Management of Extrahepatic Manifestations of Hepatitis C Virus in the Era of DAA
|
|
|
- Homer O’Connor’
- 5 years ago
- Views:
Transcription
1 Management of Extrahepatic Manifestations of Hepatitis C Virus in the Era of DAA Pr Patrice CACOUB, MD Dept of Internal Medicine and Clinical Immunology CNRS UMR 7087, INSERM UMR S-959, DHU I2B Université Pierre et Marie Curie Hôpital La Pitié-Salpêtrière, Paris, FRANCE patrice.cacoub@aphp.fr
2 Disclosures Dr P. Cacoub has received consulting and lecturing fees from: Abbvie, Astra Zeneca, Bristol-Myers Squibb, Gilead, Glaxo Smith Kline, Janssen, Merck Sharp Dohme, Roche, Servier and Vifor Dr P. Cacoub is an inventor of a patent application owned by his academic institution and licensed to ILTOO pharma, a biotechnology company developing low dose IL-2 in autoimmune diseases, in which he holds shares. Dr P. Cacoub has received grants from: CNRS, INSERM, Université Pierre et Marie Curie and ANRS
3 Chronic active HCV infection almost doubles the risk of mortality from non-liver related diseases Cumulative extra hepatic mortality (%) Non-liver related disease in patients with and without active HCV infection (n=2,199) 19.8% 12.2% 11.0% HCV+, RNA+ HCV- HCV+, RNA Follow-up (Years) P<0.001 for comparison among all 3 groups and P=0.002 for HCV RNA detectable vs. undetectable HCV, hepatitis C virus; RNA, ribonucleic acid Lee MH, et al. J Infect Dis 2012;206:469 77


4 Chronic HCV infection is more than a liver disease Depression, cognitive impairment Fatigue Stroke Sicca syndrome Lymphoma Renal complications Neuropathy Thyroid disease Myocardial perfusion defects Insulin resistance, type 2 diabetes Mixed cryoglobulinaemia vasculitis Dermatological manifestations Arthralgia HCV, hepatitis C virus. Cacoub P, et al. J Hepatol. 2016;65(1 Suppl):S82-94
5 Extra-hepatic manifestations of HCV Presentation outline 1. Autoimmune manifestations and malignant blood diseases 2. HCV infection: a new cardiovascular risk factor 3. Insulin resistance and type 2 diabetes mellitus 4. Fatigue, depression and cognitive impairment
6 Autoimmune and malignant blood diseases
7 Main (Auto)-Immune Conditions Associated with HCV Auto-Immune Condition l Vasculitis 5 15 % l Arthralgia-myalgia % l Sicca syndrome % l Auto-antibodies % l Lymphoma RR=35 Cacoub P et al, Dig Liver Dis. 2014;46 Suppl 5:S165-73

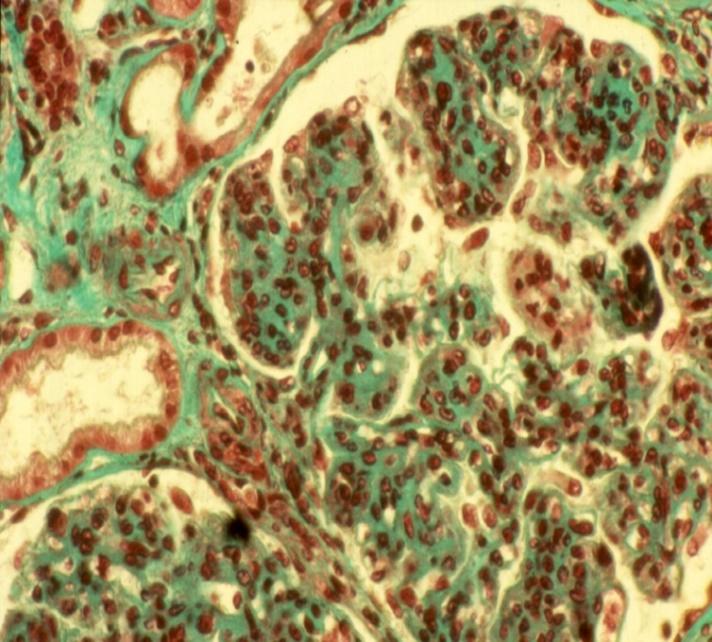
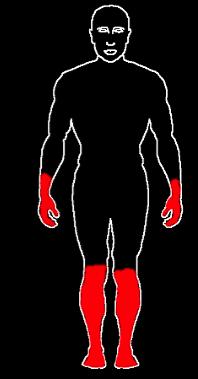
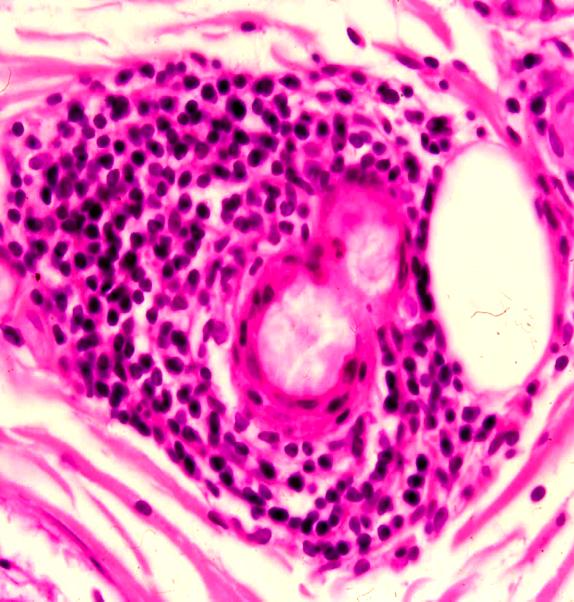
8 Cryoglobulinemia vasculitis Skin Purpura Glomerulonephritis Neuropathy CNS vasculitis
, 1,777 HCV infected patients tested for the presence of mixed cryoglobulinemia Kondili et al, EASL")
9 About 15% of HCV-infected patients will develop a symptomatic mixed cryoglobulinemia l Italian cohort (80 centers), 1,777 HCV infected patients tested for the presence of mixed cryoglobulinemia Kondili et al, EASL 2016
10 HCV causes production of abnormal antibodies which are able to induce a systemic auto-immune disease Rocatello D, Nephrol Dial Transplant, 2004;19(12):
11 New anti-virals with increased potency improve HCVrelated cryoglobulinemia vasculitis Clinical remission in HCV-related cryoglobulinemia vasculitis correlates with virological response IFN-based regimen; 6 months IFN-free regimen; 24 weeks 47 %* 88%* Saadoun et al, n=32 Saadoun et al, n = 24 Non-complete clinical response Complete clinical response *End of treatment (EoT); 24 weeks post-treatment; IFN: interferon; PEG IFN: pegylated-interferon; PI: protease inhibitor; RBV: ribavirin; SOF: sofosbuvir 1. Saadoun D, et al. Arthritis Rheum 2006;54: ; 2. Saadoun D, et al. J Hepatol 2015;62:24 30; 3. Saadoun D, et al. Ann Rheum Dis 2015; doi: /annrheumdis

12 HCV-CryoVas : Virological Response after IFN-free DAA SVR (%) 100% 83% 100% 94% 100% 80% 74% 60% 40% 20% 0% 17/23 SOF + RBV 1 24 wk 10/12 SOF + SMV ± RBV wk 44/44 SOF + LDV 3 12 wk 33/35 SOF-based/3D wk 41/41 SOF + DCV, wk 1.Saadoun, Ann Rheum 2015; 2. Sise, Hepatology 2016 ;3. Gragnani, Hepatology 2016; 4. Bonacci, Clin Gastro Hepatol 2016 ; 5. Saadoun, Gastroenterology 2017
13 HCV-CryoVas : Clinical Impact of DAAs Clinical response 12 weeks post-daa Saadoun, 2015 (n=24) Sise, 2016 (n=12) Gragnani, 2016 (n=44) Bonacci, 2017 (n=35) Saadoun, 2017 (n=41) Complete response Partia response Null response Saadoun et al. Ann Rheum Dis Oct;75(10): ; Sise et al. Hepatology 2016 Feb;63(2):408-17; Gragnani et al. Hepatology Nov;64(5): ; Bonacci and Lens et al. Clin Gastroenterol Hepatol Apr;15(4): Saadoun et al. Gastroenterology. 2017
 Severe")

:24-30 ; Ramos-Casals, et al. Med Clin (Barc).")
14 HCV-Cryoglobulinemia: Therapeutic approach Antiviral therapy with IFN-free DAAs Mild to moderate disease ( purpura, arthralgia, neuropathy) Severe disease ( progressive renal failure, slkin ulcer, mononeuritis mutlplex) Life threatening (rapid progressive nephritis, CNS, digestive and pulmonary involvement) Cacoub P. Ann Rheum Dis 2014 Jan;73(1):24-30 ; Ramos-Casals, et al. Med Clin (Barc). 2015;144(9): Rituximab Rituximab, plasma exchange and/or cyclophosphamide
15 Major Advances in Antiviral Strategies in HCV-Cryoglobulinemia Vasculitis Complete clinical response At Week 12 At end of therapy (W24) Virological response At week 12 After end of therapy (W36) PegIFN-RBV-PI 1 SOF-RBV 2 SOF-DACLA N=30 N=24 N= % 66.7% 73.9% 66.6% 71% 87.5% 92% 74% 90.2% 90.2% 100% 100% Clearance of cryoglobulin (W24) 22.2% 41.6% 50% Serious adverse event 46.6% 8% 0% Steroids and/or Rituximab 43% 16% 4.8% PegIFN, pegylated interferon; RBV, ribavirin; PI, first generation protease inhibitor; SOF, sofosbuvir; DACLA, daclatasvir 1. Saadoun D, et al. Arthritis Rheum 2006; 2. Saadoun D, et al. Ann Rheum Dis 2015
16 DAAs Revert Immune Abnormalities in HCV-CryoVas 3 * Sofosbuvir plus Daclatasvir revert Treg deficiency (A) and 1 expansion of IgM + CD21 -/low memory B cells (B), T folliculer helper 0 cells (C) and Th17 cells (D) in HCV-CryoVas A CD4 + CD25 hi Foxp3 + (%) 2 HCV-CV before DAA HCV-CV end DAA A B C CD4 + CD25 hi Foxp3 + (%) * HCV-CV before DAA HCV-CV end DAA CD27 + IgM + CD21 -/low (%) * HCV-CV before DAA HCV-CV end DAA CD4 + CXCR5 + IL21 + (%) * HCV-CV before DAA HCV-CV end DAA D CD4 + IL17 + (%) * HCV-CV before DAA HCV-CV end DAA D E 5 * 40 D4 + IL17 + (%) CD4 + IFN γ + (%) Comarmond C et al, Gastroenterology 2017
17 HCV-CryoVas: Immunological Impact of DAAs Study Cryocrit at baseline Cryocrit 12 wks post-daa Cryo negative (%) Saadoun (2016) 0.35 ( ) g/l 0 (0 0.37) g/l 46 % Sise (2016) 1.5% (0.5-4%) 0.5% (0-2%) 44 % Gragnani (2016) 7.2 ± 15% 1.8 ± 5% 39 % Bonacci/Lens (2017) 3.2% ( %) 0.5% (0-1.4)% 43 % Saadoun (2017) 0.56 ± 0.18 g/l 0.21 ± 0.14 g/l 50 % Saadoun et al. Ann Rheum Dis Oct;75(10): ; Sise et al. Hepatology 2016 Feb;63(2):408-17; Gragnani et al. Hepatology Nov;64(5): ; Bonacci and Lens et al. Clin Gastroenterol Hepatol Apr;15(4): Saadoun et al. Gastroenterology. 2017
18 From HCV-Cryoglobulinemia to B-Cell Lymphoma Antigen-Sensitive B Cell Proliferation Antigen-Insensitive B Cell Proliferation HCV (E2) CD81 Cytokines BAFF B cell Treg deficit Hyperγglobulinemia IgH-bcl2? Cryoglobulinemia Vasculitis B-cell lymphoma Other oncogenic events? HCV infection increases the risk of developing a B-cell lymphoma (RR=34) B-cell lymphoma Polyclonal proliferation Oligo/Monoclonal proliferation Uncontrolled proliferation IgG Anti-E2 IgM/Rheumatoid factor
19 Sustained Response to IFN-based Antivirals is Associated with Improvements in HCV-related B-Cell Lymphoma 1.0 l 116 patients with B-cell lymphoma (DLBCL, 39%; MZL, 39%; other, 22%) l HCV therapy given to 70 patients l SVR in 43/70 (61%) patients è SVR correlated with haematological response in MZL (P<0.001) Overall survival probability Progression-free survival probability No antiviral treatment P=0.029 Antiviral treatment Months No antiviral treatment P=0.049 Antiviral treatment Months DLBCL: diffuse large B-cell lymphoma; MZL: marginal zone lymphoma; Sustained Virological Response Michot JM, et al. Am J Hematol 2015;90:

 Clinical response (CR + PR) 67%")
20 Direct Antiviral Agents in HCV-lymphoproliferative disorders SVR in 45/46 (97.8%) Clinical response (CR + PR) 67% Arcaini L et al, Blood 2016
21 Chronic HCV infection: a new cardiovascular risk factor? Stroke Heart Kidney
22 People with HCV have an increased risk of cardiovascular disease compared to people without HCV In a meta-analysis HCV was associated with: increased risk of death from cardiovascular disease Odds ratio vs control group, 1.65, [1.07, 2.56] increased risk of stroke Odds ratio vs control group, 1.30 [1.10, 1.55] increased risk of a carotid artery plaque, a well-known risk factor of stroke Odds ratio vs control group, 2.27 [1.76, 2.94] Petta S et al, Gastroenrology 2015;150(1): e4;
23 Antiviral therapy is associated with a reduced risk of stroke in people with HCV 100 IBT Stroke-free survival rate 0.95 l IFN-based therapy was associated with a 61% IBT decreased risk of stroke in HCV 0.90 patients, Log-rank after adjusting for known prognostic factors. test, p = Non Time (years) IBT, interferon based therapy Hsu CS, et al. APT 2013;38:415 23
24 Most studies showed a significant association between ischemic heart disease and HCV infection References, year Study type Country HCV+ (n) HCV- (n) Studies showing an association Vassalle et al, 2004 Cross-over Italy Völzke et al., 2004 Transversal Germany Butt et al., 2009 Cross-over USA Tsui et al., 2009 Cohort USA 84 - Ramdeen et al., 2010 Cohort USA 78 - Studies NOT showing an association Butt et al., 2007 Cohort USA 126, ,926 Domont F & Cacoub P, Liver Int 2016

25 Improvement in myocardial perfusion defects is seen in patients with sustained virological response to antiviral therapy Myocardial SPECT images of 127 HCV infected patients without known cardiac disease at baseline treated with antiviral therapy Before therapy Before therapy Before therapy End of therapy End of therapy End of therapy 6 months after therapy 6 months after therapy 6 months after therapy Sustained virological response Relapse Non Response Before antiviral therapy (M0; A), at the completion of antiviral therapy (M6; B) and 6 months after the completion of antiviral therapy (M12; C). The arrows show the regions of myocardial perfusion defects. SPECT, Single Photon Emission Computed Tomography Maruyama S, et al. J Hepatol 2012;58:11 5
26 Sustained virological response to antiviral therapy is associated with improvements in myocardial perfusion defect severity score Response following 48 weeks of antiviral treatment P< P= Severity score P< P=0.133 NS NS Months Months Months SVR group (n=30) Relapse group (n=9) NVR group (n=6) Dashed lines indicate normal range NS: not significant; NVR: non-virological response; SVR, Sustained Virological Response Maruyama S, et al. J Hepatol 2013;58:11 5
27 Reduction in cardiovascular events after HCV eradication in patients with cirrhosis 3 yrs 5 yrs 9.1 % 2.3 % 12.3 % 3.5 % Prospective Cohort, ANRS CO12 CirVir ; 1,323 patients; F-up 51 months Nahon P et al, Gastroenterology 2015
28 Chronic HCV infection increases the risk of death related to renal disease 0,045 0,040 0,035 0,030 0,025 0,020 0,015 0,010 0,005 0,000 p < Anti-HCV negative (n = 16,629) Undetectable HCV RNA (n = 330) Low HCV RNA (n = 371) High HCV RNA (n = 124) Follow up (years) 4.3 % 2.6 % 0.5 % 0.3 % R.E.V.E.A.L. Study, Taiwan National Health Insurance Research Database n= subjects Lai TS et al., AASLD 2014, Kidney Int 2017
29 The effect of sustained virological response on the risk of HCV extrahepatic manifestations patients, HCV RNA+, , 128 VA med centers Genotype 1 (54.7%), HBV 1.3%, HIV 3.2% yrs (52.1%), male (97.1%), non-hispanic white (44.9%), overweight (BMI 25-30, 38.5%) or obese (BMI 30, 27.3%), smokers (59.2%), alcohol abusers (58.3%), APRI score 2 (24.8%). Follow-up 5.1 years (IQR, years). HCV treatment: N = (19%) received IFN based therapy for 24.2 weeks N = (34%) achieved SVR. N = (19%) no HCV treatment Mahale P et al, GUT 2017
, smoking and alcohol abuse.")
30 The effect of sustained virological response on the risk of HCV extrahepatic manifestations HRs were adjusted for age categories (20 39, 40 49, 50 59, and 70+ years), sex, race, period of service, average annual number of outpatient visits, body mass index (<25.0, 25 to <30, 30+ kg/m2), smoking and alcohol abuse. Additional adjustments for baseline diabetes mellitus and hypertension were conducted in models for glomerulonephritis, coronary heart disease and stroke. Mahale P et al, GUT 2017
31 HCV Increases the Risk of Chronic Kidney Disease while Effective HCV Treatment Decreases Its Incidence l Retrospective US cohort, l 56,448 HCV-infected patients matched with 169,344 non-hcv patients, è N = 3666 (6.6%), interferon-based dual, è N = 3534 (6.3%), interferon-based triple, è N = 4628 (8.3%), all-oral direct acting antiviral agents (DAA) è N = 43,990 (79%), did not receive any HCV treatment. Park H et al, Hepatology, 2017
32 Effective HCV Treatment Decreases the Incidence of Chronic Kidney Disease Minimum effective duration Tx HR: 0.70; 95% Cl, These associations were only significant for dual (HR, 0.60; 95% CI, ) and triple therapies (HR, 0.59; 95% CI, ) but not for the new all-oral therapy (HR, 1.03; 95% CI, ). Park H et al, Hepatology, 2017
33 HCV, insulin resistance and type 2 diabetes mellitus

34 Increased risk of Type 2 diabetes in patients with HCV: multiple mechanisms Jacobson I et al, Clin Gastroienterol Hepatol 2010; 8(12):
35 Changes in insulin sensitivity according to virological response after antiviral therapy for HCV Insulin resistance according to response to antiviral therapy for HCV Solid lines = on therapy; Dashed lines = off therapy. Changes from baseline to weeks 24, 48 and 72 were statistically significant (p<0.01) only among SVR patients. HOMA, Homeostasis model assessment; SVR, Sustained virological response.
36 Incidence of type 2 diabetes in patients with or without response to antiviral therapy for HCV Incidence of T2DM according to response to antiviral therapy for HCV in patients with cirrhosis Incidence of T2DM according to response to antiviral therapy for HCV in patients >50 years T2DM, type 2 diabetes mellitus; SVR, Sustained Virological Response Arase Y, et al. Hepatology 2009; ;49(3):739-44

37 Glycemic Control by Direct-Acting Antivirals in Type 2 Diabetes Mellitus Patients with HCV G4 Dawood, Diabetes Metab J 2017

38 Multivariate analysis for factors affecting glycemic control with direct-acting antivirals Diabetic patients receiving DAAs should be closely monitored for reduction of antidiabetic drugs, especially insulin and sulfonylurea, to avoid hypoglycemic events. T2DM, type 2 diabetes mellitus Dawood, Diabetes Metab J 2017

39 HCV, Cardiovascular and Metabolic Events: Possible Mechanisms IR, insulin-resistance; HCC, hepatocellular carcinoma 1. Negro F. J Hepatol 2014; 61:S69 S78; 2. Negro F, et al. Gastroenterology 2015; 149: ;
40 Fatigue, depression and cognitive impairment HCV & Health Related Quality of Life

41 HCV is associated with fatigue and depression, and infection of brain and nerve cells Fatigue è prevalence ranges from 50 to 67% è independently predicts poor HRQoL Depression è 28% of HCV patients depressed prior to HCV therapy. è predictive of HRQoL during antiviral therapy for HCV HCV may directly affect the central nervous system (CNS): è Infection of microglial cells within the CNS è Alterations in serotonergic and dopaminergic neurotransmission Cacoub P et al, Dig Liver Dis. 2014; 46 Suppl 5:S Negro F, et al. Gastroenterology 2015;149(6): ; Lucaciu LA, Dumitrascu DL. Ann Gastroenterol 2015; 28(4):440-7
42 HCV can interact with cells in the brain and nervous system Flaviviridae family other neurotropic viruses: japanese encephalitis japonaise, yellow fever, tickborne encephalitis, dengue Infection of microglial cells (+++) and astrocytes Not direct infection of neurones Interaction with cerebral endothelial cells Blood brain barrier Perivascular macrophage Passage of free virus and virally infected PBMC IL1β TNFα IFNγ Neuron Astrocyte Neuronal dysfunction Microglial activation Microglia Wilkinson J et al. J Virol (3): ; Negro F et al, Gastroenterology 2015; 149(6):

43 Evidence for an effect of HCV on the brain and nervous system Confirmed by other studies Cho/Cr! mi/cr! NAA/Cr " Correlated to neuropsy tests Forton D et al., Lancet 2001; 358(9275):38-9.

44 Decrease Cerebral Glucose Utilisation in HCV Patients 15 HCV non cirrhotic vs. HCV neg. Fatigue, cognitive decline, mood alteration Methods : HCV+ vs. HCV- HCV RNA+ vs. HCV RNA- Neuropsy. tests, brain PET-FDG, brain PETdopa & 5HT, brain MRI Ø Cerebral glucose utilisation is decreased in HCV+ patients Ø Correlated with dopamine transporter availability and psychometric results Heeren M et al, J Cereb Blood Flow Metabl 2011
 Hsu PC, et al. Liver Int 2009;29:449 58.")
45 Quality of life is affected at all stages of chronic HCV infection (not just in severe disease) QoL significantly poorer in all HCV disease stages compared to general population No significant association between disease stage and degree of impact on QoL P<0.005 for all disease stages vs. general population (all domains) Hsu PC, et al. Liver Int 2009;29:
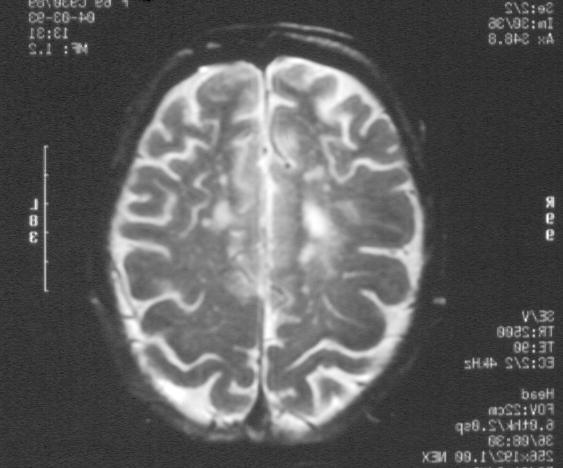
46 Brain magnetic resonance signal in basal ganglia* in HCV patients according to response to antiviral therapy After HCV clearance: improvements in verbal learning and visuo-spatial memory reduced cerebral infection and/or immune activation Baseline (T1), week 12 (T2), and for treatment candidates, 12 weeks after antiviral therapy (T3) * Myoinositol/creatinine T1 vs. T3 in SVR; p<0.05 Byrnes V, et al. J Hepatol 2012;56:549 56
47 Patients reported outcomes at Week 24 after antiviral therapy or placebo SF36 FACIT PLACEBO SOF/VEL CLDQ WPAI Younossi Z et al, J Hepatol 2
48 What is the impact of HCV eradication on extrahepatic manifestations?
49 Extrahepatic benefits of HCV eradication (SVR following antiviral therapy): Summary reduced all-cause mortality complete resolution of mixed cryoglobulin complications regression/remission of HCV-associated lymphoma improvement in myocardial perfusion defects reduced incidence of stroke reduced renal and cardiovascular outcomes in diabetics reduced risk of insulin resistance reduced risk of type 2 diabetes improved cognitive performance reduction in fatigue gains in quality of life Autoimmune and B cell malignancies Cardiovascular diseases Diabetes and insulin resistance Cognitive and functional Negro F et al, Gastroenterology 2015; 149(6):
50 HCV and extrahepatic manifestations Conclusion The disease induced by HCV is a systemic C disease which cannot be seen anymore only as an hepatitis Healthcare consequences of these extrahepatic manifestations must be urgently considered in addition to those usually associated with chronic HCV infection
51 APPENDIX Back-up slides
52 Reductions in the magnitude of protective effect with increasing time to initiation of antiviral treatment for glomerulonephritis, NHL and stroke. Mahale P et al, GUT 2017
Professor Patrice Cacoub
 Five Nations Conference on HIV and Hepatitis in partnership with Professor Patrice Cacoub La Pitié-Salpêtrière Hospital, Paris, France HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
Five Nations Conference on HIV and Hepatitis in partnership with Professor Patrice Cacoub La Pitié-Salpêtrière Hospital, Paris, France HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
Accepted Manuscript. Hepatitis C virus infection, a new modifiable cardiovascular risk factor. Patrice Cacoub
 Accepted Manuscript Hepatitis C virus infection, a new modifiable cardiovascular risk factor Patrice Cacoub PII: S0016-5085(19)30382-8 DOI: https://doi.org/10.1053/j.gastro.2019.02.009 Reference: YGAST
Accepted Manuscript Hepatitis C virus infection, a new modifiable cardiovascular risk factor Patrice Cacoub PII: S0016-5085(19)30382-8 DOI: https://doi.org/10.1053/j.gastro.2019.02.009 Reference: YGAST
IMPACT OF HCV THERAPY ON METABOLISM AND PUBLIC HEALTH
 IMPACT OF HCV THERAPY ON METABOLISM AND PUBLIC HEALTH Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need DISCLOSURES CONFLICTS OF INTEREST
IMPACT OF HCV THERAPY ON METABOLISM AND PUBLIC HEALTH Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need DISCLOSURES CONFLICTS OF INTEREST
HCV Treat now! Robert G Gish MD. Professor Consultant Stanford University
 HCV Treat now! Robert G Gish MD Professor Consultant Stanford University Steering committee and Executive Board NVHR National Viral Hepatitis Roundtable Founding Member CEVHAP Singapore Viral Hepatitis
HCV Treat now! Robert G Gish MD Professor Consultant Stanford University Steering committee and Executive Board NVHR National Viral Hepatitis Roundtable Founding Member CEVHAP Singapore Viral Hepatitis
This is an AbbVie sponsored educational webinar which is being presented
 Presented by Joseph Lim, MD April 5 th, 2017 AbbVie disclosures This is an AbbVie sponsored educational webinar which is being presented by Joseph Lim, MD, on behalf of AbbVie The purpose of the medical
Presented by Joseph Lim, MD April 5 th, 2017 AbbVie disclosures This is an AbbVie sponsored educational webinar which is being presented by Joseph Lim, MD, on behalf of AbbVie The purpose of the medical
Follow-up of patients with SVR Lawrence Serfaty Service d Hépatologie, UMR_S 938 Hôpital Saint-Antoine Université Pierre&Marie Curie Paris, France
 9th Paris Hepatitis Conference, January 11-12, 2016 Follow-up of patients with SVR Lawrence Serfaty Service d Hépatologie, UMR_S 938 Hôpital Saint-Antoine Université Pierre&Marie Curie Paris, France Disclosures
9th Paris Hepatitis Conference, January 11-12, 2016 Follow-up of patients with SVR Lawrence Serfaty Service d Hépatologie, UMR_S 938 Hôpital Saint-Antoine Université Pierre&Marie Curie Paris, France Disclosures
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain
 Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain Disclosures Advisory boards and speaker s bureau for: Gilead, Merck,
Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain Disclosures Advisory boards and speaker s bureau for: Gilead, Merck,
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
All Hands on Deck: Taking on Hepatitis C in Tennessee
 All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE. Anna Linda Zignego
 CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE Anna Linda Zignego Eur J Gastroenterol Hepatol, 2017 MC: in the setting of HCV-related pathologies, a typically female disease Direct
CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE Anna Linda Zignego Eur J Gastroenterol Hepatol, 2017 MC: in the setting of HCV-related pathologies, a typically female disease Direct
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Should Elderly CHC Patients (>70 years old) be Treated?
 be Treated?") Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Universal HCV treatment: Strategies for simplification
 Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Phase 3. Treatment Experienced. Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2. Afdhal N, et al. N Engl J Med. 2014;370:
 Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy?
 Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Efficacy and Safety of Sofosbuvir plus Daclatasvir for Treatment of HCV-associated Cryoglobulinemia Vasculitis.
 Efficacy and Safety of Sofosbuvir plus Daclatasvir for Treatment of HCV-associated Cryoglobulinemia Vasculitis. David Saadoun, Stanislas Pol, Yasmina Ferfar, Laurent Alric, Christophe Hezode, Si Nafa Si
Efficacy and Safety of Sofosbuvir plus Daclatasvir for Treatment of HCV-associated Cryoglobulinemia Vasculitis. David Saadoun, Stanislas Pol, Yasmina Ferfar, Laurent Alric, Christophe Hezode, Si Nafa Si
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
La sindrome metabolica e il suo impatto dopo la guarigione nel paziente HIV/HCV
 WORKSHOP HCV: la guarigione e il parallelismo tra risposta virologica sostenuta e outcome clinico Milano, 25 Ottobre 2018 Ospedale San Raffaele IRCCS - Sede Turro La sindrome metabolica e il suo impatto
WORKSHOP HCV: la guarigione e il parallelismo tra risposta virologica sostenuta e outcome clinico Milano, 25 Ottobre 2018 Ospedale San Raffaele IRCCS - Sede Turro La sindrome metabolica e il suo impatto
Virological Tools and Monitoring in the DAA Era
 Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
HCV: Racial Disparities. Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD
 HCV: Racial Disparities Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Research Grants Boehringer Ingelheim, Inc.
HCV: Racial Disparities Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Research Grants Boehringer Ingelheim, Inc.
Navigating The Prior Authorization Approval Process. Kristin Webb, RPCA University at Buffalo
 Navigating The Prior Authorization Approval Process Kristin Webb, RPCA University at Buffalo Disclosures DISCLOSURES Commercial Entity Relevance Role K. Webb Abbvie Merck, AbbVie, Tobira, Gilead Honorarium
Navigating The Prior Authorization Approval Process Kristin Webb, RPCA University at Buffalo Disclosures DISCLOSURES Commercial Entity Relevance Role K. Webb Abbvie Merck, AbbVie, Tobira, Gilead Honorarium
Navigating The Prior Authorization Approval Process
 Navigating The Prior Authorization Approval Process Kristin Webb, RPCA University at Buffalo Disclosures DISCLOSURES Commercial Entity Relevance Role K. Webb Abbvie Merck, AbbVie, Tobira, Gilead Honorarium
Navigating The Prior Authorization Approval Process Kristin Webb, RPCA University at Buffalo Disclosures DISCLOSURES Commercial Entity Relevance Role K. Webb Abbvie Merck, AbbVie, Tobira, Gilead Honorarium
How to optimize treatment for HCV Genotype 4
 How to optimize treatment for HCV Genotype 4 Paris Hepatitis Conference Pr Tarik Asselah 14 janvier 2014 MD, PhD Service d Hépatologie & INSERM U773 University Paris Diderot Hôpital Beaujon, Clichy tarik.asselah@bjn.aphp.fr
How to optimize treatment for HCV Genotype 4 Paris Hepatitis Conference Pr Tarik Asselah 14 janvier 2014 MD, PhD Service d Hépatologie & INSERM U773 University Paris Diderot Hôpital Beaujon, Clichy tarik.asselah@bjn.aphp.fr
ANTIVIRAL THERAPY FOR HCV. Alfredo Alberti
 CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
HEPATITIS C UPDATES. Sanaa S. Said 10 th April, 2014
 HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
CHRONIC HCV TREATMENT: In Special Populations.
 CHRONIC HCV TREATMENT: In Special Populations. By Taher EL-ZANATY Prof. of Internal Medicine CAIRO UNIVERSITY Introduction: HCV is the major cause of chronic hepatitis in Egypt. Its end stage is liver
CHRONIC HCV TREATMENT: In Special Populations. By Taher EL-ZANATY Prof. of Internal Medicine CAIRO UNIVERSITY Introduction: HCV is the major cause of chronic hepatitis in Egypt. Its end stage is liver
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE
 THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
THE THERAPEUTIC REVOLUTION THAT TRANSFORMED CHRONIC HEPATITIS C TO A CURABLE DISEASE MARIA SCHINA CONSULTANT PHYSICIAN INTERNAL MEDICINE AND HEPATOLOGY ATHENS EUROCLINIC 10 th INTERNATIONAL CONGRESS OF
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Hepatitis B Virus therapy. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Seyed Moayed Alavian Professor of Gastroenterology and Hepatology Editor in-chief of Hepatitis Monthly E mail:
 Sofosbuvir and Ledipasvir Combination with and without Ribavirin in Patients with Hepatitis C Virus Infection; Preliminary Report of an Experience from Iran Seyed Moayed Alavian Professor of Gastroenterology
Sofosbuvir and Ledipasvir Combination with and without Ribavirin in Patients with Hepatitis C Virus Infection; Preliminary Report of an Experience from Iran Seyed Moayed Alavian Professor of Gastroenterology
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Hepatitis C - results in real life
 Hepatitis C - results in real life Robert Flisiak Department of Infectious Diseases and Hepatology Medical University of Białystok, Poland 10th PHC Paris, 30-31 January 2017 Disclosures Advisor and/or
Hepatitis C - results in real life Robert Flisiak Department of Infectious Diseases and Hepatology Medical University of Białystok, Poland 10th PHC Paris, 30-31 January 2017 Disclosures Advisor and/or
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Hepatocellular Carcinoma: Can We Slow the Rising Incidence?
 Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
29th Viral Hepatitis Prevention Board Meeting
 29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice
 3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
Direct acting anti-virals: the near future
 Direct acting anti-virals: the near future Heiner Wedemeyer Hannover Medical School Germany Will IFN-free treatment be possible in the near future? Interferon-free regimens to treat hepatitis C What should
Direct acting anti-virals: the near future Heiner Wedemeyer Hannover Medical School Germany Will IFN-free treatment be possible in the near future? Interferon-free regimens to treat hepatitis C What should
HCV Viremia Was Associated With Increased Mortality in a Prospective Taiwanese Cohort Study
 Tram T. Tran, MD, FACG Approach to HCV Treatment in Patients with HCC Tram T. Tran, MD, FACG Professor of Medicine Medical Director, Liver Transplant Cedars Sinai Medical Center Natural History of HCV
Tram T. Tran, MD, FACG Approach to HCV Treatment in Patients with HCC Tram T. Tran, MD, FACG Professor of Medicine Medical Director, Liver Transplant Cedars Sinai Medical Center Natural History of HCV
The Short-Term Incidence of Hepatocellular Carcinoma Is Not Increased After Hepatitis C Treatment with Direct-Acting Antivirals: An ERCHIVES Study
 The Short-Term Incidence of Hepatocellular Carcinoma Is Not Increased After Hepatitis C Treatment with Direct-Acting Antivirals: An ERCHIVES Study DK Li, YJ Ren, DS Fierer, S Rutledge, OS Shaikh, V Lo
The Short-Term Incidence of Hepatocellular Carcinoma Is Not Increased After Hepatitis C Treatment with Direct-Acting Antivirals: An ERCHIVES Study DK Li, YJ Ren, DS Fierer, S Rutledge, OS Shaikh, V Lo
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients. Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London
 Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
HCV Treatment in 2016: is there still a role for IFNa and ribavirin?
 HCV Treatment in 2016: is there still a role for IFNa and ribavirin? Heiner Wedemeyer Hannover Medical School Germany 1 Disclosures Honoraria for consulting or speaking (last 5 years): Abbott, AbbVie,
HCV Treatment in 2016: is there still a role for IFNa and ribavirin? Heiner Wedemeyer Hannover Medical School Germany 1 Disclosures Honoraria for consulting or speaking (last 5 years): Abbott, AbbVie,
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Hepatitis C and HIV. Stanislas Pol
 Hepatitis C and HIV Stanislas Pol Unité d Hépatologie, Hôpital Cochin Inserm U1223 & USM20 Institut Pasteur Université Paris Descartes Paris, France stanislas.pol@cch.aphp.fr Lisboa, 30 January 2017 Disclosures
Hepatitis C and HIV Stanislas Pol Unité d Hépatologie, Hôpital Cochin Inserm U1223 & USM20 Institut Pasteur Université Paris Descartes Paris, France stanislas.pol@cch.aphp.fr Lisboa, 30 January 2017 Disclosures
Hepatitis B Virus therapy. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
How do you optimize HCV Treatment for Cirrhotic Patients APASL STC Cebu
 How do you optimize HCV Treatment for Cirrhotic Patients APASL STC Cebu Seng Gee Lim Chairman, APASL Liver Week 2013 Professor of Medicine Dept of Gastroenterology and Hepatology NUHS, Singapore Disclosures
How do you optimize HCV Treatment for Cirrhotic Patients APASL STC Cebu Seng Gee Lim Chairman, APASL Liver Week 2013 Professor of Medicine Dept of Gastroenterology and Hepatology NUHS, Singapore Disclosures
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
DAAs in the era of decompensated liver disease. Piero L. Almasio University of Palermo
 DAAs in the era of decompensated liver disease Piero L. Almasio University of Palermo piero.almasio@unipa.it HCV therapy in the era of interferon based therapy Priority Compensated cirrhosis Decompensated
DAAs in the era of decompensated liver disease Piero L. Almasio University of Palermo piero.almasio@unipa.it HCV therapy in the era of interferon based therapy Priority Compensated cirrhosis Decompensated
Viral hepatitis and Hepatocellular Carcinoma
 Viral hepatitis and Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Viral hepatitis and Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
Prognosis of NASH VII Workshop Intenracional de Actualizaçao em Hepatologia, Aug 29th 2014
 Prognosis of NASH VII Workshop Intenracional de Actualizaçao em Hepatologia, Aug 29th 2014 Vlad Ratziu, Université Pierre et Marie Curie, Hôpital Pitié Salpêtrière, Paris, France NASH : a severe hepatic
Prognosis of NASH VII Workshop Intenracional de Actualizaçao em Hepatologia, Aug 29th 2014 Vlad Ratziu, Université Pierre et Marie Curie, Hôpital Pitié Salpêtrière, Paris, France NASH : a severe hepatic
Personalizzazione della Cura in Epatologia. Epatite Cronica C: Pazienti con Genotipo 2
 Monotematica AISF 213 Personalizzazione della Cura in Epatologia Pisa, 17-19 Ottobre 213 Epatite Cronica C: Pazienti con Genotipo 2 Maria Grazia Rumi U.O. Epatologia, Ospedale San Giuseppe Università degli
Monotematica AISF 213 Personalizzazione della Cura in Epatologia Pisa, 17-19 Ottobre 213 Epatite Cronica C: Pazienti con Genotipo 2 Maria Grazia Rumi U.O. Epatologia, Ospedale San Giuseppe Università degli
Hepatitis C No Barriers to Cure
 2018 Digestive Diseases Conference Kansas Hepatitis C No Barriers to Cure Dr. Mauricio Lisker Melman Professor of Medicine Director Hepatology Program Division of Gastroenterology Disclosure The following
2018 Digestive Diseases Conference Kansas Hepatitis C No Barriers to Cure Dr. Mauricio Lisker Melman Professor of Medicine Director Hepatology Program Division of Gastroenterology Disclosure The following
Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London
 Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London IFN free therapy Disclosures I have received personal and institutional funding from companies that sell drug
Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London IFN free therapy Disclosures I have received personal and institutional funding from companies that sell drug
Failure after treatment with DAAs: What to do? Marseille France 2-3 th June 2016
 Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine
 Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine No financial disclosures No conflicts of interest No affiliations
Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine No financial disclosures No conflicts of interest No affiliations
ASSAYS UTILZIED TO MONITOR HCV AND ITS TREATMENT
 ASSAYS UTILZIED TO MONITOR HCV AND ITS TREATMENT Mitchell L Shiffman, MD Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA Liver Institute of Virginia Education, Research
ASSAYS UTILZIED TO MONITOR HCV AND ITS TREATMENT Mitchell L Shiffman, MD Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA Liver Institute of Virginia Education, Research
Pharmacological management of viruses in obese patients
 Cubist Pharmaceuticals The Shape of Cures to Come Pharmacological management of viruses in obese patients Dr. Dimitar Tonev, Medical Director UKINORD 1 Disclosures } The author is a pharmaceutical physician
Cubist Pharmaceuticals The Shape of Cures to Come Pharmacological management of viruses in obese patients Dr. Dimitar Tonev, Medical Director UKINORD 1 Disclosures } The author is a pharmaceutical physician
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Interferon-based and interferon-free new treatment options
 Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Viral Hepatitis The Preventive Potential of Antiviral Therapy. Thomas Berg
 Viral Hepatitis The Preventive Potential of Antiviral Therapy Thomas Berg Therapeutic and preventive strategies in patients with hepatitis virus infection Treatment of acute infection Treatment of chronic
Viral Hepatitis The Preventive Potential of Antiviral Therapy Thomas Berg Therapeutic and preventive strategies in patients with hepatitis virus infection Treatment of acute infection Treatment of chronic
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Liver transplantation and hepatitis C virus
 Liver transplantation and hepatitis C virus Where do we come from? Where are we? Where are we going? François Durand Hépatologie & Réanimation Hépato-Digestive INSERM U1149 Hôpital Beaujon, Clichy HCV:
Liver transplantation and hepatitis C virus Where do we come from? Where are we? Where are we going? François Durand Hépatologie & Réanimation Hépato-Digestive INSERM U1149 Hôpital Beaujon, Clichy HCV:
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
HEPATITIS B: WHO AND WHEN TO TREAT?
 HEPATITIS B: WHO AND WHEN TO TREAT? George V. Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National & Kapodistrian University of Athens Director of Academic Department of
HEPATITIS B: WHO AND WHEN TO TREAT? George V. Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National & Kapodistrian University of Athens Director of Academic Department of