Chapter 26. Learning Objectives. Learning Objectives (Cont d) 9/10/2012. Gastrointestinal Disorders
|
|
|
- Eleanore Fields
- 5 years ago
- Views:
Transcription
1 Chapter 26 Gastrointestinal Disorders 1 Learning Objectives Describe the incidence, morbidity, and mortality rates of GI emergencies Identify risk factors predisposing to GI emergencies Discuss the anatomy, physiology of organs, structures related to GI diseases 2 Learning Objectives (Cont d) Discuss the pathophysiology of inflammation, relation to acute abdominal pain Define somatic pain related to gastroenterology Define visceral pain related to gastroenterology 3 1
2 Learning Objectives (Cont d) Define referred pain related to gastroenterology Differentiate hemorrhagic from nonhemorrhagic abdominal pain Discuss signs, symptoms of local inflammation relative to acute abdominal pain 4 Learning Objectives (Cont d) Discuss signs, symptoms of peritoneal inflammation relative to acute abdominal pain List signs, symptoms of general inflammation relative to acute abdominal pain Based on assessment findings, differentiate local, peritoneal, and general inflammation as related to acute abdominal pain 5 Learning Objectives (Cont d) Discuss the following autoimmune disorders: Systemic lupus erythematosus Insulin-dependent diabetes mellitus Rheumatoid arthritis Celiac disease Chronic active hepatitis Multiple sclerosis Define allergic reaction 6 2
3 Learning Objectives (Cont d) Define anaphylaxis Describe the questioning technique with a focused history in a patient with abdominal pain Describe the technique for a comprehensive physical examination on a patient with abdominal pain Define abdominal wall hernia 7 Learning Objectives (Cont d) Define incarcerated hernia Etiology, signs/symptoms, treatment of incarcerated hernia Define esophagitis Describe common causes, signs/symptoms, treatment of esophagitis 8 Learning Objectives (Cont d) Define candidiasis of the esophagus Describe the etiology, signs/symptoms, treatment of candidiasis esophagitis Describe gastroesophageal reflux Define the cause of gastroesophageal reflux 9 3
4 Learning Objectives (Cont d) Describe the symptoms of reflux, how they differ from other forms of esophagitis Describe the treatment for gastroesophageal reflux Define, provide examples of caustic substances 10 Learning Objectives (Cont d) Define the type of necrosis that occurs with acidic, alkali substances Describe the importance of obtaining a history in caustic ingestion Describe pertinent parts of the physical examination, treatment in caustic ingestion 11 Learning Objectives (Cont d) Define Boerhaave syndrome Describe signs/symptoms, treatment of Boerhaave syndrome Define esophageal foreign body Describe signs/symptoms, treatment of esophageal foreign body 12 4
5 Learning Objectives (Cont d) Define hiatal hernia Describe the signs, symptoms of hiatal hernia Define Mallory-Weiss syndrome Describe the signs/symptoms, treatment of Mallory-Weiss syndrome 13 Learning Objectives (Cont d) Define esophageal stricture and stenosis Describe the signs/symptoms, treatment of esophageal stricture, stenosis Define tracheoesophageal fistula Describe the signs/symptoms, treatment of tracheoesophageal fistula 14 Learning Objectives (Cont d) Define esophageal varices Discuss the pathophysiology of esophageal varices Describe the signs/symptoms, treatment of esophageal varices 15 5
6 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with esophageal varices Define cirrhosis Describe the pathophysiology of cirrhosis 16 Learning Objectives (Cont d) Describe the signs/symptoms, treatment of cirrhosis Define hepatorenal failure Describe the signs/symptoms, treatment of hepatorenal failure Define acute hepatitis 17 Learning Objectives (Cont d) Discuss the pathophysiology of acute hepatitis Recognize the signs/symptoms related to acute hepatitis Describe the management of acute hepatitis 18 6
7 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and to implement a treatment plan for a patient with acute hepatitis Define hepatic tumors Describe signs/symptoms, treatment of hepatic tumors 19 Learning Objectives (Cont d) Define cholecystitis, cholelithiasis, cholangitis, choledocholithiasis Discuss the pathophysiology of cholecystitis Recognize the signs/symptoms, treatment of cholecystitis 20 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with cholecystitis Define pancreatitis 21 7
8 Learning Objectives (Cont d) Recognize signs, symptoms related to pancreatitis Describe the management of pancreatitis Discuss the pathophysiology of pancreatitis 22 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with pancreatitis Define pancreatic tumors Define adenocarcinoma, cyst adenoma, neuroendocrine tumors 23 Learning Objectives (Cont d) Describe the signs/symptoms, treatment of pancreatic tumors Define peritonitis Describe the signs/symptoms, treatment of peritonitis Define gastritis 24 8
9 Learning Objectives (Cont d) Describe the signs/symptoms, treatment of gastritis Define peptic ulcer disease Discuss the pathophysiology of peptic ulcer disease Recognize the signs, symptoms related to peptic ulcer disease 25 Learning Objectives (Cont d) Describe the management of peptic ulcer disease Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with peptic ulcer disease Define upper GI bleeding 26 Learning Objectives (Cont d) Discuss the pathophysiology of upper GI bleeding Recognize signs/symptoms, treatment of upper GI bleeding Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with upper GI bleeding 27 9
10 Learning Objectives (Cont d) Define lower GI bleeding Discuss the pathophysiology of lower GI bleeding Describe the signs/symptoms, treatment of lower GI bleeding 28 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with lower GI bleeding Define acute gastroenteritis Discuss the pathophysiology of acute gastroenteritis 29 Learning Objectives (Cont d) Describe the signs/symptoms, treatment of acute gastroenteritis Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with acute gastroenteritis Define bowel obstruction 30 10
11 Learning Objectives (Cont d) Discuss the pathophysiology of bowel obstruction Describe the signs/symptoms, treatment of bowel obstruction Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with bowel obstruction 31 Learning Objectives (Cont d) Define appendicitis Discuss the pathophysiology of appendicitis Describe the signs/symptoms, treatment of appendicitis 32 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with appendicitis Define colitis Discuss the pathophysiology of colitis 33 11
12 Learning Objectives (Cont d) Describe the signs/symptoms, treatment of colitis Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with colitis Define Crohn s disease 34 Learning Objectives (Cont d) Discuss the pathophysiology of Crohn s disease Describe the signs/symptoms, treatment of Crohn s disease Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with Crohn s disease 35 Learning Objectives (Cont d) Define diverticulitis Discuss the pathophysiology of diverticulitis Describe the signs/symptoms, treatment of diverticulitis 36 12
13 Learning Objectives (Cont d) Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with diverticulitis Define hemorrhoids Discuss the pathophysiology of hemorrhoids 37 Learning Objectives (Cont d) Describe the signs/symptoms, treatment of hemorrhoids Integrate the pathophysiological principles and assessment findings to formulate a field impression and implement a treatment plan for a patient with hemorrhoids Integrate the pathophysiologic principles of a patient with gastrointestinal emergency 38 Learning Objectives (Cont d) Differentiate gastrointestinal emergencies on the basis of assessment findings Correlate abnormal findings in assessment with clinical significance in a patient with abdominal pain Develop a management plan based on field impression in a patient with abdominal pain 39 13
 Anatomy of GI")
14 Introduction Abdominal pain is usually the first sign of gastrointestinal disorder May be the only sign Approximately 7% of patients with abdominal pain complaints have life-threatening conditions 40 Anatomy and Physiology GI tract All structures in eating and processing food Food degradation Nutrient absorption Waste elimination 41 Anatomy and Physiology (Cont d) Anatomy of GI Tract 42 14
15 Anatomy and Physiology (Cont d) GI tract Esophagus Starts from pharynx Distally through chest cavity Passes through diaphragm Terminates at stomach Hollow muscular organ Contracts as swallowed food moves downward from mouth to stomach Lies posterior to trachea, compressible Begin to right of aorta, passes anterior to aorta as it traverses inferiorly 43 Anatomy and Physiology (Cont d) GI tract Stomach Lies inferior to diaphragm in left upper quadrant of abdomen Partially covered by left lobe of liver Protected by ribcage Food passes from stomach, enters duodenum through pyloric sphincter 44 Anatomy and Physiology (Cont d) GI tract Duodenum First part of small intestine Nutrients absorbed as food moves through small intestine by muscular contractions peristalsis Food progresses from duodenum through jejunum and ileum 45 15
16 Anatomy and Physiology (Cont d) GI tract Ligament of Treitz Located at junction of duodenum and jejunum Appendix Small appendage arises from initial part of colon Can become inflamed, infected 46 Anatomy and Physiology (Cont d) GI tract Large intestine Water absorbed Bacteria break down ingested food into nutrients Ascending, transverse, descending 47 Anatomy and Physiology (Cont d) GI tract Small intestine Long structure, 6-7 m Curled back and forth within the abdominal cavity Colon Short, 1.5 m long 48 16
 Small and Large")
 Transverse")
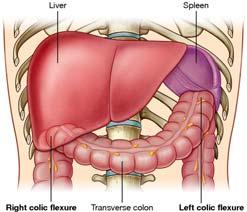
17 Anatomy and Physiology (Cont d) Small and Large Colon 49 Anatomy and Physiology (Cont d) Colon 50 Anatomy and Physiology (Cont d) Transverse Colon 51 17
 GI tract Liver Maintains blood glucose Detoxifies drugs, hormones, foreign substances Produces plasma proteins, aids in blood clotting Bile salts produced, help with food digestion 54 18")
18 Anatomy and Physiology (Cont d) Descending Colon, Rectum, and Anal Canal 52 Anatomy and Physiology (Cont d) GI tract Waste Remaining byproducts of food Feces 53 Anatomy and Physiology (Cont d) GI tract Liver Maintains blood glucose Detoxifies drugs, hormones, foreign substances Produces plasma proteins, aids in blood clotting Bile salts produced, help with food digestion 54 18

")
19 Anatomy and Physiology (Cont d) GI tract Gallbladder Stores bile Sphincter of Odi 55 Anatomy and Physiology (Cont d) Liver, Gallbladder, and Stomach 56 Anatomy and Physiology (Cont d) Abdominal Contents 57 19
 GI tract Peritoneum Thin layer, covers most intraabdominal structures Parietal peritoneum Visceral peritoneum Peritoneal cavity Mesentery 59 Anatomy and")
20 Anatomy and Physiology (Cont d) GI tract Pancreas Located in midepigastric region Endocrine functions Exocrine functions Pancreatic duct expels substances at junction with duodenum Pancreatic failure indicators 58 Anatomy and Physiology (Cont d) GI tract Peritoneum Thin layer, covers most intraabdominal structures Parietal peritoneum Visceral peritoneum Peritoneal cavity Mesentery 59 Anatomy and Physiology (Cont d) Omentum 60 20

 Pathways of Visceral Pain 62 Anatomy & Physiology (Cont d) Localization of")
21 Anatomy and Physiology (Cont d) GI tract Visceral pain Activation of pain receptors enclosed within cavity of chest, abdomen, pelvis Visceral sensory nerve fibers travel with autonomic nerves to communicate with CNS Dully, poorly localized in midline Cramping, burning, gnawing 61 Anatomy and Physiology (Cont d) Pathways of Visceral Pain 62 Anatomy & Physiology (Cont d) Localization of Visceral Pain 63 21
 Patterns of Referred Pain 65 Anatomy and Physiology (Cont d) GI tract Hemorrhage Trauma or rupture of solid or hollow organ")
22 Anatomy and Physiology (Cont d) GI tract Somatic pain Activation of pain in receptors in cutaneous tissues of body s surface or deep body tissues Referred pain Pain perceived as occurring in a part of the body other than the true source 64 Anatomy and Physiology (Cont d) Patterns of Referred Pain 65 Anatomy and Physiology (Cont d) GI tract Hemorrhage Trauma or rupture of solid or hollow organ Fibrous capsule or organs bleed Inflammation Infection, chemical irritation, toxins, autoimmune conditions Source and location help determine cause of disorder 66 22
23 Assessment Adequate history, thorough physical examination History more valuable than physical examination OPQRST Pain Constant Intermittent 67 Assessment (Cont d) Adequate history, thorough physical examination Nausea, vomiting, diarrhea, constipation, bleeding Family history Past medical problems Social history Medication use Open-ended questions 68 Assessment (Cont d) Adequate history, thorough physical examination Inspection Looking at abdomen, pelvis Distention Bruising Swelling Scars Pulsations Discoloration 69 23
 Palpation of Abdominal Quadrants 72")
24 Assessment (Cont d) Adequate history, thorough physical examination Auscultation All four quadrants Gurgling Bowel sounds 70 Assessment (Cont d) Adequate history, thorough physical examination Palpation Presence/absence of tenderness Guarding Abdominal rigidity Masses Organomegaly Rebound tenderness 71 Assessment (Cont d) Palpation of Abdominal Quadrants 72 24
25 Assessment (Cont d) Adequate history, thorough physical examination Percussion Hyperresonant/tympanic 73 Assessment (Cont d) Adequate history, thorough physical examination Disease-specific findings Murphy s sign Rebound tenderness Roving s sign Psoas sign Oburator sign Cutaneous hyperesthesia Cullen s sign Grey Turner s sign Kehr s sign 74 Management (Cont d) Primary measures Determination, treatment of immediate life threats ABCs Comfort measures Pharmacological treatment per local protocol Transport Position of comfort 75 25
26 Abdominal Wall Hernias Abdominal hernia Protrusion of abdominal content Defect/weakness in abdominal wall muscle Congenital Acquired, causes Age Obesity Prior abdominal surgery 76 Abdominal Wall Hernias (Cont d) Incarcerated hernia Abdominal contents will not return through defect into abdominal cavity Can lead to strangulation Pain, fever, nausea, vomiting, obstruction signs Do not attempt to reduce Supportive care IV fluids Rapid transport 77 Esophageal Disorders Esophagitis Any inflammation/infection of esophagus Causes Candidas Infection Caustic ingestions Esophageal reflux Esophageal rupture Pills 78 26

27 Esophagitis Higher incidents Diabetes HIV Alcoholism Cancer Pregnancy Corticosteroids 79 Esophagitis Burning in center of thorax, worse with swallowing History important With pain, use OPQRST Focused examination of neck, chest, abdomen No specific treatment 80 Esophagitis with Esophageal Ulceration 81 27

28 Esophageal candidiasis May grow in oropharynx, down into esophagus Burning pain in esophagus, pain on swallowing Dehydration, IV fluids Urge handwashing 82 Esophageal candidiasis Infectious esophagitis Hemorrhage Nausea, vomiting Fever, chills Necrosis of esophagus Chest pain Difficult pain/swallowing Supportive treatment 83 Severe Candida Esophagitis 84 28

29 Endoscopic View of Esophagus 85 Gastroesophageal reflux disease (GERD) Weakened lower esophageal sphincter Stomach contents move backward up into esophagus Burning, irritation Obesity, smoking, alcohol use weaken lower esophageal sphincter Burning pain in center of thorax 86 Caustic ingestions Intentional, accidental ingestion Toilet bowl cleaners Oven cleaners Bleach Batteries Coagulation necrosis limits penetration through tissues 87 29


30 Coagulative Necrosis 88 Caustic ingestions Alkali ingestions cause liquification necrosis Leads to full-thickness esophageal burns Orofacial burns Drooling Vomiting Pain on swallowing Hoarseness, stridor Chest pain 89 Liquification Necrosis 90 30
31 Caustic ingestions Record accurate history, relay to receiving hospital Identify and transport container Time, amount of ingestion Self-treatment 91 Caustic ingestions Late complications Tissue sloughing Scarring Esophageal stricture formation Gastric outlet obstruction 92 Caustic ingestions Drooling, protect airway Intubation Cricothyroidectomy for extensive upper airway edema Do not induce vomiting NG tube only under medical direction orders 93 31
32 Boerhaave syndrome Perforation of esophagus after forceful vomiting Mortality rate of 50% without surgery within 24 hours History of diffuse pain in chest, radiates to neck, back, abdomen Difficulty breathing or swallowing, may vomit blood Cyanotic 94 Boerhaave syndrome Late cases, esophageal content enters mediastinum Subcutaneous emphysema common if neck perforation Tachycardia, tachypnea Rigid abdomen, fever, hypotension 95 Boerhaave syndrome Treatment Early surgical intervention Rapid transport Airway, hypoxia, shock treatment while en route 96 32

33 Esophageal foreign bodies Some may easily pass Larger ones may obstruct airway Esophagus narrows in four places 97 Esophageal Constriction 98 Esophageal foreign bodies Signs/symptoms Acute onset of difficulty swallowing Foreign body sensation Oral secretion pooling 99 33
34 Esophageal foreign bodies Physical examination Airway, breathing assessment Pooling of oral secretions raises suspicion 100 Esophageal foreign bodies Airway management Rapid transport Glucagon 101 Hiatal hernia Stomach extends proximally, upward through weakness in diaphragm Symptoms similar to GERD Heartburn predominant Assess ABCs Look for esophageal rupture Abdominal pain, cardiac examination performed

35 Hiatal Hernias 103 Mallory-Weiss syndrome Longitudinal tears in distal esophagus, proximal stomach At stomach level, gastroesophageal junction Involve arterial bleeding into esophagus and stomach 104 Mallory-Weiss syndrome Hematemesis, ask about history of vomiting Transport, position of comfort Continued vomiting, antiemetics IV fluids
36 Esophageal stenosis and stricture Stenosis Abnormal narrowing 106 Esophageal stenosis and stricture Stricture Specific form of narrowing, usually from scar tissue ABCs Oral secretion management No prehospital treatment IV fluids for decreased oral intake Unable to swallow foods, liquid, oral secretions should be transported Transport in position of comfort 107 Tracheoesophageal fistula (TEF) Communication between trachea and esophagus Mostly congenital Associated with esophageal atresia, esophagus not continuous from mouth to stomach
37 TEF Potentially fatal respiratory complications Acquired after malignancy, infection, trauma Intubation and prolonged mechanical ventilator support 109 TEF Symptoms, infants Frothy white bubbles despite suctioning Rattling cough Choking Cyanosis Worsens during feeding 110 TEF Symptoms, adult Cough Fever Chills Respiratory distress Pulmonary infections

38 TEF During transport: Reduce aspiration risk Suctioning Head elevation IV hydration ET intubation 112 Esophageal Atresia and Tracheoesophageal Fistula 113 Esophageal varices Dilated vein enlarged from increased pressure Damages to valves within vein Venous pressure Retrograde blood flow Elevated pressure transmission back through GI collaterals
39 Esophageal varices Asymptomatic unless bleeding Cirrhosis most common cause 115 Esophageal varices History Alcoholism Anorexia Nausea, vomiting Weight loss Jaundice 116 Esophageal varices Sudden hematemesis Shock Risk of GI hemorrhage
40 Esophageal varices Internal bleeding Pallor Unexplained shock Cyanotic Dyspneic Tachypneic 118 Esophageal varices If ruptured, life-threatening Management ABCs Hypoxia corrected with O 2 Hemorrhagic shock with IV crystalloid Large-bore IV lines 119 Hepatic Disorders Cirrhosis Chronic liver disease complication Tissue replacement by fibrotic scar tissue Progressive liver function loss
41 Hepatic Disorders (Cont d) Cirrhosis Causes Alcoholic liver disease Hepatitis C 121 Hepatic Disorders (Cont d) Cirrhosis Signs/symptoms Spider angiomata Palmar erythema Dupuytren s contracture Gynecomastia Testicular atrophy Ascites 122 Hepatic Disorders (Cont d) Cirrhosis Signs/symptoms Caput medusa Fetor hepaticus Jaundice Asterixis Encephalopathy Esophageal varices
42 Hepatic Disorders (Cont d) Cirrhosis Effects on body Immune system Coagulation cascade Kidneys CNS Sexual organs Bone formation 124 Hepatic Disorders (Cont d) Cirrhosis Physical examination Head-to-toe Abdomen Skin and sclera, signs of icterus 125 Hepatic Disorders (Cont d) Hepatorenal failure Onset of kidney dysfunction in patients with liver disease No identifiable reason for renal pathology Decreased renal blood flow Decreased urine output Increased leg swelling
 Ascites 128 Hepatic Disorders (Cont d) Acute hepatitis Any inflammation of liver Hepatitis A Recovery, lifelong immunity Vaccine")
43 Hepatic Disorders (Cont d) Hepatorenal failure Dyspnea GI bleeding history ABCs Mental status for encephalopathy Ascites present No prehospital treatment 127 Hepatic Disorders (Cont d) Ascites 128 Hepatic Disorders (Cont d) Acute hepatitis Any inflammation of liver Hepatitis A Recovery, lifelong immunity Vaccine available
44 Hepatic Disorders (Cont d) Acute hepatitis Hepatitis B Cause acute and chronic hepatitis Transmitted by infected body fluid contact Tattoos Sexual contact Infected needles Infected mother can pass it to unborn child 130 Hepatic Disorders (Cont d) Acute hepatitis Hepatitis B Complications Chronic hepatitis Cirrhosis Liver failure Hepatocellular carcinoma Vaccine, all healthcare workers should be inoculated 131 Hepatic Disorders (Cont d) Acute hepatitis Hepatitis C Transmitted through infected blood/body fluids Leads to chronic hepatitis and cirrhosis No vaccine available Asymptomatic up to 20 years Apply standard precautions in every patient Treat life-threatening problems
45 Hepatic Disorders (Cont d) Acute hepatitis Alcoholic hepatitis Increased alcohol consumption Acute liver inflammation Leads to jaundice, liver failure Mortality high 133 Hepatic Disorders (Cont d) Acute hepatitis Drugs, toxins can cause hepatitis Halothane INH phenytoin Zidovudine NSAIDs Acetaminophen 134 Hepatic Disorders (Cont d) Hepatic tumors Prone to develop cancerous tumors after hepatitis B infection Liver common site for primary and metastatic cancers
 Gallstones")
46 Hepatic Disorders (Cont d) Hepatic tumors Signs/symptoms Mimic hepatitis Pain Abdominal distention Cirrhosis/liver failure signs/symptoms Cancer signs Treat life-threatening conditions Supportive care 136 Biliary Disorders Cholecystitis, cholelithiasis, and choledocholithiasis Cholelithiasis Bile solidifies as gallstones 80% formed from cholesterol 137 Biliary Disorders (Cont d) Gallstones
47 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Acalculous cholecystitis Obstruction of cystic duct from gallbladder sludge or inflammation Gallbladder or binary colic Persists, gallbladder becomes inflamed, distended Gallbladder wall edema, ischemia, necrosis Left untreated, bacterial infection 139 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Cholangitis Infection spreads to remainder of biliary tree Life-threatening Rare 140 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Choledocholithiasis Stones stuck or formed in common bile duct Risks Associated with racial, ethnic factors Five Fs
48 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Asymptomatic Location of pain Biliary colic 142 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Symptoms Nausea, vomiting, fever Indigestion, belching, bloating, fatty food intolerance 143 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Physical examination Right upper quadrant, epigastric tenderness Guarding Positive Murphy s sign Febrile Hypotensive ortachycardic
 Acute Pancreatitis")
49 Biliary Disorders (Cont d) Cholecystitis, cholelithiasis, and choledocholithiasis Treatment IV fluids Pain medications Antiemetics 145 Pancreatic Disorders Pancreatitis Inflammation of pancreatic gland Decrease in peristalsis Pancreatic enzymes that aid in food digestion autodigest pancreatic tissue, leads to inflammation Bowel wall edema 146 Pancreatic Disorders (Cont d) Acute Pancreatitis
50 Pancreatic Disorders (Cont d) Pancreatitis Causes Alcohol consumption Gallbladder disease Gallstones 148 Pancreatic Disorders (Cont d) Pancreatitis Findings Constant, severe midepigastric pain, radiates directly to back Pain may travel to right or left upper abdominal quadrant OPQRST Check for history of trauma, medication ingestion, illness 149 Pancreatic Disorders (Cont d) Pancreatitis Findings Symptoms Fever, nausea, vomiting Appear systemically ill Restless Tachycardia Tachypnea Febrile Hypotensive Jaundice Epigastrum or right upper quadrant tender Breath sounds diminished or absent Distention, guarding, rigidity of abdomen
51 Pancreatic Disorders (Cont d) Pancreatitis Treatment Symptomatic Address life-threatening conditions Hypotensive, dehydrated, shock, provide IV crystalloids Nasogastric tube Analgesics 151 Pancreatic Disorders (Cont d) Pancreatic tumors Divided according to cell type 95% pancreatic cancers, adenocarcinomas derived from exocrine cells Cyst adenomas Neuroendocrine tumors/islet cell tumors 152 Pancreatic Disorders (Cont d) Pancreatic tumors Symptoms Dull pain in upper abdomen, radiates to back Painless jaundice develops as tumor obstructs the bile duct Weak, dizzy, hypoglycemic
52 Pancreatic Disorders (Cont d) Pancreatic tumors Treatment Supportive care Life-threatening emergencies treated Treat pain, nausea, vomiting Transport 154 Pancreatic Disorders (Cont d) Peritonitis Peritoneal membrane inflammation Causes Infection Trauma Bowel rupture 155 Pancreatic Disorders (Cont d) Peritonitis Signs/symptoms Abdominal pain Fever Nausea, vomiting Anorexia in appendicitis Rebound tenderness Septic with fever Hypothermia Chills Hypotension Bowel sounds decreased, absent
53 Pancreatic Disorders (Cont d) Peritonitis Spontaneous bacterial peritonitis (SBP) Occurs in liver cirrhosis Asymptomatic Portal hypertension with cirrhosis causes bowel wall and mucosa swelling 157 Pancreatic Disorders (Cont d) Peritonitis Spontaneous bacterial peritonitis (SBP) Symptoms Worsening hepatic or renal function Underlying liver disease Septic shock IV fluids for tachycardia or shock Pain, nausea medications 158 Stomach Disorders Gastritis Gastric mucosa inflammation Chronic gastritis Caused by Helicobacter pylori
 Acute Gastritis 161 Stomach Disorders (Cont d) Gastritis Acute gastritis Signs/symptoms Dyspepsia Bloating Indigestion Heartburn Belching")
54 Stomach Disorders (Cont d) Gastritis Acute gastritis Result of local injury to gastric mucosa Viral infection, substance ingestion that irritates gastric mucosa Alcohol, prescription and OTC medications common causes 160 Stomach Disorders (Cont d) Acute Gastritis 161 Stomach Disorders (Cont d) Gastritis Acute gastritis Signs/symptoms Dyspepsia Bloating Indigestion Heartburn Belching Nausea, vomiting
55 Stomach Disorders (Cont d) Gastritis Acute gastritis Hemorrhagic gastritis development Hematemesis Melena Hemorrhagic shock 163 Stomach Disorders (Cont d) Gastritis Acute gastritis Thorough history Current pain Medical history Medications Social history 164 Stomach Disorders (Cont d) Gastritis Acute gastritis Treatment Treat life-threatening conditions Hemorrhagic shock, do not delay treatment Rapid transport Position of comfort Manage pain, nausea Continual reassessment ABCs
 Chronic Peptic Ulcer 167 Stomach Disorders (Cont d) Peptic ulcer disease Causes Aspirin NSAIDs Smoking Heavy, prolonged alcohol consumption H.")
56 Stomach Disorders (Cont d) Peptic ulcer disease Stomach and small intestine gastric mucosa defects Bleed, causing pain, morbidity, death Formed when production of hydrochloric acid and pepsin by gastric mucosa increased 166 Stomach Disorders (Cont d) Chronic Peptic Ulcer 167 Stomach Disorders (Cont d) Peptic ulcer disease Causes Aspirin NSAIDs Smoking Heavy, prolonged alcohol consumption H. pylori Imbalance between stomach acid production Inability of gastric mucosa to prevent acid damage Zollinger-Ellison syndrome
57 Stomach Disorders (Cont d) Peptic ulcer disease Occurs in stomach or first part of duodenum Findings Burning, gnawing pain in epigastric region Vague or cramping pain 169 Stomach Disorders (Cont d) Peptic ulcer disease Complications Perforation Inflammation and swelling to create acute obstruction Hemorrhage Bleeding Pallor Tachycardia Hypotension Frank hemorrhagic shock 170 Stomach Disorders (Cont d) Peptic ulcer disease History Focus on symptoms Pain type Relation of pain to food Previous diagnosis
58 Stomach Disorders (Cont d) Peptic ulcer disease Physical examination Primary survey Treat frank hematemesis, melena, shock with fluid resuscitation Rapid transport If stable, complete abdominal examination 172 Stomach Disorders (Cont d) Peptic ulcer disease Treatment None available Antacids, H2 blockers for pain 173 Stomach Disorders (Cont d) Upper and lower gastrointestinal bleeding Upper GI bleed Above ligament of Treitz Causes Caustic ingestions Mallory-Weiss tears Esophageal varices Gastritis and peptic ulcers Male predominance
59 Stomach Disorders (Cont d) Upper and lower gastrointestinal bleeding Upper GI bleed Abdominal pain Hematemesis Coffee ground emesis Melena 175 Stomach Disorders (Cont d) Upper and lower gastrointestinal bleeding Lower GI bleed Below ligament of Treitz Causes Distal to ligament of Treitz Diverticular disease Tumors Polyps Hemorrhoids Autoimmune disease Anal fissures Female predominance 176 Stomach Disorders (Cont d) Upper and lower gastrointestinal bleeding Lower GI bleed Hematochezia Implies larger, more rapid blood loss Rule out other sources of hemorrhage Hemorrhoids
60 Stomach Disorders (Cont d) Upper and lower gastrointestinal bleeding Lower GI bleed Good medical history History of bleeding Social history Fatigue, shortness of breath, vomiting, black tarry stool 178 Stomach Disorders (Cont d) Upper and lower gastrointestinal bleeding Lower GI bleed Treatment Mild Massive 179 Bowel Disorders Gastroenteritis Inflammation of stomach lining and intestines Causes disruption in normal functioning of the mucosal lining
61 Gastroenteritis Symptoms Cramping Abdominal pain Nausea, vomiting Fever Anorexia Malaise Headache Watery diarrhea 181 Gastroenteritis Causes Virus Typically passed from person to person, eating contaminated food Norwalk virus Norovirus Adenovirus Astrovirus Rotavirus 182 Gastroenteritis Transmission causes Fecal-oral route from poorly cooked meat, poorly refrigerated food, contaminated food Parasites Wheat intolerance Lactose intolerance Allergies Autoimmune conditions Medications Radiation therapy Chemical toxins
62 Gastroenteritis Chronic causes Infection Medication use Inflammatory conditions Toxins 184 Gastroenteritis History Onset Symptoms Pain Symptom duration Chemical exposure Possible food poisoning Camping, hiking Foreign travel Swimming in potentially infected water Previous medical conditions 185 Gastroenteritis Physical examination Detailed abdominal examination Increased bowel sounds on auscultation Mild tenderness on palpation, all four quadrants Skin for tenting, dehydration sign Muscle spasm
63 Gastroenteritis Treatment IV access, fluids Nausea, abdominal cramping medications Supportive 187 Obstruction Small or large bowel lumen blocked Large bowel obstructions Caused by malignant disease Bowel contents cannot flow forward Disrupts normal function of digestive system Ileus 188 Obstruction Results from complete mechanical obstruction of the intestine Adhesions Hernia Polyps Tumors Foreign body Impacted stool Intussusceptions Volvulus

64 Volvulus 190 Obstruction Signs/symptoms Nausea, vomiting Abdominal pain Lack of bowel movements Diarrhea Inability to pass bowel gas Abdominal distention Pain, crampy, colicky 191 Obstruction History Past medical history Previous bowel obstructions Abdominal surgery Cancer Radiation therapy Chemotherapy Hernia Abdominal illness Nausea, vomiting, bowel habits
65 Obstruction Physical examination Primary survey Thorough abdominal examination 193 Obstruction Treatment Position of comfort IV access, fluids Dehydration, fluids Avoid food/water by mouth NG tube removes normal fluids produced by stomach Medication for pain, nausea Transport 194 Appendicitis Inflammation of small tubular structure arising off colon near cecum Fecalith, obstruction Becomes highly distended, inflamed, gangrenous If it ruptures, bowel contents spill into abdomen causing peritonitis


66 Inflamed Appendix 196 Appendix Positions 197 Appendicitis Symptoms Fever, nausea Abdominal pain Poorly localized dull pain in periumbilical area Pain in right lower quadrant, right lower back
67 Appendicitis History Surgical history Appetite Pain location Onset Fever 199 Appendicitis Physical examination Abdominal examination Possible pain with movement of pelvis/hips Rovsing s sign Appendix location varies Retrocecal McBurney s point 200 Appendicitis Treatment IV access, fluids Avoid food/beverages Pain, nausea medications Transport in position of comfort

68 Ulcerative colitis Inflamed large bowel Ulcers form on mucosal surface of intestine Affects colon, mostly rectum Immune system overreacts to viral/bacterial insult 202 Acute Ulcerative Colitis 203 Ulcerative colitis Symptoms Diarrhea Abdominal cramping Bloody/purulent stools Fatigue Weakness Weight loss Appetite loss
69 Ulcerative colitis History Recurrent fatigue, diarrhea, abdominal discomfort Physical examination Thorough abdominal examination Appendicitis Obstruction Gastroenteritis 205 Ulcerative colitis Treatment Supportive IV fluids Pain, nausea, vomiting medications Transport in position of comfort 206 Crohn s disease Inflammatory bowel condition Affects small, large intestine Genetic tendencies
70 Crohn s disease Findings Significant swelling Ulcerations go through all layers of bowel Scar tissue Obstruction 208 Crohn s disease Signs and symptoms Nausea, vomiting Severe diarrhea Abdominal pain, cramping Weight loss Appetite loss Skin conditions Arthritis Gallbladder disease Inflammatory eye conditions Ulcerations of nose, mouth Kidney stones 209 Crohn s disease History Abdominal cramping RUQ pain Kidney stones Arthritis Bladder, vaginal problems Fistula with pus, stool leaking from ulcer in skin
71 Crohn s disease Physical examination Head-to-toe Thorough abdominal examination Peritonitis from ruptured bowel Abdominal distention Rebound tenderness Fever Severe sepsis 211 Crohn s disease Treatment Rapid assessment Treat life-threatening conditions Management of ABCs IV access, fluids Medication for pain Rapid transport 212 Diverticulosis and diverticulitis Small sacs, outpouches form along bowel wall Fiber-deficient diets

72 Diverticulosis and diverticulitis Diverticulosis Multiple diverticula Develop from bowel wall stretching Asymptomatic Irregular bowel movements Painless bloody stools 214 Diverticulosis and diverticulitis Diverticulitis Diverticula become inflamed, infection Digested food trapped in pouches, causes infection Fever Shaking chills Nausea, vomiting Abdominal pain Diarrhea 215 Diverticular Disease
73 Diverticulosis and diverticulitis History Nausea, vomiting Fever Chills Pain Compare to previous abdominal complaints 217 Diverticulosis and diverticulitis Physical examination Comprehensive Abdomen, pelvis 218 Diverticulosis and diverticulitis Treatment Supportive IV access, fluids Pain, nausea medication
74 Hemorrhoids Swollen venous tissue originating from anal area Internal or external Increased pressure or straining during defecation 220 Hemorrhoids Signs/symptoms Itching, pain, burning Rectal bleeding Bleeding that drips into toilet after defecation 221 Hemorrhoids History Bowel habits Presence of hemorrhoids Bleeding that stains toilet tissue Large bloody stools treated as GI bleed
75 Hemorrhoids Physical examination Thorough examination of the abdomen Treatment Supportive 223 Gastrointestinal Illness Accurate history important Can be life-threatening Thorough history and physical examination Open-ended questions OPQRST for pain Nausea, vomiting, diarrhea, stool consistency/color 224 Gastrointestinal Illness (Cont d) Treatment Immediately address life-threatening conditions Shock, large blood loss, assess quickly and transport IV fluids en route
76 Chapter Summary Abdominal pain is one of the most common reasons why patients seek emergency care Etiology of abdominal pain varies with patient s age, risk factors GI system includes all organs responsible for ingestion and digestion of food 226 Chapter Summary (Cont d) Pain well localized, somatic pain Pain poorly localized, visceral pain Pain felt at distant location, referred pain Assess pain with OPQRST 227 Chapter Summary (Cont d) Assessment, ask open-ended questions Management of GI symptoms should include primary survey, secondary survey, pain and nausea management, fluid replacement Local protocols should be followed for appropriate treatment and management
77 Chapter Summary (Cont d) Hernias that become strangulated/incarcerated can pose a serious medical condition Esophagitis, inflammation of the esophagus, has many causes GERD, common disorder, leads to esophagitis 229 Chapter Summary (Cont d) Caustic ingestions can cause trauma to the esophagus Historical facts, time of ingestion, chemical ingestion, and amount ingested are important Airway control important in caustic ingestions 230 Chapter Summary (Cont d) Esophageal obstruction can occur with caustic ingestions Most foreign objects will pass through the GI tract if enters the stomach Vomiting may lead to longitudinal tears in the esophagus called Mallory-Weiss tears Hematemesis may occur
78 Chapter Summary (Cont d) Esophageal stenosis can occur from esophagitis Tracheoesophageal fistula and esophageal atresia are congenital conditions Tracheoesophageal fistula can lead to aspiration of food and liquids into the lungs 232 Chapter Summary (Cont d) Esophageal varices can be caused by portal hypertension Hematemesis may occur with varices, may be serious Cirrhosis can lead to liver failure Cirrhosis is caused by damage to liver cells 233 Chapter Summary (Cont d) Cirrhosis can lead to ascites, fluid in the abdominal cavity Ascites can become infected, lead to sepsis (SBP) Cirrhosis can cause encephalopathy, altered consciousness/coma
79 Chapter Summary (Cont d) Renal failure may follow liver failure Hepatitis, an inflammatory condition of the liver Hepatitis may be self-limiting, progress to liver failure Hepatitis A transmitted by fecal-oral route 235 Chapter Summary (Cont d) Hepatitis B transmitted by sexual contact, body fluid, tattoos, blood transfusions Hepatitis C transmitted by infected blood, body fluids Cholelithiasis, the presence of stones in the gallbladder 236 Chapter Summary (Cont d) Cholelithiasis occurs in 10-20% of the population in developed countries Pancreatitis, inflammation of the pancreas Pancreatitis can present with severe abdominal pain, nausea, vomiting
80 Chapter Summary (Cont d) Peritonitis, inflamed lining of the abdominal cavity Rebound tenderness may be present with peritonitis Gastritis, inflammation of the gastric mucosa 238 Chapter Summary (Cont d) Gastritis can present with significant abdominal pain Peptic ulcers can cause significant GI bleeding GI bleeding has many causes; begin treatment with primary survey 239 Chapter Summary (Cont d) Appendicitis begins with periumbilical pain Appendicitis can lead to sepsis if the luminal cavity ruptures Ulcerative colitis typically affects the rectum; an inflammatory condition that involves the mucosal lining of the GI tract
81 Chapter Summary (Cont d) Crohn s disease can affect the small and large intestines; it can cause erosion through all layers of the bowel, leading to fistula formation Patients with Crohn s disease may have arthritis, skin conditions, inflammatory conditions of the eye, bowel symptoms 241 Chapter Summary (Cont d) Diverticular disease caused by stretching of the bowel during straining, low-fiber diets, disease of colonic diverticula, inflammation of 1+ of outpouchings Hemorrhoids, distended veins either internal or external to the anal opening 242 Questions?
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
The Digestive System. Chapter
 The Digestive System Chapter 15.1 Functions: mechanical and chemical breakdown of food *absorption of nutrients Consists of alimentary canal and accessory organs Wall of the Alimentary Canal 15.2 Characteristics
The Digestive System Chapter 15.1 Functions: mechanical and chemical breakdown of food *absorption of nutrients Consists of alimentary canal and accessory organs Wall of the Alimentary Canal 15.2 Characteristics
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
Chapter 18 - Gastrointestinal & Urologic Emergencies
 1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
1 2 3 4 5 6 7 8 Chapter 18 Gastrointestinal and Urologic National EMS Education Standard Competencies (1 of 4) Medicine Applies fundamental knowledge to provide basic emergency care and transportation
Glencoe Health. Lesson 3 The Digestive System
 Glencoe Health Lesson 3 The Digestive System Health espotlight Video BIG IDEA The digestive system provides nutrients and energy for your body through the digestion of food. New Vocabulary mastication
Glencoe Health Lesson 3 The Digestive System Health espotlight Video BIG IDEA The digestive system provides nutrients and energy for your body through the digestion of food. New Vocabulary mastication
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Digestive System. Unit 6.11 (6 th Edition) Chapter 7.11 (7 th Edition)
 Chapter 7.11 (7 th Edition)") Digestive System Unit 6.11 (6 th Edition) Chapter 7.11 (7 th Edition) 1 Learning Objectives Identify the major organs of the digestive system. Explain the locations and functions of three organs in the
Digestive System Unit 6.11 (6 th Edition) Chapter 7.11 (7 th Edition) 1 Learning Objectives Identify the major organs of the digestive system. Explain the locations and functions of three organs in the
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Diet and Gastrointestinal Problems
 Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
ESSENTIAL QUESTION. What are the structures of the digestive system? THE DIGESTIVE SYSTEM
 ESSENTIAL QUESTION What are the structures of the digestive system? THE DIGESTIVE SYSTEM DIGESTIVE SYSTEM, AKA. ALIMENTARY CANAL digestive tract or gastrointestinal tract (GI Tract). A 30 ft. tube from
ESSENTIAL QUESTION What are the structures of the digestive system? THE DIGESTIVE SYSTEM DIGESTIVE SYSTEM, AKA. ALIMENTARY CANAL digestive tract or gastrointestinal tract (GI Tract). A 30 ft. tube from
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Student Notes Chapter 16: Gastrointestinal and Urologic Emergencies 1. Chapter 16. Gastrointestinal and Urologic Emergencies
 Student Notes Chapter 16: Gastrointestinal and Urologic Emergencies 1 Chapter 16 Gastrointestinal and Urologic Emergencies Unit Summary Students who complete this chapter presentation and the related course
Student Notes Chapter 16: Gastrointestinal and Urologic Emergencies 1 Chapter 16 Gastrointestinal and Urologic Emergencies Unit Summary Students who complete this chapter presentation and the related course
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
- Digestion occurs during periods of low activity - Produces more energy than it uses. - Mucosa
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
64a Pathology: Digestive System!
 64a Pathology: Digestive System! 64a Pathology: Digestive System! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:" 25 minutes "Lecture:" 15 minutes "Active
64a Pathology: Digestive System! 64a Pathology: Digestive System! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:" 25 minutes "Lecture:" 15 minutes "Active
Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain
 Flexbook by Brian Lindshield is in the public domain") Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain in the United States. 5 Common Digestive Problems Before
Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain in the United States. 5 Common Digestive Problems Before
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Digestive System. Digestion Myths
 Digestive System Digestion Myths Myth # 1 Ulcers: Spicy food and stress cause stomach ulcers. Myth # 2 Heartburn: Smoking a cigarette helps relieve heartburn. Myth # 3 Celiac Disease: Celiac disease is
Digestive System Digestion Myths Myth # 1 Ulcers: Spicy food and stress cause stomach ulcers. Myth # 2 Heartburn: Smoking a cigarette helps relieve heartburn. Myth # 3 Celiac Disease: Celiac disease is
- Digestion occurs during periods of low activity - Produces more energy than it uses. 3 Copyright 2016 by Elsevier Inc. All rights reserved.
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
HCPCS Codes (Alphanumeric, CPT AMA) ICD-9-CM Codes Covered by Medicare Program
 ICD-9-CM Codes Covered by Medicare Program") HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
NCD for Fecal Occult Blood Test
 NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
PLEASE COMPLETE ALL SECTIONS OF THIS FORM
 PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
Figure Care of the Patient with a Gastrointestinal Disorder. Location of digestive organs.
 Care of the Patient with a Gastrointestinal Disorder 1 Slide 1 Slide 2 Figure 45-1 (From Thibodeau, G.A., Patton, K.T. [1987]. Anatomy and physiology. St. Louis: Mosby.) Location of digestive organs. Slide
Care of the Patient with a Gastrointestinal Disorder 1 Slide 1 Slide 2 Figure 45-1 (From Thibodeau, G.A., Patton, K.T. [1987]. Anatomy and physiology. St. Louis: Mosby.) Location of digestive organs. Slide
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
The Nature of Disease Pathology for the Health Professions. Chapter 11. Disorders of the GI Tract. Lecture 11
 The Nature of Disease Pathology for the Health Professions Thomas H. McConnell Chapter 11 Disorders of the GI Tract Lecture 11 Review of the GI Tract Anatomy & Function Figures from: McConnell, The Nature
The Nature of Disease Pathology for the Health Professions Thomas H. McConnell Chapter 11 Disorders of the GI Tract Lecture 11 Review of the GI Tract Anatomy & Function Figures from: McConnell, The Nature
: Abdominal Emergencies
 INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 20 Caring for Clients with Bowel Disorders Diarrhea Pathophysiology Result from impaired water absorption
Digestive System. In one end and out the other.
 Digestive System In one end and out the other. Overview Every cell in the body needs nourishment, yet most cells cannot leave their position in the body and travel to a food source, so the food must be
Digestive System In one end and out the other. Overview Every cell in the body needs nourishment, yet most cells cannot leave their position in the body and travel to a food source, so the food must be
An overview of the digestive system. mouth pharynx esophagus stomach small intestine large intestine rectum anus
 An overview of the digestive system mouth pharynx esophagus stomach small intestine large intestine rectum anus Why GIT? What are the main steps in the digestive process? Ingestion intake of food via the
An overview of the digestive system mouth pharynx esophagus stomach small intestine large intestine rectum anus Why GIT? What are the main steps in the digestive process? Ingestion intake of food via the
Chapter 15. Cardiovascular, Respiratory, Digestive Systems
 Chapter 15 Cardiovascular, Respiratory, Digestive Systems Cardiovascular/Respiratory Systems Cardiovascular System Blood is pumped to the body 24/7 Heart s tasks: Carries oxygen from lungs to body cells
Chapter 15 Cardiovascular, Respiratory, Digestive Systems Cardiovascular/Respiratory Systems Cardiovascular System Blood is pumped to the body 24/7 Heart s tasks: Carries oxygen from lungs to body cells
The Digestive System
 The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
ORGANS OF THE DIGESTIVE SYSTEM
 ORGANS OF THE DIGESTIVE SYSTEM OBJECTIVES: 1. List and describe the major activities of the digestive system. 2. Identify and give the functions of the organs in and along the digestive tract. MAJOR ACTIVITIES
ORGANS OF THE DIGESTIVE SYSTEM OBJECTIVES: 1. List and describe the major activities of the digestive system. 2. Identify and give the functions of the organs in and along the digestive tract. MAJOR ACTIVITIES
Digestive System 7/15/2015. Outline Digestive System. Digestive System
 Digestive System Biology 105 Lecture 18 Chapter 15 Outline Digestive System I. Functions II. Layers of the GI tract III. Major parts: mouth, pharynx, esophagus, stomach, small intestine, large intestine,
Digestive System Biology 105 Lecture 18 Chapter 15 Outline Digestive System I. Functions II. Layers of the GI tract III. Major parts: mouth, pharynx, esophagus, stomach, small intestine, large intestine,
Tissues: systems of cells working together to perform specialized tasks. Ex muscles, nerves, blood
 Chapter 3 Cells: the smallest units in which independent life can exist. All living things are single cells or organisms made of cells. Need water and nutrients to survive Enzyme: any of the great working
Chapter 3 Cells: the smallest units in which independent life can exist. All living things are single cells or organisms made of cells. Need water and nutrients to survive Enzyme: any of the great working
Includes mouth, pharynx, esophagus, stomach, small intestine, large intestine, rectum, anus. Salivary glands, liver, gallbladder, pancreas
 Chapter 14 The Digestive System and Nutrition Digestive System Brings Nutrients Into the Body The digestive system includes Gastrointestinal (GI) tract (hollow tube) Lumen: space within this tube Includes
Chapter 14 The Digestive System and Nutrition Digestive System Brings Nutrients Into the Body The digestive system includes Gastrointestinal (GI) tract (hollow tube) Lumen: space within this tube Includes
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Chapter 26 The Digestive System
 Chapter 26 The Digestive System Digestive System Gastroenterology is the study of the stomach and intestine. Digestion Catabolism Absorption Anabolism The actions of the digestive system are controlled
Chapter 26 The Digestive System Digestive System Gastroenterology is the study of the stomach and intestine. Digestion Catabolism Absorption Anabolism The actions of the digestive system are controlled
Gastrointestinal & Genitourinary Emergencies. Lesson Goal. Learning Objectives 9/10/2012
 Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
Gastrointestinal & Genitourinary Emergencies Lesson Goal Recognize, assess & provide care to patients with abdominal cavity injuries Learning Objectives Discuss different causes of nontraumatic abdominal
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
3/16/2016. Food--mixture of carbohydrates, proteins, and lipids
 Food--mixture of carbohydrates, proteins, and lipids Food being broken down into small molecules Takes place in the alimentary canal Complete digestive system 4 layers of tissue (in book) Lumen 1) MECHANICAL/PHYSICAL--
Food--mixture of carbohydrates, proteins, and lipids Food being broken down into small molecules Takes place in the alimentary canal Complete digestive system 4 layers of tissue (in book) Lumen 1) MECHANICAL/PHYSICAL--
Bellwork. Define (page 347 and 348): Peristalsis Chyme hepa chole Copy the underlined portion of the state standards on the next slide.
: Peristalsis Chyme hepa chole Copy the underlined portion of the state standards on the next slide.") Digestive System Bellwork Define (page 347 and 348): Peristalsis Chyme hepa chole Copy the underlined portion of the state standards on the next slide. State Standards 11) Outline the gross normal structure
Digestive System Bellwork Define (page 347 and 348): Peristalsis Chyme hepa chole Copy the underlined portion of the state standards on the next slide. State Standards 11) Outline the gross normal structure
Chapter 44 10/17/2015. Care of the Patient with a Gastrointestinal Disorder. The Digestive System. Organs of the Digestive System
 Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
Chapter Outline. Structural defects. Obstructive disorders. Preview from Notesale.co.uk Page 3 of 98. Cleft lip and cleft palate
 Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Digestion. Absorption and Transport. Digestion. Digestion. (Chapter 3) Your GI tract is like a tube!
 Your GI tract is like a tube!") Digestion Absorption and Transport Digestion the process of breaking down food into its basic components so they can be absorbed CHO, fat, pro are hydrolysed Vits, mins, water aren t (Chapter 3) Digestion
Digestion Absorption and Transport Digestion the process of breaking down food into its basic components so they can be absorbed CHO, fat, pro are hydrolysed Vits, mins, water aren t (Chapter 3) Digestion
PHYSIOLOGY OF THE DIGESTIVE SYSTEM
 Student Name CHAPTER 26 PHYSIOLOGY OF THE DIGESTIVE SYSTEM D igestion is the process of breaking down complex nutrients into simpler units suitable for absorption. It involves two major processes: mechanical
Student Name CHAPTER 26 PHYSIOLOGY OF THE DIGESTIVE SYSTEM D igestion is the process of breaking down complex nutrients into simpler units suitable for absorption. It involves two major processes: mechanical
Digestion. Intake and assimilation of nutrients Elimination of waste Eating Required physically Pleasurable Social Emotional
 Digestive System 1 Digestion Intake and assimilation of nutrients Elimination of waste Eating Required physically Pleasurable Social Emotional Food behaviors can become just as addictive as any other pleasurable
Digestive System 1 Digestion Intake and assimilation of nutrients Elimination of waste Eating Required physically Pleasurable Social Emotional Food behaviors can become just as addictive as any other pleasurable
GI -A & P Review PUD. Peptic Ulcer Disease (PUD) Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer
 Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer") GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
Two main groups Alimentary canal continuous coiled hollow tube Accessory digestive organs
 Digestion Breakdown of ingested food Absorption of nutrients into the blood Metabolism Production of cellular energy (ATP) Constructive and degradative cellular activities Two main groups Alimentary canal
Digestion Breakdown of ingested food Absorption of nutrients into the blood Metabolism Production of cellular energy (ATP) Constructive and degradative cellular activities Two main groups Alimentary canal
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Jhia Anjela D. Rivera 1 1. BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines
 DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
The Digestive System. Chapter 25
 The Digestive System Chapter 25 Introduction Structure of the digestive system A tube that extends from mouth to anus Accessory organs are attached Functions include Ingestion Movement Digestion Absorption
The Digestive System Chapter 25 Introduction Structure of the digestive system A tube that extends from mouth to anus Accessory organs are attached Functions include Ingestion Movement Digestion Absorption
Clinical Manifestations of Gastrointestinal Disorders. Awni Taleb Abu sneineh
 Clinical Manifestations of Gastrointestinal Disorders Awni Taleb Abu sneineh Major areas of Interest in GIT Esophageal disorders Peptic ulcer disease Inflamatory bowel disease Malignancy Liver disease
Clinical Manifestations of Gastrointestinal Disorders Awni Taleb Abu sneineh Major areas of Interest in GIT Esophageal disorders Peptic ulcer disease Inflamatory bowel disease Malignancy Liver disease
PATIENT HISTORY FORM
 PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Pediatric Ingestion Injuries: Assessment & Treatment
 Pediatric Ingestion Injuries: Assessment & Treatment Benjamin L. Eithun, MSN, CRNP, RN, CPNP-AC, CCRN, TCRN Andrea L. Williams, PhD, RN UW Health & AFCH Case #1 Presentation Dispatched to Sandstone Ridge
Pediatric Ingestion Injuries: Assessment & Treatment Benjamin L. Eithun, MSN, CRNP, RN, CPNP-AC, CCRN, TCRN Andrea L. Williams, PhD, RN UW Health & AFCH Case #1 Presentation Dispatched to Sandstone Ridge
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
HASPI Medical Anatomy & Physiology 15a Lab Activity
 HASPI Medical Anatomy & Physiology 15a Lab Activity Name(s): Period: Date: The Digestive System Digestion is an important process that involves breaking down food and drink into small molecules that can
HASPI Medical Anatomy & Physiology 15a Lab Activity Name(s): Period: Date: The Digestive System Digestion is an important process that involves breaking down food and drink into small molecules that can
TEST 5. Module 9 & 10
 TEST 5 Module 9 & 10 Questions from the GVLS website 1. Heart 2. Blood 3. Blood Vessels 4. Circulation 5. Blood Pressure 6. Respiratory system 7. Lungs 8. Oxygen 9. Carbon Dioxide 10. The heart is made
TEST 5 Module 9 & 10 Questions from the GVLS website 1. Heart 2. Blood 3. Blood Vessels 4. Circulation 5. Blood Pressure 6. Respiratory system 7. Lungs 8. Oxygen 9. Carbon Dioxide 10. The heart is made
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
FY 2016 MCRCEDP Approved ICD-10 Code List
 Approved List C18.0 Malignant neoplasm of cecum C18.1 Malignant neoplasm of appendix C18.2 Malignant neoplasm of ascending colon C18.3 Malignant neoplasm of hepatic flexure C18.4 Malignant neoplasm of
Approved List C18.0 Malignant neoplasm of cecum C18.1 Malignant neoplasm of appendix C18.2 Malignant neoplasm of ascending colon C18.3 Malignant neoplasm of hepatic flexure C18.4 Malignant neoplasm of
Learning Targets. The Gastrointestinal (GI) Tract. Also known as the alimentary canal. Hollow series of organs that food passes through
 Tract. Also known as the alimentary canal. Hollow series of organs that food passes through") Digestion the multistep process of breaking down food into molecules the body can use Learning Targets Describe the path food takes through the digestive system. Identify the major organs of the digestive
Digestion the multistep process of breaking down food into molecules the body can use Learning Targets Describe the path food takes through the digestive system. Identify the major organs of the digestive
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Gastrointestinal System: Accessory Organ Disorders
 Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
Gastrointestinal System: Accessory Organ Disorders Mary DeLetter, PhD, RN Associate Professor Dept. of Baccalaureate and Graduate Nursing Eastern Kentucky University Disorders of Accessory Organs Portal
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module
 SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Dawn Daniels Tucson Medical Center January 2016 PURPOSE This SAEMS Standing Order Training Module has been developed to serve as a template for
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Dawn Daniels Tucson Medical Center January 2016 PURPOSE This SAEMS Standing Order Training Module has been developed to serve as a template for
Ingestion Digestion- Absorption- Elimination
 DIGESTIVE SYSTEM 1 FUNCTIONS Organization GI tract==mouth anus Accessory organs Salivary glands, liver, pancreas, gallbladder Major Functions: Ingestion-mouth, teeth, tongue Digestion- chemical and mechanical
DIGESTIVE SYSTEM 1 FUNCTIONS Organization GI tract==mouth anus Accessory organs Salivary glands, liver, pancreas, gallbladder Major Functions: Ingestion-mouth, teeth, tongue Digestion- chemical and mechanical
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
JOHN MICHAEL ROACH, MD
 GASTROENTEROLOGY JOHN MICHAEL ROACH, MD 520 N. 4 TH AVE. PASCO, WA 99301 Phone: (509) 546-8383 Name: Date of Birth: First Middle (full) Last m/d/yr Primary care provider: Referring physician: Local Pharmacy:
GASTROENTEROLOGY JOHN MICHAEL ROACH, MD 520 N. 4 TH AVE. PASCO, WA 99301 Phone: (509) 546-8383 Name: Date of Birth: First Middle (full) Last m/d/yr Primary care provider: Referring physician: Local Pharmacy:
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
Ulcerative Colitis. ulcerative colitis usually only affects the colon.
 Ulcerative Colitis Introduction Ulcerative colitis is an inflammatory bowel disease. It is one of the 2 most common inflammatory bowel diseases. The other one is Crohn s disease. Ulcerative colitis and
Ulcerative Colitis Introduction Ulcerative colitis is an inflammatory bowel disease. It is one of the 2 most common inflammatory bowel diseases. The other one is Crohn s disease. Ulcerative colitis and
Chapter 14 GASTROINTESTINAL IMPAIRMENT
 Chapter 14 GASTROINTESTINAL IMPAIRMENT Introduction This chapter provides criteria for assessing permanent impairment from entitled conditions of the gastrointestinal tract and the accessory organs of
Chapter 14 GASTROINTESTINAL IMPAIRMENT Introduction This chapter provides criteria for assessing permanent impairment from entitled conditions of the gastrointestinal tract and the accessory organs of
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
Index Note: Page numbers of article titles are in boldface type. A Abdominal pain, abdominal considerations in, 183 184 antiemetics in, 182 auscultation in, 170 C-reactive protein in, 174 175 character
The Digestive System
 The Digestive System Combining Forms Append/o appendix Hepat/o liver Appendic/o appendix Lingu/o tongue Col/o colon Myc/o fungus Dent/o teeth Odont/o teeth Enter/o intestine Or/o mouth Esophag/o esophagus
The Digestive System Combining Forms Append/o appendix Hepat/o liver Appendic/o appendix Lingu/o tongue Col/o colon Myc/o fungus Dent/o teeth Odont/o teeth Enter/o intestine Or/o mouth Esophag/o esophagus
The focus of this week s lab will be pathology of the gastrointestinal and hepatobiliary systems.
 GASTROINTESTINAL AND HEPATOBILIARY SYSTEMS The focus of this week s lab will be pathology of the gastrointestinal and hepatobiliary systems. GASTROINTESTINAL SYSTEM AND HEPATOBILIARY SYSTEM We will examine
GASTROINTESTINAL AND HEPATOBILIARY SYSTEMS The focus of this week s lab will be pathology of the gastrointestinal and hepatobiliary systems. GASTROINTESTINAL SYSTEM AND HEPATOBILIARY SYSTEM We will examine
Pediatric Gastroenterology Referral Guidelines
 Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure