall Period n=78 Asthenia 24 (31) 29 (38) 45 (58) 28 (36) 35 (45) Headache 16 (21) 13 (17) 21 (27) 27 (35) 31 (40) Pruritus 14 (18) 11 (14) 22 (29) 4 (5) 7 (9) Insomnia 9 (12) 7 (9) 17 (22) 11 (14) 13 (17) Nausea 8 (10) 8 (11) 14 (18) 7 (9) 8 (10) Fatigue 3 (4) 5 (7) 7(9) 13 (17) 15 (19) Dry skin 6 (8) 5 (7) 12 (16) 4 (5) 4 (5) Arthralgia 5 (6) 0 6 (8) 6 (8) 12 (15) Bronchitis 1 (1) 4 (5) 4 (5) 4 (5) 13 (17) Bourliere et al, Lancet Inf Dis 2015
32 SIRIUS: Retreatment of Cirrhotic Subjects Who Failed Both PegIFN+RBV and PI+PegIFN+RBV Conclusions 97% of prior PI-failure subjects with cirrhosis achieved SVR12 Similar SVR12 rates after 12 weeks of LDV/SOF with RBV compared with 24 weeks of LDV/SOF LDV/SOF with and without RBV was well tolerated Only two AEs (headache and fatigue) occurred at a higher frequency with LDV/SOF compared with placebo The majority of these AEs were mild to moderate in severity 12 weeks of LDV/SOF with RBV results in high SVR rates among treatment-experienced subjects with cirrhosis who have failed a prior PIbased regimen Bourliere et al, Lancet Inf Dis 2015

33 HCV RNA <LLOQ, % LDV/SOF ± RBV in treatment experienced GT 1 HCV (SOF Study Retreatment/ ELECTRON-2/ SYNERGY * 50/51 19/19 14/14 SOF Retreatment Study ELECTRON-2 SYNERGY *One subject who relapsed had GT 3a infection LDV/SOF ± RBV for 12 weeks achieved 100% SVR in GT 1 subjects who failed prior SOF-based therapy Wyles, AASLD, 2014, Oral #235 Gane, EASL, 2014, Oral #6 Osinusi, et al. Ann Intern Med. 2014
 Mean age, years (range) 58 (35-71) Male, n (%) 34 (83) Black, n (%) 10 (24) Cirrhosis, n (%) 19 (46) IL28B non-cc, n")
 *All 11 had failed 8 weeks of LDV/SOF No NS5B SOF-associated variants (S282T, L159F, V321A) detected at baseline Of 12 patients with NS5A RAVs at baseline who failed treatment, NS5B and NS5A")
34 Retreatment of Patients Who Failed 8 or 12 Weeks of LDV/SOF- Based Regimens With LDV/SOF for 24 Weeks Wk 0 Wk 12 Wk 24 Wk 36 SOF failures (n=51) LDV/SOF failures* (n=41) LDV/SOF + RBV LDV/SOF SVR12 98% SVR12 71% *LDV/SOF failures from ION 1-3, LONESTAR and TRILOGY-1 GT 1 (n=41) Mean age, years (range) 58 (35-71) Male, n (%) 34 (83) Black, n (%) 10 (24) Cirrhosis, n (%) 19 (46) IL28B non-cc, n (%) 38 (93) 100% SVR n=11/11 27% No n=11/41* Baseline NS5A RAVs 73% Yes n=30/41 40% Failure n=12/30 60% SVR n=18/30 Mean HCV RNA, log 10 IU/mL (range) 6.2 ( ) *All 11 had failed 8 weeks of LDV/SOF No NS5B SOF-associated variants (S282T, L159F, V321A) detected at baseline Of 12 patients with NS5A RAVs at baseline who failed treatment, NS5B and NS5A variants were detected in 4 and 12 patients, respectively Wyles, AASLD, 2014, Oral #235 Lawitz, et al. EASL 2015, O005
35 LDV NS5A inhibitor SOF - NS5B nucleotide polymerase inhibitor Failure to prior treatment with DAAs HCV/HIV co-infection Advanced cirrhosis/ post transplant Patients with hemoglobulinopathies
 52 (26-72) Male, n (%) 276 (82) Black, n (%) 115 (34) Hispanic or Latino, n (%) 56 (17) Mean BMI, kg/m 2 (range) 27 (18-66) IL28B CC, n (%) 81")
36 Study Design ION-4 Phase 3, multicenter, open-label study in US, PR, Canada, and New Zealand Wk 0 Wk 12 Wk 24 GT 1 and 4 TN and TE N=335 LDV/SOF SVR12 HIV-1 positive, HIV RNA <50 copies/ml; CD4 cell count >100 cells/mm 3 Demographics Mean age, y (range) 52 (26-72) Male, n (%) 276 (82) Black, n (%) 115 (34) Hispanic or Latino, n (%) 56 (17) Mean BMI, kg/m 2 (range) 27 (18-66) IL28B CC, n (%) 81 (24) GT 1, n (%) 327 (98) HCV treatment experienced, n (%) 185 (55) Cirrhosis, n (%) 67 (20) Demographics Mean HCV RNA, log 10 IU/mL ± SD 6.7 ± 0.6 Median CD4 cell count, cells/µl (range) 628 ( ) HIV ART, n (%) Efavirenz + FTC + TDF 160 (48) Raltegravir + FTC + TDF 146 (44) Rilpivirine + FTC + TDF 29 (9) FTC, emtricitabine; TDF, tenofovir disoproxil fumarate Naggie et al, NEJM 2015
 achieved an SVR12 Naggie et al, NEJM")
37 SVR12 (%) ION-4: LDV/SOF in HIV/HCV Results Overall Naïve vs Experienced Cirrhosis Status 321/ / / /268 63/67 LDV/SOF 12 Weeks Naïve Experienced No Cirrhosis Cirrhosis Among those who were treatment-experienced with cirrhosis, 98% (46/47) achieved an SVR12 Naggie et al, NEJM 2015
 Grade 3 4 laboratory abnormality 36 (11) Patients, n (%) LDV/SOF 12 Weeks N=335 Headache 83 (25) Fatigue 71 (21) Diarrhea 36 (11) Nausea 33 (10) Arthralgia 22 (7) Upper respiratory tract")
38 ION-4: LDV/SOF in HIV/HCV Safety Summary Adverse Events (> 5%) Overall safety Patients, n (%) LDV/SOF 12 Weeks N=335 AEs 257 (77) Grade 3 4 AE 14 (4) Serious AE 8 (2)* Treatment D/C due to AE 0 Death 1 (<1) Grade 3 4 laboratory abnormality 36 (11) Patients, n (%) LDV/SOF 12 Weeks N=335 Headache 83 (25) Fatigue 71 (21) Diarrhea 36 (11) Nausea 33 (10) Arthralgia 22 (7) Upper respiratory tract infection 18 (5) *Serious AEs in >1 patient were hepatocellular carcinoma (n=2) and portal vein thrombosis (n=2) in patients with cirrhosis. Confirmed IV drug user developed Staphylococcus aureus sepsis, endocarditis with associated embolic brain abscesses, and multi-organ system failure. Naggie et al, NEJM 2015

39 SVR12 (%) LDV/SOF x 12 Weeks SVR12 in HCV Mono-infected and HCV/HIV Co-infected 520/538 HCV Mono-infected ION 1, /385 HIV/HCV Co-infected ION4, ERADICATE Similar response rates in HCV/HIV co-infected patients compared to HCV mono-infected patients Afdhal N, et al. N Engl J Med 2014; 370: ; Afdhal N, et al. N Engl J Med 2014; 370: ; Kowdley K, et al. N Engl J Med 2014; 370: ; Naggie et al, CROI 2015, Oral #LB-152; Osinusi A, et al JAMA Published online February 23, 2015
40 LDV NS5A inhibitor SOF - NS5B nucleotide polymerase inhibitor Failure to prior treatment with DAAs HCV/HIV co-infection Advanced cirrhosis/ post-transplant Patients with hemoglobulinopathies
41 SOLAR-1 and SOLAR-2 LDV/SOF+RBV for 12 or 24 Weeks in 659 Decompensated and Post-Liver Transplant HCV GT 1 and GT 4 Patients Week Pre-Transplant N= 215 CTP B (7 9) CTP C (10 12) Fibrosis (F0 F3) LDV/SOF + RBV SVR12 Post-Transplant N= 444 CTP A (5 6) CTP B (7 9) CTP C (10 12) LDV/SOF + RBV SVR12 FCH Broad inclusion criteria: No hepatocellular carcinoma (HCC) Total bilirubin 10 mg/dl, Haemoglobin 10 g/dl CrCl 40 ml/min, Platelets > 30,000/mL RBV dosing FCH, Metavir F0 F3 and CTP A cirrhosis: weight-based (1000 mg or 1200 mg) CTP B and C cirrhosis (pre- and post-transplant: dose escalation, mg/d Charlton et al, Gastroenterology 2015 Manns et al, Lancet Infect Dis 2016
42 SOLAR-1/2: Decompensated and Post-Liver Transplant Patients Demographics Pre-Transplant Post-Transplant Patients, n (%) HCV GT, n (%) CTP B + C n=215 F0 3 + CTP A n=330 CTP B + C n=114 Total n=659 1a 124 (58) 197 (60) 71 (62) 392 (59) 1b 78 (36) 111 (34) 36 (32) 225 (34) 4 13 (6) 22 (7) 7 (6) 42 (6) IL28B non-cc, n (%) 167 (77) 272 (83) 92 (81) 431 (81) Prior HCV treatment, n (%) 150 (70) 270 (82) 96 (84) 516 (78) Cirrhosis, n (%) 215 (100) 118 (36) 114 (100) 447 (68) Median egfr, ml/min/1.73 m 2 (range) 84 (34 224) 63 (20 132) 64 (29 124) 69 (20 224) MELD, n (%) <10 24 (11) 64 (54) 26 (23) 114 (26) (61) 51 (43) 69 (61) 252 (56) (25) 3 (3) 16 (14) 73 (16) (2) 0 3 (3) 8 (2) Median albumin, g/dl (range) 2.8 ( ) 3.9 ( ) 3.0 ( ) NR Median platelets, x 10 3 /µl (range) 76 (27 212) 136 (35 434) 90 (32 237) NR Ascites, n (%) 163 (76) 9 (3) 83 (73) NR Encephalopathy, n (%) 140 (65) 4 (1) 53 (46) NR NR, not reported Charlton et al, Gastroenterology 2015 Manns et al, Lancet Infect Dis 2016
43 SOLAR-1 and SOLAR-2 Results Analysis excluded 13 patients transplanted prior to posttreatment Week (FU) 12 with HCV RNA <LLOQ at last measurement prior to transplant, and 3 pretransplant patients who were CTP A at baseline. Error bars represent 95% confidence intervals (CIs). Charlton et al, Gastroenterology 2015 Manns et al, Lancet Infect Dis 2016
44 SOLAR-1/2: Decompensated and Post-Liver Transplant Patients Safety Summary Pre-Transplant Post-Transplant Patients, n (%) CTP B + C n=215 F0 3 + CTP A n=330 CTP B + C n=114 Total n=659 Any AE 208 (97) 316 (96) 109 (96) 633 (96) Grade 3 4 AE 51 (24) 76 (23) 33 (29) 160 (24) Serious AE 61 (28) 49 (15) 34 (30) 144 (22) Serious treatment-related AE 5 (2) 10 (3) 4 (4) 19 (3) AE leading to D/C of LDV/SOF 9 (4) 5 (2) 5 (4) 19 (3) Death 10 (5) 4 (1) 6 (5) 20 (3) Rejection episode Graft loss Liver transplantation Treatment-related SAEs were mostly related to RBV treatment Deaths and AEs that led to D/C of LDV/SOF were not attributed to study treatment LDV/SOF+RBV was well tolerated in decompensated cirrhosis and post-transplantation Charlton et al, Gastroenterology 2015 Manns et al, Lancet Infect Dis 2016
45 SOLAR-1 and SOLAR-2 MELD Score Change from Baseline to FU-24 in CTP B/C Patients Who Achieved SVR12 Gane, AASLD, 2015, 1049 No FU-24 assessment for *9 patients, 9 patients.

46 LDV NS5A inhibitor SOF - NS5B nucleotide polymerase inhibitor Failure to prior treatment with DAAs HCV/HIV co-infection Advanced cirrhosis/ post-transplant Patients with hemoglobulinopathies


")

47 AASLD 2015 Patients N= 24 Genotype 1a 1b 1a/4c 1a/1b 1a/ All Sofosbuvir /Ledipasvir 12w SVR 12: 22/24 (91.7%) Stage (metavir) F0-F1 F2 F3/F Failure: 2/24 (gen 1a/4c and 1a/3) Side effects: mild (gastrointestinal 17/24, headache 6/24, insomnia 8/24, anemia 2/24, urinary tract infection 3/24)





48
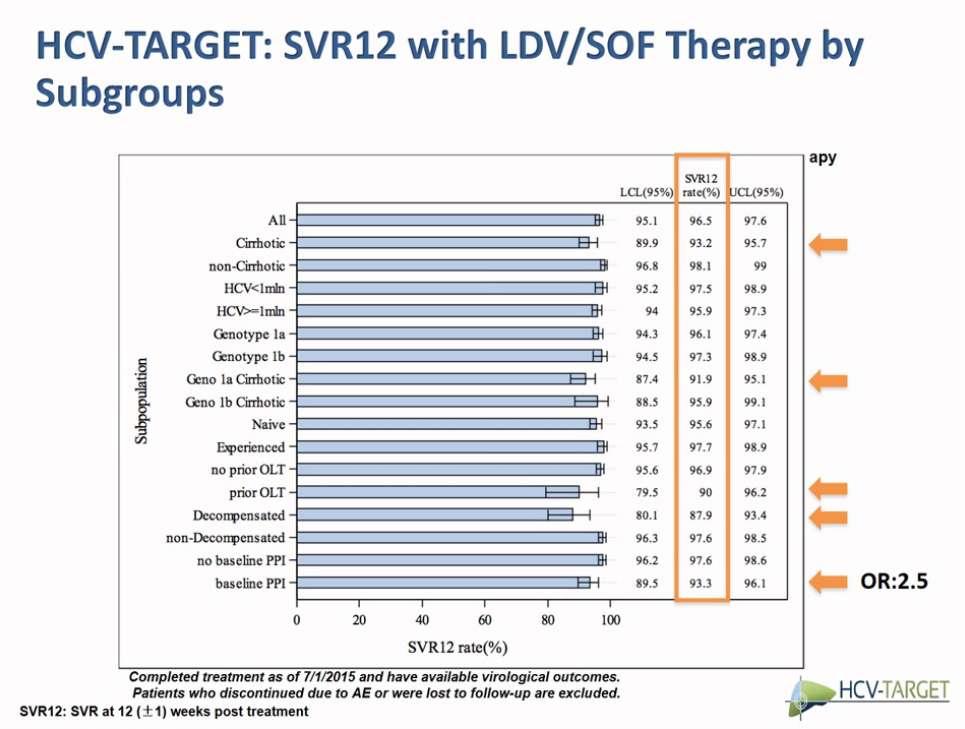
49 Real life data LDV/ SOF: 3 large studies in AASLD 2015 (VA)- Effectiveness of Ledipasvir/ Sofosbuvir in Treatment Naïve Genotype 1 Patients Treated in Routine Medical Practice; Backus Abst % cirrhotics 3763 LDV/SOF 602 LDV/SOF+RBV (HCV-TARGET) -Treatment Outcomes With 8, 12 and 24 Week Regimens of Ledipasvir/Sofosbuvir for the Treatment of Hepatitis C Infection: Analysis of a Multicenter Prospective, Observational Study; Terrault Abst with virol outcome 47% TE 38% cirrhotics 13% Ch B-C LDV/SOF 105 LDV/SOF+RBV LDV/SOF (Trio)- Failure with All-Oral DAA Regimens:Academic and Community Treatment of a Real-World Popu-lation from the TRIO Network; Afdhal Abst LB17; Curry Abst % TE 30% cirrhotics 76 LDV/SOF+RBV 41 SIM+SOF±RBV 47 VKP± RBV


50 HCV-TARGET (Terrault, abstr 94) VA (Backus, abstr 93)

51 TRIO (Afdhal abstr LB17) PrOD +/- RBV The results shown here have been derived from a real life patient cohort and not from a randomised trial involving direct comparison of therapeutic factors, therefore they do not suggest such comparison. PrOD: paritaprevir, ritonavir, ombitasvir, dasabuvir, SMV: Simeprevir PrOD +/- RBV

52 AASLD, 2015

53

54
55

56 N. Terrault, Debrief AASLD 2015
 age, years 50 (22 77) Male gender, n (%) 43 (42) Caucasian, n (%) 103 (100) Genotype, n (%) GT 1a GT 1b GT 4 Metavir stage, n (%) F0 F1 F2 F3 Baseline Demographics 49 (46) 52 (51) 2")
57 SVR12 % German Real-World LDV/SOF for 8 Weeks Single center German study of 103 primarily naïve, non-cirrhotic patients with baseline HCV RNA < 6 million IU/mL treated with LDV/SOF for 8 weeks N=103 Median (range) age, years 50 (22 77) Male gender, n (%) 43 (42) Caucasian, n (%) 103 (100) Genotype, n (%) GT 1a GT 1b GT 4 Metavir stage, n (%) F0 F1 F2 F3 Baseline Demographics 49 (46) 52 (51) 2 (2) 56 (54) 25 (24) 17 (17) 5 (5) Median baseline HCV RNA, IU/mL* 870,964 Treatment-naïve, n (%) 100 (97) HIV/HCV coinfection, n (%) 3 (3) At least one comorbidity, n (%) 94 (91) SVR12 103/103 LDV/SOF for 8 weeks resulted in high rates of SVR12 and was well tolerated 2.3% (n=2) had Grade 3 or 4 AEs No AE led to treatment discontinuation or death *Roche COBAS AmpliPrep/COBAS TaqMan, cut-off < 12 IU/mL including 3 PegIFN+RBV Relapsers Fibrosis was measured by FibroScan with cut-off values for METAVIR stage F3 or less of 12.3kPa. Buggisch, AASLD, 2015, 1205.
 72 (49) Median age, years (IQR) 52 (44 58) GT 1, n (%) 144 (97) GT 4, n (%) 3 (2) HIV/HCV coinfection, n (%) 28 (19) Prior HCV treatment, n (%)")
58 GECCO Real-World Cohort LDV/SOF for 8 Weeks in HCV-Monoinfected and HIV/HCV- Coinfected Patients: Interim Analysis Real-world data from Germany on 148 GT 1 and 4 HCV patients receiving LDV/SOF for 8 weeks Baseline Demographics Patients n=148 Male, n (%) 72 (49) Median age, years (IQR) 52 (44 58) GT 1, n (%) 144 (97) GT 4, n (%) 3 (2) HIV/HCV coinfection, n (%) 28 (19) Prior HCV treatment, n (%) 26 (18) FibroScan >12.5 kpa or APRI >2, n (%) 5 (3) Median HCV viral load, IU/mL (IQR) 8.1 x 10 5 (2.5 x x 10 6 ) High viral load* 13 (8.8) *1 patient relapsed High viral load defined as >6M IU/mL (Roche) or >2M IU/mL (Abbott) at baseline * Christensen, AASLD, 2015, 1081


59 Gane, AASLD, 2015, 1049; Kwok, AASLD 2015, 1101; Shoreibah, AASLD 2015, 1174; Hassett, AASLD, 2015, LB-28 SVR12 Rates Among Patients with Recurrent HCV Post-Liver Transplant LDV/SOF+RBV 12 weeks LDV/SOF+RBV 24 weeks LDV/SOF 12 weeks 21% F3-F4 24% F4 Noncirrho tics 102/ / / 60 56/ 58 40/ 41 F0 F3 CTP A Kwok, et al. Shoreibah, et al. Hassett, et al. 11/ 11 28/ 28 18/ 18 SOLAR-1 and SOLAR-2 Real-World (Non-cirrhotic and cirrhotic)

60 Conclusions Clinical trials found high SVR12 rates of LDV/SOF in patients with Gen 1 (and 4) in different groups of patients with CHC Real world data support the high SVR12 rates of LDV/ SOF found in clinical trials in Gen 1 HCV patients




61
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Learning Objective. After completing this educational activity, participants should be able to:
 Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Learning Objective After completing this educational activity, participants should be able to: Use patient characteristics and preferences to select HCV treatment strategies that maximize the potential
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Preliminary Results of an Evaluation of Ledipasvir/Sofosbuvir in Patients with Chronic HCV or HCV/HIV Co-Infection
 Preliminary Results of an Evaluation of Ledipasvir/Sofosbuvir in Patients with Chronic HCV or HCV/HIV Co-Infection Konstantin Zhdanov 1, Viacheslav Morozov 2, Elena A Orlova-Morozova 3, Riina Salupere
Preliminary Results of an Evaluation of Ledipasvir/Sofosbuvir in Patients with Chronic HCV or HCV/HIV Co-Infection Konstantin Zhdanov 1, Viacheslav Morozov 2, Elena A Orlova-Morozova 3, Riina Salupere
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos
 Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
The ASTRAL Program Abstracts LB-2, LB-12, 205, 209
 The ASTRAL Program Abstracts LB-2, LB-12, 5, 9 The ASTRAL Program FDC 1. 2. 3. 4. 5. SOF Nucleotide polymerase inhibitor VEL NS5A inhibitor ASTRAL1 GT1, 2, 4 6 ASTRAL2 GT2 Jacobson IM, et al. N Engl J
The ASTRAL Program Abstracts LB-2, LB-12, 5, 9 The ASTRAL Program FDC 1. 2. 3. 4. 5. SOF Nucleotide polymerase inhibitor VEL NS5A inhibitor ASTRAL1 GT1, 2, 4 6 ASTRAL2 GT2 Jacobson IM, et al. N Engl J
SOLAR-1 (Cohorts A and B)
") Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; 149:649-59. Ledipasvir-Sofosbuvir
Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; 149:649-59. Ledipasvir-Sofosbuvir
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Phase 3. Treatment Experienced. Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2. Afdhal N, et al. N Engl J Med. 2014;370:
 Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
Case 2: A 71-year-old man with cirrhosis
 Case 2: A 71-year-old man with cirrhosis 1 JM, 71 year old African American male with known cirrhosis Asymptomatic apart from fatigue No prior history of decompensation Past history: Diabetes for 11 years
Case 2: A 71-year-old man with cirrhosis 1 JM, 71 year old African American male with known cirrhosis Asymptomatic apart from fatigue No prior history of decompensation Past history: Diabetes for 11 years
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Hepatitis C: New Therapies in
 Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
NS5A inhibitors: ideal candidates for combination?
 NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
IFN-free for Genotype 1 HCV: the current landscape. Prof. Graham R Foster
 IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
HCV Update from AASLD 2016
 HCV Update from AASLD 2016 Ahmed Elsharkawy Consultant Hepatologist QE Birmingham Secretary and Chair-Elect of BVHG BHIVA/BVHG Feedback Meeting November 2016 Speaker Name Ahmed Elsharkawy Statement Speaking
HCV Update from AASLD 2016 Ahmed Elsharkawy Consultant Hepatologist QE Birmingham Secretary and Chair-Elect of BVHG BHIVA/BVHG Feedback Meeting November 2016 Speaker Name Ahmed Elsharkawy Statement Speaking
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
HIV-HCV coinfection. Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland
 HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
HIV-HCV coinfection Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Baltimore, Maryland Disclosures Principal investigator for research grants Funds paid to Johns Hopkins
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
SOLAR-1 (Cohorts A and B)
") Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; [Epub ahead of print]
Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; [Epub ahead of print]
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING. Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona
 TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
Hepatitis C: New Antivirals in the Liver Transplant Setting. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Epclusa (Sofosbuvir/Velpatasvir) for HIV/HCV
 for HIV/HCV") Mountain West AIDS Education and Training Center Epclusa (Sofosbuvir/Velpatasvir) for HIV/HCV John Scott, MD, MSc Associate Professor University of Washington Jul 28, 2016 This presentation is intended
Mountain West AIDS Education and Training Center Epclusa (Sofosbuvir/Velpatasvir) for HIV/HCV John Scott, MD, MSc Associate Professor University of Washington Jul 28, 2016 This presentation is intended
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Summary from AASLD 2014 for Hepatitis C Boston 7-11 November 2014
 Summary from AASLD 2014 for Hepatitis C Boston 7-11 November 2014 Feedback from the real-world: do HCV cure rates in real-life patient cohorts hold what clinical trials promised? Summary from AASLD 2014
Summary from AASLD 2014 for Hepatitis C Boston 7-11 November 2014 Feedback from the real-world: do HCV cure rates in real-life patient cohorts hold what clinical trials promised? Summary from AASLD 2014
Hepatitis C 17 months experience with Sofosbuvir/Ledipasvir (Harvoni)
") Hepatitis C 17 months experience with Sofosbuvir/Ledipasvir (Harvoni) Prof. Dr. Markus Cornberg Klinik für Gastroenterologie, Hepatologie und Endokrinologie Antalya, 13.05.2016 Markus Cornberg, Hannover
Hepatitis C 17 months experience with Sofosbuvir/Ledipasvir (Harvoni) Prof. Dr. Markus Cornberg Klinik für Gastroenterologie, Hepatologie und Endokrinologie Antalya, 13.05.2016 Markus Cornberg, Hannover
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Addressing Unmet Medical Needs in HCV Genotype 3
 Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
Disclosures. I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences.
 Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences. Chronic Hepatitis C Prof CL Lai University Department of
Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences. Chronic Hepatitis C Prof CL Lai University Department of
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Treating HCV Prior to Liver Transplantation. What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona
 Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Treatment of Patients with HCV and HIV
 Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Treatment of Patients with HCV and HIV BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Four Questions Is HIV/HCV
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College
 Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Ari Bunim, M.D. Director of Hepatology New York Hospital Queens Assistant Professor of Clinical Medicine Weill Cornell Medical College New York State Law Goes into Effect January 1, 2014 Hepatitis C Virus
Treatment of Hepatitis C Recurrence after Liver Transplantation. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Antiviral treatment in Unique Populations
 Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Antiviral treatment in Unique Populations Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Unique HCV Populations HIV/HCV co-infected
Global Prevalence of HBV, HCV, HIV
 Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Treatment of Patients with HCV and HIV Paul Y. Kwo, MD, FACG Professor of Medicine Stanford University email: pkwo@stanford.edu Global Prevalence of HBV, HCV, HIV 24 m Journal of Clinical Virology Page
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
PEARL-I. Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4. Treatment Naïve and Treatment Experienced
 Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
DAA-based treatment in cirrhotic and post-transplanted patients. Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France
 DAA-based treatment in cirrhotic and post-transplanted patients Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France Cirrhosis and transplantation 2 populations with similar issues Hepatic impairment
DAA-based treatment in cirrhotic and post-transplanted patients Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France Cirrhosis and transplantation 2 populations with similar issues Hepatic impairment
8/5/2014. A new era of HCV clinical management. Direct-Acting Antivirals for Hepatitis C. Goal of HCV treatment is viral cure HIV HBV HCV
 NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World
 Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki
 O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research
O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research
Harvoni. Harvoni (ledipasvir & sofosbuvir) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.03.32 Subject: Harvoni Page: 1 of 7 Last Review Date: December 3, 2015 Harvoni Description Harvoni (ledipasvir
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.03.32 Subject: Harvoni Page: 1 of 7 Last Review Date: December 3, 2015 Harvoni Description Harvoni (ledipasvir
Management of HCV in Decompensated Liver Disease
 Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),