Case Report Pulmonary-Renal Syndrome with Negative ANCAs and Anti-GBM Antibody
|
|
|
- Ashley Chase
- 5 years ago
- Views:
Transcription
1 Case Reports in Nephrology Volume 2013, Article ID , 6 pages Case Report Pulmonary-Renal Syndrome with Negative ANCAs and Anti-GBM Antibody Hiroshi Yamaguchi, 1,2 Atsuhisa Shirakami, 1 Takashi Haku, 3 Takashige Taoka, 3 Yoshikazu Nakanishi, 4 Toru Inai, 4 and Takanori Hirose 5 1 Department of Diabetology and Metabolic Medicine, Tokushima Prefectural Central Hospital, , Kuramoto, Tokushima , Japan 2 Department of Internal Medicine, Tokushima Prefectural Central Hospital, , Kuramoto, Tokushima , Japan 3 Department of Respiratory Medicine, Tokushima Prefectural Central Hospital, , Kuramoto, Tokushima , Japan 4 Department of Urology, Tokushima Prefectural Central Hospital, , Kuramoto, Tokushima , Japan 5 Department of Diagnostic Pathology, Tokushima Prefectural Central Hospital, , Kuramoto, Tokushima , Japan Correspondence should be addressed to Hiroshi Yamaguchi; futuyaso007@yahoo.co.jp Received 4 September 2013; Accepted 25 September 2013 Academic Editors: A. L. de Francisco, S. Lionaki, and H. Schiffl Copyright 2013 Hiroshi Yamaguchi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. We report the case of a 76-year-old woman who was referred to our hospital for a gradually worsening cough and renal dysfunction. Although pneumonia was initially suspected, imaging findings of the lungs revealed diffuse alveolar hemorrhage at a later date. Renal failure developed and hemodiafiltration was performed on the 9th day. Rapidly progressive glomerulonephritis with crescent formation was diagnosed by renal biopsy. This case presentation has important clinical implications because uncategorizable pulmonary-renal syndrome (PRS) without the presence of ANCAs and anti-gbm antibody is extremely rare and has high rates of morbidity and mortality. No treatment has been established. 1. Introduction Pulmonary renal-syndrome (PRS), characterized by a combination of diffuse alveolar hemorrhage (DAH) and rapidly progressive glomerulonephritis (RPGN), is caused by varied etiologies, including Goodpasture s syndrome, antineutrophil cytoplasmic antibody (ANCA)-associated small vessel vasculitis (ASVV), cryoglobulinemia, systemic lupus erythematosus, environmental factors, and certain drugs [1, 2]. ASSV, which can be caused by microscopic polyangiitis (MPA), Wegener s granulomatosis, and Churg-Strauss syndrome,accountsforapproximately70%ofthecasesofprs. Antiproteinase-3 (anti-pr3, c-anca) and antimyeloperoxidase (anti-mpo, p-anca) antibodies, which have been reported to play a major role in the pathogenesis of ASSV, are detectable in 70 90% of cases and facilitate diagnosis. Our present patient could not be classified into known subgroups because all commercially available serologic studies were negative. Therefore, a renal biopsy was performed for diagnostic clues at a later date. As a result, PRS was diagnosed on the basis of clinical manifestations and pathological findings. 2. Case Report A 76-year-old Japanese woman presented to our hospital complaining of a worsening cough of 10-day duration. Her past medical history included hypertension since age 70. Her activities of daily living had been independent before admission. On admission, her vital signs were as follows: body temperature, 35.3 C; heart rate, 86 beats/min; SpO 2, 96% (on room air); respiratory rate, 14 breaths/min; and blood pressure, 161/78 mmhg. No skin lesions or peripheral neuropathy were noted. A laboratory examination revealed leukocytosis (white blood cell count [WBC]: 11,900/mm), normocytic normochromic anemia (Hb: 6.1 g/dl), elevation of C-reactive
2 2 Case Reports in Nephrology Hemosputum On a ventilator Off a ventilator Renal biopsy (64th day) HDF Maintenance HD mpsl 500 mg 250 mg 125 mg CTRX 1.0 g 2 PZFX 500 mg AZM SR 2.0 g MCFG 150 mg MEPM 0.5 g VCM PSL 60 mg 50 mg 40 mg 35 mg 30 mg 1.0 g 25 mg 20 mg (day) 1st 7th 9th 31st 74th 119th S-Cr (mg/dl) P-ANCA (U/mL) <1.0 C-ANCA (U/mL) <3.5 <3.5 <1.0 <1.0 Anti-GBM (EU) <10 <10 <10 Figure 1: The patient s clinical course. protein (CRP) level (6.1 mg/dl), and renal dysfunction (BUN: 42.6 mg/dl, Cr: 4.04 mg/dl). Urinalysis showed the following results: proteinuria 3+ (1.48 g/day) and hematuria 3+. The red cell counts in the urinary sediment were elevated (388 per high-power field). Serological tests for MPO- ANCA, PR3-ANCA, and anti-gbm antibodies were performed using enzyme-linked immunosorbent assay (ELISA). Antineutrophil cytoplasm antibodies against myeloperoxidase (MPO-ANCA) and antibodies against proteinase 3 (PR3-ANCA) and antiglomerular basement membrane (anti- GBM) antibodies were not identified, although these assays were performed several times during the clinical course (Figure 1). Testing for hepatitis B and C viruses, and antinuclear antibody titer was negative. The complement levels were normal. ChestX-rayandthoraciccomputedtomography(CT) scan revealed patchy alveolar infiltrates throughout the upper andlowerzonesinbothlungs(figures2(a) and 2(b)). An electrocardiogram showed normal sinus rhythm. Echocardiography revealed a normal ejection fraction of 60%, normal right-ventricular size, no evidence of a pericardial effusion, and no findings that were consistent with pulmonary edema. Abdominal ultrasound showed bilateral normal-sized kidneys with increased echogenicity. Pneumonia was suspected on admission and several antibiotics were initiated based on an increase in inflammatory reaction including WBC and CRP levels. However, as alveolar patchy infiltrates gradually expanded after admission (Figures 2(c), 2(d), and 2(e)) and she expectorated bloody sputum on the 3rd day, we evaluated these antibiotic drugs as ineffective and she was treated with a blood transfusion because of worsening of anemia. To determine the causative organism, culture tests were performed for sputum culture five times and blood culture three times over the course of hospitalization; however, no bacterial species causing pneumonia were detected. Serological tests for Cytomegalovirus, Mycoplasma, and fungus were also negative. No infectious explanation for these imaging findings was found. On the 10th day, as the oxygen saturation fell to 82% despite the administration of oxygen (10 liters per minute) by face mask, she was moved to the intensive care unit (ICU) and the trachea was intubated and mechanical ventilation was begun. Her renal function worsened with serum creatinine increasing steadily from 4.04 mg/dl on admission to a peak of 5.76 mg/dl on the 9th day. Rapidly progressive glomerulonephritis (RPGN) was diagnosed by urinary findings and progressive loss of renal function. As there had been no urine output on the 9th day, a hemodialysis catheter was placed, and hemodiafiltration (HDF) was begun. The findings of chest X-ray and chest CT scan indicated the more specific group of disorders known as diffuse alveolar hemorrhage accompanied by glomerulonephritis. Therefore, the patient was started on 500 mg of methylprednisolone intravenously daily for 3 days under the administration of antibiotics on the 9th day. After that, methylprednisolone wassequentiallyadministeredat250mgdailyfor3daysand 125 mg daily for 3 days, followed by oral prednisolone. The administration of prednisolone was started at 60 mg daily on the 20th day and the prednisolone dose was gradually decreasedto20mgdailyonthe96thday.
 The radiograph obtained after intubation on the 10th day showed increased confluence of the opacities.")
 Chest CT scan on the 10th day showed bilateral ground-glass opacities corresponding to the central and perihilar opacities and both small pleural effusions.")
 Chest X-ray on the 92nd day showed the disappearance of infiltrative shadows in both lung fields.")
).")
, and crescentic glomeruli was 2. The PAS and PAM stain identified sclerotic glomeruli.")

3 Case Reports in Nephrology 3 (a) (c) (f) (b) (d) (e) Figure 2: (a), (b) Chest X-ray and CT on admission showed bilateral central opacities, which are more confluent in the right upper and lower lung zone than elsewhere. There is slight cardiomegaly. (c) The radiograph obtained after intubation on the 10th day showed increased confluence of the opacities. The right hemidiaphragm is partially obscured. (d) Chest CT scan on the 10th day showed bilateral ground-glass opacities corresponding to the central and perihilar opacities and both small pleural effusions. (e) Chest CT scan on the 36th day showed progressed bilateral ground-glass opacities, confluent, and consolidated opacities, and a large quantity of pleural effusions in both lung fields. (f) Chest X-ray on the 92nd day showed the disappearance of infiltrative shadows in both lung fields. We performed a tracheotomy on the 14th day because we expected that she would need prolonged mechanical ventilation, and she was taken off a ventilator on the 30th day. Chest radiograph and chest CT scan showed a bilateral pulmonary infiltrative shadow that improved on the 64th day and disappeared without lung damage on the 92nd day (Figure 2(f)). A kidney biopsy was performed on the 64th day, because her general condition improved and she was able to move to a prone position. The total number of glomeruli was 32, sclerotic glomeruli was 24 (75%), and crescentic glomeruli was 2. The PAS and PAM stain identified sclerotic glomeruli. The linear deposition of IgG was observed in part of the basement membrane by immunofluorescence micrography (see Figure 3). Therefore, although an anti-gbm antibody was not detected in the serum, anti-gbm glomerulonephritis was suspected histopathologically. She was transferred to a nearby hospital to continue rehabilitation and maintenance dialysis on the 96th day. One year after onset, there has been no recurrence of PRS with maintenance dosage of prednisolone 10 mg daily. 3. Discussion The term pulmonary renal syndrome (PRS) is used to describe a combination of diffuse pulmonary hemorrhage and glomerulonephritis occurring as the presenting manifestation of multisystem autoimmune disease [3]. The occurrence of pulmonary renal syndrome, which is a rare and etiologically heterogeneous group of diseases, constitutes a medical emergency associated with a high risk of fatal outcome. The outcome data for PRS remain confined to small studies with limited follow-up. Gallagher et al. previously reported 12 of 14 patients who were initially dialysis dependent and 5 patients (36%) who died in the first months in a single-center retrospective study of 14 consecutive patients for four years [4]. On the other hand, the term Goodpasture s syndrome, which has diverse mechanisms and is used synonymously for PRS, is applied to the combination of lung purpura and nephritis, regardless of the underlying pathogenesis. A useful clinical approach to differential diagnosis involves serologic categorization [5]. When evaluating a patient with a possible pulmonary renal syndrome, ANCA and anti-gbm assays currently play a critical role in the diagnosis and classification of vasculitic syndrome. In 1982, antibodies directed against neutrophil cytoplasmic antigens were first described in patients with pauci-immune glomerulonephritis [6]. In Japan, clinical test items for MPO-ANCA antibody and anti-gbm antibody were listed in health-insurance system in 1998 and 1999, respectively.

 Immunofluorescence microscopy showed slightly bright granular staining for C3 in the mesangium area.")



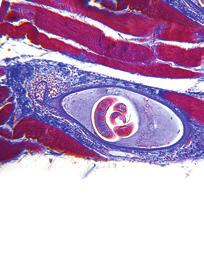
4 4 Case Reports in Nephrology (a) (b) (d) (c) (e) Figure 3: (a), (b), (c) Light-microscopy examination of renal-biopsy specimens showed proliferative-appearing glomeruli with focal formation of cellular and fibrocellular crescents. The GBM was duplicated. Many glomeruli were globally sclerosed, indicating disease chronicity. (A periodic acid Schiff staining, B periodic acid silver-methenamine staining, C Masson s trichrome staining). (d) Immunofluorescence microscopy showed slightly bright granular staining for C3 in the mesangium area. (e) Immunofluorescence microscopy showed weak staining with IgG in a linear pattern in part of the GBM. GBM: glomerular basement membrane. Single-center experience suggests that 60% to 70% of cases of PRS are associated with autoantibodies to ANCAs and 20% are associated with anti-gbm antibodies [7, 8]. In addition, approximately 95% of the patients with ANCA-associated vasculitis have detectable ANCA, whereas circulating anti-gbm antibodies using ELISAs are found in up to 92% of the cases of anti-gbm disease [9]. That is, approximately 90% of the patients with PRS have one or more autoantibodies. Therefore, uncategorizable PRS with no detection of various antibodies in the serum, as in this case, is extremely rare. It has been only recently that minimal outcome data for this severe syndrome have become available in the literature. Only five cases of seronegative PRS, of which two reports are written in Japanese and therefore not cited here, have been reported since 1980 [2, 10, 11]. All reported patients are Asian and had already had severe renal dysfunction (BUN: 82 mg/dl 167 mg/dl, Cr: 5.4 mg/dl 11.9 mg/dl) at the time of admission. To preserve organ function, it is important to make the correct diagnosis and institute adequate therapy early on in the acute phase. However, in the present case, differential diagnosis was difficult and better management for PRS could not be performed before she had progressed to end-stage renal failure, as autoantibodies available at our hospital were all negative in multiple examinations. With regard to therapy for seronegative PRS, no specific therapeutic option that has shown clear benefit has been reported because of the limited numbers of cases. Only two cases that underwent plasma exchange were able to avoid subsequent maintenance dialysis [2]. As it has been described above, although the group of disorders mediated by anti-gbm antibody is one of the less common causes of DAH and nephritis, the prognosis of Goodpasture s syndrome is the worst and the occurrence of anti-gbm antibody with or without other antibodies has been reported to be associated with significantly poor outcome in patients with PRS [12]. In this case, no events to precipitate lung hemorrhage, such as lung infection, were documented and systemic manifestations other than those attributable to uremia or respiratory insufficiency were absent. DAH is an acute, life-threatening event, and the causes and clinical features vary widely. Once the diagnosis of diffuse alveolar hemorrhage is established, the clinician should ascertain whether an underlying cause is present. The diagnosis of DAH was established by dyspnea, cough, hemoptysis, and new alveolar infiltrates in conjugation with bloody bronchoalveolar lavage specimens (with numerous erythrocytes and siderophages). The diagnostic evaluation in diffuse alveolar hemorrhage usually includes bronchoscopic examination for two purposes, which are to document alveolar hemorrhage by bronchoalveolar lavage, to exclude airway sources of bleeding by visual inspection and to exclude an associated infection [13].
5 Case Reports in Nephrology 5 Although, in the present patient, bronchoscopy was not performed and the lavage specimens were not obtained, DAH was strongly suspected based on the response to steroid therapy, clinical course, the findings of chest CT, and a complication of RPGN. Although our patient was negative for ANCAs and anti-gbm antibody throughout hospitalization, Salama et al. reported that it is possible to prove the existence of low titer anti-gbm antibody using the Biosensor analysis (biomolecular interaction analysis system) for patients with anti-gbm disease [14]. However, this testing is difficult in the laboratory of our hospital, like many other laboratories, because complicated biochemical methods are required. Observing each antibody in greater detail, an antibody titer of P-ANCA was below cutoff value on admission, gradually decreased during hospitalization, and was below the measurement sensitivity on the 119th day. It is not clear whether the decline in antibody titer of P-ANCA within the normalrangewasaresultofadecreaseinthediseaseactivity or a good response to treatment with corticosteroids. In general, when these assays are negative, as in this case, renal biopsy is recommended for all patients with renal involvement because light microscopy and immunofluorescence studies can assess the extent and activity of glomerulonephritis [9]. As the underlying cause remained elusive after a thorough clinical evaluation that included imaging studies and frequent serologic studies, a renal biopsy was performed for diagnostic clues at a later date and specimens were evaluated pathologically. As the specimens showed crescent-shaped changes in the glomeruli, RPGN with crescent formation was diagnosed. However, as most specimens had already progressed to glomerular sclerosis because of the extensive time since the onset, linear IgG deposition along the capillary basement membrane was observed in only a very smallnumberofglomerulionfluorescentstaining.linear IgG deposition along the capillary basement membrane is virtually diagnostic of Goodpasture s syndrome. Therefore, although accurate diagnosis had been difficult, we thought that the clinical condition of this patient was most likely Goodpasture s syndrome based on clinical and histopathological manifestations. GlucocorticoidisthemaintherapyfortheDAHsyndrome associated with systemic vasculitis, connective tissue disease, and Goodpasture s syndrome. For the treatment of DAH, intravenous pulse methylprednisolone 500 to 2000 mg daily for up to five days was recommended in initial treatment, followed by gradual tapering depending on the response to therapy and then maintenance on an oral preparation [9]. In this patient, 500 mg intravenous methylprednisolone daily for 3 days with a subsequent tapering dose of intravenous methylprednisolone and long-term oral prednisolone were administered. On the other hand, plasma exchange therapy may also be performed as well as the administration of immunosuppressive agents, such as corticosteroid medications and cyclophosphamide for Goodpasture s syndrome. Plasmapheresis is usually continued for several weeks, until there is a marked decline in serum anti-gbm antibody titers and the patient s hemoptysis stops. In most cases, bleeding in the lungs stops and no permanent lung damage occurs, butdamagetothekidneysislonglasting.themeritsof plasmapheresis in diffuse alveolar hemorrhage associated with conditions other than Goodpasture s syndrome have not been evaluated in prospective studies [9, 14]. In this case, because we could not establish an accurate diagnosis of Goodpasture s syndrome and we did not detect target autoantibodies to remove through plasmapheresis, we did not perform plasma exchange. In hindsight, as plasma exchange regimens have been shown to be beneficial for patients with uncategorizable PRS, it might have been better to perform plasma exchange, considering that this patient quickly developed end-stage renal failure. 4. Conclusion Uncategorizable pulmonary-renal syndrome, in which double ANCAs and anti-gbm antibodies are negative, is extremely rare and no effective treatment has been established. Since PRS is fatal unless treated promptly, early diagnosis and timely initiation of treatment are crucial for good patient outcome. For these cases, rapid treatment with high-dose corticosteroids coupled with plasma exchange for uncategorizable PRS should be performed, as this was effective in a small subset of patients for preventing end-stage renal disease or death. Consent Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. References [1] S. A. Papiris, E. D. Manali, I. Kalomenidis, G. E. Kapotsis, A. Karakatsani, and C. Roussos, Bench-to-bedside review: pulmonary-renal syndromes an update for the intensivist, Critical Care, vol. 11, no. 3, pp , [2] C.-C. Wang, J.-C. Shiang, M.-K. Tsai et al., Prompt plasmapheresis successfully rescue pulmonary-renal syndrome caused by ANCA-negative microscopic polyangiitis, Clinical Rheumatology,vol.28,no.12,pp ,2009. [3]C.D.Pusey, Anti-glomerularbasementmembranedisease, Kidney International,vol.64,no.4,pp ,2003. [4]H.Gallagher,J.T.C.Kwan,andD.R.W.Jayne, Pulmonary renal syndrome: a 4-year, single-center experience, American Kidney Diseases,vol.39,no.1,pp.42 47,2002. [5] R.J.Glassock,L.Khorashadi,andY.B.Kushner, Caserecords of the Massachusetts General Hospital. Case A 35-yearold man with respiratory and renal failure, The New England Medicine,vol.367,pp ,2012. [6] D. J. Davies, J. E. Moran, J. F. Niall, and G. B. Ryan, Segmental necrotising glomerulonephritis with antineutrophil antibody: possible arbovirus aetiology? British Medical Journal,vol.285, no. 6342, p. 606, [7] R. Sexena, P. Bygren, B. Arvastson, and J. Wieslander, Circulating autoantibodies as serological markers in the differential diagnosis of pulmonary renal syndrome, Internal Medicine,vol.238,no.2,pp ,1995.
6 6 Case Reports in Nephrology [8] J.L.Niles,E.P.Böttinger,G.R.Saurinaetal., Thesyndromeof lung hemorrhage and nephritis is usually an ANCA-associated condition, Archives of Internal Medicine, vol. 156, no. 4, pp , [9]K.W.A.Westman,P.G.Bygren,I.Eilert,A.Wiik,andJ. Wieslander, Rapid screening assay for anti-gbm antibody and ANCAs; an important tool for the differential diagnosis of pulmonary renal syndromes, Nephrology Dialysis Transplantation, vol.12,no.9,pp ,1997. [10]S.C.West,N.Arulkumaran,P.W.Ind,andC.D.Pusey, Pulmonary-renal syndrome: a life threatening but treatable condition, Postgraduate Medical Journal, vol. 89, pp , [11] Y. Uji, T. Shimizu, T. Yoshioka, H. Yamamoto, Y. Endo, and T. Tani, A case report of pulmonary-renal syndrome treated with continuous hemodiafiltration and hemodialysis, Therapeutic Apheresis and Dialysis,vol.10,no.5,pp ,2006. [12] K. Sampathkumar, M. Ramakrishnan, A. K. Sah, S. Gowtham, and R. N. Ajeshkumar, ANCA negative pauci-immune glomerulonephritis with systemic involvement, Indian Journal of Nephrology,vol.20,no.1,pp.43 47,2010. [13] O.C.LoachimescuandJ.K.Stoller, Diffusealveolarhemorrhage: diagnosing it and finding the cause, Cleveland Clinic Medicine,vol.75,pp ,2008. [14] A. D. Salama, T. Dougan, J. B. Levy et al., Goodpasture s disease in the absence of circulating anti-glomerular basement membrane antibodies as detected by standard techniques, American Kidney Diseases,vol.39,no.6,pp , 2002.
















7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Protocol Version 2.0 Synopsis
 Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman
 CASE REPORT Advance Access publication 20 May 2014 Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman Rubina Naqvi 1, Muhammed Mubarak 2 1 Department of Nephrology
CASE REPORT Advance Access publication 20 May 2014 Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman Rubina Naqvi 1, Muhammed Mubarak 2 1 Department of Nephrology
The Sequential Development of Antiglomerular Basement Membrane Nephritis and Myeloperoxidase-antineutrophil Cytoplasmic Antibody-associated Vasculitis
 doi: 10.2169/internalmedicine.8757-16 http://internmed.jp CASE REPORT The Sequential Development of Antiglomerular Basement Membrane Nephritis and Myeloperoxidase-antineutrophil Cytoplasmic Antibody-associated
doi: 10.2169/internalmedicine.8757-16 http://internmed.jp CASE REPORT The Sequential Development of Antiglomerular Basement Membrane Nephritis and Myeloperoxidase-antineutrophil Cytoplasmic Antibody-associated
Case Report Severe Uncompensated Metabolic Alkalosis due to Plasma Exchange in a Patient with Pulmonary-Renal Syndrome: A Clinician s Challenge
 Case Reports in Critical Care Volume 2015, Article ID 802186, 5 pages http://dx.doi.org/10.1155/2015/802186 Case Report Severe Uncompensated Metabolic Alkalosis due to Plasma Exchange in a Patient with
Case Reports in Critical Care Volume 2015, Article ID 802186, 5 pages http://dx.doi.org/10.1155/2015/802186 Case Report Severe Uncompensated Metabolic Alkalosis due to Plasma Exchange in a Patient with
A TRICKY PROBLEM. Presenter-Dr Lakshmi PK
 A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
Anestesia Pediatrica e Neonatale, Vol. 10, N. 1, May-July 2012
 Goodpasture s Syndrome in a 17 years girl. Fast track ICU support as bridge to full recovery after pulmonary failure. Daniela Codazzi 1, Antonio di Coste 2, Maria A. Scalera 1, Maria T. Ficarella 1 1 Division
Goodpasture s Syndrome in a 17 years girl. Fast track ICU support as bridge to full recovery after pulmonary failure. Daniela Codazzi 1, Antonio di Coste 2, Maria A. Scalera 1, Maria T. Ficarella 1 1 Division
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Development of anti-glomerular basement membrane glomerulonephritis during the course of IgA nephropathy: a case report
 Kojima et al. BMC Nephrology (2019) 20:25 https://doi.org/10.1186/s12882-019-1207-3 CASE REPORT Open Access Development of anti-glomerular basement membrane glomerulonephritis during the course of IgA
Kojima et al. BMC Nephrology (2019) 20:25 https://doi.org/10.1186/s12882-019-1207-3 CASE REPORT Open Access Development of anti-glomerular basement membrane glomerulonephritis during the course of IgA
Case Report Top Differential Diagnosis Should Be Microscopic Polyangiitis in ANCA-Positive Patient with Diffuse Pulmonary Hemorrhage and Hemosiderosis
 Case Reports in Pathology, Article ID 286030, 5 pages http://dx.doi.org/10.1155/2014/286030 Case Report Top Differential Diagnosis Should Be Microscopic Polyangiitis in ANCA-Positive Patient with Diffuse
Case Reports in Pathology, Article ID 286030, 5 pages http://dx.doi.org/10.1155/2014/286030 Case Report Top Differential Diagnosis Should Be Microscopic Polyangiitis in ANCA-Positive Patient with Diffuse
Management of Acute Vasculitis. CMT teaching 3 rd June 2015 Caroline Wroe
 Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Retraction Retracted: Anti-GBM of Pregnancy: Acute Renal Failure Resolved after Spontaneous Abortion, Plasma Exchange, Hemodialysis, and Steroids
 Hindawi Publishing Corporation Volume 015, Article ID 369087, 1 page http://dx.doi.org/10.1155/015/369087 Retraction Retracted: Anti-GBM of Pregnancy: Acute Renal Failure Hemodialysis, and Steroids Received
Hindawi Publishing Corporation Volume 015, Article ID 369087, 1 page http://dx.doi.org/10.1155/015/369087 Retraction Retracted: Anti-GBM of Pregnancy: Acute Renal Failure Hemodialysis, and Steroids Received
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Elevated Expression of Pentraxin 3 in Anti-neutrophil Cytoplasmic Antibody-associated Glomerulonephritis with Normal Serum C-reactive Protein
 CASE REPORT Elevated Expression of Pentraxin 3 in Anti-neutrophil Cytoplasmic Antibody-associated Glomerulonephritis with Normal Serum C-reactive Protein Risa Ishida 1,KentaroNakai 1, Hideki Fujii 1, Shunsuke
CASE REPORT Elevated Expression of Pentraxin 3 in Anti-neutrophil Cytoplasmic Antibody-associated Glomerulonephritis with Normal Serum C-reactive Protein Risa Ishida 1,KentaroNakai 1, Hideki Fujii 1, Shunsuke
The Effects of Plasma Exchange on Severe Vasculitis with Diffuse Alveolar Hemorrhage
 CASE REPORT The Effects of Plasma Exchange on Severe Vasculitis with Diffuse Alveolar Hemorrhage Kimihiko Goto, Kentaro Nakai, Hideki Fujii and Shinichi Nishi Abstract Antineutrophil cytoplasmic autoantibody
CASE REPORT The Effects of Plasma Exchange on Severe Vasculitis with Diffuse Alveolar Hemorrhage Kimihiko Goto, Kentaro Nakai, Hideki Fujii and Shinichi Nishi Abstract Antineutrophil cytoplasmic autoantibody
Case Report Crescentic Glomerulonephritis with Anti-GBM and p-anca Antibodies
 Case Reports in Nephrology Volume 2012, Article ID 132085, 4 pages doi:10.1155/2012/132085 Case Report Crescentic Glomerulonephritis with Anti-GBM and p-anca Antibodies TariqJavedandParagVohra Department
Case Reports in Nephrology Volume 2012, Article ID 132085, 4 pages doi:10.1155/2012/132085 Case Report Crescentic Glomerulonephritis with Anti-GBM and p-anca Antibodies TariqJavedandParagVohra Department
RATIONALE. K Without therapy, ANCA vasculitis with GN is associated. K There is high-quality evidence for treatment with
 http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
Case Report Hydralazine Induces Myeloperoxidase and Proteinase 3 Anti-Neutrophil Cytoplasmic Antibody Vasculitis and Leads to Pulmonary Renal Syndrome
 Case Reports in Nephrology, Article ID 868590, 4 pages http://dx.doi.org/10.1155/2014/868590 Case Report Hydralazine Induces Myeloperoxidase and Proteinase 3 Anti-Neutrophil Cytoplasmic Antibody Vasculitis
Case Reports in Nephrology, Article ID 868590, 4 pages http://dx.doi.org/10.1155/2014/868590 Case Report Hydralazine Induces Myeloperoxidase and Proteinase 3 Anti-Neutrophil Cytoplasmic Antibody Vasculitis
Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases
 Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Anti-MPO ANCA-Associated Diffuse Alveolar Hemorrhage is Associated with Increased Mortality Compared to Anti-PR3 Disease
 Anti-MPO ANCA-Associated Diffuse Alveolar Hemorrhage is Associated with Increased Mortality Compared to Anti-PR3 Disease Grace M. Lee, Yara A. Park, Marshall Mazepa, Jay S. Raval Introduction Anti-neutrophil
Anti-MPO ANCA-Associated Diffuse Alveolar Hemorrhage is Associated with Increased Mortality Compared to Anti-PR3 Disease Grace M. Lee, Yara A. Park, Marshall Mazepa, Jay S. Raval Introduction Anti-neutrophil
A Case of Pulmonary Hemorrhage and Renal Failure
 Send Orders of Reprints at bspsaif@emirates.net.ae 40 The Open Urology & Nephrology Journal, 2012, 5, 40-47 A Case of Pulmonary Hemorrhage and Renal Failure Alexa S. Meara *,1, Daphne M. Harrington 1,
Send Orders of Reprints at bspsaif@emirates.net.ae 40 The Open Urology & Nephrology Journal, 2012, 5, 40-47 A Case of Pulmonary Hemorrhage and Renal Failure Alexa S. Meara *,1, Daphne M. Harrington 1,
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
Pulmonary Renal Syndrome
 C H A P T E R 41 Pulmonary Renal Syndrome Yojana Gokhale, Raosaheb Rathod INTRODUCTION 1. Pulmonary Renal Syndrome (PRS), is a combination of diffuse alveolar haemorrhage (DAH) and glomerulonephritis (GN),
C H A P T E R 41 Pulmonary Renal Syndrome Yojana Gokhale, Raosaheb Rathod INTRODUCTION 1. Pulmonary Renal Syndrome (PRS), is a combination of diffuse alveolar haemorrhage (DAH) and glomerulonephritis (GN),
Dense deposit disease with steroid pulse therapy
 Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Simultaneous comprehensive multiplex autoantibody analysis by CytoBead technology for Rapidly Progressive Glomerulonephritis.
 Simultaneous comprehensive multiplex autoantibody analysis by CytoBead technology for Rapidly Progressive Glomerulonephritis l Assays Indirect Immunofluorescence Goldstandard for Diagnosis of Autoimmune
Simultaneous comprehensive multiplex autoantibody analysis by CytoBead technology for Rapidly Progressive Glomerulonephritis l Assays Indirect Immunofluorescence Goldstandard for Diagnosis of Autoimmune
CASE REPORT. Introduction
 doi: 10.2169/internalmedicine.9188-17 http://internmed.jp CASE REPORT Diffuse Alveolar Hemorrhage Developing Immediately after Immunosuppressive Treatments in a Patient with Granulomatosis with Polyangiitis
doi: 10.2169/internalmedicine.9188-17 http://internmed.jp CASE REPORT Diffuse Alveolar Hemorrhage Developing Immediately after Immunosuppressive Treatments in a Patient with Granulomatosis with Polyangiitis
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
anti-neutrophil cytoplasmic antibody, myeloperoxidase, microscopic polyangiitis, cyclophosphamide, corticosteroid
 Online publication June 24, 2009 ANCA JMAAV 1 2 ANCA JMAAV MPO-ANCA 18 17 50 J Jpn Coll Angiol, 2009, 49: 53 61 anti-neutrophil cytoplasmic antibody, myeloperoxidase, microscopic polyangiitis, cyclophosphamide,
Online publication June 24, 2009 ANCA JMAAV 1 2 ANCA JMAAV MPO-ANCA 18 17 50 J Jpn Coll Angiol, 2009, 49: 53 61 anti-neutrophil cytoplasmic antibody, myeloperoxidase, microscopic polyangiitis, cyclophosphamide,
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Hidden Tiger: An Atypical Presentation of Anti-Glomerular Basement Membrane Disease
 Elmer Press Case Report Hidden Tiger: An Atypical Presentation of Anti-Glomerular Basement Membrane Disease Ashani Lecamwasam a, Darren Lee a, b, d, Alison Skene c, Lawrence McMahon a Abstract Anti-glomerular
Elmer Press Case Report Hidden Tiger: An Atypical Presentation of Anti-Glomerular Basement Membrane Disease Ashani Lecamwasam a, Darren Lee a, b, d, Alison Skene c, Lawrence McMahon a Abstract Anti-glomerular
AKI Case study -Vasculitis. Sarah Mackie Renal Practice Development Nurse King s College Hospital - London
 AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
4. KIDNEYS AND AUTOIMMUNE DISEASE
 How to Cite this article: Kidneys and Autoimmune Disease - ejifcc 20/01 2009 http://www.ifcc.org 4. KIDNEYS AND AUTOIMMUNE DISEASE Maksimiljan Gorenjak 4.1 Autoimmune diseases The human immune system limits
How to Cite this article: Kidneys and Autoimmune Disease - ejifcc 20/01 2009 http://www.ifcc.org 4. KIDNEYS AND AUTOIMMUNE DISEASE Maksimiljan Gorenjak 4.1 Autoimmune diseases The human immune system limits
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Clinical features and outcome of patients with both ANCA and anti-gbm antibodies
 Kidney International, Vol. 66 (24), pp. 1535 154 Clinical features and outcome of patients with both ANCA and anti-gbm antibodies JEREMY B. LEVY, TARIG HAMMAD, ANNE COULTHART, TAMMY DOUGAN, and CHARLES
Kidney International, Vol. 66 (24), pp. 1535 154 Clinical features and outcome of patients with both ANCA and anti-gbm antibodies JEREMY B. LEVY, TARIG HAMMAD, ANNE COULTHART, TAMMY DOUGAN, and CHARLES
Significance of Anti-C1q Antibodies in Patients with Systemic Lupus Erythematosus as A Marker of Disease Activity and Lupus Nephritis
 THE EGYPTIAN JOURNAL OF IMMUNOLOGY Vol. 23 (1), 2016 Page: 00-00 Significance of Anti-C1q Antibodies in Patients with Systemic Lupus Erythematosus as A Marker of Disease Activity and Lupus Nephritis 1
THE EGYPTIAN JOURNAL OF IMMUNOLOGY Vol. 23 (1), 2016 Page: 00-00 Significance of Anti-C1q Antibodies in Patients with Systemic Lupus Erythematosus as A Marker of Disease Activity and Lupus Nephritis 1
Braden Powers, Aditya Uppalapati, Sindhura Gogineni, and Zafar Akram Jamkhana
 Case Reports in Critical Care Volume 2013, Article ID 123134, 4 pages http://dx.doi.org/10.1155/2013/123134 Case Report Rituximab A Drug with Many Facets and Cures: A Treatment for Acute Refractory Hypoxemic
Case Reports in Critical Care Volume 2013, Article ID 123134, 4 pages http://dx.doi.org/10.1155/2013/123134 Case Report Rituximab A Drug with Many Facets and Cures: A Treatment for Acute Refractory Hypoxemic
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura)
") Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura) J. Charles Jennette Ronald J. Falk The kidneys are affected by a variety of systemic vasculitides
Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura) J. Charles Jennette Ronald J. Falk The kidneys are affected by a variety of systemic vasculitides
Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors of Renal Outcome
 International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
Case Report A Case Report Describing a Rare Presentation of Simultaneous Occurrence of MPO-ANCA-Associated Vasculitis and Rheumatoid Arthritis
 Case Reports in Nephrology Volume 2016, Article ID 9340524, 5 pages http://dx.doi.org/10.1155/2016/9340524 Case Report A Case Report Describing a Rare Presentation of Simultaneous Occurrence of MPO-ANCA-Associated
Case Reports in Nephrology Volume 2016, Article ID 9340524, 5 pages http://dx.doi.org/10.1155/2016/9340524 Case Report A Case Report Describing a Rare Presentation of Simultaneous Occurrence of MPO-ANCA-Associated
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Small Vessel Vasculitis
 Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS
 GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
Complicated Acute Motor Axonal Neuropathy with Delayed Acute Respiratory Distress Syndrome and Rapidly Progressive Glomerulonephritis: a Case Report
 26 Complicated Acute Motor Axonal Neuropathy with Delayed Acute Respiratory Distress Syndrome and Rapidly Progressive Glomerulonephritis: a Case Report An-Chih Chen 1,6,7, Chiu-Mei Chen 1,6,7, Horng-Rong
26 Complicated Acute Motor Axonal Neuropathy with Delayed Acute Respiratory Distress Syndrome and Rapidly Progressive Glomerulonephritis: a Case Report An-Chih Chen 1,6,7, Chiu-Mei Chen 1,6,7, Horng-Rong
RAPIDLY FAILING KIDNEYS. Dr Paul Johny 2 nd yr DNB Medicine Resident
 RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Tell me more about vasculitis. Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital
 Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Anti-Neutrophil Cytoplasmic Antibody (ANCA)-Negative Small Vessel Vasculitis: A Rare Cause of Pulmonary Renal Syndrome
-Negative Small Vessel Vasculitis: A Rare Cause of Pulmonary Renal Syndrome") CASE REPORT Anti-Neutrophil Cytoplasmic Antibody (ANCA)-Negative Small Vessel Vasculitis: A Rare Cause of Pulmonary Renal Syndrome Boudhayan Das Munshi, Sarbani Sengupta, Abhijeet Sharan, Sarmishtha Mukhopadhyay,
CASE REPORT Anti-Neutrophil Cytoplasmic Antibody (ANCA)-Negative Small Vessel Vasculitis: A Rare Cause of Pulmonary Renal Syndrome Boudhayan Das Munshi, Sarbani Sengupta, Abhijeet Sharan, Sarmishtha Mukhopadhyay,
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Diffuse Alveolar Infiltrates and Macroscopic Hematuria: A Run-and-Gun Affair
 What Is Your Diagnosis? Respiration 2010;79:511 515 DOI: 10.1159/000282170 Received: September 8, 2009 Accepted after revision: December 14, 2009 Published online: February 5, 2010 Diffuse Alveolar Infiltrates
What Is Your Diagnosis? Respiration 2010;79:511 515 DOI: 10.1159/000282170 Received: September 8, 2009 Accepted after revision: December 14, 2009 Published online: February 5, 2010 Diffuse Alveolar Infiltrates
Wegener s Granulomatosis JUN-KI PARK
 Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Membranous nephropathy. By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University
 Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Alveolar Hemorrhage Syndromes
 PULMONARY DISEASE BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, PUBLISHER Bruce M.White EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Miranda J. Hughes, PhD EDITOR Becky Krumm ASSISTANT EDITOR Kathryn
PULMONARY DISEASE BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, PUBLISHER Bruce M.White EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Miranda J. Hughes, PhD EDITOR Becky Krumm ASSISTANT EDITOR Kathryn
Key words: Crescentic glomerulonephritis, Microscopic polyarteritis, MPO-ANCA, Steroid therapy
 Hiroshima J. Med. Sci. Vol.46, No.3, 99~ 104, September, 1997 HIJM 46-13 99 Myeloperoxidase Antineutrophil Cytoplasmic Autoantibody -associated Glomerulonephritis in a Very Elderly Patient with Generalized
Hiroshima J. Med. Sci. Vol.46, No.3, 99~ 104, September, 1997 HIJM 46-13 99 Myeloperoxidase Antineutrophil Cytoplasmic Autoantibody -associated Glomerulonephritis in a Very Elderly Patient with Generalized
Near-lethal acute kidney injury due to Goodpasture s syndrome: A case report
 Case report Near-lethal acute kidney injury due to Goodpasture s syndrome: A case report Vivek K Sinha and Caroline Hibbert Journal of the Intensive Care Society 2015, Vol. 16(4) 350 354! The Intensive
Case report Near-lethal acute kidney injury due to Goodpasture s syndrome: A case report Vivek K Sinha and Caroline Hibbert Journal of the Intensive Care Society 2015, Vol. 16(4) 350 354! The Intensive
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
SHO Teaching. Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth
 SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
VCRC-OMERACT ANCA-Vasculitis Outcome Measure Initiative Comparative Outcome Measure Exercise-Training Cases
 Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
Case Report Pulmonary Tuberculosis and Lepromatous Leprosy Coinfection
 Case Reports in Dermatological Medicine Volume 2015, Article ID 898410, 4 pages http://dx.doi.org/10.1155/2015/898410 Case Report Pulmonary Tuberculosis and Lepromatous Leprosy Coinfection F. A. Sendrasoa,
Case Reports in Dermatological Medicine Volume 2015, Article ID 898410, 4 pages http://dx.doi.org/10.1155/2015/898410 Case Report Pulmonary Tuberculosis and Lepromatous Leprosy Coinfection F. A. Sendrasoa,
Anti-neutrophil Cytoplasmic Antibody-associated Pauci-immune Crescentic Glomerulonephritis Complicating Sjögren s Syndrome
 Volume 110 Number 7 July 2011 Enterovirus 71 vaccine: When will it be available? GRP78 in embryonic development and neurological disorders Directly observed therapy for Tuberculosis patients in Taiwan
Volume 110 Number 7 July 2011 Enterovirus 71 vaccine: When will it be available? GRP78 in embryonic development and neurological disorders Directly observed therapy for Tuberculosis patients in Taiwan
Case Report Pauci-Immune Crescentic Glomerulonephritis in Connective Tissue Disease
 Case Reports in Rheumatology Volume 2016, Article ID 9070487, 6 pages http://dx.doi.org/10.1155/2016/9070487 Case Report Pauci-Immune Crescentic Glomerulonephritis in Connective Tissue Disease Supraja
Case Reports in Rheumatology Volume 2016, Article ID 9070487, 6 pages http://dx.doi.org/10.1155/2016/9070487 Case Report Pauci-Immune Crescentic Glomerulonephritis in Connective Tissue Disease Supraja
RENAL BIOPSIES in patients with the clinical
 RENAL BIOPSY TEACHING CASE Crescentic Glomerulonephritis With a Paucity of Glomerular Immunoglobulin Localization Alexis A. Harris, MD, Ronald J. Falk, MD, and J. Charles Jennette, MD RENAL BIOPSIES in
RENAL BIOPSY TEACHING CASE Crescentic Glomerulonephritis With a Paucity of Glomerular Immunoglobulin Localization Alexis A. Harris, MD, Ronald J. Falk, MD, and J. Charles Jennette, MD RENAL BIOPSIES in
Hiroyuki Kamiya 1), Soichiro Ikushima 1), Tetsu Sakamoto 1), Kozo Morimoto 1), Tsunehiro Ando 1), Masaru Oritsu 1), Atsuo Goto 2), Tamiko Takemura 3)
, Soichiro Ikushima 1), Tetsu Sakamoto 1), Kozo Morimoto 1), Tsunehiro Ando 1), Masaru Oritsu 1), Atsuo Goto 2), Tamiko Takemura 3)") 29 2001 ACE39.7IU/l X TBLB 2002 11 Langhans [ ] A Case of Granulomatous Interstitial Nephritis with Progressive Renal Impairment Due to Sarcoidosis in the Course of Spontaneous Improvement of Pulmonary
29 2001 ACE39.7IU/l X TBLB 2002 11 Langhans [ ] A Case of Granulomatous Interstitial Nephritis with Progressive Renal Impairment Due to Sarcoidosis in the Course of Spontaneous Improvement of Pulmonary
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
FAQ Identifying and enrolling participants
 FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
Research Article Predictions of the Length of Lumbar Puncture Needles
 Computational and Mathematical Methods in Medicine, Article ID 732694, 5 pages http://dx.doi.org/10.1155/2014/732694 Research Article Predictions of the Length of Lumbar Puncture Needles Hon-Ping Ma, 1,2
Computational and Mathematical Methods in Medicine, Article ID 732694, 5 pages http://dx.doi.org/10.1155/2014/732694 Research Article Predictions of the Length of Lumbar Puncture Needles Hon-Ping Ma, 1,2
Jones slide di 23
 1 di 23 The patient with ANCA- associated vasculitis and pulmonary haemorrhage Rachel B Jones, Cambridge, UK Chairs:Hans-Joachim Anders, Munich, Germany Vladimir Tesar, Prague, Czech Republic Prof. Rachel
1 di 23 The patient with ANCA- associated vasculitis and pulmonary haemorrhage Rachel B Jones, Cambridge, UK Chairs:Hans-Joachim Anders, Munich, Germany Vladimir Tesar, Prague, Czech Republic Prof. Rachel
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
W J N. World Journal of Nephrology. Antineutrophil cytoplasmic antibodies crescentic allograft glomerulonephritis after sofosbuvir therapy.
 W J N World Journal of Nephrology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5527/wjn.v5.i6.547 World J Nephrol 2016 November 6; 5(6):
W J N World Journal of Nephrology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5527/wjn.v5.i6.547 World J Nephrol 2016 November 6; 5(6):
INTRODUCTION. nephropathy, however, usually presents as membranoproliferative
 Hong Kong J Journal Nephrol of 2001;3(2):97-102. Nephrology 2001;3(2):97-102. A KURUSU, et al C A S E R E P O R T Monitoring of serum hepatitis C virus RNA level during steroid therapy for hepatitis C
Hong Kong J Journal Nephrol of 2001;3(2):97-102. Nephrology 2001;3(2):97-102. A KURUSU, et al C A S E R E P O R T Monitoring of serum hepatitis C virus RNA level during steroid therapy for hepatitis C
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Predictors of renal and patient outcomes in anti-gbm disease: clinicopathologic analysis of a two-centre cohort
 NDT Advance Access published January 20, 2015 Nephrol Dial Transplant (2015) 0: 1 7 doi: 10.1093/ndt/gfu399 Original Article Predictors of renal and patient outcomes in anti-gbm disease: clinicopathologic
NDT Advance Access published January 20, 2015 Nephrol Dial Transplant (2015) 0: 1 7 doi: 10.1093/ndt/gfu399 Original Article Predictors of renal and patient outcomes in anti-gbm disease: clinicopathologic
Rapidly Progressive Pulmonary Fibrosis Following the Onset of Diffuse Alveolar Hemorrhage in Sjögren s Syndrome: An Autopsy Case Report
 CASE REPORT Rapidly Progressive Pulmonary Fibrosis Following the Onset of Diffuse Alveolar Hemorrhage in Sjögren s Syndrome: An Autopsy Case Report Yusuke Tomita 1,2, Shunsuke Mori 3, Nobuyuki Arima 4,
CASE REPORT Rapidly Progressive Pulmonary Fibrosis Following the Onset of Diffuse Alveolar Hemorrhage in Sjögren s Syndrome: An Autopsy Case Report Yusuke Tomita 1,2, Shunsuke Mori 3, Nobuyuki Arima 4,