SLE and the Antiphospholipid Syndrome
|
|
|
- Michael Crawford
- 5 years ago
- Views:
Transcription
1 SLE and the Antiphospholipid Syndrome Susan Y. Ritter MD, PhD Associate Physician Division of Rheumatology, Immunology and Allergy Department of Medicine Brigham and Women s Hospital Instructor in Medicine Harvard Medical School
2 Spouse is employee of Pfizer Disclosures
3 Overview SLE different presentations and severity Classification criteria Cutaneous and drug induced Treatment Antiphospholipid Syndrome
4 SLE Epidemiology Prevalence ~1 in 1000 Most common in females in reproductive years 9:1 female : male ratio More common in Black, Latino and Asian
5 What is Lupus? Great imitator Many different organ-systems may be involved Disease occurs in the presence of autoantibodies most commonly ANA
6 Many faces of SLE 51 yo white male glomerulonephritis (GN), + ANA, + dsdna, seizures 32 yo black female arthritis, discoid rash, pleurisy, + ANA, + Ro 52 yo female thrombocytopenia, hemolytic anemia, renal disease, +ANA, + APLA 27 yo female fevers, class V GN, low WBC, + ANA, + dsdna, low complements, arthritis
7 What is shared? Positive autoantibodies Clinical manifestations suggestive of SLE
8 Classification Criteria for SLE 4 are necessary, and 1 should be + ANA Malar Rash Discoid Rash Photosensitivity Apthous ulcers Neurologic: seizures or psychosis Hematologic: anemia, leuko or lymphopenia, thrombocytopenia Arthritis Serositis (pericarditis or pleuritis) Immunologic: anti-dna, anti- Smith, antiphospholipid antibody Positive ANA Renal (proteinuria or casts)
9 Other common symptoms Fatigue Headaches Malaise Cognitive impairment lupus fog Myalgias
10 Case 1 33 yo woman comes to see you. She has mouth sores and a rash over the bridge of her nose that looks like this:

11

12
13 Case 1: continued Her PCP sent off an ANA that was positive at a titer of 1:320 and she had dsdna at 45 units. Does she have SLE?
14 Case 1: Malar rash Photosensitivity Aphthous ulcers Positive ANA Positive anti-dsdna
15 Other skin manifestations of SLE

16 Discoid lupus
17 Cutaneous Lupus: Discoid Lupus Patient have defined plaques that become thickened over time. Can scar and leave hypopigmented lesions 10-15% of patients develop systemic lupus in those that are ANA positive In SLE patients, 10-15% will have discoid lesions Treatment: sun avoidance, antimalarials, dapsone, immunosuppressive agents, thalidomide
18 Cutaneous Lupus: SCLE (subacute cutaneous lupus erythematosus) More common in Caucasians 75% are women Lesions occur in sun-exposed areas Two types of lesions: Papulosquamous Polycyclic annular

19 SCLE
20 Other Skin Findings in SLE Alopecia Vasculitis Raynaud s Bullous lesions Urticarial lesions Panniculitis Nail lesions
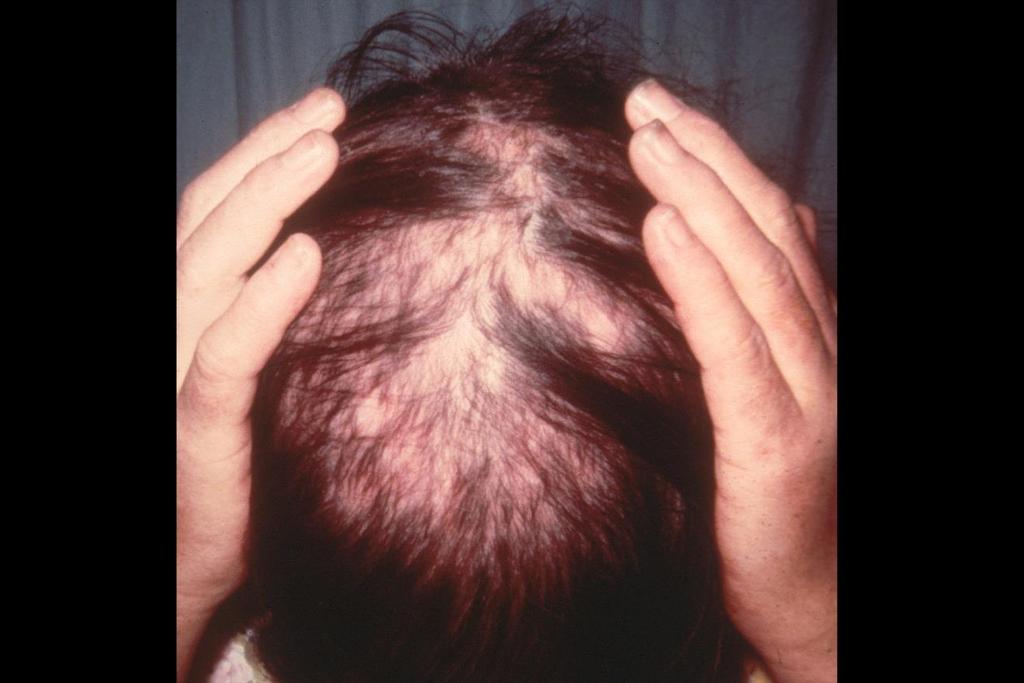
21 Alopecia

22 Raynaud s
23 Case 2 40 yo man whom you have been following for several years with SLE (malar rash, positive serologies and renal disease) complains of chest pain when he takes a deep breath Is this related to lupus?
24 Pulmonary Manifestations of SLE Pleuritis Lupus pneumonitis Chronic interstitial lung disease Pulmonary hemorrhage (high mortality) Shrinking lung syndrome (secondary to diaphragmatic paralysis and lung disease)
25 Case 3 35 yo female whom you have followed for SLE for many years (joint symptoms, renal disease, positive serologies, requiring steroids) has read on the internet that she is at risk for having a heart attack How do you counsel her?
26 Cardiovascular Manifestations of SLE Accelerated atherosclerosis Disease + drugs Pericarditis Valvular heart disease usually in conjunction with the antiphospholipid syndrome Coronary vasculitis rare Myocarditis rare
27 Case 4 32 yo woman referred from her PCP with one month of joint swelling affecting her PIPs and MCPs. She has a history of psoriasis and her PCP believes she has psoriatic arthritis.
28 Case 4: continued Despite being placed on NSAIDs and low dose steroids, she continues to feel unwell. Calls your office with fevers 102, feels terrible Initial labs reveal a WBC 2.8. You decide to send off an ANA which returns at 1:1280 and dsdna is 84.
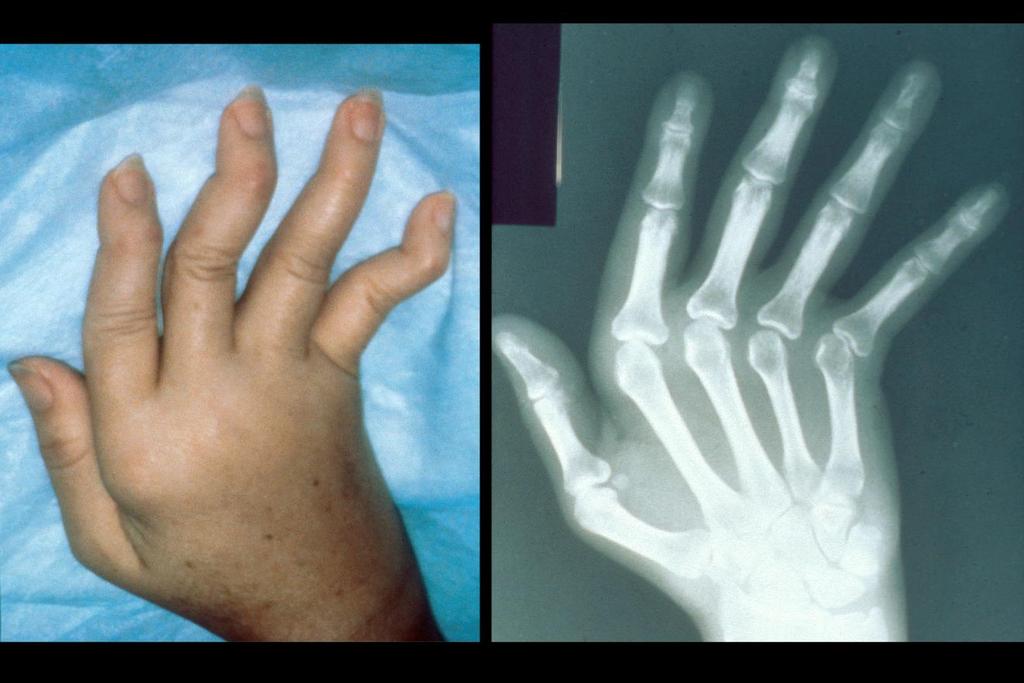
29 Jaccoud s arthropathy
30 Musculoskeletal manifestations of SLE 95% will have musculoskeletal complains Arthralgias and arthritis Septic arthritis Osteonecrosis risk increases with steroid use > 20 mg per day Myositis more commonly seen in patients with Mixed Connective Tissue Disease (MCTD) Myopathy secondary to steroids proximal muscle weakness
31 Case 5 25 yo woman referred to you with anemia and thrombocytopenia Hemocrit 25 Platelet count 90,000 She has a history of pleuritis Positive ANA and false positive VDRL
32 Hematologic manifestations of SLE Anemia usually Coomb s positive Leukopenia WBC < 4000 Lymphopenia Lymphocytes < 1500 Thrombocytopenia Platelets < 100,000
33 Case 6 29 yo woman with history of mild SLE (arthritis, malar rash, positive serologies) presents with edema, proteinuria, and RBC in her urine What do you do?
34 Renal disease in SLE Proteinuria > 500 mg protein/24 hr urine Presence of casts
35 WHO Classification Class I: Normal or Minimal Change Class II: Mesangial glomerulonephritis Class III: Focal proliferative glomerulonephritis Class IV: Diffuse proliferative glomerulonephritis Class V: Membranous glomerulonephritis Class VI: Global sclerosis > 90% sclerosed lesions
36 Activity vs. Chronicity Look for the degree of activity in the involved renal specimen High disease activity implies better response to therapy Chronic lesions are scarred, and will not improve with immunosuppression
37 Case 7 25 yo woman with history of SLE (hematologic and arthritis) presents with altered mental status
38 Neuropsychiatric Manifestations of SLE Neurologic CVA Seizures Transverse myelitis Optic neuritis Meningitis Headaches Organic brain syndromes Neuropathies Associated with antiphospholipid antibodies Psychiatric Psychosis Cognitive disorder Pseudo dementia Functional
39 Other SLE manifestations Sjogren s Syndrome GI abnormalities Abdominal pain Anorexia Peritonitis Pancreatitis Hepatitis Secondary fibromyalgia
40 Case 8 You are asked to see a 38 yo woman with a history of a rash over the bridge of her nose which she has been told is acne rosacea and some joint achiness She has an ANA sent that is positive at 1:40 Does she have lupus?
41 Few notes about ANA test ANA test was not designed as a screening test Up to 20% of healthy adults, particularly women, have a low titer ANA and do not go on to develop rheumatic diseases Causes of false positive tests: viral infections family history of rheumatic disease other autoimmune disease like GI or thyroid disease Once a patient has a positive ANA, it does not need to be retested, unless symptoms change and there is an increased suspicion for a rheumatic disease.
42 Autoantibodies in SLE ANA found in 95% of patients Anti-dsDNA in 40-80% of patients Anti-Sm 25% of patients Anti-histone seen in drug induced SLE Anti-Ro(SSA), Anti-La(SSB) Sjogren s, SCLE Anti-RNP Mixed Connective Tissue disease False positive VDRL antiphospholipid antibody
43 Choosing Wisely Campaign Don t test ANA sub-serologies without a positive ANA and clinical suspicion of immune-mediated disease. Tests for anti-nuclear antibody (ANA) sub-serologies are usually negative if the ANA is negative. Exceptions include anti-jo1, which can be positive in some forms of myositis, or occasionally anti-ssa, in the setting of lupus or Sjögren s syndrome. Broad testing of autoantibodies should be avoided; instead the choice of autoantibodies should be guided by the specific disease under consideration.
44 Case 9 63 yo man started on procainamide for an abnormal heart rhythm. He develops joint pain and a skin rash Work-up reveals a positive ANA and anti-histone antibody
45 Drug Induced SLE Patients present with lupus-like illness Usually arthritis, rash and serositis Positive ANA and anti-histone antibody Rare to have renal, neuropsychiatric or vasculitic disease Often responds to drug withdrawal, NSAIDs or low dose prednisone
46 Drugs Involved in Drug-Induced SLE
47 Drugs Involved in Drug-Induced SLE Common Procainamide Hydralazine Rare Beta-blockers D-Penicillamine INH Quinidine PTU Hydantoins Trimethadione Chlorpromazine
48 General Treatment Advice in SLE Sun avoidance and protection Diet Exercise Smoking cessation
49 Lupus Flare A flare is a measurable increase in disease activity in one or more organ systems involving new or worse clinical signs and symptoms and/or laboratory measurements. It must be considered clinically significant by the assessor and usually there would be at least consideration of a change or an increase in treatment. International consensus for a definition of disease flare in lupus. Ruperto et al. Lupus Apr;20(5):
50 Treatment: Mild Disease Symptoms: low grade fever, rash, arthralgia, fatigue NSAIDs Antimalarials hydroxychloroquine most common Low dose prednisone < 10 mg/day
51 Treatment: Severe Disease Steroids: mg/kg/day renal, CNS Cyclophosphamide monthly pulses mg/m2 or biweekly for 12 weeks renal, CNS Azathioprine renal Mycophenolate mofetil renal, skin Tacrolimus renal, skin Methotrexate arthritis, skin Belimumab steroid resistant serositis and arthritis
52 Other therapies (off label) Cyclosporine A Rituximab Abatacept joint symptoms, in trials for renal disease Bone marrow transplant
53 Summary of SLE SLE is a multi-system autoimmune disorder SLE can look like many different disease entities To diagnose SLE, the ANA should be positive A positive ANA dose NOT make a diagnosis of SLE Direct treatment towards the underlying system involved All patients unless contraindicated should be offered hydroxychloroquine Can use steroids and other immunosuppressives Biologics other than belimumab are under investigation
54 Antiphospholipid Antibody Syndrome
55 When to think about antiphopholipid antibodies? Early miscarriages Thrombocytopenia Stroke/TIA in younger patients DVT/PE Patients with lupus
56 Antiphospholipid Antibody Syndrome: Major criteria Presence of an anticardiolipin antibody (IgG or IgM) and/or lupus anticoagulant on 2 separate occasions 12 weeks apart PLUS one of the following clinical events: Arterial thrombotic event Venous thrombotic event Recurrent pregnancy losses 2 or more 1 st trimester losses 2 nd trimester loss or severe intrauterine growth restriction
57 Other clinical features (not part of criteria) Thrombocytopenia Coomb s positive hemolytic anemia Livedo reticularis Raynaud s phenomenon Migraines and cognitive dysfunction Valvular vegetations or thickening Renal disease thrombotic microangiopathy
58 Associated medical conditions Sneddon s syndrome: Strokes and livedo reticularis in young women Evan s syndrome: Thrombocytopenia and Coomb s positive hemolytic anemia CVAs and MIs in individuals under 40 SLE Catastrophic APS (CAPS) sudden multisystem occlusive disease
59 Antiphospholipid Antibody Tests Lupus Anticoagulant Anti-Cardiolipin Beta-2 glycoprotein I
60 Lupus Anticoagulant In vitro prolongation of clotting test In vivo it is a pro-coagulant Activated PTT, platelet neutralizing procedure, dilute Russell Viper Venom time are used Lupus anticoagulant should be confirmed by adding phospholipid and normalizing the test result
61 3 Possibilities Lupus Anticoagulant Confirmatory What dose it mean? - Negative + - Negative + + Positive
62 Anticardiolipin Antibodies ELISA test: standardized using international standard GPL units All subsets: IgG, IgM, IgA, IgD can be seen, but IgG is the most clinically relevant Clinically relevant titer is 40 units
63 Anti-beta-2 glycoprotein I ELISA test IgG and IgM forms Clinically relevant titer is 40 units drvvt (used with LAC) is sensitive to the presence of anti-beta-2-glycoprotein I Closely correlated with thrombotic events
64 Antibodies in Various Patient Populations Healthy controls: 1-2% Recurrent miscarriage population: 5-10% SLE: 20-40% SLE with livedo or Raynaud s: 80% Stroke, MI under age 40: 20% HIV infected: IgM 50-60%
65 Who should be evaluated for antiphospholipid antibodies? SLE patients Patients under age 40 with CVA, MI, no obvious risk factors Recurrent venous or arterial clots Women with recurrent first trimester pregnancy losses, or second trimester loss
66 Treatment: Patients with documented clot + antibodies Lifelong anticoagulation generally warfarin Target INR 2.5 Recurrent episodes, severe arterial episodes, target INR There is insufficient data regarding the efficacy of direct oral anticoagulants in this condition.
67 Treatment: Antibodies in the absence of clinical events Some advocate the use of prophylactic aspirin therapy in those with positive antibodies. This therapy has NOT been shown to decrease the risk of clotting episodes except in patients with co-existing SLE
68 Catastrophic Antiphospholipid Syndrome (CAPS) Consider when multiple clots over 7 days Renal failure, diffuse alveolar hemorrhage, adrenal hemorrhage, encephalopathy can be seen Can look similar to other thrombotic microangiopathies Treatment with anticoagulants, corticosteroids, IVIG and plasma exchange Some use Rituximab or Eculizumab (off label) if refractory
69 Summary of APS The antiphosholipid syndrome is defined as: Arterial clots, venous clots or obstetrical complications in the presence of an antiphospholipid antibody The antibody testing needs to be positive on 2 separate occasions at least 12 weeks apart Treatment for the arterial or venous complications is life-long anticoagulation
70 Question 1 23 F with a history of malaise, facial rash and achiness. Appropriate work-up includes: A) ANA B) CBC w/ diff, LFTs, creatinine and urinalysis C) dsdna D) All of the above
71 Answer B) CBC, LFTs, renal function screen As a first pass for the evaluation of suspected SLE, a complete history and physical should be performed. Appropriate laboratory testing includes a CBC with differential, liver function tests, creatinine and urinalysis. Avoid sending an ANA and/or dsdna unless there is a strong suspicion of SLE.
72 Question 2 43 F presents with a DVT with no clear precipitant. PMHx is notable for 2 first trimester miscarriages and one second trimester miscarriage. Appropriate testing includes: A) Lupus anti-coagulant B) Anticardiolipin antibody C) VDRL D) A, B, and C E) A and B only
73 Answer E) A and B should be sent The history is suggestive of antiphospholipid syndrome Send off both the lupus anticoagulant and anticardiolipin antibody when you have a high suspicion for the antiphospholipid antibody syndrome VDRL is not a good screening assay for this disorder
74 References Classification criteria for systemic lupus erythematosus: a review. Petri M, Magder L. Lupus. 2004;13(11):829 Guidelines for referral and management of systemic lupus erythematosus in adults. American College of Rheumatology Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum Sep; 42(9): Diagnosis and Management of the Antiphospholipid Syndrome. Garcia D and Erkan D. NEJM May 24; 378 (21):
Conflict of Interest. Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital.
 Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital Conflict of Interest Disclosures: None Overview Diagnostic Classification Criteria of SLE
Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital Conflict of Interest Disclosures: None Overview Diagnostic Classification Criteria of SLE
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS LUPUS 101 SLE SUBSETS AUTOIMMUNE DISEASE 11/4/2013 HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS
 LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
Systemic Lupus Erythematosus
 Systemic Lupus Erythematosus Marc C. Hochberg, MD, MPH Professor of Medicine and Head, Division of Rheumatology University of Maryland School of Medicine CASE: HISTORY A 26-year-old woman is seen for migratory
Systemic Lupus Erythematosus Marc C. Hochberg, MD, MPH Professor of Medicine and Head, Division of Rheumatology University of Maryland School of Medicine CASE: HISTORY A 26-year-old woman is seen for migratory
Insights into the DX of Pediatric SLE
 Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS
 UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. October 20, 2012 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement Diagnosis Treatment Pregnancy
UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. October 20, 2012 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement Diagnosis Treatment Pregnancy
Definition Chronic autoimmune disease The body s immune system starts attacking itself Can affect most organs and tissues in the body Brain, lungs, he
 LIVING WITH SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. Rowan Diagnostic Clinic Salisbury, N.C. May 11, 2013 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement
LIVING WITH SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. Rowan Diagnostic Clinic Salisbury, N.C. May 11, 2013 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement
9/25/2013 SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)
") SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
Living with Lupus: An Insider s Perspective
 Living with Lupus: An Insider s Perspective Pamela Thorpe, MD, FACP Lupus Foundation of America, Inc. Philadelphia Tri-State Chapter Volunteer May 2014 My Own Story Is it Lupus Yet? The What What is this?
Living with Lupus: An Insider s Perspective Pamela Thorpe, MD, FACP Lupus Foundation of America, Inc. Philadelphia Tri-State Chapter Volunteer May 2014 My Own Story Is it Lupus Yet? The What What is this?
.,Dr Ali Alkazzaz Babylon collage of medicine 2016
 .,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
.,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
Development of SLE among Possible SLE Patients Seen in Consultation: Long-Term Follow-Up. Disclosures. Background. Evidence-Based Medicine.
 Development of SLE among Patients Seen in Consultation: Long-Term Follow-Up Abstract # 1699 May Al Daabil, MD Bonnie L. Bermas, MD Alexander Fine Hsun Tsao Patricia Ho Joseph F. Merola, MD Peter H. Schur,
Development of SLE among Patients Seen in Consultation: Long-Term Follow-Up Abstract # 1699 May Al Daabil, MD Bonnie L. Bermas, MD Alexander Fine Hsun Tsao Patricia Ho Joseph F. Merola, MD Peter H. Schur,
Lupus. Fast facts. What is lupus? What causes lupus? Who gets lupus?
 Lupus Systemic lupus erythematosus, referred to as SLE or lupus, is sometimes called the "great imitator." Why? Because of its wide range of symptoms, people often confuse lupus with other health problems.
Lupus Systemic lupus erythematosus, referred to as SLE or lupus, is sometimes called the "great imitator." Why? Because of its wide range of symptoms, people often confuse lupus with other health problems.
Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS
 Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients
Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients
Benlysta (belimumab) Prior Authorization Criteria Program Summary
 Prior Authorization Criteria Program Summary") Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z
 from Harvard Medical School Health Topics A-Z") Topic Page: Systemic Lupus Erythematosus Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z What Is It? Lupus is thought to develop when the immune system
Topic Page: Systemic Lupus Erythematosus Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z What Is It? Lupus is thought to develop when the immune system
ONE of the following:
 Medical Coverage Policy Belimumab (Benlysta) EFFECTIVE DATE: 01 01 2012 POLICY LAST UPDATED: 11 21 2017 OVERVIEW Belimumab (Benlysta ) is indicated for the treatment of adult patients with active, autoantibody-positive,
Medical Coverage Policy Belimumab (Benlysta) EFFECTIVE DATE: 01 01 2012 POLICY LAST UPDATED: 11 21 2017 OVERVIEW Belimumab (Benlysta ) is indicated for the treatment of adult patients with active, autoantibody-positive,
Rheumatology Primer: What Labs and When
 Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Lupus and Friends Perspectives on common syndromes and Primary care responses
 Lupus and Friends Perspectives on common syndromes and Primary care responses Paul H Caldron DO, PhD, FACP, FACR, MBA Arizona Arthritis and Rheumatology Associates, PC University of Arizona College of
Lupus and Friends Perspectives on common syndromes and Primary care responses Paul H Caldron DO, PhD, FACP, FACR, MBA Arizona Arthritis and Rheumatology Associates, PC University of Arizona College of
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Policy. Section: Medicine Effective Date: January 15, 2015 Subsection: Pathology/Laboratory Original Policy Date: December 5, 2014 Subject:
 Last Review Status/Date: December 2014 Page: 1 of 10 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Last Review Status/Date: December 2014 Page: 1 of 10 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
To live with lupus, we need to know about lupus.
 To live with lupus, we need to know about lupus. Zineb Aouhab, MD Assistant Professor of Medicine Loyola University Medical Center Division of Rheumatology 1 Where did the word lupus come from? The word
To live with lupus, we need to know about lupus. Zineb Aouhab, MD Assistant Professor of Medicine Loyola University Medical Center Division of Rheumatology 1 Where did the word lupus come from? The word
LUPUS (SLE) MEDICAL SOURCE STATEMENT
 MEDICAL SOURCE STATEMENT") LUPUS (SLE) MEDICAL SOURCE STATEMENT From: Re: (Name of Patient) (Social Security No.) Please answer the following questions concerning your patient s impairments. Attach relevant treatment notes, radiologist
LUPUS (SLE) MEDICAL SOURCE STATEMENT From: Re: (Name of Patient) (Social Security No.) Please answer the following questions concerning your patient s impairments. Attach relevant treatment notes, radiologist
Learning about Lupus. Learning About Lupus. Lupus Society of Illinois
 Learning About Lupus Learning about Lupus Lupus Society of Illinois 525 W. Monroe Street, Suite 900 Chicago, Illinois 60661 Robert S. Katz, M.D. Professor of Medicine Rush University Medical Center Northwestern
Learning About Lupus Learning about Lupus Lupus Society of Illinois 525 W. Monroe Street, Suite 900 Chicago, Illinois 60661 Robert S. Katz, M.D. Professor of Medicine Rush University Medical Center Northwestern
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital
 Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Systemic Lupus Erythematosus among Jordanians: A Single Rheumatology Unit Experience
 Systemic Lupus Erythematosus among Jordanians: A Single Rheumatology Unit Experience Ala M. AlHeresh MD* ABSTRACT Objectives: To study the characteristics of Systemic Lupus Erythematosus in Jordan and
Systemic Lupus Erythematosus among Jordanians: A Single Rheumatology Unit Experience Ala M. AlHeresh MD* ABSTRACT Objectives: To study the characteristics of Systemic Lupus Erythematosus in Jordan and
Take Home Messages: Hint: Use all the Q and A sa My view of what is board and clinically relevant
 Take Home Messages: Hint: Use all the Q and A sa My view of what is board and clinically relevant Jonathan S. Coblyn MD Systemic Lupus Erythematosus Summary SLE is a multi-system autoimmune disorder SLE
Take Home Messages: Hint: Use all the Q and A sa My view of what is board and clinically relevant Jonathan S. Coblyn MD Systemic Lupus Erythematosus Summary SLE is a multi-system autoimmune disorder SLE
The Power of the ANA. April 2018 Emily Littlejohn, DO MPH
 Emergent Rheumatologic Diseases and Disorders for Primary Care. The Power of the ANA April 2018 Emily Littlejohn, DO MPH Question 1: the ANA test is: A) A screening test with high specificity to diagnose
Emergent Rheumatologic Diseases and Disorders for Primary Care. The Power of the ANA April 2018 Emily Littlejohn, DO MPH Question 1: the ANA test is: A) A screening test with high specificity to diagnose
Manifestation of Antiphospholipid Syndrome among Saudi patients :examining the applicability of sapporo Criteria
 Manifestation of Antiphospholipid Syndrome among Saudi patients :examining the applicability of sapporo Criteria Farjah H AlGahtani Associate professor,md,mph Leukemia,Lymphoma in adolescent,thromboembolic
Manifestation of Antiphospholipid Syndrome among Saudi patients :examining the applicability of sapporo Criteria Farjah H AlGahtani Associate professor,md,mph Leukemia,Lymphoma in adolescent,thromboembolic
10/6/08. Systemic Lupus Erythematosus. SLE Epidemiology: who is at risk? Margrit Wiesendanger Division of Rheumatology, CUMC.
 Systemic Lupus Erythematosus SLE Epidemiology: who is at risk? One of the most common autoimmune diseases affecting women of all ages Predominantly women in child-bearing years (M:F ratio is 1:10) Incidence
Systemic Lupus Erythematosus SLE Epidemiology: who is at risk? One of the most common autoimmune diseases affecting women of all ages Predominantly women in child-bearing years (M:F ratio is 1:10) Incidence
COMPLEX CUTANEOUS LUPUS CASES PEARLS AND PITFALLS
 COMPLEX CUTANEOUS LUPUS CASES PEARLS AND PITFALLS Benjamin F. Chong, MD, MSCS February 17, 2018 CONFLICTS OF INTEREST D I S CLOSURE OF R E LATI ONSHIPS W I T H I NDUSTRY Benjamin Chong, MD, MSCS F059 Complex
COMPLEX CUTANEOUS LUPUS CASES PEARLS AND PITFALLS Benjamin F. Chong, MD, MSCS February 17, 2018 CONFLICTS OF INTEREST D I S CLOSURE OF R E LATI ONSHIPS W I T H I NDUSTRY Benjamin Chong, MD, MSCS F059 Complex
Policy. Background
 Last Review Status/Date: December 2016 Page: 1 of 11 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Last Review Status/Date: December 2016 Page: 1 of 11 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Section: Medicine Effective Date: January 15, 2016 Subsection: Pathology/Laboratory Original Policy Date: December 5, 2014 Subject:
 Last Review Status/Date: December 2015 Page: 1 of 11 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Last Review Status/Date: December 2015 Page: 1 of 11 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Lupus as a risk factor for cardiovascular disease
 Lupus as a risk factor for cardiovascular disease SØREN JACOBSEN Department Rheumatology, Rigshospitalet Søren Jacobsen Main sponsors: Gigtforeningen Novo Nordisk Fonden Rigshospitalet Disclaimer: Novo
Lupus as a risk factor for cardiovascular disease SØREN JACOBSEN Department Rheumatology, Rigshospitalet Søren Jacobsen Main sponsors: Gigtforeningen Novo Nordisk Fonden Rigshospitalet Disclaimer: Novo
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital
 Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
CSTAR CASE STUDIES: BLOCK F Type 3 Hypersensitivity Reaction
 CSTAR CASE STUDIES: BLOCK F Type 3 Hypersensitivity Reaction Setting: ER Mr. Smith I ve just felt so weak for so long, and I ve lost so much weight, and now I m having trouble breathing it s affecting
CSTAR CASE STUDIES: BLOCK F Type 3 Hypersensitivity Reaction Setting: ER Mr. Smith I ve just felt so weak for so long, and I ve lost so much weight, and now I m having trouble breathing it s affecting
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
SLE-key Case Studies
 SLE-key Case Studies Ellen M. Field, M.D. Lehigh Valley Health Network, Bethlehem, PA Donald E. Thomas, Jr., M.D., FACP, FACR, RhMSUS, CCD Arthritis and Pain Assoc. of PG County, Greenbelt, MD Case Study
SLE-key Case Studies Ellen M. Field, M.D. Lehigh Valley Health Network, Bethlehem, PA Donald E. Thomas, Jr., M.D., FACP, FACR, RhMSUS, CCD Arthritis and Pain Assoc. of PG County, Greenbelt, MD Case Study
Evidence Based Treatment of SLE with Treatment Algorithm. Dr. Md. Mujibur Rahman Professor of Medicine Shaheed Suhrawardy Medical College
 Evidence Based Treatment of SLE with Treatment Algorithm Dr. Md. Mujibur Rahman Professor of Medicine Shaheed Suhrawardy Medical College Natural Histoty Inflammatory multisystem disease Onset usually between
Evidence Based Treatment of SLE with Treatment Algorithm Dr. Md. Mujibur Rahman Professor of Medicine Shaheed Suhrawardy Medical College Natural Histoty Inflammatory multisystem disease Onset usually between
DISCUSSION BY: Dr M. R. Shakeebi, MD, Rheumatologist
 Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
UPDATES ON PEDIATRIC SLE
 UPDATES ON PEDIATRIC SLE BY ANGELA MIGOWA, PEDIATRIC RHEUMATOLOGIST/SENIOR INSTRUCTOR AKUHN MBCHB-UON, MMED-AKUHN,PEDIATRIC RHEUMATOLOGY- MCGILL UNIVERSITY HEALTH CENTRE ROSA PARKS OBJECTIVES RECOGNIZE
UPDATES ON PEDIATRIC SLE BY ANGELA MIGOWA, PEDIATRIC RHEUMATOLOGIST/SENIOR INSTRUCTOR AKUHN MBCHB-UON, MMED-AKUHN,PEDIATRIC RHEUMATOLOGY- MCGILL UNIVERSITY HEALTH CENTRE ROSA PARKS OBJECTIVES RECOGNIZE
Patient with Musculo-skeletal Complaints - Summary
 Patient with Musculo-skeletal Complaints - Summary 1. Soft Tissue Rheumatism or Arthritis 2. Arthritis Monoarticular Polyarticular - :- (Asymmetrical) (Symetrical) :- -Crystals, Gout - Infective acute
Patient with Musculo-skeletal Complaints - Summary 1. Soft Tissue Rheumatism or Arthritis 2. Arthritis Monoarticular Polyarticular - :- (Asymmetrical) (Symetrical) :- -Crystals, Gout - Infective acute
PS + MPs PS - MPs 37% 36% 64% 64%
 Supplementary Figure 1. Amount and distribution of phosphatidylserine negative (PS - ) and phosphatidylserine positive (PS + ) MPs in 280 SLE patients and 280 controls. Circles are proportional to the
Supplementary Figure 1. Amount and distribution of phosphatidylserine negative (PS - ) and phosphatidylserine positive (PS + ) MPs in 280 SLE patients and 280 controls. Circles are proportional to the
Living with Lupus. Helping Your Patient With Systemic Lupus Erythematosus By Hussein M. Halaby, MBBS, ABIM, FRCPC; and John M. Esdaile, MD, MPH, FRCPC
 Focus on CME at the University McGill University of British Columbia Living with Lupus Helping Your Patient With Systemic Lupus Erythematosus By Hussein M. Halaby, MBBS, ABIM, FRCPC; and John M. Esdaile,
Focus on CME at the University McGill University of British Columbia Living with Lupus Helping Your Patient With Systemic Lupus Erythematosus By Hussein M. Halaby, MBBS, ABIM, FRCPC; and John M. Esdaile,
Residual Functional Capacity Questionnaire SYSTEMIC LUPUS ERYTHEMATOSUS
 Residual Functional Capacity Questionnaire SYSTEMIC LUPUS ERYTHEMATOSUS Patient: DOB: Physician completing this form: Please complete the following questions regarding this patient's impairments and attach
Residual Functional Capacity Questionnaire SYSTEMIC LUPUS ERYTHEMATOSUS Patient: DOB: Physician completing this form: Please complete the following questions regarding this patient's impairments and attach
Systemic Lupus Erythematosus. Margrit Wiesendanger Division of General Medicine, CUMC
 Systemic Lupus Erythematosus Margrit Wiesendanger Division of General Medicine, CUMC October 13, 2009 SLE Epidemiology: who is at risk? One of the most common autoimmune diseases affecting women of all
Systemic Lupus Erythematosus Margrit Wiesendanger Division of General Medicine, CUMC October 13, 2009 SLE Epidemiology: who is at risk? One of the most common autoimmune diseases affecting women of all
Is it Autoimmune or NOT! Presented to AONP! October 2015!
 Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Living with Lupus. LFA - Georgia Gary E Myerson MD Arthritis and Rheumatology of GA
 Living with Lupus LFA - Georgia Gary E Myerson MD Arthritis and Rheumatology of GA LUPUS A REALITY CHECK LUPUS A REALITY CHECK LUPUS A REALITY CHECK LUPUS A REALITY CHECK SLE 1.5 million Americans: some
Living with Lupus LFA - Georgia Gary E Myerson MD Arthritis and Rheumatology of GA LUPUS A REALITY CHECK LUPUS A REALITY CHECK LUPUS A REALITY CHECK LUPUS A REALITY CHECK SLE 1.5 million Americans: some
Undifferentiated Connective Tissue Disease and Overlap Syndromes. Mark S. Box, MD
 Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Test Name Results Units Bio. Ref. Interval
 LL - LL-ROHINI (NATIONAL REFERENCE 135091593 Age 25 Years Gender Male 30/8/2017 91600AM 30/8/2017 93946AM 31/8/2017 84826AM Ref By Final COLLAGEN DISEASES ANTIBODY ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF),
LL - LL-ROHINI (NATIONAL REFERENCE 135091593 Age 25 Years Gender Male 30/8/2017 91600AM 30/8/2017 93946AM 31/8/2017 84826AM Ref By Final COLLAGEN DISEASES ANTIBODY ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF),
Committee Approval Date: May 9, 2014 Next Review Date: May 2015
 Medication Policy Manual Policy No: dru248 Topic: Benlysta, belimumab Date of Origin: May 13, 2011 Committee Approval Date: May 9, 2014 Next Review Date: May 2015 Effective Date: June 1, 2014 IMPORTANT
Medication Policy Manual Policy No: dru248 Topic: Benlysta, belimumab Date of Origin: May 13, 2011 Committee Approval Date: May 9, 2014 Next Review Date: May 2015 Effective Date: June 1, 2014 IMPORTANT
Test Name Results Units Bio. Ref. Interval
 135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
CIBMTR Center Number: CIBMTR Recipient ID: RETIRED. Today s Date: Date of HSCT for which this form is being completed: &
 Systemic Lupus Erythematosus Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: & HSCT type: o autologous o allogeneic, o
Systemic Lupus Erythematosus Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: & HSCT type: o autologous o allogeneic, o
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Serum Biomarker Panel Testing for Systemic Lupus Erythematosus
 Serum Biomarker Panel Testing for Systemic Lupus Erythematosus Policy Number: 2.04.123 Last Review: 8/2017 Origination: 8/2015 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Serum Biomarker Panel Testing for Systemic Lupus Erythematosus Policy Number: 2.04.123 Last Review: 8/2017 Origination: 8/2015 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue
Antiphospholipid Syndrome Handbook
 Antiphospholipid Syndrome Handbook Maria Laura Bertolaccini, Oier Ateka-Barrutia, and Munther A. Khamashta Antiphospholipid Syndrome Handbook Maria Laura Bertolaccini, MD, PhD Lupus Research Unit The Rayne
Antiphospholipid Syndrome Handbook Maria Laura Bertolaccini, Oier Ateka-Barrutia, and Munther A. Khamashta Antiphospholipid Syndrome Handbook Maria Laura Bertolaccini, MD, PhD Lupus Research Unit The Rayne
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Demystifying. Systemic Lupus Erythematosus: Signs and Symptoms for Early Recognition. Teaching Fellows in Lupus Project
 Demystifying Systemic Lupus Erythematosus: Signs and Symptoms for Early Recognition Teaching Fellows in Lupus Project Introduction: Why are we here? Lupus can take 4-6 years and 3 providers before diagnosis*
Demystifying Systemic Lupus Erythematosus: Signs and Symptoms for Early Recognition Teaching Fellows in Lupus Project Introduction: Why are we here? Lupus can take 4-6 years and 3 providers before diagnosis*
The Diagnosis of Lupus
 The Diagnosis of Lupus LUPUSUK 2017 This information booklet has been produced by LUPUS UK 2017 LUPUS UK LUPUS UK is the registered national charity for people with systemic lupus erythematosus (SLE) and
The Diagnosis of Lupus LUPUSUK 2017 This information booklet has been produced by LUPUS UK 2017 LUPUS UK LUPUS UK is the registered national charity for people with systemic lupus erythematosus (SLE) and
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: belimumab_benlysta 6/2011 2/2018 2/2019 3/2018 Description of Procedure or Service Belimumab (Benlysta) is
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: belimumab_benlysta 6/2011 2/2018 2/2019 3/2018 Description of Procedure or Service Belimumab (Benlysta) is
Epidemiology and aetiology
 Juvenile SLE Paul Brogan Professor of Vasculitis and Consultant in Paediatric Rheumatology UCL Institute of child health and Great Ormond Street Hospital NHS foundation trust, London, UK Overview Epidemiology
Juvenile SLE Paul Brogan Professor of Vasculitis and Consultant in Paediatric Rheumatology UCL Institute of child health and Great Ormond Street Hospital NHS foundation trust, London, UK Overview Epidemiology
Cases I have Learned From. Jeffrey P. Callen, MD Professor of Medicine (Dermatology) University of Louisville
 University of Louisville") Cases I have Learned From Jeffrey P. Callen, MD Professor of Medicine (Dermatology) University of Louisville Jeffrey P. Callen, MD Disclosure (previous 12 months) Consultant/Advisory board Auxilium Consultant
Cases I have Learned From Jeffrey P. Callen, MD Professor of Medicine (Dermatology) University of Louisville Jeffrey P. Callen, MD Disclosure (previous 12 months) Consultant/Advisory board Auxilium Consultant
Systemic Lupus Erythematosus (SLE) Epidemiology of SLE (United States)
 Epidemiology of SLE (United States)") 1:10-2:25pm Closing the Loop on Lupus: Primary Care s Key Role in the Elusive Diagnosis and Management of Patients SPEAKER Richard Sadovsky, MD Richard Furie, MD Disclosures This session is supported by
1:10-2:25pm Closing the Loop on Lupus: Primary Care s Key Role in the Elusive Diagnosis and Management of Patients SPEAKER Richard Sadovsky, MD Richard Furie, MD Disclosures This session is supported by
Autoimmune diseases. SLIDE 3: Introduction to autoimmune diseases Chronic
 SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
MANAGING THE PATIENT WITH POSITIVE ANA
 MANAGING THE PATIENT WITH POSITIVE ANA Rafael F. Rivas-Chacon, M.D. Disclosures Grant/Research support for: Pfizer Study JIA A3921104 Tofacitinib not related to this presentation 1 Positive Antinuclear
MANAGING THE PATIENT WITH POSITIVE ANA Rafael F. Rivas-Chacon, M.D. Disclosures Grant/Research support for: Pfizer Study JIA A3921104 Tofacitinib not related to this presentation 1 Positive Antinuclear
Systemic Lupus Erythematosus
 A Patient s Guide to Systemic Lupus Erythematosus 2 kidneys. These changes make it impossible for the kidneys to function normally. The inflammation of SLE can be seen in the lining, covering, and muscles
A Patient s Guide to Systemic Lupus Erythematosus 2 kidneys. These changes make it impossible for the kidneys to function normally. The inflammation of SLE can be seen in the lining, covering, and muscles
ACP Rheumatology Pearls. Adam Q Carlson MD Assistant Professor UVA Rheumatology
 ACP Rheumatology Pearls Adam Q Carlson MD Assistant Professor UVA Rheumatology Disclosures I have no personal or professional disclosures Case #1 27 yo woman with a history of systemic lupus complicated
ACP Rheumatology Pearls Adam Q Carlson MD Assistant Professor UVA Rheumatology Disclosures I have no personal or professional disclosures Case #1 27 yo woman with a history of systemic lupus complicated
MP Serum Biomarker Panel Testing for Systemic Lupus Erythematosus and Other Connective Tissue Diseases
 Medical Policy MP 2.04.123 Serum Biomarker Panel Testing for Systemic Lupus Erythematosus and Other Connective Tissue Diseases BCBSA Ref. Policy: 2.04.123 Last Review: 06/27/2018 Effective Date: 06/27/2018
Medical Policy MP 2.04.123 Serum Biomarker Panel Testing for Systemic Lupus Erythematosus and Other Connective Tissue Diseases BCBSA Ref. Policy: 2.04.123 Last Review: 06/27/2018 Effective Date: 06/27/2018
Systemic Lupus Erythematosus (SLE) Learning Objectives. Presenter Disclosure Information
 Learning Objectives. Presenter Disclosure Information") 9:30 10:45 AM Closing the Loop on Lupus: Primary Care s Key Role in the Elusive Diagnosis and Management of Patients Presenter Disclosure Information The following relationships exist related to this presentation:
9:30 10:45 AM Closing the Loop on Lupus: Primary Care s Key Role in the Elusive Diagnosis and Management of Patients Presenter Disclosure Information The following relationships exist related to this presentation:
Acute Emergencies in Rheumatology
 Acute Emergencies in Rheumatology Clare Higgens Northwick Park hospital and St George s Hospital London Acute Rheumatological Emergencies The Acute Hot joint Inflammatory back pain.. Systemic lupus erythematosus(sle)
Acute Emergencies in Rheumatology Clare Higgens Northwick Park hospital and St George s Hospital London Acute Rheumatological Emergencies The Acute Hot joint Inflammatory back pain.. Systemic lupus erythematosus(sle)
Antiphospholipid antibodies
 CARDIOLOGY PATIENT PAGE CARDIOLOGY PATIENT PAGE Antiphospholipid Antibodies Caron P. Misita, PharmD; Stephan Moll, MD Antiphospholipid antibodies (APLAs) are proteins that may be present in the blood and
CARDIOLOGY PATIENT PAGE CARDIOLOGY PATIENT PAGE Antiphospholipid Antibodies Caron P. Misita, PharmD; Stephan Moll, MD Antiphospholipid antibodies (APLAs) are proteins that may be present in the blood and
Mohammadreza Tabatabaei IBTO COAG LAB
 Tests for the Evaluation of Lupus Anticoagulants t Mohammadreza Tabatabaei MSc Hematology blood bank MSc Hematology blood bank IBTO COAG LAB Lupus Anticoagulants General Background Lupus anticoagulants
Tests for the Evaluation of Lupus Anticoagulants t Mohammadreza Tabatabaei MSc Hematology blood bank MSc Hematology blood bank IBTO COAG LAB Lupus Anticoagulants General Background Lupus anticoagulants
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Cutaneous manifestations and systemic correlation in patients with lupus erythematosus and its subsets: a study of 40 cases
 International Journal of Research in Dermatology Mahajan R et al. Int J Res Dermatol. 2018 Nov;4(4):479-483 http://www.ijord.com Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4529.intjresdermatol20183407
International Journal of Research in Dermatology Mahajan R et al. Int J Res Dermatol. 2018 Nov;4(4):479-483 http://www.ijord.com Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4529.intjresdermatol20183407
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Belimumab Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 4 Effective Date... 11/15/2017 Next
Cigna Drug and Biologic Coverage Policy Subject Belimumab Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 4 Effective Date... 11/15/2017 Next
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Serum Biomarker Panel Testing for Systemic Lupus Erythematosus and Other Connective Tissue Diseases
 Serum Biomarker Panel Testing for Systemic Lupus Erythematosus and Other Connective Tissue Diseases Policy Number: 2.04.123 Last Review: 8/2018 Origination: 8/2015 Next Review: 8/2019 Policy Blue Cross
Serum Biomarker Panel Testing for Systemic Lupus Erythematosus and Other Connective Tissue Diseases Policy Number: 2.04.123 Last Review: 8/2018 Origination: 8/2015 Next Review: 8/2019 Policy Blue Cross
10/25/2018. Autoimmunity and how to treat it. Disclosure. Why do we get autoimmunity? James Verbsky MD/PhD Pediatric Rheumatology/Immunology
 Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Late onset systemic lupus erythematosus in southern Chinese. Citation Annals Of The Rheumatic Diseases, 1998, v. 57 n. 7, p.
 Title Late onset systemic lupus erythematosus in southern Chinese Author(s) Ho, CTK; Mok, CC; Lau, CS; Wong, RWS Citation Annals Of The Rheumatic Diseases, 1998, v. 57 n. 7, p. 437-440 Issued Date 1998
Title Late onset systemic lupus erythematosus in southern Chinese Author(s) Ho, CTK; Mok, CC; Lau, CS; Wong, RWS Citation Annals Of The Rheumatic Diseases, 1998, v. 57 n. 7, p. 437-440 Issued Date 1998
Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist
 Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist Wisconsin Institute of Discovery Karen Rossi/Bristol-Myers Squibb Morey A. Blinder, MD Washington University, St. Louis, MO March
Antiphospholipid Antibody Syndrome: Management Issues for the Hematologist Wisconsin Institute of Discovery Karen Rossi/Bristol-Myers Squibb Morey A. Blinder, MD Washington University, St. Louis, MO March
Systemic lupus erythematosus in 50 year olds
 Postgrad Med J (1992) 68, 440-444 The Fellowship of Postgraduate Medicine, 1992 Systemic lupus erythematosus in 50 year olds I. Domenech, 0. Aydintug, R. Cervera, M. Khamashta, A. Jedryka-Goral, J.L. Vianna
Postgrad Med J (1992) 68, 440-444 The Fellowship of Postgraduate Medicine, 1992 Systemic lupus erythematosus in 50 year olds I. Domenech, 0. Aydintug, R. Cervera, M. Khamashta, A. Jedryka-Goral, J.L. Vianna
Systemic Lupus Erythematosus in Children and Adolescents Beth S. Gottlieb and Norman T. Ilowite. DOI: /pir
 Systemic Lupus Erythematosus in Children and Adolescents Beth S. Gottlieb and Norman T. Ilowite Pediatr. Rev. 2006;27;323-330 DOI: 10.1542/pir.27-9-323 The online version of this article, along with updated
Systemic Lupus Erythematosus in Children and Adolescents Beth S. Gottlieb and Norman T. Ilowite Pediatr. Rev. 2006;27;323-330 DOI: 10.1542/pir.27-9-323 The online version of this article, along with updated
Immune tolerance, autoimmune diseases
 Immune tolerance, autoimmune diseases Immune tolerance Central: negative selection during thymic education deletion of autoreactive B-lymphocytes in bone marrow Positive selection in the thymus Negative
Immune tolerance, autoimmune diseases Immune tolerance Central: negative selection during thymic education deletion of autoreactive B-lymphocytes in bone marrow Positive selection in the thymus Negative
Myositis and Your Lungs
 Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Manifestations and Presentations of Collagen Vascular Diseases. Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL
 Manifestations and Presentations of Collagen Vascular Diseases Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL June 29, 2018 Disclosures Joseph LaConti, M.D., Ph.D., has
Manifestations and Presentations of Collagen Vascular Diseases Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL June 29, 2018 Disclosures Joseph LaConti, M.D., Ph.D., has
Rheumatology 101 A Pediatrician s Guide
 Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Controversies in Women s Health: Clinical Dilemmas in Arthritis
 Controversies in Women s Health: Clinical Dilemmas in Arthritis Jonathan Graf, M.D. Assistant Professor of Medicine, UCSF Division of Rheumatology, SFGH December, 2008 Approximate Prevalence of Rheumatic
Controversies in Women s Health: Clinical Dilemmas in Arthritis Jonathan Graf, M.D. Assistant Professor of Medicine, UCSF Division of Rheumatology, SFGH December, 2008 Approximate Prevalence of Rheumatic
NATIONAL LABORATORY HANDBOOK. Laboratory Testing for Antinuclear antibodies
 NATIONAL LABORATORY HANDBOOK Laboratory Testing for Antinuclear antibodies Document reference number CSPD013/2018 Document developed by National Clinical Programme for Pathology Revision number Version
NATIONAL LABORATORY HANDBOOK Laboratory Testing for Antinuclear antibodies Document reference number CSPD013/2018 Document developed by National Clinical Programme for Pathology Revision number Version
Neuropsychiatric SLE (NPSLE) Dr. MTL NYO FCP(SA), Cert Rheum (Phys) Division of Rheumatology Department of Internal Medicine DGMAH / SMU
 Dr. MTL NYO FCP(SA), Cert Rheum (Phys) Division of Rheumatology Department of Internal Medicine DGMAH / SMU") Neuropsychiatric SLE (NPSLE) Dr. MTL NYO FCP(SA), Cert Rheum (Phys) Division of Rheumatology Department of Internal Medicine DGMAH / SMU NPSLE represents a diagnostic and therapeutic challenge Wide range
Neuropsychiatric SLE (NPSLE) Dr. MTL NYO FCP(SA), Cert Rheum (Phys) Division of Rheumatology Department of Internal Medicine DGMAH / SMU NPSLE represents a diagnostic and therapeutic challenge Wide range
Rheumatology E-learning. University of Szeged Department of Rheumatology and Immunology
 Rheumatology E-learning University of Szeged Department of Rheumatology and Immunology Overview Prototype autoimmune disease The most common and variable systemic autoimmune connective disease Female:male:
Rheumatology E-learning University of Szeged Department of Rheumatology and Immunology Overview Prototype autoimmune disease The most common and variable systemic autoimmune connective disease Female:male:
DRAFT. AAF Case Discussion Guide. Key Learning Objectives
 AAF Case Discussion Guide Key Learning Objectives List the differential diagnosis for a systemic disease presentation with multisystem involvement Identify the key questions from the history to look for
AAF Case Discussion Guide Key Learning Objectives List the differential diagnosis for a systemic disease presentation with multisystem involvement Identify the key questions from the history to look for
Mary Derlacki, FNP. No financial relationships to disclose. Office Rheumatology for the Nurse Practitioner. Rheumatoid Arthritis
 Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
Early diagnosis of systemic lupus erythematosus in primary care by family doctors
 ISSN 2229-5518 2,302 Early diagnosis of systemic lupus erythematosus in primary care by family doctors Saad Ali Alalyani, Abdullah Saad Alalyani, Sultan Salem Algethami, Hamad Sulayyih Alosaimi, Abdullah
ISSN 2229-5518 2,302 Early diagnosis of systemic lupus erythematosus in primary care by family doctors Saad Ali Alalyani, Abdullah Saad Alalyani, Sultan Salem Algethami, Hamad Sulayyih Alosaimi, Abdullah
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
4. Behçet s - Treatment
 Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk 4. Behçet s - Treatment Introduction Because Behçet s Syndrome/Disease is a multisystem disorder,
Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk 4. Behçet s - Treatment Introduction Because Behçet s Syndrome/Disease is a multisystem disorder,
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa
 Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally