Oncologic Emergencies. Angelina The, MD Lynn Cancer Institute August 30, 2016
|
|
|
- Warren McBride
- 5 years ago
- Views:
Transcription
1 Oncologic Emergencies { Angelina The, MD Lynn Cancer Institute August 30, 2016
2 What constitutes an oncologic emergency? Complications arising from Cancer Paraneoplastic syndrome Treatment of cancer Requires immediate attention and reversal
3 Outline Hyperleukocytosis Tumor lysis syndrome Disseminated intravascular coagulation Hypercalcemia Thrombotic thrombocytopenic purpura/hus Hyperviscosity Spinal cord compression SVC Syndrome

4
5 Hyperleukocytosis 5-20% of adults dx d with AML 3 main complications of HL include: Leukostasis DIC Tumor lysis syndrome Early mortality increased in AML patients with HL Shorter overall survival

6 Christoph Röllig, and Gerhard Ehninger Blood 2015;125: Pathogenetic mechanisms in leukostasis

7
8 Clinical Unexplained fever Fatigue Weight loss Bone pain Bruising/Bleeding Gum hypertrophy Hepatosplenomegaly AMS Hypoxia Lab Abnormal CBC Leukocytosis or pancytopenia Coagulopathy/DIC High LDH Peripheral smear

9 Management of HL *Definitive treatment* Hydroxyurea 1-3 g PO q 6 hours Leukopheresis
10 Leukoreduction Apheresis Rapidly removes excess leukocytes by mechanical separation Single round of leukopheresis reduced WBC by 10-70% Debate: -Majority of leukemic burden in marrow -Beneficial clinical effect on early outcomes could not be shown consistently in clinical trials
11 Leukoreduction Apheresis Contraindications Hemodynamic instability Coagulopathy Cardiovascular comorbidites No evidence for clinical benefit in HL patients without leukostasis symptoms Given pros and cons, routine leukophoresis can not be routinely recommended.

12 Tumor Lysis Syndrome TLS is the most common oncologic emergency. Constellation of metabolic abnormalities resulting from either spontaneous or chemotherapy-induced tumor cell death {
13 Tumor cell lysis Hyperkalemia Cardiac arrhythmias Release of DNA Purines Hyperphosphatemia Allopurinol Rasburicase Hypoxanthine/Xanthine Xanthine oxidase Uricase Uric acid Allantoin Ca-phos precipitation Hypocalcemia Urate nephropathy Ca-phos nephropathy
14 Risk factors for TLS Clinical Large tumor burden with rapid cell turnover (acute leukemias, lymphomas) Sensitivity of tumors to chemotherapy Eldery/reduced GFR Volume depletion Laboratory Elevated LDH Baseline hyperuricemia Baseline renal dysfunction
15 Prophylaxis against TLS Aggressive hydration Prevent uric acid deposition into renal tubules Urinary alkalinization Target urine ph 7 Allopurinol 300 mg daily to BID Rasburicase
16 Disseminated Intravascular Coagulopathy Loss of normal hemostatic control in response to sustained and systemic cell injury
17 Triggers of DIC -Sepsis/severe infection -Trauma/burn/heatstroke -Malignancy -Solid tumors -Acute leukemia -Obstetrical conditions -Amniotic fluid embolism -Abruptio placentae -HELLP syndrome -Vascular abnormalities -Kasabach-Merrit syndrome -Other vascular malformations -Aortic aneurysms -Severe allergic/toxic reactions -Severe immunologic reactions (e.g., transfusion reaction)
18 Mechanisms in DIC 2013 by American Society of Hematology Cheng Hock Toh, and Yasir Alhamdi Hematology 2013;2013:
19 Relevance of DIC Microvascular thrombosis Organ dysfunction Bleeding Increased mortality
20 Management of DIC = Treatment of underlying cause
21 Management of DIC Blood product support Platelets in the bleeding patient if < /L Fresh frozen plasma if bleeding and prolonged PT and PTT Cryoprecipitate (2 pools) can be considered in patients with bleeding and fibrinogen levels less than 1.5 g/l Modulating profibrinolytic activity Tranexamic acid Modulating thrombin generation Heparin/LMWH Antithrombin controversial APC Prowess-SHOCK Trial showed no benefit


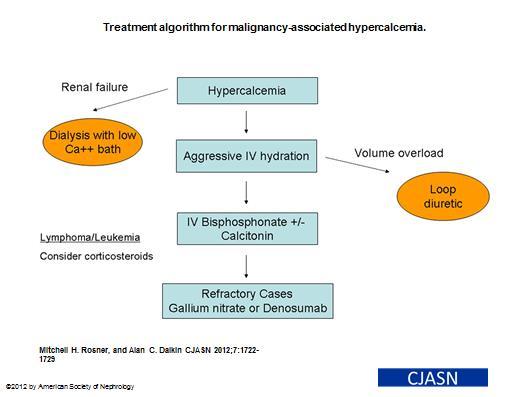
22 Hypercalcemia 20-30% of cancer patients Myeloma, lymphomas, cancers of prostate, lung, breast, and kidneys

23
24 Hypercalcemia: Symptoms N/V Constipation Decreased mental status Renal dysfunction
25
26 Thrombotic Thrombocytopenic Purpura Characterized by microangiopathic hemolytic anemia, thrombocytopenia, and microvascular thrombosis Mortality rate of TTP without treatment ~ 80-90%
27 Acquired TTP Usually occurs in older children and adults Secondary to IgG autoantibody against ADAMTS13 May be idiopathic or associated with mitomycin C, cyclosporin, tacrolimus, quinine, ticlopidine, clopidogrel, TBI, allogeneic BMT, solid organ txpt, or pregnancy/postpartum state
28 In the U.S., ~1000 new cases diagnosed per year Most patients range in age from Slight female predominance 3:2 Relapses occur in ~1/3 of those who achieve remissions.
29 Pathophysiology of TTP vwf ADAMTS13 Inhibitor of ADAMTS13
30 ADAMTS13 A disintegrin and metalloprotease with eight thrombospondin type 1 repeats #13 a family of 19 distinct ADAMTS enzymes identified to date Encoded on chromosome 9q34 Produced by the liver
31 Normal release of vwf into circulation P selectin Stress! Weibel- Palade body Endothelial Cell Sadler, et al Hematology
32 Normal release of vwf into circulation P selectin Cleaved ULVWF Multimers 200 kd Stress! Weibel- Palade body ADAMTS13 cleaving protease Endothelial Cell Sadler, et al Hematology
33 ADAMTS13 inhibitors: no cleavage of ULVWF P selectin Stress! Weibel- Palade body Endothelial Cell Sadler, et al Hematology



34 ADAMTS13 inhibitors: no cleavage of ULVWF Sadler, et al Hematology
35 Absence of ADAMTS13: ULvWF predominance ULvWF adheres to platelets and causes platelets to aggregate ULvWF has greater binding affinity to platelets than smaller vwf, possibly secondary to more effective exposure of gp1bα ULvWF may detach from endothelial cells in the presence of fluid shear stress/increasing torque generated by platelet adherence to ULvWF and embolize to downstream microvessels resulting in organ ischemia
36 Classic TTP pentad 1. Neurologic abnormality 2. Renal failure 3. Thrombocytopenia 4. Microangiopathic hemolytic anemia (MAHA) 5. Fever Amorosi et al Thombotic thrombocytopenic purpura: report of 16 cases and review of the literature. Medicine (Baltimore). 45:
37 Laboratory Findings Thrombocytopenia (often <20K) Increased LDH secondary to lysis and diffuse organ ischemia RBC fragmentation (e.g. schistocytes and helmet cells) due to passage of RBCs through microvessels that are partially occluded by plt aggregates

38
39 Comparison of plasma exchange with plasma infusion in the treatment of TTP (p=0.036) Rock et al Comparison of plasma exchange with plasma infusion in the treatment of TTP. NEJM. 325 (6):
40 Comparison of plasma exchange with plasma infusion in the treatment of TTP Conclusions: 1. Plasma exchange is superior to plasma infusion in the treatment of TTP, both at the end of the first cycle of tx and after six months. 2. The significantly lower death rate when plasma is exchanged suggests a possible role for the removal of some plasma constituent in addition to the supply of fresh plasma. Rock et al Comparison of plasma exchange with plasma infusion in the treatment of TTP. NEJM. 325 (6):
41 Plasma Exchange No defined schedule Performed on a daily basis until platelet count reaches ~150 (also monitor for normalization of Hb, LDH, and any clinical abnormalities at diagnosis), then taper If response to initial treatment is poor, may need intensification of plasma volume exchange (1.5 vs. 1.0 or bid treatment) or initiation of immunosuppressive agents
42 Glucocorticoids Prednisone 1 mg/kg/d or Methylprednisolone 125 mg IV bid Suppresses production of ADAMTS13 autoantibodies by inducing lymphocytic apoptosis
43 Acquired HUS Occurs in 9-30% of children about a week after an episode of bloody diarrhea precipitated by ingestion of enterohemorrhagic bacteria that produce the shiga toxin (e.g. e.coli 0157:H7 and shigella dysenteriae) Sources include contaminated milk, cheese, or meat Common in Buenos Aires, Argentina, and Calgary, Canada Moake et al Thrombotic Microangiopathies. New England Journal of Medicine. 347 (8):
44 Role of Shiga Toxin, Cytokines, ulvwf, and Cellular Injury -Epithelial cells/monocytes release cytokines and chemokines. -Endothelial cells secrete ULVWF and activate plts. Shiga toxin CH glc gal gal Globotriaosylceramide receptor
45 HUS - Treatment Plasma Exchange Supportive IVF s RBC transfusions Dialysis if appropriate
46 Atypical HUS Accounts for 5-10% of HUS Mortality rate ~50% vs 3-5% for typical, acquired HUS About 50% relapse, and over 33% require long-term dialysis; 16% who receive kidney allografts lose function of graft within 1 mo. Noris, et al Hypocomplementemia discloses genetic predisposition to HUS and TTP: role of factor H abnormalities. J Am Soc Nephrol. 10:
47 ahus Due to a regulatory protein defect in the alternative complement pathway Results in excessive activation, endothelial damage, platelet activation, thrombus formation C3bBb Factor H C3b Bb C3b C3b Inactive C3b Cell lysis
48 ahus If suspicion for ahus, begin plasma exchange but if no improvement after 3-5 days, may be unresponsive eculizumab Eculizumab Recombinant humanized monoclonal antibody that target C5 Blocks cleavage of C5 and prevents formation of membrane attack complex
49 Hyperviscosity Increased serum viscosity resulting from increased serum Ig s Waldenstrom s macroglobulinemia/myeloma - Symptoms Typically occur when serum viscosity >5 cp Mucosal bleeding* CNS symptoms Cardiopulmonary symptoms

50 Tx for HVS: Plasmapheresis Effective short-term treatment for HVS in WM A relatively small reduction in IgM concentration has a significant effect on lowering serum viscosity. Bleeding is the most common sign of HVS Urgent plasmapheresis should be carried out for patients experiencing visual symptoms to reduce the likelihood of blindness from retinal hemorrhages/retinal detachment. Plasma exchange reduces plasma viscosity approximately 20% to 30% per session.

51

52
53 Epidural Spinal Cord Compression Major complications include pain and irreversible loss of neurologic function Goals of therapy Pain control Preservation of neuro function

54
55 ESCC - Therapy Symptomatic Tx Glucocorticoids Opioids Aggressive bowel regimen Definitive Tx Assess spinal stability Spine Instability Neoplasia Score Surgery -> RT +/-Chemotherapy

56 Superior vena cava syndrome

57 Typical clinical findings in a patient with superior vena cava syndrome A: Plethora B: Distended jugular veins C: Cyanosis D. Swelling hand/arm E. Collateral circulation F. Compression of SVC/tracheal compression Philipp M Lepper et al. Respir Care 2011;56: (c) 2012 by Daedalus Enterprises, Inc.
58 SVC syndrome - Mechanism SVC surrounded by relatively rigid structures (sternum, trachea, right bronchus, aorta) Extends ~6-8 cm, from inominate veins to right atrium SVC syndrome causes by neoplastic invasion of venous wall with associated thrombus or by extrinsic compression
59 Prompts collateral venous return through: -Azygous venous system -Internal mammary venous system -Long thoracic venous system Develops in 5-10% of patients with right sided intrathoracic mass lesions Majority of cases due to bronchogenic cancer; 10-15% due to lymphoma Prognosis depends on underlying histology of tumor, presence of laryngeal and/or cerebral edema Symptoms often absent until obstruction near complete -Dyspnea -Facial and arm swelling -Chest pain -Dysphagia -Change in vision -Head fullness, headache
60 Treatment of SVC syndrome Supportive Elevation of head Oxygen Corticosteroids Diuretics Definitive Treatment Chemotherapy Radiation Stenting, particularly while bx being pursued

61
62 The End
Hematologic Emergency. Le Wang, MD, PhD Hematology & Oncology
 Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
* Renal insufficiencies
 Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
Index. Note: Page numbers of article numbers are in boldface type.
 Index Note: Page numbers of article numbers are in boldface type. A Abdomen, acute, as cancer emergency, 381 399 in cancer patients, etiologies unique to, 390 392 in perforation, 388 surgery of, portal
Index Note: Page numbers of article numbers are in boldface type. A Abdomen, acute, as cancer emergency, 381 399 in cancer patients, etiologies unique to, 390 392 in perforation, 388 surgery of, portal
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
HEMATOLOGIC & ONCOLOGIC EMERGENCIES MEG KELLEY MS, FNP- BC, OCN
 HEMATOLOGIC & ONCOLOGIC EMERGENCIES MEG KELLEY MS, FNP- BC, OCN COURSE OBJECTIVES At the conclusion of this presentation, participants should be able to: 1. Define hematological and oncologic (heme-onc)
HEMATOLOGIC & ONCOLOGIC EMERGENCIES MEG KELLEY MS, FNP- BC, OCN COURSE OBJECTIVES At the conclusion of this presentation, participants should be able to: 1. Define hematological and oncologic (heme-onc)
Hematologic Emergencies. Udomsak Bunworasate Chulalongkorn University
 Hematologic Emergencies Udomsak Bunworasate Chulalongkorn University Hematologic Emergencies Hyperleukocytosis Tumor lysis syndrome SVC syndrome Spinal cord compression Hypercalcemia 1. Hyperleukocytosis
Hematologic Emergencies Udomsak Bunworasate Chulalongkorn University Hematologic Emergencies Hyperleukocytosis Tumor lysis syndrome SVC syndrome Spinal cord compression Hypercalcemia 1. Hyperleukocytosis
Managing patients with bulky cancers
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p2pjfjp8nha
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p2pjfjp8nha
Thrombotic Thrombocytopenic
 The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal radiotherapy, toxic effects of, 636 637 Acute promyelocytic leukemia, associated with acquired bleeding problems, 614 615 Acute renal
Note: Page numbers of article titles are in boldface type. A Abdominal radiotherapy, toxic effects of, 636 637 Acute promyelocytic leukemia, associated with acquired bleeding problems, 614 615 Acute renal
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL
 DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL") Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Approccio morfologico alle microangiopatie trombotiche
 Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdomen, acute, in oncological surgery patients, critical care issues in, 101 102 Acquired factor VIII inhibitors, in critically ill cancer
Index Note: Page numbers of article titles are in boldface type. A Abdomen, acute, in oncological surgery patients, critical care issues in, 101 102 Acquired factor VIII inhibitors, in critically ill cancer
LAMA SHATAT TTP, ITP, DIC
 TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
TTP, ITP, DIC Reduction in platelet number (thrombocytopenia) constitutes an important cause of generalized bleeding. A count less than 100,000 platelets/μl is generally considered to constitute thrombocytopenia.
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital
 Ray Mun Koo Haematology Advanced Trainee Canberra Hospital") Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Therapeutic Leukocyte Reduction (TLR) For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India
 For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India") Therapeutic Leukocyte Reduction (TLR) For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India Anita Tendulkar, Jain P, Gupta A, Sharma N, Navkudkar A, Patle V Dr Anita Tendulkar
Therapeutic Leukocyte Reduction (TLR) For Myeloid Leukaemia's : A Four Year Experience From An Oncology Centre In India Anita Tendulkar, Jain P, Gupta A, Sharma N, Navkudkar A, Patle V Dr Anita Tendulkar
Oncologic Emergencies
 Oncologic Emergencies Objectives Identify the major oncologic emergencies Describe the assessment for each emergency Outline the standard of care of patients experiencing oncologic emergencies Structural
Oncologic Emergencies Objectives Identify the major oncologic emergencies Describe the assessment for each emergency Outline the standard of care of patients experiencing oncologic emergencies Structural
JC Hofmann, MD 1,2 ; KM Grant, MD 3 ; DD Kiprov, MD 1,2. Apheresis Care Group, 2. Division of Immunotherapy, 3
 Greater Than Ninety Percent of Patients with Acute Leukemia and Hyperleukocytosis Who Receive Leukocytapheresis Treatment Successfully Undergo Induction Chemotherapy: Follow-up Analysis of Data from 2006-2013
Greater Than Ninety Percent of Patients with Acute Leukemia and Hyperleukocytosis Who Receive Leukocytapheresis Treatment Successfully Undergo Induction Chemotherapy: Follow-up Analysis of Data from 2006-2013
Tumor Lysis Syndrome Nephrology Grand Rounds Tuesday, July 27 th, 2010 Aditya Mattoo
 Tumor Lysis Syndrome Nephrology Grand Rounds Tuesday, July 27 th, 2010 Aditya Mattoo Outline Background/Definition Epidemiology/Risk Stratification Pathophysiology Treatment Renal Replacement Therapy Background/Definition
Tumor Lysis Syndrome Nephrology Grand Rounds Tuesday, July 27 th, 2010 Aditya Mattoo Outline Background/Definition Epidemiology/Risk Stratification Pathophysiology Treatment Renal Replacement Therapy Background/Definition
Hematological Emergencies: What every Hospitalist needs to know
 Hematological Emergencies: What every Hospitalist needs to know C. Tom Kouroukis MD MSc FRCPC Juravinski Hospital and Cancer Centre Division of Malignant Hematology Department of Oncology McMaster University
Hematological Emergencies: What every Hospitalist needs to know C. Tom Kouroukis MD MSc FRCPC Juravinski Hospital and Cancer Centre Division of Malignant Hematology Department of Oncology McMaster University
PLASMA EXCHANGE J MANION NEPEAN HOSPITAL
 PLASMA EXCHANGE J MANION NEPEAN HOSPITAL PLASMA The fluid portion of blood Normally approx 5% body weight or 3.5L in 70kg male Clots on standing unless anticoagulated Common plasma proteins are albumin,
PLASMA EXCHANGE J MANION NEPEAN HOSPITAL PLASMA The fluid portion of blood Normally approx 5% body weight or 3.5L in 70kg male Clots on standing unless anticoagulated Common plasma proteins are albumin,
Thrombotic thrombocytopenic purpura: a look at the future
 Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura
 Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura Robert A. Brodsky, MD Johns Hopkins Family Professor
Not So Benign Hematology Aplastic anemia, Paroxysmal Nocturnal Hemoglobinuria, atypical Hemolytic Uremic Syndrome, Thrombotic Thrombocytopenic Purpura Robert A. Brodsky, MD Johns Hopkins Family Professor
DIC. Bert Vandewiele Fellow Critical Care 23 May 2011
 DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
DIC Bert Vandewiele Fellow Critical Care 23 May 2011 Dissiminated Intravascular Coagulopathie 11/3/2011 Dr. Bert Vandewiele 2 Dissiminated Intravascular Coagulopathie = Consumption coagulopathie = Defibrination
Disseminated Intravascular Coagulation (DIC) Seminar. Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.
 Seminar. Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.") Disseminated Intravascular Coagulation (DIC) Seminar Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.2012 1 Our plan: Understand the pathophysiology Identify risk factors
Disseminated Intravascular Coagulation (DIC) Seminar Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.2012 1 Our plan: Understand the pathophysiology Identify risk factors
Diagnosis / Lab Findings
 Diagnosis / Lab Findings During at acute episode may see Peripheral smear bite cells, Heinz bodies Reticulocytosis Increased indirect bilirubin G6PD will be normal or high during an acute crisis Repeat
Diagnosis / Lab Findings During at acute episode may see Peripheral smear bite cells, Heinz bodies Reticulocytosis Increased indirect bilirubin G6PD will be normal or high during an acute crisis Repeat
Pathology note 8 BLEEDING DISORDER
 Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Pathology note 8 BLEEDING DISORDER Slide75 ( Types of clotting factors deficiency): Today we will talk about public public factor deficiency it could be acquired or inherited, acquired diseases are more
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Educational Session: Oncology Emergencies
 Educational Session: Oncology Emergencies Diane M. Birnbaumer, MD, FACEP 3/24/2010 10:00 AM - 11:00 AM Oncologic Emergencies Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California,
Educational Session: Oncology Emergencies Diane M. Birnbaumer, MD, FACEP 3/24/2010 10:00 AM - 11:00 AM Oncologic Emergencies Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California,
2.1 mmol/l or 25% increase from baseline mmol/l or 25% decrease from baseline
 22.1 Hyperleukocytosis and tumour lysis syndrome The guideline is addressed for ALL patients with hyperleukocytosis (WBC 100 x109/l) only and should not be used without modifications in case of other diseases
22.1 Hyperleukocytosis and tumour lysis syndrome The guideline is addressed for ALL patients with hyperleukocytosis (WBC 100 x109/l) only and should not be used without modifications in case of other diseases
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Non-immune acquired haemolytic anaemias. Dr.Maysem
 Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
GOOD MORNING! July 3, 2014
 GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
GOOD MORNING! July 3, 2014 OUR PATIENT 4yo Female with: 2 days of fever, sore throat, swollen nodes in neck and abdominal pain PMH: Tonsillectomy age 2 Immunizations: UTD NKDA DIFFERENTIAL: OUR PATIENT
Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal
 Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal What is Oncologic Emergency? An oncologic emergency is an acute, potentially life-threatening event resulting from
Professor Dr. Saiyeedur Rahman Professor and Head Department of Medicine SBMCH, Barisal What is Oncologic Emergency? An oncologic emergency is an acute, potentially life-threatening event resulting from
Thrombotic Microangiopathies
 Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
Thrombotic Microangiopathies ASH/San Antonio Breast Cancer Symposium Review James N. George March 14, 2015 Thrombotic Microangiopathies (TMA): Everything you need to know from 5 patient stories Thrombotic
2 Diagnosis and Staging of Cancer 2.1 Pathophysiology of cancer 2.2 Classification and staging 2.3 Diagnostic measures for specific cancer types
 Oncology Nursing Sub-Specialty Module Reference: Gobel B. M., Triest-Robertson S. & Vogel W.H. (Eds). (205). Advanced Oncology Nursing Certificate Review and Resources Manual. Pittsburgh: Oncology Nursing
Oncology Nursing Sub-Specialty Module Reference: Gobel B. M., Triest-Robertson S. & Vogel W.H. (Eds). (205). Advanced Oncology Nursing Certificate Review and Resources Manual. Pittsburgh: Oncology Nursing
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
 Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Primary causes: Complement dysregulation (50% of non-shiga toxin-producing E. coli ) Secondary causes:
 Secondary causes:") General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Thrombotic thrombocytopenic purpura: 2008 Update
 MEDICAL GRAND ROUNDS CME CREDIT MARK A. CROWTHER, MD Director, Division of Hematology, McMaster University, Hamilton, Ontario, Canada JAMES N. GEORGE, MD Hematology-Oncology Section, Department of Medicine,
MEDICAL GRAND ROUNDS CME CREDIT MARK A. CROWTHER, MD Director, Division of Hematology, McMaster University, Hamilton, Ontario, Canada JAMES N. GEORGE, MD Hematology-Oncology Section, Department of Medicine,
TMA in HUS and TTP: new insights
 TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
Sara K. Vesely, James N. George, Bernhard Lämmle, Jan-Dirk Studt, Lorenzo Alberio, Mayez A. El-Harake, and Gary E. Raskob
 CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS ADAMTS13 activity in thrombotic thrombocytopenic purpura hemolytic uremic syndrome: relation to presenting features and clinical outcomes in
CLINICAL OBSERVATIONS, INTERVENTIONS, AND THERAPEUTIC TRIALS ADAMTS13 activity in thrombotic thrombocytopenic purpura hemolytic uremic syndrome: relation to presenting features and clinical outcomes in
Bleeding Disorders.2 MS Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD
 Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
Bleeding Disorders.2 MS4.25.02.2019 Abdallah Awidi Abbadi.MD. FRCP.FRCPath Feras Fararjeh MD Email: abdalla.awidi@gmail.com Case 6: GT 18 yr old female was admitted with pallor, abdominal pain and gum
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Medical Surgical Review Handout- Hematology/Oncology 2016
 Medical Surgical Review Handout- Hematology/Oncology 2016 Overview Blood circulates in the cardiovascular system o Carries oxygen to the cells o Carries waste away from the cells Functions of blood o Transportation:
Medical Surgical Review Handout- Hematology/Oncology 2016 Overview Blood circulates in the cardiovascular system o Carries oxygen to the cells o Carries waste away from the cells Functions of blood o Transportation:
5/5/2010. Goldilocks picture from
 Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
MS.4/ Acute Leukemia: AML. Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD
 MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
MS.4/ 27.02.2019 Acute Leukemia: AML Abdallah Al Abbadi.MD.FRCP.FRCPath Feras Fararjeh MD Case 9: Acute Leukemia 29 yr old lady complains of fever and painful gums for 1 week. She developed easy bruising
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
A 36 year old previously healthy female develops fever and ruising
 Renal vascular diseases CPC G.A. Appel MD M.B. Stokes MD Case 1 A 36 year old previously healthy female develops fever and bruising. She goes to her LMD and CBC shows plats 15 K, Hct 28%, normal PT and
Renal vascular diseases CPC G.A. Appel MD M.B. Stokes MD Case 1 A 36 year old previously healthy female develops fever and bruising. She goes to her LMD and CBC shows plats 15 K, Hct 28%, normal PT and
Schematic Of Heparin Induced Thrombocytopenia Platelet Count
 Schematic Of Heparin Induced Thrombocytopenia Platelet Count Normal IgG and IgG2 differentially inhibit HIT antibody-dependent platelet activation that platelet counts were lower in FcγRIIA 131RR patients
Schematic Of Heparin Induced Thrombocytopenia Platelet Count Normal IgG and IgG2 differentially inhibit HIT antibody-dependent platelet activation that platelet counts were lower in FcγRIIA 131RR patients
Hemostatic System - general information
 PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
PLATELET DISORDERS Hemostatic System - general information Normal hemostatic system vessel wall circulating blood platelets blood coagulation and fibrynolysis Bleeding Diathesis inherited or acquired defects
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
Renal failure and thrombocytopaenia? Don t forget TTP/HUS. Jonathan Wala Nephrologist
 Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Document Title: Hemostasis: Platelet and Coagulation Disorders. Author(s): Joseph H. Hartmann (University of Michigan), DO 2012
: Joseph H. Hartmann (University of Michigan), DO 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
Project: Ghana Emergency Medicine Collaborative Document Title: Hemostasis: Platelet and Coagulation Disorders Author(s): Joseph H. Hartmann (University of Michigan), DO 2012 License: Unless otherwise
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Apheresis: Clinical Indications
 PART 2 Apheresis: Clinical Indications Clinical Vignettes: Hematology Cardiology/Vascular Neurology Solid Organ Transplantation Anatomy of an ASFA Fact Sheet Hematology 40 yo M presenting to the Emergency
PART 2 Apheresis: Clinical Indications Clinical Vignettes: Hematology Cardiology/Vascular Neurology Solid Organ Transplantation Anatomy of an ASFA Fact Sheet Hematology 40 yo M presenting to the Emergency
Malignant related superior vena cava (SVC) syndrome
 syndrome") Malignant related superior vena cava (SVC) syndrome Manit Sae-teaw B.Pharm, BCP, BCOP Grad dip in Pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University 1 Outline Introduction Etiology
Malignant related superior vena cava (SVC) syndrome Manit Sae-teaw B.Pharm, BCP, BCOP Grad dip in Pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University 1 Outline Introduction Etiology
Immunological transfusion reactions
 Immunological transfusion reactions Immunological transfusion reactions can be hemolytic or non-hemolytic in nature. Both types can be separated into acute (those occurring immediately after transfusion)
Immunological transfusion reactions Immunological transfusion reactions can be hemolytic or non-hemolytic in nature. Both types can be separated into acute (those occurring immediately after transfusion)
Contents. Contributors. Reviewers. Acknowledgements I CARDIOVASCULAR COMPLICATIONS
 Contributors Reviewers Acknowledgements Preface xii xvi xvii xviii I CARDIOVASCULAR COMPLICATIONS 1 Cardiac Complications of Cancer and Anticancer Treatment 3 Introduction 3 Malignant Pericardial Effusion
Contributors Reviewers Acknowledgements Preface xii xvi xvii xviii I CARDIOVASCULAR COMPLICATIONS 1 Cardiac Complications of Cancer and Anticancer Treatment 3 Introduction 3 Malignant Pericardial Effusion
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Soliris (eculizumab) DRUG.00050
 DRUG.00050") Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
1. INSTRUCTIONS 2. DEFINITION OF HUS
 CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
Nicole Laferriere MD PhD FRCPC April 10, Patient Case Studies: Sticky Situations For Platelet Transfusions
 Nicole Laferriere MD PhD FRCPC April 10, 2019 Patient Case Studies: Sticky Situations For Platelet Transfusions Disclosures Ad Board: Celgene, Jansen, Takeda, Roche, Sanofi, Leo, Shire, Servier, Phizer,
Nicole Laferriere MD PhD FRCPC April 10, 2019 Patient Case Studies: Sticky Situations For Platelet Transfusions Disclosures Ad Board: Celgene, Jansen, Takeda, Roche, Sanofi, Leo, Shire, Servier, Phizer,
The function of the bone marrow. Living with Aplastic Anemia. A Case Study - I. Hypocellular bone marrow failure 5/14/2018
 The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162
 Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Immunosuppressants. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
monoclonal gammopathy of undetermin Citation Rheumatology international, 33(1),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
Not So Benign Hematology. Robert A. Brodsky, MD Johns Hopkins Family Professor of Medicine and Oncology Division Chief Hematology
 Not So Benign Hematology Robert A. Brodsky, MD Johns Hopkins Family Professor of Medicine and Oncology Division Chief Hematology Disclosures Dr. Brodsky serves as a Scientific Advisory Board member to:
Not So Benign Hematology Robert A. Brodsky, MD Johns Hopkins Family Professor of Medicine and Oncology Division Chief Hematology Disclosures Dr. Brodsky serves as a Scientific Advisory Board member to: