Replaces: 04/13/17. / Formulated: 7/05 SYPHLIS
|
|
|
- Ami Richardson
- 6 years ago
- Views:
Transcription
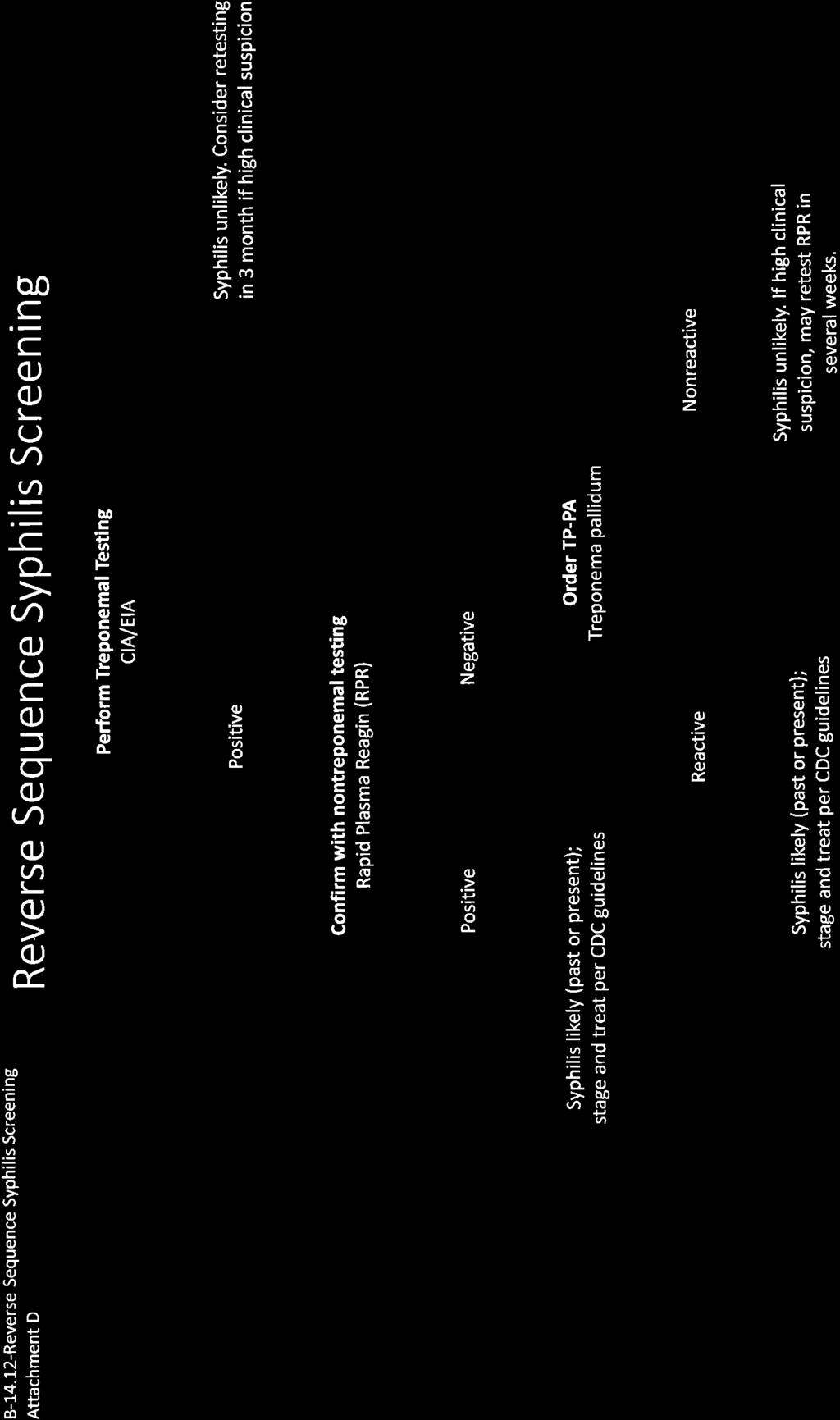
1 Effective Date: Replaces: Page 1 of 7 POLICY: The Texas Department of Criminal Justice (TDCJ) will identify, test, and manage all offenders with suspected or confirmed syphilis with a uniform testing and management program. PROCEDURES: I. Indications for Serologic Tests for Syphilis (STSRPR) A. Admission screening for all incoming offenders. B. Any offender exhibiting suspicious signs or symptoms of syphilis. C. Any offender with a history of sexual contact with a confirmed case of syphilis during incarceration OR prior to incarceration. D. Any current sexually transmitted infection (STI). II. Serologic Tests for Syphilis A. There are two types of tests for syphilis: nontreponemal antibody tests and treponemal antibody tests. 1. Nontreponemal tests include RPR (Rapid Plasma Reagin) and VDRL (Veneral Disease Research Laboratory) tests. RPR tests are reported as nonreactive or reactive at dilutions of 1:1, 1:2, 1:4, 1:8, etc. a. A four-fold (or two dilution) increase in titer (e.g., from 1:2 to 1:8) signifies new infection or treatment failure. b. These tests, in time, usually revert to negative after successful treatment of primary and secondary syphilis. A four-fold (or two dilution decrease in titer e.g., from 1:8 to 1:2) signifies successful treatment. c. These tests may remain reactive, however, at a varying low dilution (e.g., 1:1, 1:2) even after completion of successful therapy. This is called serofast serology. 2. Treponemal antibody tests include the TP-PA (Treponema pallidum Particle Agglutination), FTA-ABS (Fluorescent Treponemal Antibody Absorption Test), enzyme immunoassay (EIA), and chemiluminescence immunoassays (CIA). a. Treponemal tests detect antibody directed toward pathogenic members of the genus Treponema.
2 Effective Date: Replaces: Page 2 of 7 b. The TP-PA and the FTA-ABS usually do not revert to nonreactivity after successful treatment of syphilis. Once reactive, they almost always stay reactive and should not be repeated. Treponemal antibody tests are confirmatory tests and are inappropriate for screening. They are not quantitative and cannot be used for following response to therapy or progression of disease. III. Reverse Sequence Syphilis Screening A. Recent studies have demonstrated that reverse sequence syphilis screening (see attachment) may detect more cases of early or latent syphilis compared to the traditional screening algorithm. As such, many laboratories have adopted this method of testing. This method begins with a treponemal assay, EIACIA, due to the high sensitivity of this test. It must be noted that this is only a screening test and the diagnosis of syphilis may not be based on this result alone. All positivereactive results must be reflexly tested with a nontreponemal test (i.e., RPR). For negative EIACIA, clinicians may retest in three months if there is a high index of suspicion for syphilis. B. If the RPR is positivereactive, the algorithm stops here, and past or present syphilis is likely. If the TP-PA is positivereactive, syphilis either past or present is likely. Continue to section IV of this policy. If the TP-PA is negativenonreactive, syphilis is unlikely. However, clinical judgement should be used and if a high index of suspicion remains for syphilis, the RPR may be repeated in several weeks not to exceed 3 months. C. If the TP-PA is positivereactive, syphilis either past or present is likely. Continue to section IV of this policy. If the TP-PA is negativenonreactive, syphilis is unlikely. However, clinical judgement should be used and if a high index of suspicion remains for syphilis, the RPR may be repeated in several weeks not to exceed 3 months. IV. Interpretation and Follow-up of Nontreponemal (i.e., RPR) Serologic Tests for Syphilis A. Primary syphilis nontreponemal tests usually reach a titer of at least 1:4. During the first few days of primary syphilis, i.e., onset of primary lesion (< 7days), the RPR andor TP-PA may be nonreactive. In this scenario, the case should be confirmed through the use of dark-field microscopy. If this procedure cannot be performed, i.e., the equipment is not available, the offender should be presumptively treated and the RPRTP-PA should be repeated in one week. Following treatment, RPR titer may
3 Effective Date: Replaces: Page 3 of 7 rise slightly but usually reverts to nonreactive within six to 12 months following treatment. B. Secondary or early latent syphilis titers are usually 1:32 or higher. After successful treatment, the titer usually reverts to nonreactive within 18 months. Seventy five percent or more will be nonreactive within two years. C. Latent syphilis: early latent, or syphilis of less than one year duration, and late latent syphilis of greater than one year duration, are asymptomatic. After successful treatment of latent syphilis, titers usually decrease at least four-fold (e.g., from 1:32 to 1:8). A stable or rising titer during the two years of observation after treatment suggests treatment failure, re-infection, or a diagnostic error. D. Symptomatic late syphilis (i.e., neurosyphilis, cardiovascular syphilis or gummatous disease) should be considered in anyone with longstanding untreated syphilis. E. In any treatment situation, failure of the highest titer to decrease four-fold within one year suggests a treatment failure and warrants re-evaluation of the case and retreatment. F. Although many patients have a nonreactive nontreponemal test within two years after successful treatment, in some, the titer may remain persistently positive at a low level (but with a four-fold fall from the highest titer). This condition is called serofast. Serofast titers are generally 1:4 or lower. Although higher serofast titers may occur, the possibility of persistent infection or re-infection should be carefully considered before dismissing a result as serofast. A diagnosis of serofast must not be made unless the patient has a documented history of previous treatment with a documented four-fold or greater drop in titer after treatment. G. A spinal fluid examination should be considered for patients with any one of the following criteria: Neurologic or ophthalmic signs or symptoms Other evidence of tertiary disease (aortitis, gumma, iritis) Treatment failure HIV infection with late latent syphilis or syphilis of unknown duration Non-penicillin therapy planned, unless duration of infection is known to be < one year. If a CSF examination is performed and the results show abnormalities consistent with CNS syphilis, the patient should be treated for neurosyphilis.
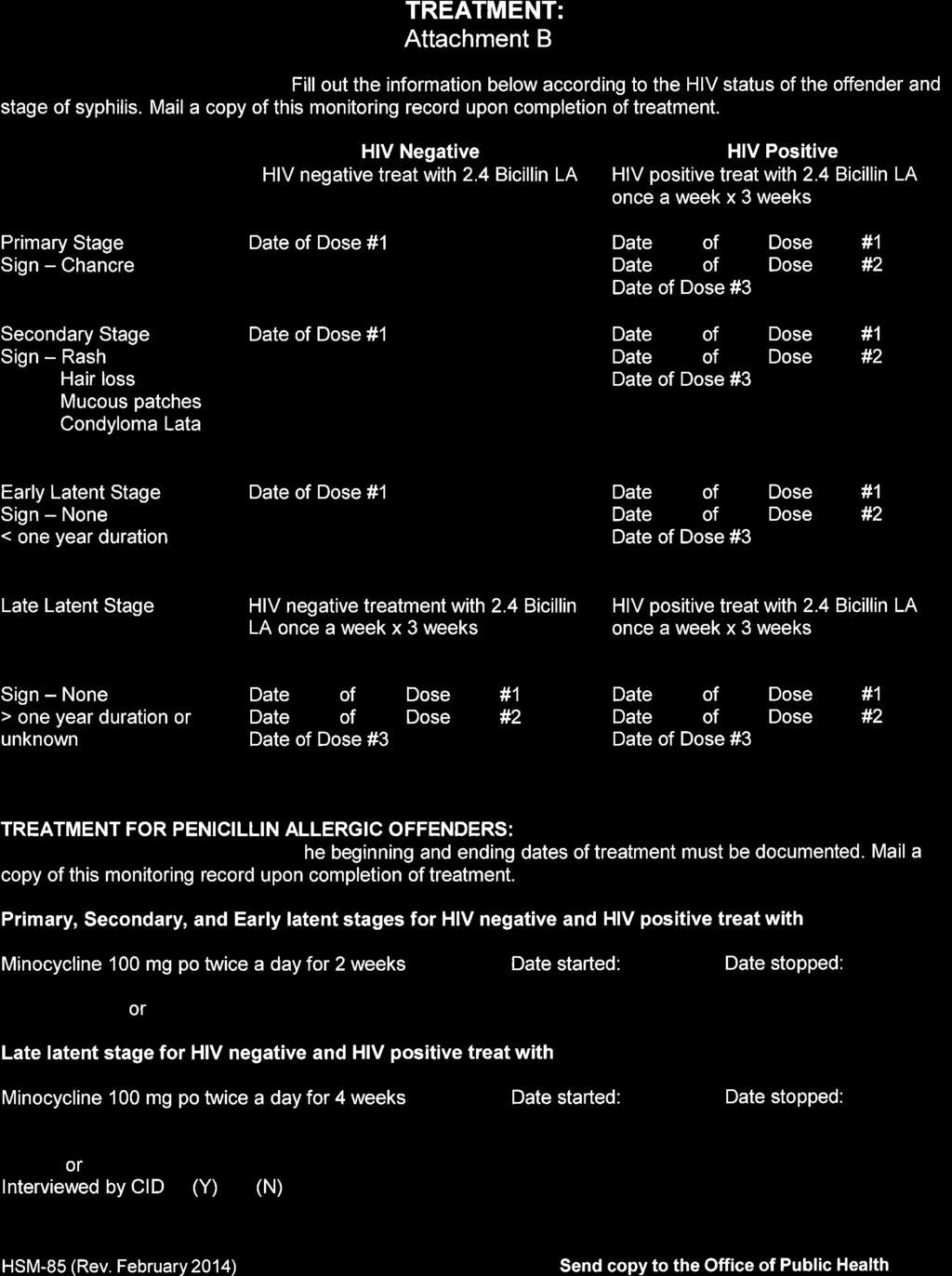
4 Effective Date: Replaces: Page 4 of 7 H. All patients with syphilis or a history of syphilis must be offered counseling and testing for HIV infection. I. Syphilis testing in patients with HIV infection. V. Treatment When clinical findings suggest syphilis, but serologic tests are negative, other tests should be used to determine if syphilis is present. These tests include dark-field microscopy and direct fluorescent antibody for T. pallidum (DFA-TP), staining of lesion exudate or examination of biopsy tissue using DFA-TP or Steiner stain. Patients who have untreated syphilis in any stage must be treated. Treatment should follow the current guidelines promulgated by the Centers for Disease Control and Prevention (CDC). The guidelines for syphilis treatment are: A. Primary, secondary, or early latent syphilis (less than one year s duration) in HIV negative individuals: Benzathine penicillin G (Bicillin L-A), 2.4 million units IM in one dose. B. Late latent syphilis (indeterminate length or of more than one year s duration), or any HIV positive individual regardless of stage: Bicillin L-A 7.2 million units total, administered as 2.4 million units IM given one week apart for three consecutive weeks. C. Neurosyphilis and other forms of tertiary syphilis. Inpatient therapy recommended; see STD Treatment Guidelines for regimen or contact Office of Public Health for guidance. D. See STD Treatment Guidelines for special considerations and alternative regimens (including treatment of pregnant and penicillin-allergic persons). Contact the Office of Public Health for guidance in the management of patients with special consideration.
5 Effective Date: Replaces: Page 5 of 7 Summary of Recommended Treatment and Follow-Up+ Stage Treatment Treatment Follow-Up Serology Discharge Primary & Secondary HIV negative: Bicillin L-A 2.4 mil units HIV positive: Bicillin L-A 2.4 mil units a week x 3 weeks (7.2 mil units total) 6 and 12 months After a four-fold decline in titers 3, 6, 9, 12, and 24 months RPR- negative contact of Primary, Secondary or Early Latent case1 Bicillin L-A 2.4 million units None At end of treatment Latent, a) Early (<one year duration) HIV negative: Bicillin L-A 2.4 million units HIV positive: Bicillin L-A 2.4 mil units a week x 3 weeks (7.2 mil units total) HIV negative: 6, 12 and 24 Months HIV positive: 3, 6, 9, 12, 18, and 24 months After a four-fold decline in titers b) Late ( 1 year, or unknown duration) b) Bicillin L-A 2.4 mil units a week x 3 weeks (7.2 mil units total) Serological follow-up post treatment must occur according to the schedule under the Serology column, at a minimum. Patients may be discharged from follow-up at the end of the follow-up period if they have had a sustained four-fold or greater drop in titer.
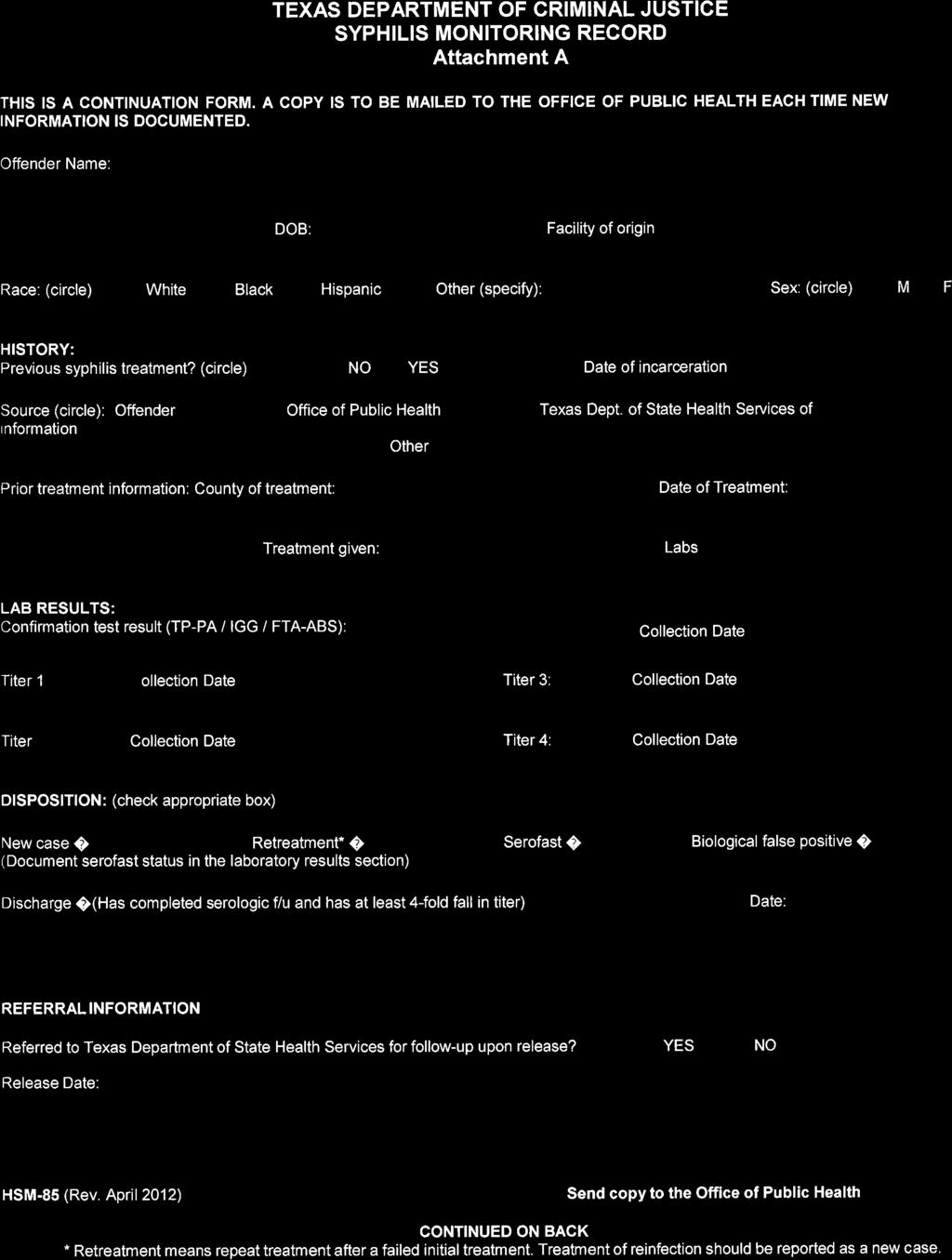
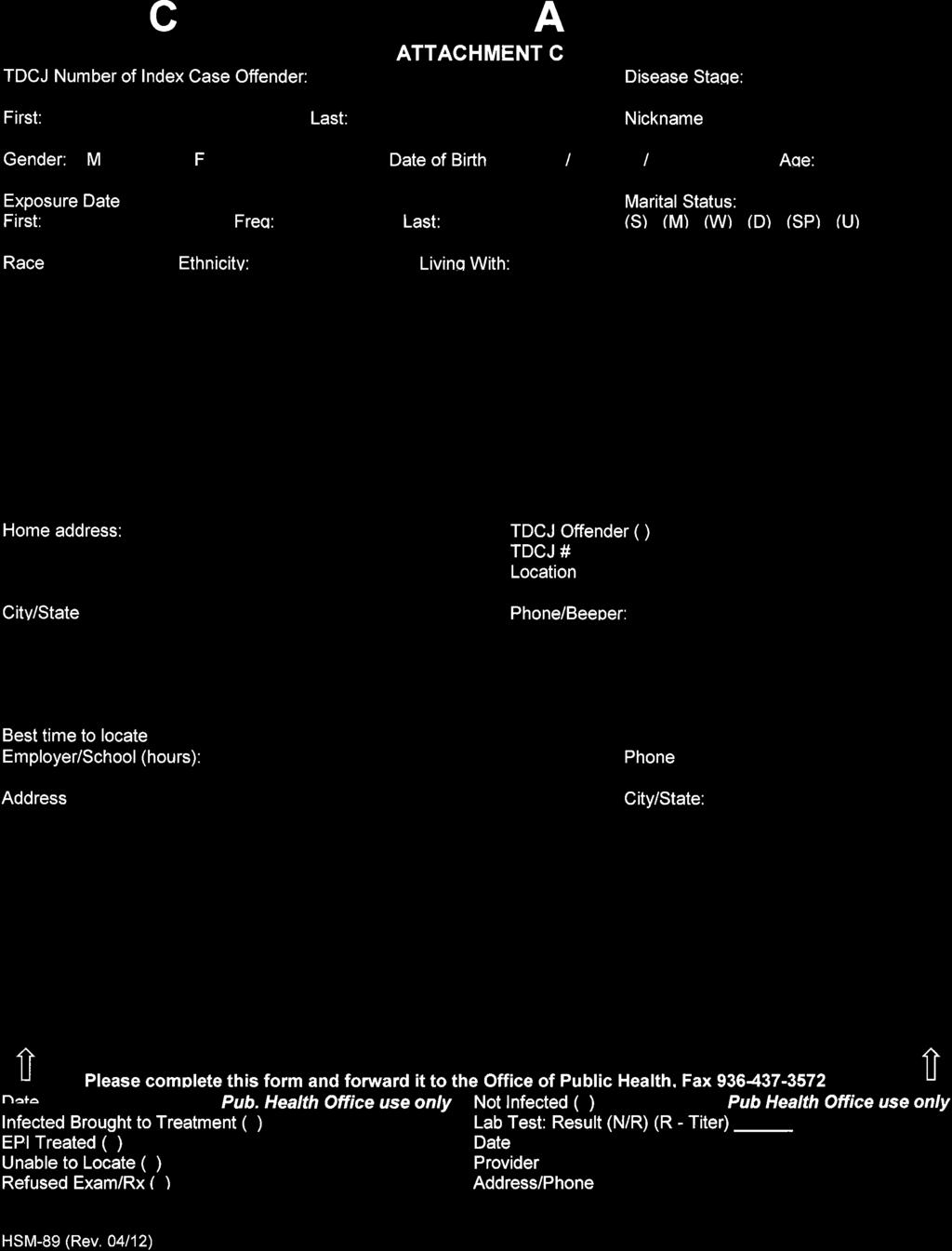
6 Effective Date: Replaces: Page 6 of 7 VI. Contacts A. All offenders with a case of syphilis meeting the criteria referenced in Section III: A D, Interpretation and Follow-Up of serologic Tests for Syphilis are to be interviewed by the Infection Control Nurse (ICN). This interview will include risk reductiondisease comprehension counseling and contact elicitation. All interview information is to be recorded on the appropriate forms: HSM-85 (Syphilis Monitoring record) and HSM-89 (Contact Information Guide). B. Contacts of all reported cases of syphilis are to be documented on the Contact Information Guide, HSM-89 (Attachment B). This sheet(s) is to be forwarded, in a sealed envelope stamped confidential to the Office of Public Health in conjunction with the HSM-85, Syphilis Monitoring Record. The Contact Information Guide is not to be placed in the medical record of the offender. 1. The critical period for contact elicitation for early syphilis cases is as follows: a) Primary 90 days prior to the onset of symptoms andor reactive RPRTP- PA; b) Secondary six months prior to the onset of symptoms andor reactive RPRTP-PA; c) Early Latent one year prior to the reactive RPRTP-PA; d) Late LatentSyphilis of Unknown Duration one year prior to the reactive RPRTP-PA. 2. Contact elicitation should include contacts within TDCJ as well as contacts prior to entry into TDCJ during the critical period in which the history suggests the patient was infectious. 3. TDCJ offenders identified as contacts within the time frames listed in V.B.1, above, must be tested for syphilis. 4. Contacts of primary, secondary and early latent syphilis cases whose last exposure was within 90 days prior to testing should be given prophylactic treatment as indicated in the table above, even if the RPR is nonreactive. 5. Contacts identified according to V.B.1, above, must be treated for syphilis if their RPR is reactive and they have not already received treatment, even if they have no other signs or symptoms of syphilis. In general they should receive the treatment for early latent syphilis, as the maximum time frame for contact elicitation is one year, indicating their exposure was within the past year. C. State and Local Health Departments have legal authority to investigate cases of infectious disease. Unit medical staff may be contacted by StateLocal Health Department staff
7 Effective Date: Replaces: Page 7 of 7 (Disease Intervention Specialists, or DIS workers) to schedule interviews with o f f e n d e r s diagnosed with syphilis. U n i t s t a f f s h a l l r e f e r S t a t e L o c a l H e a l t h D e p a r t m e n t s t a f f t o t h e T D C J H e a l t h S e r v i c e s D i v i s i o n, O f f i c e o f P u b l i c H e a l t h ( O P H ) f o r s c h e d u l i n g o f t h e s e v i s i t s. I n f o r m a t i o n r e l e a s e d f o r t h e p u r p o s e of these i n v e s t i ga t i o n s w i l l a l s o b e r e l e a s e d t h r o u g h O P H. Any concerns related to this activity should be directed to TDCJ Health Services Division, Office of Public Health Director. VII. Reporting A. A HSM-85, Syphilis Monitoring Record (Attachment A), must be initiated on all persons who have a reactive RPR. Diagnosis must include the disease stage (Primary, Secondary, Early Latent, Late Latent, etc.). A copy must be sent to the Office of Public Health. B. Initial positive RPR titers of 1:16 or greater must be reported to the Office of Public Health on the day the results are received by the unit, or the next working day if received outside of regular work hours. In addition, all cases of primary or secondary syphilis must be reported to the Office of Public Health the same day the diagnosis is made. Reports may be faxed to (secure fax) or sent by webmail. C. Initial positive RPR titers less than 1:16 must be reported to the Office of Public Health within seven days of receipt. Reports may be faxed or sent by EMR . D. The date and dosage of each dose of medication must be reported within seven days of completion of treatment, and each follow-up RPR must be reported to the Office of Public Health within seven days. The reports may be submitted to the Office of Public Health by webmail or EMR giving the offender name and TDCJ number, date, and dosage of medication administered andor RPR titer (depending on what information is being updated) or by mailing or faxing an updated HSM-85. References: Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, MMWR JUNE 5, 2015, Vol. 64, No 3. Centers for Disease Control and Prevention. Discordant Results from Reverse Sequence Syphilis Screening. MMWR February 11, 2011, Vol. 60, No. 5. The CDC Guidelines may change from time to time. For the latest version, check the CDC web site:
8
9
10
11
Syphilis Treatment Protocol
 STD, HIV, AND TB SECTION Syphilis Treatment Protocol CLINICAL GUIDANCE FOR PRIMARY AND SECONDARY SYPHILIS AND LATENT SYPHILIS www.lekarzol.com (4/2016) Page 1 of 8 Table of Contents Description... 3 Stages
STD, HIV, AND TB SECTION Syphilis Treatment Protocol CLINICAL GUIDANCE FOR PRIMARY AND SECONDARY SYPHILIS AND LATENT SYPHILIS www.lekarzol.com (4/2016) Page 1 of 8 Table of Contents Description... 3 Stages
Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis
 Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis Guidance for Medical Providers and Laboratories in California These guidelines were developed by the California Department of Public
Use of Treponemal Immunoassays for Screening and Diagnosis of Syphilis Guidance for Medical Providers and Laboratories in California These guidelines were developed by the California Department of Public
Syphilis Technical Instructions for Civil Surgeons
 National Center for Emerging and Zoonotic Infectious Diseases Syphilis Technical Instructions for Civil Surgeons Joanna J. Regan, MD, MPH, FAAP Medical Officer Medical Assessment and Policy Team Immigrant,
National Center for Emerging and Zoonotic Infectious Diseases Syphilis Technical Instructions for Civil Surgeons Joanna J. Regan, MD, MPH, FAAP Medical Officer Medical Assessment and Policy Team Immigrant,
Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections?
 Abstract no. WEPE 494 Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections? G.Chrysos 1, D.Karageorgopoulos
Abstract no. WEPE 494 Serological screening for syphilis in HIV-infected individuals: is a non-treponemal test adequate in the era of increasing of new syphilis infections? G.Chrysos 1, D.Karageorgopoulos
SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM
 IMMEDIATE NOTIFICATION STD PROGRAM") SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM Event Name: Event Time Period: Clinical Description (CDC 2014) Syphilis 180 days Syphilis is a complex sexually transmitted disease that
SYPHILIS (Treponema pallidum) IMMEDIATE NOTIFICATION STD PROGRAM Event Name: Event Time Period: Clinical Description (CDC 2014) Syphilis 180 days Syphilis is a complex sexually transmitted disease that
Sexually Transmitted Diseases Treatment Guidelines, 2015
 Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers
Morbidity and Mortality Weekly Report Recommendations and Reports / Vol. 64 / No. 3 June 5, 2015 Sexually Transmitted Diseases Treatment Guidelines, 2015 U.S. Department of Health and Human Services Centers
Direct Comparison of the Traditional and Reverse Syphilis Screening Algorithms
 JCM Accepts, published online ahead of print on 16 November 2011 J. Clin. Microbiol. doi:10.1128/jcm.05636-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 16 November 2011 J. Clin. Microbiol. doi:10.1128/jcm.05636-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services.
 Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services Disclosures: None 1 PRIMARY Fitzgerald TJ, Cleveland P, Johnson RC et al: Scanning
Lisa Villarroel, MD MPH Medical Director, Division of Public Health Preparedness Arizona Department of Health Services Disclosures: None 1 PRIMARY Fitzgerald TJ, Cleveland P, Johnson RC et al: Scanning
Management of Syphilis in Patients with HIV
 Management of Syphilis in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS
Management of Syphilis in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the Guideline Increase the numbers of NYS
Learning Objectives. Syphilis. Lessons. Epidemiology: Disease in the U.S. Syphilis Definition. Transmission. Treponema pallidum
 Learning Objectives Syphilis Treponema pallidum 1 Upon completion of this content, the learner will be able to 1. Describe the epidemiology of syphilis in the U.S. 2. Describe the pathogenesis of T. pallidum.
Learning Objectives Syphilis Treponema pallidum 1 Upon completion of this content, the learner will be able to 1. Describe the epidemiology of syphilis in the U.S. 2. Describe the pathogenesis of T. pallidum.
Sexually Transmitted Disease Treatment Tables
 Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory
 CM, SM Montana Public Health Laboratory") Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory Describe the challenges in syphilis diagnostics Present two testing algorithms Non-treponemal test as initial screen Treponemal
Susanne Norris Zanto, MPH, MLS (ASCP) CM, SM Montana Public Health Laboratory Describe the challenges in syphilis diagnostics Present two testing algorithms Non-treponemal test as initial screen Treponemal
9/9/2015. Began to see a shift in 2012 Early syphilis cases more than doubled from year before
 George Walton, MPH, CPH, MLS(ASCP) CM STD Program Manager Bureau of HIV, STD, and Hepatitis September 15, 2015 1 1) Discuss the changing epidemiology of syphilis in Iowa; 2) Explore key populations affected
George Walton, MPH, CPH, MLS(ASCP) CM STD Program Manager Bureau of HIV, STD, and Hepatitis September 15, 2015 1 1) Discuss the changing epidemiology of syphilis in Iowa; 2) Explore key populations affected
SYPHILIS. The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS
 SYPHILIS The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS Learning Objectives At the end of this presentation, the participants will be able to 1. Describe the epidemiology of syphilis in the United
SYPHILIS The Great Pretender K. Amen Eguakun, MSN, APRN, AAHIVS Learning Objectives At the end of this presentation, the participants will be able to 1. Describe the epidemiology of syphilis in the United
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046)
") Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, San Diego, CA February
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, San Diego, CA February
WHAT DO U KNOW ABOUT STIS?
 WHAT DO U KNOW ABOUT STIS? Rattiya Techakajornkeart MD. Bangrak STIs Cluster, Bureau of AIDS, TB and STIs, Department of Disease Control, MOPH, Thailand SEXUALLY TRANSMITTED INFECTIONS? STIs Infections
WHAT DO U KNOW ABOUT STIS? Rattiya Techakajornkeart MD. Bangrak STIs Cluster, Bureau of AIDS, TB and STIs, Department of Disease Control, MOPH, Thailand SEXUALLY TRANSMITTED INFECTIONS? STIs Infections
Public/Private Partnerships: Intervening in the Spread of Syphilis
 Public/Private Partnerships: Intervening in the Spread of Diana Torres-Burgos MD, MPH Gerard Castaneda, BSN Alana Thomas, BS STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline overview Stages
Public/Private Partnerships: Intervening in the Spread of Diana Torres-Burgos MD, MPH Gerard Castaneda, BSN Alana Thomas, BS STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline overview Stages
10/19/2012. Serologic Testing for Syphilis. Disclosures. Comparison of the Traditional and Reverse Screening Algorithms. Outline.
 Serologic Testing for Syphilis Comparison of the Traditional and Reverse Screening Algorithms Disclosures Elli S. Theel, Ph.D. Director, Infectious Diseases Serology Laboratory Assistant Professor of Laboratory
Serologic Testing for Syphilis Comparison of the Traditional and Reverse Screening Algorithms Disclosures Elli S. Theel, Ph.D. Director, Infectious Diseases Serology Laboratory Assistant Professor of Laboratory
Syphilis Testing in Northern California Kaiser
 Syphilis Testing in Northern California Kaiser Jen Shieh, MS, CLS Test Development Scientist Kaiser Permanente TPMG Regional Laboratory Microbiology Department Kaiser Permanente 3.3 million members 22
Syphilis Testing in Northern California Kaiser Jen Shieh, MS, CLS Test Development Scientist Kaiser Permanente TPMG Regional Laboratory Microbiology Department Kaiser Permanente 3.3 million members 22
4/18/2018. Syphilis Testing. Disclosure. Learner Objectives. Outline. Employee and stockholder of Bio-Rad Laboratories, Inc.
 Disclosure Employee and stockholder of Bio-Rad Laboratories, Inc. Unraveling the Complexities of Syphilis Testing Maria Crisostomo, April 30 & May 1, 2018 2 Learner Objectives Syphilis Testing Upon completion
Disclosure Employee and stockholder of Bio-Rad Laboratories, Inc. Unraveling the Complexities of Syphilis Testing Maria Crisostomo, April 30 & May 1, 2018 2 Learner Objectives Syphilis Testing Upon completion
Sexually transmitted infections (in women)
") Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
To view an archived recording of this presentation please click the following link:
 To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p16lj8z0qm3/ Please scroll down this file to view a copy of the slides from the session.
To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p16lj8z0qm3/ Please scroll down this file to view a copy of the slides from the session.
Guidance for Industry
 Guidance for Industry Revised Recommendations for Donor and Product Management Based on Screening Tests for Syphilis DRAFT GUIDANCE This document is being distributed for comment purposes only. Submit
Guidance for Industry Revised Recommendations for Donor and Product Management Based on Screening Tests for Syphilis DRAFT GUIDANCE This document is being distributed for comment purposes only. Submit
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES
 ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
The Use of a Rapid Syphilis Test with Specimens from an HIV Cluster Investigation in Rural West Virginia
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention The Use of a Rapid Syphilis Test with Specimens from an HIV Cluster Investigation in Rural West Virginia Lara E. Pereira, Ph.D. Centers
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention The Use of a Rapid Syphilis Test with Specimens from an HIV Cluster Investigation in Rural West Virginia Lara E. Pereira, Ph.D. Centers
Didactic Series. STD Screening & Management: Syphilis. Christian B. Ramers, MD, MPH
 Didactic Series STD Screening & Management: Syphilis Christian B. Ramers, MD, MPH Assistant Medical Director Family Health Centers of San Diego Ciaccio Memorial Clinic 3/26/15 ACCREDITATION STATEMENT:
Didactic Series STD Screening & Management: Syphilis Christian B. Ramers, MD, MPH Assistant Medical Director Family Health Centers of San Diego Ciaccio Memorial Clinic 3/26/15 ACCREDITATION STATEMENT:
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046)
") Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, Orlando, FL March 4, 2017
Sex, Sores, Science, and Surveillance: Syphilis in the 21 st Century (U046) Kenneth A. Katz, MD, MSc, MSCE Dermatologist, Kaiser Permanente, San Francisco, CA AAD Annual Meeting, Orlando, FL March 4, 2017
Nothing to disclose.
 Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
2/13/ Graphic photographs or cartoons used during this presentation might be offensive to some; for this I apologize in advance.
 Leon Bullard, MD, MA Medical Consultant, DHEC, DADE The 23 rd Annual APRN Conference Charleston, SC February 24, 2017 1. Provide a brief (very) review of the syphilis story. 2. Define and discuss the stages
Leon Bullard, MD, MA Medical Consultant, DHEC, DADE The 23 rd Annual APRN Conference Charleston, SC February 24, 2017 1. Provide a brief (very) review of the syphilis story. 2. Define and discuss the stages
January Dear Physician:
 Richard F. Daines, M.D. Commissioner Wendy E. Saunders Executive Deputy Commissioner January 2009 Dear Physician: The purpose of this letter is to bring your attention to the significant increase in reported
Richard F. Daines, M.D. Commissioner Wendy E. Saunders Executive Deputy Commissioner January 2009 Dear Physician: The purpose of this letter is to bring your attention to the significant increase in reported
Annals of Internal Medicine. 1991;114:
 Serologic Response to Treatment of Infectious Syphilis Barbara Romanowski, MD; Ruth Sutherland, DPH, RN; Gordon H. Fick, PhD; Debbie Mooney, BSc; and Edgar J. Love, MD, PhD Objective: To evaluate the serologic
Serologic Response to Treatment of Infectious Syphilis Barbara Romanowski, MD; Ruth Sutherland, DPH, RN; Gordon H. Fick, PhD; Debbie Mooney, BSc; and Edgar J. Love, MD, PhD Objective: To evaluate the serologic
Syphilis Update: New Presentations of an Old Disease
 Syphilis Update: New Presentations of an Old Disease Bradley Stoner, MD, PhD Washington University in St. Louis Disclosure: Bradley Stoner, MD, PhD STDs in the United States Where do we stand right now?
Syphilis Update: New Presentations of an Old Disease Bradley Stoner, MD, PhD Washington University in St. Louis Disclosure: Bradley Stoner, MD, PhD STDs in the United States Where do we stand right now?
Performance Characteristics of the Reverse Syphilis Screening Algorithm in a Population With a Moderately High Prevalence of Syphilis
 Performance Characteristics of the Reverse Syphilis Screening Algorithm in a Population With a Moderately High Prevalence of Syphilis Angela R. Rourk, Frederick S. Nolte, PhD, and Christine M. Litwin,
Performance Characteristics of the Reverse Syphilis Screening Algorithm in a Population With a Moderately High Prevalence of Syphilis Angela R. Rourk, Frederick S. Nolte, PhD, and Christine M. Litwin,
Sexually transmitted infections (in women)
") Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Validation of a New Testing Algorithm for Syphilis in Trinidad & Tobago
 Validation of a New Testing Algorithm for Syphilis in Trinidad & Tobago R. Dass, A. Sebro, J. Edwards Ministry of Health, Trinidad and Tobago rianna.dass@hotmail.com, asebro@yahoo.com, jeffreye2000@gmail.com
Validation of a New Testing Algorithm for Syphilis in Trinidad & Tobago R. Dass, A. Sebro, J. Edwards Ministry of Health, Trinidad and Tobago rianna.dass@hotmail.com, asebro@yahoo.com, jeffreye2000@gmail.com
Syphilis among MSM: Clinical Care and Public Health Reporting
 Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences Syphilis among MSM: Clinical Care and Public Health Reporting Kevin Ard, MD, MPH, Medical Director, National
Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences Syphilis among MSM: Clinical Care and Public Health Reporting Kevin Ard, MD, MPH, Medical Director, National
5/1/2017. Sexually Transmitted Diseases Burning Questions
 Sexually Transmitted Diseases Burning Questions Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles Los Angeles, California FORMATTED: 04-03-17 Financial
Sexually Transmitted Diseases Burning Questions Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles Los Angeles, California FORMATTED: 04-03-17 Financial
The Great Imitator Revealed: Syphilis
 The Great Imitator Revealed: Syphilis Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles David Geffen School of Medicine Los Angeles, California Learning
The Great Imitator Revealed: Syphilis Jeffrey D. Klausner, MD, MPH Professor of Medicine and Public Health University of California Los Angeles David Geffen School of Medicine Los Angeles, California Learning
INFECTIOUS SYPHILIS NOTIFICATION FORM
 INFECTIOUS SYPHILIS NOTIFICATION FORM This is a Schedule 1, Section C disease notifiable to the Medical Officer of Health under Sections 74 and 74AA of the Health Act 1956 using non-identifiable data.
INFECTIOUS SYPHILIS NOTIFICATION FORM This is a Schedule 1, Section C disease notifiable to the Medical Officer of Health under Sections 74 and 74AA of the Health Act 1956 using non-identifiable data.
Discordant Results from Reverse Sequence Syphilis Screening Five Laboratories, United States,
 Please note: An erratum has been published for this issue. To view the erratum, please click here. Morbidity and Mortality Weekly Report Weekly / Vol. 60 / No. 5 February 11, 2011 Discordant Results from
Please note: An erratum has been published for this issue. To view the erratum, please click here. Morbidity and Mortality Weekly Report Weekly / Vol. 60 / No. 5 February 11, 2011 Discordant Results from
SYPHILIS (REPORTABLE)
") SYPHILIS (REPORTABLE) PREAMBLE In BC, the diagnosis of syphilis is determined by the BCCDC Provincial STI/HIV Clinic physician directly or in coordination with the*physician or nurse practitioner (NP)
SYPHILIS (REPORTABLE) PREAMBLE In BC, the diagnosis of syphilis is determined by the BCCDC Provincial STI/HIV Clinic physician directly or in coordination with the*physician or nurse practitioner (NP)
Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance. Syphilis in Men
 Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance Syphilis in Men Kenneth A. Katz, MD, MSc, MSCE Kaiser Permanente, San Francisco, CA AAD Annual Meeting Washington, D.C. March 2, 2019
Syphilis in the 21 st Century: Sex, Sores, Science, and Surveillance Syphilis in Men Kenneth A. Katz, MD, MSc, MSCE Kaiser Permanente, San Francisco, CA AAD Annual Meeting Washington, D.C. March 2, 2019
Learning Objectives. Epidemiology 5/3/2013. Treponema pallidum Diagnosis, Treatment and Prevention. Anne Rompalo, MD, ScM Professor of Medicine
 Treponema pallidum Diagnosis, Treatment and Prevention Anne Rompalo, MD, ScM Professor of Medicine Learning Objectives Describe the epidemiology of syphilis in the U.S.Describe the pathogenesis of Treponema
Treponema pallidum Diagnosis, Treatment and Prevention Anne Rompalo, MD, ScM Professor of Medicine Learning Objectives Describe the epidemiology of syphilis in the U.S.Describe the pathogenesis of Treponema
Background. Restricted Siemens Healthcare GmbH, >1 year Late latent syphilis. Restricted Siemens Healthcare GmbH, 2017
 Background Nonneutralizing The Evolution of Syphilis Testing: Clinical Benefits of a Reverse Screening Algorithm Katherine Soreng PhD Lafond RE, et al. Clin Microbiol Rev. 06;19(1):29 49. Disease course:
Background Nonneutralizing The Evolution of Syphilis Testing: Clinical Benefits of a Reverse Screening Algorithm Katherine Soreng PhD Lafond RE, et al. Clin Microbiol Rev. 06;19(1):29 49. Disease course:
6/11/15. BACTERIAL STDs IN A POST- HIV WORLD. Learning Objectives. How big a problem are STIs in the U.S.?
 BACTERIAL STDs IN A POST- HIV WORLD Tracey Graney, PhD, MT(ASCP) Monroe Community College Learning Objectives Describe the epidemiology and incidence of bacterial STDs in the U.S. Describe current detection
BACTERIAL STDs IN A POST- HIV WORLD Tracey Graney, PhD, MT(ASCP) Monroe Community College Learning Objectives Describe the epidemiology and incidence of bacterial STDs in the U.S. Describe current detection
SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria
 Dr D. Tenea Department of Dermatology University of Pretoria") SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria INTRODUCTION Venereal disease = old term STD infections transmitted by sexual contact Sexually
SEXUALLY TRANSMITED DISEASES SYPHILIS ( LUES ) Dr D. Tenea Department of Dermatology University of Pretoria INTRODUCTION Venereal disease = old term STD infections transmitted by sexual contact Sexually
NIH Public Access Author Manuscript Clin Infect Dis. Author manuscript; available in PMC 2009 October 1.
 NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
CAP Laboratory Improvement Programs. Prevalence of Traditional and Reverse-Algorithm Syphilis Screening in Laboratory Practice
 CAP Laboratory Improvement Programs Prevalence of Traditional and Reverse-Algorithm Syphilis Screening in Laboratory Practice A Survey of Participants in the College of American Pathologists Syphilis Serology
CAP Laboratory Improvement Programs Prevalence of Traditional and Reverse-Algorithm Syphilis Screening in Laboratory Practice A Survey of Participants in the College of American Pathologists Syphilis Serology
Spirochetes. Treponema pallidum
 Spirochetes Treponema pallidum Dr. Hala Al Daghistani - Spirochetes are a large, heterogeneous group of spiral, motile bacteria. - One family Spirochaetaceae consists of two genera whose members are human
Spirochetes Treponema pallidum Dr. Hala Al Daghistani - Spirochetes are a large, heterogeneous group of spiral, motile bacteria. - One family Spirochaetaceae consists of two genera whose members are human
STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention
 STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention Palliative Care Conference Faculty Development Conference August 13, 2015 Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS
STDs in HIV Clinical Care: New Guidelines on Treatment and Prevention Palliative Care Conference Faculty Development Conference August 13, 2015 Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS
Emerging Issues in STDs and Resistance
 Emerging Issues in STDs and Resistance Toye H. Brewer, MD Asst. Professor of Clinical Medicine University of Miami School of Medicine Co-Director- Fogarty International Training Program Outline Syphilis-
Emerging Issues in STDs and Resistance Toye H. Brewer, MD Asst. Professor of Clinical Medicine University of Miami School of Medicine Co-Director- Fogarty International Training Program Outline Syphilis-
Neurosyphilis as an Emerging Feature in the HIV Setting. Christina M. Marra, MD University of Washington Seattle, WA, USA
 Neurosyphilis as an Emerging Feature in the HIV Setting Christina M. Marra, MD University of Washington Seattle, WA, USA Syphilis in the Developing World Region 1995 1999 Sub-Saharan 3,530,000 3,828,000
Neurosyphilis as an Emerging Feature in the HIV Setting Christina M. Marra, MD University of Washington Seattle, WA, USA Syphilis in the Developing World Region 1995 1999 Sub-Saharan 3,530,000 3,828,000
STDs and Hepatitis C
 STDs and Hepatitis C Catherine S. O Neal, MD Assistant Professor of Clinical Medicine, Infectious Diseases Louisiana State University Health Sciences Center March 3, 2018 Objectives Review patient risk
STDs and Hepatitis C Catherine S. O Neal, MD Assistant Professor of Clinical Medicine, Infectious Diseases Louisiana State University Health Sciences Center March 3, 2018 Objectives Review patient risk
Syphilis Update. roadmap
 AND Nurse Practitioners!!! AND Physician Assistants!!! Oliver Bacon, MD, MPH Physician, SF City Clinic Disease Prevention and Control Branch Population Health Division roadmap 1. Syphilis: diagnosis and
AND Nurse Practitioners!!! AND Physician Assistants!!! Oliver Bacon, MD, MPH Physician, SF City Clinic Disease Prevention and Control Branch Population Health Division roadmap 1. Syphilis: diagnosis and
Revisions to the Syphilis Surveillance Case Definitions, 2018
 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Revisions to the Syphilis Surveillance Case Definitions, 2018 Sarah Kidd, MD, MPH Medical Epidemiologist Division of STD Prevention
National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention Revisions to the Syphilis Surveillance Case Definitions, 2018 Sarah Kidd, MD, MPH Medical Epidemiologist Division of STD Prevention
26. Screening for Syphilis
 26. Screening for Syphilis RECOMMENDATION Routine serologic screening for syphilis is recommended for all pregnant women and for persons at increased risk of infection (see Clinical Inter - vention). See
26. Screening for Syphilis RECOMMENDATION Routine serologic screening for syphilis is recommended for all pregnant women and for persons at increased risk of infection (see Clinical Inter - vention). See
February 3, Division of Dockets Management (HFA 305) Food and Drug Administration 5630 Fishers Lane, Rm Rockville, MD 20852
 Food and Drug Administration 5630 Fishers Lane, Rm Rockville, MD 20852") February 3, 2014 Division of Dockets Management (HFA 305) Food and Drug Administration 5630 Fishers Lane, Rm. 1061 Rockville, MD 20852 ATTN: Leslie Kux, Assistant Commissioner for Policy Ref: [Docket No.
February 3, 2014 Division of Dockets Management (HFA 305) Food and Drug Administration 5630 Fishers Lane, Rm. 1061 Rockville, MD 20852 ATTN: Leslie Kux, Assistant Commissioner for Policy Ref: [Docket No.
Edward W. Hook, III, M.D.
 Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
Clinical Practice Objectives
 STD Essentials for the Busy Clinician Susan S. Philip, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Director, STD Prevention and Control Services San Francisco Department of Public
STD Essentials for the Busy Clinician Susan S. Philip, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Director, STD Prevention and Control Services San Francisco Department of Public
Syphilis Update. Dr. Bauer has no disclosures. STD Clinical Update San Diego California Prevention Training Center October 11, 2018
 Heidi M. Bauer, MD MS MPH Chief, STD Control Branch, California Department of Public Health California STD/HIV Prevention Training Center San Diego Dr. Bauer has no disclosures 1 Learning Objectives 1.
Heidi M. Bauer, MD MS MPH Chief, STD Control Branch, California Department of Public Health California STD/HIV Prevention Training Center San Diego Dr. Bauer has no disclosures 1 Learning Objectives 1.
STD Essentials for the Busy Clinician. Stephanie E. Cohen, MD, MPH
 STD Essentials for the Busy Clinician Stephanie E. Cohen, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Medical Director, City Clinic San Francisco Department of Public Health Disclosures
STD Essentials for the Busy Clinician Stephanie E. Cohen, MD, MPH Assistant Professor, Division of Infectious Diseases, UCSF Medical Director, City Clinic San Francisco Department of Public Health Disclosures
Chapter 11. Sexually Transmitted Diseases
 Chapter 11. Sexually Transmitted Diseases General Guidelines Persons identified as having one sexually transmitted disease (STD) are at risk for others and should be screened as appropriate. Partners of
Chapter 11. Sexually Transmitted Diseases General Guidelines Persons identified as having one sexually transmitted disease (STD) are at risk for others and should be screened as appropriate. Partners of
Analysis of 3 Algorithms for Syphilis Serodiagnosis and Implications for Clinical Management
 MAJOR ARTICLE Analysis of 3 Algorithms for Syphilis Serodiagnosis and Implications for Clinical Management Man-Li Tong, 1,a Li-Rong Lin, 1,2,a Li-Li Liu, 1,2,3,a Hui-Lin Zhang, 1 Song-Jie Huang, 1 Yu-Yan
MAJOR ARTICLE Analysis of 3 Algorithms for Syphilis Serodiagnosis and Implications for Clinical Management Man-Li Tong, 1,a Li-Rong Lin, 1,2,a Li-Li Liu, 1,2,3,a Hui-Lin Zhang, 1 Song-Jie Huang, 1 Yu-Yan
Guidance for Industry
 Reprinted from FDA s website by Guidance for Industry Recommendations for Screening, Testing, and Management of Blood Donors and Blood and Blood Components Based on Screening Tests for Syphilis DRAFT GUIDANCE
Reprinted from FDA s website by Guidance for Industry Recommendations for Screening, Testing, and Management of Blood Donors and Blood and Blood Components Based on Screening Tests for Syphilis DRAFT GUIDANCE
Results of the 2014 Survey
 Syphilis Testing Practices in the Region of the Americas: 1 Syphilis Testing Practices in the Americas Region: Washington, D.C. 2016 Prepared by: Thuy Trinh¹, Mary L Kamb¹, Minh Luu², D. Cal Ham¹, Freddy
Syphilis Testing Practices in the Region of the Americas: 1 Syphilis Testing Practices in the Americas Region: Washington, D.C. 2016 Prepared by: Thuy Trinh¹, Mary L Kamb¹, Minh Luu², D. Cal Ham¹, Freddy
Medical Bacteriology Lecture 11
 Medical Bacteriology Lecture 11 Spirochaetaceae Treponema Borrelia 1 Spirochaetaceae Characteristics - Gran negative rods - spiral single cells, or cork-screw-shaped, extremely thin and can be very long
Medical Bacteriology Lecture 11 Spirochaetaceae Treponema Borrelia 1 Spirochaetaceae Characteristics - Gran negative rods - spiral single cells, or cork-screw-shaped, extremely thin and can be very long
Disclosures. STD Screening for Women. Chlamydia & Gonorrhea. I have no disclosures or conflicts of interest to report.
 Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Guidance for Industry
 Reprinted from FDA s website by EAS Consulting Group, LLC Guidance for Industry Recommendations for Screening, Testing, and Management of Blood Donors and Blood and Blood Components Based on Screening
Reprinted from FDA s website by EAS Consulting Group, LLC Guidance for Industry Recommendations for Screening, Testing, and Management of Blood Donors and Blood and Blood Components Based on Screening
Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S.
 and U.S.") Special paper Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S. (CDC) guidelines Maciej Pastuszczak, Anna Wojas-Pelc
Special paper Current standards for diagnosis and treatment of syphilis: selection of some practical issues, based on the European (IUSTI) and U.S. (CDC) guidelines Maciej Pastuszczak, Anna Wojas-Pelc
test. It appeared that the MHA-TP test could be
 JOURNAL OF CLINICAL MICROBIOLOGY, Mar. 1983, p. 405-409 0095-1137/83/030405-05$02.00/0 Copyright 1983, American Society for Microbiology Vol. 17, No. 3 Reactivity of Microhemagglutination, Fluorescent
JOURNAL OF CLINICAL MICROBIOLOGY, Mar. 1983, p. 405-409 0095-1137/83/030405-05$02.00/0 Copyright 1983, American Society for Microbiology Vol. 17, No. 3 Reactivity of Microhemagglutination, Fluorescent
Clinical Practice Guideline with Delegation of Function
 1 of 8 1.0 Purpose 1.1 To improve and focus efforts to treat those at risk for undiagnosed/untreated incubating, primary, secondary, or early latent infectious syphilis. 2.0 Scope and Goal 2.1 Antibiotic
1 of 8 1.0 Purpose 1.1 To improve and focus efforts to treat those at risk for undiagnosed/untreated incubating, primary, secondary, or early latent infectious syphilis. 2.0 Scope and Goal 2.1 Antibiotic
The U.S. Preventive Services Task Force (USPSTF) makes
 makes") Annals of Internal Medicine Clinical Guidelines Screening for Syphilis Infection in Pregnancy: U.S. Preventive Services Task Force Reaffirmation Recommendation Statement U.S. Preventive Services Task Force*
Annals of Internal Medicine Clinical Guidelines Screening for Syphilis Infection in Pregnancy: U.S. Preventive Services Task Force Reaffirmation Recommendation Statement U.S. Preventive Services Task Force*
Dr. R. Someshwaran, MBBS, MD., Assistant professor, Dept. of Microbiology, KFMS&R
 Dr. R. Someshwaran, MBBS, MD., Assistant professor, Dept. of Microbiology, KFMS&R 1 What is Syphilis? Syphilis is a systemic, sexually transmitted disease (STD) caused by the Treponema pallidum bacterium.
Dr. R. Someshwaran, MBBS, MD., Assistant professor, Dept. of Microbiology, KFMS&R 1 What is Syphilis? Syphilis is a systemic, sexually transmitted disease (STD) caused by the Treponema pallidum bacterium.
BMJ Open. Comparison of the automated rapid plasma reagin (RPR) test versus the conventional RPR card test in syphilis testing
 test versus the conventional RPR card test in syphilis testing") Comparison of the automated rapid plasma reagin (RPR) test versus the conventional RPR card test in syphilis testing Journal: BMJ Open Manuscript ID: bmjopen-0-00 Article Type: Research Date Submitted
Comparison of the automated rapid plasma reagin (RPR) test versus the conventional RPR card test in syphilis testing Journal: BMJ Open Manuscript ID: bmjopen-0-00 Article Type: Research Date Submitted
MID 15. Syphilis. Simon Tsiouris, MD, MPH. 1. Introduction
 Syphilis Simon Tsiouris, MD, MPH 1. Introduction Syphilis is a chronic infection caused by the bacterium Treponema pallidum which was first described over 500 years ago. The manifestations of disease are
Syphilis Simon Tsiouris, MD, MPH 1. Introduction Syphilis is a chronic infection caused by the bacterium Treponema pallidum which was first described over 500 years ago. The manifestations of disease are
Ann Dermatol Vol. 29, No. 6, 2017 https://doi.org/ /ad
 JI Kim, et al pissn 113-987ㆍeISSN 25-3894 Ann Dermatol Vol. 29, No. 6, 217 https://doi.org/1.521/ad.217.29.6.768 ORIGINAL ARTICLE Serologic Response to Treatment in Human Immunodeficiency Virus-Negative
JI Kim, et al pissn 113-987ㆍeISSN 25-3894 Ann Dermatol Vol. 29, No. 6, 217 https://doi.org/1.521/ad.217.29.6.768 ORIGINAL ARTICLE Serologic Response to Treatment in Human Immunodeficiency Virus-Negative
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy
 Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
Michigan Guidelines: HIV, Syphilis, HBV in Pregnancy Presenter: Theodore B. Jones, MD Maternal Fetal Medicine Wayne State University School of Medicine Beaumont Dearborn Hospital HIV, Syphilis, HBV in
CHAPTER-X SYPHILIS R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR.
 CHAPTER-X SYPHILIS R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR. Trepanoma pallidum D. Clinical Infection: Syphilis Transmission Usually
CHAPTER-X SYPHILIS R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR. Trepanoma pallidum D. Clinical Infection: Syphilis Transmission Usually
Clinical Practice Guideline
 1 of 10 1.0 Purpose 1.1 To improve and focus efforts to respond to clusters and outbreaks of infectious syphilis and reduce transmission in the Winnipeg Health Region by enhancing treatment options for
1 of 10 1.0 Purpose 1.1 To improve and focus efforts to respond to clusters and outbreaks of infectious syphilis and reduce transmission in the Winnipeg Health Region by enhancing treatment options for
Case 1. Case 1. Physical exam
 11/13/2012 Case 28 year-old woman Complains of very painful lesions in vulvar area Increasing severity since 4 days Pain aggravated by urination She has a slight fever and also complains of headache and
11/13/2012 Case 28 year-old woman Complains of very painful lesions in vulvar area Increasing severity since 4 days Pain aggravated by urination She has a slight fever and also complains of headache and
Division of Dermatology Dr A Motau
 Division of Dermatology Dr A Motau CASE 1 Histopathology H&E H&E H&E Wartin Starry Immunohistochemical stain for T. pallidum Investigations FBC, U&E, LFT Normal T. pallidum Abs Reactive RPR screen
Division of Dermatology Dr A Motau CASE 1 Histopathology H&E H&E H&E Wartin Starry Immunohistochemical stain for T. pallidum Investigations FBC, U&E, LFT Normal T. pallidum Abs Reactive RPR screen
Evaluation of a New Rapid Plasma Reagin Card Test as a Screening Test for Syphilis
 JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 1982, p. 286-290 0095-1 137/82/080286-05$02.00/0 Vol. 16, No. 2 Evaluation of a New Rapid Plasma Reagin Card Test as a Screening Test for Syphilis MARY W. PERRYMAN,'*
JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 1982, p. 286-290 0095-1 137/82/080286-05$02.00/0 Vol. 16, No. 2 Evaluation of a New Rapid Plasma Reagin Card Test as a Screening Test for Syphilis MARY W. PERRYMAN,'*
Profile of Syphilis. By Karley Delahoussaye
 Profile of Syphilis By Karley Delahoussaye Etiologic Agent: Treponema pallidum₁ Transmission: People transmit syphilis to each other directly through contact with a sore. The sores are known as chancres
Profile of Syphilis By Karley Delahoussaye Etiologic Agent: Treponema pallidum₁ Transmission: People transmit syphilis to each other directly through contact with a sore. The sores are known as chancres
VDRL v/s TPHA for diagnosis of syphilis among HIV sero-reactive patients in a tertiary care hospital
 ISSN: 2319-7706 Volume 3 Number 5 (2014) pp. 726-730 http://www.ijcmas.com Original Research Article VDRL v/s TPHA for diagnosis of syphilis among HIV sero-reactive patients in a tertiary care hospital
ISSN: 2319-7706 Volume 3 Number 5 (2014) pp. 726-730 http://www.ijcmas.com Original Research Article VDRL v/s TPHA for diagnosis of syphilis among HIV sero-reactive patients in a tertiary care hospital
Medical Bacteriology- Lecture 13 Spirochaetales 1- Spirochaetaceae Treponema Borrelia 2- Leptospiraceae Leptospira
 Medical Bacteriology- Lecture 13 Spirochaetales 1- Spirochaetaceae Treponema Borrelia 2- Leptospiraceae Leptospira OS = outer sheath AF = axial fibrils AF Leptospira interrogans Characteristics: Spirochaetaceae
Medical Bacteriology- Lecture 13 Spirochaetales 1- Spirochaetaceae Treponema Borrelia 2- Leptospiraceae Leptospira OS = outer sheath AF = axial fibrils AF Leptospira interrogans Characteristics: Spirochaetaceae
Syphilis Outbreak Investigation Report
 ` Office of the Chief Medical Officer of Health Syphilis Outbreak Investigation Report Office of the Chief Medical Officer of Health Health il 2014 Table of Contents Summary... 1 Acronyms... 1 Introduction...
` Office of the Chief Medical Officer of Health Syphilis Outbreak Investigation Report Office of the Chief Medical Officer of Health Health il 2014 Table of Contents Summary... 1 Acronyms... 1 Introduction...
Comparison of Doxycycline and Benzathine Penicillin G for the Treatment of Early Syphilis
 2017;25(2):107-111 Clinical article Comparison of Doxycycline and Benzathine Penicillin G for the Treatment of Early Syphilis Hailu Xiao *1,2,3, Dianchang Liu *1,2,4, Zhen Li 1,2,4, Rongtao Zheng 1,2,4,
2017;25(2):107-111 Clinical article Comparison of Doxycycline and Benzathine Penicillin G for the Treatment of Early Syphilis Hailu Xiao *1,2,3, Dianchang Liu *1,2,4, Zhen Li 1,2,4, Rongtao Zheng 1,2,4,
Documentation, Codebook, and Frequencies
 Documentation, Codebook, and Frequencies MEC Laboratory Component: Syphilis(IgG), Syphilis Rapid Plasma Reagin (RPR), and Treponema pallidum Particle Agglutination (TP- PA) Survey Years: 2003 to 2004 SAS
Documentation, Codebook, and Frequencies MEC Laboratory Component: Syphilis(IgG), Syphilis Rapid Plasma Reagin (RPR), and Treponema pallidum Particle Agglutination (TP- PA) Survey Years: 2003 to 2004 SAS
Diagnosis and Management of Acute HIV
 Diagnosis and Management of Acute HIV A New HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV, this committee
Diagnosis and Management of Acute HIV A New HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV, this committee
The Resurgence of Syphilis in British Columbia: Who is affected? What are the challenges? How can we improve our response?
 The Resurgence of Syphilis in British Columbia: Who is affected? What are the challenges? How can we improve our response? Gillian Hill-Carroll Travis Salway Hottes Pacific AIDS Network Webinar Series
The Resurgence of Syphilis in British Columbia: Who is affected? What are the challenges? How can we improve our response? Gillian Hill-Carroll Travis Salway Hottes Pacific AIDS Network Webinar Series
Using Mathematical Models to Inform Syphilis Control Strategies in Men Who Have Sex With Men
 Using Mathematical Models to Inform Syphilis Control Strategies in Men Who Have Sex With Men by Ashleigh Tuite A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Using Mathematical Models to Inform Syphilis Control Strategies in Men Who Have Sex With Men by Ashleigh Tuite A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Clinical Application of New Treponemal Antibody Test in Blood Donors
 Clinical Application of New Treponemal Antibody Test in Blood Donors Parichart Permpikul, MD Department of Transfusion Medicine Faculty of Medicine Siriraj Hospital Mahidol University Bangkok, Thailand
Clinical Application of New Treponemal Antibody Test in Blood Donors Parichart Permpikul, MD Department of Transfusion Medicine Faculty of Medicine Siriraj Hospital Mahidol University Bangkok, Thailand
BMJ Open. Comparing the Performance Characteristics of CSF-TRUST and CSF-VDRL: A Cross-sectional Study
 Comparing the Performance Characteristics of CSF-TRUST and CSF-VDRL: A Cross-sectional Study Journal: Manuscript ID: bmjopen-0-000 Article Type: Research Date Submitted by the Author: 0-Oct-0 Complete
Comparing the Performance Characteristics of CSF-TRUST and CSF-VDRL: A Cross-sectional Study Journal: Manuscript ID: bmjopen-0-000 Article Type: Research Date Submitted by the Author: 0-Oct-0 Complete
Bacteriology. Spirochetes. Three important genera: 1. Treponema 2. Borrelia 3. Leptospira. Treponema pallidum. Causes syphilis.
 Bacteriology Spirochetes Three important genera: 1. Treponema 2. Borrelia 3. Leptospira Treponema pallidum Causes syphilis Organism: - Spirochetes with 6-14 regularly spaced spirals - Its length is the
Bacteriology Spirochetes Three important genera: 1. Treponema 2. Borrelia 3. Leptospira Treponema pallidum Causes syphilis Organism: - Spirochetes with 6-14 regularly spaced spirals - Its length is the
Infectious syphilis in Canada:
 30 CCDR 05 February 2015 Volume 41-2 https://doi.org/10.14745/ccdr.v41i02a03 Infectious syphilis in Canada: 2003-2012 Totten S 1,*, MacLean R 1, Payne E 1 1 Centre for Communicable Diseases and Infection
30 CCDR 05 February 2015 Volume 41-2 https://doi.org/10.14745/ccdr.v41i02a03 Infectious syphilis in Canada: 2003-2012 Totten S 1,*, MacLean R 1, Payne E 1 1 Centre for Communicable Diseases and Infection
Trends in Sexually Transmitted Infections (STIs) C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017
 C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017") Trends in Sexually Transmitted Infections (STIs) C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017 1 Speaker Disclosure Dr. Woo has disclosed that she has no
Trends in Sexually Transmitted Infections (STIs) C. Junda Woo, MD, MPH, Medical Director San Antonio Metropolitan Health District June 3, 2017 1 Speaker Disclosure Dr. Woo has disclosed that she has no
Gonorrhea, Chlamydia, and Syphilis in Alaska
 Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
Department of Health and Social Services Division of Public Health Section of Epidemiology Karen Perdue, Commissioner Karen Pearson, Director John Middaugh, MD, Editor 361 C Street, Suite 54, P.O. Box
ANNUAL MORBIDITY REPORT
 DUTCHESS COUNTY DEPARTMENT OF HEALTH S ANNUAL MORBIDITY REPORT Marcus J. Molinaro, Dutchess County Executive Kari Reiber, MD, Acting Commissioner of Health Volume 8, Issue FIRST CONGENITAL SYPHILIS CASE
DUTCHESS COUNTY DEPARTMENT OF HEALTH S ANNUAL MORBIDITY REPORT Marcus J. Molinaro, Dutchess County Executive Kari Reiber, MD, Acting Commissioner of Health Volume 8, Issue FIRST CONGENITAL SYPHILIS CASE
Frequent Screening for Syphilis as Part of HIV Monitoring Increases the Detection of Early Asymptomatic Syphilis Among HIV-Positive Homosexual Men
 CLINICAL SCIENCE Frequent Screening for Syphilis as Part of HIV Monitoring Increases the Detection of Early Asymptomatic Syphilis Among HIV-Positive Homosexual Men Melanie Bissessor, FRACGP,* Christopher
CLINICAL SCIENCE Frequent Screening for Syphilis as Part of HIV Monitoring Increases the Detection of Early Asymptomatic Syphilis Among HIV-Positive Homosexual Men Melanie Bissessor, FRACGP,* Christopher
Screening for Syphilis With the Treponemal Immunoassay: Analysis of Discordant Serology Results and Implications for Clinical Management
 MAJOR ARTICLE Screening for Syphilis With the Treponemal Immunoassay: Analysis of Discordant Serology Results and Implications for Clinical Management Ina U. Park, 1,2 Joan M. Chow, 1 Gail Bolan, 1 Mark
MAJOR ARTICLE Screening for Syphilis With the Treponemal Immunoassay: Analysis of Discordant Serology Results and Implications for Clinical Management Ina U. Park, 1,2 Joan M. Chow, 1 Gail Bolan, 1 Mark