Invasive sino-orbital mycosis in an aplastic anemia patient caused by Neosartorya laciniosa
|
|
|
- Howard Manning
- 5 years ago
- Views:
Transcription
1 JCM Accepts, published online ahead of print on 23 January 2013 J. Clin. Microbiol. doi: /jcm Copyright 2013, American Society for Microbiology. All Rights Reserved. 1 1 Invasive sino-orbital mycosis in an aplastic anemia patient caused by Neosartorya laciniosa 2 3 Kathy Malejczyk Department of Laboratory Medicine and Pathology, Division of Infection Diseases, University of Alberta, Edmonton, Alberta, Canada Lynne Sigler, Connie Fe C. Gibas University of Alberta Microfungus Collection and Herbarium, Edmonton, Alberta, Canada Stephanie W. Smith # Infection Control, University of Alberta Hospitals, and Division of Infection Diseases, University of Alberta, Edmonton, AB, Canada Running title: Sino-orbital mycosis caused by Neosartorya laciniosa Keywords: mycosis, sino-orbital, Neosartorya laciniosa, Aspergillus, beta-tubulin, calmodulin Correspondent footnote: Stephanie Smith, ssmith1@med.ualberta.ca
2 We report the first case of Neosartorya laciniosa invasive sinusitis involving the orbit in an immunocompromised male with aplastic anemia. Treatment included surgical debridement with enucleation of the eye, combination voriconazole and micafungin therapy followed by voriconazole alone. The fungus was identified using sequencing of partial bena and calmodulin genes. Downloaded from on September 9, 2018 by guest
3 Case Report A 66-year-old male was diagnosed with aplastic anemia in March 2011 and subsequently treated with bone marrow transplant (BMT) followed by immunosuppressive therapy with lymphocyte immune globulin anti-thymocyte globulin (Atgam, Pfizer Canada Inc., Kirkland, QC), steroids and cyclosporine. On May 19, he was referred from a community hospital to the University of Alberta Hospital with a history of pancytopenia (absolute neutrophil count (ANC) < 500 cells/µl) beginning in February and intermittent fevers since mid April. Additional findings included increased left-sided periorbital swelling and radiographic evidence of pneumonia, but no respiratory symptoms were evident. He had not received antifungal prophylaxis. On admission he was hemodynamically stable and febrile (temperature of 39.1 C). A complete blood count (CBC) revealed pancytopenia with a white blood count of 400 cells/µl (ANC 0 cells/µl), a creatinine of 112 µmol/l (Estimated Glomerular Filtration Rate 57 ml/min). Electrolytes and liver enzymes were normal. Urine and blood cultures were negative. The patient was treated empirically with vancomycin and ciprofloxacin for presumed periorbital cellulitis. A computed tomography (CT) of the head showed left-sided protposis and progression of fluid and high density material causing opacification within all of visualized paranasal sinuses on the left side. This finding was interpreted to represent probable chronic paranasal sinus inflammation. A prior head CT done at the time of the BMT was normal. The patient deteriorated clinically with adverse changes including advancing opacification of frontal, ethmoidal and maxillary sinuses with erosions of bony septations of ethmoidal air cells on the left side seen on repeat CT on day 6 post admission. An abscess along the wall of the left medial orbit was documented on CT on day 13 and the patient was sent to the operating room the next day for drainage of a subperiosteal enhancing fluid collection. Intraoperative tissue samples were
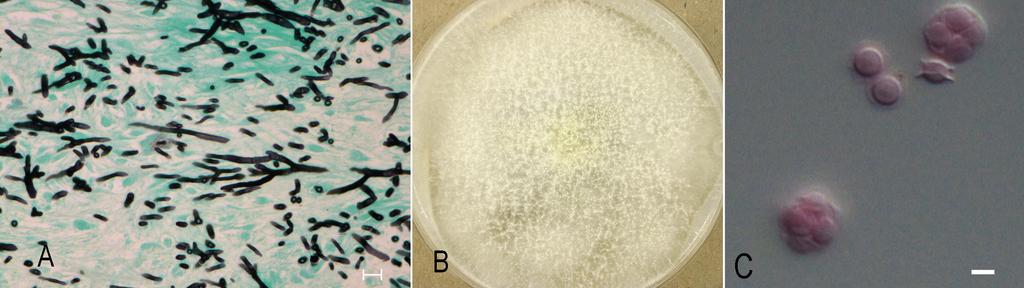
4 sent for pathological analysis as well as for bacterial and fungal cultures. Bacterial culture yielded only coagulase negative Staphylococcus (CoNS). No fungal elements were seen on direct smear with calcofluor white (BD Diagnostic Systems, Sparks, MD) and fungal cultures were negative. However, the pathology report documented hemorrhagic necrotic sinus mucosal tissue with numerous branched, septate hyphae and focal vascular invasion consistent with invasive fungal infection (Fig. 1A). The patient was promptly started on liposomal amphotericin B (5 mg/kg/day). Tissue from a second debridement done on day 16 was again negative for hyphae by direct microscopy but culture yielded growth of a mold within three days that was suspected later to be a possible white, non-sporulating Aspergillus. An exoantigen immunodiffusion test, in which a filtrate from the culture was tested against commercially available antibody reagents (Pulse Scientific Inc., Burlington, ON), gave a positive result for Aspergillus fumigatus. The isolate was identified as a Neosartorya species when characteristic ascospores were produced two weeks later. A serum galactomannan enzyme immunoassay (Platelia TM Apergillus EIA,Bio- Rad Laboratories (Canada) Ltd., Montreal, QC) performed on day 21 was also positive with an optical density (OD) index value of 2.8 (0.5 used as cut-off value) confirming the diagnosis of invasive aspergillosis. Antifungal therapy was switched to voriconazole 300 mg twice daily and the patient continued on vancomycin, ciprofloxacin in addition to cyclosporine and acyclovir for immunosuppression and antiviral prophylaxis respectively. Despite the antifungal and broad antimicrobial coverage, the patient continued to be pancytopenic and was persistently febrile. A CT scan on day 26 showed suggestion of dehiscence of the sphenoid sinus and possible communication with the anterior cranial fossa could not be excluded. No intracranial venous thrombosis was noted on magnetic resonance imaging of the brain. A repeat CT on day 33 revealed evidence of gas within a large collection of
5 fluid infraorbitally measuring 5.6 cm in coronal diameter and again extensive mucoperiosteal thickening within frontal and ethmoidal regions as well as the right maxillary sinus. The patient was taken for surgical enucleation of the left eye on day 35 and further debridement was performed three days later. Fungal hyphae accompanied by tissue necrosis were again seen on histopathology of tissue and cortical bone samples and bacterial cultures were positive for Enterococcus species and CoNS. The patient was continued on vancomycin for a total of 6 weeks of therapy. Unfortunately, fungal culture was not requested at surgery but a repeat serum galactomannan on day 40 remained positive with OD index value of Based on our patient s tenuous clinical picture, we elected to continue him on oral voriconazole 300mg twice daily and to add intravenous micafungin 150mg daily based on reported uniform susceptibility to this drug among Neosartorya and related species classified within Aspergillus section Fumigati (1, 2). A final CT done on day 40 documented mucosal thickening within the remainder of paranasal sinuses and no fluid collections. He remained transfusion dependant for his pancytopenias, but defervesced and had gradual clinical improvement resulting in his transfer to a community hospital 13 days later. The patient completed a total of six months of antifungal therapy (7 weeks of combination voriconazole and micafungin and four months of monotherapy with voriconazole). He was discharged from hospital seven months after his initial presentation. He continued on cyclosporine for his aplastic anemia and his blood counts stabilized. He was scheduled to have reconstructive surgery to his left orbital area. There was no evidence of recurrence of his fungal infection two months after stopping voriconazole therapy. Mycology. As per review of the literature which indicated variable susceptibility to voriconazole depending on species of Neosartorya, the isolate was submitted for further
6 identification to the University of Alberta Microfungus Collection and Herbarium (UAMH) where it was accessioned as UAMH Subcultures on potato dextrose agar (PDA) (BD) and oatmeal salts agar (OAT; prepared in-house) were incubated at 30ºC and 35ºC. Growth was faster at 35ºC with the colony on PDA reaching a diameter of 6 cm after 3 days of incubation. The submitting laboratory reported growth at 45ºC but no growth at 50ºC. Colonies remained yellowish white with no blue-green surface coloration after 14 days. Conidial heads were sparse. The vesicle was about 15 µm wide and bore few phialides on the upper surface. Characteristic yellowish-white, thin-walled ascomata were produced on both media within 7 days, but were more profuse on OAT (Fig. 1B). Ascospores were broadly lenticular with two prominent equatorial crests and measured 4.5 to 5 µm long (Fig 1C). Sequences of the beta-tubulin and calmodulin gene regions were obtained for species identification. DNA was extracted using the E.Z.N.A. SP Fungal DNA kit (United Bioinformatica Inc., Saskatoon, SK). The partial bena and calmodulin genes were sequenced using primers previously described (3, 4). Sequences were edited using Sequencher ver. 5.0 (Gene Codes Corp., Ann Arbor, MI) and compared with available sequences in the Genbank nucleotide database using a Blast search. Results were similar for both searches with the case isolate showing % bena similarity and % calmodulin similarity with several sequences of Neosartorya spinosa and N. laciniosa, including the ex-type strain KACC To further assess the genetic relationship between the case isolate and these Neosartorya species, a dataset of combined bena and calmodulin sequences was obtained and a parsimony analysis was performed using PAUP* v.4.0b10 ( ) and with N. fischeri as outgroup. The robustness of the trees obtained was evaluated by 1,000 bootstrap replications. In the resultant tree, the case isolate is shown
7 grouping with isolates of N. laciniosa with 100% bootstrap support and the group is sister to N. spinosa (Fig 2). Susceptibility testing performed retrospectively on isolate UAMH yielded MICs (mg/l) of amphotericin B 0.5, 5-fluorouracil 8, fluconazole >64, itraconazole 1, posaconazole 0.25 mg, voriconazole 1, caspofungin 0.5. Invasive aspergillosis (IA) is the most common filamentous fungal infection among immunocompromised patients with very high mortality rates. Although the majority of infections are attributed to Aspergillus fumigatus, there is increasing recognition of the role of related species in causing invasive disease especially since the advent of molecular methods allowing for more precise identification of the etiologic agent involved. There are currently nine Aspergillus species and 27 Neosartorya teleomorphs included within the Aspergillus section Fumigati (2, Mycobank Neosartorya species are generally recognized by their rapidly growing, poorly sporulating white to pale green colonies in primary culture, by their thermotolerance (all growing at 37ºC and a few up to 50ºC), and by formation of ascomata containing ascospores on sporulation media. Currently, N. hiratsukae, N. pseudofischeri, N. udagawae are confirmed as opportunistic pathogens, with the latter species gaining recent attention (5-13). Although N. fischeri and N. spinosa have been identified in some reports, their roles in causing infection have not been reliably confirmed. Isolates from some older cases have been re-identified as N. pseudofischeri and isolates from more recent cases have not been identified using sequencing of genes appropriate for Neosartorya identification (14-17). Neosartorya infections in humans may include invasive infections of eye, ear or lung, endocarditis, peritonitis, multifocal brain abscesses and osteomyelitis (5-16). We report the first
8 case of N. laciniosa invasive sino-orbital aspergillosis (SOA) in a patient with aplastic anemia. How our patient acquired his infection is unknown. He did not live on a farm or acreage and had not worked for some time due to illness so no specific exposures could be identified. Neosartorya laciniosa was described in 2006 for 12 isolates mainly from agricultural soils with a single isolation from strawberry fruit pulp (4). The species has a broad geographic distribution in Korea, Dominican Republic, Kenya, Pakistan, Netherlands, Surinam and the USA. N. laciniosa is genetically closest to N. spinosa and these species could not be reliably distinguished based on results of blast search. However, the differentiation between the species is clearly supported in the phylogenetic tree based on the combined dataset (Fig 2). Neosartorya species are uncommonly isolated in our hospital, so there was concern 4 months after this patient s presentation when a pediatric patient with acute lymphocytic leukemia presented with a necrotic nasal lesion from which a Neosartorya species was again cultured. However, sequencing of the isolate from the second patient determined its identity as N. pseudofischeri. SOA is a relatively uncommon form of aspergillosis, occurring in both immunocompetent and immunosuppressed humans, as well as in canines and felines. Most cases have been described based on clinical and histopathological features and the etiologic agent has been infrequently identified to the species level (e.g. 18). A recent study of the etiology of feline SOA in Australia determined that Neosartorya species were the cause of all 17 cases documented (19). Although sequencing of the internal transcribed spacer regions was insufficient to identify the isolates to the species level, the high % similarity, the production of ascospores in some mating studies, and the frequent treatment failure suggests that N. udagawae was the main
9 species involved. N. udagawae differs from N. lacinosa in being heterothallic, in failing to grow above 42ºC and in being refractory to antifungal therapy (10, 12, 13, 19). Our patient was successfully treated with voriconazole and micafungin together with surgical debridement. Antifungal susceptibility testing done retrospectively on the case isolate showed that N. laciniosa is similar to N. hiratsukae in showing low MICs to amphotericin, itraconazole, voriconazole and caspofungin (1). In contrast, both N. udagawae and N. pseudofischeri show high MICs to voriconazole and itraconazole (1, 10). It is therefore clinically important to not only differentiate Neosartorya isolates from the related Aspergillus within the section Fumigati, but also to identify Neosartorya isolates to the species level. This case confirms that Neosartorya species should be suspected when a white thermotolerant Aspergillus with sparse conidiation is isolated and that identification to the species level can be obtained by sequencing of partial bena and calmodulin genes. Accurate identification is necessary to elucidate clinical or therapeutic differences between Neosartorya species. Nucleotide sequence accession numbers. Sequences for N. laciniosa UAMH were deposited in GenBank under accession no. JX for the partial calmodulin gene and JX for the partial bena gene. Acknowledgements. We thank the Mycology Unit, Laboratory Medicine and Pathology, University of Alberta Hospitals, for providing results of susceptibility testing. L. Sigler acknowledges financial support from the Natural Sciences and Engineering Research Council of Canada (G ). References
10 Alcazar-Fuoll L, Mellado E, Alastruey-Izqulerdo A, Cuenca-Estrella M, Rodriguez-Tudela JL Aspergillus Section Fumigati: Antifungal susceptibility patterns and sequencebased identification. Antimicrob. Agents Chemother. 52: Samson RA, Hong S, Peterson SW, Frisvad JC, Varga J Polyphasic taxonomy of Aspergillus section Fumigati and its teleomorph Neosartorya. Stud. Mycol. 59: Glass NL, Donaldson GC Development of primer sets designed for use with the PCR to amplify conserved genes from filamentous ascomycetes. Appl. Environ. Microbiol. 61: Hong SB, Cho HS, Shin HD, Frisvad JC, Samson RA Novel Neosartorya species isolated from soil in Korea. Int. J. Syst. Evol. Microbiol. 56: Shivaprakash MR, Jain N, Gupta S, Baghela A, Gupta A, Chakrabarti A Allergic fungal rhinosinusitis caused by Neosartorya hiratsukae from India. Med. Mycol. 47: Koutroutsos K, Arabatzis M, Bougatsos G, Xanthaki A, Toutouza M, Belegraki A Neosartorya hiratsukae through continuous ambulatory peritoneal dialsysis. J. Med. Micro. 59: Lehtmaa JH, Summerbell RC, Hoekstra ES, Samson RA, Naaber P. 2004, Isolation of Neosartorya pseudofischeri from blood: first hint of pulmonary aspergillosis. J Clin Microbiol 42: Ghebremedhin B, Bluemel A, Neumann KH, Koenig B, Koenig W Peritonitis due to Neosarotrya pseudofischeri in an elderly patient undergoing peritoneal dialysis successfully treated with voriconazole. J. Med. Microbiol. 58:
11 Balajee AS, Gribskov J, Brandt M, Ito J, Fothergill A, Marr KA Mistaken identity: Neosartorya pseudofischeri and its anamorph masquerading as Aspergillus fumigatus. J. Clin. Microbiol. 43: Vinh DC, Shea YR, Sugui JA, Parrilla-Castellar ER, Freeman AD, Campbell JW, Pittaluga S, Jones PA, Zelazny A, Kleiner D, Kwon-Chung KJ, Holland SM Invasive aspergillosis due to Neosartorya udagawe. Clin. Infect. Dis. 49: Sugui JA, Vinh DC, Nardone G, Shea YR, Chang YC, Zelazny AM, Marr KA, Holland SM, Kwong-Chung KJ Neosartorya udagawe (Aspergillus udagawe), an emerging agent of aspergillosis: How different is it from Aspergillus fumigatus? J. Clin. Microbiol. 48: Posteraro B, Mattei R, Trivella F, Maffei A, Torre A, De Carolis E, Posteraro P, Fadda G, Sanguinetti M Uncommon Neosartorya udagawe fungus as a causative agent of severe corneal infection. J. Clin. Microbiol. 49: Gyotoku H, Izumikawa K, Ikeda H, Takazono T, Morinaga Y, Nakamura S, Imamura Y, Nishino T, Miyazaki T, Kakeya H, Yamamoto Y, Yanagihara K, Yasuoka A, Yaguchi T, Ohno H, Miyzaki Y, Kamei K, Kanda T, Kohno S A case of bronchial aspergillosis caused by Aspergillus udagawae and its mycological features. Med. Mycol. 50: Lonial S, Wiliams L, Carrum G, Ostrowski M, McCarthy Jr. P Neosartorya fischeri: an invasive fungal pathogen in an allogeneic bone marrow transplant patient. Bone Marrow Transplant. 19: Summerbell RC, de Repentigny L, Chartrand C, St Germain G Graft-related endocarditis caused by Neosartorya fischeri var. spinosa. J. Clin. Microbiol 30:
12 Padhye AA, Godfrey JH, Chandler FW, Peterson SW Osteomyelitis caused by Neosartorya pseudofischeri. J. Clin. Microbiol. 32: Krockenberger MB, Swinney G, Martin P, Rothwell TR, Malik R Sequential opportunistic infection in two German Shepherd dogs. Aust. Vet. J. 89: Pushker N, Meel R, Kashyap S, Bajaj MS, Sen S Invasive aspergillois of orbit in immunocompetent patients: treatment and outcome. Ophthalmology 118: Barrs VR, Halliday C, Martin P, Wilson B, Krockenberger M, Gunew M, Bennett S, Koehlmeyer E, Thompson A, Filegner R, Hocking A, Sleiman S, O'Brien C, Beatty JA Sinonasal and sino-orbital aspergillosis in 23 cats: Aetiology, clinicopathological features and treatment outcomes. Vet. J. 191: Downloaded from on September 9, 2018 by guest
13 Legend to figures FIG 1. Panel A, Gomorri methanamine silver stained section of sinus mucosal tissue showing numerous branched, septate hyphae (Bar = 20 µm); Panel B, colony on OAT showing ascomata after 7 days growth at 35ºC; Panel C, ascospores in face and side view showing two crests (Bar = 5 µm). FIG 2. One of 19 equally parsimonious trees (CI 0.891, RI 0.867, HI 0.109) inferred from maximum parsimony analysis of combined partial beta-tubulin and calmodulin gene sequences showing the placement of the case isolate. Bootstrap values above 50% are shown. For each isolate, GenBank accession numbers and culture collection number are listed. Culture collection acronyms are CBS Centraalbureau voor Schimmelcultures, Utrecht, Netherlands; IBT Culture Collection of Fungi, Technical University of Denmark, Lyngby, Denmark; KACC Korean Agricultural Culture Collection, Suwon, South Korea; NRRL USDA Agricultural Research Service Culture Collection, Peoria, IL; SUM Medical Mycology Research Center, Chiba University, Chiba, Japan; UAMH University of Alberta Microfungus Collection and Herbarium, Edmonton, Canada.
14 Neosartorya pseudofischeri CBS T (AY870742, AY870702) Neosartorya pseudofischeri NRRL (EF669805, EF669874) 100 Neosartorya quadricincta NRRL 2154 T (EF669806, EF669875) 100 Neosartorya glabra CBS T (AY870734, AY870693) Neosartorya hiratsukae KACC (DQ534095, DQ534169) Aspergillus viridinutans NRRL 4365 T (EF669834, EF669904) Neosartorya laciniosa SUM 3330 (AB514193, AB514194) 67 Neosartorya laciniosa KACC (AY870747, AY870707) 100 Neosartorya laciniosa CBS (UAMH 6422) (AY870754, AY870714) Neosartorya laciniosa CBS T (KACC 41657) (AY870756, AY870716) Case isolate UAMH Neosartorya spinosa NRRL 5034 T (EF669844, EF669914) Aspergillus fumigatiaffinis IBT (DQ094884, DQ094890) 97 Aspergillus novofumigatus IBT (DQ094886, DQ094893) Aspergillus lentulus NRRL T (EF669825, EF669895) Aspergillus fumigatus CBS (AY685149, AY689333) Neosartorya fischeri NRRL 181 T (AF057322, AY689370) 10 changes T = ex-type culture
15
Dr. Arghya Samanta PG-3 Department of Pediatrics
 Dr. Arghya Samanta PG-3 Department of Pediatrics A 3 year old male K/C/O B-cell Acute lymphoblastic leukemia Undergoing induction phase of chemotherapy On day 23 of induction Presented with - high grade
Dr. Arghya Samanta PG-3 Department of Pediatrics A 3 year old male K/C/O B-cell Acute lymphoblastic leukemia Undergoing induction phase of chemotherapy On day 23 of induction Presented with - high grade
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
2046: Fungal Infection Pre-Infusion Data
 2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
AUSTRALIAN ANTIFUNGAL SUSCEPTIBILITY DATA : PART 2 THE MOULDS ASPERGILLUS, SCEDOSPORIUM AND FUSARIUM.
 AUSTRALIAN ANTIFUNGAL SUSCEPTIBILITY DATA 00-0: PART THE MOULDS ASPERGILLUS, SCEDOSPORIUM AND FUSARIUM. AUSTRALIAN Sarah Kidd, Rose Handke and ANTIFUNGAL David Ellis SUSCEPTIBILITY DATA 00-00 David SA
AUSTRALIAN ANTIFUNGAL SUSCEPTIBILITY DATA 00-0: PART THE MOULDS ASPERGILLUS, SCEDOSPORIUM AND FUSARIUM. AUSTRALIAN Sarah Kidd, Rose Handke and ANTIFUNGAL David Ellis SUSCEPTIBILITY DATA 00-00 David SA
Medical Mycology Case Reports
 Medical Mycology Case Reports 1 (2012) 107 111 Contents lists available at SciVerse ScienceDirect Medical Mycology Case Reports journal homepage: www.elsevier.com/locate/mmcr Granulomatous invasive fungal
Medical Mycology Case Reports 1 (2012) 107 111 Contents lists available at SciVerse ScienceDirect Medical Mycology Case Reports journal homepage: www.elsevier.com/locate/mmcr Granulomatous invasive fungal
Lung Abscess due to Clostridium barati in a Patient with Invasive Pulmonary Aspergillosis ACCEPTED
 JCM Accepts, published online ahead of print on 3 January 2008 J. Clin. Microbiol. doi:10.1128/jcm.02446-07 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 3 January 2008 J. Clin. Microbiol. doi:10.1128/jcm.02446-07 Copyright 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All
Case Studies in Fungal Infections and Antifungal Therapy
 Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Introduction. Study of fungi called mycology.
 Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
In vivo response in a mixed infection model of azole susceptible and resistant Aspergillus spp. strains Laura Alcazar-Fuoli, CNM, ISCIII
 In vivo response in a mixed infection model of azole susceptible and resistant Aspergillus spp. strains Laura Alcazar-Fuoli, CNM, ISCIII Pre-Advances Against Aspergillosis Workshop: Aspergillus Speciation
In vivo response in a mixed infection model of azole susceptible and resistant Aspergillus spp. strains Laura Alcazar-Fuoli, CNM, ISCIII Pre-Advances Against Aspergillosis Workshop: Aspergillus Speciation
TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS. Part I: EMPIRICAL THERAPY
 TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS Part I: EMPIRICAL THERAPY CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES NIJMEGEN, THE NETHERLANDS n = 328 BACTERIAL INFECTION FUNGAL INFECTION 7% 36%
TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS Part I: EMPIRICAL THERAPY CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES NIJMEGEN, THE NETHERLANDS n = 328 BACTERIAL INFECTION FUNGAL INFECTION 7% 36%
No Evidence As Yet. Georg Maschmeyer. Dept. of Hematology, Oncology & Palliative Care Klinikum Ernst von Bergmann Potsdam, Germany
 Is Combined Antifungal Therapy More Efficient than Single Agent Therapy? No Evidence As Yet www.ichs.org Georg Maschmeyer Dept. of Hematology, Oncology & Palliative Care Klinikum Ernst von Bergmann Potsdam,
Is Combined Antifungal Therapy More Efficient than Single Agent Therapy? No Evidence As Yet www.ichs.org Georg Maschmeyer Dept. of Hematology, Oncology & Palliative Care Klinikum Ernst von Bergmann Potsdam,
Nationwide survey of treatment for pediatric patients with invasive fungal infections in Japan
 J Infect Chemother (2013) 19:946 950 DOI 10.1007/s10156-013-0624-7 ORIGINAL ARTICLE Nationwide survey of treatment for pediatric patients with invasive fungal infections in Japan Masaaki Mori Received:
J Infect Chemother (2013) 19:946 950 DOI 10.1007/s10156-013-0624-7 ORIGINAL ARTICLE Nationwide survey of treatment for pediatric patients with invasive fungal infections in Japan Masaaki Mori Received:
Nijmegen Institute for Infection, Inflammation and Immunity (N4i) 2, Nijmegen, the. and Hematology 4, University Medical Center
 2, Nijmegen, the. and Hematology 4, University Medical Center") JCM Accepts, published online ahead of print on January 0 J. Clin. Microbiol. doi:./jcm.01-0 Copyright 0, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.
JCM Accepts, published online ahead of print on January 0 J. Clin. Microbiol. doi:./jcm.01-0 Copyright 0, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases. Y.L. Kwong Department of Medicine University of Hong Kong
 Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
PAGL Inclusion Approved at January 2017 PGC
 Guideline for the prophylaxis and treatment of fungal infections in Haematology patients 1. Introduction PAGL Inclusion Approved at January 2017 PGC Haematology, CHUGGS June 2016 This guideline sets out
Guideline for the prophylaxis and treatment of fungal infections in Haematology patients 1. Introduction PAGL Inclusion Approved at January 2017 PGC Haematology, CHUGGS June 2016 This guideline sets out
ENT Infections. Case 1. Diagnosis. Marlene L. Durand, M.D. Mass. General Hospital Mass. Eye & Ear Infirmary
 ENT Infections Marlene L. Durand, M.D. Mass. General Hospital Mass. Eye & Ear Infirmary Case 1 18 yr-old patient presents with L eyelid swelling, redness, and pain. He was well until 10 days ago, when
ENT Infections Marlene L. Durand, M.D. Mass. General Hospital Mass. Eye & Ear Infirmary Case 1 18 yr-old patient presents with L eyelid swelling, redness, and pain. He was well until 10 days ago, when
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
ESCMID Online Lecture Library. by author. Salvage Therapy of Invasive Aspergillosis Refractory to Primary Treatment with Voriconazole
 Salvage Therapy of Invasive Aspergillosis Refractory to Primary Treatment with Voriconazole J.A. Maertens, hematologist, MD, PhD University Hospital Gasthuisberg Leuven, Belgium Current guidelines: first-line
Salvage Therapy of Invasive Aspergillosis Refractory to Primary Treatment with Voriconazole J.A. Maertens, hematologist, MD, PhD University Hospital Gasthuisberg Leuven, Belgium Current guidelines: first-line
Condition First line Alternative Comments Candidemia Nonneutropenic adults
 Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
Recommendations for the treatment of candidiasis. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Condition First line Alternative
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS
 MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
HAEMATOLOGY ANTIFUNGAL POLICY
 HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
New Directions in Invasive Fungal Disease: Therapeutic Considerations
 New Directions in Invasive Fungal Disease: Therapeutic Considerations Coleman Rotstein, MD, FRCPC, FACP University of Toronto University Health Network Toronto, Ontario Disclosure Statement for Coleman
New Directions in Invasive Fungal Disease: Therapeutic Considerations Coleman Rotstein, MD, FRCPC, FACP University of Toronto University Health Network Toronto, Ontario Disclosure Statement for Coleman
Fungal ball.. Clinical and radiological features DR. AHMED ALTUWAIJRI 1/5/2017
 Fungal ball.. Clinical and radiological features DR. AHMED ALTUWAIJRI 1/5/2017 Fungal Rhinosinusitis (FRS) Rhinosinusitis, is a common disorder affecting approximately 20% of the population at some time
Fungal ball.. Clinical and radiological features DR. AHMED ALTUWAIJRI 1/5/2017 Fungal Rhinosinusitis (FRS) Rhinosinusitis, is a common disorder affecting approximately 20% of the population at some time
ESCMID Online Lecture Library. by author. CASE PRESENTATION ECCMID clinical grand round May Anat Stern, MD Rambam medical center Haifa, Israel
 CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
Challenges and controversies of Invasive fungal Infections
 Challenges and controversies of Invasive fungal Infections Mona Al-Dabbagh, MD, MHSc Assistant Professor of Pediatrics, COM-KSAU-HS Consultant Pediatric Infectious Diseases and Transplant Infectious Diseases
Challenges and controversies of Invasive fungal Infections Mona Al-Dabbagh, MD, MHSc Assistant Professor of Pediatrics, COM-KSAU-HS Consultant Pediatric Infectious Diseases and Transplant Infectious Diseases
Case Report Chronic Invasive Nongranulomatous Fungal Rhinosinusitis in Immunocompetent Individuals
 Case Reports in Otolaryngology Volume 2016, Article ID 6854121, 7 pages http://dx.doi.org/10.1155/2016/6854121 Case Report Chronic Invasive Nongranulomatous Fungal Rhinosinusitis in Immunocompetent Individuals
Case Reports in Otolaryngology Volume 2016, Article ID 6854121, 7 pages http://dx.doi.org/10.1155/2016/6854121 Case Report Chronic Invasive Nongranulomatous Fungal Rhinosinusitis in Immunocompetent Individuals
Monitorization, Separation and Quantification of Antifungals used for Invasive Aspergillosis Treatment by High Performance Thin Layer Chromatography
 Monitorization, Separation and Quantification of Antifungals used for Invasive Aspergillosis Treatment by High Performance Thin Layer Chromatography M. P. Domingo, M. Vidal, J. Pardo, A. Rezusta, L. Roc,
Monitorization, Separation and Quantification of Antifungals used for Invasive Aspergillosis Treatment by High Performance Thin Layer Chromatography M. P. Domingo, M. Vidal, J. Pardo, A. Rezusta, L. Roc,
Is pre-emptive therapy a realistic approach?
 Is pre-emptive therapy a realistic approach? J Peter Donnelly PhD, FRCPath Department of Haematology Radboud University Nijmegen Medical Centre Nijmegen, The Netherlands Is pre-emptive therapy a realistic
Is pre-emptive therapy a realistic approach? J Peter Donnelly PhD, FRCPath Department of Haematology Radboud University Nijmegen Medical Centre Nijmegen, The Netherlands Is pre-emptive therapy a realistic
Neutropenic Sepsis Guideline
 Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
ASPERGILLOSIS IN THE NON-NEUTROPENIC HOST
 ASPERGILLOSIS IN THE NON-NEUTROPENIC HOST Dr J Garbino University Hospital Geneva ASPERGILLOSIS IN THE NON-NEUTROPENIC HOST INTRODUCTION SWISS ASPERGILLOSIS SURVEY IN THE NON-NEUTROPENIC HOST Introduction
ASPERGILLOSIS IN THE NON-NEUTROPENIC HOST Dr J Garbino University Hospital Geneva ASPERGILLOSIS IN THE NON-NEUTROPENIC HOST INTRODUCTION SWISS ASPERGILLOSIS SURVEY IN THE NON-NEUTROPENIC HOST Introduction
WHICH ANTIFUNGAL AGENT IS THE CHOICE FOR SUSPECTED FUNGAL INFECTIONS?
 WHICH ANTIFUNGAL AGENT IS THE CHOICE FOR SUSPECTED FUNGAL INFECTIONS? Assoc. Prof. Dr. Serkan SENER Acibadem University Medical School Department of Emergency Medicine, Istanbul Acibadem Ankara Hospital,
WHICH ANTIFUNGAL AGENT IS THE CHOICE FOR SUSPECTED FUNGAL INFECTIONS? Assoc. Prof. Dr. Serkan SENER Acibadem University Medical School Department of Emergency Medicine, Istanbul Acibadem Ankara Hospital,
Mucor Mycosis maxilla with palatal destruction An Interesting Case Report with Literature Review
 ISSN 2250-0359 Volume 3 Issue 3.5 2013 Mucor Mycosis maxilla with palatal destruction An Interesting Case Report with Literature Review 1 Balasubramanian Thiagarajan 2 Venkatesan Ulaganathan 1 Stanley
ISSN 2250-0359 Volume 3 Issue 3.5 2013 Mucor Mycosis maxilla with palatal destruction An Interesting Case Report with Literature Review 1 Balasubramanian Thiagarajan 2 Venkatesan Ulaganathan 1 Stanley
Antifungal Pharmacodynamics A Strategy to Optimize Efficacy
 Antifungal Pharmacodynamics A Strategy to Optimize Efficacy David Andes, MD Associate Professor, Department of Medicine Division of Infectious Diseases Medical Microbiology and Immunology University of
Antifungal Pharmacodynamics A Strategy to Optimize Efficacy David Andes, MD Associate Professor, Department of Medicine Division of Infectious Diseases Medical Microbiology and Immunology University of
First Report of Penicillium adametzioides from Decayed Grapes (Vitis vinifera) in Pakistan
 in Pakistan") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 12 (2016) pp. 316-320 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.512.034
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 5 Number 12 (2016) pp. 316-320 Journal homepage: http://www.ijcmas.com Original Research Article http://dx.doi.org/10.20546/ijcmas.2016.512.034
Fungal infections in ICU. Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia
 Fungal infections in ICU Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia Epidemiology of invasive fungal infections - US +300% Martin GS, et al. N Engl J Med 2003;348:1546-1554
Fungal infections in ICU Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia Epidemiology of invasive fungal infections - US +300% Martin GS, et al. N Engl J Med 2003;348:1546-1554
amphotericin B empiric therapy; preemptive therapy presumptive therapy Preemptive therapy Presumptive therapy ET targeted therapy ET
 4 17 9 27 17 1 7 amphotericin B 34 empiric therapy; ET preemptive therapy presumptive therapy Preemptive therapy Presumptive therapy ET targeted therapy ET Key words: antifungal therapyempiric therapypreemptive
4 17 9 27 17 1 7 amphotericin B 34 empiric therapy; ET preemptive therapy presumptive therapy Preemptive therapy Presumptive therapy ET targeted therapy ET Key words: antifungal therapyempiric therapypreemptive
Invasive Aspergillosis Associated Bacterial Infection in the Nasal Septum After Sphenoid Sinus Surgery
 Case Report Korean J Otorhinolaryngol-Head Neck Surg 2018;61(10):541-5 / pissn 2092-5859 / eissn 2092-6529 https://doi.org/10.3342/kjorl-hns.2017.17657 Invasive Aspergillosis Associated Bacterial Infection
Case Report Korean J Otorhinolaryngol-Head Neck Surg 2018;61(10):541-5 / pissn 2092-5859 / eissn 2092-6529 https://doi.org/10.3342/kjorl-hns.2017.17657 Invasive Aspergillosis Associated Bacterial Infection
TOWARDS PRE-EMPTIVE? TRADITIONAL DIAGNOSIS. GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% β-d-glucan Neg Predict Value 100% PCR
 TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
Research Article Invasive Fungal Rhinosinusitis versus Bacterial Rhinosinusitis with Orbital Complications: A Case-Control Study
 The Scientific World Journal Volume 2013, Article ID 453297, 5 pages http://dx.doi.org/10.1155/2013/453297 Research Article Invasive Fungal Rhinosinusitis versus Bacterial Rhinosinusitis with Orbital Complications:
The Scientific World Journal Volume 2013, Article ID 453297, 5 pages http://dx.doi.org/10.1155/2013/453297 Research Article Invasive Fungal Rhinosinusitis versus Bacterial Rhinosinusitis with Orbital Complications:
Pathophysiology and Etiology
 Sinusitis Pathophysiology and Etiology Sinusitis is inflammation of the mucosa of one or more sinuses. It can be either acute chronic. Chronic sinusitis is diagnosed if symptoms are present for more than
Sinusitis Pathophysiology and Etiology Sinusitis is inflammation of the mucosa of one or more sinuses. It can be either acute chronic. Chronic sinusitis is diagnosed if symptoms are present for more than
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Use of Antifungals in the Year 2008
 Use of Antifungals in the Year 2008 Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine Diagnosis
Use of Antifungals in the Year 2008 Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine Diagnosis
Actinomycosis and aspergillosis in the nose of a diabetic: A case report
 Volume 2 Issue 3 2012 ISSN 2250-0359 Actinomycosis and aspergillosis in the nose of a diabetic: A case report 1 Meenu Khurana Cherian 1*, Rajarajeswari 2 1 Department of ENT, Gulf Medical College Hospital
Volume 2 Issue 3 2012 ISSN 2250-0359 Actinomycosis and aspergillosis in the nose of a diabetic: A case report 1 Meenu Khurana Cherian 1*, Rajarajeswari 2 1 Department of ENT, Gulf Medical College Hospital
Invasive Fungal Rhinosinusitis: A 15-Year Experience With 29 Patients
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Invasive Fungal Rhinosinusitis: A 15-Year Experience With 29 Patients Marcus M. Monroe, MD; Max McLean, BA;
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Invasive Fungal Rhinosinusitis: A 15-Year Experience With 29 Patients Marcus M. Monroe, MD; Max McLean, BA;
ORIGINAL ARTICLE. Computed Tomographic Findings in Patients With Invasive Fungal Sinusitis
 ORIGINAL ARTICLE Computed Tomographic Findings in Patients With Invasive Fungal Sinusitis John M. DelGaudio, MD; Ron E. Swain Jr, MD; Todd T. Kingdom, MD; Susan Muller, DMD; Patricia A. Hudgins, MD Objective:
ORIGINAL ARTICLE Computed Tomographic Findings in Patients With Invasive Fungal Sinusitis John M. DelGaudio, MD; Ron E. Swain Jr, MD; Todd T. Kingdom, MD; Susan Muller, DMD; Patricia A. Hudgins, MD Objective:
Aspergillosis in the critically ill patient
 Aspergillosis in the critically ill patient José Artur Paiva Director of Emergency and Intensive Care Department Centro Hospitalar São João Porto Associate Professor of Medicine University of Porto Infection
Aspergillosis in the critically ill patient José Artur Paiva Director of Emergency and Intensive Care Department Centro Hospitalar São João Porto Associate Professor of Medicine University of Porto Infection
History of Aspergillus. History of Aspergillus. Biology of Aspergillus flavus Fungus Saphrophyte Haploid filamentous fungi Mycelium secrets enzymes
 Anthony Fossaceca Anthony Nuzzi Swati Vasireddy History of Aspergillus Pier Antonio Micheli Italian priest and Biologist Discovered the fungi in 1729 Structure Aspergillum (holy water sprinkler) Hence
Anthony Fossaceca Anthony Nuzzi Swati Vasireddy History of Aspergillus Pier Antonio Micheli Italian priest and Biologist Discovered the fungi in 1729 Structure Aspergillum (holy water sprinkler) Hence
Antifungal Resistance in Asia: Mechanisms, Epidemiology, and Consequences
 5th MMTN Conference 5-6 November 2016 Bangkok, Thailand 10:20-10:45, 6 Nov, 2016 Antifungal Resistance in Asia: Mechanisms, Epidemiology, and Consequences Yee-Chun Chen, M.D., PhD. Department of Medicine,
5th MMTN Conference 5-6 November 2016 Bangkok, Thailand 10:20-10:45, 6 Nov, 2016 Antifungal Resistance in Asia: Mechanisms, Epidemiology, and Consequences Yee-Chun Chen, M.D., PhD. Department of Medicine,
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
PROGRESSI NELLA TERAPIA ANTIFUNGINA. A tribute to Piero Martino
 PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
Rhinosinusitis. John Ramey, MD Joseph Russell, MD
 Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Antifungal Susceptibility of Aspergillus Isolates from the Respiratory Tract of Patients in Canadian Hospitals: Results of the CANWARD 2016 Study.
 1 Antifungal Susceptibility of Aspergillus Isolates from the Respiratory Tract of Patients in Canadian Hospitals: Results of the CANWARD 2016 Study. J. FULLER 1,3, A. BULL 2, S. SHOKOPLES 2, T.C. DINGLE
1 Antifungal Susceptibility of Aspergillus Isolates from the Respiratory Tract of Patients in Canadian Hospitals: Results of the CANWARD 2016 Study. J. FULLER 1,3, A. BULL 2, S. SHOKOPLES 2, T.C. DINGLE
An Update in the Management of Candidiasis
 An Update in the Management of Candidiasis Daniel B. Chastain, Pharm.D., AAHIVP Infectious Diseases Pharmacy Specialist Phoebe Putney Memorial Hospital Adjunct Clinical Assistant Professor UGA College
An Update in the Management of Candidiasis Daniel B. Chastain, Pharm.D., AAHIVP Infectious Diseases Pharmacy Specialist Phoebe Putney Memorial Hospital Adjunct Clinical Assistant Professor UGA College
EMERGING FUNGAL INFECTIONS IN IMMUNOCOMPROMISED PATIENTS
 EMERGING FUNGAL INFECTIONS IN IMMUNOCOMPROMISED PATIENTS DR LOW CHIAN YONG MBBS, MRCP(UK), MMed(Int Med), FAMS Consultant, Dept of Infectious Diseases, SGH Introduction The incidence of invasive fungal
EMERGING FUNGAL INFECTIONS IN IMMUNOCOMPROMISED PATIENTS DR LOW CHIAN YONG MBBS, MRCP(UK), MMed(Int Med), FAMS Consultant, Dept of Infectious Diseases, SGH Introduction The incidence of invasive fungal
Reverse Halo Sign in Pulmonary Mucormyosis
 QJM Advance Access published February 6, 2014 Reverse Halo Sign in Pulmonary Mucormyosis Yu-Hsiang Juan MD 1,2, Sachin S Saboo, MD FRCR 1, Yu-Ching Lin MD 2, James R. Conner MD, Ph.D 3, Francine L. Jacobson
QJM Advance Access published February 6, 2014 Reverse Halo Sign in Pulmonary Mucormyosis Yu-Hsiang Juan MD 1,2, Sachin S Saboo, MD FRCR 1, Yu-Ching Lin MD 2, James R. Conner MD, Ph.D 3, Francine L. Jacobson
Multi-clonal origin of macrolide-resistant Mycoplasma pneumoniae isolates. determined by multiple-locus variable-number tandem-repeat analysis
 JCM Accepts, published online ahead of print on 30 May 2012 J. Clin. Microbiol. doi:10.1128/jcm.00678-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Multi-clonal origin
JCM Accepts, published online ahead of print on 30 May 2012 J. Clin. Microbiol. doi:10.1128/jcm.00678-12 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Multi-clonal origin
, Aspergillus A. terreus. 4 Candida albicans. 2 Otomycosis. , Histoplasmosis Paracoccidiomycosis
 Jpn. J. Med. Mycol. Vol. 44, 277 283, 2003 ISSN 0916 4804 1 2 2 1 2, Aspergillus A. terreus, A. flavus, A. niger, Candida,. A. terreus,, CT, fungus ball, drainage,, Key words: otolaryngologic mycosis,
Jpn. J. Med. Mycol. Vol. 44, 277 283, 2003 ISSN 0916 4804 1 2 2 1 2, Aspergillus A. terreus, A. flavus, A. niger, Candida,. A. terreus,, CT, fungus ball, drainage,, Key words: otolaryngologic mycosis,
Fungal Infection Post-Infusion Data
 Fungal Infection Post-Infusion Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: Event date: / / Visit: 100 day 6 months 1 year 2 years >2 years. Specify: CIBMTR Form 2146 revision
Fungal Infection Post-Infusion Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: Event date: / / Visit: 100 day 6 months 1 year 2 years >2 years. Specify: CIBMTR Form 2146 revision
Aspergillosis in Dogs A Destructive Sinus & Nasal Disease
 Aspergillosis in Dogs A Destructive Sinus & Nasal Disease No one likes having a runny nose. Primary viral and secondary bacterial infections are common in pets and people. Most of the time these infections
Aspergillosis in Dogs A Destructive Sinus & Nasal Disease No one likes having a runny nose. Primary viral and secondary bacterial infections are common in pets and people. Most of the time these infections
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Voriconazole Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 4004 Table of Contents Coverage Policy... 1 General Background...
Cigna Drug and Biologic Coverage Policy Subject Voriconazole Effective Date... 3/15/2018 Next Review Date... 3/15/2019 Coverage Policy Number... 4004 Table of Contents Coverage Policy... 1 General Background...
Update on Antifungal Stewardship
 Update on Antifungal Stewardship Dr Jacqueline Sneddon, MRPharmS Scottish Antimicrobial Prescribing Group Antimicrobial Management Team event 7 th November 2017 ANTIFUNGAL STEERING GROUP CHAIR Prof Brian
Update on Antifungal Stewardship Dr Jacqueline Sneddon, MRPharmS Scottish Antimicrobial Prescribing Group Antimicrobial Management Team event 7 th November 2017 ANTIFUNGAL STEERING GROUP CHAIR Prof Brian
Controversies surrounding categorization of fungal sinusitis
 Controversies surrounding categorization of fungal sinusitis Arunaloke Chakrabarti Professor,Department of Medical Microbiology Center for Advanced Research in Medical Mycology Postgraduate Institute of
Controversies surrounding categorization of fungal sinusitis Arunaloke Chakrabarti Professor,Department of Medical Microbiology Center for Advanced Research in Medical Mycology Postgraduate Institute of
Mucin-Related Rhinosinusitis YOUSEF ALJATHLANY ORL-HNS RESIDENT
 Mucin-Related Rhinosinusitis YOUSEF ALJATHLANY ORL-HNS RESIDENT Free PPT Click to add title This PowerPoint Template has clean and neutral design that can be adapted to any content and meets various market
Mucin-Related Rhinosinusitis YOUSEF ALJATHLANY ORL-HNS RESIDENT Free PPT Click to add title This PowerPoint Template has clean and neutral design that can be adapted to any content and meets various market
INTERNATIONAL JOURNAL OF PHARMACEUTICAL RESEARCH AND BIO-SCIENCE
 INTERNATIONAL JOURNAL OF PHARMACEUTICAL RESEARCH AND BIO-SCIENCE RHINOCEREBRAL MUCORMYCOSIS DUE TO RHIZOPUS IN A RECENTLY DIAGNOSED DIABETIC FEMALE: A CASE REPORT KULKARNI KV 1, PATHAK NP 2 1. Assistant
INTERNATIONAL JOURNAL OF PHARMACEUTICAL RESEARCH AND BIO-SCIENCE RHINOCEREBRAL MUCORMYCOSIS DUE TO RHIZOPUS IN A RECENTLY DIAGNOSED DIABETIC FEMALE: A CASE REPORT KULKARNI KV 1, PATHAK NP 2 1. Assistant
Use of Antifungal Drugs in the Year 2006"
 Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis
 Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis Identify the structures neutrophils macrophages x40 Organisms 8 30 micron in size, with variable capsule
Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis Identify the structures neutrophils macrophages x40 Organisms 8 30 micron in size, with variable capsule
Prophylaxis, Empirical, Pre-emptive Therapy of Aspergillosis in Hematological Patients: Which Strategy?
 TIMM-4 18-21 October 2009 Athens, Greece Prophylaxis, Empirical, Pre-emptive Therapy of Aspergillosis in Hematological Patients: Which Strategy? www.ichs.org Georg Maschmeyer Dept. of Hematology, Oncology
TIMM-4 18-21 October 2009 Athens, Greece Prophylaxis, Empirical, Pre-emptive Therapy of Aspergillosis in Hematological Patients: Which Strategy? www.ichs.org Georg Maschmeyer Dept. of Hematology, Oncology
Patient s s headache is our headache
 Patient s s headache is our headache Princess Margaret Hospital Dr. Lo Man Wai / Dr. Tang Hon Lok 8 th Nov 2006 History SM Leung, F/66 DM nephropathy, HT ESRF with pre-emptive emptive cadaveric renal transplant
Patient s s headache is our headache Princess Margaret Hospital Dr. Lo Man Wai / Dr. Tang Hon Lok 8 th Nov 2006 History SM Leung, F/66 DM nephropathy, HT ESRF with pre-emptive emptive cadaveric renal transplant
Brain Abscess Caused by Schizophyllum commune: an Emerging Basidiomycete Pathogen
 JOURNAL OF CLINICAL MICROBIOLOGY, July 1996, p. 1628 1632 Vol. 34, No. 7 0095-1137/96/$04.00 0 Copyright 1996, American Society for Microbiology Brain Abscess Caused by Schizophyllum commune: an Emerging
JOURNAL OF CLINICAL MICROBIOLOGY, July 1996, p. 1628 1632 Vol. 34, No. 7 0095-1137/96/$04.00 0 Copyright 1996, American Society for Microbiology Brain Abscess Caused by Schizophyllum commune: an Emerging
Brain Abscess Caused by Schizophyllum commune: an Emerging Basidiomycete Pathogen
 JOURNAL OF CLINICAL MICROBIOLOGY, July 1996, p. 1628 1632 Vol. 34, No. 7 0095-1137/96/$04.00 0 Copyright 1996, American Society for Microbiology Brain Abscess Caused by Schizophyllum commune: an Emerging
JOURNAL OF CLINICAL MICROBIOLOGY, July 1996, p. 1628 1632 Vol. 34, No. 7 0095-1137/96/$04.00 0 Copyright 1996, American Society for Microbiology Brain Abscess Caused by Schizophyllum commune: an Emerging
Clinical relevance of resistance in Aspergillus. David W. Denning University Hospital of South Manchester [Wythenshawe Hospital]
![Clinical relevance of resistance in Aspergillus. David W. Denning University Hospital of South Manchester [Wythenshawe Hospital]](/thumbs/83/88034429.jpg "Clinical relevance of resistance in Aspergillus. David W. Denning University Hospital of South Manchester [Wythenshawe Hospital]") Clinical relevance of resistance in Aspergillus David W. Denning University Hospital of South Manchester [Wythenshawe Hospital] The University of Manchester Steps to establishing clinical validity of resistance/susceptibility
Clinical relevance of resistance in Aspergillus David W. Denning University Hospital of South Manchester [Wythenshawe Hospital] The University of Manchester Steps to establishing clinical validity of resistance/susceptibility
Patient s s headache is our headache
 History Patient s s headache is our headache Princess Margaret Hospital Dr. Lo Man Wai / Dr. Tang Hon Lok 8 th Nov 2006 SM Leung, F/66 DM nephropathy, HT ESRF with pre-emptive emptive cadaveric renal transplant
History Patient s s headache is our headache Princess Margaret Hospital Dr. Lo Man Wai / Dr. Tang Hon Lok 8 th Nov 2006 SM Leung, F/66 DM nephropathy, HT ESRF with pre-emptive emptive cadaveric renal transplant
Evidence-Based Approaches to the Safe and Effective Management of Invasive Fungal Infections. Presenter. Disclosures
 Evidence-Based Approaches to the Safe and Effective Management of Invasive Fungal Infections Presenter James S. Lewis II, PharmD, FIDSA ID Clinical Pharmacy Coordinator Oregon Health and Science University
Evidence-Based Approaches to the Safe and Effective Management of Invasive Fungal Infections Presenter James S. Lewis II, PharmD, FIDSA ID Clinical Pharmacy Coordinator Oregon Health and Science University
Case Report Mixed Fungal Infection (Aspergillus, Mucor,andCandida)of Severe Hand Injury
of Severe Hand Injury") , Article ID 954186, 4 pages http://dx.doi.org/10.1155/2014/954186 Case Report Mixed Fungal Infection (Aspergillus, Mucor,andCandida)of Severe Hand Injury Milana Obradovic-Tomasev, 1,2 Aleksandra Popovic,
, Article ID 954186, 4 pages http://dx.doi.org/10.1155/2014/954186 Case Report Mixed Fungal Infection (Aspergillus, Mucor,andCandida)of Severe Hand Injury Milana Obradovic-Tomasev, 1,2 Aleksandra Popovic,
Micafungin and Candida spp. Rationale for the EUCAST clinical breakpoints. Version February 2013
 Micafungin and Candida spp. Rationale for the EUCAST clinical breakpoints. Version 1.0 5 February 2013 Foreword EUCAST The European Committee on Antimicrobial Susceptibility Testing (EUCAST) is organised
Micafungin and Candida spp. Rationale for the EUCAST clinical breakpoints. Version 1.0 5 February 2013 Foreword EUCAST The European Committee on Antimicrobial Susceptibility Testing (EUCAST) is organised
Pott s Puffy Tumor. Shahad Almohanna 15/1/2018
 Pott s Puffy Tumor Shahad Almohanna R2 15/1/2018 Definition First described in 1760 by Sir Percival Pott. s he originally suggested that trauma of the frontal bone was causative for this lesion, but later,
Pott s Puffy Tumor Shahad Almohanna R2 15/1/2018 Definition First described in 1760 by Sir Percival Pott. s he originally suggested that trauma of the frontal bone was causative for this lesion, but later,
CURRENT AND NEWER ANTI-FUNGAL THERAPIES- MECHANISMS, INDICATIONS, LIMITATIONS AND PROBLEMS. Dr AMIT RAODEO DM SEMINAR
 CURRENT AND NEWER ANTI-FUNGAL THERAPIES- MECHANISMS, INDICATIONS, LIMITATIONS AND PROBLEMS Dr AMIT RAODEO DM SEMINAR Introduction The incidence of invasive fungal infections in critically ill intensive
CURRENT AND NEWER ANTI-FUNGAL THERAPIES- MECHANISMS, INDICATIONS, LIMITATIONS AND PROBLEMS Dr AMIT RAODEO DM SEMINAR Introduction The incidence of invasive fungal infections in critically ill intensive
Mycology Reference Centre, Leeds Information for Service Users 2017
 The Leeds Teaching Hospitals NHS Trust NHS Mycology Reference Centre, Leeds Information for Service Users 2017 Contents Contents...1 The Mycology Reference Centre...1 Request Forms... 1 Specimen Transportation...
The Leeds Teaching Hospitals NHS Trust NHS Mycology Reference Centre, Leeds Information for Service Users 2017 Contents Contents...1 The Mycology Reference Centre...1 Request Forms... 1 Specimen Transportation...
Fungal Infections in Neutropenic Hematological Disorders
 Fungal Infections in Neutropenic Hematological Disorders 23 Dr Farah Jijina 24 Fungal Infections in Neutropenic Hematological Disorders 25 Dr Farah Jijina 26 Fungal Infections in Neutropenic Hematological
Fungal Infections in Neutropenic Hematological Disorders 23 Dr Farah Jijina 24 Fungal Infections in Neutropenic Hematological Disorders 25 Dr Farah Jijina 26 Fungal Infections in Neutropenic Hematological
Antifungals and current treatment guidelines in pediatrics and neonatology
 Dragana Janic Antifungals and current treatment guidelines in pediatrics and neonatology Dragana Janic. University Children`s Hospital, Belgrade, Serbia 10/10/17 Hotel Crowne Plaza, Belgrade, Serbia; www.dtfd.org
Dragana Janic Antifungals and current treatment guidelines in pediatrics and neonatology Dragana Janic. University Children`s Hospital, Belgrade, Serbia 10/10/17 Hotel Crowne Plaza, Belgrade, Serbia; www.dtfd.org
In vitro cross-resistance between azoles in Aspergillus fumigatus: a reason for concern in the clinic?
 4 th Congress on Trends in Medical Mycology (TIMM) In vitro cross-resistance between azoles in Aspergillus fumigatus: a reason for concern in the clinic? Emilia Mellado Mycolgy Reference Laboratory Centro
4 th Congress on Trends in Medical Mycology (TIMM) In vitro cross-resistance between azoles in Aspergillus fumigatus: a reason for concern in the clinic? Emilia Mellado Mycolgy Reference Laboratory Centro
Received 18 December 2008/Returned for modification 9 February 2009/Accepted 9 April 2009
 JOURNAL OF CLINICAL MICROBIOLOGY, June 2009, p. 1942 1946 Vol. 47, No. 6 0095-1137/09/$08.00 0 doi:10.1128/jcm.02434-08 Copyright 2009, American Society for Microbiology. All Rights Reserved. Activity
JOURNAL OF CLINICAL MICROBIOLOGY, June 2009, p. 1942 1946 Vol. 47, No. 6 0095-1137/09/$08.00 0 doi:10.1128/jcm.02434-08 Copyright 2009, American Society for Microbiology. All Rights Reserved. Activity
Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients
 BVIKM-SBIMC La Hulpe, 6 November 2008 Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients Johan Maertens, MD Acute Leukemia and SCT Unit University Hospital Gasthuisberg Catholic
BVIKM-SBIMC La Hulpe, 6 November 2008 Antifungals in Invasive Fungal Infections: Antifungals in neutropenic patients Johan Maertens, MD Acute Leukemia and SCT Unit University Hospital Gasthuisberg Catholic
EMA Pediatric Web Synopsis Protocol A November 2011 Final PFIZER INC.
 PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
Fungal Rhinosinusitis: Report of uncommon Aspergillus species as etiological agents
 www.edoriumjournals.com Case SERIES OPEN ACCESS Fungal Rhinosinusitis: Report of uncommon Aspergillus species as etiological agents Chadiesh Nagarajan, Premamalini Thayanidhi, Anupma J Kindo, Vijayakumar
www.edoriumjournals.com Case SERIES OPEN ACCESS Fungal Rhinosinusitis: Report of uncommon Aspergillus species as etiological agents Chadiesh Nagarajan, Premamalini Thayanidhi, Anupma J Kindo, Vijayakumar
Tailored Antifungal Modification in Breakthrough Mold Infections. Russell E. Lewis University of Bologna
 Tailored Antifungal Modification in Breakthrough Mold Infections Russell E. Lewis University of Bologna 45 year-old patient with AML and documented pulmonary aspergillosis during remissioninduction chemotherapy
Tailored Antifungal Modification in Breakthrough Mold Infections Russell E. Lewis University of Bologna 45 year-old patient with AML and documented pulmonary aspergillosis during remissioninduction chemotherapy
Guideline for the Management of Fever and Neutropenia in Children with Cancer and/or Undergoing Hematopoietic Stem-Cell Transplantation
 Guideline for the Management of Fever Neutropenia in Children with Cancer /or Undergoing Hematopoietic Stem-Cell Transplantation COG Supportive Care Endorsed Guidelines Click here to see all the COG Supportive
Guideline for the Management of Fever Neutropenia in Children with Cancer /or Undergoing Hematopoietic Stem-Cell Transplantation COG Supportive Care Endorsed Guidelines Click here to see all the COG Supportive
Fungal infection in the immunocompromised patient. Dr Kirsty Dodgson
 Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Staphylococci. Gram stain: gram positive cocci arranged in clusters.
 Microbiology lab Respiratory system Third medical year Lab contents: Gram positive bacteria (Staphylococcus and Streptococcus spp), two types of filamentous fungi (Aspergillus and Penicillium spp), and
Microbiology lab Respiratory system Third medical year Lab contents: Gram positive bacteria (Staphylococcus and Streptococcus spp), two types of filamentous fungi (Aspergillus and Penicillium spp), and
Therapy of Hematologic Malignancies Period at high risk of IFI
 Therapy of Hematologic Malignancies Period at high risk of IFI Neutrophils (/mm 3 ) 5 Chemotherapy Conditioning Regimen HSCT Engraftment GVHD + Immunosuppressive Treatment Cutaneous and mucositis : - Direct
Therapy of Hematologic Malignancies Period at high risk of IFI Neutrophils (/mm 3 ) 5 Chemotherapy Conditioning Regimen HSCT Engraftment GVHD + Immunosuppressive Treatment Cutaneous and mucositis : - Direct
ISHAM Symposium: S33: Ocular aspects of Fungal Infections Friday, 8 May 2015, ; MR101/102 Level 1
 ISHAM Symposium: S33: Ocular aspects of Fungal Infections Friday, 8 May 2015, 14.15 15.45; MR101/102 Level 1 Chairs: Ariya Chindamporn, TH and Phillip A Thomas, IN 14:15-14:35 AGENDA Clinical overview
ISHAM Symposium: S33: Ocular aspects of Fungal Infections Friday, 8 May 2015, 14.15 15.45; MR101/102 Level 1 Chairs: Ariya Chindamporn, TH and Phillip A Thomas, IN 14:15-14:35 AGENDA Clinical overview
Controversies in management: prophylaxis or diagnostics
 5 th Advances Against Aspergillosis Controversies in management: prophylaxis or diagnostics Caveats in the use of biological markers for early diagnosis Drosos E. Karageorgopoulos, MD Researcher, Alfa
5 th Advances Against Aspergillosis Controversies in management: prophylaxis or diagnostics Caveats in the use of biological markers for early diagnosis Drosos E. Karageorgopoulos, MD Researcher, Alfa
Therapeutic Drug Monitoring in Antifungal Therapy. Why, When and How
 Therapeutic Drug Monitoring in Antifungal Therapy Why, When and How Roger Brüggemann Radboud University Nijmegen Medical Centre and Nijmegen Institute for Infection, Inflammation and Immunology (N4i) Trends
Therapeutic Drug Monitoring in Antifungal Therapy Why, When and How Roger Brüggemann Radboud University Nijmegen Medical Centre and Nijmegen Institute for Infection, Inflammation and Immunology (N4i) Trends
Fungal infections. Ematologia. Corrado Girmenia. Ematologia, Azienda Policlinico Umberto I Sapienza University of Rome, Italy
 Fungal infections Corrado Girmenia Ematologia, Azienda Policlinico Umberto I Sapienza University of Rome, Italy Ematologia Epidemiology Diagnostic approach Prevention strategies Monitoring of IFDs in
Fungal infections Corrado Girmenia Ematologia, Azienda Policlinico Umberto I Sapienza University of Rome, Italy Ematologia Epidemiology Diagnostic approach Prevention strategies Monitoring of IFDs in
Presentation of Invasive Fungal Rhinosinusitis in Sudanese Children: A Report of Four Cases
 Volume 13, Issue no. 2, DOI 10.18502/sjms.v13i2.2643 Production and Hosting by Knowledge E Case Report Presentation of Invasive Fungal Rhinosinusitis in Sudanese Children: A Report of Four Cases Faculty
Volume 13, Issue no. 2, DOI 10.18502/sjms.v13i2.2643 Production and Hosting by Knowledge E Case Report Presentation of Invasive Fungal Rhinosinusitis in Sudanese Children: A Report of Four Cases Faculty
CASE REPORT POST-OPERATIVE ENDOPHTHALMITIS DUE TO FUSARIUM DIMERUM
 CASE REPORT POST-OPERATIVE ENDOPHTHALMITIS DUE TO FUSARIUM DIMERUM Sadia Khan 1, Gopal S Pillai 2, V Vivek 1, Kavitha Dinesh 1 and PM Shamsul Karim 1 1 Department of Microbiology, 2 Department of Ophthalmology,
CASE REPORT POST-OPERATIVE ENDOPHTHALMITIS DUE TO FUSARIUM DIMERUM Sadia Khan 1, Gopal S Pillai 2, V Vivek 1, Kavitha Dinesh 1 and PM Shamsul Karim 1 1 Department of Microbiology, 2 Department of Ophthalmology,
Antifungal susceptibility testing: Which method and when?
 Antifungal susceptibility testing: Which method and when? Maiken Cavling Arendrup mad@ssi.dk SSI & Juan Luis Rodriguez Tudela jlrtudela@isciii.es ISCIII Agenda Summary of current standards and selected
Antifungal susceptibility testing: Which method and when? Maiken Cavling Arendrup mad@ssi.dk SSI & Juan Luis Rodriguez Tudela jlrtudela@isciii.es ISCIII Agenda Summary of current standards and selected
Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting
 Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting Professor Retno Wahyuningsih Professor of Medical Mycology Department of Parasitology, Faculty of Medicine Universitas
Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting Professor Retno Wahyuningsih Professor of Medical Mycology Department of Parasitology, Faculty of Medicine Universitas