PEDIATRIC RHEUMATOLOGY:A PRIMARY CARE PERSPECTIVE STEVE TRAVIS, MD, FAAP, FACP
|
|
|
- Allen Houston
- 6 years ago
- Views:
Transcription
1 PEDIATRIC RHEUMATOLOGY:A PRIMARY CARE PERSPECTIVE STEVE TRAVIS, MD, FAAP, FACP
2 PEDIATRIC RHEUMATOLGY I I have no personal or financial conflicts of interest involving this presentation. I WILL BE discussing some treatments that are not FDA approved.
3 OBJECTIVES INTRODUCE THE LEARNER TO COMMON PEDIATRIC RHEUMATOLOGICAL PROCESSES. DISCUSS COMMON CLINICAL PRESENTATIONS AND APPROPRIATE EVALUATION UNDERSTAND GENERALIZED TREATMENT APPROACHES FOR TREATMENT OF ABOVE.
4 JUVENILE IDIOPATHIC ARTHRITIS Confusing because of various nomenclatures and confusion with adult specific disease processes. Some overlap and imperfect classification. New classification is based on the 1997 International League of Associations for the Rheumatology (ILAR) Terms Juvenile Rheumatoid Arthritis and Juvenile Chronic Arthritis where abandoned. The new term Juvenile Idiopathic Arthritis (JIA) was adopted.
5 JUVENILE IDIOPATHIC ARTHRITIS Occurring before the age of 16 y/o. Involving Persistent Synovitis in one or more joints. Synovitis for at least 6 weeks.
6 JUVENILE IDIOPATHIC ARTHRITIS OLIGOARTICULAR POLYARTICULAR- RHEUMATOID FACTOR POSITIVE POLYARTICULAR RHEUMATOID FACTOR NEGATIVE JUVENILE PSORIATIC ARTHRITIS ENTHESITIS-RELATED ARTHROPATHIES UNDIFFERENTIATEDJIA SYSTEMIC JIA
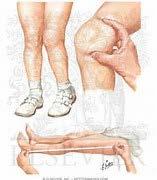
7 OLIGOARTICULAR JIA Four or fewer joints during the first 6 months. 1-7 years of age F:M 3:1 Uveitis F:M 6.5:1 Typically involves incidental joint swelling or limp Knee>ankle>elbow>wrists Fever, rash, and night pain typically do not occur
8 OLIGOARTICULAR JIA Persistent- only 4 or fewer joints throughout the course of the disease Extended- Initially develops 4 or fewer joints but other joint involvement after 6 months
9 OLIGOARTICULAR JIA
10 OLIGOARTICULAR JIA UVEITIS is most commonly associated with this form of JIA Typically asymptomatic but if not diagnosed and treated appropriately can result in cataracts, glaucoma and blindness ANA status is determined strictly to determine risk of Uveitis and determine frequency of slit lamp examination High risk factors include positive ANA, female sex, age at onset less than 6 years old, and duration of disease less than 4 years

11 OLIGOARTICULAR JIA
12 OLIGOARTICULAR JIA If ANA positive, less than 6y/o at diagnosis and duration less than 4 years then needs eye exam every 3 months. If ANA positive, age at onset less than 6 y/o and duration of disease greater than 4 years then check every 6 months. If ANA positive, age at onset less than 6 y/o and duration of disease >7 years then check every 12 months. If ANA positive, age at onset greater than 6y/o and duration less than 4 years then check every 6 months. If ANA positive, age at onset greater than 6 y/o and duration more than 4 years then check every 12 months.
13 OLIGOARTICULAR JIA Treatment usually involves joint injections and NSAIDS. Occasionally requires Disease Modifying Rheumatological Diseases (DMRDs) or biologics. Pts will often out grow this disease. Continue eye exams even if arthritis is quiet.
14 POLYARTICULAR JIA Rheumatoid Factor Negative- peaks at 1-3 y/o and at 10 y/o. Rheumatoid Factor Positive- More common in teens. Probably early onset of Adult type Rheumatoid Arthritis. Uveitis only in 10-15% of ANA positive. Needs eye exams every 6 months. Typically do require DMRD and often times biologic.

15 POLYARTICULAR JIA
16 PSORIATIC ARTHRITIS Arthritis and psoriasis Arthritis and at least two of the following: Dactylitis Nail pitting or oil spots or onycholysis Family history of psoriasis in at least one 1 st degree relative

17 PSORIATIC ARTHRITIS

18 PSORIATIC ARTHRITIS

19 PSORIATIC ARTHRITIS
20 PSORIATIC ARTHRITIS About 20% of Pts with Psoriasis develop arthritis. Arthritis can proceed Psoriasis by months to years. Uveitis and positive ANA in 30-50% of Pts. DIP involvement can occur.
21 PSORIATIC ARTHRITIS Almost all these Pts will require Methotrexate. Many will require biologics. Topical Steroids are safe but be careful with systemic steroids. Systemic Steroids can induce erythroderma.

22 PSORIATIC ARTHRITIS
23 ENTHESITIS-RELATED ARTHRITIS Presence or history of SI joint tenderness and /or inflammatory lumbosacral pain HLA B27 Antigen Positive Male >6 years of age Associated Uveitis 1 st Degree relative with Ankylosing Spondylitis, Enthesitis-Related Arthropathy, SI with IBD, or Reactive Arthritis
24 ENTHESITIS-RELATED ARTHRITIS 25% of Enthesitis Related Arthritis Pts are HLA-B27 Negative Most People with HAL-B27 Antigen do NOT have Enthesitis-Related Arthritis Older, male children Familial 10-20% of the time Worse after rest Peripheral Arthritis Sacroiliac Pain

25 ENTHESITIS-RELATED ARTHRITIS

26 ENTHESITIS-RELATED ARTHROPATHIES

27 ENTHESITIS-RELATED ARTHROPATHIES
28 ENTHESITIS-RELATED ARTHROPATHIES Peripheral arthritis will respond to NSAIDs, Steroids, DMRDs. Axial Symptoms typically axial symptoms require biologic. Increased activity and PT is critical
29 UNDIFFERENTIATED JIA ARTHRITIS ASSOCIATED WITH INFLAMMATORY BOWEL DISEASE REACTIVE ARTHRITIS
30 ARTHRITIS ASSOCIATED WITH INFLAMMATORY BOWEL DISEASE 25% of Pts with IBD PERIPHERAL ARTHRITIS AXIAL ARTHRITIS
31 PERIPHERAL IBD ARTHRITIS Arthritis flares are correlated with GI flares M=F NOT ASSOCIATED WITH HLA-B27
32 AXIAL IBD ARTHRITIS Spine, hips, SI joints M>>F ASSOCIATED WITH HLA-B27 Independent of GI flares
33 REACTIVE ARTHRITIS Associated with GI or GU infections Yersinia, Shigella, Salmonella, Campylobacter Chlamydia or Mycoplasma May be associated with oral and genital ulcers, and popular skinlesions. Enthesitis and dactylitis Large weight bearing joints Treat active infection Start with NSAIDs, may require Methotrexate, sulfasalazine or biologics
34 SYSTEMIC JIA (STILL S DISEASE) Not truly a JIA but more closely related to recurrent fever syndromes Autoinflammatory (Intrinsic Immune System) vs Autoimmune (Adaptive Immune System) M=F Peak Age 5-10 years old Fever is always present and usually quotidian Toxic appearing during fever but can appear normal when afebrile
35 SYSTEMIC JIA (STILL S DISEASE) Migratory rash, often with the fever Macular, pink to salmon color May be pruritic Koebner s Phenomenon

36 SYSTEMIC JIA (STILL S DISEASE)
37 SYSTEMIC JIA (STILL S DISEASE) Synovitis-may be delayed for weeks or months Myalgia-CPK usually normal but aldolase can be elevated Pericarditis and myocarditis Serositis Lymphadenopathy Hepatosplenomegaly Abdominal Pain Weight loss and fatigue
38 SYSTEMIC JIA (STILL S DISEASE) WBC typically high 10s to 40 or 50K PLTs typically 400K or higher Normocytic, normochromic anemia Elevated Ferritin Elevated CRP and ESR
39 SYSTEMIC JIA (STILL S DISEASE) Diagnosis of exclusion R/O Infectious Processes R/O Leukemia/Lymphoma (Peripheral Smear, LDH, UA) R/O Kawasaki s Dz
40 SYSTEMIC JIA (STILL S DISEASE) Treatment includes NSAIDs, Steroids, Methotrexate Does not respond well to TNF antagonists Responds well to IL-1 (Anakinra, Ilaris) and IL-6 Antagonist (Actemra) Risk of progressing to Macrophage Activation Syndrome which can be fatal
41 MACROPHAGE ACTIVATION SYNDROME (MAS) A progressive inflammatory response in which the inhibitors of inflammation are not adequately controlling the inflammatory system. Leads to depletion to NK Cell and a Cytokine Storm Very similar to Hemophagocytic Lymphocytic Histiocytosis (HLH) HLH is a genetic defect in counter inflammatory regulators-typically occurs in younger Pts and usually requires Bone Marrow Transplant for cure
42 MACROPHAGE ACTIVATION SYNDROME (MAS) Can be caused by infections process - EBV, Rickettsial Dz, Gram negative sepsis Leukemia/Lymphoma Immunodeficiency Rheumatologic Processes-Typically Still s Disease but also Systemic Lupus Erythematosus
43 MACROPHAGE ACTIVATION SYNDROME (MAS) Results in high fever Rash HSM LAD Elevated LFTs DIC ARDS AKI
44 MACROPHAGE ACTIVATION SYNDROME (MAS) Ferritin is typically high, often above 10,000 CRP is high but ESR can be low (secondary to depletion of fibrinogen) Cytopenia of WBCs and PLTs (be wary of a sudden drop of either)
45 MACROPHAGE ACTIVATION SYNDROME (MAS) Treat the underlying cause Steroids Methotrexate IL-1 Inhibitor Anakinra

46 SYSTEMIC LUPUS ERYTHEMATOSIS
47 SYSTEMIC LUPUS ERYTHEMATOSIS A chronic inflammatory disease affecting the skin, kidneys, lungs, nervous system, serous membranes and other organs. Involves excessive activation of the Innate Immune System. Involves excessive activation of the adaptive immune system including both the humoral and cell mediated pathways.
48 SYSTEMIC LUPUS ERYTHEMATOSIS Clear Genetic Component- concordance rate of 14-57% in monozygotic twins. Hormonal Factors Prepubertal F: M ratio 3.1 while post puberty that Ratio increases to 7-15:1 X Chromosome Factors- XXY (Klinefelter s) 14 fold increase XO (Turner s) significantly lower rate
49 SYSTEMIC LUPUS ERYTHEMATOSIS Infectious Triggers EBV and CMV most notable UV light exposure
50 SYSTEMIC LUPUS ERYTHEMATOSIS Much more common in Americans of Asian, African, or Hispanic Descent Overall Prevalence is 1-2/1, % Diagnosed before the age of 18
51 SYSTEMIC LUPUS ERYTHEMATOSIS HEMATOLOGIC Anemia Chronic Inflammation Hemolytic Anemia Thrombocytopenia Leukopenia-especially lymphopenia Coagulopathies
52 SYSTEMIC LUPUS ERYTHEMATOSIS MUCOCUTANEOUS CHANGES Malar Rash Oral Ulcers Nasal Ulcers Photosensitivity Alopecia

53 SYSTEMIC LUPUS ERYTHEMATOSIS

54 SYSTEMIC LUPUS ERYTHEMATOSIS

55 SYSTEMIC LUPUS ERYTHEMATOSIS

56 SYSTEMIC LUPUS ERYTHEMATOSIS
57 SYSTEMIC LUPUS ERYTHEMATOSIS MUSCULOSKELETAL INVOLVEMENT Arthritis Arthralgia Osteopenia
58 SYSTEMIC LUPUS ERYTHEMATOSIS FEVER- If Greater than 38.6 or associated with chills consider infectious until proven otherwise
59 SYSTEMIC LUPUS ERYTHEMATOSIS NEUROLOGIC Depression Headaches Seizures Peripheral Neuropathy
60 SYSTEMIC LUPUS ERYTHEMATOSIS RENAL DISEASE 27 percent of children with SLE Class of Disease based on renal biopsy Class I- VI Class III and IV require aggressive immunosuppression Class V requires Mycophenolate
61 SYSTEMIC LUPUS ERYTHEMATOSIS PULMONARY Pneumonitis Plevritis Pulmonary Hemorrhage Pulmonary HTN Shrinking Lung Syndrome
62 SYSTEMIC LUPUS ERYTHEMATOSIS CARDIAC Pericarditis Valvular Disease Myocarditis Increased Risk for future CAD
63 SYSTEMIC LUPUS ERYTHEMATOSIS EVALUATION: CBC/Peripheral Smear CMP- elevated liver enzymes, Increased BUN/Cr C3 and C4- both decreased in active Dz UA- can see proteinuria, pyuria, hematuria Urine Pr: Cr Ratio Blood Cultures if Febrile
64 SYSTEMIC LUPUS ERYTHEMATOSIS What about an ANA? If ANA positive will need further check with Extractable Nuclear Antigens (ENA) and Anti DS DNA
65 SYSTEMIC LUPUS ERYTHEMATOSIS Anti-DS ANA >97% Specific for SLE Anti-Smith >95 % Specific for SLE Anti-Ro and Anti-Ro associated with Neonatal Lupus as well as congenital heart block
66 SYSTEMIC LUPUS ERYTHEMATOSIS Chest Xray +/- Echo Amylase/Lipase, abdominal imaging if abdominal pain
67 SYSTEMIC LUPUS ERYTHEMATOSIS Steroids Hydroxychloroquine Mycophenolate Methotrexate Tacrolimus Rituximab Cyclophosphamide
68 KAWASAKI DISEASE A vasculitis involving medium sized arteries which if untreated can result in aneurysms of the coronary arteries and early onset myocardial infarction in children or young adults. Associated with fever, nonexudative conjunctivitis, mucositis, rash, edema of the hands and feet and lymphadenopathy
69 KAWASAKI DISEASE Bilateral bulbar conjunctival injection (dry) can also involve anterior uveitis Oral mucous membrane changes including cracked lips, injected pharynx or stawberry tongue Peripheral erythema and/or edema of the hands and feet
70 KAWASAKI DISEASE Polymorphous rash Cervical lymphadenopathy-at least 1.5cm in diameter, usually unilateral

71 KAWASAKI DISEASE

72 KAWASAKI DISEASE

73 KAWASAKI DISEASE
74 KAWASAKI DISEASE CBC-Leukocytosis and thrombocytosis Elevated AST/ALT Elevated CRP and ESR Urinalysis- sterile pyuria. Remember that the source of this is urethral so may miss with catheterized sample. Inflammatory Cells are not neutrophils so leukocyte esterase will be negative
75 KAWASAKI DISEASE Echo Ultrasound
76 KAWASAKI DISEASE IVIG and Aspirin High Dose Solumedrol Remicade
77 JUVENILE DERMATOMYOSITIS An autoimmune disease associate with T-cell infiltration of skeletal muscles and vasculitis Similar to the adult form of Dermatomyositis but JDM does not have an association with increase risk of occult neoplasia Variants include Amyopathic JDM and Polymyositis
78 JUVENILE DERMATOMYOSITIS Typical presentation includes a history increasing proximal weakness Typical Rash including: Heliotropic Rash Shawl Sign V Sign Gottron s Papules Capillary Drop Out

79 JUVENILE DERMATOMYOSITIS

80 JUVENILE DERMATOMYOSITIS

81 JUVENILE DERMATOMYOSITIS
82 JUVENILE DERMATOMYOSITIS Climbing Stairs Getting up from the chair or toilet Combing or fixing their hair Problems swallowing Voice change
83 JUVENILE DERMATOMYOSITIS CPK Aldolase LDH Von Willebrand s level Remember that AST and ALT are also muscle enzymes
84 JUVENILE DERMATOMYOSITIS Treatment includes steroids, methotrexate, IVIG, Mycophenolate Rule of 1/3rds 1/3 Remission without relapse 1/3 with Remission but subsequently relapse 1/3 Improvement in inflammation but never go into remission

85
86 HENOCH-SCHONLEIN PURPURA Also known as Ig A vasculitis Most common vasculitis in childhood Typically occurs in children between 3 and 15 years old Disease in older patients associated with more severe disease and an increased risk of renal disease
87 HENOCH-SCHONLEIN PURPURA Skin Joints GI Tract Kidney Brain

88 HENOCH-SCHONLEIN PURPURA
89 HENOCH-SCHONLEIN PURPURA CBC PT/PTT/INR UA including Urine Pr:Cr Ratio
90 HENOCH-SCHONLEIN PURPURA DDX: Sepsis including meningiococcus and Strep pneumo Rickettsial Disease Coagulopathy Non accidental Trauma Other vasculitis
91 HENOCH-SCHONLEIN PURPURA Treatment: NSAIDs-Consider COX-2 specific or adding PPI Steroids-Risk of relapse if course is too short
92 HENOCH-SCHONLEIN PURPURA Complications: Intussusception Chronic Renal Disease Relapse

93
94 HENOCH-SCHONLEIN PURPURA Uncertain of the diagnosis Severe abdominal pain or significant GI bleeding Debilitating Pain
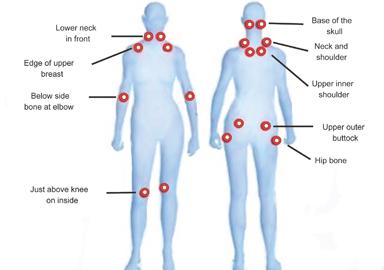
95 FIBROMYALGIA A syndrome of chronic pain associated with poor sleep, cognitive dysfunction, and deconditioning
96 FIBROMYALGIA-ETIOLOGY Not an inflammatory lesion Thought to be related to a central processing disorder Related to sleep disturbances Some evidence of small fiber disorder
97 FIBROMYALGIA-ETIOLOGY Functional scans show completely different brain activity response in those with FM and those without in response to both painful and non painful stimuli Increased sensitivity to non painful stimuli Increased Substance P in CSF Evidence of derangement in endogenous opioid response
98 FIBROMYALGIA-ETIOLOGY Skin biopsies show decreased numbers of small nerve fibers

99
100

101
102 FIBROMYALGIA Not an inflammatory disease Most likely a neuropathic disease involving both CNS and PNS Genetic Predisposition Clearly associated with environmental factors
103 EPIDEMIOLGY Worldwide the prevalence is felt to be between % Increases in frequency in age-approx 4% in older patients Prevalence 1% In Pediatric Patients Prevalence is consistent regardless of economic status of the country Prevalence can ranges between 20-40% of primary care patients Can be seen in 20-40% of Pts with RA, SLE Secondary Fibromyalgia Rate also increased with other chronic diseases CKD, CHF, COPD
104 HX Length of time with symptom Disturbed sleep pattern Altered mental state- FIBRO FOG Fatigue Absence of joint swelling- sometimes subjective swelling Absence of Fever
105 PE Absence of joint effuisions May have some enthesitis Poor posture Lack of dermatological findings Normal neurological exam except for subtle sensory findings
106 LAB No set of universal labs A reasonable approach CBC CMP TSH ESR/CRP CPK Celiac Disease
107 FIBROMYALGIA TX EDUCATION RECONDITIONING/EXERCISE PHARMACOLOGICAL
108 EDUCATION Call it like your see it Diagnosis is often relieving May be cost effective You have to have buy in to be successful
109 EXERCISE/RECONDITIONING Aerobic exercise most effective although strength training may help Start graduated and progressive program
110 SLEEP HYGIENE Same sleep/wake time Use an hour wind down time Repeat 20 minutes of wind down time if unable to go sleep If Pt has a bad night go ahead and get up at regular time May nap- no longer than 1 hour Avoid non sex or sleep activities in the bedroom
111 MEDICATIONS-What doesn t work Steroids Opioids** NSAIDs
112 MEDICATIONS what does work Nortriptyline/Amitriptyline-helps the pain, also can improve sleep Duloxetine* Pregabalin* Milnacipran* Cyclobenzaprine SSRIs +/- TCAs Tramadol * Approved by the FDA for the treatment of Fibromyalgia
113 ALTERNATIVE THERAPIES None proven in large studies Some small studies have shown improvement with Tai Chi, Stretching, chiropractic Acupuncture has been disappointing IF not harmful encourage Pt to try
114 FOLLOW UP Need to follow closely as relapse is common if Pts do not continue lifestyle changes Trigger point pain is not consistent in determining response Use severity scores, sleep quality, quality of life to determine response May be able to wean pharmacological interventions
115 WHEN TO REFER Dx and treatment is clearly in the realm of Primary Care Provider Unclear Diagnoses Complicated medication regimen Often times a single consult with return to PCP can be valuable
116 QUESTIONS????
Juvenile Idiopathic Arthritis (JIA)
") Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
JuvenileIdiopathicArthritis. Dr Johan Siebert
 JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
Department of Paediatrics Clinical Guideline. Guideline for the child with possible arthritis (joint swelling/pain, loss of function)
") Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Department of Paediatrics Clinical Guideline
 Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS LUPUS 101 SLE SUBSETS AUTOIMMUNE DISEASE 11/4/2013 HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS
 LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
Kawasaki Disease. 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD. Children s Specialty Group. All rights reserved.
 Kawasaki Disease 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD Disclosures We have no relevant financial relationships to disclose. Objectives Describe the characteristic signs and symptoms of Kawasaki
Kawasaki Disease 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD Disclosures We have no relevant financial relationships to disclose. Objectives Describe the characteristic signs and symptoms of Kawasaki
Rheumatology 101 A Pediatrician s Guide
 Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Definition Chronic autoimmune disease The body s immune system starts attacking itself Can affect most organs and tissues in the body Brain, lungs, he
 LIVING WITH SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. Rowan Diagnostic Clinic Salisbury, N.C. May 11, 2013 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement
LIVING WITH SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. Rowan Diagnostic Clinic Salisbury, N.C. May 11, 2013 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
FIBROMYALGIA ANNE WINKLER MD PHD MO ACP MEETING SEPT 2016
 FIBROMYALGIA ANNE WINKLER MD PHD MO ACP MEETING SEPT 2016 DEFINITION CHRONIC MUSCILOSKELETAL DISORDER CHARACTERIZED BY GENERALIZED PAIN AND TENDERNESS AT SPECIFIC ANATOMIC SITES. CRITERIA DEFINED IN 1990
FIBROMYALGIA ANNE WINKLER MD PHD MO ACP MEETING SEPT 2016 DEFINITION CHRONIC MUSCILOSKELETAL DISORDER CHARACTERIZED BY GENERALIZED PAIN AND TENDERNESS AT SPECIFIC ANATOMIC SITES. CRITERIA DEFINED IN 1990
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
8/29/2012. Outline Juvenile idiopathic arthritis. 1. Classification-ILAR. 1. Classification-clinical diagnosis. 1. JIA classification
 Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS
 UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. October 20, 2012 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement Diagnosis Treatment Pregnancy
UNDERSTANDING SYSTEMIC LUPUS ERYTHEMATOSUS Stacy Kennedy, M.D.,M.B.A. October 20, 2012 Agenda What is lupus Who is affected Causes of lupus Symptoms and organ involvement Diagnosis Treatment Pregnancy
Pediatric Rheumatology: A Case-based Approach to the Basics. Hilary M. Haftel, MD, MHPE University of Michigan Department of Pediatrics
 Pediatric Rheumatology: A Case-based Approach to the Basics Hilary M. Haftel, MD, MHPE University of Michigan Department of Pediatrics Disclosures I have no relevant financial relationships with the manufacturer(s)
Pediatric Rheumatology: A Case-based Approach to the Basics Hilary M. Haftel, MD, MHPE University of Michigan Department of Pediatrics Disclosures I have no relevant financial relationships with the manufacturer(s)
PGALS: Approach to Child with Arthritis. Prof Chris Scott Paediatric Rheumatology
 PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis
 Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
9/25/2013 SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)
") SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
Jeopardy. What s the rash? $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400
 Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
.,Dr Ali Alkazzaz Babylon collage of medicine 2016
 .,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
.,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
Pyrexia of unknown origin? Think still
 Pyrexia of unknown origin? Think still Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. DISCLAIMER
Pyrexia of unknown origin? Think still Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. DISCLAIMER
JIA and Other Rheumatic Diseases in Children. Norma Liburd, RN-BC, MN
 JIA and Other Rheumatic Diseases in Children Norma Liburd, RN-BC, MN Define Juvenile Idiopathic Arthritis (JIA) and discuss the diagnostic criteria. Objectives Identify the subtypes of JIA and discuss
JIA and Other Rheumatic Diseases in Children Norma Liburd, RN-BC, MN Define Juvenile Idiopathic Arthritis (JIA) and discuss the diagnostic criteria. Objectives Identify the subtypes of JIA and discuss
Juvenile Chronic Arthritis
 Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Insights into the DX of Pediatric SLE
 Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
Insights into the DX of Pediatric SLE Dr. John H. Yost Pediatric Rheumatology Children s Hospital at Dartmouth Assistant Professor of Medicine Geisel School of Medicine at Dartmouth john.h.yost@hitchcock.org
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
Rheumatology Primer: What Labs and When
 Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
 www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
Living with Lupus: An Insider s Perspective
 Living with Lupus: An Insider s Perspective Pamela Thorpe, MD, FACP Lupus Foundation of America, Inc. Philadelphia Tri-State Chapter Volunteer May 2014 My Own Story Is it Lupus Yet? The What What is this?
Living with Lupus: An Insider s Perspective Pamela Thorpe, MD, FACP Lupus Foundation of America, Inc. Philadelphia Tri-State Chapter Volunteer May 2014 My Own Story Is it Lupus Yet? The What What is this?
10/25/2018. Autoimmunity and how to treat it. Disclosure. Why do we get autoimmunity? James Verbsky MD/PhD Pediatric Rheumatology/Immunology
 Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
A CRP B FBC C LFT D blood culture E uric acid
 1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Lupus. Fast facts. What is lupus? What causes lupus? Who gets lupus?
 Lupus Systemic lupus erythematosus, referred to as SLE or lupus, is sometimes called the "great imitator." Why? Because of its wide range of symptoms, people often confuse lupus with other health problems.
Lupus Systemic lupus erythematosus, referred to as SLE or lupus, is sometimes called the "great imitator." Why? Because of its wide range of symptoms, people often confuse lupus with other health problems.
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care. Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018
 Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Nausheen Khuddus, MD Melissa Elder, MD, PhD
 Nausheen Khuddus, MD Melissa Elder, MD, PhD Nausheen Khuddus, MD Pediatric Ophthalmologist and Strabismus Specialist Accent Physicians Gainesville, Florida What Is Uveitis? Uveitis is caused by inflammatory
Nausheen Khuddus, MD Melissa Elder, MD, PhD Nausheen Khuddus, MD Pediatric Ophthalmologist and Strabismus Specialist Accent Physicians Gainesville, Florida What Is Uveitis? Uveitis is caused by inflammatory
Pediatric Rheumatology Board Review
 Pediatric Rheumatology Board Review Simona Nativ, MD Pediatric Rheumatology Goryeb Children s Hospital Question #1 A 2 year old male (pictured at left) presents with his mother who complains that his left
Pediatric Rheumatology Board Review Simona Nativ, MD Pediatric Rheumatology Goryeb Children s Hospital Question #1 A 2 year old male (pictured at left) presents with his mother who complains that his left
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R
 The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
MANAGING THE PATIENT WITH POSITIVE ANA
 MANAGING THE PATIENT WITH POSITIVE ANA Rafael F. Rivas-Chacon, M.D. Disclosures Grant/Research support for: Pfizer Study JIA A3921104 Tofacitinib not related to this presentation 1 Positive Antinuclear
MANAGING THE PATIENT WITH POSITIVE ANA Rafael F. Rivas-Chacon, M.D. Disclosures Grant/Research support for: Pfizer Study JIA A3921104 Tofacitinib not related to this presentation 1 Positive Antinuclear
Treatment modalities Prof Ally 2012
 Treatment modalities Prof Ally 2012 Analgesia Types of Pain Nociceptive /neuropathic nociceptive Tissue damage - trauma, inflammation Somatic (musculoskeletal): local pain referred pain Neuropathic pain:
Treatment modalities Prof Ally 2012 Analgesia Types of Pain Nociceptive /neuropathic nociceptive Tissue damage - trauma, inflammation Somatic (musculoskeletal): local pain referred pain Neuropathic pain:
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Rheum-inations For the physical therapist
 Rheum-inations For the physical therapist All you wanted to know about rheumatology and more! Susan Shenoi MD, MS, RhMsUS Assistant Professor Clinical Director Seattle Children s Hospital 10-2017 Objectives
Rheum-inations For the physical therapist All you wanted to know about rheumatology and more! Susan Shenoi MD, MS, RhMsUS Assistant Professor Clinical Director Seattle Children s Hospital 10-2017 Objectives
Undifferentiated Connective Tissue Disease and Overlap Syndromes. Mark S. Box, MD
 Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Mary Derlacki, FNP. No financial relationships to disclose. Office Rheumatology for the Nurse Practitioner. Rheumatoid Arthritis
 Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
DISCUSSION BY: Dr M. R. Shakeebi, MD, Rheumatologist
 Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
9/13/2015. Nothing to disclose
 Jared Bozeman Kathleen Luskin MD Bipin Thapa MD Medical College of Wisconsin Milwaukee, Wisconsin Nothing to disclose 24 Year old previously healthy woman presenting from OSH Fatigue Weakness Neck swelling
Jared Bozeman Kathleen Luskin MD Bipin Thapa MD Medical College of Wisconsin Milwaukee, Wisconsin Nothing to disclose 24 Year old previously healthy woman presenting from OSH Fatigue Weakness Neck swelling
Learning about Lupus. Learning About Lupus. Lupus Society of Illinois
 Learning About Lupus Learning about Lupus Lupus Society of Illinois 525 W. Monroe Street, Suite 900 Chicago, Illinois 60661 Robert S. Katz, M.D. Professor of Medicine Rush University Medical Center Northwestern
Learning About Lupus Learning about Lupus Lupus Society of Illinois 525 W. Monroe Street, Suite 900 Chicago, Illinois 60661 Robert S. Katz, M.D. Professor of Medicine Rush University Medical Center Northwestern
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS
 Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients
Arthritis & Rheumatology Clinics of Kansas PATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients
SLE-key Case Studies
 SLE-key Case Studies Ellen M. Field, M.D. Lehigh Valley Health Network, Bethlehem, PA Donald E. Thomas, Jr., M.D., FACP, FACR, RhMSUS, CCD Arthritis and Pain Assoc. of PG County, Greenbelt, MD Case Study
SLE-key Case Studies Ellen M. Field, M.D. Lehigh Valley Health Network, Bethlehem, PA Donald E. Thomas, Jr., M.D., FACP, FACR, RhMSUS, CCD Arthritis and Pain Assoc. of PG County, Greenbelt, MD Case Study
Inflammatory Myopathies 4 th year MBBS. Marwan Adwan MBChB, MSc, MRCPI, MRCP(rheum) Consultant Rheumatologist
 Consultant Rheumatologist") Inflammatory Myopathies 4 th year MBBS Marwan Adwan MBChB, MSc, MRCPI, MRCP(rheum) Consultant Rheumatologist Case A 64 woman presents with erythematous itchy rash over back of hands & forehead. For 1 month
Inflammatory Myopathies 4 th year MBBS Marwan Adwan MBChB, MSc, MRCPI, MRCP(rheum) Consultant Rheumatologist Case A 64 woman presents with erythematous itchy rash over back of hands & forehead. For 1 month
Rayos Prior Authorization Program Summary
 Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
Case Presentation. By Eman El Sharkawy Ass. Professor of cardiology Alexandria University
 Case Presentation By Eman El Sharkawy Ass. Professor of cardiology Alexandria University 6m old baby girl Past history : - At the age of 2m attack of fever, diarrhea, mouth ulcers, difficult breast feeding
Case Presentation By Eman El Sharkawy Ass. Professor of cardiology Alexandria University 6m old baby girl Past history : - At the age of 2m attack of fever, diarrhea, mouth ulcers, difficult breast feeding
Rheumatoid Arthritis. Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011
 Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition
 Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Autoimmune diseases. SLIDE 3: Introduction to autoimmune diseases Chronic
 SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
SLIDE 3: Introduction to autoimmune diseases Chronic Autoimmune diseases Sometimes relapsing : and remitting. which means that they present as attacks Progressive damage Epitope spreading more and more
Clinical Guidance. Kawasaki disease. Summary This guideline includes therapy and follow up including investigations (echocardiography, MRI).
.") Clinical Guidance Kawasaki disease Summary This guideline includes therapy and follow up including investigations (echocardiography, MRI). Document Detail Document type Clinical Guideline Document name
Clinical Guidance Kawasaki disease Summary This guideline includes therapy and follow up including investigations (echocardiography, MRI). Document Detail Document type Clinical Guideline Document name
LUPUS (SLE) MEDICAL SOURCE STATEMENT
 MEDICAL SOURCE STATEMENT") LUPUS (SLE) MEDICAL SOURCE STATEMENT From: Re: (Name of Patient) (Social Security No.) Please answer the following questions concerning your patient s impairments. Attach relevant treatment notes, radiologist
LUPUS (SLE) MEDICAL SOURCE STATEMENT From: Re: (Name of Patient) (Social Security No.) Please answer the following questions concerning your patient s impairments. Attach relevant treatment notes, radiologist
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z
 from Harvard Medical School Health Topics A-Z") Topic Page: Systemic Lupus Erythematosus Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z What Is It? Lupus is thought to develop when the immune system
Topic Page: Systemic Lupus Erythematosus Summary Article: Lupus (Systemic Lupus Erythematosus) from Harvard Medical School Health Topics A-Z What Is It? Lupus is thought to develop when the immune system
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Systemic examination
 PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
SLE and the Antiphospholipid Syndrome
 SLE and the Antiphospholipid Syndrome Susan Y. Ritter MD, PhD Associate Physician Division of Rheumatology, Immunology and Allergy Department of Medicine Brigham and Women s Hospital Instructor in Medicine
SLE and the Antiphospholipid Syndrome Susan Y. Ritter MD, PhD Associate Physician Division of Rheumatology, Immunology and Allergy Department of Medicine Brigham and Women s Hospital Instructor in Medicine
Kawasaki Disease: What you need to know from the 2017 Guidelines
 Kawasaki Disease: What you need to know from the 2017 Guidelines S. Kristen Sexson Tejtel, MD, PhD, MPH Pediatric Preventive Cardiology TCHAPP Conference April 4, 2019 No disclosures to report Outline
Kawasaki Disease: What you need to know from the 2017 Guidelines S. Kristen Sexson Tejtel, MD, PhD, MPH Pediatric Preventive Cardiology TCHAPP Conference April 4, 2019 No disclosures to report Outline
Idiopathic inflammatory muscle diseases. Dr. Paul Etau Ekwom MBChB, MMED Kenyatta National Hospital, Nairobi-Kenya
 Idiopathic inflammatory muscle diseases. Dr. Paul Etau Ekwom MBChB, MMED Kenyatta National Hospital, Nairobi-Kenya I.W, 28 YRS, FEMALE SHOP STEWARD Referred to KNH on 16/06/09 from Thika Nursing Home Weakness
Idiopathic inflammatory muscle diseases. Dr. Paul Etau Ekwom MBChB, MMED Kenyatta National Hospital, Nairobi-Kenya I.W, 28 YRS, FEMALE SHOP STEWARD Referred to KNH on 16/06/09 from Thika Nursing Home Weakness
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abatacept, for rheumatoid arthritis, 789 Acetaminophen, for low back pain, 735 Acupuncture for fibromyalgia, 753 for low back pain, 738
Index Note: Page numbers of article titles are in boldface type. A Abatacept, for rheumatoid arthritis, 789 Acetaminophen, for low back pain, 735 Acupuncture for fibromyalgia, 753 for low back pain, 738
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Rheumatology Cases for the Internist
 Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Benlysta (belimumab) Prior Authorization Criteria Program Summary
 Prior Authorization Criteria Program Summary") Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
DEPARTMENT OF RHEUMATOLOGY
 DEPARTMENT OF RHEUMATOLOGY PG Teaching Schedule Theory (8 30 am to 9am) DATE TOPIC PRESENTER FACULTY 01/10/16 Approach to Arthritis Dr. Sandeep Dr. Suma Balan 03/10/16 Cardiovascular risk in Rheumatic
DEPARTMENT OF RHEUMATOLOGY PG Teaching Schedule Theory (8 30 am to 9am) DATE TOPIC PRESENTER FACULTY 01/10/16 Approach to Arthritis Dr. Sandeep Dr. Suma Balan 03/10/16 Cardiovascular risk in Rheumatic
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
CONTENT OUTLINE. Pediatric Rheumatology
 THE AMERICAN BOARD OF PEDIATRICS CONTENT OUTLINE Pediatric Rheumatology Subspecialty In-Training, Certification, and Maintenance of Certification (MOC) Examinations INTRODUCTION This document was prepared
THE AMERICAN BOARD OF PEDIATRICS CONTENT OUTLINE Pediatric Rheumatology Subspecialty In-Training, Certification, and Maintenance of Certification (MOC) Examinations INTRODUCTION This document was prepared
What prescribers need to know
 HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
Systemic Lupus Erythematosus
 A Patient s Guide to Systemic Lupus Erythematosus 2 kidneys. These changes make it impossible for the kidneys to function normally. The inflammation of SLE can be seen in the lining, covering, and muscles
A Patient s Guide to Systemic Lupus Erythematosus 2 kidneys. These changes make it impossible for the kidneys to function normally. The inflammation of SLE can be seen in the lining, covering, and muscles
Autoimmunity and autoinflammation
 Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
Drugs and Applicable Coding: J-code: Enbrel-J1438; Humira-J0135; Remicade-J1745; Inflectra-Q5102; Cimzia-J0718; Simponi-J1602 Renflexis - pending
 Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Autoimmune Disease. Autoimmunity. Epidemiology. ACR Criteria for Diagnosis. Signs and Symptoms. Autoreactivity: Reactivity to self antigens:
 Autoimmunity Reactivity to self antigens: Autoreactivity: Autoimmune Disease T cells B cells Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection Epidemiology SLE Pathogenesis
Autoimmunity Reactivity to self antigens: Autoreactivity: Autoimmune Disease T cells B cells Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection Epidemiology SLE Pathogenesis
L. Nandini Moorthy, MD MS 2012
 L. Nandini Moorthy, MD MS 2012 L Nandini Moorthy, MD MS 09 17 yo Ashkenazi male with proximal muscle pain and weakness, mild malar erythema and erythema over knees and dorsal aspect of PIPs Mild tenderness
L. Nandini Moorthy, MD MS 2012 L Nandini Moorthy, MD MS 09 17 yo Ashkenazi male with proximal muscle pain and weakness, mild malar erythema and erythema over knees and dorsal aspect of PIPs Mild tenderness
Autoimmunity. Autoimmune Disease
 Autoimmunity Reactivity to self antigens: T cells B cells Autoimmune Disease Autoreactivity: Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection 1 SLE Pathogenesis Immune
Autoimmunity Reactivity to self antigens: T cells B cells Autoimmune Disease Autoreactivity: Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection 1 SLE Pathogenesis Immune
Conflict of Interest. Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital.
 Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital Conflict of Interest Disclosures: None Overview Diagnostic Classification Criteria of SLE
Systemic Lupus Erythematosus and the Antiphospholipid Syndrome Bonnie L. Bermas, MD Brigham and Women s Hospital Conflict of Interest Disclosures: None Overview Diagnostic Classification Criteria of SLE
Rheumatoid arthritis
 Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
13. Behçet s - In Children
 Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk 13. Behçet s - In Children How are children affected by Behçet s disease? Behçet s disease (also
Registered Charity No: 326679 Caring for those with a rare, complex and lifelong disease www.behcets.org.uk 13. Behçet s - In Children How are children affected by Behçet s disease? Behçet s disease (also
By Your Sis: Ghada Odeh :)
") By Your Sis: Ghada Odeh :) Hx: Chest pain ACS. Hx.: Cough Bronchiectasis. Hx: Epigastric pain Peptic ulcer disease. Hx: Joints Pain SLE. Hx: Hematurea post-strep Glomerulonephritis. Hx: Jaundice Chronic
By Your Sis: Ghada Odeh :) Hx: Chest pain ACS. Hx.: Cough Bronchiectasis. Hx: Epigastric pain Peptic ulcer disease. Hx: Joints Pain SLE. Hx: Hematurea post-strep Glomerulonephritis. Hx: Jaundice Chronic
Update on Enthesitis-Related Arthritis, a Subtype of Juvenile Idiopathic Arthritis
 Hong Kong Bull Rheum Dis 2010;10:15-19 Review Article Update on Enthesitis-Related Arthritis, a Subtype of Juvenile Idiopathic Arthritis Tsz-Leung Lee Abstract: Keywords: Enthesitis related arthritis (ERA)
Hong Kong Bull Rheum Dis 2010;10:15-19 Review Article Update on Enthesitis-Related Arthritis, a Subtype of Juvenile Idiopathic Arthritis Tsz-Leung Lee Abstract: Keywords: Enthesitis related arthritis (ERA)
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
IMACS FORM 07b: MYOSITIS DISEASE ACTIVITY ASSESSMENT TOOL, Version
 IMACS FORM 07b: MYOSITIS ASSESSMENT TOOL, Version 2 2005 Subject s IMACS number: ASSESSOR: Date Assessed: Assessment number: The clinical features recorded are based upon the previous 4 weeks and the judgment
IMACS FORM 07b: MYOSITIS ASSESSMENT TOOL, Version 2 2005 Subject s IMACS number: ASSESSOR: Date Assessed: Assessment number: The clinical features recorded are based upon the previous 4 weeks and the judgment
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Manifestations and Presentations of Collagen Vascular Diseases. Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL
 Manifestations and Presentations of Collagen Vascular Diseases Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL June 29, 2018 Disclosures Joseph LaConti, M.D., Ph.D., has
Manifestations and Presentations of Collagen Vascular Diseases Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL June 29, 2018 Disclosures Joseph LaConti, M.D., Ph.D., has
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
THE MANAGEMENT OF JUVENILE IDIOPATHIC ARTHRITIS
 THE MANAGEMENT OF JUVENILE IDIOPATHIC ARTHRITIS Prof Chris Scott PAEDIATRIC RHEUMATOLOGIST UNIVERSITY OF CAPE TOWN RED CROSS WAR MEMORIAL CHILDRENS S HOSPITAL Chronic Arthritis >6wks JIA No other cause
THE MANAGEMENT OF JUVENILE IDIOPATHIC ARTHRITIS Prof Chris Scott PAEDIATRIC RHEUMATOLOGIST UNIVERSITY OF CAPE TOWN RED CROSS WAR MEMORIAL CHILDRENS S HOSPITAL Chronic Arthritis >6wks JIA No other cause
CME for Family Medicine Specialists. Evelyn Sutton, MD, FRCPC, FACP November 17, 2018
 CME for Family Medicine Specialists Evelyn Sutton, MD, FRCPC, FACP November 17, 2018 Disclosures Received $ from Advisory Board Consultant: Amgen, Abvie, Pfizer, Actelion, Lilly, Grants: Arthritis Society,
CME for Family Medicine Specialists Evelyn Sutton, MD, FRCPC, FACP November 17, 2018 Disclosures Received $ from Advisory Board Consultant: Amgen, Abvie, Pfizer, Actelion, Lilly, Grants: Arthritis Society,
Following the bite of a mosquito infected with CHIKV, most individuals will
 3. CLINICAL 3A. Clinical Presentation of Acute Disease Following the bite of a mosquito infected with CHIKV, most individuals will present with symptomatic disease after an incubation period of 3-7 days
3. CLINICAL 3A. Clinical Presentation of Acute Disease Following the bite of a mosquito infected with CHIKV, most individuals will present with symptomatic disease after an incubation period of 3-7 days