Osteoporosis, Osteomalasia & rickets. Bone disorders
|
|
|
- Baldwin Dennis
- 6 years ago
- Views:
Transcription
1 Osteoporosis, Osteomalasia & rickets Bone disorders
2 Thank You for Your comments Voice--- Ok Lecture too long--- this is in schedule??? More interaction--- I can do that inshalla Slides are crowded--- but slides r the ref No short not in exam--- no can do Topics--- unfortunately I don t choose them More S & S--- in therapeutics (dr. hous)
3 Bone function and composition 1. The skeleton provides structural support, 2. protects vital organs & the hematopoietic system, 3. and maintains homeostasis of calcium & other ions. The two types of bone: 1. trabecular (cancellous) 2. and cortical (compact) bone
4 occur in varying amounts at different anatomic sites: Distal radius: 75% cortical and 25% trabecular Lumbar spine: 34% cortical and 66% trabecular Femoral neck: 75% cortical and 25% trabecular Trochanter: 50% cortical and 50% trabecular.
5 Bone function & compestion Trabecular bone is a meshwork of struts giving it a large surface area that is in close contact with the bone marrow cavity for bone turnover and metabolic activity. Cortical bone is formed in layers & is highly calcified (about 80% to 90%). Because of these different structures & environments, trabecular bone is more metabolically active & cortical bone is more structurally strong and protective.
6 Bone function & composition Bone comprises minerals (50-70%), an organic matrix (20-40%), water (5-10%), and lipids (<3%). The predominant mineral is hydroxyapatite [3Ca3(PO4)2(OH)2]. Bone contains 99% of the body s calcium and 85% of its phosphorus.
7 Bone function & composition The organic matrix is primarily protein; 90% type I collagen & 10-15% non collagenous protein and γ -carboxylated proteins; and cells (osteoclasts, osteoblasts, and osteocytes). The mineral provides strength & rigidity while the proteins provide elasticity & flexibility.
8 Bone remodeling and its control The skeleton undergoes constant remodeling throughout life. Peak bone mass is achieved by age years, long after maximum bone length has been achieved. Men achieve higher peak bone mass than women. For 5-10 years after menopause, women have accelerated bone loss, up to 3% per year. Age-related bone loss, about 0.5% per year, begins years after menopause in women & in men at about age 55 years.
9 Bone remodeling & its control Bone is a dynamic tissue. The majority of the skeleton is replaced approximately every 7-10 years. Remodeling repairs microfractures, prepares bone for weight bearing, & provides access to mineral stores. Teams of osteoclasts & osteoblasts, termed basic multicellular units (BMUs), perform this remodeling process. Steps in remodeling are resorption, reversal, formation, and quiescence
10 Bone remodeling & its control This process begins with activation of osteoclasts, causing bone resorption. Osteoclasts attach to bone by an integrin, αvβ3, and create a leakproof seal. The osteoclast s ruffled border secretes acid and proteases, such as H+ & cathepsin K, to dissolve bone.
11 Bone remodeling & its control Osteoclasts create tunnels in cortical bone and pits in trabecular bone. By-products of collagen degradation include hydroxyproline, and N-terminal and C-terminal collagen peptides, which can also serve as biomarkers of resorption. When excavation is complete, reversal begins by osteoclasts undergoing apoptosis or moving to a new section. Resorption takes 3 to 4 weeks.
12 Bone remodeling & its control Formation begins with osteoblasts making osteoid that is mineralized over the ensuing 3 to 4 months. Osteoblasts then either line the bone (lining cells) or become part of the bone as osteocytes. Quiescence follows mineralization
13 Bone remodeling & its control Numerous agents control mesenchymal stem cell derivation and differentiation of osteoblasts Osteoclasts are derived from the myeloid/monocyte cell line with derivation & differentiation also under the control of numerous agents, some of which are expressed from osteoblasts.
14 Bone remodeling & its control A complex array and timing of cytokines and hormones control osteoblasts & osteoclasts during bone remodeling Intensive investigation continues to define the complete process. Although the triggers to begin remodeling are not completely understood, osteocytes may act as mechanosensors, reacting to bone strain & sensing fatigue and damage. Osteocytes communicate with lining cells via a homing signal, which is thought to summon osteoclast precursors to initiate resorption.
15 Bone remodeling & its control Osteoblasts regulate osteoclastic activity by secreting colony-stimulating factors (macrophage colony-stimulating factor [MCSF]; CSF-1) to promote differentiation of osteoclast precursors, receptor activator of nuclear factor κb ligand (RANKL) to promote osteoclast differentiation and maturation, and osteoprotegerin (OPG) to compete with RANKL and prevent osteoclastic differentiation.
16 Bone remodeling & its control Regulation of osteoblast secretion of CSF 1, RANKL, and OPG is complex, involving parathyroid hormone (PTH), 1α-25- dihydroxyvitamin D, leptin, estrogen, and other agents. Transforming growth factor-β (TGF-β), plateletderived growth factor (PDGF), insulin-like growth factor-1 (IGF-1), PTH, growth hormone, & other factors promote bone formation.
17 Bone remodeling & its control Bone mineral density peaks between the ages of 20 & 30 in men and women. Peak bone mass and rate of bone loss is controlled partly by genetics. Under normal conditions in adults, resorption equals formation for no net loss or gain of bone mass. Aging, menopause, & certain diseases & drugs can create an imbalance between formation & resorption & result in bone loss.
18 Serum Ca & Phos Regulation & Vitamin D Metabolism
19 Serum Ca & Phos Regulation & Vitamin D Metabolism Vitamin D and PTH maintain calcium homeostasis. The sun converts 7-dehydrocholesterol in the skin to vitamin D3. Sunscreens inhibit vitamin D skin production. Although a few foods naturally contain vitamin D3 (e.g.,cholecalciferol from fish oils) or vitamin D2 (e.g., ergocalciferol from plants), most dietary intake is from foods fortified with vitamin D.
20 Serum Ca & Phos Regulation & Vitamin D Metabolism Because both vitamin D3 & D2 work similarly in the body, they are referred to here as vitamin D. Vitamin D undergoes hepatic conversion to 25(OH) vitamin D (calcidiol) via D-25-hydroxylase (cytochrome P450 27A1). PTH stimulates renal conversion of 25- hydroxyvitamin D to the active form, 1α-25- dihydroxyvitamin D (calcitriol), via 25(OH)D-1αhydroxylase (cytochrome P450 27B1).
21 Serum Ca & Phos Regulation & Vitamin D Metabolism Decreased serum calcium concentrations lead to increased serum PTH concentrations, which lead to elevated calcitriol concentrations Calcitriol promotes intestinal calcium absorption, & calcitriol & PTH work together to release calcium from bone to restore homeostasis.
22 Serum Ca & Phos Regulation & Vitamin D Metabolism Vitamin D receptors are found in many tissues, such as bone, intestine, brain, heart, stomach, pancreas, lymphocytes, skin, and gonads. Serum phosphorus is less tightly regulated than serum calcium. Excess ingested phosphorus is absorbed and adjusted by the kidney. PTH also controls the kidney set point and decreases renal phosphorus reabsorption.
23 Pathophysiology of osteoporosis
24
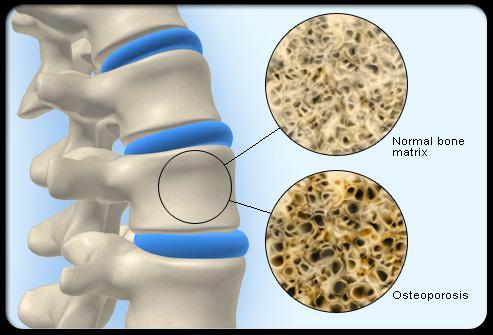
25 Pathophysiology of osteoporosis Osteoporosis is characterized by low bone mass and microarchitectural deterioration of bone tissue leading to enhanced bone fragility and a consequent increase in fracture risk. Bone loss results when resorption exceeds formation. TheWorld Health Organization classifies bone mass based on T-score (number of standard deviations from the mean compared to bone mass of average young women).
26 Pathophysiology of osteoporosis Normal bone mass is defined as a T-score greater than 1, osteopenia as a Tscore of 1 to 2.5, and osteoporosis as a T-score of less than 2.5. In addition to low BMD, high bone turnover, poor bone strength, & impaired bone architecture result in the bone s increased susceptibility to fracture.
27 Pathophysiology of osteoporosis Women with osteopenia have a 1.8-fold increase in fracture rate, & women with osteoporosis have a fourfold increase in fracture rate, compared to women with normal BMD.
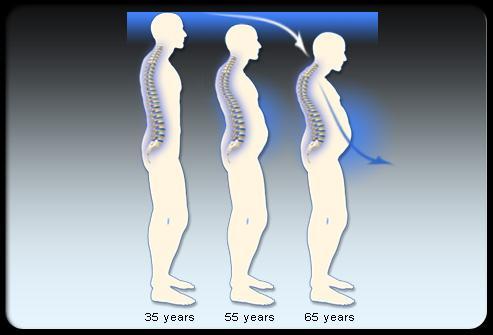
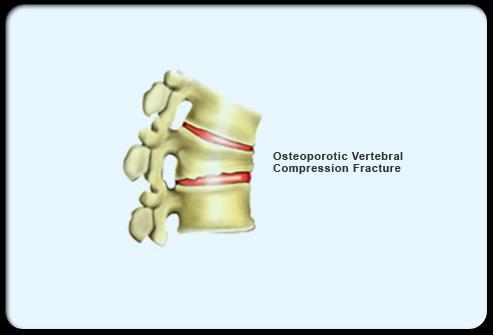
28 Pathophysiology of osteoporosis Clinically, osteoporosis is categorized as postmenopausal, age related, or secondary. Postmenopausal osteoporosis affects primarily trabecular bone in the decade following menopause, with fractures occurring predominantly at vertebral & distal forearm sites. Within a few years after peak BMD is attained, usually in the mid- to late-30s, bone loss slowly begins.
29 Pathophysiology of osteoporosis The cumulative effect over time can translate into age-related osteoporosis that affects both cortical and trabecular bone & leads to vertebral, hip, & wrist fractures. Secondary osteoporosis is caused by either diseases or medications & afflicts both bone types. Secondary causes can be found in 11-31% of women & 30-54% of men.
30 Postmenaposal The rate of bone loss commonly accelerates at menopause due to a decline in trophic sex hormone production, especially when a bone healthy lifestyle is not practiced. In older studies, approximately 10-25% of bone loss was documented in the decade after menopause. Bone loss then slows to 8-12% per decade, a rate that was similar to that of older men. This accelerated loss has not been demonstrated in most of the placebo groups who were taking calcium and vitamin D supplements in recently conducted randomized controlled trials.
31 Postmenaposal Estrogen deficiency increases bone resorption more than formation. This process appears to depend on tumor necrosis factor (TNF), interleukin-1 (IL-1), interleukin-11, interleukin-6, MCSF, and prostaglandin E2, which stimulate osteoclastic activity through the OPG/RANK/RANKL system.
32 Postmenaposal Reduced TGF-β, associated with estrogen loss, enhances osteoclast action through decreased apoptosis. Osteocytes also may play a role. Normally, with more weight bearing, osteocytes trigger increased BMD. With menopause, osteocyte apoptosis blunts this response.
33 Age-related Bone resorption increases with age, but changes in bone formation are not observed consistently. Increased osteocyte apoptosis may decrease responses to mechanical strain & hinder bone repair. Cortical porosity from years of remodeling & decreased trabecular connectivity, particularly of horizontal struts, promotes microarchitectural deterioration of bone that is not always reflected in BMD. Aging also increases fracture risk in other ways that are independent of BMD.
34 Age-related Comorbid conditions, cognitive impairment, medications, & deconditioning can increase falls. Inadequate calcium, vitamin D, & nutritional intake also contribute to bone loss & fractures. Vitamin D insufficiency results from poor sun exposure, decreased cutaneous production, insufficient dietary intake, & decreased absorption. Calcium & vitamin D insufficiency promotes secondary hyperparathyroidism & associated bone loss.
35
36 Men For many reasons, men experience fewer osteoporosis-related fractures than women. Men comprise only approximately 20% of all persons with osteoporosis. This is likely attributable to men attaining a 20-40% higher peak BMD than women & losing BMD at a slower rate after the peak. Men s bones also have a mechanical advantage because the larger bone diameter makes them more fracture resistant.
37 Men Finally, men have a shorter life expectancy and experience fewer falls than women. Male osteoporosis remains an under recognized problem. Although fewer men than women have osteoporosis, men still suffer up to 30% of all hip fractures and are more likely than women to die within 1 year after fracture.
38 Men Hypogonadism, secondary to age-related decreased testosterone and increased sex hormone binding globulin (SHBG), endocrine dysfunction, or androgen ablation, can also cause bone loss. Estrogen, synthesized from testosterone by the enzyme aromatase, appears more important than testosterone in men for bone maintenance, with greater bone density seen in men with higher estradiol concentrations. Secondary causes often contribute to male osteoporosis.
39 Secondary causes Numerous diseases and drugs can decrease bone mass. Secondary causes are suspected when osteoporosis occurs in premenopausal women, men younger than age 70, those with no risk factors, multiple low trauma fractures (especially at a young age), or bone loss despite adequate drug treatment & calcium supplementation. Patients suspected of having secondary causes should undergo careful evaluation that includes a comprehensive physical exam and laboratory assessment. Both the osteoporosis & contributing disorders should be treated.
40 Drug induced Unfortunately, several medications can cause bone loss by a variety of mechanisms. Examples include systemic glucocorticoids, thyroid hormone replacement, some antiepileptic drugs, and heparin use. Thyroid dose adjustment is needed to keep the thyroid-stimulating hormone (TSH) in the upper half of the normal range to minimize bone loss. Some anticonvulsants, like phenobarbital & phenytoin, hasten vitamin D metabolism & the resultant effects can lead to osteomalacia.
41 Drug induced Those at higher risk include people who take multiple anticonvulsants, are institutionalized, or have multiple comorbidities. Heparin therapy, in excess of 15,000 to 30,000 units daily for greater than 3 to 6 months, is associated with bone loss and vertebral fractures. Low-molecular-weight heparins such as enoxaparin may pose less risk of bone loss.
42 Drug induced A black-box warning has been added to the product labeling of medroxyprogesterone acetate injectable contraceptive warning that it significantly decreases bone loss that increases with longer durations of therapy. Thus, this contraceptive product should be used only when other medications prove inadequate.
43 Clinical presentation
44
45 Osteomalycia
46 Introduction Osteomalacia results from defective osteoid mineralization. Defective mineralization in the infant or child produces rickets. In the adult, the syndrome is called osteomalacia.
47 Epidemiology The incidence of osteomalacia is not known precisely, but is lower in the United States because foods are supplemented with vitamin D. Osteomalacia is more prevalent in countries with little sun exposure, minimal dietary supplementation, malnutrition, or traditional clothing covering most of the skin. Dark-skinned individuals synthesize less vitamin D cutaneously & can be at risk for hypovitaminosis D.
48 Pathophysiology Mechanisms leading to osteomalacia include low serum calcium or phosphorus, chronic acidosis, hypophosphatemia, liver or renal disease, and drug-induced mineralization defects.
49 Pathophysiology most common cause is vitamin D deficiency secondary to inadequate intake, decreased sun exposure, malabsorption, or decreased metabolism. Renal disease is associated with decreased 25(OH) vitamin D 1α-hydroxylase, with consequently decreased calcitriol and poor calcium absorption. In vitamin D dependent rickets type I, a genetic defect exists in 25(OH) vitamin D 1α-hydroxylase. Vitamin D dependent rickets type II results from defects in the vitamin D receptor or its activity.
50 Pathophysiology In vitamin D resistant rickets, renal phosphate reabsorption is defective, & 25(OH) vitamin D 1αhydroxylase activity is inadequate. A genetic defect in the PHEX gene may allow inappropriate activity of an undefined inhibitor of phosphate reabsorption that also lowers serum calcitriol concentrations. Pancreatitis, chronic hepatobiliary disease, Crohn s disease, gastrectomy are also risk factors for vitamin D deficiency
51 Pathophysiology Other chronic disorders cause osteomalacia. Phosphate depletion from low dietary intake, phosphate-binding antacids, and oncogenic osteomalacia can cause osteomalacia. Hypophosphatasia is an inborn error of metabolism in which deficient activity of alkaline phosphatase causes impaired mineralization of bone matrix. Acidosis from renal dysfunction, distal renal tubular acidosis, hypergammaglobulinemic states (e.g., multiple myeloma), and drugs (e.g., chemotherapy) compromises bone mineralization.
52 Pathophysiology Renal tubular disorders secondary to Fanconi s syndrome, hereditary diseases (e.g., Wilson s disease, a defect in copper metabolism), acquired disease (e.g., myeloma), and toxins (e.g., lead) cause osteomalacia to varying degrees. Chronic wastage of phosphorus &/or calcium limits mineralization, which may be further compromised by acidosis & secondary hyperparathyroidism.
53 Drug induced Drugs induce osteomalacia through various mechanisms. Phenytoin, primidone, phenobarbital, carbamazepine, rifampin, and some hypnotic medications may cause osteomalacia, potentially through hepatic microsomal cytochrome P450 induction and increased vitamin D metabolism. Anticonvulsant-associated osteomalacia usually occurs only in patients living in an institution or those receiving multiple anticonvulsant drugs. Cholestyramine may decrease vitamin D absorption.
54 Drug induced Defective mineralization can result from continuous or intermittent etidronate treatment or sodium fluoride. Aluminum accumulation in patients with severe renal impairment or in patients undergoing hemodialysis may lead to osteomalacia, potentially through insoluble complexes with phosphates and inhibition of mineral deposition.
55 Clinical presentation Adult osteomalacia often has an insidious presentation. Diffuse skeletal pain, bony tenderness, and proximal muscle weakness may occur. Pain on movement and muscle weakness may result in a characteristic waddling gait. Hypophosphatemia and secondary hyperparathyroidism may contribute to these symptoms. Tetany can result from sufficiently depressed serum ionized calcium. Skeletal deformities (infrequent in adults) include leg bowing, pigeon chest, scoliosis, kyphosis, and shortening of the spine.
56 HW 4 Summaries the pathophysiology of osteomalacia in one page.
The Skeletal Response to Aging: There s No Bones About It!
 The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
Pathophysiology of Postmenopausal & Glucocorticoid Induced Osteoporosis. March 15, 2016 Bone ECHO Kate T Queen, MD
 Pathophysiology of Postmenopausal & Glucocorticoid Induced Osteoporosis March 15, 2016 Bone ECHO Kate T Queen, MD Review: normal bone formation Bone Modeling Remodeling Peak Bone Mass Maximum bone mass
Pathophysiology of Postmenopausal & Glucocorticoid Induced Osteoporosis March 15, 2016 Bone ECHO Kate T Queen, MD Review: normal bone formation Bone Modeling Remodeling Peak Bone Mass Maximum bone mass
Osteoporosis. When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of.
 Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Osteoporosis When we talk about osteoporosis, we have to be familiar with the constituents of bone and what it is formed of. Osteoblasts by definition are those cells present in the bone and are involved
Endocrine Regulation of Calcium and Phosphate Metabolism
 Endocrine Regulation of Calcium and Phosphate Metabolism Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C516, Block C, Research Building, School of Medicine Tel: 88208252 Email: wanghuiping@zju.edu.cn
Endocrine Regulation of Calcium and Phosphate Metabolism Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C516, Block C, Research Building, School of Medicine Tel: 88208252 Email: wanghuiping@zju.edu.cn
Functions of the Skeletal System. Chapter 6: Osseous Tissue and Bone Structure. Classification of Bones. Bone Shapes
 Chapter 6: Osseous Tissue and Bone Structure Functions of the Skeletal System 1. Support 2. Storage of minerals (calcium) 3. Storage of lipids (yellow marrow) 4. Blood cell production (red marrow) 5. Protection
Chapter 6: Osseous Tissue and Bone Structure Functions of the Skeletal System 1. Support 2. Storage of minerals (calcium) 3. Storage of lipids (yellow marrow) 4. Blood cell production (red marrow) 5. Protection
Deposition of Bone by the Osteoblasts. Bone is continually being deposited by osteoblasts, and it is continually being resorbed where osteoclasts are
 Bone remodeling Deposition of Bone by the Osteoblasts. Bone is continually being deposited by osteoblasts, and it is continually being resorbed where osteoclasts are active. This mechanism is always is
Bone remodeling Deposition of Bone by the Osteoblasts. Bone is continually being deposited by osteoblasts, and it is continually being resorbed where osteoclasts are active. This mechanism is always is
Sachin Soni DNB Pediatrics
 Sachin Soni DNB Pediatrics Vitamin D physiology Introduction Etiology Clinical feature Radiology Diagnosis Lab Treatment Source: -Fish, liver and oil, - Human milk (30-40 IU/L) - Exposure to sun light
Sachin Soni DNB Pediatrics Vitamin D physiology Introduction Etiology Clinical feature Radiology Diagnosis Lab Treatment Source: -Fish, liver and oil, - Human milk (30-40 IU/L) - Exposure to sun light
BONE REMODELLING. Tim Arnett. University College London. Department of Anatomy and Developmental Biology
 BONE REMODELLING Tim Arnett Department of Anatomy and Developmental Biology University College London The skeleton, out of sight and often out of mind, is a formidable mass of tissue occupying about 9%
BONE REMODELLING Tim Arnett Department of Anatomy and Developmental Biology University College London The skeleton, out of sight and often out of mind, is a formidable mass of tissue occupying about 9%
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Bone Remodeling & Repair Pathologies
 Bone Remodeling & Repair Pathologies Skeletal system remodels itself to maintain homeostasis Remodeling Maintainence replaces mineral reserves (osteocytes) of the matrix Remodelling recycles (osteoclasts)
Bone Remodeling & Repair Pathologies Skeletal system remodels itself to maintain homeostasis Remodeling Maintainence replaces mineral reserves (osteocytes) of the matrix Remodelling recycles (osteoclasts)
Rama Nada. - Mousa Al-Abbadi. 1 P a g e
 - 1 - Rama Nada - - Mousa Al-Abbadi 1 P a g e Bones, Joints and Soft tissue tumors Before we start: the first 8 minutes was recalling to Dr.Mousa s duties, go over them in the slides. Wherever you see
- 1 - Rama Nada - - Mousa Al-Abbadi 1 P a g e Bones, Joints and Soft tissue tumors Before we start: the first 8 minutes was recalling to Dr.Mousa s duties, go over them in the slides. Wherever you see
Vitamin D: Is it a superhero??
 Vitamin D: Is it a superhero?? Dr. Ashraf Abdel Basset Bakr Prof. of Pediatrics 1 2 History of vitamin D discovery Sources of vitamin D and its metabolism 13 Actions of vitamin D 4 Vitamin D deficiency
Vitamin D: Is it a superhero?? Dr. Ashraf Abdel Basset Bakr Prof. of Pediatrics 1 2 History of vitamin D discovery Sources of vitamin D and its metabolism 13 Actions of vitamin D 4 Vitamin D deficiency
An Introduction to the Skeletal System Skeletal system includes Bones of the skeleton Cartilages, ligaments, and connective tissues
 An Introduction to the Skeletal System Skeletal system includes Bones of the skeleton Cartilages, ligaments, and connective tissues Functions of the Skeletal System Support Storage of minerals (calcium)
An Introduction to the Skeletal System Skeletal system includes Bones of the skeleton Cartilages, ligaments, and connective tissues Functions of the Skeletal System Support Storage of minerals (calcium)
Chapter 39: Exercise prescription in those with osteoporosis
 Chapter 39: Exercise prescription in those with osteoporosis American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Chapter 39: Exercise prescription in those with osteoporosis American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York:
Drugs Affecting Bone. Rosa McCarty PhD. Department of Pharmacology & Therapeutics
 Drugs Affecting Bone Rosa McCarty PhD Department of Pharmacology & Therapeutics rmccarty@unimelb.edu.au Objectives At the end of this lecture you should have gained: An understanding of bone metabolism
Drugs Affecting Bone Rosa McCarty PhD Department of Pharmacology & Therapeutics rmccarty@unimelb.edu.au Objectives At the end of this lecture you should have gained: An understanding of bone metabolism
PARATHYROID, VITAMIN D AND BONE
 PARATHYROID, VITAMIN D AND BONE G M Kellerman Pathology North Hunter Service 30/01/2015 BIOLOGY OF BONE Bone consists of protein, polysaccharide components and mineral matrix. The mineral is hydroxylapatite,
PARATHYROID, VITAMIN D AND BONE G M Kellerman Pathology North Hunter Service 30/01/2015 BIOLOGY OF BONE Bone consists of protein, polysaccharide components and mineral matrix. The mineral is hydroxylapatite,
Helpful information about bone health & osteoporosis Patient Resource
 Helpful information about bone health & osteoporosis Patient Resource Every year In the United States, 2.5 million fractures occur due to osteoporosis. Out of these, 330,000 are hip fractures, and half
Helpful information about bone health & osteoporosis Patient Resource Every year In the United States, 2.5 million fractures occur due to osteoporosis. Out of these, 330,000 are hip fractures, and half
BIOLOGY and BIOMECHANICS OF NORMAL & OSTEOPOROTIC BONE
 BIOLOGY and BIOMECHANICS OF NORMAL & OSTEOPOROTIC BONE Andreas Panagopoulos, MD, PhD Assistant Professor in Orthopaedics University Hospital of Patras, Orthopaedic Clinic Objectives Bone structure and
BIOLOGY and BIOMECHANICS OF NORMAL & OSTEOPOROTIC BONE Andreas Panagopoulos, MD, PhD Assistant Professor in Orthopaedics University Hospital of Patras, Orthopaedic Clinic Objectives Bone structure and
Pediatric metabolic bone diseases
 Pediatric metabolic bone diseases Classification and overview of clinical and radiological findings M. Mearadji International Foundation for Pediatric Imaging Aid www.ifpia.com Introduction Metabolic bone
Pediatric metabolic bone diseases Classification and overview of clinical and radiological findings M. Mearadji International Foundation for Pediatric Imaging Aid www.ifpia.com Introduction Metabolic bone
DISEASES WITH ABNORMAL MATRIX
 DISEASES WITH ABNORMAL MATRIX MSK-1 FOR 2 ND YEAR MEDICAL STUDENTS Dr. Nisreen Abu Shahin CONGENITAL DISEASES WITH ABNORMAL MATRIX OSTEOGENESIS IMPERFECTA (OI): also known as "brittle bone disease" a group
DISEASES WITH ABNORMAL MATRIX MSK-1 FOR 2 ND YEAR MEDICAL STUDENTS Dr. Nisreen Abu Shahin CONGENITAL DISEASES WITH ABNORMAL MATRIX OSTEOGENESIS IMPERFECTA (OI): also known as "brittle bone disease" a group
Regulation of the skeletal mass through the life span
 Regulation of the skeletal mass through the life span Functions of the skeletal system Mechanical protection skull Movement leverage for muscles Mineral metabolism calcium store Erythropoiesis red blood
Regulation of the skeletal mass through the life span Functions of the skeletal system Mechanical protection skull Movement leverage for muscles Mineral metabolism calcium store Erythropoiesis red blood
OSTEOMALACIA UPDATE. Nothing to Disclose. Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco
 OSTEOMALACIA UPDATE Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco Nothing to Disclose 1 Case History 59 YO WM referred for evaluation of diffuse
OSTEOMALACIA UPDATE Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco Nothing to Disclose 1 Case History 59 YO WM referred for evaluation of diffuse
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Osteoporosis. Open Access. John A. Kanis. Diseases, University of Sheffield, UK
 Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
HAART HIV & BONE METABOLISM HAART EDITORIAL. Bologna, April 5 th, 2013
 HIV correlated pathologies and other infections HIV & BONE METABOLISM Bologna, April 5 th, 2013 Morning Session: Davide Gibellini, Fabio Vescini, Paolo Bonfanti, Stefano Mora, Antonio Di Biagio, Tiziana
HIV correlated pathologies and other infections HIV & BONE METABOLISM Bologna, April 5 th, 2013 Morning Session: Davide Gibellini, Fabio Vescini, Paolo Bonfanti, Stefano Mora, Antonio Di Biagio, Tiziana
TREATMENT OF OSTEOPOROSIS
 TREATMENT OF OSTEOPOROSIS Summary Prevention is the key issue in the management of osteoporosis. HRT is the agent of choice for prevention of postmenopausal osteoporosis. Bisphosphonates and Calcitonin
TREATMENT OF OSTEOPOROSIS Summary Prevention is the key issue in the management of osteoporosis. HRT is the agent of choice for prevention of postmenopausal osteoporosis. Bisphosphonates and Calcitonin
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
The Role of the Laboratory in Metabolic Bone Disease
 The Role of the Laboratory in Metabolic Bone Disease Howard Morris PhD, FAACB, FFSc(RCPA) President, IFCC Professor of Medical Sciences, University of South Australia, Clinical Scientist, SA Pathology
The Role of the Laboratory in Metabolic Bone Disease Howard Morris PhD, FAACB, FFSc(RCPA) President, IFCC Professor of Medical Sciences, University of South Australia, Clinical Scientist, SA Pathology
Trebeculae. Step 4. compact bone. Diploë Pearson Education, Inc.
 Trebeculae compact bone Step 4 Diploë Abnormalities in bone growth Fibrodysplasia ossificans progressiva (FOP) autosomal dominant, Codon 206: Arg à Hist 1 : 2, 000, 000 endothelial cells à mesenchymal
Trebeculae compact bone Step 4 Diploë Abnormalities in bone growth Fibrodysplasia ossificans progressiva (FOP) autosomal dominant, Codon 206: Arg à Hist 1 : 2, 000, 000 endothelial cells à mesenchymal
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Nutritional Aspects of Osteoporosis Care and Treatment Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, Ohio
 Osteoporosis 1 Nutritional Aspects of Osteoporosis Care and Treatment Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, Ohio 1) Objectives: a) To understand bone growth and development
Osteoporosis 1 Nutritional Aspects of Osteoporosis Care and Treatment Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, Ohio 1) Objectives: a) To understand bone growth and development
BONE HEALTH Dr. Tia Lillie. Exercise, Physical Activity and Osteoporosis
 BONE HEALTH Dr. Tia Lillie Exercise, Physical Activity and Osteoporosis Food for thought... How old would you be if you didn t know how old you were? DEFINITION: Osteoporosis Osteoporosis (OP) is a disease
BONE HEALTH Dr. Tia Lillie Exercise, Physical Activity and Osteoporosis Food for thought... How old would you be if you didn t know how old you were? DEFINITION: Osteoporosis Osteoporosis (OP) is a disease
Index. B BMC. See Bone mineral content BMD. See Bone mineral density Bone anabolic impact, Bone mass acquisition
 A Acid base balance dietary protein detrimental effects of, 19 Acid base balance bicarbonate effects, 176 in bone human studies, 174 mechanisms, 173 174 in muscle aging, 174 175 alkali supplementation
A Acid base balance dietary protein detrimental effects of, 19 Acid base balance bicarbonate effects, 176 in bone human studies, 174 mechanisms, 173 174 in muscle aging, 174 175 alkali supplementation
Osseous Tissue and Bone Structure
 C h a p t e r 6 Osseous Tissue and Bone Structure PowerPoint Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Copyright 2009 Pearson Education, Inc., publishing as Pearson Benjamin
C h a p t e r 6 Osseous Tissue and Bone Structure PowerPoint Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Copyright 2009 Pearson Education, Inc., publishing as Pearson Benjamin
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
CHAPTER 6 LECTURE OUTLINE
 CHAPTER 6 LECTURE OUTLINE I. INTRODUCTION A. Bone is made up of several different tissues working together: bone, cartilage, dense connective tissue, epithelium, various blood forming tissues, adipose
CHAPTER 6 LECTURE OUTLINE I. INTRODUCTION A. Bone is made up of several different tissues working together: bone, cartilage, dense connective tissue, epithelium, various blood forming tissues, adipose
Elecsys bone marker panel. Optimal patient management starts in the laboratory
 bone marker panel Optimal patient management starts in the laboratory Complete solution for osteoporosis The most complete bone metabolism panel on a single platform bone marker assays are important diagnostic
bone marker panel Optimal patient management starts in the laboratory Complete solution for osteoporosis The most complete bone metabolism panel on a single platform bone marker assays are important diagnostic
OMICS Journals are welcoming Submissions
 OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible
OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible
Osteoporosis in Men Wendy Rosenthal PharmD. This program has been brought to you by PharmCon
 Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Chapter 6: Osseous Tissue and Bone Structure
 Chapter 6: Osseous Tissue and Bone Structure I. An Introduction to the Skeletal System, p. 180 Objective: Describe the functions of the skeletal system The skeletal system includes: - bones of the skeleton
Chapter 6: Osseous Tissue and Bone Structure I. An Introduction to the Skeletal System, p. 180 Objective: Describe the functions of the skeletal system The skeletal system includes: - bones of the skeleton
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
The Skeletal System:Bone Tissue
 The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
Chapter 6: SKELETAL SYSTEM
 Chapter 6: SKELETAL SYSTEM I. FUNCTIONS A. Support B. Protection C. Movement D. Mineral storage E. Lipid storage (Fig. 6.8b) F. Blood cell production (Fig. 6.4) II. COMPONENTS A. Cartilage 1. Hyaline 2.
Chapter 6: SKELETAL SYSTEM I. FUNCTIONS A. Support B. Protection C. Movement D. Mineral storage E. Lipid storage (Fig. 6.8b) F. Blood cell production (Fig. 6.4) II. COMPONENTS A. Cartilage 1. Hyaline 2.
SKELETAL SYSTEM I NOTE: LAB ASSIGNMENTS for this topic will run over 3 Weeks. A SEPARATE WORKSHEET WILL BE PROVIDED.
 BIO 211; Anatomy and Physiology I REFERENCE: CHAPTER 07 1 Dr. Lawrence Altman Naugatuck Valley Community College LECTURE TOPICS OUTLINE SKELETAL SYSTEM I NOTE: LAB ASSIGNMENTS for this topic will run over
BIO 211; Anatomy and Physiology I REFERENCE: CHAPTER 07 1 Dr. Lawrence Altman Naugatuck Valley Community College LECTURE TOPICS OUTLINE SKELETAL SYSTEM I NOTE: LAB ASSIGNMENTS for this topic will run over
Disclosure and Conflicts of Interest Steven T Harris MD Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis
 Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis Steven T Harris MD FACP Clinical Professor of Medicine University of California, San Francisco Disclosure and Conflicts of Interest
Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis Steven T Harris MD FACP Clinical Professor of Medicine University of California, San Francisco Disclosure and Conflicts of Interest
Vitamin D. Vitamin functioning as hormone. Todd A Fearer, MD FACP
 Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS
 OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS The Skeletal System Skeletal system includes: bones of the skeleton, cartilages, ligaments, and connective tissues What are the functions of
OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS The Skeletal System Skeletal system includes: bones of the skeleton, cartilages, ligaments, and connective tissues What are the functions of
Skeletal System. The skeletal System... Components
 Skeletal System The skeletal System... What are the general components of the skeletal system? What does the skeletal system do for you & how does it achieve these functions? Components The skeletal system
Skeletal System The skeletal System... What are the general components of the skeletal system? What does the skeletal system do for you & how does it achieve these functions? Components The skeletal system
Biochemistry. Vitamin D, Rickets and Osteoporosis. Editing file. One day you ll be person between the patient and his grief. Please study well..
 HbA NH2 H2 O2 Cl2O7 KClO3 CH2O PO4 NAOH KMnO4 MEDICINE COOH KING SAUD UNIVERSITY Co2 MgCl2 H 2O SO2 Doctors slides Important Extra Information Doctors notes Biochemistry Vitamin D, Rickets and Osteoporosis
HbA NH2 H2 O2 Cl2O7 KClO3 CH2O PO4 NAOH KMnO4 MEDICINE COOH KING SAUD UNIVERSITY Co2 MgCl2 H 2O SO2 Doctors slides Important Extra Information Doctors notes Biochemistry Vitamin D, Rickets and Osteoporosis
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
To understand bone growth and development across the lifespan. To develop a better understanding of osteoporosis.
 Nutrition Aspects of Osteoporosis Care and Treatment t Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, OH. Objectives To understand bone growth and development across the lifespan.
Nutrition Aspects of Osteoporosis Care and Treatment t Cynthia Smith, FNP-BC, RN, MSN, CCD Pars Osteoporosis Clinic, Belpre, OH. Objectives To understand bone growth and development across the lifespan.
Normal Bone Health and Bone Disease. Mr Ryan Trickett Consultant Hand and Wrist Surgeon 6 th February 2017
 Normal Bone Health and Bone Disease Mr Ryan Trickett Consultant Hand and Wrist Surgeon 6 th February 2017 Learning outcomes Understand the structure and function of bone and articular cartilage Explain
Normal Bone Health and Bone Disease Mr Ryan Trickett Consultant Hand and Wrist Surgeon 6 th February 2017 Learning outcomes Understand the structure and function of bone and articular cartilage Explain
The Skeletal System:Bone Tissue
 The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
BMD: A Continuum of Risk WHO Bone Density Criteria
 Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Outline. Skeletal System. Functions of Bone. Bio 105: Skeletal System 3/17/2016. The material from this lecture packet will be on the lecture exam
 Bio 105: Skeletal System Lecture 8 Chapter 5 The material from this lecture packet will be on the lecture exam The identification that you do after this lecture will be on the lab exam Outline I. Overview
Bio 105: Skeletal System Lecture 8 Chapter 5 The material from this lecture packet will be on the lecture exam The identification that you do after this lecture will be on the lab exam Outline I. Overview
Vitamin D Hormone Du Jour
 Vitamin D Hormone Du Jour J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Why Is Vitamin D Important? Musculo-skeletal effects Possible other effects Immunomodulatory
Vitamin D Hormone Du Jour J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Why Is Vitamin D Important? Musculo-skeletal effects Possible other effects Immunomodulatory
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Osteoporosis - Pathophysiology and diagnosis. Bente L Langdahl Department of Endocrinology Aarhus University Hospital Aarhus, Denmark
 Osteoporosis - Pathophysiology and diagnosis Bente L Langdahl Department of Endocrinology Aarhus University Hospital Aarhus, Denmark Objective General knowledge about osteoporosis Optimise your protocols
Osteoporosis - Pathophysiology and diagnosis Bente L Langdahl Department of Endocrinology Aarhus University Hospital Aarhus, Denmark Objective General knowledge about osteoporosis Optimise your protocols
Biochemistry #01 Bone Formation Dr. Nabil Bashir Farah Banyhany
 Biochemistry #01 Bone Formation Dr. Nabil Bashir Farah Banyhany Greetings This lecture is quite detailed, but I promise you will make it through, it just requires your 100% FOCUS! Let s begin. Today s
Biochemistry #01 Bone Formation Dr. Nabil Bashir Farah Banyhany Greetings This lecture is quite detailed, but I promise you will make it through, it just requires your 100% FOCUS! Let s begin. Today s
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Fig Articular cartilage. Epiphysis. Red bone marrow Epiphyseal line. Marrow cavity. Yellow bone marrow. Periosteum. Nutrient foramen Diaphysis
 Fig. 7.1 Articular cartilage Epiphysis Red bone marrow Epiphyseal line Marrow cavity Yellow bone marrow Nutrient foramen Diaphysis Site of endosteum Compact bone Spongy bone Epiphyseal line Epiphysis Articular
Fig. 7.1 Articular cartilage Epiphysis Red bone marrow Epiphyseal line Marrow cavity Yellow bone marrow Nutrient foramen Diaphysis Site of endosteum Compact bone Spongy bone Epiphyseal line Epiphysis Articular
Prevention And Treatment. References. Vertebral Fracture Management KEY POINTS
 OSTEOPOROSISLoren M. Wilkerson, MD; Kenneth W. Lyles, MD, AGSF Key Points Epidemiology And Impact Bone Remodeling And Bone Loss.. Pathogenesis Diagnosis And Prediction Of Fr.. Prevention And Treatment
OSTEOPOROSISLoren M. Wilkerson, MD; Kenneth W. Lyles, MD, AGSF Key Points Epidemiology And Impact Bone Remodeling And Bone Loss.. Pathogenesis Diagnosis And Prediction Of Fr.. Prevention And Treatment
Welcome to mmlearn.org
 Welcome to mmlearn.org VITAMIN D SUNSHINE VITAMIN INTRODUCTION Familiar with skeletal needs Rickets Osteoporosis Fractures INTRODUCTION Not as familiar other associations Immune system Cancer Cardiovascular
Welcome to mmlearn.org VITAMIN D SUNSHINE VITAMIN INTRODUCTION Familiar with skeletal needs Rickets Osteoporosis Fractures INTRODUCTION Not as familiar other associations Immune system Cancer Cardiovascular
Outline. Estrogens and SERMS The forgotten few! How Does Estrogen Work in Bone? Its Complex!!! 6/14/2013
 Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
The Parathyroid Glands
 The Parathyroid Glands Bởi: OpenStaxCollege The parathyroid glands are tiny, round structures usually found embedded in the posterior surface of the thyroid gland ([link]). A thick connective tissue capsule
The Parathyroid Glands Bởi: OpenStaxCollege The parathyroid glands are tiny, round structures usually found embedded in the posterior surface of the thyroid gland ([link]). A thick connective tissue capsule
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
SKELETAL SYSTEM CHAPTER 07. Bone Function BIO 211: ANATOMY & PHYSIOLOGY I. Body Movement interacts with muscles bones act as rigid bar of a lever
 Page 1 BIO 211: ANATOMY & PHYSIOLOGY I 1 CHAPTER 07 SKELETAL SYSTEM Dr. Lawrence G. G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. Some illustrations are courtesy of
Page 1 BIO 211: ANATOMY & PHYSIOLOGY I 1 CHAPTER 07 SKELETAL SYSTEM Dr. Lawrence G. G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. Some illustrations are courtesy of
SKELETAL SYSTEM CHAPTER 07 BIO 211: ANATOMY & PHYSIOLOGY I
 BIO 211: ANATOMY & PHYSIOLOGY I 1 CHAPTER 07 SKELETAL SYSTEM Dr. Lawrence G. G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. Some illustrations are courtesy of McGraw-Hill.
BIO 211: ANATOMY & PHYSIOLOGY I 1 CHAPTER 07 SKELETAL SYSTEM Dr. Lawrence G. G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. Some illustrations are courtesy of McGraw-Hill.
Chapter 6: Skeletal System: Bones and Bone Tissue
 Chapter 6: Skeletal System: Bones and Bone Tissue I. Functions A. List and describe the five major functions of the skeletal system: 1. 2. 3.. 4. 5.. II. Cartilage A. What do chondroblasts do? B. When
Chapter 6: Skeletal System: Bones and Bone Tissue I. Functions A. List and describe the five major functions of the skeletal system: 1. 2. 3.. 4. 5.. II. Cartilage A. What do chondroblasts do? B. When
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
بسم هللا الرحمن الرحيم. Rickets
 بسم هللا الرحمن الرحيم Rickets 1 Rickets IS defined as failure of mineralization of growing bone or osteoid tissue due to vitamin D deficiency. Vitamin D appear as rickets in children and as oteomalacia
بسم هللا الرحمن الرحيم Rickets 1 Rickets IS defined as failure of mineralization of growing bone or osteoid tissue due to vitamin D deficiency. Vitamin D appear as rickets in children and as oteomalacia
Osteoporosis: Risk Factors, Diagnostic Methods And Treatment Options
 ISPUB.COM The Internet Journal of Academic Physician Assistants Volume 1 Number 1 Osteoporosis: Risk Factors, Diagnostic Methods And Treatment Options K Ihrke Citation K Ihrke.. The Internet Journal of
ISPUB.COM The Internet Journal of Academic Physician Assistants Volume 1 Number 1 Osteoporosis: Risk Factors, Diagnostic Methods And Treatment Options K Ihrke Citation K Ihrke.. The Internet Journal of
CIC EDIZIONI INTERNAZIONALI. Bone fragility: current reviews and clinical features. Mini review
 Mini review Paolo Tranquilli Leali, MD, FBSE Carlo Doria, MD, PhD Alexandros Zachos, MD Adriano Ruggiu, MD Fabio Milia, MD Francesca Barca, MD Orthopaedic Department, University of Sassari, Sassari, Italy
Mini review Paolo Tranquilli Leali, MD, FBSE Carlo Doria, MD, PhD Alexandros Zachos, MD Adriano Ruggiu, MD Fabio Milia, MD Francesca Barca, MD Orthopaedic Department, University of Sassari, Sassari, Italy
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
454 Secondary Causes of Osteoporosis Mayo Clin Proc, May 2002, Vol 77 Table 1. Secondary Causes of Osteoporosis Endocrine disorders Acromegaly Adrenal
 Mayo Clin Proc, May 2002, Vol 77 Secondary Causes of Osteoporosis 453 Review Secondary Causes of Osteoporosis LORRAINE A. FITZPATRICK, MD Secondary causes of bone loss are not often considered in patients
Mayo Clin Proc, May 2002, Vol 77 Secondary Causes of Osteoporosis 453 Review Secondary Causes of Osteoporosis LORRAINE A. FITZPATRICK, MD Secondary causes of bone loss are not often considered in patients
BIOH111. o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system
 BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 TEXTBOOK AND REQUIRED/RECOMMENDED
Vitamin D & Cardiovascular Disease
 Vitamin D & Cardiovascular Disease Disclosures None Vitamin D Objectives: Discuss the basics of vitamin D metabolism Discuss the role of vitamin D deficiency in the development of coronary disease Review
Vitamin D & Cardiovascular Disease Disclosures None Vitamin D Objectives: Discuss the basics of vitamin D metabolism Discuss the role of vitamin D deficiency in the development of coronary disease Review
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
For more information about how to cite these materials visit
 Author(s): University of Michigan Medical School, Department of Cell and Developmental Biology License: Unless otherwise noted, the content of this course material is licensed under a Creative Commons
Author(s): University of Michigan Medical School, Department of Cell and Developmental Biology License: Unless otherwise noted, the content of this course material is licensed under a Creative Commons
Because the low bone mass and deterioration
 OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Dr Seeta Durvasula.
 Dr Seeta Durvasula seeta.durvasula@sydney.edu.au 1 Avoid sun skin cancer risk Australia has highest rates of skin cancer in the world Epidemic of Vitamin D deficiency Lack of Vitamin D increases risk of
Dr Seeta Durvasula seeta.durvasula@sydney.edu.au 1 Avoid sun skin cancer risk Australia has highest rates of skin cancer in the world Epidemic of Vitamin D deficiency Lack of Vitamin D increases risk of
Effects of Anti RANK ligand Denosumab on Beta Thalassemia induced osteoporosis
 Effects of Anti RANK ligand Denosumab on Beta Thalassemia induced osteoporosis Mohamed Yassin 1 Ashraf T. Soliman2, Mohamed O. Abdelrahman3, Vincenzo De Sanctis 4 Departments of, 1 Hematology 2Pediatric
Effects of Anti RANK ligand Denosumab on Beta Thalassemia induced osteoporosis Mohamed Yassin 1 Ashraf T. Soliman2, Mohamed O. Abdelrahman3, Vincenzo De Sanctis 4 Departments of, 1 Hematology 2Pediatric
IEHP UM Subcommittee Approved Authorization Guidelines DEXA Scan
 Policy: IEHP UM Subcommittee Approved Authorization Guidelines IEHP considers bone mineral density testing using DEXA medically necessary for members who meet any of the following criteria: Women aged
Policy: IEHP UM Subcommittee Approved Authorization Guidelines IEHP considers bone mineral density testing using DEXA medically necessary for members who meet any of the following criteria: Women aged
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A A Diabetes Outcome Progression Trial (ADOPT), 194 Adaptive immunity, 129 131 ADOPT (A Diabetes Outcome Progression Trial), 194 Aging, vitamin
Note: Page numbers of article titles are in boldface type. A A Diabetes Outcome Progression Trial (ADOPT), 194 Adaptive immunity, 129 131 ADOPT (A Diabetes Outcome Progression Trial), 194 Aging, vitamin
From Fragile to Firm. Monika Starosta MD. Advocate Medical Group
 From Fragile to Firm Monika Starosta MD Advocate Medical Group Bone Remodeling 10% remodeled each year Calcium homoeostasis Maintain Mechanical strength Replace Osteocytes Release Growth Factors Bone remodeling
From Fragile to Firm Monika Starosta MD Advocate Medical Group Bone Remodeling 10% remodeled each year Calcium homoeostasis Maintain Mechanical strength Replace Osteocytes Release Growth Factors Bone remodeling
Additional Research is Needed to Determine the Effects of Soy Protein on Calcium Binding and Absorption NDFS 435 3/26/2015. Dr.
 Additional Research is Needed to Determine the Effects of Soy Protein on Calcium Binding and Absorption NDFS 435 3/26/2015 Dr. Tessem Osteoporosis is a public health problem in all stages of life. Many
Additional Research is Needed to Determine the Effects of Soy Protein on Calcium Binding and Absorption NDFS 435 3/26/2015 Dr. Tessem Osteoporosis is a public health problem in all stages of life. Many
Bone Health in the Cancer Patient. Stavroula Otis, M.D. Primary Care and Oncology: Practical Lessons Conference Brea Community Center May 10, 2018
 Bone Health in the Cancer Patient Stavroula Otis, M.D. Primary Care and Oncology: Practical Lessons Conference Brea Community Center May 10, 2018 Overview Healthy bone is in a constant state of remodelling
Bone Health in the Cancer Patient Stavroula Otis, M.D. Primary Care and Oncology: Practical Lessons Conference Brea Community Center May 10, 2018 Overview Healthy bone is in a constant state of remodelling
Objectives. Discuss bone health and the consequences of osteoporosis on patients medical and disability status.
 Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team