Histoplasma, Coccidioides, Aspergillus, Other Systemic Fungal Pathogens And Paragonimus westermani
|
|
|
- Susan Cook
- 5 years ago
- Views:
Transcription
1 Histoplasma, Coccidioides, Aspergillus, Other Systemic Fungal Pathogens And Paragonimus westermani Dr. Sameer Naji, MB, BCh, PhD (UK) Dept. of Basic Medical Sciences Faculty of Medicine The Hashemite University
2 H i s t o p l a s m a c a p s u l a t u m Histoplasma capsulatum is a dimorphic fungus that grows in the yeast phase in tissue and in cultures incubated at 37 C. The mold phase grows in cultures incubated at 22 to 25 C and as a saprophyte in soil. The yeast forms are small for fungi (2 to 4 µm) and reproduce by budding (blastoconidia). The mycelia are septate and produce microconidia and macroconidia. Growth is obtained on blood agar, chocolate agar, and Sabouraud s agar, but may take many weeks.

3
4 DIMORPHISM The morphologic and physiologic events associated with conversion from the mold to the yeast phase of H. capsulatum have been extensively studied. They are understandably complex given the dramatic change of milieu encountered by the fungus when its mold conidia float from their soil habitat to the pulmonary alveoli. Conversion to the yeast phase is then triggered by the host temperature (37 C) and possibly by other aspects of the new environment. In vitro studies show that the earliest events in this shift from the mold to yeast form involve induction of the heat shock response and uncoupling of oxidative phosphorylation. Dimorphism in fungi is reversible, a feature that distinguishes it from developmental processes such as embryogenesis seen in higher eukaryotes.
5 H I S T O P L A S M O S I S Histoplasmosis is limited to the endemic area, where the vast majority of cases are asymptomatic or show only a fever and cough. If affected individuals are seen by a physician, a pulmonary infiltrate and hilar adenopathy may or may not be evident on a radiograph. Progressive cases show extension in the lung or enlargement of lymph nodes, liver, and spleen.
6 EPIDEMIOLOGY H. capsulatum grows in soil under humid climatic conditions, particularly soil containing bird or bat droppings. Inhalation of the mold microconidia, which are small enough (2 to 5 µm) to reach the terminal bronchioles and alveoli, is believed to be the mode of infection. The organism has a worldwide distribution but is particularly prevalent in certain temperate, subtropical, and tropical zones. The infection is not transmitted from person to person. Disease is more common in men but there are no racial or ethnic differences in susceptibility.
7 PATHOGENESIS The hallmark of histoplasmosis is infection of the lymph nodes, spleen, bone marrow, and other elements of the reticuloendothelial system with intracellular growth in phagocytic macrophages. The initial infection is pulmonary, through inhalation of infectious conidia, which convert to the yeast form in the host. They attach to CD18 integrin receptors and are readily phagocytosed by macrophages and PMNs. Inside phagocytes, they continue to multiply in the cytoplasm, surviving the combined effects of the oxidative burst and phagolysosomal fusion. With continued growth, there is lymphatic spread and development of a primary lesion similar to that seen in tuberculosis. Pathologically, granulomatous inflammation with necrosis is prominent in pulmonary lesions, but H. capsulatum may be difficult to detect, even with special fungal stains.
8 IMMUNITY Infection with H. capsulatum is associated with the development of cell-mediated immunity, as demonstrated by a positive delayed hypersensitivity skin test to a mycelial antigen called histoplasmin. Infection is believed to confer long-lasting immunity, the most important component of which is CD4+ T lymphocyte mediated.
9 C L I N I C A L A S P E C T S H I S T O P L A S M O S I S MANIFESTATIONS Most cases of H. capsulatum infection are asymptomatic or show only fever and cough for a few days or weeks. Mediastinal lymphadenopathy and slight pulmonary infiltrates may be seen on x-rays. The histoplasmin skin test becomes positive after about 3 weeks. More severe cases may have chills, malaise, chest pain, and more extensive infiltrates, which usually resolve nonetheless. A residual nodule may continue to enlarge over a period of years, causing a differential diagnostic problem with pulmonary neoplasms. Progressive pulmonary disease occurs in a form similar to that of pulmonary tuberculosis, including the development of cavities, with sputum production, night sweats, and weight loss. The course is chronic and relapsing, lasting many months to years. Disseminated histoplasmosis generally appears as a febrile illness with enlargement of reticuloendothelial organs.
10 DIAGNOSIS In most forms of pulmonary histoplasmosis, the diagnostic yield of direct examinations or culture of sputum is low. In disseminated disease, blood culture or biopsy samples of a reticuloendothelial organ are the most likely to contain Histoplasma. Bone marrow culture has the highest yield. Because of their small size, the yeast cells are difficult to see in potassium hydroxide (KOH) preparations, and their morphology is not sufficiently distinctive to be diagnostic. Selective fungal stains such as methenamine silver demonstrate the organism but may not differentiate it from other yeasts. Hematoxylin and eosin (H& E)-stained tissue or Wright-stained bone marrow often demonstrates the organisms in their intracellular location in macrophages.
11 TREATMENT Primary infections and localized lung lesions usually resolve without treatment. Amphotericin B remains the treatment of choice, but its toxicity limits its use to cases of extensive disease such as progressive pulmonary and disseminated histoplasmosis. Itraconazole and ketoconazole have been effective for treatment and for suppression in AIDS patients with histoplasmosis. In some cases amphotericin B treatment may be followed with a course of itraconazole.
12 C o c c i d i o i d e s i m m i t i s Coccidioides immitis is also a dimorphic fungus, but instead of a yeast phase, a large (12 to 100µm), distinctive, round-walled spherule is produced in the invasive tissue form. This structure is unique among the pathogenic fungi. In alkaline soils and in culture, C. immitis grows only as a mold regardless of temperature. Growth becomes visible in 2 to 5 days. The hyphae are septate and produce thickwalled, barrel-shaped arthroconidia which are the infectious unit in nature and highly infectious when they develop in the laboratory.

13
14 C O C C I D I O I D O M Y C O S I S Acute primary infection with C. immitis is either asymptomatic or presents as a complex called valley fever by residents of the endemic areas. Valley fever includes fever, malaise, dry cough, joint pains, and sometimes a rash. There are few physical or radiologic findings, but the illness persists for weeks. Disseminated disease involves lesions in the bones, joints, skin, and a progressive chronic meningitis.
15 EPIDEMIOLOGY Coccidioidomycosis is the most geographically restricted of the systemic mycoses, because C. immitis grows only in the alkaline soil. Coccidioidomycosis is not transmissible from person to person. It is geographically restricted to Sonoran desert. High proportion of locals have been infected. Arthroconidia can be spread by dust storms. Rainfall pattern influences attack rate.
16 PATHOGENESIS Inhaled arthroconidia are small enough (2 to 6 µm) to bypass the defenses of the upper tracheobronchial tree and lodge in the terminal bronchioles. Human monocytes can ingest and kill some arthroconidia on initial exposure, although the outer portion of the wall of the arthroconidium has antiphagocytic properties, which persist in the early stages of spherule development.
17 IMMUNITY Lifelong immunity to coccidioidomycosis clearly develops in the vast majority of those who become infected. This immunity is associated with strong polymorphonuclear leukocyte and T lymphocyte-mediated responses to coccidioidal antigens. In most cases, a mixed inflammatory response is associated with early resolution of the infection and development of a positive delayed hypersensitivity skin test. Progressive disease is associated with weak or absent cellular immunity and skin test anergy. In most infected persons the infection is controlled after mild or inapparent illness. The disease progresses if cell-mediated immunity and consequent macrophage activation do not develop. Such immune deficits may be a result of disease (AIDS) or immunosuppressive therapy but may occur in persons with no other known cellular immune compromise. Humoral mechanisms are not known to play any role in immunity.
18 C O C C I D I O I D O M Y C O S I S C L I N I C A L A S P E C T S MANIFESTATIONS More than one half of those infected with C. immitis suffer no symptoms, or the disease is so mild that it cannot be recalled when skin test conversion is discovered. Others develop malaise, cough, chest pain, fever, and arthralgia 1 to 3 weeks after infection. This disease, which lasts 2 to 6 weeks, is known as valley fever by the local populations in the United States. Objective findings are few. The chest x-ray is usually clear or shows only hilar adenopathy. Erythema nodosum may develop midway through the course, particularly in women. In most cases, resolution is spontaneous but only after considerable discomfort and loss of productivity. Disseminated disease is more common in men; in dark-skinned races, particularly Filipinos; and in AIDS patients and other immunosuppressed persons. Evidence of extrapulmonary infection almost always appears in the first year after infection. If untreated, the disease is slowly progressive and fatal.
19 DIAGNOSIS With enough persistence, direct examinations are usually rewarding. The thick-walled spherules are so large and characteristic that they are difficult to miss in a KOH preparation or biopsy section. Skin and visceral lesions are most likely to demonstrate spherules; CSF is least likely. Culture of C. immitis from sputum, visceral lesions, or skin lesions is not difficult. Skin and serologic tests are particularly useful in diagnosis and management of coccidioidomycosis. The coccidioidin skin test usually becomes positive 1 to 4 weeks after the onset of symptoms of primary infection and remains so for life.
20 TREATMENT Primary coccidioidomycosis is self-limiting, and no antifungal therapy is indicated. Progressive pulmonary disease and disseminated disease require the use of antifungal agents, usually amphotericin B. Ketoconazole has proved effective, but relapses are common. Fluconazole and itraconazole are also active against C. immitis. With the exception of fluconazole, none of these agents have significant penetration into the CNS. Amphotericin B is commonly given directly into the CSF for the treatment of C. immitis meningitis.
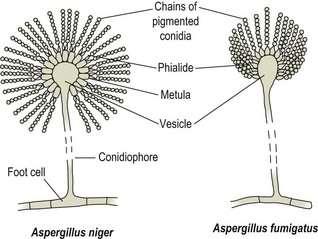
21 ASPERGILLUS M Y C O L O G Y Aspergillus species are rapidly growing molds with branching septate hyphae and characteristic arrangement of conidia on the conidiophore. Fluffy colonies appear in 1 to 2 days and, by 5 days, may cover an entire plate with pigmented growth. Species are defined on the basis of differences in the structure of the conidiophore and the arrangement of the conidia. The most frequent in human infections are Aspergillus fumigatus and Aspergillus flavus, but others, such as Aspergillus niger, may be involved.

22
23 A S P E R G I L L O S I S Invasive aspergillosis is distinguished by its setting in immunocompromised individuals and its rapid progression to death. The typical patient is one with leukemia or under immunosuppression for a bone marrow transplant. The appearance of fever and a dry cough may be the only signs until pulmonary infiltrates are demonstrated radiologically. Until Aspergillus hyphae are demonstrated, almost any of the causes of pneumonia could be responsible.
24 EPIDEMIOLOGY Aspergillus species are widely distributed in nature and found throughout the world. They seem to adapt to a wide range of environmental conditions, and the heat-resistant conidia provide a good mechanism for dispersal. Like bacteria spores, the conida survive well in the environment and their inhalation is the mode of infection. Hospital air and air ducts have received attention as sources of nosocomial Aspergillus isolates. Occasionally, construction, remodelling, or other kinds of major environmental disruption have been associated with increased frequency of Aspergillus contamination, colonization, or infection.
25 PATHOGENESIS Aspergillus conidia are small enough to readily reach the alveoli when inhaled, but disease is rare in those without compromised defenses. Factors that aid the fungus in the initial stages are not known, but the ability of proteins on the surface of the conidia to bind fibrinogen and laminin probably contribute to adherence. Production of extracellular elastase, proteinases, and phospholipases has been associated with the more virulent species. The appearance of antibodies to these enzymes during and following invasive aspergillosis argues for their importance, but the pathogenic role of these enzymes remains to be demonstrated. Most species produce aflatoxins and other toxic secondary metabolites but their role in infection is also unknown.
26 IMMUNITY Macrophages, particularly pulmonary macrophages, are the first line of defense against inhaled Aspergillus conidia phagocytosing and killing them by nonoxidative mechanisms. For the conidia that survive and germinate, PMNs become the primary defense. They are able to attach to the growing hyphae, generate an oxidative burst, and secrete reactive oxygen intermediates. Little is known of adaptive immunity in humans. Antibodies are formed but their protective value is unknown. Although AIDS patients do develop Aspergillus infections, the association with T-cell deficiencies is not strong enough to draw conclusions about their importance.
27 A S P E R G I L L O S I S C L I N I C A L A S P E C T S MANIFESTATIONS Aspergillus can cause clinical allergies or occasional invasive infection. In both cases, the lung is the organ primarily involved. Allergic aspergillosis, which can be a mechanism of exacerbation in patients with asthma, is characterized by transient pulmonary infiltrates, eosinophilia, and a rise in Aspergillus-specific antibodies. These conditions follow direct inhalation of fungal elements or, more commonly, colonization of the respiratory tract. Areas of the bronchopulmonary tree with poor drainage because of underlying disease or anatomic abnormalities may serve as a site for growth of organisms and continuous seeding with antigen.
28 Invasive aspergillosis occurs in the settings of pre-existing pulmonary disease (bronchiectasis, chronic bronchitis, asthma, tuberculosis) or immunosuppression. Colonization with Aspergillus can lead to invasion into the tissue by branching septate hyphae. In patients who already have a chronic pulmonary disease, mycelial masses can form a radiologically visible fungus ball (aspergilloma) within a pre-existing cavity. An acute pneumonia may occur in severely immunocompromised patients, particularly those with phagocyte defects or depressed neutrophil counts due to immunosuppressive drugs. Multifocal pulmonary infiltrates expanding to consolidation are present with high fever. The prognosis is grave and dissemination to other organs common, which is not the case in immunocompetent hosts.
29 DIAGNOSIS Aspergillus is relatively easy to isolate and identify. Its rapidly spreading mold growth. The diagnostic problem is distinguishing contamination and colonization with Aspergillus from invasive disease. The diagnosis cannot be made for certain without the use of lung aspiration, biopsy, or bronchoalveolar lavage. With material directly from the lesion, the presence of large, branching, septate hyphae and a positive culture are diagnostic. Serologic methods have been developed to demonstrate Aspergillus antibodies. Although these tests may be helpful in suggesting allergic aspergillosis, they have little value in invasive disease because anti-aspergillus antibody is common in healthy persons.
30 TREATMENT AND PREVENTION Amphotericin B and itraconazole are the recommended antimicrobics for invasive aspergillosis. Neither can be considered particularly effective, because the mortality rate of invasive disease approaches 100%. In cases with pulmonary structural abnormalities and fungus balls, chemotherapy has little effect. Surgical removal of localized lesion is sometimes helpful, even in the brain. Construction of rooms with filtered air has been attempted to reduce exposure to environmental conidia.
31 P A R A G O N I M U S S P E C I E S Several Paragonimus species may infect humans. P. westermani, which is widely distributed in East Asia, is the species most frequently involved. The short, plump (10 by 5 mm), reddish-brown adults are characteristically found encapsulated in the pulmonary parenchyma of their definitive host. Here they deposit operculate, goldenbrown eggs, which are distinguished from similar structures by their size (50 by 90 µm) and prominent periopercular shoulder. When the capsule erodes into a bronchiole, the eggs are coughed up and spat out or swallowed and passed in the stool. If they reach fresh water, they embryonate several weeks before the ciliated miracidia emerge through the open opercula.
32 After invasion of an appropriate snail host, 3 to 5 months pass before cercariae are released. These larval forms invade the gills, musculature, and viscera of certain crayfish or freshwater crabs; over 6 to 8 weeks, the larval forms transform into metacercariae. When the raw or undercooked flesh of the second intermediate host is ingested by humans, the metacercariae encyst in the duodenum and burrow through the gut wall into the peritoneal cavity. The majority continue their migration through the diaphragm and reach maturity in the lungs 5 to 6 weeks later. Immature ectopic adults in the striated muscles of the pig may infect humans after ingestion of undercooked pork.
33 P A R A G O N I M I A S I S ( L U N G F L U K E I N F E C T I O N ) EPIDEMIOLOGY Although most of the human infections are concentrated in the Far East, paragonimiasis has recently been described in India, Africa, Latin America, eastern Canada and the USA. Approximately 1% of recent Indochinese immigrants to the United States are found to be infected with P. westermani. Human disease occurs when food shortages or local customs expose individuals to infected crabs. When these crustaceans are prepared for cooking, juice containing metacercariae may be left behind on the working surface and contaminate other foods subsequently prepared in the same area.

34
35 P A R A G O N I M I A S I S C L I N I C A L A S P E C T S MANIFESTATIONS The presence of the adult worms in the lung elicits an eosinophilic inflammatory reaction and, eventually, the formation of a 1 to 2 cm fibrous capsule that surrounds and encloses one or more parasites. With the onset of oviposition, the capsule swells and erodes into a bronchiole, resulting in expectoration of the brownish eggs, blood, and an inflammatory exudate. Secondary bacterial infection of the evacuated cysts is common, producing a clinical picture of chronic bronchitis or bronchiectasis. When cysts rupture into the pleural cavity, chest pain and effusion can result.
36 DIAGNOSIS Eggs are usually absent from the sputum during the first 3 months of overt infection; however, repeated examinations eventually demonstrate them in more than 75% of infected patients. When a pleural effusion is present, it should be checked for eggs. Stool examination is frequently helpful, particularly in children who swallow their expectorated sputum. A diagnosis in these cases, however, often depends on the detection of circulating antibodies. Their presence usually correlates well with acute disease and disappears with successful therapy.
37 TREATMENT AND PREVENTION The disease responds well to praziquantel or bithionol therapy. Control requires adequate cooking of shellfish before ingestion.
Lecture 7: Mycoses Caused by Dimorphic Fungi, Part I
 BIOL 4849 Medical Mycology Summer 2006 Histoplasmosis Lecture 7: Mycoses Caused by Dimorphic Fungi, Part I u Most common endemic mycotic disease in the United States u Two different varieties (actually
BIOL 4849 Medical Mycology Summer 2006 Histoplasmosis Lecture 7: Mycoses Caused by Dimorphic Fungi, Part I u Most common endemic mycotic disease in the United States u Two different varieties (actually
Fungal Diseases of the Respiratory System
 Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
Fungal Diseases of the Respiratory System Histoplasmosis(cave disease) Dr. Hala Al Daghistani Histoplasmosis is a disease caused by the fungus Histoplasma capsulatum. Histoplasma capsulatum, is usually
Introduction. Study of fungi called mycology.
 Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
Fungi Introduction Study of fungi called mycology. Some fungi are beneficial: ex a) Important in production of some foods, ex: cheeses, bread. b) Important in production of some antibiotics, ex: penicillin
8/2/10. Sanaz Jalali, Jennifer Demler, Jeremy King. Histoplasmosis is an intracellular mycotic infection of the reticuloendothelial system.
 Histoplasmosis is an intracellular mycotic infection of the reticuloendothelial system. Type of chronic respiratory infection http://www.eregimens.com/regimens/antifungal%20general.htm Sanaz Jalali, Jennifer
Histoplasmosis is an intracellular mycotic infection of the reticuloendothelial system. Type of chronic respiratory infection http://www.eregimens.com/regimens/antifungal%20general.htm Sanaz Jalali, Jennifer
Histoplasmosis. Disease Etiology: Disease Transmission: Reservoirs: Specific Microbial Characteristics: By: Ernest Aguilar
 Histoplasmosis By: Ernest Aguilar Disease Etiology: Histoplasmosis is an infection resulting from the inhalation of spores belonging to the fungus Histoplasma capsulatum. [1] This one of three fungi that
Histoplasmosis By: Ernest Aguilar Disease Etiology: Histoplasmosis is an infection resulting from the inhalation of spores belonging to the fungus Histoplasma capsulatum. [1] This one of three fungi that
PARASITOLOGY CASE HISTORY #82 (Lynne S. Garcia)
") PARASITOLOGY CASE HISTORY #82 (Lynne S. Garcia) ***Reminder: Slides are copyrighted and cannot be copied for publication. A 57 year old male was seen at a local clinic with a year-long history of productive
PARASITOLOGY CASE HISTORY #82 (Lynne S. Garcia) ***Reminder: Slides are copyrighted and cannot be copied for publication. A 57 year old male was seen at a local clinic with a year-long history of productive
Fungal Infections. Fungal Infections
 Fungal Infection in the Immune Competent Host Steven L. Primack, MD Fungal Infection in the Immune Competent Host Steven L. Primack, MD Department of Radiology Oregon Health & Science University Fungal
Fungal Infection in the Immune Competent Host Steven L. Primack, MD Fungal Infection in the Immune Competent Host Steven L. Primack, MD Department of Radiology Oregon Health & Science University Fungal
Ex. Schistosoma species (blood flukes) and Fasciola hepatica.
 and Fasciola hepatica.") TREMATODES: INTRODUCTION: Ex. Schistosoma species (blood flukes) and Fasciola hepatica. The life cycle of trematodes involves a sexual cycle in humans and asexual reproduction in freshwater snails (intermediate
TREMATODES: INTRODUCTION: Ex. Schistosoma species (blood flukes) and Fasciola hepatica. The life cycle of trematodes involves a sexual cycle in humans and asexual reproduction in freshwater snails (intermediate
Alberta Health and Wellness Public Health Disease Under Surveillance Management Guidelines March 2011
 March 2011 Histoplasmosis Case Definition Confirmed Case Clinical illness [1] with laboratory confirmation of infection: Isolation of Histoplasma capsulatum from an appropriate clinical specimen (tissue
March 2011 Histoplasmosis Case Definition Confirmed Case Clinical illness [1] with laboratory confirmation of infection: Isolation of Histoplasma capsulatum from an appropriate clinical specimen (tissue
California digging. Task 1 Interpret the chest radiograph. L. Hendriks
 Case history An18-yr-old male presented at the emergency department with a 4-week history of fever, coughing and dyspnoea. Symptoms presented on a holiday in California (USA) searching the desert for fossils.
Case history An18-yr-old male presented at the emergency department with a 4-week history of fever, coughing and dyspnoea. Symptoms presented on a holiday in California (USA) searching the desert for fossils.
HISTOPLASMOSIS - LABORATORY DIAGNOSIS IN VIETNAM
 HISTOPLASMOSIS - LABORATORY DIAGNOSIS IN VIETNAM National Institute of Hygiene and Epidemiology, Hanoi, Vietnam, National Institute of Infectious Diseases, Tokyo, Japan, Bach Mai hospital, Vietnam, Military
HISTOPLASMOSIS - LABORATORY DIAGNOSIS IN VIETNAM National Institute of Hygiene and Epidemiology, Hanoi, Vietnam, National Institute of Infectious Diseases, Tokyo, Japan, Bach Mai hospital, Vietnam, Military
Medical Virology Immunology. Dr. Sameer Naji, MB, BCh, PhD (UK) Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University
 Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University") Medical Virology Immunology Dr. Sameer Naji, MB, BCh, PhD (UK) Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University Human blood cells Phases of immune responses Microbe Naïve
Medical Virology Immunology Dr. Sameer Naji, MB, BCh, PhD (UK) Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University Human blood cells Phases of immune responses Microbe Naïve
Fungal biology. Fungal Infections. Fungal cell structure. Pathogenesis
 Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Yersinia pestis. Yersinia and plague. Dr. Hala Al Daghistani
 Yersinia pestis Dr. Hala Al Daghistani Yersinia species Short, pleomorphic gram-negative rods that can exhibit bipolar staining. Catalase positive, and microaerophilic or facultatively anaerobic. Animals
Yersinia pestis Dr. Hala Al Daghistani Yersinia species Short, pleomorphic gram-negative rods that can exhibit bipolar staining. Catalase positive, and microaerophilic or facultatively anaerobic. Animals
Fungal biology. Pathogenesis. Fungal cell structure. Fungal Infections MID 25 & 26. Eukaryotic (organized nucleus and cell structure) Non-motile
 Non-motile") Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Fungal Infections Once exotic and rare; now increasingly common Fungi are not virulent But they are good at taking advantage Opportunistic in many senses Fungal biology Eukaryotic (organized nucleus and
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Mycobacteria and fungal infections of the respiratory tract
 Before you start: You must read the slides! The Dr. did not bother to explain them all Mycobacteria and fungal infections of the respiratory tract - TB is a global problem that the WHO is trying to combat.
Before you start: You must read the slides! The Dr. did not bother to explain them all Mycobacteria and fungal infections of the respiratory tract - TB is a global problem that the WHO is trying to combat.
Epidemiology and ecology of fungal diseases
 Epidemiology and ecology of fungal diseases Healthcare Focus on: - individual - diagnosis - treatment Public Health Focus on: - population - prevention The nature of fungi Kingdom Fungi (lat. fungus, -i)
Epidemiology and ecology of fungal diseases Healthcare Focus on: - individual - diagnosis - treatment Public Health Focus on: - population - prevention The nature of fungi Kingdom Fungi (lat. fungus, -i)
North American Endemic Fungi
 North American Endemic Fungi Boni Elizabeth Elewski, MD Chair Department of Dermatology University of Alabama at Birmingham James Elder Professor of Graduate Medical Education DISCLOSURE OF FINANCIAL RELATIONSHIPS
North American Endemic Fungi Boni Elizabeth Elewski, MD Chair Department of Dermatology University of Alabama at Birmingham James Elder Professor of Graduate Medical Education DISCLOSURE OF FINANCIAL RELATIONSHIPS
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Mycology. BioV 400. Subcutaneous Mycoses. Ecological associations. Geographic distribution World-wide
 BioV 400 Mycology Handout 8 Subcutaneous Mycoses Lymphocutaneous sporotrichosis Chromoblastomycosis Phaeohyphomycosis Zygomycosis Mycetoma Lymphocutaneous sporotrichosis Sporothrix schenckii Chronic infection
BioV 400 Mycology Handout 8 Subcutaneous Mycoses Lymphocutaneous sporotrichosis Chromoblastomycosis Phaeohyphomycosis Zygomycosis Mycetoma Lymphocutaneous sporotrichosis Sporothrix schenckii Chronic infection
Epidemiology and Laboratory Diagnosis of Fungal Diseases
 Medical Mycology (BIOL 4849) Summer 2007 Dr. Cooper Epidemiology of Mycoses Epidemiology and Laboratory Diagnosis of Fungal Diseases Mycosis (pl., mycoses) - an infection caused by a fungus Two broad categories
Medical Mycology (BIOL 4849) Summer 2007 Dr. Cooper Epidemiology of Mycoses Epidemiology and Laboratory Diagnosis of Fungal Diseases Mycosis (pl., mycoses) - an infection caused by a fungus Two broad categories
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Hyphomycetes & Coelomycetes Identification. Taxonomic Systems for Identification of the Anamorphs of Conidiogenous Fungi
 Hyphomycetes & Coelomycetes Identification Saccardo ~1880 devised the first practical scheme for identifying fungi based on structure (morphology) of the conidium. "Sylloge Fungorum IV" Vuillemin ~ 1910
Hyphomycetes & Coelomycetes Identification Saccardo ~1880 devised the first practical scheme for identifying fungi based on structure (morphology) of the conidium. "Sylloge Fungorum IV" Vuillemin ~ 1910
The Differentiation of Yeast and Yeast-Like Forms in Human Tissues. Introduction. Histochemical Stains Used to Detect Fungi. Histopathologic Diagnoses
 The Differentiation of Yeast and Yeast-Like Forms in Human Tissues Gary W. Procop, MD Chair, Clinical Pathology Staff, Anatomic Pathology Director, Molecular Microbiology, Mycology, and Parasitology Cleveland
The Differentiation of Yeast and Yeast-Like Forms in Human Tissues Gary W. Procop, MD Chair, Clinical Pathology Staff, Anatomic Pathology Director, Molecular Microbiology, Mycology, and Parasitology Cleveland
Coccidioidomycosis Update for Primary Care
 Coccidioidomycosis Update for Primary Care SW Conference on Medicine April 26, 2018 John N Galgiani MD University of Arizona What Is? Caused by soil fungi Coccidioides immitis Coccidioides posadasii Other
Coccidioidomycosis Update for Primary Care SW Conference on Medicine April 26, 2018 John N Galgiani MD University of Arizona What Is? Caused by soil fungi Coccidioides immitis Coccidioides posadasii Other
2046: Fungal Infection Pre-Infusion Data
 2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
2046: Fungal Infection Pre-Infusion Data Fungal infections are significant opportunistic infections affecting transplant patients. Because these infections are quite serious, it is important to collect
L:7, L:8 Parasitology
 L:7, L:8 Parasitology 2.Fasciola hepatica Adult The adult Fasciola hepatica worm is flattened, leaf like shape, equipped with shoulders, somewhat oblong. Adult Fasciola hepatica measuring 3cm by 1cm in
L:7, L:8 Parasitology 2.Fasciola hepatica Adult The adult Fasciola hepatica worm is flattened, leaf like shape, equipped with shoulders, somewhat oblong. Adult Fasciola hepatica measuring 3cm by 1cm in
GAFFI Fact Sheet. Disseminated histoplasmosis
 F GAFFI Fact Sheet Disseminated histoplasmosis ION NS ACT ALOR ECTIO B O F F L G ND L IN FU NGA FU Disseminated histoplasmosis is a sub- acute infection that may be diagnosed in patients with impaired
F GAFFI Fact Sheet Disseminated histoplasmosis ION NS ACT ALOR ECTIO B O F F L G ND L IN FU NGA FU Disseminated histoplasmosis is a sub- acute infection that may be diagnosed in patients with impaired
Histoplasmosis. *resolution protective immunity. a 1 o "endemic" mycosis; 1 o "pulmonary" mycosis
 Histoplasmosis Definition - a granulomatous infection* initiated as a primary pulmonary disease, that may range in severity from inapparent and subclinical to acute, chronic or systemic and is caused by
Histoplasmosis Definition - a granulomatous infection* initiated as a primary pulmonary disease, that may range in severity from inapparent and subclinical to acute, chronic or systemic and is caused by
Paragonimiasis added Jan 2016
 added Jan 2016 BASIC EPIDEMIOLOGY Infectious Agent Paragonimus species, a parasitic lung fluke (flat worm). More than 30 species of trematodes (flukes) of the genus Paragonimus have been reported which
added Jan 2016 BASIC EPIDEMIOLOGY Infectious Agent Paragonimus species, a parasitic lung fluke (flat worm). More than 30 species of trematodes (flukes) of the genus Paragonimus have been reported which
Helminths (Worms) General Characteristics: Eukaryotic, multicellular parasites, in the kingdom Animalia.
 General Characteristics: Eukaryotic, multicellular parasites, in the kingdom Animalia.") Parasite II Helminths (Worms) General Characteristics: Eukaryotic, multicellular parasites, in the kingdom Animalia. They are worm-like organisms that live and feed off living hosts, receiving nourishment
Parasite II Helminths (Worms) General Characteristics: Eukaryotic, multicellular parasites, in the kingdom Animalia. They are worm-like organisms that live and feed off living hosts, receiving nourishment
Ali Alabbadi. Sarah Jaar ... Nader
 24 Ali Alabbadi Sarah Jaar... Nader Intro to Mycology *underlined text was explained in the lecture but is not found in the slides -mycology: the study of the mycoses of man (fungal infections) -less than
24 Ali Alabbadi Sarah Jaar... Nader Intro to Mycology *underlined text was explained in the lecture but is not found in the slides -mycology: the study of the mycoses of man (fungal infections) -less than
Pulmonary Infections: Fungus. Part I: Background Information and Dimorphic Fungus. Part II: Opportunistic Yeast and Molds
 Pulmonary Infections: Fungus Part I: Background Information and Dimorphic Fungus Part II: Opportunistic Yeast and Molds Howard J. Sachs, MD www.12daysinmarch.com Classification: Unicellular Budding Yeast,
Pulmonary Infections: Fungus Part I: Background Information and Dimorphic Fungus Part II: Opportunistic Yeast and Molds Howard J. Sachs, MD www.12daysinmarch.com Classification: Unicellular Budding Yeast,
Hyphomycetes & Coelomycetes Identification
 Hyphomycetes & Coelomycetes Identification Saccardo ~ 1880 devised the first practical scheme for identifying fungi based on structure (morphology) of the conidium. "Sylloge Fungorum IV" Vuillemin ~ 1910
Hyphomycetes & Coelomycetes Identification Saccardo ~ 1880 devised the first practical scheme for identifying fungi based on structure (morphology) of the conidium. "Sylloge Fungorum IV" Vuillemin ~ 1910
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
3/16/16 COCCIDIOIDOMYCOSIS COCCIDIOIDOMYCOSIS COCCIDIOIDOMYCOSIS COCCIDIOIDOMYCOSIS COCCIDIOIDOMYCOSIS COCCIDIOIDOMYCOSIS. Selected References
 10 MARCH 2006 Updated 5 June 2008 Updated 11 February 2011 Updated 4 March 2016 Herbert Boro, M.D., F.A.C.P. Selected References 1. Fiese, Marshall J. 1958. Coccidioidomycosis. Charles C. Thomas. 253 pp.
10 MARCH 2006 Updated 5 June 2008 Updated 11 February 2011 Updated 4 March 2016 Herbert Boro, M.D., F.A.C.P. Selected References 1. Fiese, Marshall J. 1958. Coccidioidomycosis. Charles C. Thomas. 253 pp.
Fungi. Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy:
 Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy:") MYCOLOGY Mycology I Fungi Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy: Morphology Spore formation FFungi Yeast Mold Yeastlike
MYCOLOGY Mycology I Fungi Eucaryotic Rigid cell wall(chitin, glucan) Cell membrane ergosterol Unicellular, multicellular Classic fungus taxonomy: Morphology Spore formation FFungi Yeast Mold Yeastlike
Value o f Immunodiffusion Tests in the Diagnosis o f Systemic M ycotic Diseases
 A n n a l s of C l i n i c a l L a b o r a t o r y S c i e n c e, Vol. 3, N o. 2 Copyright 1 9 7 3, Institute for Clinical Science Value o f Immunodiffusion Tests in the Diagnosis o f Systemic M ycotic
A n n a l s of C l i n i c a l L a b o r a t o r y S c i e n c e, Vol. 3, N o. 2 Copyright 1 9 7 3, Institute for Clinical Science Value o f Immunodiffusion Tests in the Diagnosis o f Systemic M ycotic
number Done by Corrected by Doctor د.حامد الزعبي
 number Fungi#1 Done by نرجس الس ماك Corrected by مهدي الشعراوي Doctor د.حامد الزعبي Introduction to Mycology -Terms: -Medical Mycology: The study of mycosis and their etiological agents -Mycosis: Disease
number Fungi#1 Done by نرجس الس ماك Corrected by مهدي الشعراوي Doctor د.حامد الزعبي Introduction to Mycology -Terms: -Medical Mycology: The study of mycosis and their etiological agents -Mycosis: Disease
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Pneumocystis. Pneumocystis BIOL Summer Introduction. Mycology. Introduction (cont.) Introduction (cont.)
 Introduction (cont.)") Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
Introduction Pneumocystis Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner, as indicated
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY
 CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of INFECTIOUS DISEASES MICROSCOPY Rengin Ahıskalı Macroscopy samples are shown in the macroscopy presentations of the first two courses.
CELL AND TISSUE INJURY COURSE-II PATHOLOGY LABORATORY PATHOLOGY of INFECTIOUS DISEASES MICROSCOPY Rengin Ahıskalı Macroscopy samples are shown in the macroscopy presentations of the first two courses.
2. The normal of the gut, and vagina keep the growth of pathogens in check. 3. in the respiratory tract sweep out bacteria and particles.
 Chapter 39 Immunity I. Three Lines of Defense A. Surface Barriers to Invasion 1. is an important barrier. 2. The normal of the gut, and vagina keep the growth of pathogens in check. 3. in the respiratory
Chapter 39 Immunity I. Three Lines of Defense A. Surface Barriers to Invasion 1. is an important barrier. 2. The normal of the gut, and vagina keep the growth of pathogens in check. 3. in the respiratory
8/11/16. Kevin Letz DNP, MSN, MBA, RN, CEN, CNE, FNP-C, PCPNP-BC, ANP-BC, FAANP
 Kevin Letz DNP, MSN, MBA, RN, CEN, CNE, FNP-C, PCPNP-BC, ANP-BC, FAANP Eosinophilia Eosinophilia refers to an absolute eosinophil count in the peripheral blood of 500 eosinophils/microl; this is considered
Kevin Letz DNP, MSN, MBA, RN, CEN, CNE, FNP-C, PCPNP-BC, ANP-BC, FAANP Eosinophilia Eosinophilia refers to an absolute eosinophil count in the peripheral blood of 500 eosinophils/microl; this is considered
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Epidemiology of Fungal Diseases
 Lecture 2 Epidemiology of Fungal Diseases Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner,
Lecture 2 Epidemiology of Fungal Diseases Disclaimer: This lecture slide presentation is intended solely for educational purposes. Many of the images contained herein are the property of the original owner,
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
The Immune System & Non- Infectious Disease. Ch. 18: Sections 1, 2, & 4
 The Immune System & Non- Infectious Disease Ch. 18: Sections 1, 2, & 4 What is the Immune System? The purpose of the immune system is to: keep infectious microorganisms, such as certain bacteria, viruses,
The Immune System & Non- Infectious Disease Ch. 18: Sections 1, 2, & 4 What is the Immune System? The purpose of the immune system is to: keep infectious microorganisms, such as certain bacteria, viruses,
Eosinophils and effusion: a clinical conundrum
 Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Ruth Sobala, Kevin Conroy, Hilary Tedd, Salem Elarbi kevin.peter.conroy@gmail.com Respiratory Dept, Queen Elizabeth Hospital, Gateshead, UK. Eosinophils and effusion: a clinical conundrum Case report A
Subcutaneous Fungi 10/13/2009. General Characteristics. Pathogenesis. Epidemiology. Laboratory Diagnosis. Specimens. Growth rate: 1-4 weeks
 General Characteristics Growth rate: 1-4 weeks Subcutaneous Fungi Clinical Laboratory Science Program Carol Larson MSEd, MT(ASCP) Dematiaceous septate hyphae Hyaline septate hyphae Branching GPR Epidemiology
General Characteristics Growth rate: 1-4 weeks Subcutaneous Fungi Clinical Laboratory Science Program Carol Larson MSEd, MT(ASCP) Dematiaceous septate hyphae Hyaline septate hyphae Branching GPR Epidemiology
محاضرة مناعت مدرس المادة :ا.م. هدى عبدالهادي علي النصراوي Immunity to Infectious Diseases
 محاضرة مناعت مدرس المادة :ا.م. هدى عبدالهادي علي النصراوي Immunity to Infectious Diseases Immunity to infection depends on a combination of innate mechanisms (phagocytosis, complement, etc.) and antigen
محاضرة مناعت مدرس المادة :ا.م. هدى عبدالهادي علي النصراوي Immunity to Infectious Diseases Immunity to infection depends on a combination of innate mechanisms (phagocytosis, complement, etc.) and antigen
Eosinophilic lung diseases
 Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
Eosinophilic lung diseases Chai Gin Tsen Department of Respiratory and Critical Care Medicine Tan Tock Seng Hospital The eyes do not see what the mind does not know Not very common A high index of suspicion
LYMPHATIC AND IMMUNE SYSTEMS. Chapter 33
 LYMPHATIC AND IMMUNE SYSTEMS Chapter 33 THE LYMPHATIC SYSTEM The lymphatic system has three main functions Take up excess tissue fluid and return it to the bloodstream Receive fats called lipoproteins
LYMPHATIC AND IMMUNE SYSTEMS Chapter 33 THE LYMPHATIC SYSTEM The lymphatic system has three main functions Take up excess tissue fluid and return it to the bloodstream Receive fats called lipoproteins
Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis
 Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis Identify the structures neutrophils macrophages x40 Organisms 8 30 micron in size, with variable capsule
Impression smear from a nasal mass on a 2 year old cat Presented with: one month duration of epistaxis Identify the structures neutrophils macrophages x40 Organisms 8 30 micron in size, with variable capsule
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Immunity to Malaria Immunity to sporozoites injected by mosquito Mediated by antibody that prevents infection of liver cells
 IMMUNITY TO PARASITIC AND FUNGAL INFECTIONS Chapter 20 Topics Covered Overview of parasitic diseases Immune response to parasitic infections Immunity to malaria Immunity to schistosomiasis Immune effectors
IMMUNITY TO PARASITIC AND FUNGAL INFECTIONS Chapter 20 Topics Covered Overview of parasitic diseases Immune response to parasitic infections Immunity to malaria Immunity to schistosomiasis Immune effectors
Fungal infection in the immunocompromised patient. Dr Kirsty Dodgson
 Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Definition. Paracoccidioidmycosis. History. Paracoccidioides brasiliensis. Epidemiology
 Definition Paracoccidioidmycosis Hillary Howard Carlisle Heinselman Sarah Maher Arjun Vikuntam A systematic endemic disease produced by Paracoccidioides brasiliensis Primarily a pulmonary disease Disseminated
Definition Paracoccidioidmycosis Hillary Howard Carlisle Heinselman Sarah Maher Arjun Vikuntam A systematic endemic disease produced by Paracoccidioides brasiliensis Primarily a pulmonary disease Disseminated
Neurosciences- Lecture 2 Virus associated meningitis Polio Virus
 Al- Balqa Applied University Faculty of Medicine Neurosciences- Lecture 2 Virus associated meningitis Polio Virus Dr. Hala Al Daghistani The most important Enteroviruses are the three poliovirus serotypes
Al- Balqa Applied University Faculty of Medicine Neurosciences- Lecture 2 Virus associated meningitis Polio Virus Dr. Hala Al Daghistani The most important Enteroviruses are the three poliovirus serotypes
PARASITOLOGY INTRODUCTION
 PARASITOLOGY INTRODUCTION DEFINITION Parasite means : one who eats at the table of another. Differs from bacteria and viruses in their complex life cycles, intermediate hosts and chronicity. Evolved to
PARASITOLOGY INTRODUCTION DEFINITION Parasite means : one who eats at the table of another. Differs from bacteria and viruses in their complex life cycles, intermediate hosts and chronicity. Evolved to
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Overview of Coccidioidomycosis (Valley Fever) Stephen Munday, MD MPH Imperial County Public Health May 21, 2013
 Stephen Munday, MD MPH Imperial County Public Health May 21, 2013") Overview of Coccidioidomycosis (Valley Fever) Stephen Munday, MD MPH Imperial County Public Health May 21, 2013 Objectives Assess the epidemiology of Coccidioidomycosis (aka Valley Fever) Describe the
Overview of Coccidioidomycosis (Valley Fever) Stephen Munday, MD MPH Imperial County Public Health May 21, 2013 Objectives Assess the epidemiology of Coccidioidomycosis (aka Valley Fever) Describe the
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
 Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting
 Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting Professor Retno Wahyuningsih Professor of Medical Mycology Department of Parasitology, Faculty of Medicine Universitas
Chronic pulmonary aspergillosis diagnosis and management in resource-limited setting Professor Retno Wahyuningsih Professor of Medical Mycology Department of Parasitology, Faculty of Medicine Universitas
Streptococcus pneumonia
 Streptococcus pneumonia The pneumococci (S. pneumoniae) are gram-positive diplococci. Often lancet shaped or arranged in chains, possessing a capsule of polysaccharide that permits typing with specific
Streptococcus pneumonia The pneumococci (S. pneumoniae) are gram-positive diplococci. Often lancet shaped or arranged in chains, possessing a capsule of polysaccharide that permits typing with specific
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Nursing college, Second stage Microbiology Dr.Nada Khazal K. Hendi Medical Microbiology
 1 Nursing college, Second stage Microbiology Medical Microbiology Lecture-1- Fungi (Mycosis) They are a diverse group of saprophytic and parasitic eukaryotic organisms. Human fungal diseases (mycoses)
1 Nursing college, Second stage Microbiology Medical Microbiology Lecture-1- Fungi (Mycosis) They are a diverse group of saprophytic and parasitic eukaryotic organisms. Human fungal diseases (mycoses)
BACTERIAL PATHOGENESIS
 BACTERIAL PATHOGENESIS A pathogen is a microorganism that is able to cause disease. Pathogenicity is the ability to produce disease in a host organism. Virulence a term which refers to the degree of pathogenicity
BACTERIAL PATHOGENESIS A pathogen is a microorganism that is able to cause disease. Pathogenicity is the ability to produce disease in a host organism. Virulence a term which refers to the degree of pathogenicity
Question 1. Kupffer cells, microglial cells and osteoclasts are all examples of what type of immune system cell?
 Abbas Chapter 2: Sarah Spriet February 8, 2015 Question 1. Kupffer cells, microglial cells and osteoclasts are all examples of what type of immune system cell? a. Dendritic cells b. Macrophages c. Monocytes
Abbas Chapter 2: Sarah Spriet February 8, 2015 Question 1. Kupffer cells, microglial cells and osteoclasts are all examples of what type of immune system cell? a. Dendritic cells b. Macrophages c. Monocytes
Ascaris lumbricoides
 Case History A 4-year-old Caucasian male child of Turkish nationality was admitted to the emergency department with Abdominal pain and biliary vomiting for three days. Physical Examination revealed abdomen
Case History A 4-year-old Caucasian male child of Turkish nationality was admitted to the emergency department with Abdominal pain and biliary vomiting for three days. Physical Examination revealed abdomen
Pneumothorax: A Rare Presentation of. Pulmonary Mycetoma. Prem Parkash Gupta* Sanjay Fotedar* Dipti Agarwal** Kuldeep Saini* Sarita Magu***
 Pneumothorax: A Rare Presentation of Pulmonary Mycetoma Prem Parkash Gupta* Sanjay Fotedar* Dipti Agarwal** Kuldeep Saini* Sarita Magu*** Departments of *Respiratory Medicine, **Physiology, and ***Radiodiagnosis,
Pneumothorax: A Rare Presentation of Pulmonary Mycetoma Prem Parkash Gupta* Sanjay Fotedar* Dipti Agarwal** Kuldeep Saini* Sarita Magu*** Departments of *Respiratory Medicine, **Physiology, and ***Radiodiagnosis,
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
INNATE IMMUNITY Non-Specific Immune Response. Physiology Unit 3
 INNATE IMMUNITY Non-Specific Immune Response Physiology Unit 3 Protection Against Infection The body has several defenses to protect itself from getting an infection Skin Mucus membranes Serous membranes
INNATE IMMUNITY Non-Specific Immune Response Physiology Unit 3 Protection Against Infection The body has several defenses to protect itself from getting an infection Skin Mucus membranes Serous membranes
Bloodborne Pathogens. Introduction to Fungi. Next >> COURSE 2 MODULE 4
 Bloodborne Pathogens COURSE 2 MODULE 4 to is a general term used to encompass the diverse morphologic forms of yeasts and molds. Originally classified as primitive plants without chlorophyll, the fungi
Bloodborne Pathogens COURSE 2 MODULE 4 to is a general term used to encompass the diverse morphologic forms of yeasts and molds. Originally classified as primitive plants without chlorophyll, the fungi
phagocytic leukocyte Immune System lymphocytes attacking cancer cell lymph system
 phagocytic leukocyte Immune System lymphocytes attacking cancer cell lymph system 2006-2007 1) recognizing the presence of an infection; 2) containing the infection and working to eliminate it; 3) regulating
phagocytic leukocyte Immune System lymphocytes attacking cancer cell lymph system 2006-2007 1) recognizing the presence of an infection; 2) containing the infection and working to eliminate it; 3) regulating
What are bacteria? Microbes are microscopic(bacteria, viruses, prions, & some fungi etc.) How do the sizes of our cells, bacteria and viruses compare?
 How do the sizes of our cells, bacteria and viruses compare?") 7.1 Microbes, pathogens and you Chp. 7 Lymphatic System & Immunity The interaction between microbes and humans? Microbes are very abundant in the environment and as well as in and on our bodies GOOD: We
7.1 Microbes, pathogens and you Chp. 7 Lymphatic System & Immunity The interaction between microbes and humans? Microbes are very abundant in the environment and as well as in and on our bodies GOOD: We
Immunodeficiencies HIV/AIDS
 Immunodeficiencies HIV/AIDS Immunodeficiencies Due to impaired function of one or more components of the immune or inflammatory responses. Problem may be with: B cells T cells phagocytes or complement
Immunodeficiencies HIV/AIDS Immunodeficiencies Due to impaired function of one or more components of the immune or inflammatory responses. Problem may be with: B cells T cells phagocytes or complement
Anthrax: An Epidemiologic Perspective. Denise Dietz Public Health Epidemiologist
 Anthrax: An Epidemiologic Perspective Denise Dietz Public Health Epidemiologist Outline Overview of anthrax Explain different types of anthrax Clinical Why a good weapon Epidemiology Bacillus anthracis
Anthrax: An Epidemiologic Perspective Denise Dietz Public Health Epidemiologist Outline Overview of anthrax Explain different types of anthrax Clinical Why a good weapon Epidemiology Bacillus anthracis
COCCIDIOIDES SPP. EXPOSURE/INJURY RESPONSE PROTOCOL
 PLEASE POST THIS PAGE IN AREAS WHERE COCCIDIOIDES IS USED IN RESEARCH LABORATORIES UNIVERSITY OF CALIFORNIA, SAN FRANCISCO ENVIRONMENTAL HEALTH AND SAFETY/BIOSAFETY COCCIDIOIDES SPP. EXPOSURE/INJURY RESPONSE
PLEASE POST THIS PAGE IN AREAS WHERE COCCIDIOIDES IS USED IN RESEARCH LABORATORIES UNIVERSITY OF CALIFORNIA, SAN FRANCISCO ENVIRONMENTAL HEALTH AND SAFETY/BIOSAFETY COCCIDIOIDES SPP. EXPOSURE/INJURY RESPONSE
Warm-up. Parts of the Immune system. Disease transmission. Disease transmission. Why an immune system? Chapter 43 3/9/2012.
 Warm-up Objective: Explain how antigens react with specific lymphocytes to induce immune response and immunological memory. Warm-up: Which of the following would normally contain blood with the least amount
Warm-up Objective: Explain how antigens react with specific lymphocytes to induce immune response and immunological memory. Warm-up: Which of the following would normally contain blood with the least amount
Innate Immunity. Bởi: OpenStaxCollege
 Innate Immunity Bởi: OpenStaxCollege The vertebrate, including human, immune system is a complex multilayered system for defending against external and internal threats to the integrity of the body. The
Innate Immunity Bởi: OpenStaxCollege The vertebrate, including human, immune system is a complex multilayered system for defending against external and internal threats to the integrity of the body. The
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Lecture (14) Amiedi Ph.D.Microbiology
 Amiedi Ph.D.Microbiology") AEROBIC BACILLUS Lecture (14) Dr. Baha,H,AL-Amiedi Amiedi Ph.D.Microbiology General Characteristics of Bacillus 60 species; Gram-positive or Gram-variable bacilli Large (0.5 x 1.2 to 2.5 x 10 um) Most
AEROBIC BACILLUS Lecture (14) Dr. Baha,H,AL-Amiedi Amiedi Ph.D.Microbiology General Characteristics of Bacillus 60 species; Gram-positive or Gram-variable bacilli Large (0.5 x 1.2 to 2.5 x 10 um) Most
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Histopathology Description:
 2013-2-1 CANINE HEART Ahmed M. Abubakar BOVINE PATHOLOGY CONTRIBUTING INSTITUTION : The Royal Veterinary college, Dept. of Pathology and Biology Signalment: 11-month-old male Border Collie dog (Canis familiaris)
2013-2-1 CANINE HEART Ahmed M. Abubakar BOVINE PATHOLOGY CONTRIBUTING INSTITUTION : The Royal Veterinary college, Dept. of Pathology and Biology Signalment: 11-month-old male Border Collie dog (Canis familiaris)
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 28 The Immune System Lesson 1: The Immune System Lesson Objectives Upon completion of this lesson,
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 28 The Immune System Lesson 1: The Immune System Lesson Objectives Upon completion of this lesson,
SWABCHA Fact Sheet: Tuberculosis (TB)
") SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
Offending agents like: 1. Infectious agents: 2. toxic agents(toxins) Micro-organisms Bacteria Viruses Parasites Fungi
 Micro-organisms Bacteria Viruses Parasites Fungi") Immunity Dr.Talar Immunity: is the ability of the human body to resist almost all types of offending agents that tend to damage the tissues and organs or it s a special system for combating different infectious
Immunity Dr.Talar Immunity: is the ability of the human body to resist almost all types of offending agents that tend to damage the tissues and organs or it s a special system for combating different infectious
ANATOMY OF THE IMMUNE SYSTEM
 Immunity Learning objectives Explain what triggers an immune response and where in the body the immune response occurs. Understand how the immune system handles exogenous and endogenous antigen differently.
Immunity Learning objectives Explain what triggers an immune response and where in the body the immune response occurs. Understand how the immune system handles exogenous and endogenous antigen differently.