NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP
|
|
|
- Rosanna Phillips
- 6 years ago
- Views:
Transcription
1
2
3 PROGNOSIS Mortality rates as high as 18-30% are reported for hyponatremic patients. High mortality rates reflect the severity of underlying conditions and are not influenced by treatment of hyponatremia (Hochman I, et al. Isr J Med Sci. 1989;25:73-6).
4
5 NATURAL HISTORY AND SURVIVAL OF PATIENTS WITH ASCITES. PATIENTS WHO DO NOT DEVELOP COMPLICATIONS HAVE MARKEDLY BETTER SURVIVAL THAN THOSE WHO DEVELOP DILUTIONAL HYPONATREMIA, REFRACTORY ASCITES, OR HEPATORENAL SYNDROME.
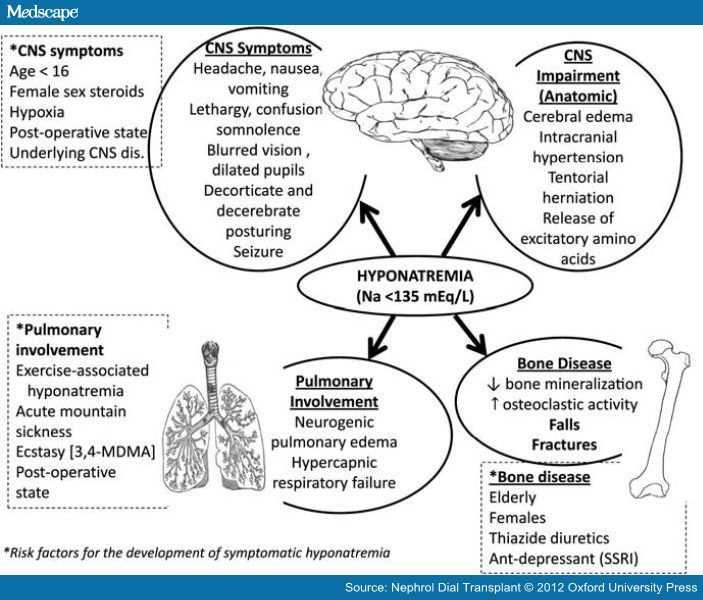
6 HYPONATREMIA AND HEART FAILURE HAVE SEVERAL OVERLAPPING SYMPTOMS.
7
8 PREVALENCE Most common electrolyte disorder encountered in hospitalized patients. Prevalence at initial presentation to acute care setting reported as high as 28% (Hawkins RC. Clin Chim Acta 2003;337:169-72) 72). Prevalence of hyponatremia in hospitalized patients has been reported as 15-18%. 18%. Common in nursing home residents (18% prevalence).
9
10 A 76-YEARS LADY RESIDING IN A NURSING HOME She was seen by general practitioner (GP) because of high blood pressure (BP 165/85 mmhg). In her history no particular medical problems were recorded, although she was treated with low dose aspirin.
11 GP diagnosed mild hypertension and prescribed hydrochlorthiazide (25 mg/day). Moreover the lady was advised to reduce as much as possible her dietary salt intake. Six weeks later her BP went down to 135/80 mmhg, however some changes in her mental status were recorded.
12 SYMPTOMS She was less alert She had difficulties in concentrating Her appetite decreased, she could only drink fluids She had increasing gait instability She suffered a fall, fortunately without any fractures
13 PHYSICAL EXAMINATION Normal skin turgor (it is not easy to evaluate skin turgor in older adults) No orthostatic fall in BP or acceleration of the pulse BP 125/80 mmhg No focal neurological findings Evident gait disturbance that necessitated a walker for ambulation Body weight stable around 58 Kg
14 LABORATORY TESTS PLASMA Na 116 K 2.8 Cl 74 HCO3 30 SCr 1.4 mg/dl Osmolality 244 Uric acid 4.9 mg/dl URINE 65 mmol/l 60 mmol/l 60 mmol/l 340 mosm/kg water
15 CALCULATIONS Glomerular filtration rate 39 ml/min/m 2 Fractional excretion of uric acid 9%
16 DIAGNOSIS Acute renal failure Hyponatremia (hypotonic) Hypokaliemia Mild metabolic alkalosis Gait disturbance Normal total body water
17 KEY POINTS
18 IS HYPONATREMIA REALLY HYPOTONIC? A decrease in serum Na reflects a state of hypotonicity. Both Na and osmolality are low Consider concentration of solutes that do not cross the cell membrane glucose mannitol lipid protein
19 IS THERE AN EMERGENCY PRESENT ON ADMISSION NECESSITATING ACUTE THERAPEUTIC ACTION TO IMPROVE THE ELECTROLYTE DISTURBANCE? Symptoms pointed to chronic hyponatremia. Acute hyponatremia usually develops in 48 hours
20 WHAT IS THE BEST APPROACH TO OBTAINING A CORRECT DIAGNOSIS? Evaluation of the status of extracellular fluid volume (ECFV) is critical hypervolemic, Hypovolemic, euvolemic hyponatremia, thus determining the treatment strategy Risk of hyponatremia is higher in older adults in whom evaluation of volemic status is difficult.
21 FIRST STEP IS DETERMINATION OF URINARY SODIUM (SPOT URINE) HYPOVOLEMIC OR HYPERVOLEMIC DISORDERS U-Na<30 mmol/l SYNDROME OF INAPPROPRIATE ANTIDIURESIS (SIAD) U-Na>30 mmol/l U-Na is of limited diagnostic utility in subjects on diuretic therapy due to inhibition of tubular Na reabsorption. In patients using diuretics a fractional excretion of uric acid<12% may be useful.
22 Contraction of ECFV decreases Expansion of ECFV enhances FEUa FEUa Case: U-Na FE UA 9 % UA 65 mmol/l

23 WHAT IS THE BEST APPROACH TO RAISE SERUM NA? Drugs known to be associated with syndrome of inappropriate antidiuresis (SIAD)

24 WHAT IS THE BEST APPROACH TO RAISE SERUM NA? Aging decreases the excretion of water due to reduced expression of Na-K-Cl cotransporter in the ascending limb of the loop of Henle and the Na-Cl cotransporter in the distal tubule (free water clearance is limited)
25 WHAT ARE THE RISK FACTORS, SYMPTOMS AND PATHOPHYSIOLOGY OF THIAZIDE INDUCED HYPONATREMIA? The relative risk of hyponatremia is approximately 60% higher in patients exposed to thiazide diuretics compared to alternative therapy, especially if they are treated with selective serotonin reuptake inhibitors. Thiazide diuretics may induce both inappropriate ADH secretion and ADH- independent water retention (Hix JK. Semin nephrol 2011; 31: ). Thiazide diuretics block sodium chloride cotransport in the distal tubule. Low distal delivery of filtrate and water reabsorption by residual water permeability
26
27 WHAT IS THE ROLE OF HYPOKALEMIA IN THE PATHOPHYSIOLOGY OF HYPONATREMIA? Hypokalemia induced by thiazide diuretics is an independent predictive factor for the development of hyponatremia. Potassium depletion results in a shift of sodium into the cells with a commensurate exit of potassium from the cell into extracellular fluid
28 WHAT ARE THE OPTIONS FOR THERAPY TO RAISE THE PLASMA SODIUM IN THIS PATIENT? The main goal was to administer NaCl 0.9% + KCl aiming at raising plasma Na to an upper limit of ~8 mmol/l per 24 h due to the risk of osmotic demyelinization. In the case like this one physicians should pay particular attention to plasma sodium correction at the time of diuresis onset, it could be that water diuresis, leading to a rapid rise in plasma Na, may increase the risk of osmotic demyelinization syndrome
29 HOW SHOULD CONCOMITANT HYPOKALEMIA BE TREATED, AND IS IT AN ADDITIONAL DANGER IN THE TREATMENT OF HYPONATREMIA? Many patients with hyponatremia resulting from thiazide diuretics therapy appear euvolemic and SIAD has been implicated in the pathogensis. Potassium depletion could increase the sensitivity for ADH release, however this mechanism has not been demonstrated yet.
30
31
32 INCREASED PREVALENCE OF MILD HYPONATREMIA SEEN AMONG PATIENTS WITH TYPE-2 DIABETES MELLITUS AS COMPARED WITH THOSE WITHOUT DIABETES (AL QAHTANI M ET AL 2013)

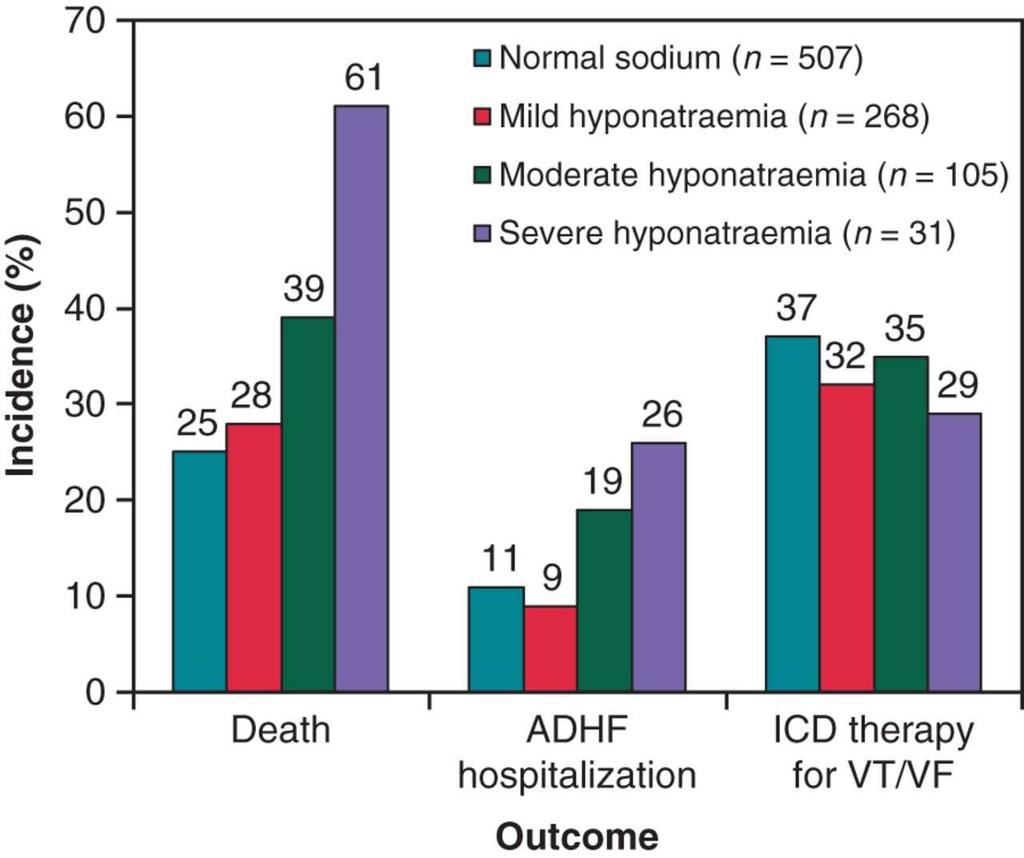
33 MEAN AGE OF THE PATIENTS WITH NORMAL SODIUM AND MILD, MODERATE AND SEVERE HYPONATREMIA, SHOWING THE SIGNIFICANT INVERSE ASSOCIATION BETWEEN SERUM SODIUM AND AGE (AL QAHTANI M ET AL 2013)
34 HUANG CC ET AL. CLINICAL AND GENETIC FACTORS ASSOCIATED WITH THIAZIDE-INDUCEDHYPONATREMIA. MEDICINE (BALTIMORE) 2015;94:E1422 Possible predictors of thiazide-induced induced hyponatremia. A total of 48 patients admitted to the ward or to the emergency department due to severe thiazide-induced induced hyponatremia (Na < 125 mmol/l) were evaluated Twelve tag single nucleotide polymorphism markers were selected from the Potassium Channel, Multivariate logistic regression revealed that age (odds ratio [OR], 1.13; 95% confidence interval [CI], , 1.19, P < 0.001), female gender (OR, 4.49; 95% CI, , 13.11, P = 0.006), BMI (OR, 0.80; 95% CI, , 0.93, P = 0.003), and KCNJ1 rs C/T or T/T polymorphisms (OR, 5.75; 95% CI, , 26.45, P = 0.03) were independent predictors for thiazide-induced induced
35 MAKAM AN, BOSCARDIN WJ, MIAO Y, STEINMAN MA. RISK OF THIAZIDE-INDUCED METABOLIC ADVERSE EVENTS IN OLDER ADULTS. J AM GERIATR SOC 2014;62: Over 9 months of follow-up, 14.3% of new thiazide users developed an adverse event AE (number needed to harm (NNH) 12)) 1.8% of new users developed a severe AE (NNH = 82) 3.8% of new users had an emergency department visit or hospitalization with an AE (NNH = 56) having five or more comorbidities was associated with 3.0 times the odds of developing an AE as having one comorbidity
36 AUTHORS EXPLORED THE IMPACT OF HYPONATRAEMIA ON OUTCOMES: 30 DAYS IN- HOSPITAL MORTALITY, LENGTH OF STAY AND COSTS (CONWAY R J CLIN MED 2014;3: )
37 HYPONATREMIA ICD9-CM CM CODE 276.1
38
39
40
41
42
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Hyponatræmia: analysis
 ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
ESPEN Congress Nice 2010 Hyper- and hyponatraemia - serious and iatrogenic problems Hyponatræmia: analysis Mathias Plauth Hyponatremia Case Analysis Mathias Plauth Klinik für Innere Medizin Städtisches
Functions of Proximal Convoluted Tubules
 1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
** TMP mean page 340 in 12 th edition. Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2:
 QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
Iposodiemia: diagnosi e trattamento
 Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Iposodiemia: diagnosi e trattamento Enrico Fiaccadori Unita di Fisiopatologia dell Insufficienza Renale Acuta e Cronica Dipartimento di Medicina Clinica e Sperimentale Universita degli Studi di Parma Hyponatremia
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Faculty version with model answers
 Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Guidelines for management of. Hyponatremia
 Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Guidelines for management of Hyponatremia Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the authors reviewing available
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Renal Pharmacology. Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics BIMM118
 Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics Renal Pharmacology Kidneys: Represent 0.5% of total body weight, but receive ~25% of the total arterial blood
Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics Renal Pharmacology Kidneys: Represent 0.5% of total body weight, but receive ~25% of the total arterial blood
For more information about how to cite these materials visit
 Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Michael Heung, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Questions? Homework due in lab 6. PreLab #6 HW 15 & 16 (follow directions, 6 points!)
") Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI
 Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI This activity may be done in conjunction with a more traditional urinalysis lab.
Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI This activity may be done in conjunction with a more traditional urinalysis lab.
Mannitol-induced Metabolic Alkalosis
 Electrolyte & Blood Pressure :, 00 ) Mannitolinduced Metabolic Alkalosis Kyung Pyo Kang, M.D., Sik Lee, M.D., Kyung Hoon Lee, M.D., and Sung Kyew Kang, M.D. Department of Internal Medicine, Research Institute
Electrolyte & Blood Pressure :, 00 ) Mannitolinduced Metabolic Alkalosis Kyung Pyo Kang, M.D., Sik Lee, M.D., Kyung Hoon Lee, M.D., and Sung Kyew Kang, M.D. Department of Internal Medicine, Research Institute
Na + Transport 1 and 2 Linda Costanzo, Ph.D.
 Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
Kidney Physiology. Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed
 Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Renal Physiology II Tubular functions
 Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Human Urogenital System 26-1
 Human Urogenital System 26-1 Urogenital System Functions Filtering of blood, Removal of wastes and metabolites Regulation of blood volume and composition concentration of blood solutes ph of extracellular
Human Urogenital System 26-1 Urogenital System Functions Filtering of blood, Removal of wastes and metabolites Regulation of blood volume and composition concentration of blood solutes ph of extracellular
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1
 Lecture 18: Endocrine control of renal function. p. 1") BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
Answers and Explanations
 Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
mid ihsan (Physiology ) GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B **
 GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B **") (Physiology ) mid ihsan GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B ** Colloid pressure in the efferent arteriole is: A- More than that leaving
(Physiology ) mid ihsan GFR is increased when A -Renal blood flow is increased B -Sym. Ganglion activity is reduced C-A and B ** Colloid pressure in the efferent arteriole is: A- More than that leaving
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Kidney and urine formation
 Kidney and urine formation Renal structure & function Urine formation Urinary y concentration and dilution Regulation of urine formation 1 Kidney and urine formation 1.Renal structure & function 1)General
Kidney and urine formation Renal structure & function Urine formation Urinary y concentration and dilution Regulation of urine formation 1 Kidney and urine formation 1.Renal structure & function 1)General
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
MS1 Physiology Review of Na+, K+, H + /HCO 3. /Acid-base, Ca+² and PO 4 physiology
 MS1 Physiology Review of,, / /Acidbase, Ca+² and PO 4 physiology I. David Weiner, M.D. Professor of Medicine and Physiology University of Florida College of Medicine Basic principles Proximal tubule Majority
MS1 Physiology Review of,, / /Acidbase, Ca+² and PO 4 physiology I. David Weiner, M.D. Professor of Medicine and Physiology University of Florida College of Medicine Basic principles Proximal tubule Majority
Na concentration in the extracellular compartment is 140
 هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
Hyponatremia Clinical Significance. Ágnes Haris MD PhD, St. Margit Hospital, Budapest
 Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Hyponatremia Clinical Significance Ágnes Haris MD PhD, St. Margit Hospital, Budapest 1 Case of hyponatremia 70 years old male Past medical history: DM, HTN Heavy smoker (20 packs/day) Recently: epigastrial
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Osmotic Regulation and the Urinary System. Chapter 50
 Osmotic Regulation and the Urinary System Chapter 50 Challenge Questions Indicate the areas of the nephron that the following hormones target, and describe when and how the hormones elicit their actions.
Osmotic Regulation and the Urinary System Chapter 50 Challenge Questions Indicate the areas of the nephron that the following hormones target, and describe when and how the hormones elicit their actions.
BCH 450 Biochemistry of Specialized Tissues
 BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Renal-Related Questions
 Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**
![بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**](/thumbs/87/96174275.jpg "بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.**") بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.** INULIN characteristics : 1 filtered 100 %. 2-Not secreted. 3-Not reabsorbed
بسم هللا الرحمن الرحيم ** Note: the curve discussed in this page [TF]/[P] curve is found in the slides, so please refer to them.** INULIN characteristics : 1 filtered 100 %. 2-Not secreted. 3-Not reabsorbed
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
IX: Electrolytes. Sodium disorders. Specific Learning Objectives: Dan Henry, MD Clerkship Director University of Connecticut School of Medicine
 IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
IX: Electrolytes. Sodium disorders Dan Henry, MD Clerkship Director University of Connecticut School of Medicine Specific Learning Objectives: Knowledge Subinterns should be able to describe: a) The differentinal
Hyponatremia. Mis-named talk? Basic Pathophysiology
 Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
Hyponatremia Great Lakes Hospital Medicine Symposium by Brian Wolfe, MD Assistant Professor of Internal Medicine University of Colorado Denver Mis-named talk? Why do we care about Hyponatremia? concentration
1. remove: waste products: urea, creatinine, and uric acid foreign chemicals: drugs, water soluble vitamins, and food additives, etc.
 Making Water! OR is it really Just Water Just Ask the Nephron!! Author: Patricia L. Ostlund ostlundp@faytechcc.edu (910) 678-9892 Fayetteville Technical Community College Fayetteville, NC 28303 Its just
Making Water! OR is it really Just Water Just Ask the Nephron!! Author: Patricia L. Ostlund ostlundp@faytechcc.edu (910) 678-9892 Fayetteville Technical Community College Fayetteville, NC 28303 Its just
Renal Physiology - Lectures
 Renal Physiology - Lectures Physiology of Body Fluids PROBLEM SET, RESEARCH ARTICLE Structure & Function of the Kidneys Renal Clearance & Glomerular Filtration PROBLEM SET Regulation of Renal Blood Flow
Renal Physiology - Lectures Physiology of Body Fluids PROBLEM SET, RESEARCH ARTICLE Structure & Function of the Kidneys Renal Clearance & Glomerular Filtration PROBLEM SET Regulation of Renal Blood Flow
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Hyponatremia in Heart Failure: why it is important and what should we do about it?
 Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
Objectives Hyponatremia in Heart Failure: why it is important and what should we do about it? Pathophysiology of sodium and water retention in heart failure Hyponatremia in heart failure (mechanism and
12/7/10. Excretory System. The basic function of the excretory system is to regulate the volume and composition of body fluids by:
 Excretory System The basic function of the excretory system is to regulate the volume and composition of body fluids by: o o removing wastes returning needed substances to the body for reuse Body systems
Excretory System The basic function of the excretory system is to regulate the volume and composition of body fluids by: o o removing wastes returning needed substances to the body for reuse Body systems
Chapter 15 Diuretic Agents
 Chapter 15 Diuretic Agents Diuretics Diuretics are agents that increase the rate of urine formation and salt excretion. Diuresis = increased water formation, but the term is also used to indicate increased
Chapter 15 Diuretic Agents Diuretics Diuretics are agents that increase the rate of urine formation and salt excretion. Diuresis = increased water formation, but the term is also used to indicate increased
Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi
 Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi At the end of this lecture student should be able to describe: The loop of Henle is referred to as countercurrent
Done By: Lulu Al-Obaid - Abdulrahman Al-Rashed Reviewed By: Mohammed Jameel Khulood Al-Raddadi At the end of this lecture student should be able to describe: The loop of Henle is referred to as countercurrent
DIURETICS CARBONIC ANHYDRASE INHIBITORS THIAZIDE THIAZIDE-LIKE OSMOTIC DIURETICS LOOP DIURETICS POTASSIUM SPARING DIURETICS
 DIURETICS A diuretic is any substance that promotes diuresis, that is, the increased production of urine. This includes forced diuresis. There are several categories of diuretics. All diuretics increase
DIURETICS A diuretic is any substance that promotes diuresis, that is, the increased production of urine. This includes forced diuresis. There are several categories of diuretics. All diuretics increase
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Osmoregulation and Excretion
 Animal Life and Excretion Harder for multicellular organisms Internal circulation Coordination, information transfer Structural maintenance Movement Maintenance of homeostatic internal environment 15 July
Animal Life and Excretion Harder for multicellular organisms Internal circulation Coordination, information transfer Structural maintenance Movement Maintenance of homeostatic internal environment 15 July
11/05/1431. Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate
 Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
DIURETICS-3 Dr. Shariq Syed
 DIURETICS-3 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Diuretics primarily prevent the reabsorption of K Na Cl I Don t know, Too busy with periodic exams! AIKTC - Knowledge
DIURETICS-3 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Diuretics primarily prevent the reabsorption of K Na Cl I Don t know, Too busy with periodic exams! AIKTC - Knowledge
Basic approach to: Hyponatremia Adley Wong, MHS PA-C
 2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
2016 Topics in Acute and Ambulatory Care CAPA Conference 2018 for Advanced Practice Providers Basic approach to: Hyponatremia Adley Wong, MHS PA-C Goals Physiology of hyponatremia Why we care about hyponatremia
Urinary System. Dr. ZHANG Xiong. Dept. of Physiology. ZJU School of Medicine. QUESTION 6
 Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine http://10.71.121.158 Copyright@ Xiong Zhang QUESTION 6 How is the filtrate reabsorbed in tubular system? Copyright@ Xiong Zhang
Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine http://10.71.121.158 Copyright@ Xiong Zhang QUESTION 6 How is the filtrate reabsorbed in tubular system? Copyright@ Xiong Zhang
Excretory System 1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- X- Y- Z- b) Which of the following is not a function of the organ shown? A. to produce
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- X- Y- Z- b) Which of the following is not a function of the organ shown? A. to produce
Physio 12 -Summer 02 - Renal Physiology - Page 1
 Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Metabolism of water and electrolytes. 2. Special pathophysiology disturbances of intravascular volume and
 Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
Metabolism of water and electrolytes 1. Physiology and general pathophysiology Compartments of body fluids Regulation of volume and tonicity (osmolality) Combinations of volume and osmolality disorders
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
P215 Spring 2018: Renal Physiology Chapter 18: pp , Chapter 19: pp ,
 P215 Spring 2018: Renal Physiology Chapter 18: pp. 504-520, 525-527 Chapter 19: pp. 532-548, 553-560 I. Main Components of the Renal System 1. kidneys 2. ureters 3. urinary bladder 4. urethra 4 Major Functions
P215 Spring 2018: Renal Physiology Chapter 18: pp. 504-520, 525-527 Chapter 19: pp. 532-548, 553-560 I. Main Components of the Renal System 1. kidneys 2. ureters 3. urinary bladder 4. urethra 4 Major Functions
Homeostatic Regulation
 Homeostatic Regulation A hormone is :a Water-soluble hormones: Composed of amino acids and bind a receptor protein on the of the target cell. This starts a signal cascade inside the cell and the signal
Homeostatic Regulation A hormone is :a Water-soluble hormones: Composed of amino acids and bind a receptor protein on the of the target cell. This starts a signal cascade inside the cell and the signal
Furosemide: Properties, Alternatives, and the Medication Approval Process. Heather Brown EMS 209-Advanced Pharmacology Don Knox
 Furosemide: Properties, Alternatives, and the Medication Approval Process Heather Brown EMS 209-Advanced Pharmacology Don Knox Pre-hospital treatment of critical patients is a key factor in determining
Furosemide: Properties, Alternatives, and the Medication Approval Process Heather Brown EMS 209-Advanced Pharmacology Don Knox Pre-hospital treatment of critical patients is a key factor in determining
Human Physiology - Problem Drill 17: The Kidneys and Nephronal Physiology
 Human Physiology - Problem Drill 17: The Kidneys and Nephronal Physiology Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully, (2) Work the problems on paper
Human Physiology - Problem Drill 17: The Kidneys and Nephronal Physiology Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully, (2) Work the problems on paper
Diuretic Agents Part-1. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-1 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Kidneys eliminates waste products and regulates the volume, electrolyte and ph of
Diuretic Agents Part-1 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Kidneys eliminates waste products and regulates the volume, electrolyte and ph of
Volemic status estimation in clinical practice
 Volemic status estimation in clinical practice Marion VALLET, Pierre-Yves CHARLES, Acil JAAFAR, Françoise PRADDAUDE, Ivan TACK Service des Explorations Fonctionnelles Physiologiques ; Hôpital de Rangueil,
Volemic status estimation in clinical practice Marion VALLET, Pierre-Yves CHARLES, Acil JAAFAR, Françoise PRADDAUDE, Ivan TACK Service des Explorations Fonctionnelles Physiologiques ; Hôpital de Rangueil,
BLOCK REVIEW Renal Physiology. May 9, 2011 Koeppen & Stanton. EXAM May 12, Tubular Epithelium
 BLOCK REVIEW Renal Physiology Lisa M. HarrisonBernard, Ph.D. May 9, 2011 Koeppen & Stanton EXAM May 12, 2011 Tubular Epithelium Reabsorption Secretion 1 1. 20, 40, 60 rule for body fluid volumes 2. ECF
BLOCK REVIEW Renal Physiology Lisa M. HarrisonBernard, Ph.D. May 9, 2011 Koeppen & Stanton EXAM May 12, 2011 Tubular Epithelium Reabsorption Secretion 1 1. 20, 40, 60 rule for body fluid volumes 2. ECF
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
DIURETICS-2. Dr. Shariq Syed. Shariq AIKC/TYB/2014
 DIURETICS-2 Dr. Syed Structure of Kidney Blood filtered by functional unit: Nephron Except for cells, proteins, other large molecules, rest gets filtered Structure of Kidney 3 major regions of nephron
DIURETICS-2 Dr. Syed Structure of Kidney Blood filtered by functional unit: Nephron Except for cells, proteins, other large molecules, rest gets filtered Structure of Kidney 3 major regions of nephron
LESSON ASSIGNMENT. Diuretic and Antidiuretic Agents. After you finish this lesson you should be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 8 Therapeutics III. Diuretic and Antidiuretic Agents. LESSON ASSIGNMENT Paragraphs 8-1--8-7. LESSON OBJECTIVES After you finish this lesson you should be able
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 8 Therapeutics III. Diuretic and Antidiuretic Agents. LESSON ASSIGNMENT Paragraphs 8-1--8-7. LESSON OBJECTIVES After you finish this lesson you should be able
Functional morphology of kidneys Clearance
 Functional morphology of kidneys Clearance Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important
Functional morphology of kidneys Clearance Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Counter-Current System Regulation of Renal Functions
 Counter-Current System Regulation of Renal Functions Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most
Counter-Current System Regulation of Renal Functions Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most
Dept. of Physiology. ZJU School of Medicine.
 Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine Http://10.10.10.151/Able.Acc2.Web/Template/View.aspx?action =view&coursetype=0&courseid=26519 QUESTION 6 How is the filtrate reabsorbed
Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine Http://10.10.10.151/Able.Acc2.Web/Template/View.aspx?action =view&coursetype=0&courseid=26519 QUESTION 6 How is the filtrate reabsorbed
KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin
![KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin](/thumbs/87/96174332.jpg "KD02 [Mar96] [Feb12] Which has the greatest renal clearance? A. PAH B. Glucose C. Urea D. Water E. Inulin") Renal Physiology MCQ KD01 [Mar96] [Apr01] Renal blood flow is dependent on: A. Juxtaglomerular apparatus B. [Na+] at macula densa C. Afferent vasodilatation D. Arterial pressure (poorly worded/recalled
Renal Physiology MCQ KD01 [Mar96] [Apr01] Renal blood flow is dependent on: A. Juxtaglomerular apparatus B. [Na+] at macula densa C. Afferent vasodilatation D. Arterial pressure (poorly worded/recalled
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Renal Functions: Renal Functions: Renal Function: Produce Urine
 Renal Functions: Excrete metabolic waste products Reabsorb vital nutrients Regulate osmolarity: Maintain ion balance Regulate extracellular fluid volume (and thus blood pressure) Renal Functions: Regulate
Renal Functions: Excrete metabolic waste products Reabsorb vital nutrients Regulate osmolarity: Maintain ion balance Regulate extracellular fluid volume (and thus blood pressure) Renal Functions: Regulate
EXCRETION QUESTIONS. Use the following information to answer the next two questions.
 EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
Faculty version with model answers
 Faculty version with model answers Fluid & Electrolytes Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. A 40 year old, obese man is seen by his physician, and found to be hypertensive.
Faculty version with model answers Fluid & Electrolytes Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. A 40 year old, obese man is seen by his physician, and found to be hypertensive.
Normal Renal Function
 Normal Renal Function Functions of the Kidney: balances solute and water transport excretes metabolic waste products conserves nutrient regulates acid-base balance secretes hormones that help regulate
Normal Renal Function Functions of the Kidney: balances solute and water transport excretes metabolic waste products conserves nutrient regulates acid-base balance secretes hormones that help regulate
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
DOWNLOAD OR READ : SYNDROME OF INAPPROPRIATE SECRETION OF ANTIDIURETIC HORMONE IN MALIGNANCY PDF EBOOK EPUB MOBI Page 1 Page 2 syndrome of inappropriate secretion of antidiuretic hormone in malignancy
Renal System and Excretion
 Renal System and Excretion Biology 105 Lecture 19 Chapter 16 Outline Renal System I. Functions II. Organs of the renal system III. Kidneys 1. Structure 2. Function IV. Nephron 1. Structure 2. Function
Renal System and Excretion Biology 105 Lecture 19 Chapter 16 Outline Renal System I. Functions II. Organs of the renal system III. Kidneys 1. Structure 2. Function IV. Nephron 1. Structure 2. Function
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (4) Dr. Attila Nagy 2018
 Dr. Attila Nagy 2018") RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (4) Dr. Attila Nagy 2018 Intercalated cells Intercalated cells secrete either H + (Typ A) or HCO 3- (Typ B). In intercalated cells Typ A can be observed
RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (4) Dr. Attila Nagy 2018 Intercalated cells Intercalated cells secrete either H + (Typ A) or HCO 3- (Typ B). In intercalated cells Typ A can be observed
1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
BIOL2030 Human A & P II -- Exam 6
 BIOL2030 Human A & P II -- Exam 6 Name: 1. The kidney functions in A. preventing blood loss. C. synthesis of vitamin E. E. making ADH. B. white blood cell production. D. excretion of metabolic wastes.
BIOL2030 Human A & P II -- Exam 6 Name: 1. The kidney functions in A. preventing blood loss. C. synthesis of vitamin E. E. making ADH. B. white blood cell production. D. excretion of metabolic wastes.
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Chapter 44. Regulating the Internal Environment. AP Biology
 Chapter 44. Regulating the Internal Environment Homeostasis Living in the world organisms had a choice: regulate their internal environment maintain relatively constant internal conditions conform to the
Chapter 44. Regulating the Internal Environment Homeostasis Living in the world organisms had a choice: regulate their internal environment maintain relatively constant internal conditions conform to the
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1
 Problem Set #8 Solutions p. 1") BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
Diuretic Use in Neonates
 Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Renal System Dr. Naim Kittana Department of Biomedical Sciences Faculty of Medicine & Health Sciences An-Najah National University
 Renal System Dr. Naim Kittana Department of Biomedical Sciences Faculty of Medicine & Health Sciences An-Najah National University Declaration The content and the figures of this seminar were directly
Renal System Dr. Naim Kittana Department of Biomedical Sciences Faculty of Medicine & Health Sciences An-Najah National University Declaration The content and the figures of this seminar were directly
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
Other Factors Affecting GFR. Chapter 25. After Filtration. Reabsorption and Secretion. 5 Functions of the PCT
 Other Factors Affecting GFR Chapter 25 Part 2. Renal Physiology Nitric oxide vasodilator produced by the vascular endothelium Adenosine vasoconstrictor of renal vasculature Endothelin a powerful vasoconstrictor
Other Factors Affecting GFR Chapter 25 Part 2. Renal Physiology Nitric oxide vasodilator produced by the vascular endothelium Adenosine vasoconstrictor of renal vasculature Endothelin a powerful vasoconstrictor