Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
|
|
|
- Michael Barker
- 5 years ago
- Views:
Transcription
1 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital
 } Regular clinics American Hospital General Paediatrics Skin Prick Testing Asthma / Lung function Food allergy")
2 } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate) } Regular clinics American Hospital General Paediatrics Skin Prick Testing Asthma / Lung function Food allergy testing/challenges } Written papers on asthma management in community in UK } Involved in study looking at why people die from asthma
3 } Discuss GINA guidelines of chronic management } Learning points from recent UK study Why do people die from asthma } Practical advice to help your patients } Case studies 2 nd part of lecture

4 Prevalence of asthma in children aged years Global Initiative for Asthma GINA 2014 Appendix Box A1-1; figure provided by R Beasley
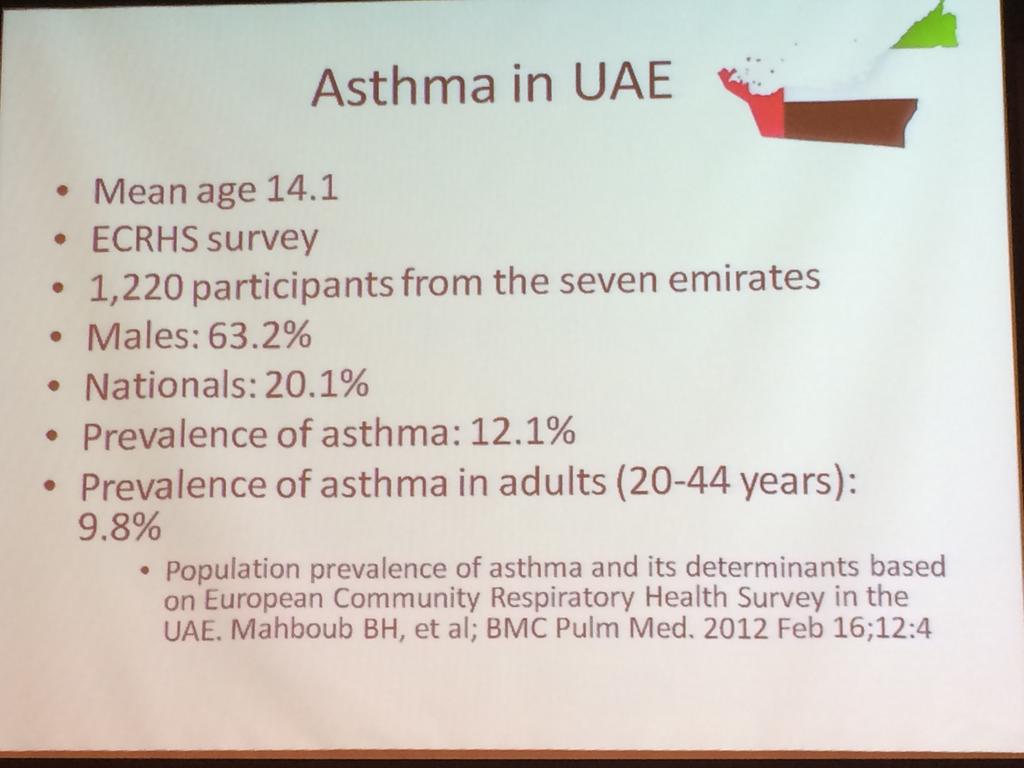
5
6 Asthma Diagnosis

7 Allergic March
8 Clinical Features that increase probability it is asthma?
9
10 GINA 2014 What is known about asthma? n Asthma can be effectively treated n When asthma is well-controlled, patients can ü Avoid troublesome symptoms during the day and night ü Need little or no reliever medication ü Have productive, physically active lives ü Have normal or near-normal lung function ü Avoid serious asthma flare-ups (also called exacerbations, or severe attacks)
11
12 GINA 2014 Diagnosis of asthma n The diagnosis of asthma should be based on: A history of characteristic symptom patterns Evidence of variable airflow limitation, from bronchodilator reversibility testing or other tests n Document evidence for the diagnosis in the patient s notes, preferably before starting controller treatment It is often more difficult to confirm the diagnosis after treatment has been started n Asthma is usually characterized by airway inflammation and airway hyperresponsiveness, but these are not necessary or sufficient to make the diagnosis of asthma.
13 GINA 2014 Typical spirometric tracings Volume Normal Flow FEV 1 Asthma (after BD) Asthma (before BD) Normal Asthma (after BD) Asthma (before BD) Time (seconds) Volume Note: Each FEV 1 represents the highest of three reproducible measurements
14 GINA 2014 The role of lung function in asthma n n n n Diagnosis Demonstrate variable expiratory airflow limitation Reconsider diagnosis if symptoms and lung function are discordant Frequent symptoms but normal FEV 1 : cardiac disease; lack of fitness? Few symptoms but low FEV 1 : poor perception; restriction of lifestyle? Risk assessment Low FEV 1 is an independent predictor of exacerbation risk Monitoring progress Measure lung function at diagnosis, 3-6 months after starting treatment (to identify personal best), and then periodically Consider long-term PEF monitoring for patients with severe asthma or impaired perception of airflow limitation Adjusting treatment? Utility of lung function for adjusting treatment is limited by between-visit variability of FEV 1 (15% year-to-year)
15 Diagnosis of asthma physical examination n Physical examination in people with asthma Often normal The most frequent finding is wheezing on auscultation, especially on forced expiration n Wheezing is also found in other conditions, for example: Respiratory infections Upper airway dysfunction Endobronchial obstruction Inhaled foreign body n Wheezing may be absent during severe asthma exacerbations ( silent chest ) GINA 2014
16 GINA 2014, Box 2-1 Assessment of asthma 1. Asthma control - two domains Assess symptom control over the last 4 weeks Assess risk factors for poor outcomes, including low lung function 2. Treatment issues Check inhaler technique and adherence Ask about side-effects Does the patient have a written asthma action plan? What are the patient s attitudes and goals for their asthma? 3. Comorbidities Think of rhinosinusitis, GERD, obesity, obstructive sleep apnea, depression, anxiety These may contribute to symptoms and poor quality of life

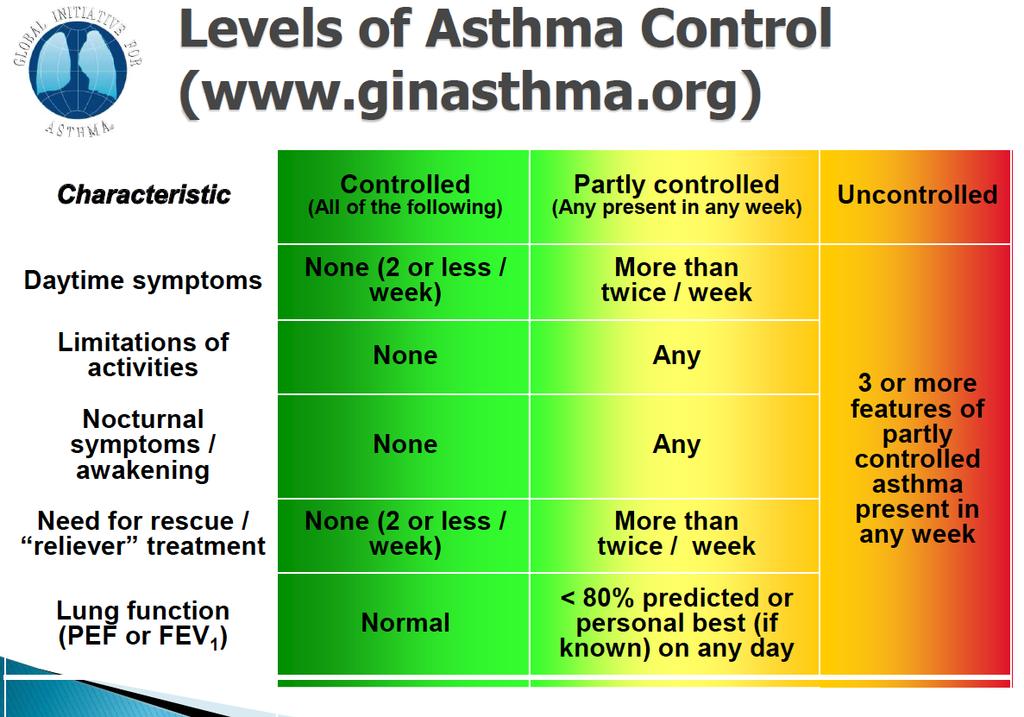
17 GINA assessment of asthma control GINA 2014, Box 2-2A
18 GINA 2014, Box 2-2B Assessment of risk factors for poor asthma outcomes Risk factors for exacerbations include: Ever intubated for asthma Uncontrolled asthma symptoms Having 1 exacerbation in last 12 months Low FEV 1 (measure lung function at start of treatment, at 3-6 months to assess personal best, and periodically thereafter) Incorrect inhaler technique and/or poor adherence Smoking Obesity, pregnancy, blood eosinophilia Risk factors for fixed airflow limitation include: No ICS treatment, smoking, occupational exposure, mucus hypersecretion, blood eosinophilia Risk factors for medication side-effects include: Frequent oral steroids, high dose/potent ICS, P450 inhibitors
19 GINA 2014 Assessing asthma severity n How? Asthma severity is assessed retrospectively from the level of treatment required to control symptoms and exacerbations n When? Assess asthma severity after patient has been on controller treatment for several months Severity is not static it may change over months or years, or as different treatments become available n Categories of asthma severity Mild asthma: well-controlled with Steps 1 or 2 (as-needed SABA or low dose ICS) Moderate asthma: well-controlled with Step 3 (low-dose ICS/LABA) Severe asthma: requires Step 4/5 (moderate or high dose ICS/ LABA ± add-on), or remains uncontrolled despite this treatment
20 GINA 2014 Goals of asthma management n The long-term goals of asthma management are 1. Symptom control: to achieve good control of symptoms and maintain normal activity levels 2. Risk reduction: to minimize future risk of exacerbations, fixed airflow limitation and medication side-effects n Achieving these goals requires a partnership between patient and their health care providers Ask the patient about their own goals regarding their asthma Good communication strategies are essential Consider the health care system, medication availability, cultural and personal preferences and health literacy
21 Key strategies to facilitate good communication n Improve communication skills Friendly manner Allow the patient to express their goals, beliefs and concerns Empathy and reassurance Encouragement and praise Provide appropriate (personalized) information Feedback and review n Benefits include: Increased patient satisfaction Better health outcomes Reduced use of health care resources GINA 2014, Box 3-1
22 GINA 2014 Treating to control symptoms and minimize risk n Establish a patient-doctor partnership n Manage asthma in a continuous cycle: Assess Adjust treatment (pharmacological and non-pharmacological) Review the response n Teach and reinforce essential skills Inhaler skills Adherence Guided self-management education Written asthma action plan Self-monitoring Regular medical review

23 The control-based asthma management cycle GINA 2014, Box 3-2
24 GINA 2014, Box 3-4 (1/2) Initial controller treatment for adults, adolescents and children 6 11 years n n n n Start controller treatment early For best outcomes, initiate controller treatment as early as possible after making the diagnosis of asthma Indications for regular low-dose ICS - any of: Asthma symptoms more than twice a month Waking due to asthma more than once a month Any asthma symptoms plus any risk factors for exacerbations Consider starting at a higher step if: Troublesome asthma symptoms on most days Waking from asthma once or more a week, especially if any risk factors for exacerbations If initial asthma presentation is with an exacerbation: Give a short course of oral steroids and start regular controller treatment (e.g. high dose ICS or medium dose ICS/LABA, then step down)
25 GINA 2014, Box 3-4 (2/2) Initial controller treatment n Before starting initial controller treatment Record evidence for diagnosis of asthma, if possible Record symptom control and risk factors, including lung function Consider factors affecting choice of treatment for this patient Ensure that the patient can use the inhaler correctly Schedule an appointment for a follow-up visit n After starting initial controller treatment Review response after 2-3 months, or according to clinical urgency Adjust treatment (including non-pharmacological treatments) Consider stepping down when asthma has been well-controlled for 3 months

26 GINA 2014, Box 3-5 (upper part) Stepwise management - pharmacotherapy *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/ formoterol maintenance and reliever therapy

27 Stepwise management additional components GINA 2014, Box 3-5 (lower part)
28 } Inhaled generally preferred to oral / iv in order to provide rapid relief with fewer side effects } Systematic review shows delivery of β 2 -agonists is more effective by pmdi then nebuliser, recovery quicker, risk of admission reduced by 60%:

29 } More expensive } Take longer to give and more to clean } Little evidence better then spacers } Main concern is might lead to delayed presentation } Need to show family how to use spacers } GINA guidance supports spacers

30 } Key is use device parents want and will use } Key is use device the doctor is prepared to show the family } Pulmicort safe steroid for short term use in children and only give as neb } Encourage inh too though as child gets older
31 GINA 2014, Box 3-5, Step 1 Step 1 as-needed inhaled short-acting beta 2 -agonist (SABA) *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
32 GINA 2014 Step 1 as-needed reliever inhaler n Preferred option: as-needed inhaled short-acting beta 2 -agonist (SABA) SABAs are highly effective for relief of asthma symptoms However. there is insufficient evidence about the safety of treating asthma with SABA alone This option should be reserved for patients with infrequent symptoms (less than twice a month) of short duration, and with no risk factors for exacerbations n Other options Consider adding regular low dose inhaled corticosteroid (ICS) for patients at risk of exacerbations
33 GINA 2014 SABA use a good marker of control n Definition of good control n If someone is well controlled they need 1 pmdi every 2-3 months n Ask how often need to replace inhaler n Regular use of ventolin might mean they can lead normal life, but issue of risk of exacerbation as NO EFFECT on inflammation
34 GINA 2014, Box 3-5, Step 2 Step 2 low-dose controller + as-needed inhaled SABA *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
35 GINA 2014 Step 2 Low dose controller + as-needed SABA n n Preferred option: regular low dose ICS with as-needed inhaled SABA Low dose ICS reduces symptoms and reduces risk of exacerbations and asthma-related hospitalization and death Other options Leukotriene receptor antagonists (LTRA) with as-needed SABA Less effective than low dose ICS May be used for some patients with both asthma and allergic rhinitis, or if patient will not use ICS Combination low dose ICS/long-acting beta2-agonist (LABA) with as-needed SABA Reduces symptoms and increases lung function compared with ICS More expensive, and does not further reduce exacerbations Intermittent ICS with as-needed SABA for purely seasonal allergic asthma with no interval symptoms Start ICS immediately symptoms commence, and continue for 4 weeks after pollen season ends
36 GINA 2014, Box 3-5, Step 3 Step 3 one or two controllers + as-needed inhaled reliever *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
37 GINA 2014 Step 3 one or two controllers + as-needed inhaled reliever n n n n Before considering step-up Check inhaler technique and adherence, confirm diagnosis Adults/adolescents: preferred options are either combination low dose ICS/ LABA maintenance with as-needed SABA, OR combination low dose ICS/ formoterol maintenance and reliever regimen* Adding LABA reduces symptoms and exacerbations and increases FEV 1, while allowing lower dose of ICS In at-risk patients, maintenance and reliever regimen significantly reduces exacerbations with similar level of symptom control and lower ICS doses compared with other regimens Children 6-11 years: preferred option is medium dose ICS with as-needed SABA Other options Adults/adolescents: Increase ICS dose or add LTRA or theophylline (less effective than ICS/LABA) Children 6-11 years add LABA (similar effect as increasing ICS) *Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol
38 GINA 2014, Box 3-5, Step 4 Step 4 two or more controllers + as-needed inhaled reliever *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
39 GINA 2014 Step 4 two or more controllers + as-needed inhaled reliever n Before considering step-up Check inhaler technique and adherence n Adults or adolescents: preferred option is combination low dose ICS/formoterol as maintenance and reliever regimen*, OR combination medium dose ICS/LABA with as-needed SABA n Children 6 11 years: preferred option is to refer for expert advice n Other options (adults or adolescents) Trial of high dose combination ICS/LABA, but little extra benefit and increased risk of side-effects Increase dosing frequency (for budesonide-containing inhalers) Add-on LTRA or low dose theophylline *Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol

40 GINA 2014, Box 3-5, Step 5 Step 5 higher level care and/or add-on treatment *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy
41 GINA 2014 Step 5 higher level care and/or add-on treatment n Preferred option is referral for specialist investigation and consideration of add-on treatment If symptoms uncontrolled or exacerbations persist despite Step 4 treatment, check inhaler technique and adherence before referring Add-on omalizumab (anti-ige) is suggested for patients with moderate or severe allergic asthma that is uncontrolled on Step 4 treatment n Other add-on treatment options at Step 5 include: Sputum-guided treatment: this is available in specialized centers; reduces exacerbations and/or corticosteroid dose Add-on low dose oral corticosteroids ( 7.5mg/day prednisone equivalent): this may benefit some patients, but has significant systemic side-effects. Assess and monitor for osteoporosis See Severe Asthma Guidelines (Chung et al, ERJ 2014) for more detail
42 GINA 2014, Box 3-6 (2/2) Low, medium and high dose inhaled corticosteroids Children 6 11 years Inhaled corticosteroid Total daily dose (mcg) Low Medium High Beclometasone dipropionate (CFC) > >400 Beclometasone dipropionate (HFA) > >200 Budesonide (DPI) > >400 Budesonide (nebules) > >1000 Ciclesonide (HFA) 80 > >160 Fluticasone propionate (DPI) > >400 Fluticasone propionate (HFA) > >500 Mometasone furoate < Triamcinolone acetonide > >1200 This is not a table of equivalence, but of estimated clinical comparability Most of the clinical benefit from ICS is seen at low doses High doses are arbitrary, but for most ICS are those that, with prolonged use, are associated with increased risk of systemic side-effects

43 Reviewing response and adjusting treatment n n n GINA 2014 How often should asthma be reviewed? 1-3 months after treatment started, then every 3-12 months During pregnancy, every 4-6 weeks After an exacerbation, within 1 week Stepping up asthma treatment Sustained step-up, for at least 2-3 months if asthma poorly controlled Important: first check for common causes (symptoms not due to asthma, incorrect inhaler technique, poor adherence) Short-term step-up, for 1-2 weeks, e.g. with viral infection or allergen May be initiated by patient with written asthma action plan Day-to-day adjustment For patients prescribed low-dose ICS/formoterol maintenance and reliever regimen* Stepping down asthma treatment Consider step-down after good control maintained for 3 months Find each patient s minimum effective dose, that controls both symptoms and exacerbations *Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol
44 General principles for stepping down controller treatment n n n n n Aim To find the lowest dose that controls symptoms and exacerbations, and minimizes the risk of side-effects When to consider stepping down When symptoms have been well controlled and lung function stable for 3 months No respiratory infection, patient not travelling, not pregnant Prepare for step-down Record the level of symptom control and consider risk factors Make sure the patient has a written asthma action plan Book a follow-up visit in 1-3 months Step down through available formulations Stepping down ICS doses by 25 50% at 3 month intervals is feasible and safe for most patients See GINA 2014 report Box 3-7 for specific step-down options Stopping ICS is not recommended in adults with asthma GINA 2014, Box 3-7
45 GINA 2014, Box 3-8 Treating modifiable risk factors n n n n n Provide skills and support for guided asthma self-management This comprises self-monitoring of symptoms and/or PEF, a written asthma action plan and regular medical review Prescribe medications or regimen that minimize exacerbations ICS-containing controller medications reduce risk of exacerbations For patients with 1 exacerbations in previous year, consider low-dose ICS/formoterol maintenance and reliever regimen* Encourage avoidance of tobacco smoke (active or ETS) Provide smoking cessation advice and resources at every visit For patients with severe asthma Refer to a specialist center, if available, for consideration of add-on medications and/or sputum-guided treatment For patients with confirmed food allergy: Appropriate food avoidance Ensure availability of injectable epinephrine for anaphylaxis *Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol
46 Indications for considering referral, where available n Difficulty confirming the diagnosis of asthma Symptoms suggesting chronic infection, cardiac disease etc Diagnosis unclear even after a trial of treatment Features of both asthma and COPD, if in doubt about treatment n Suspected occupational asthma Refer for confirmatory testing, identification of sensitizing agent, advice about eliminating exposure, pharmacological treatment n Persistent uncontrolled asthma or frequent exacerbations Uncontrolled symptoms or ongoing exacerbations or low FEV 1 despite correct inhaler technique and good adherence with Step 4 Frequent asthma-related health care visits n Risk factors for asthma-related death Near-fatal exacerbation in past Anaphylaxis or confirmed food allergy with asthma GINA 2014, Box 3-10 (1/2)
47 Indications for considering referral, where available n Significant side-effects (or risk of side-effects) Significant systemic side-effects Need for oral corticosteroids long-term or as frequent courses n Symptoms suggesting complications or sub-types of asthma Nasal polyposis and reactions to NSAIDS (may be aspirin exacerbated respiratory disease) Chronic sputum production, fleeting shadows on CXR (may be allergic bronchopulmonary aspergillosis) n Additional reasons for referral in children 6-11 years Doubts about diagnosis, e.g. symptoms since birth Symptoms or exacerbations remain uncontrolled Suspected side-effects of treatment, e.g. growth delay Asthma with confirmed food allergy GINA 2014, Box 3-10 (2/2)
48 Guided asthma self-management and skills training Essential components are: n Skills training to use inhaler devices correctly n Encouraging adherence with medications, appointments n Asthma information n Guided self-management support Self-monitoring of symptoms and/or PEF Written asthma action plan Regular review by a health care provider GINA 2014
49 GINA 2014, Box 3-11 Provide hands-on inhaler skills training Choose Choose an appropriate device before prescribing. Consider medication options, arthritis, patient skills and cost. For ICS by pmdi, prescribe a spacer Avoid multiple different inhaler types if possible Check Check technique at every opportunity Can you show me how you use your inhaler at present? Identify errors with a device-specific checklist Correct Give a physical demonstration to show how to use the inhaler correctly Check again (up to 2-3 times) Re-check inhaler technique frequently, as errors often recur within 4-6 weeks Confirm Can you demonstrate correct technique for the inhalers you prescribe? Brief inhaler technique training improves asthma control
50 GINA 2014, Box 3-12 Check adherence with asthma medications n n n Poor adherence: Is very common: it is estimated that 50% of adults and children do not take controller medications as prescribed Contributes to uncontrolled asthma symptoms and risk of exacerbations and asthma-related death Contributory factors Unintentional (e.g. forgetfulness, cost, confusion) and/or Intentional (e.g. no perceived need, fear of side-effects, cultural issues, cost) How to identify patients with low adherence: Ask an empathic question, e.g. Do you find it easier to remember your medication in the morning or the evening?, or Would you say you are taking it 3 days a week, or less, or more? Check prescription date, label date and dose counter Ask patient about their beliefs and concerns about the medication
51
52 GINA 2014, Box 3-12 Inhaled corticosteroids risks n No one has ever died because they fell 1cm short of their potential final height. n Risk of drop can t be attributed to ICS alone n Children die from asthma every day n Height deficit occurs in first 2 years, and then growth velocity normalises there after n What should be our approach Careful monitoring of height and growth every review Review dose of ICS and control to see if can reduce Minimise other steroid exposure (nose and skin) Poor control, don t just increase ICS dose (see case study) Clear communication with family
53 GINA 2014 Strategies to improve adherence in asthma n Only a few interventions have been studied closely in asthma and found to be effective for improving adherence Shared decision-making Simplifying the medication regimen (once vs twice-daily) Comprehensive asthma education with nurse home visits Inhaler reminders for missed doses Reviewing patients detailed dispensing records
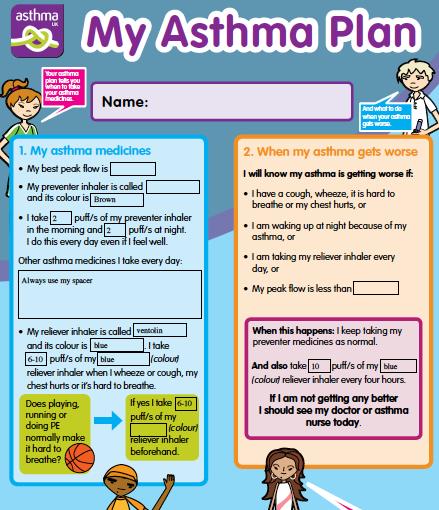
54 GINA 2014 Guided self-management education n Highly effective in improving asthma outcomes Reduced hospitalizations, ED visits, symptoms, night waking, time off work, improved lung function and quality of life n Three essential components Self-monitoring of symptoms and/or PEF Written asthma action plan Describe how to recognize and respond to worsening asthma Individualize the plan for the patient s health literacy and autonomy Provide advice about a change in ICS and how/when to add OCS If using PEF, base action plan on personal best rather than predicted Regular medical review
55
56
57
58 Asthma deaths 195 people who died from asthma analysed 174 expert clinical assessors 2 assessors per case who present to panel and agreement sought 28 children and young people died of asthma < 10yrs = 10 (5%) youngest 4yrs 10-19yrs = 18 (9%)

59 Location of death 45% of all died from asthma without any medical help during final episode 11% tried to get help but died before any help arrived 80% of < 10yrs 72% of 10-19yrs Died before reaching hospital
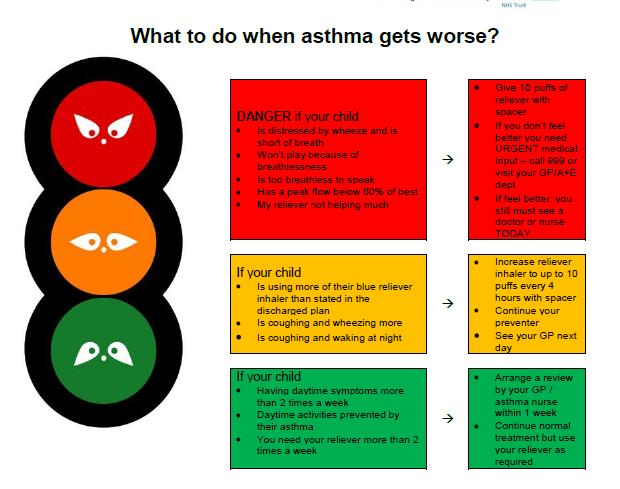
60 Personal asthma action plan } Only 23% of the 195 patients that died was there a record of them having a PAAP } Only 4/28 children had a PAAP } RECOMMENDATION All people with asthma should have PAAP that mentions: 1. Triggers and current treatment 2. How to spot symptoms getting worse and what to do then 3. What to do in emergency and when to call for help
61
62
63 Asthma severity * Overall data (n=155) * Mild = 14 (9%) * Moderate = 76 (49%) * Severe = 61 (39%) * In children 1. < 10 years 1. Mild 0% 2. Moderate 30% 3. Severe 60% 4. NK 10% years 1. Mild 6% 2. Moderate 44% 3. Severe 39% 4. NK 11%
64 Ask about control of asthma * Education is key and little evidence its being asked * Complacency of patient AND doctor * Do parents realise what should be aiming for? * Check adherence * Check ventolin use only this one helps doctor * EVERY consultation
65

66 My daughter Emily died of an asthma attack last year, she was 15. I didn t think for one second asthma would take her life. She took her medication as directed, even on day she died, but I now realise she had no asthma plan nor were we told the seriousness of her condition. I realise if we d been seen more regularly and by a specialist she d be alive now. We felt let down by our doctor
67 } After every admission to hospital } After 2 or more visits to ER in 1 year } If needed >2 courses of prednisolone in 1 year } Poor compliance / persistent allergy exposure

68
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D.
 Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Global Initiative for Asthma (GINA) What s new in GINA 2017?
 What s new in GINA 2017?") Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2017 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2017 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Revised 2014 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Revised 2014 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Asthma Update Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine
 Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine Goals/Objectives Review of 2014 GINA guidelines Significant
Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine Goals/Objectives Review of 2014 GINA guidelines Significant
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA
, BRONCHIAL ASTHMA") CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Public Dissemination
 1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
1. THE ASTHMA CONDITION 9 18 3 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
The clinical effectiveness and costeffectiveness. treatment of chronic asthma in children under the age of 12 years
 The clinical effectiveness and costeffectiveness of corticosteroids for the treatment of chronic asthma in children under the age of 12 years Submission of evidence from AstraZeneca UK Ltd regarding the
The clinical effectiveness and costeffectiveness of corticosteroids for the treatment of chronic asthma in children under the age of 12 years Submission of evidence from AstraZeneca UK Ltd regarding the
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asma e BPCO: le strategie terapeutiche
 Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Interventions to improve adherence to inhaled steroids for asthma. Respiratory department
 Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Australian Asthma Handbook. Key table and figures Version 1.2
 Australian Asthma Handbook Key table and figures Version 1.2 DIAGNOSIS OF ASTHMA Figure. Steps in the diagnosis of asthma in adults Table. Findings that increase or decrease the probability of asthma in
Australian Asthma Handbook Key table and figures Version 1.2 DIAGNOSIS OF ASTHMA Figure. Steps in the diagnosis of asthma in adults Table. Findings that increase or decrease the probability of asthma in
Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred inhaler choices
 ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
WEBINAR. Difficult-to-treat and severe asthma: changing the paradigm
 WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Global Initiative for Asthma (GINA) What s new in GINA 2015?
 What s new in GINA 2015?") Global Initiative for Asthma (GINA) What s new in GINA 2015? GINA Global Strategy for Asthma Management and Prevention What s new in GINA 2015 (1) Add-on tiotropium by soft-mist inhaler is a new other
Global Initiative for Asthma (GINA) What s new in GINA 2015? GINA Global Strategy for Asthma Management and Prevention What s new in GINA 2015 (1) Add-on tiotropium by soft-mist inhaler is a new other
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
Adult Summary flowchart for Asthma Switch and Step Down to preferred inhaler choices
 HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017
 Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs
 Step Down guidance Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs Important Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients
Step Down guidance Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs Important Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Minimum Competencies for Asthma Care in Schools: School Nurse
 Minimum Competencies for Asthma Care in Schools: School Nurse Area I. Pathophysiology 1. Explain using simple language and appropriate educational aids the following concepts: a. Normal lung anatomy and
Minimum Competencies for Asthma Care in Schools: School Nurse Area I. Pathophysiology 1. Explain using simple language and appropriate educational aids the following concepts: a. Normal lung anatomy and
CHARM ASTHMA TREATMENT GUIDELINE
 NHS City and Hackney Prescribing Guidelines Adults ( 12 years of age) CHARM ASTHMA TREATMENT GUIDELINE Written by: Hetal Dhruve (Specialist Respiratory Pharmacist, City and Hackney CCG) Checked by: Prof
NHS City and Hackney Prescribing Guidelines Adults ( 12 years of age) CHARM ASTHMA TREATMENT GUIDELINE Written by: Hetal Dhruve (Specialist Respiratory Pharmacist, City and Hackney CCG) Checked by: Prof
Do We Need Biologics in Pediatric Asthma Management?
 Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Position within the Organisation
 ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
PCRS-UK briefing document Asthma guidelines. November 2017
 PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA TREATMENT GUIDE (ADULTS)
") ASTHMA TREATMENT GUIDE (ADULTS) The BTS/SIGN guideline provides a wide range of information and guidance on the treatment of patients with asthma. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/
ASTHMA TREATMENT GUIDE (ADULTS) The BTS/SIGN guideline provides a wide range of information and guidance on the treatment of patients with asthma. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma
 The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
beclometasone 100 MDI 2 puffs twice a day (recently changed to non CFC (Clenil Modulite))
)") Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital
 Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Asthma Assessment & Review
 ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
Diagnostics Assessment Programme. Measurement of exhaled nitric oxide concentration in asthma; NIOX MINO and NObreath. Final scope
 Diagnostics Assessment Programme Measurement of exhaled nitric oxide concentration in asthma; NIOX MINO and NObreath Final scope February 2013 1. Introduction The Medical Technologies Advisory Committee
Diagnostics Assessment Programme Measurement of exhaled nitric oxide concentration in asthma; NIOX MINO and NObreath Final scope February 2013 1. Introduction The Medical Technologies Advisory Committee
Preschool Wheeze. AC Jeevarathnum 04/03/16. Paediatric Pulmonologist Steve Biko Academic Hospital
 Preschool Wheeze AC Jeevarathnum Paediatric Pulmonologist Steve Biko Academic Hospital MBBCh FcPaed(SA) MMED Dip Allergy(SA) Cert Pulm(Paed)(SA) European Respiratory Diploma 04/03/16 Overview Introduction
Preschool Wheeze AC Jeevarathnum Paediatric Pulmonologist Steve Biko Academic Hospital MBBCh FcPaed(SA) MMED Dip Allergy(SA) Cert Pulm(Paed)(SA) European Respiratory Diploma 04/03/16 Overview Introduction
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Information for Parents and Young People on New and Emerging Treatments in Asthma
 Information for Parents and Young People on New and Emerging Treatments in Asthma Asthma continues to be a very common condition that causes a lot of distress to children and their families. For some it
Information for Parents and Young People on New and Emerging Treatments in Asthma Asthma continues to be a very common condition that causes a lot of distress to children and their families. For some it
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12
 North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Medicines Management of Asthma
 Wandsworth Borough Team Medicines Management of Guidelines for Primary Care September 2011 Version 1 Guideline Authors: Shaneez Dhanji (Wandsworth borough) Reena Rabheru-Dodhy (Sutton & Merton borough)
Wandsworth Borough Team Medicines Management of Guidelines for Primary Care September 2011 Version 1 Guideline Authors: Shaneez Dhanji (Wandsworth borough) Reena Rabheru-Dodhy (Sutton & Merton borough)
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Asthma - An update BTS Asthma Guidelines 2016
 Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
ASTHMA PROTOCOL CELLO
 ASTHMA PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives, non medical and medical therapy and a scheme for inhaler dosage.
ASTHMA PROTOCOL CELLO Leiden May 2011 1 Introduction This protocol includes an explanation of the clinical picture, diagnosis, objectives, non medical and medical therapy and a scheme for inhaler dosage.
Adjustment of Inhaled Controller Therapy of Asthma in the Yellow Zone, Based on the Inhaler Product Used in the Green Zone Age 16 Years and Older
 Adjustment of Inhaled Controller Therapy of Asthma in the Yellow Zone, Based on the Inhaler Product Used in the Green Zone Age 16 Years and Older The Canadian Thoracic Society and other international asthma
Adjustment of Inhaled Controller Therapy of Asthma in the Yellow Zone, Based on the Inhaler Product Used in the Green Zone Age 16 Years and Older The Canadian Thoracic Society and other international asthma
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Guidelines for the Diagnosis and Management of Asthma Clinical Practice Guideline September 2013
 Guidelines for the Diagnosis and Management of Asthma Clinical Practice Guideline September 2013 MedStar Health and MedStar Family Choice accept and endorse the clinical guidelines set forth by the National
Guidelines for the Diagnosis and Management of Asthma Clinical Practice Guideline September 2013 MedStar Health and MedStar Family Choice accept and endorse the clinical guidelines set forth by the National
Adult Asthma Clinical Practice Guideline Summary
 Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
In 2002, it was reported that 72 of 1000
 REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom
 Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Children 5 Years and Younger) A Guide for Health Care Professionals Updated 2015 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Children 5 Years and Younger) A Guide for Health Care Professionals Updated 2015 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND PREVENTION
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
3. Respiratory System
 1 3. Respiratory System Also see Appendix 3A Guidance on Management of Also see Appendix 3B Preferred Inhaler Devices for Adults Also see Appendix 3C Preferred Inhaler Devices for Adolescents (12-18 years)
1 3. Respiratory System Also see Appendix 3A Guidance on Management of Also see Appendix 3B Preferred Inhaler Devices for Adults Also see Appendix 3C Preferred Inhaler Devices for Adolescents (12-18 years)
ASTHMA CARE FOR CHILDREN BASKET OF CARE SUBCOMMITTEE Report to: Minnesota Department of Health. June 22, 2009
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp ASTHMA CARE FOR CHILDREN
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp ASTHMA CARE FOR CHILDREN
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Treatment. Assessing the outcome of interventions Traditionally, the effects of interventions have been assessed by measuring changes in the FEV 1
 58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
58 COPD 59 The treatment of COPD includes drug therapy, surgery, exercise and counselling/psychological support. When managing COPD patients, it is particularly important to evaluate the social and family
Include patients: with a confirmed diagnosis of asthma who have been free of asthma symptoms for 3 months or more.
 Corby Clinical Commissioning Group Kettering General Hospital NHS Trust Nene Clinical Commissioning Group rthampton General Hospital NHS Trust rthamptonshire Healthcare Foundation Trust Stepping down asthma
Corby Clinical Commissioning Group Kettering General Hospital NHS Trust Nene Clinical Commissioning Group rthampton General Hospital NHS Trust rthamptonshire Healthcare Foundation Trust Stepping down asthma
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma