The ABC s of ILD LIP AIP NSIP
|
|
|
- Barry Manning
- 5 years ago
- Views:
Transcription

1 The ABC s of ILD LIP NSIP AIP
2 Classification Clinical Idiopathic Disorders Pulmonary Fibrosis NSIP COP AIP Sarcoidosis Connective Tissue Disease Drug-Induced Occupational/Environmental Pulmonary Alveolar Proteinosis Cystic Lung Disease Pulmonary Langerhans Cell Histiocytosis LAM LIP Pathologic Diffuse Alveolar Damage Organizing Pneumonia Desquamative Interstitial Pneumonia Nonspecific Interstitial Pneumonia Usual Interstitial Pneumonia Lymphocytic Interstitial Pneumonia Eosinophilc Pneumonia Alveolar Proteinosis
3 Classification Clinical Idiopathic Disorders Pulmonary Fibrosis NSIP COP AIP Sarcoidosis Connective Tissue Disease Drug-Induced Occupational/Environmental Pulmonary Alveolar Proteinosis Cystic Lung Disease Pulmonary Langerhans Cell Histiocytosis LAM LIP Pathologic Diffuse Alveolar Damage Organizing Pneumonia Desquamative Interstitial Pneumonia Nonspecific Interstitial Pneumonia Usual Interstitial Pneumonia Lymphocytic Interstitial Pneumonia Alveolar Proteinosis
4 First Step in Diagnosing ILD TAKE A HISTORY!
5 Clinical Approach to ILD Demographics Age Gender Duration of Illness Smoking History Family History Current and prior medications Occupational History Environmental History
6 Idiopathic Pulmonary Fibrosis Age of onset 50-70, slight male predominance Increasing Incidence Insidious onset of DOE and nonproductive cough Family History (Familial Pulmonary Fibrosis) PE shows bibasilar late inspiratory dry crackles or velcro crackles Serologies to r/o CTD CXR/HRCT Pathology: UIP pattern, not necessary if classic hx and radiographic pattern
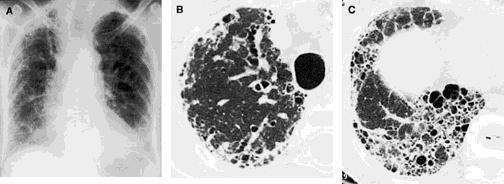
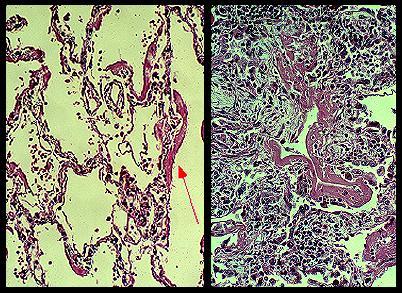
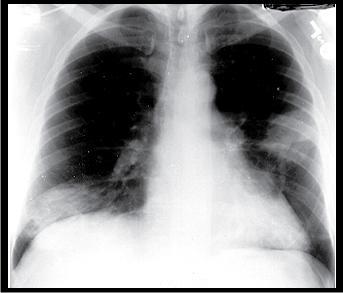
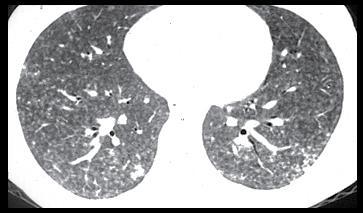
7 Imaging

8 Normal Lung
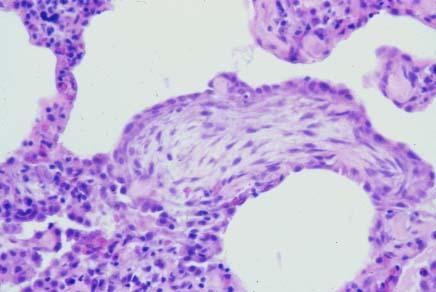

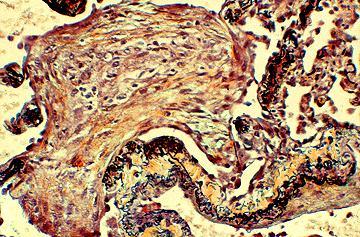
9 Pathology
10 Pathogenesis Genetic Predisposition + Inciting Event + Uncontrolled/Abnormal Repair Mechanism (Inflammatory, Immune, Fibrosis) Genetic Predisposition Initiation Event Smoking Inhalational Injury Virus Inflammation
11 Treatment?
12 Treatment No therapy has been proven to be efficacious Supportive care (O2, pulm rehab, vaccines) Consider referring to clinical trials Immunosuppressant/Antioxidant Therapy Prednisone + azathioprine + NAC (PANTHER trial) Antifibrotic Therapy Pirfenidone Decrease in number of exacerbations; 14% versus 0% Approved in Japan, Canada, Europe
13 Treatment Treat GERD/microaspiration ( up to 90% of pts) Referral for lung transplantation Future Therapies? Thalidomide Tyrosine Kinase Inhibitors Cytokine Inhibitors Growth Factor Inhibitors
14 Prognosis/Clinical Course Slow, indolent course; mean survival 2-3 yrs since time of diagnosis Rapid progression Acute exacerbations Rapid, progressive SOB Unknown cause (r/o infection, PE, heart failure) CT will show new GG infiltrates Path shows DAD or acute alveolar injury wirh background of UIP Treatment Solumedrol 1 to 2 gm/day Mortality rate 80%
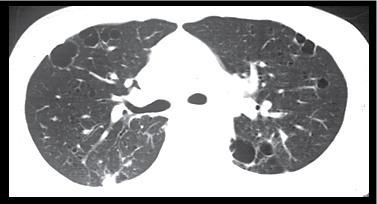
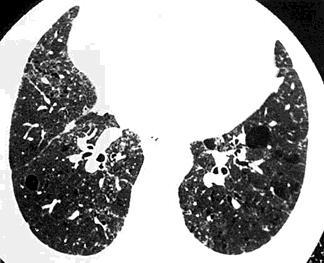
15 NSIP 40 to 50 Chronic dyspnea, cough PE with bibasilar crackles Idiopathic cases but NEED to r/o a known cause (CVD, drugs, HP) HRCT shows GG airspace consolidation, and reticular abnormalities 2 pathologic patterns: cellular, fibrotic

16 HRCT


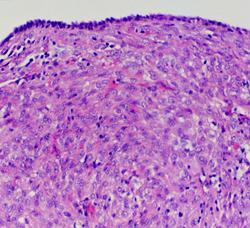
17 Path Cellular NSIP Fibrotic NSIP
18 Treatment Much better response to treatment Cellular 100% Fibrotic 35-90% 5 yr survival; 70%
19 Respiratory Bronchiolitis-ILD and Desquamative interstitial Pneumonia (RBILD/DIP) Young 30-40, CIGARETTE smokers Cough, dyspnea. Chronic, progressive sx? Distinct entities vs. a continuum of same disease (RBILD -> DIP) HRCT: centrilobular nodules, GG, air trapping Path: pigmented laden macrophages in resp. bronchioles (RBILD) and diffusely throughout alveoli (DIP)


20
21 Pathology
22 RBILD/DIP Treatment: STOP smoking + glucocorticosteroids 60% of pts improve 5 yr survival of 70%
23 Acute Interstitial Pneumonia Formerly, Hamman-Rich Disease Acute to subacute onset of dyspnea and cough, rapidly progressive to resp failure Fever PE with diffuse insp crackles ARDS without a cause HRCT with GG infiltrates, consolidation Pathology shows DAD
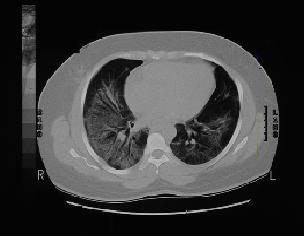
24 CT

25 Path
26 Treatment/Prognosis No proven treatment Most tx with abx, steroids Worse survival than ARDS, >50% mortality
27 COP Idiopathic BOOP Non-idiopathic causes (post-infectious, drugs, CVD, post-transplant) Dyspnea and cough over days to months Fever Often misdiagnosed as pneumonia PE bibasilar crackles HRCT with bilateral patchy consolidation, peribronchovascualr nodules

28 Imaging
29 Path
30 Treatment Very responsive to tx with steroids >80% of pts respond to tx 5 yr survival close to 100%
31 Collagen Vascular Disease RA Lupus Systemic sclerosis Polymyositis/Dermatomyositis MCTD Sjogren s Relapsing polychondritis Ankylosing Spondylitis Behcet s Disease Systemic vasculitides
32 Lung disease Underlying Disease Complication of treatment Opportunistic Infection Associated with Increased morbidity and mortality Pulmonary Involvement CAN BE initial manifestation of CVD
33 Rheumatoid Arthritis ILD (men > women) Pulm fibrosis BOOP Apical fibrobullous disease Amyloid Pleural Disease Effusions Pleuritis Rheumatoid Nodules Airways Disease Cricoarytenoid arthritis Airflow limitation Follicular bronchitis bo Bronchiectasis Drug-Induced MTX Penicillamine Gold Pulmonary HTN
34 Lupus ILD Lupus pneumonitis BOOP DAH Airways Disease Bronchiectasis BO BOOP Epiglottitis, laryngitis, cricoarytenoid arthritis Pleural Disease Pulm HTN Diaphragmatic Dysfunction/Shrinking Lung Syndrome
35 Systemic sclerosis ILD (25-45%) Pulm fibrosis Aspiration pneumonitis DAH DAD Airways Disease Airflow limitation Follicular bronchiolitis Pleural Disease Pleuritis Pleural Effusion Spont PTX Pulm HTN
36 Polymyositis/Dermatomyositis ILD Pulm fibrosis Aspiration pneumonitis BOOP DAH DAAD Aspiration Pneumonia Respiratory Muscle Dysfunction Diaphragmatic Dysfxn Atelectasis Vent failure Pulm HTN Malignancy
37 Work-up RF (anti-ccp) ANA Scl-70 CPK, aldolase SS-A, SS-B Anti-jo 1
38 Treatment DMARDs (Azathioprine, Cellcept, Cyclophoasphamide) Pulmonary involvement associated with reduced survival Prognosis is better then idiopathic cases
39 Drug-Induced Amiodarone Bleomycin Busulfan Chlorambucil Carmustine Flecainide Gold Methotrexate Nitrofurantoin Taxol/taxotere
40 Occupational Asbestosis Plumbers, Pipefittersm Electricians, Insulation Workers, Construction, Shipbuilders, Railways Silicosis Miners, masonry, Sandblasting, Foundry, Ceramics, Glass Maufacturing Berylliosis Machine shops, electronics, defense industry
41 Hypersensitivity Pneumonitis Immunolgic reaction to an inhaled agent (organic) Cigarette smoking associated with decreased risk of HP
42 Occupations Farming, vegetable, or dairy cattle workers Ventilation and water-related contamination Bird and poultry handling Veterinary work and animal handling Grain and flour processing Lumber milling, construction, wood stripping, paper manufacturing Plastic manufacture, painting, other chemicals Textile workers
43 Acute HP 4 to 6 hrs following an acute exposure Fevers, chills, malaise, cough, dyspnea, wheezing May be confused with an infection Removal of exposure results in resolution of sx, usually days CXR micronodular interstitial pattern in midlower lung zones Path poorly formed noncaseating granulomas
44 Subacute HP Fatigue, anorexia, weight loss, productive cough, dyspnea CT shows nodules, GG, mild fibrotic changes in upper lungs Treatment removal from exposure and glucosteroids
45 HRCT
46 Chronic HP Insidious onset of cough, DOE, fatigue, weight loss HRCT with GG, micronodules accompanied by honeycombing Often misdiagnosed as IPF

47 HRCT
48 Sarcoidosis Radiographic Stages O : No disease I : B hilar/mediastinal LAD II : LAD + diffuse interstitial pattern III : parenchymal disease w/o nodal enlargement IV : pulm fibrosis with honeycomb changes Bronchoscopy Increased CD4/CD8 ratio TBBx yield 40-90% Noncaseating granulomas Prognosis 2/3 spont remission Treatment Pred + MTX Azathioprine, hydroxychloroquine, CPA
49 Pulmonary Alveolar Proteinosis 30 to 50 2:1 male predominance Dyspnea 1/3 of pts asx and present with abnl CXR Caused by decreased GM- CSF protein or altered fxn. Large % of adults will have autoantibodies. CXR with B alveolar opacities in bat-wing HRCT with GG opacities, thickened intralobular septa in polygonal shapes crazypaving Bronch is usually sufficient to make dx Filling of alveolar spaces with PAS + lipoproteinaceous material Tx Whole lung lavage (20L) GM-CSF


50 Chest imaging


51 Path
52 Pulmonary Langerhans Cell Histiocytosis Isolated lung involvement (85%) Multisystem Syndrome (lungs, bone, skin, pituitary, liver, LN, thyroid) 20 to 40 CIGARETTE smokers (90% current smokers) Nonproductive cough, dyspnea, pleuritic CP 1/3 constitutional symptoms PTX 15-25% Extrapulmonary sx (bone pain, DI, rash, LAD)
53 CT
54 Treatment Smoking cessation In most, sx stabilize with quitting alone Corticosteroids in those with progressive disease or persistent sx despite quitting Prognosis 50% respond to no tx other then smoking cessation 10-20% rapid progression -> fibrotic lung disease 5 yr survival 74% Referral for lung transplant (recurrence may occur)
55 Lymphangioleiomyomatosis (LAM) Almost exclusively premenopausal women Dyspnea, cough, CP, PTX 50% initial presentation PTX (81% during course of disease) Chylous effusions, ascites 50% renal angiomyolipomas Associated with TSC-2 Proliferation of atypical SM cells around airways blood vessels, lymphatics

56 CT

57 Bleb vs. Cyst

58 Pathology
59 Treatment Pregnancy and supplemental estrogen may accelerate disease Hormonal manipulation Oophrectomy Progestin Tamoxifen LH-RH Most will have progressive decline and will need to be referred for transplant (may recur in allograft) Median survival 8-10 yrs
60 LIP Idiopathic, RA, Sjogren s, HIV, Congenital Immunodeficiency 30 to 50, predominantly female Constitutional sx Slowly progressive DOE Bibasilar crackles, LAD CT with GG infiltrates, centrilobular nodules, LAD, cysts Path: Dense interstitial infiltrates of lymphocytes, plasma cells, and other lymphoreticular elements
61 CT

62 Pathology
63 Treatment Corticosteroids +/- immunomodulation therapy Most stabilize or improve (60%) 40% rapid decline 5 yr mortality 60%? Possible malignant transformation to lymphoma
64 Summary Take a HISTORY Identify an underlying condition, may effect treatment and prognosis Fibrosis = BAD
65 Case #1 66 yo female with dry cough and 1 block (had been attributed to aging, weight gain) for up to 2 yrs On ROS: intermittent heartburn, myalgias, joint pain in wrists and elbows,?raynaud s phenomenon Social Hx unremarkable Family Hx + mother with pulm fibrosis (no bx performed)
66 PE remarkable for bibasilar crackles, periungal erythema, slt thickened skin on her fingers PFTs: FEV (81%), FVC 2.45 (78%), ratio 83%, DLCO 65% with DLCO/VA 110% HRCT: Subpleural interstitial thickening with mild contraction bronchiectasis
67 Serologies sent: ANA 1:160 homogeneous Scl-70, RF, anti-ccp, dsdna, SSA, SSB, CPK, Aldolase negative ECHO showed mild pulm htn
68 Scleroderma Diagnosis
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Case Presentations in ILD. Harold R. Collard, MD Department of Medicine University of California San Francisco
 Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases
 Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy
 Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
CLEARING THE AIR ON DIFFUSE PARENCHYMAL (INTERSTITIAL) LUNG DISEASE (ILD)
 LUNG DISEASE (ILD)") CLEARING THE AIR ON DIFFUSE PARENCHYMAL (INTERSTITIAL) LUNG DISEASE (ILD) David Northrop MBA, RRT Assistant Director of Respiratory Therapy Services The University of Kansas Health System Clinical Assistant
CLEARING THE AIR ON DIFFUSE PARENCHYMAL (INTERSTITIAL) LUNG DISEASE (ILD) David Northrop MBA, RRT Assistant Director of Respiratory Therapy Services The University of Kansas Health System Clinical Assistant
Interstitial Lung Diseases(ILD) By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun
 By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun") Interstitial Lung Diseases(ILD) By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun. 26.11.11 Introduction Interstitial Lung Diseases (ILD) are group of diseases that affect the interstitium of the lungs,
Interstitial Lung Diseases(ILD) By : Dr. Shaher M. Samrah Done by : Ibrahim M. sun. 26.11.11 Introduction Interstitial Lung Diseases (ILD) are group of diseases that affect the interstitium of the lungs,
Lines and crackles. Making sense of ILD
 Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Update on Therapies for Idiopathic Pulmonary Fibrosis. Outline
 Update on Therapies for Idiopathic Pulmonary Fibrosis Paul Wolters Associate Professor University of California, San Francisco Outline Classification of Interstitial lung disease Clinical classification
Update on Therapies for Idiopathic Pulmonary Fibrosis Paul Wolters Associate Professor University of California, San Francisco Outline Classification of Interstitial lung disease Clinical classification
Multidisciplinary Diagnosis in Action: Challenging Case Presentations
 Multidisciplinary Diagnosis in Action: Challenging Case Presentations Interstitial Lung Disease: Advances in Diagnosis and Management UCSF CME November 8, 2014 Case 1 69 yo M 3 year history of intermittent
Multidisciplinary Diagnosis in Action: Challenging Case Presentations Interstitial Lung Disease: Advances in Diagnosis and Management UCSF CME November 8, 2014 Case 1 69 yo M 3 year history of intermittent
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Disclosures. Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting. Relevant financial relationships: None. Off-label usage: None
 Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Radiologic Approach to Smoking Related Interstitial Lung Disease
 Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Case 4 History. 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar
 Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines
 Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
CTD-related Lung Disease
 13 th Cambridge Chest Meeting King s College, Cambridge April 2015 Imaging of CTD-related Lung Disease Dr Sujal R Desai King s College Hospital, London Disclosure Statement No Disclosures / Conflicts of
13 th Cambridge Chest Meeting King s College, Cambridge April 2015 Imaging of CTD-related Lung Disease Dr Sujal R Desai King s College Hospital, London Disclosure Statement No Disclosures / Conflicts of
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates
 and Updates") Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Daria Manos RSNA 2016 RC 401. https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html
 Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Non-neoplastic Lung Disease II
 Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies A Rheumatologist s Approach to Interstitial Lung Disease Outline ILD classification and patterns in CTD The clinical landscape and
Annual Rheumatology & Therapeutics Review for Organizations & Societies A Rheumatologist s Approach to Interstitial Lung Disease Outline ILD classification and patterns in CTD The clinical landscape and
International consensus statement on idiopathic pulmonary fibrosis
 Eur Respir J 2001; 17: 163 167 Printed in UK all rights reserved Copyright #ERS Journals Ltd 2001 European Respiratory Journal ISSN 0903-1936 PERSPECTIVE International consensus statement on idiopathic
Eur Respir J 2001; 17: 163 167 Printed in UK all rights reserved Copyright #ERS Journals Ltd 2001 European Respiratory Journal ISSN 0903-1936 PERSPECTIVE International consensus statement on idiopathic
IPF: Epidemiologia e stato dell arte
 IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
Cystic Lung Disease. Cristopher A. Meyer, MD
 Cystic Lung Disease Cristopher A. Meyer, MD Air filled structure with definable wall typically less than 1 mm thick Cris A. Meyer, M.D. Professor of Radiology University of Wisconsin School of Medicine
Cystic Lung Disease Cristopher A. Meyer, MD Air filled structure with definable wall typically less than 1 mm thick Cris A. Meyer, M.D. Professor of Radiology University of Wisconsin School of Medicine
Pathologic Assessment of Interstitial Lung Disease
 Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
NONE OVERVIEW FINANCIAL DISCLOSURES UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF (UIP) FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP
 FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP") UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
I have no relevant conflicts of interest to disclose
 I have no relevant conflicts of interest to disclose Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures
I have no relevant conflicts of interest to disclose Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
Epidemiology and classification of smoking related interstitial lung diseases
 Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
Epidemiology and classification of smoking related interstitial lung diseases Šterclová M. Department of Respiratory Diseases, Thomayer Hospital, Prague, Czech Republic Supported by an IGA Grant No G 1207
DIFFERENCES IN FIBROPROLIFERATIVE HEALING IN EXOGENEOUS AND IDIOPATHIC ILDs. ARE THERE ANY?
 NIHR Southampton Respiratory Biomedical Research Unit DIFFERENCES IN FIBROPROLIFERATIVE HEALING IN EXOGENEOUS AND IDIOPATHIC ILDs. ARE THERE ANY? Fibrosing Interstitial Lung Diseases CPFS/WASOG/AIPO/ERS
NIHR Southampton Respiratory Biomedical Research Unit DIFFERENCES IN FIBROPROLIFERATIVE HEALING IN EXOGENEOUS AND IDIOPATHIC ILDs. ARE THERE ANY? Fibrosing Interstitial Lung Diseases CPFS/WASOG/AIPO/ERS
Disclosures. Clinical Approach: Evaluating CTD-ILD for the pulmonologist. ILD in CTD. connective tissue disease or collagen vascular disease
 Disclosures Clinical Approach: Evaluating CTD-ILD for the pulmonologist Industry relationships: Actelion, atyr Pharma, Boehringer-Ingelheim, Genentech- Roche, Gilead Aryeh Fischer, MD Associate Professor
Disclosures Clinical Approach: Evaluating CTD-ILD for the pulmonologist Industry relationships: Actelion, atyr Pharma, Boehringer-Ingelheim, Genentech- Roche, Gilead Aryeh Fischer, MD Associate Professor
IPF - Inquadramento clinico
 IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Diagnostic challenges in IPF
 Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Unpaid scientific collaborator & advisor with Veracyte, Inc.
 Diagnosis and Classification of Idiopathic Interstitial Pneumonias: Role of Histopathology in the Golden Age of Consensus Jeffrey L. Myers, M.D. A. James French Professor of Diagnostic Pathology Vice Chair
Diagnosis and Classification of Idiopathic Interstitial Pneumonias: Role of Histopathology in the Golden Age of Consensus Jeffrey L. Myers, M.D. A. James French Professor of Diagnostic Pathology Vice Chair
Bronkhorst colloquium Interstitiële longziekten. Katrien Grünberg, klinisch patholoog
 Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
Bronkhorst colloquium 2013-2014 Interstitiële longziekten De pathologie achter de CT Katrien Grünberg, klinisch patholoog K.grunberg@vumc.nl Preparing: introduction and 3 cases The introduction on microscopic
The connective tissue disorders (CTDs), also. Pivotal clinical dilemmas in collagen vascular diseases associated with interstitial lung involvement
, also. Pivotal clinical dilemmas in collagen vascular diseases associated with interstitial lung involvement") Eur Respir J 2009; 33: 882 896 DOI: 10.1183/09031936.00152607 CopyrightßERS Journals Ltd 2009 REVIEW Pivotal clinical dilemmas in collagen vascular diseases associated with interstitial lung involvement
Eur Respir J 2009; 33: 882 896 DOI: 10.1183/09031936.00152607 CopyrightßERS Journals Ltd 2009 REVIEW Pivotal clinical dilemmas in collagen vascular diseases associated with interstitial lung involvement
Diffuse Interstitial Lung Diseases: Is There Really Anything New?
 : Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
: Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete Prague, June 2014
 Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Idiopathic Pulmonary Fibrosis Treatable and Not Idiopathic
 Idiopathic Pulmonary Fibrosis Treatable and Not Idiopathic Brett Ley, MD University of California San Francisco CTS 1/26/18 Disclosures Speaker s bureau honorarium from Genentech (makers of pirfenidone)
Idiopathic Pulmonary Fibrosis Treatable and Not Idiopathic Brett Ley, MD University of California San Francisco CTS 1/26/18 Disclosures Speaker s bureau honorarium from Genentech (makers of pirfenidone)
Dr.kassim.m.sultan F.R.C.P
 Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
Dr.kassim.m.sultan F.R.C.P inflammatory disorder of the lung, involving alveolar walls and terminal airways, that is induced, in a susceptible host, by repeated inhalation of a variety of organic agents.
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT
 Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Disclosures. Traditional Paradigm. Overview 4/17/2010. I have relationships with the following organizations and companies:
 Disclosures Pharmacological Therapy for ILD What to Use and How to Use It Harold R Collard MD Interstitial Lung Disease Program University of California San Francisco (UCSF) I have relationships with the
Disclosures Pharmacological Therapy for ILD What to Use and How to Use It Harold R Collard MD Interstitial Lung Disease Program University of California San Francisco (UCSF) I have relationships with the
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings
 Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings Poster No.: C-2358 Congress: ECR 2013 Type: Educational Exhibit Authors: V. Cuartero Revilla, M. Nogueras Carrasco, P. Olmedilla
Smoking-related Interstitial Lung Diseases: High-Resolution CT Findings Poster No.: C-2358 Congress: ECR 2013 Type: Educational Exhibit Authors: V. Cuartero Revilla, M. Nogueras Carrasco, P. Olmedilla
Spectrum of Cystic Lung Disease and its Mimics. Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology
 Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Definition, classification and epidemiology
 Interstitial Lung Diseases Definition, classification and epidemiology Haluk Türktaş Professor of Pulmonary Medicine Gazi University Ankara Interstitial Lung Diseases Definition of ILD A diverse group
Interstitial Lung Diseases Definition, classification and epidemiology Haluk Türktaş Professor of Pulmonary Medicine Gazi University Ankara Interstitial Lung Diseases Definition of ILD A diverse group
Bronchiolar disorders: Current perspective on diagnosis & management. Puneet Malhotra Senior Resident, Dept. of Pulmonary Medicine, PGIMER
 Bronchiolar disorders: Current perspective on diagnosis & management Puneet Malhotra Senior Resident, Dept. of Pulmonary Medicine, PGIMER Anatomic considerations Classification Diagnostic approach Specific
Bronchiolar disorders: Current perspective on diagnosis & management Puneet Malhotra Senior Resident, Dept. of Pulmonary Medicine, PGIMER Anatomic considerations Classification Diagnostic approach Specific
The Pathologic Manifestations of Small Airway Disease. Samuel A. Yousem, MD. Small Airway Disease (SAD) SAD
 SAD") The Pathologic Manifestations of Small Airway Disease Samuel A. Yousem, MD Small Airway Disease (SAD) A clinicopathologic syndrome reflecting a CHRONIC inflammatory and cicatricial process primarily affecting
The Pathologic Manifestations of Small Airway Disease Samuel A. Yousem, MD Small Airway Disease (SAD) A clinicopathologic syndrome reflecting a CHRONIC inflammatory and cicatricial process primarily affecting
C h a p t e r 1 3 Interstitial Lung Disease
 C h a p t e r 1 3 Interstitial Lung Disease Shirish P Shah 1, Somesh Chaudhary 2, P Shetty 2 1 Consultant Chest Physician, Nanavati Hospital, Mumbai, Former Head of Department of Chest Medicine, BYL Nair
C h a p t e r 1 3 Interstitial Lung Disease Shirish P Shah 1, Somesh Chaudhary 2, P Shetty 2 1 Consultant Chest Physician, Nanavati Hospital, Mumbai, Former Head of Department of Chest Medicine, BYL Nair
CASE OF THE MONTH. Lung Disease in Rheumatoid Arthritis
 CASE OF THE MONTH Lung Disease in Rheumatoid Arthritis 61 year old male Maōri Height: 174 cm Weight: 104.6kg BMI: 34.55 Problems 1. Rheumatoid related interstitial lung disease with UIP pattern 2. Secondary
CASE OF THE MONTH Lung Disease in Rheumatoid Arthritis 61 year old male Maōri Height: 174 cm Weight: 104.6kg BMI: 34.55 Problems 1. Rheumatoid related interstitial lung disease with UIP pattern 2. Secondary
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Progress in Idiopathic Pulmonary Fibrosis
 Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Pulmonary Manifestations Of Skeletal Disorders
 Pulmonary Manifestations Of Skeletal Disorders U. A. Saeed, MBBS FCPS, J. Nair, MBBS MD, R. Khosla, MD FRCR, K. Sayegh, MD FRCPC, J. Kosiuk, MD FRCPC, J. Taylor, MD FRCPC; Department of Radiology, McGill
Pulmonary Manifestations Of Skeletal Disorders U. A. Saeed, MBBS FCPS, J. Nair, MBBS MD, R. Khosla, MD FRCR, K. Sayegh, MD FRCPC, J. Kosiuk, MD FRCPC, J. Taylor, MD FRCPC; Department of Radiology, McGill
The Egyptian Journal of Hospital Medicine (July 2017) Vol.68 (2), Page
 Vol.68 (2), Page") The Egyptian Journal of Hospital Medicine (July 2017) Vol.68 (2), Page 1135-1140 Role of High Resolution Computed Tomography in Diagnosis of Interstitial Lung Diseases in Patients with Collagen Diseases
The Egyptian Journal of Hospital Medicine (July 2017) Vol.68 (2), Page 1135-1140 Role of High Resolution Computed Tomography in Diagnosis of Interstitial Lung Diseases in Patients with Collagen Diseases
Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy
 Idiopathic Pulmonary Fibrosis Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy JMAJ 46(11): 469 474, 2003 Yukihiko SUGIYAMA Professor, Division of Pulmonary Medicine, Department of
Idiopathic Pulmonary Fibrosis Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy JMAJ 46(11): 469 474, 2003 Yukihiko SUGIYAMA Professor, Division of Pulmonary Medicine, Department of
Challenges in the Diagnosis of Interstitial Lung Disease
 Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Diagnosing ILD. What is important in 2016? Chris Grainge
 Diagnosing ILD What is important in 2016? Chris Grainge Senior Staff Specialist Respiratory Medicine John Hunter Hospital Conjoint A/Prof University of Newcastle Conflict of interest I have acted as a
Diagnosing ILD What is important in 2016? Chris Grainge Senior Staff Specialist Respiratory Medicine John Hunter Hospital Conjoint A/Prof University of Newcastle Conflict of interest I have acted as a
Chest imaging II. Interstitial lung diseases
 Chest imaging II. Interstitial lung diseases Dávid L. Tárnoki MD, PhD Ádám D. TárnokiMD, PhD Department of Radiology Semmelweis University Topics 1. Interstitial lung diseases 2. Occupational lung diseases
Chest imaging II. Interstitial lung diseases Dávid L. Tárnoki MD, PhD Ádám D. TárnokiMD, PhD Department of Radiology Semmelweis University Topics 1. Interstitial lung diseases 2. Occupational lung diseases
Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment
 Prague, June 2014 Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Prague, June 2014 Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Case Presentation. Case Presentation (continued) PHYSICAL EXAMINATION. 60 year old college professor dyspnea with exertion dry cough, throat clearing
 PHYSICAL EXAMINATION. 60 year old college professor dyspnea with exertion dry cough, throat clearing") Primary Care Medicine: Concepts and Controversies Thursday, February 18, 21 Fiesta Americana Puerto Vallarta, Mexico Interstitial Lung Disease: A Clinician s Approach to Diagnosis and Management Talmadge
Primary Care Medicine: Concepts and Controversies Thursday, February 18, 21 Fiesta Americana Puerto Vallarta, Mexico Interstitial Lung Disease: A Clinician s Approach to Diagnosis and Management Talmadge
Hypersensitivity Pneumonitis Common Diagnostic and Treatment Dilemmas
 Hypersensitivity Pneumonitis Common Diagnostic and Treatment Dilemmas Rishi Raj MD Director, Interstitial Lung Diseases Program Clinical Professor of Pulmonary and Critical Care Medicine Stanford University
Hypersensitivity Pneumonitis Common Diagnostic and Treatment Dilemmas Rishi Raj MD Director, Interstitial Lung Diseases Program Clinical Professor of Pulmonary and Critical Care Medicine Stanford University
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than
 TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
Radiological Imaging of Drug-Induced Pulmonary Lesions
 Review Article imedpub Journals www.imedpub.com Journal of Clinical Radiology and Case Reports Radiological Imaging of Drug-Induced Pulmonary Lesions D souza M *, Rajiah P, Khan A and Irion K Department
Review Article imedpub Journals www.imedpub.com Journal of Clinical Radiology and Case Reports Radiological Imaging of Drug-Induced Pulmonary Lesions D souza M *, Rajiah P, Khan A and Irion K Department
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Spectrum of Findings on HRCT in Evaluation of Interstitial Lung Diseases: A Single Centre Prospective Observational Study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 11 Ver. 7 (November. 2018), PP 53-63 www.iosrjournals.org Spectrum of Findings on HRCT in Evaluation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 11 Ver. 7 (November. 2018), PP 53-63 www.iosrjournals.org Spectrum of Findings on HRCT in Evaluation
Idiopathic interstitial pneumonias (IIPs) are a group of
 are a group of") SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
Interstitial Lung Disease in the Connective Tissue Diseases
 Interstitial Lung Disease in the Connective Tissue Diseases Danielle Antin-Ozerkis, MD a, *, Ami Rubinowitz, MD b, Janine Evans, MD c, Robert J. Homer, MD, PhD d, Richard A. Matthay, MD e KEYWORDS Connective
Interstitial Lung Disease in the Connective Tissue Diseases Danielle Antin-Ozerkis, MD a, *, Ami Rubinowitz, MD b, Janine Evans, MD c, Robert J. Homer, MD, PhD d, Richard A. Matthay, MD e KEYWORDS Connective
Interstitial Lung Disease
 Interstitial Lung Disease Interstitial lung disease (ILD) is a broad category of lung diseases that includes more than 130 disorders which are characterized by scarring (i.e. fibrosis ) and/or inflammation
Interstitial Lung Disease Interstitial lung disease (ILD) is a broad category of lung diseases that includes more than 130 disorders which are characterized by scarring (i.e. fibrosis ) and/or inflammation
How to identify interstitial pneumonias.
 How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
How to identify interstitial pneumonias. Poster No.: C-0804 Congress: ECR 2014 Type: Educational Exhibit Authors: S. claret loaiza, M. C. Cañete Moslero, R. Carreño Gonzalez, C. de la Torre; Malaga/ES
Careful histopathological evaluation has shown the traditionally clinical diagnosis of
 Demystifying Idiopathic Interstitial Pneumonia Harold R. Collard, MD; Talmadge E. King, Jr, MD REVIEW ARTICLE Careful histopathological evaluation has shown the traditionally clinical diagnosis of idiopathic
Demystifying Idiopathic Interstitial Pneumonia Harold R. Collard, MD; Talmadge E. King, Jr, MD REVIEW ARTICLE Careful histopathological evaluation has shown the traditionally clinical diagnosis of idiopathic
Interstitial Lung Disease in Children
 Interstitial Lung Disease in Children Sankaran Krishnan, MD, MPH, FAAP Associate Professor, Pediatrics and Public Health Associate Program Director, Pediatric Pulmonology New York Medical College Maria
Interstitial Lung Disease in Children Sankaran Krishnan, MD, MPH, FAAP Associate Professor, Pediatrics and Public Health Associate Program Director, Pediatric Pulmonology New York Medical College Maria
Pleuropulmonary complications 50% incidence. More in patients with more severe chronic articular disease, with high titers of RA factor, patients
 Dr Romi Singla Pleuropulmonary complications 50% incidence. More in patients with more severe chronic articular disease, with high titers of RA factor, patients with subcutaneous nodules plus other systemic
Dr Romi Singla Pleuropulmonary complications 50% incidence. More in patients with more severe chronic articular disease, with high titers of RA factor, patients with subcutaneous nodules plus other systemic
Guidelines for Diagnosis and Treatment of IPF
 Guidelines for Diagnosis and Treatment of IPF Katerina Antoniou, MD, PhD Lecturer in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete Classification of Interstitial Lung Disease
Guidelines for Diagnosis and Treatment of IPF Katerina Antoniou, MD, PhD Lecturer in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete Classification of Interstitial Lung Disease
ILD and systemic disease
 Department for Pulmonology, University Hospital Berne ILD and systemic disease Dr. med. Manuela Funke-Chambour Oberärztin I Female patient, born 1945 Portuguese Presented with cough and dyspnea, no other
Department for Pulmonology, University Hospital Berne ILD and systemic disease Dr. med. Manuela Funke-Chambour Oberärztin I Female patient, born 1945 Portuguese Presented with cough and dyspnea, no other
DIAGNOSTIC NOTE TEMPLATE
 DIAGNOSTIC NOTE TEMPLATE SOAP NOTE TEMPLATE WHEN CONSIDERING A DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS (IPF) CHIEF COMPLAINT HISTORY OF PRESENT ILLNESS Consider IPF as possible diagnosis if any of the
DIAGNOSTIC NOTE TEMPLATE SOAP NOTE TEMPLATE WHEN CONSIDERING A DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS (IPF) CHIEF COMPLAINT HISTORY OF PRESENT ILLNESS Consider IPF as possible diagnosis if any of the
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases
 Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
9/15/11. Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September Scleroderma. Hard skin
 Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
A case of a patient with IPF treated with nintedanib. Prof. Kreuter and Prof. Heussel
 A case of a patient with IPF treated with nintedanib Prof. Kreuter and Prof. Heussel Case Overview This case describes the history of a patient with IPF who, at the time of diagnosis, had symptoms typical
A case of a patient with IPF treated with nintedanib Prof. Kreuter and Prof. Heussel Case Overview This case describes the history of a patient with IPF who, at the time of diagnosis, had symptoms typical
Interstitial Lung Disease
 Interstitial Lung Disease Interstitial lung disease (ILD) is a broad category of lung diseases that includes more than 130 disorders which are characterized by scarring (i.e. fibrosis ) and/or inflammation
Interstitial Lung Disease Interstitial lung disease (ILD) is a broad category of lung diseases that includes more than 130 disorders which are characterized by scarring (i.e. fibrosis ) and/or inflammation
Pulmonary Test Brenda Shinar
 Pulmonary Test 2016 Brenda Shinar 1. What is a Renal Tubular Acidosis? What is the difference between the types of RTAs in terms of who gets them and how to diagnose them? Type 1, 2, and 4? Metabolic acidosis
Pulmonary Test 2016 Brenda Shinar 1. What is a Renal Tubular Acidosis? What is the difference between the types of RTAs in terms of who gets them and how to diagnose them? Type 1, 2, and 4? Metabolic acidosis
Challenges in the Diagnosis of Interstitial Lung Disease
 Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Histopathologic Approach to Interstitial Lung Disease
 Histopathologic Approach to Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu Disclosures I have nothing to disclose 1 Why? Much of interstitial lung disease biopsies
Histopathologic Approach to Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept of Pathology kirk.jones@ucsf.edu Disclosures I have nothing to disclose 1 Why? Much of interstitial lung disease biopsies
Mimics in chest disease: interstitial opacities
 Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation