Pediatric Rheumatology: A Case-based Approach to the Basics. Hilary M. Haftel, MD, MHPE University of Michigan Department of Pediatrics
|
|
|
- Emil Griffith
- 5 years ago
- Views:
Transcription
1 Pediatric Rheumatology: A Case-based Approach to the Basics Hilary M. Haftel, MD, MHPE University of Michigan Department of Pediatrics
2 Disclosures I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in this CME activity I am not discussing any off-label uses of medications Duty hours (if they applied to me) were violated in the making of this presentation
3 Objectives Identify signs and symptoms of common rheumatologic disorders Understand appropriate laboratory testing in each disorder Understand disease course and therapy for common rheumatologic disorders
4 The Five Pediatric Rheumatology Disorders Juvenile Arthritis Systemic Lupus Erythematosus Juvenile Dermatomyositis Scleroderma (localized and systemic) Vasculitis
5 Case One A two-year-old female is brought to your office by her mother who reports that the patient was running in the front yard and fell and the mother, upon picking her up, noticed that the right knee was swollen and is worried that something is broken Exam reveals a large effusion, widening of the surrounding bones, and you are unable to fully extend the knee on range of motion
6 Juvenile Idiopathic Arthritis (JIA) (FKA Juvenile Rheumatoid Arthritis) Most common childhood arthritis** Occurs in 1:1000 children Affects children of all ages, but two peaks, at age 1-2 and age 8-12**
7 Basic Questions to Ask Acute or Chronic? Localized to joints or more systemic features? Fever or not? Actual arthritis or arthalgias? (ie., evidence of inflammation?) Complaints proportionate to physical findings or not?
8 JIA: Diagnosis** Evidence of joints inflammation -redness -swelling -limitation of range of motion -pain Duration of Arthritis > 6 weeks Age at onset < 16 years

9 JIA: Evidence of Chronicity** Synovial thickening Bony proliferation Contracture Limb length discrepancy
10 Classification of JIA Oligoarticular JIA involvement of <5 joints Polyarticular JIA involvement of 5 joints RF positive vs. RF negative Systemic JIA presence of systemic inflammation Juvenile Spondyloarthopathies Juvenile ankylosing spondylitis Inflammatory bowel disease-related arthritis Juvenile psoriatic arthritis Reactive Arthritis (FKA Reiter s syndrome)


11 Oligoarticular JIA: Clinical Features Less than 5 joints Typically affects medium to large joints Asymmetric

12 Polyarticular JIA: Clinical Features 5 or more joints affected Typically affects small to medium joints, but can include large joints Symmetric Other less common joints


13 Polyarticular JIA: Other Features Temporomandibular Joint Cervical Spine Involvement
14 Systemic JIA (aka Still s Disease) Think of it as a systemic inflammation that precedes the onset of arthritis typical fever curve** daily or diurnal temperature spike over 39ºC returns quickly to below baseline child feels well between temperature spikes
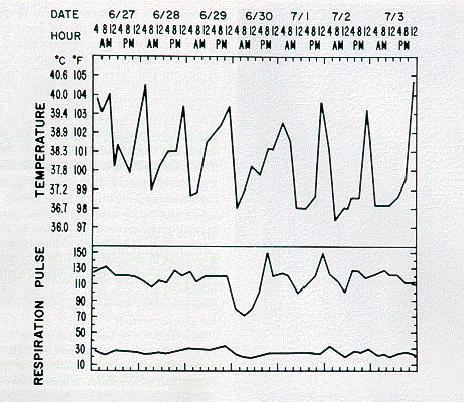
15
16 Systemic JIA (aka Still s Disease) Characteristic rash** occurs frequently at peak of fever erythematous macules on trunk and proximal extremities migratory and evanescent



17 Still s rash

18 Koebner s Phenomenon (dermatographia) Isomorphic reaction in which skin lesions appear at the site of trauma
19 Systemic JIA (Cont d) Signs of visceral involvement** hepatomegaly splenomegaly lymphadenopathy serositis pleuritis pericarditis, including pericardial effusions peritonitis No peak age of onset No gender predilection
20
21 Laboratory Testing in JIA Evidence of systemic inflammation** white blood cell count red blood cell count platelet count erythrocyte sedimentation rate C reactive protein serum proteins Antinuclear antibodies Rheumatoid factors
22 Rheumatoid Factors Antibodies directed against the Fc portion of another antibody Rheumatoid factors are negative in children with JIA** Rheumatoid factors are positive in adolescents and adults with rheumatoid arthritis Most common reason for child to make a RF is infection.
23 ANAs in JIA Frequency varies from 24-66% overall Highest frequency in patients with young (<7yrs), female Highest prevalence in patients with oligoarticular JIA and uveitis** BUT up to 20% false positive rate, especially with Hep-2 substrate
24 Laboratory Studies for Critical Exclusions Joint fluid analysis -if acute presentation, must exclude septic arthritis Complete blood count try to exclude hematologic malignancy Serologic testing for Lyme Radiography may show peri-articular osteopenia may demonstrate other abnormalities, including osteomyelitis or bone cancer
25 Goals of therapy for JIA** Control of pain and inflammation Preservation and improvement of function Prevention of disability and chronic deformity
26 Pharmacologic Therapy for JIA** Anti-inflammatory agents -NSAIDs -ASA -[corticosteroids] Disease-modifying agents -hydroxychloroquine -methotrexate -sulfasalazine -biologic agents (etanercept, infliximab, adalimumab, etc) -anakinra
27 Complications of JIA: Uveitis** Inflammation of the iris, ciliary body, and choroid Tends to be asymptomatic in children Screening in required for all children with chronic arthritis** Number One treatable cause of blindness in children**
28 Musculoskeletal Deformity Complications of JIA** Regular stretching program Splinting or bracing Regular physical exercise Constitutional Growth Delay Macrophage Activation Syndrome (HLH)
29 Outcome in JIA Remission rates 70-85% within 2-5 years** oligoarticular >90% polyarticular ~50% systemic <50% After disease, all that s left is chronic deformities and visual disturbance previously untreated
30 Case Two A 14-year-old male presents to the local ER in September with complaints of headache for one week. He also notes some weight loss, rash on his face, and diffuse joint pain Exam reveals a tired-appearing male with a pulse of 122, blood pressure 186/96, resp rate 16, temp 36.7

31 Case Two (continued) Facial rash Diffuse joint swelling UA reveals blood, protein, and red cell casts
32 Systemic Lupus Erythematosus Incidence/Prevalence per 100,000 incidence approx 5-10,000 cases in US Approximately 15% present before age 16 rare < 5 years, in freq through adolescence Gender 0-9 years, 4:3 F:M yrs, 4: yrs, 5:1

33 Clinical Manifestations of SLE** Mucous Membranes Frequency 12% Mouth ulcers Nasal ulcers large mouth ulcer
34 Clinical Manifestation of SLE** Musculoskeletal (72%) arthralgias/arthritis myalgias/myositis Serositis (30-40%) pericarditis pleuritis peritonitis Cardiovascular (15%) raynaud s phenomenon myocarditis/endocarditis
35 Clinical Manifestations of SLE** Renal (82%) proteinuria casts Neurologic (44%) seizures psychosis Depression Hematologic (50%) Bleeding/bruising Petechiae
36 Clinical Manifestations of SLE** Non-specific (100%) malaise fever weight loss Cutaneous (80-95%) malar rash discoid LE subacute cutaneous LE photosensitivity
37 Laboratory Testing in SLE** Cytopenias hemolytic anemia leukopenia/lymphopenia thrombocytopenia Antinuclear antibodies Anti-DNA antibodies Extractable Nuclear Antibodies (Ro, La, Sm, RNP) Complement
38 Criteria to Diagnose SLE 2012 SLICC Criteria versus 1997 ACR criteria Require presence of both clinical and immunologic abnormalities Both require at least 4 criteria** SLICC includes at least 1 clinical and 1 immunologic SLICC includes renal-isolated lupus and more neuro features
39 ACR Criteria for SLE 1997: Clinical Malar rash Discoid rash Photosensitivity Oral ulceration Arthritis Serositis Renal Neurologic (seizures or psychosis) Hematologic (hemolytic anemia, leukopenia, lymphopenia, thrombocytopenia)
40 ACR Criteria1997: Laboratory Positive ANA Positive immunoserology ds DNA antibodies Sm antibody Antiphospholipid Ab 4 of 11 criteria sensitivity of 83%, specificity of 96%
41 SLICC Criteria for SLE 2012: Clinical Acute cutaneous lupus Chronic cutaneous lupus Oral or nasal ulceration Non-scarring alopecia Synovitis Serositis Renal Neurologic involvement (seizure, psychosis, mononeuritis multiplex, nyelitis, neuropathy, acute confusional state) Hemolytic anemia Leukopenia or lymphopenia Thrombocytopenia
42 SLICC Criteria 2012: Laboratory Positive ANA Anti-ds DNA antibodies Anti-Sm antibody Antiphospholipid Antibodies (lupus anticoagulant, falsepositive RPR, anticardiolipin antibodies, anti-beta 2- glycoprotein I) Low complement (low C3, low C4, low CH50) Positive direct Coombs test without a hemolytic anemia 4 of 11 criteria sensitivity of 97%, specificity of 94%
43 Corticosteroids Oral Intravenous SLE: Treatment** Hydroxychloroquine (Plaquenil) Methotrexate Mycophenolate Mofetil Cyclophosphamide Other Calcium Vitamin D
44 Growth failure Fertility/amenorrhea Osteoporosis Body image Complications of Treatment** weight gain cushingoid appearance acne
45 Case Three A five-year-old male is brought to your office by his parents for complaints of decreased energy and difficulty performing regular tasks. This has been worsening over the last several weeks. He denies any muscle or joint tenderness. On review of systems, his parents report that he has had eczema on his face for the last several months that has been resistant to any medical therapy Physical exam reveals a cooperative male who is unable to lift his arms above his head or get up from a sitting position. Skin exam reveals a facial rash and red bumps on his fingers.
46 Juvenile Dermatomyositis (JDM) Frequency in population 0.5 per 100,000 Bimodal peak of age of onset years (approx 16-20%) years Gender predilection: approx 2:1 F:M
47 Clinical Manifestions of JDM Cutaneous Manifestations** JDM rash heliotrope rash Gottron s papules periungual erythema ulcerative disease [acanthosis nigricans] Proximal muscle weakness** large muscle groups versus small clues on movement and gait

48 Clinical Manifestations of JDM Evidence of inflammatory myositis** elevated muscle enzymes eletromyography muscle biopsy magnetic resonance imaging Gastrointestinal Respiratory Calcinosis Lipoatrophy
49 Laboratory Testing in JDM Muscle enzymes** AST/SGOT ALT/SGPT CPK aldolase LDH Antibodies Antinuclear antibodies (frequency 10-80%) PM1, Jo1, etc (<20% in children)
50 JDM: Differential Diagnosis Dermatomyositis versus polymyositis Muscular dystrophy Guillain-Barre disease Other inflammatory myopathies
51 JDM: Treatment** Immunosuppressive therapy Prednisone Steroid-sparing agents: -methotrexate -cyclophosphamide -cyclosporine -azathioprine Intravenous immunoglobulin Stretching to maintain range of motion Continuation of other regular activities
52 JDM: Complications** Respiratory impairment GI vasculitis Steroid-related side effects Side effects of steroid-sparing agents Calcinosis Insulin resistance/lipoatrophy
53 JDM: Long Term Outcomes** 70% well and functional 20% long term complications 10% die
54 Case Four A 13-year-old female presents with persistent and increasing rash on her left lower extremity. It is red, nontender, and nonpruritic, but is interfering with her ability to extend her leg Physical exam reveals a firm, shiny, erythematous strip of skin extending from the left hip, down the lateral side of her leg, across her knee to the dorsal surface of her foot.

55
56 Scleroderma and Relatives Types Localized scleroderma** morphea linear scleroderma Diffuse scleroderma** systemic sclerosis CREST Mixed Connective Tissue Disease Eosinophilic Fasciitis

57
58 Clinical Manifestations of Scleroderma** Cutaneous (skin thickening) Musculoskeletal Limitation of range of motion Abnormal limb growth Raynaud s phenomenon Gastrointestinal Pulmonary Renal
59 Laboratory Testing in Scleroderma Antinuclear Antibodies SCL-70 (DNA-topoisomerase 1) 26% freq anticentromere (kinetochore) 22% freq anti-rnp (100% freq in MCTD) Rheumatoid Factors Proteinuria/hematuria Hematologic anemia eosinophilia
60 Scleroderma: Treatment** Immune modulators/anti-inflammatory therapy Prednisone Methotrexate Cyclophosphamide Decrease Collagen cross linking [D-penicillamine] Prevention of further organ injury: -Ca channel blockers -cold precautions Preservation of function: -intensive PT/OT General supportive care
61 Systemic Vasculitis Very rare in children** Peak age 9-11 yrs, range 3-16 yrs Equal incidence male/female Most presentations of systemic vasculitis do not follow specific patterns Some more common vasculitic syndromes of childhood present as a constellation of otherwise nonspecific symptoms Most common vasculitis of childhood is Kawasaki Disease (discussed elsewhere)
62 Case Five An eight-year-old boy presents to the emergency room with bruising on his lower extremities and abdominal pain. Physical exam reveals purpura on both legs, as well as bilateral ankle arthritis. His scrotum is swollen and ecchymotic. Abdominal exam demonstrates normal bowel sounds and no HSM.
63 Henoch-Schonlein Purpura AKA anaphylactoid purpura Second most common vasculitis of childhood Most common in children 5-15 years of age, rare in adults** Male to female 1.5 : 1 Incidence varies from 0.1 to 13.5 per 100,000 Seasonal variation: peaks during winter? Relationship to streptococcus
64 HSP: Clinical Manifestations Cutaneous Manifestations** Palpable purpura (100%) most prominent in dependent areas, legs, buttocks range from petechiae to ecchymoses can be preceded by urticaria or MP SQ edema of hands and feet, face, scrotum

65
66 HSP: Clinical Manifestations Arthalgias/Arthritis (65-85%)** usually involves large joints (knees, ankles) periarticular swelling and tenderness, but usually non-erythematous transient, but not migratory lasts few days to a week
67 HSP: Clinical Manifestations Gastrointestinal involvement (60-100%)** Gut vasculitis colicky abdominal pain heme (+) stools intestinal perforation within one wk to one month of rash Renal involvement (20-50%)** acute glomerulonephritis hematuria/proteinuria hypertension renal failure within one to three months of rash
68 HSP: Laboratory Testing Pathology: leukocytoclastic vasculitis with IgA deposition Must not have thrombocytopenia** May have elevated inflammatory parameters Normochromic normocytic anemia Abnormal urinary sediment Normal complements
69 EULAR Consensus Criteria for HSP classical palpable nonthrombocytopenic purpuric rash and any one of the following: Arthritis or arthralgia Abdominal pain and/or GI bleeding Any biopsy with predominant IgA deposition
70 Supportive care NSAIDs for arthritis Corticosteroids for severe GI disease Active renal disease 1 mg/kg/d divided bid HSP: Treatment**
71 HSP: Disease Course Resolves within one month in 66% At least 50% will have recurrence, usually of rash or GI symptoms** usually within first 6 wks, but up to 1-2 years Don t forget intussussception** Late renal outcome: less than 5% progress to end stage renal disease
72 Any additional questions?
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS LUPUS 101 SLE SUBSETS AUTOIMMUNE DISEASE 11/4/2013 HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS
 LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Definition Chronic autoimmune disease The body s immune system starts attacking itself Can affect most organs and tissues in the body Brain, lungs, he
 LIVING WITH SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. Rowan Diagnostic Clinic Salisbury, N.C. May 11, 2013 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement
LIVING WITH SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. Rowan Diagnostic Clinic Salisbury, N.C. May 11, 2013 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement
Rheumatology 101 A Pediatrician s Guide
 Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Systemic Lupus Erythematosus
 Systemic Lupus Erythematosus Marc C. Hochberg, MD, MPH Professor of Medicine and Head, Division of Rheumatology University of Maryland School of Medicine CASE: HISTORY A 26-year-old woman is seen for migratory
Systemic Lupus Erythematosus Marc C. Hochberg, MD, MPH Professor of Medicine and Head, Division of Rheumatology University of Maryland School of Medicine CASE: HISTORY A 26-year-old woman is seen for migratory
JuvenileIdiopathicArthritis. Dr Johan Siebert
 JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
Rheumatology Primer: What Labs and When
 Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
MANAGING THE PATIENT WITH POSITIVE ANA
 MANAGING THE PATIENT WITH POSITIVE ANA Rafael F. Rivas-Chacon, M.D. Disclosures Grant/Research support for: Pfizer Study JIA A3921104 Tofacitinib not related to this presentation 1 Positive Antinuclear
MANAGING THE PATIENT WITH POSITIVE ANA Rafael F. Rivas-Chacon, M.D. Disclosures Grant/Research support for: Pfizer Study JIA A3921104 Tofacitinib not related to this presentation 1 Positive Antinuclear
Insights into the DX of Pediatric SLE
 Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
PGALS: Approach to Child with Arthritis. Prof Chris Scott Paediatric Rheumatology
 PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
LUPUS (SLE) MEDICAL SOURCE STATEMENT
 MEDICAL SOURCE STATEMENT") LUPUS (SLE) MEDICAL SOURCE STATEMENT From: Re: (Name of Patient) (Social Security No.) Please answer the following questions concerning your patient s impairments. Attach relevant treatment notes, radiologist
LUPUS (SLE) MEDICAL SOURCE STATEMENT From: Re: (Name of Patient) (Social Security No.) Please answer the following questions concerning your patient s impairments. Attach relevant treatment notes, radiologist
UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS
 UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. October 20, 2012 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement Diagnosis Treatment Pregnancy
UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. October 20, 2012 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement Diagnosis Treatment Pregnancy
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis
 Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Juvenile Idiopathic Arthritis (JIA)
") Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Department of Paediatrics Clinical Guideline. Guideline for the child with possible arthritis (joint swelling/pain, loss of function)
") Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Rheumatoid Arthritis. Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011
 Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
Living with Lupus: An Insider s Perspective
 Living with Lupus: An Insider s Perspective Pamela Thorpe, MD, FACP Lupus Foundation of America, Inc. Philadelphia Tri-State Chapter Volunteer May 2014 My Own Story Is it Lupus Yet? The What What is this?
Living with Lupus: An Insider s Perspective Pamela Thorpe, MD, FACP Lupus Foundation of America, Inc. Philadelphia Tri-State Chapter Volunteer May 2014 My Own Story Is it Lupus Yet? The What What is this?
Treatment modalities Prof Ally 2012
 Treatment modalities Prof Ally 2012 Analgesia Types of Pain Nociceptive /neuropathic nociceptive Tissue damage - trauma, inflammation Somatic (musculoskeletal): local pain referred pain Neuropathic pain:
Treatment modalities Prof Ally 2012 Analgesia Types of Pain Nociceptive /neuropathic nociceptive Tissue damage - trauma, inflammation Somatic (musculoskeletal): local pain referred pain Neuropathic pain:
9/25/2013 SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)
") SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
Conflict of Interest. Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital.
 Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital Conflict of Interest Disclosures: None Overview Diagnostic Classification Criteria of SLE
Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital Conflict of Interest Disclosures: None Overview Diagnostic Classification Criteria of SLE
Henoch Schonlein Purpura
 CHILDREN S SERVICES Henoch Schonlein Purpura Definition A vasculitic syndrome of small vessels classically characterised by a purpuric rash, abdominal pain, arthritis, and nephritis. Platelet count and
CHILDREN S SERVICES Henoch Schonlein Purpura Definition A vasculitic syndrome of small vessels classically characterised by a purpuric rash, abdominal pain, arthritis, and nephritis. Platelet count and
Jeopardy. What s the rash? $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400
 Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z
 from Harvard Medical School Health Topics A-Z") Topic Page: Systemic Lupus Erythematosus Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z What Is It? Lupus is thought to develop when the immune system
Topic Page: Systemic Lupus Erythematosus Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z What Is It? Lupus is thought to develop when the immune system
SLE and the Antiphospholipid Syndrome
 SLE and the Antiphospholipid Syndrome Susan Y. Ritter MD, PhD Associate Physician Division of Rheumatology, Immunology and Allergy Department of Medicine Brigham and Women s Hospital Instructor in Medicine
SLE and the Antiphospholipid Syndrome Susan Y. Ritter MD, PhD Associate Physician Division of Rheumatology, Immunology and Allergy Department of Medicine Brigham and Women s Hospital Instructor in Medicine
Juvenile Chronic Arthritis
 Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Is it Autoimmune or NOT! Presented to AONP! October 2015!
 Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Autoimmune diseases. SLIDE 3: Introduction to autoimmune diseases Chronic
 SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Residual Functional Capacity Questionnaire SYSTEMIC LUPUS ERYTHEMATOSUS
 Residual Functional Capacity Questionnaire SYSTEMIC LUPUS ERYTHEMATOSUS Patient: DOB: Physician completing this form: Please complete the following questions regarding this patient's impairments and attach
Residual Functional Capacity Questionnaire SYSTEMIC LUPUS ERYTHEMATOSUS Patient: DOB: Physician completing this form: Please complete the following questions regarding this patient's impairments and attach
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital
 Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital
 Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Rheumatoid Arthritis
 Rheumatoid Arthritis What is rheumatoid arthritis? Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Rheumatoid arthritis can also cause inflammation of
Rheumatoid Arthritis What is rheumatoid arthritis? Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Rheumatoid arthritis can also cause inflammation of
Development of SLE among Possible SLE Patients Seen in Consultation: Long-Term Follow-Up. Disclosures. Background. Evidence-Based Medicine.
 Development of SLE among Patients Seen in Consultation: Long-Term Follow-Up Abstract # 1699 May Al Daabil, MD Bonnie L. Bermas, MD Alexander Fine Hsun Tsao Patricia Ho Joseph F. Merola, MD Peter H. Schur,
Development of SLE among Patients Seen in Consultation: Long-Term Follow-Up Abstract # 1699 May Al Daabil, MD Bonnie L. Bermas, MD Alexander Fine Hsun Tsao Patricia Ho Joseph F. Merola, MD Peter H. Schur,
.,Dr Ali Alkazzaz Babylon collage of medicine 2016
 .,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
.,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
A CRP B FBC C LFT D blood culture E uric acid
 1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
Test Name Results Units Bio. Ref. Interval
 LL - LL-ROHINI (NATIONAL REFERENCE 135091593 Age 25 Years Gender Male 30/8/2017 91600AM 30/8/2017 93946AM 31/8/2017 84826AM Ref By Final COLLAGEN DISEASES ANTIBODY ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF),
LL - LL-ROHINI (NATIONAL REFERENCE 135091593 Age 25 Years Gender Male 30/8/2017 91600AM 30/8/2017 93946AM 31/8/2017 84826AM Ref By Final COLLAGEN DISEASES ANTIBODY ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF),
Test Name Results Units Bio. Ref. Interval
 135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
Undifferentiated Connective Tissue Disease and Overlap Syndromes. Mark S. Box, MD
 Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Department of Paediatrics Clinical Guideline
 Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
JIA and Other Rheumatic Diseases in Children. Norma Liburd, RN-BC, MN
 JIA and Other Rheumatic Diseases in Children Norma Liburd, RN-BC, MN Define Juvenile Idiopathic Arthritis (JIA) and discuss the diagnostic criteria. Objectives Identify the subtypes of JIA and discuss
JIA and Other Rheumatic Diseases in Children Norma Liburd, RN-BC, MN Define Juvenile Idiopathic Arthritis (JIA) and discuss the diagnostic criteria. Objectives Identify the subtypes of JIA and discuss
ONE of the following:
 Medical Coverage Policy Belimumab (Benlysta) EFFECTIVE DATE: 01 01 2012 POLICY LAST UPDATED: 11 21 2017 OVERVIEW Belimumab (Benlysta ) is indicated for the treatment of adult patients with active, autoantibody-positive,
Medical Coverage Policy Belimumab (Benlysta) EFFECTIVE DATE: 01 01 2012 POLICY LAST UPDATED: 11 21 2017 OVERVIEW Belimumab (Benlysta ) is indicated for the treatment of adult patients with active, autoantibody-positive,
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Reporting Autoimmune Diseases in Hematopoietic Stem Cell Transplantation
 Reporting Autoimmune Diseases in Hematopoietic Stem Cell Transplantation Marcelo C. Pasquini, MD, MSc HVD05_1.ppt Outline Review of autoimmune diseases (AID). Role of transplantation for AID Data collection:
Reporting Autoimmune Diseases in Hematopoietic Stem Cell Transplantation Marcelo C. Pasquini, MD, MSc HVD05_1.ppt Outline Review of autoimmune diseases (AID). Role of transplantation for AID Data collection:
Benlysta (belimumab) Prior Authorization Criteria Program Summary
 Prior Authorization Criteria Program Summary") Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Rheumatoid arthritis
 Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Acute Emergencies in Rheumatology
 Acute Emergencies in Rheumatology Clare Higgens Northwick Park hospital and St George s Hospital London Acute Rheumatological Emergencies The Acute Hot joint Inflammatory back pain.. Systemic lupus erythematosus(sle)
Acute Emergencies in Rheumatology Clare Higgens Northwick Park hospital and St George s Hospital London Acute Rheumatological Emergencies The Acute Hot joint Inflammatory back pain.. Systemic lupus erythematosus(sle)
PEDIATRIC RHEUMATOLOGY:A PRIMARY CARE PERSPECTIVE STEVE TRAVIS, MD, FAAP, FACP
 PEDIATRIC RHEUMATOLOGY:A PRIMARY CARE PERSPECTIVE STEVE TRAVIS, MD, FAAP, FACP PEDIATRIC RHEUMATOLGY I I have no personal or financial conflicts of interest involving this presentation. I WILL BE discussing
PEDIATRIC RHEUMATOLOGY:A PRIMARY CARE PERSPECTIVE STEVE TRAVIS, MD, FAAP, FACP PEDIATRIC RHEUMATOLGY I I have no personal or financial conflicts of interest involving this presentation. I WILL BE discussing
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
To live with lupus, we need to know about lupus.
 To live with lupus, we need to know about lupus. Zineb Aouhab, MD Assistant Professor of Medicine Loyola University Medical Center Division of Rheumatology 1 Where did the word lupus come from? The word
To live with lupus, we need to know about lupus. Zineb Aouhab, MD Assistant Professor of Medicine Loyola University Medical Center Division of Rheumatology 1 Where did the word lupus come from? The word
Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS
 Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients
Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients
HENOCH SCHÖNLEIN PURPURA (VASCULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests (SC)
 IN CHILDREN Single choice tests (SC)") HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
L. Nandini Moorthy, MD MS 2012
 L. Nandini Moorthy, MD MS 2012 L Nandini Moorthy, MD MS 09 17 yo Ashkenazi male with proximal muscle pain and weakness, mild malar erythema and erythema over knees and dorsal aspect of PIPs Mild tenderness
L. Nandini Moorthy, MD MS 2012 L Nandini Moorthy, MD MS 09 17 yo Ashkenazi male with proximal muscle pain and weakness, mild malar erythema and erythema over knees and dorsal aspect of PIPs Mild tenderness
Lupus and Friends Perspectives on common syndromes and Primary care responses
 Lupus and Friends Perspectives on common syndromes and Primary care responses Paul H Caldron DO, PhD, FACP, FACR, MBA Arizona Arthritis and Rheumatology Associates, PC University of Arizona College of
Lupus and Friends Perspectives on common syndromes and Primary care responses Paul H Caldron DO, PhD, FACP, FACR, MBA Arizona Arthritis and Rheumatology Associates, PC University of Arizona College of
What will we discuss today?
 Autoimmune diseases What will we discuss today? Introduction to autoimmune diseases Some examples Introduction to autoimmune diseases Chronic Sometimes relapsing Progressive damage Epitope spreading more
Autoimmune diseases What will we discuss today? Introduction to autoimmune diseases Some examples Introduction to autoimmune diseases Chronic Sometimes relapsing Progressive damage Epitope spreading more
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition
 Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
10/25/2018. Autoimmunity and how to treat it. Disclosure. Why do we get autoimmunity? James Verbsky MD/PhD Pediatric Rheumatology/Immunology
 Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
CIBMTR Center Number: CIBMTR Recipient ID: RETIRED. Today s Date: Date of HSCT for which this form is being completed:
 Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic,
Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic,
Guideline on the clinical management of Henoch Schonlein Purpura (HSP)
") Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
SCLERODERMA 101. Maureen D. Mayes, MD, MPH Professor of Medicine University of Texas - Houston
 SCLERODERMA 101 Maureen D. Mayes, MD, MPH Professor of Medicine University of Texas - Houston TYPES OF SCLERODERMA Localized versus Systemic Two Kinds of Scleroderma Localized Scleroderma Morphea Linear
SCLERODERMA 101 Maureen D. Mayes, MD, MPH Professor of Medicine University of Texas - Houston TYPES OF SCLERODERMA Localized versus Systemic Two Kinds of Scleroderma Localized Scleroderma Morphea Linear
ERROR CORRECTION FORM
 Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Registry Use Only Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic, syngeneic unrelated related
Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Registry Use Only Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic, syngeneic unrelated related
Henoch-Schonlein Purpura Guidelines
 Henoch-Schonlein Purpura Guidelines Henoch-Schonlein purpura (HSP) is the commonest vasculitis of childhood which is selflimiting in majority of cases. Epidemiology: Incidence varies from 10-20 per 100000
Henoch-Schonlein Purpura Guidelines Henoch-Schonlein purpura (HSP) is the commonest vasculitis of childhood which is selflimiting in majority of cases. Epidemiology: Incidence varies from 10-20 per 100000
Patient with Musculo-skeletal Complaints - Summary
 Patient with Musculo-skeletal Complaints - Summary 1. Soft Tissue Rheumatism or Arthritis 2. Arthritis Monoarticular Polyarticular - :- (Asymmetrical) (Symetrical) :- -Crystals, Gout - Infective acute
Patient with Musculo-skeletal Complaints - Summary 1. Soft Tissue Rheumatism or Arthritis 2. Arthritis Monoarticular Polyarticular - :- (Asymmetrical) (Symetrical) :- -Crystals, Gout - Infective acute
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
The Power of the ANA. April 2018 Emily Littlejohn, DO MPH
 Emergent Rheumatologic Diseases and Disorders for Primary Care. The Power of the ANA April 2018 Emily Littlejohn, DO MPH Question 1: the ANA test is: A) A screening test with high specificity to diagnose
Emergent Rheumatologic Diseases and Disorders for Primary Care. The Power of the ANA April 2018 Emily Littlejohn, DO MPH Question 1: the ANA test is: A) A screening test with high specificity to diagnose
Reiter s Syndrome: Clinical Features
 Reiter s Syndrome: Clinical Features Arthritis lower extremities Enthesitis Spondylitis Tenosynovitis Dactylitis Urethritis Uveitis Oral ulcers Keratoderma Balanitis HLA B-27 Positive (80%) Reactive Arthritis:
Reiter s Syndrome: Clinical Features Arthritis lower extremities Enthesitis Spondylitis Tenosynovitis Dactylitis Urethritis Uveitis Oral ulcers Keratoderma Balanitis HLA B-27 Positive (80%) Reactive Arthritis:
Systemic Lupus Erythematosus in Libyan Children: Diagnosis and Management
 Research Article imedpub Journals www.imedpub.com ARCHIVES OF MEDICINE DOI: 10.21767/1989-5216.1000276 Abstract Systemic Lupus Erythematosus in Libyan Children: Diagnosis and Management Background: Childhood
Research Article imedpub Journals www.imedpub.com ARCHIVES OF MEDICINE DOI: 10.21767/1989-5216.1000276 Abstract Systemic Lupus Erythematosus in Libyan Children: Diagnosis and Management Background: Childhood
Pediatric Rheumatology Board Review
 Pediatric Rheumatology Board Review Simona Nativ, MD Pediatric Rheumatology Goryeb Children s Hospital Question #1 A 2 year old male (pictured at left) presents with his mother who complains that his left
Pediatric Rheumatology Board Review Simona Nativ, MD Pediatric Rheumatology Goryeb Children s Hospital Question #1 A 2 year old male (pictured at left) presents with his mother who complains that his left
When is it Rheumatoid Arthritis When to Refer
 When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
Systemic examination
 PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
UPDATES ON PEDIATRIC SLE
 UPDATES ON PEDIATRIC SLE BY ANGELA MIGOWA, PEDIATRIC RHEUMATOLOGIST/SENIOR INSTRUCTOR AKUHN MBCHB-UON, MMED-AKUHN,PEDIATRIC RHEUMATOLOGY- MCGILL UNIVERSITY HEALTH CENTRE ROSA PARKS OBJECTIVES RECOGNIZE
UPDATES ON PEDIATRIC SLE BY ANGELA MIGOWA, PEDIATRIC RHEUMATOLOGIST/SENIOR INSTRUCTOR AKUHN MBCHB-UON, MMED-AKUHN,PEDIATRIC RHEUMATOLOGY- MCGILL UNIVERSITY HEALTH CENTRE ROSA PARKS OBJECTIVES RECOGNIZE
Lupus. Fast facts. What is lupus? What causes lupus? Who gets lupus?
 Lupus Systemic lupus erythematosus, referred to as SLE or lupus, is sometimes called the "great imitator." Why? Because of its wide range of symptoms, people often confuse lupus with other health problems.
Lupus Systemic lupus erythematosus, referred to as SLE or lupus, is sometimes called the "great imitator." Why? Because of its wide range of symptoms, people often confuse lupus with other health problems.
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
13. Behçet s - In Children
 Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk 13. Behçet s - In Children How are children affected by Behçet s disease? Behçet s disease (also
Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk 13. Behçet s - In Children How are children affected by Behçet s disease? Behçet s disease (also
Policy. Section: Medicine Effective Date: January 15, 2015 Subsection: Pathology/Laboratory Original Policy Date: December 5, 2014 Subject:
 Last Review Status/Date: December 2014 Page: 1 of 10 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Last Review Status/Date: December 2014 Page: 1 of 10 Summary Systemic lupus erythematosus (SLE) is an autoimmune connective tissue disease that can be difficult to diagnose because patients often present
Autoantibodies in the Idiopathic Inflammatory Myopathies
 Autoantibodies in the Idiopathic Inflammatory Myopathies Steven R. Ytterberg, M.D. Division of Rheumatology Mayo Clinic Rochester, MN The Myositis Association Annual Conference St. Louis, MO Sept. 25,
Autoantibodies in the Idiopathic Inflammatory Myopathies Steven R. Ytterberg, M.D. Division of Rheumatology Mayo Clinic Rochester, MN The Myositis Association Annual Conference St. Louis, MO Sept. 25,
Inflammatory Myopathies 4 th year MBBS. Marwan Adwan MBChB, MSc, MRCPI, MRCP(rheum) Consultant Rheumatologist
 Consultant Rheumatologist") Inflammatory Myopathies 4 th year MBBS Marwan Adwan MBChB, MSc, MRCPI, MRCP(rheum) Consultant Rheumatologist Case A 64 woman presents with erythematous itchy rash over back of hands & forehead. For 1 month
Inflammatory Myopathies 4 th year MBBS Marwan Adwan MBChB, MSc, MRCPI, MRCP(rheum) Consultant Rheumatologist Case A 64 woman presents with erythematous itchy rash over back of hands & forehead. For 1 month
Myositis and Your Lungs
 Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Learning about Lupus. Learning About Lupus. Lupus Society of Illinois
 Learning About Lupus Learning about Lupus Lupus Society of Illinois 525 W. Monroe Street, Suite 900 Chicago, Illinois 60661 Robert S. Katz, M.D. Professor of Medicine Rush University Medical Center Northwestern
Learning About Lupus Learning about Lupus Lupus Society of Illinois 525 W. Monroe Street, Suite 900 Chicago, Illinois 60661 Robert S. Katz, M.D. Professor of Medicine Rush University Medical Center Northwestern
Test Name Results Units Bio. Ref. Interval
 135091660 Age 44 Years Gender Male 29/8/2017 120000AM 29/8/2017 100219AM 29/8/2017 105510AM Ref By Final EXTRACTABLENUCLEAR ANTIGENS (ENA), QUANTITATIVE ROFILE CENTROMERE ANTIBODY, SERUM 20-30 Weak ositive
135091660 Age 44 Years Gender Male 29/8/2017 120000AM 29/8/2017 100219AM 29/8/2017 105510AM Ref By Final EXTRACTABLENUCLEAR ANTIGENS (ENA), QUANTITATIVE ROFILE CENTROMERE ANTIBODY, SERUM 20-30 Weak ositive
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abatacept, for rheumatoid arthritis, 789 Acetaminophen, for low back pain, 735 Acupuncture for fibromyalgia, 753 for low back pain, 738
Index Note: Page numbers of article titles are in boldface type. A Abatacept, for rheumatoid arthritis, 789 Acetaminophen, for low back pain, 735 Acupuncture for fibromyalgia, 753 for low back pain, 738
Systemic Lupus Erythematosus among Jordanians: A Single Rheumatology Unit Experience
 Systemic Lupus Erythematosus among Jordanians: A Single Rheumatology Unit Experience Ala M. AlHeresh MD* ABSTRACT Objectives: To study the characteristics of Systemic Lupus Erythematosus in Jordan and
Systemic Lupus Erythematosus among Jordanians: A Single Rheumatology Unit Experience Ala M. AlHeresh MD* ABSTRACT Objectives: To study the characteristics of Systemic Lupus Erythematosus in Jordan and
SCLERODERMA. Scleroderma update. No disclosures or conflicts. Leslie Kahl, M.D. April 10, 2015
 Scleroderma update Leslie Kahl, M.D. April 10, 2015 No disclosures or conflicts KT is a 45 year old woman who developed puffiness in her fingers 1/2013 and carpal tunnel syndrome and arthralgias 3/2013.
Scleroderma update Leslie Kahl, M.D. April 10, 2015 No disclosures or conflicts KT is a 45 year old woman who developed puffiness in her fingers 1/2013 and carpal tunnel syndrome and arthralgias 3/2013.
Autoimmunity and autoinflammation
 Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
New Onset Arthritis. Clinical Dilemmas in Arthritis and Rheumatology. Physical Examination. Other Pertinent History
 New Onset Arthritis Clinical Dilemmas in Arthritis and Rheumatology Primary Care Principles and Practice October 2008 Jonathan Graf, MD Assistant Professor of Medicine, UCSF Division of Rheumatology, SFGH
New Onset Arthritis Clinical Dilemmas in Arthritis and Rheumatology Primary Care Principles and Practice October 2008 Jonathan Graf, MD Assistant Professor of Medicine, UCSF Division of Rheumatology, SFGH
Dhanalakshmi.R II yr MD Stanley medical college
 Dhanalakshmi.R II yr MD Stanley medical college 10 Yr old female child - abdominal pain & vomiting for 1 day. Diffuse in nature, moderate in intensity, not related to food intake & radiates to back. No
Dhanalakshmi.R II yr MD Stanley medical college 10 Yr old female child - abdominal pain & vomiting for 1 day. Diffuse in nature, moderate in intensity, not related to food intake & radiates to back. No
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
10/6/08. Systemic Lupus Erythematosus. SLE Epidemiology: who is at risk? Margrit Wiesendanger Division of Rheumatology, CUMC.
 Systemic Lupus Erythematosus SLE Epidemiology: who is at risk? One of the most common autoimmune diseases affecting women of all ages Predominantly women in child-bearing years (M:F ratio is 1:10) Incidence
Systemic Lupus Erythematosus SLE Epidemiology: who is at risk? One of the most common autoimmune diseases affecting women of all ages Predominantly women in child-bearing years (M:F ratio is 1:10) Incidence
VASCULITIC SYNDROMES. Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018
 VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
Physical examination of the musculosceletal- and nervous system. Pánczél Pál dr.
 Physical examination of the musculosceletal- and nervous system in the practice of internal medicine. Pánczél Pál dr. Bursae = sacks of the synovial membrane fulfilled with synovium. Localised between
Physical examination of the musculosceletal- and nervous system in the practice of internal medicine. Pánczél Pál dr. Bursae = sacks of the synovial membrane fulfilled with synovium. Localised between
CIBMTR Center Number: CIBMTR Recipient ID: RETIRED. Today s Date: Date of HSCT for which this form is being completed: &
 Systemic Lupus Erythematosus Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: & HSCT type: o autologous o allogeneic, o
Systemic Lupus Erythematosus Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: & HSCT type: o autologous o allogeneic, o