Asthma Update Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine
|
|
|
- Aron Lang
- 5 years ago
- Views:
Transcription

1 Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine
2 Goals/Objectives Review of 2014 GINA guidelines Significant changes/additions Severe asthma and exacerbations Newer therapies Omalizumab (Xolair) Bronchial thermoplasty Tiotropium (Spiriva) Other (time permitting) Pregnancy AERD
3 What s truly new in asthma? Not much Vitamin D? Monoclonal antibodies? New inhalers? Only one: ciclesonide (Alvesco) Single agent ICS only Some theoretical benefits fluticasone/vilanterol (Breo)?
4 Abbreviations SABA: Short Acting Beta Agonist (albuterol) LABA: Long Acting Beta Agonist (salmeterol/formoterol) LTRA: LeukoTriene Receptor Antagonist ABPA: Allergic BronchoPulmonary Aspergillosis
5 Abbreviations AERD: Aspirin Excaerbated Respiratory Disease VCD: Vocal Cord Dysfunction ICS: Inhaled CorticoSteroid EPR-3: Expert Panel Report #3 GINA: Global INitiative for Asthma PEF: Peak Expiratory Flow
6 Abbreviations BT: Bronchial Thermoplasty ACOS: Asthma/COPD Overlap Syndrome
7 Epidemiology Asthma is reported to affect 8-11% of the US population Over 22 million people Annual treatment costs (adults): 18 billion dollars Total costs (incl. missed work/school) is likely double that
8 Epidemiology Getting worse Prevalence of asthma has increased by 25-75% every 10 years since 1960 The relative prevalence of severe asthma has also increased Total hospitalizations have decreased but % intubated has increased
9 Epidemiology More bad news: 40% of patients need urgent care for exacerbation at least once a year US mortality rate from asthma actually increased from the 1970 s s (opposite trend in most other western countries)
10 Epidemiology Much of this can be attributed to socioeconomic factors as minorities and others in urban areas with lower income, education, and access to care have 2x (adults) to 3x (children) the morbidity and mortality
11 Initial evaluation Establish/confirm the diagnosis of asthma Assess symptoms (and control) Identify precipitants/comorbidities that may aggravate asthma Classify asthma severity
12 Definition of asthma Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation. NEW! GINA 2014 Global Initiative for Asthma
13 Establish the diagnosis of asthma Episodic symptoms of airflow obstruction (i.e., wheezing, cough, chest tightness) Obstruction is at least partially reversible Alternative diagnoses are excluded
14 Establish the diagnosis of asthma Pulmonary Function Testing (PFT s) are crucial for the diagnosis of asthma Simple spirometry with postbronchodilator testing is adequate if COPD is not being considered in the differential


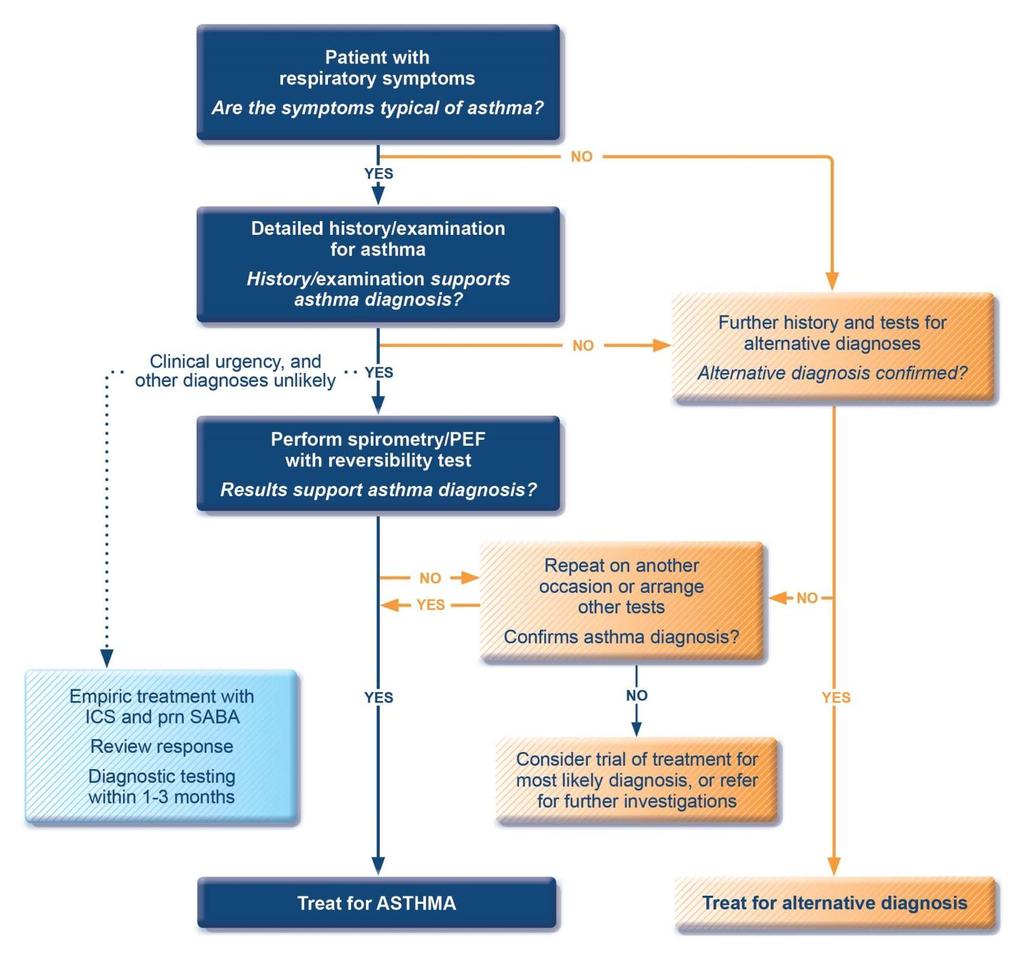
15 NEW! GINA 2014, Box 1-1 Global Initiative for Asthma
16 Diagnosis of asthma symptoms Increased probability that symptoms are due to asthma if: More than one type of symptom (wheeze, shortness of breath, cough, chest tightness) Symptoms often worse at night or in the early morning Symptoms vary over time and in intensity Symptoms are triggered by viral infections, exercise, allergen exposure, changes in weather, laughter, irritants such as car exhaust fumes, smoke, or strong smells Decreased probability that symptoms are due to asthma if: Isolated cough with no other respiratory symptoms Chronic production of sputum Shortness of breath associated with dizziness, light-headedness or peripheral tingling Chest pain Exercise-induced dyspnea with noisy inspiration (stridor) GINA 2014 Global Initiative for Asthma
17 Establish the diagnosis of asthma When to suspect it is not asthma? Long-time smoker (COPD) Older than 50 with no prior history

18 GINA GINA , Box 5-4 Global Initiative for Asthma
19 Establish the diagnosis of asthma When to suspect it is not asthma? Long-time smoker (COPD) Older than 50 with no prior history Symptoms such as palpitations or syncope Poor response to asthma treatment

20 Establish the diagnosis of PFT s sometimes WNL asthma Reversibility criteria are somewhat controversial Methacholine challenge: Better negative predictive value? Other testing as needed to rule out alternate diagnoses (CXR, etc)
21 All that wheezes is not asthma Coined by Chevalier Jackson Laryngologist Developed modern open tracheostomy techniques Pioneer in the development of selflighted endoscopes A specialist in foreign body retrieval
22
23 Initial evaluation Identify and treat comorbidities that may aggravate asthma GERD Sinusitis Vit. D deficiency Allergies OSA
24 Initial evaluation Identify and treat comorbidities that may aggravate asthma GERD Little evidence that treating silent GERD improves asthma control Sinusitis Vit D. Deficiency Allergies OSA
25 Initial evaluation Identify and treat comorbidities that may aggravate asthma GERD Sinusitis Preferred therapy is first generation antihistamines and nasal steroids Vit D. Deficiency Allergies OSA
26 Initial evaluation Identify and treat comorbidities that may aggravate asthma GERD Sinusitis Vit D. Deficiency Ineffective at reducing exacerbations vs placebo Allergies OSA
27 Initial evaluation Identify and treat comorbidities that may aggravate asthma GERD Sinusitis Vit D. Deficiency Allergies Allergy shots have limited efficacy in asthma OSA
28 Initial evaluation Diagnosis made Classify asthma severity (two domains) Future risk (exacerbations) Current impairment (symptoms/pfts) May not respond to therapy in parallel
29 Assessment of risk factors for poor asthma outcomes Risk factors for exacerbations include: Ever intubated for asthma Uncontrolled asthma symptoms Having 1 exacerbation in last 12 months Low FEV 1 (measure lung function at start of treatment, at 3-6 months to assess personal best, and periodically thereafter) Incorrect inhaler technique and/or poor adherence Smoking Obesity, pregnancy, blood eosinophilia Risk factors for fixed airflow limitation include: No ICS treatment, smoking, occupational exposure, mucus hypersecretion, blood eosinophilia Risk factors for medication side-effects include: Frequent oral steroids, high dose/potent ICS, P450 inhibitors GINA 2014, Box 2-2B Global Initiative for Asthma
30 Classification of severity Classic categories of intermittent or mild/mod/severe persistent asthma were static, complex, and often inappropriately applied to patients on high intensity therapy Could result in under-treatment or underestimation of the true severity of disease
31 Classification of severity Severity classification is now based on level or intensity of therapy needed to control the individual patient s asthma
32 Assessing asthma severity How? Asthma severity is assessed retrospectively from the level of treatment required to control symptoms and exacerbations When? Assess asthma severity after patient has been on controller treatment for several months Severity is not static it may change over months or years, or as different treatments become available Categories of asthma severity Mild asthma: well-controlled with Steps 1 or 2 (as-needed SABA or low dose ICS) Moderate asthma: well-controlled with Step 3 (low-dose ICS/LABA) Severe asthma: requires Step 4/5 (moderate or high dose ICS/LABA ± add-on), or remains uncontrolled despite this treatment GINA 2014 Global Initiative for Asthma

33
34 Classification of Severity Assigning severity in follow up based on response helps differentiate between truly severe vs uncontrolled asthma More on this later

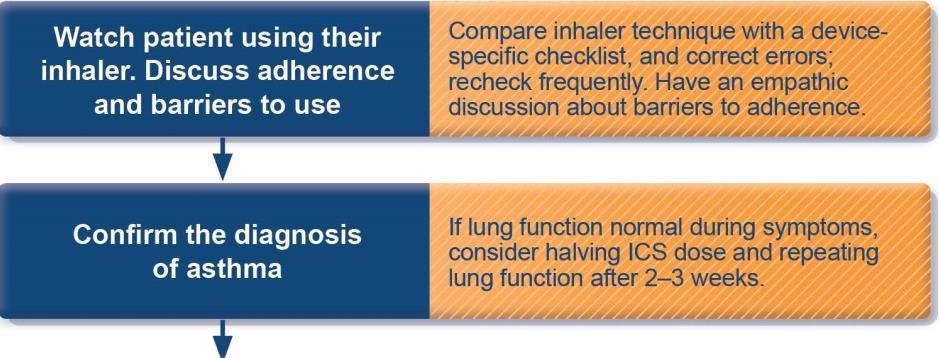

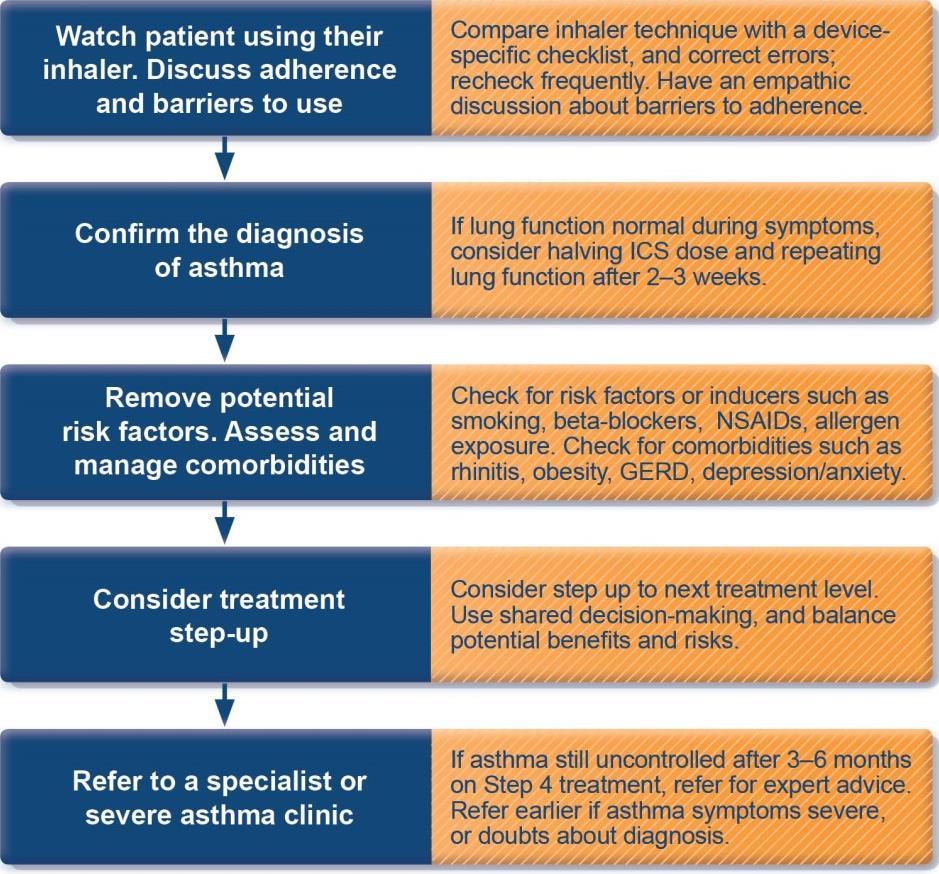
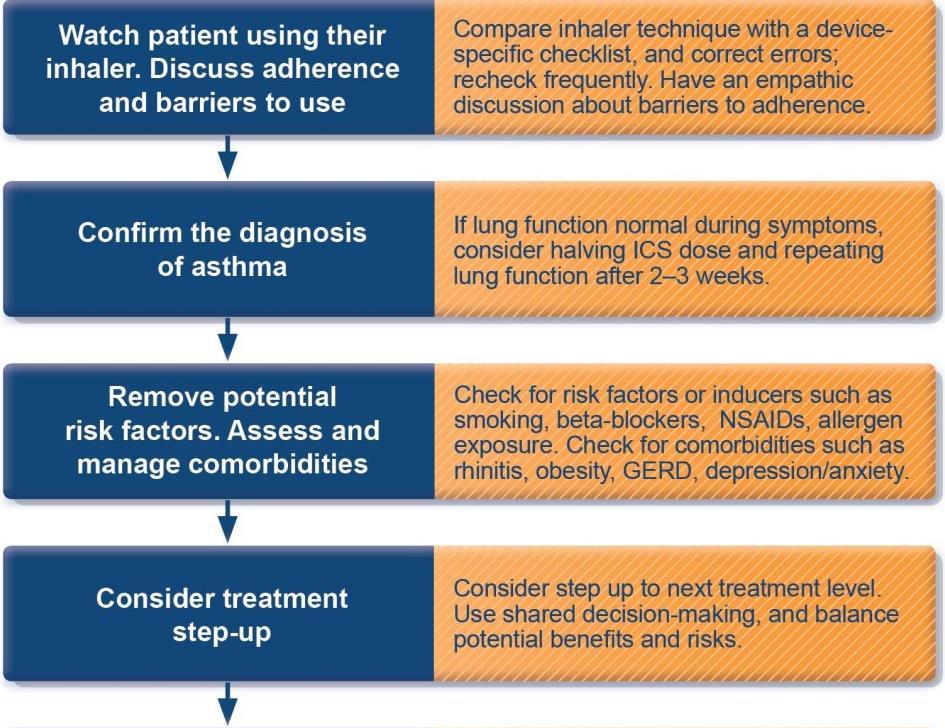
35 How to distinguish between uncontrolled and severe asthma NEW! GINA 2014, Box 2-4 Global Initiative for Asthma

36 Stepwise approach to control asthma symptoms and reduce risk NEW! GINA 2014, Box 3-5 Global Initiative for Asthma
37
38
39 Choosing initial therapy Based on the severity of symptoms at presentation/diagnosis Rule of two s continues to apply
40 Initial controller treatment for adults, adolescents and children 6 11 years NEW! Start controller treatment early For best outcomes, initiate controller treatment as early as possible after making the diagnosis of asthma Indications for regular low-dose ICS - any of: Asthma symptoms more than twice a month Waking due to asthma more than once a month Any asthma symptoms plus any risk factors for exacerbations Consider starting at a higher step if: Troublesome asthma symptoms on most days Waking from asthma once or more a week, especially if any risk factors for exacerbations If initial asthma presentation is with an exacerbation: Give a short course of oral steroids and start regular controller treatment (e.g. high dose ICS or medium dose ICS/LABA, then step down) GINA 2014, Box 3-4 (1/2) Global Initiative for Asthma

41 Step 2 low-dose controller + as-needed inhaled SABA *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy GINA 2014, Box 3-5, Step 2 Global Initiative for Asthma
42 Low, medium and high dose inhaled corticosteroids Adults and adolescents ( 12 years) Inhaled corticosteroid Total daily dose (mcg) Low Medium High Beclometasone dipropionate (CFC) > >1000 Beclometasone dipropionate (HFA) > >400 Budesonide (DPI) > >800 Ciclesonide (HFA) > >320 Fluticasone propionate (DPI or HFA) > >500 Mometasone furoate > >440 Triamcinolone acetonide > >2000 This is not a table of equivalence, but of estimated clinical comparability Most of the clinical benefit from ICS is seen at low doses High doses are arbitrary, but for most ICS are those that, with prolonged use, are associated with increased risk of systemic side-effects GINA 2014, Box 3-6 (1/2) Global Initiative for Asthma
43 LTRA s in one slide Inferior to addition of LABA to ICS in the large majority of trials Has been suggested that improved adherence to pills compared to inhalers is an advantage No readily available method to predict who will respond Try it and see generic soon!

44 Reviewing response and adjusting treatment How often should asthma be reviewed? 1-3 months after treatment started, then every 3-12 months During pregnancy, every 4-6 weeks After an exacerbation, within 1 week Stepping up asthma treatment Sustained step-up, for at least 2-3 months if asthma poorly controlled Important: first check for common causes (symptoms not due to asthma, incorrect inhaler technique, poor adherence) Short-term step-up, for 1-2 weeks, e.g. with viral infection or allergen May be initiated by patient with written asthma action plan Day-to-day adjustment For patients prescribed low-dose ICS/formoterol maintenance and reliever regimen* Stepping down asthma treatment Consider step-down after good control maintained for 3 months Find each patient s minimum effective dose, that controls both symptoms and exacerbations *Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol GINA 2014 Global Initiative for Asthma
45 Stepping down therapy With the exception of those patients with severe asthma or at high risk for severe exacerbations, all asthma patients should be considered for stepping down therapy once well controlled Should not take adult patients completely off ICS, however
46 Stepping down therapy If a patient exhibits good control for over 3 months, consider stepping down therapy Ideally should try to identify the lowest amount of medication necessary to maintain control Can also cycle seasonally for those with allergic asthma
47 Why is my patient s asthma not controlled? Maybe their asthma is that bad Other issues are more likely Compliance? Can they use their inhalers? (80%) Do they know what they are for? Do they know how important it is? Can they afford them?
48 Why is my patient s asthma not controlled? Uncontrolled comorbidities? Obesity? Is it even asthma?
49 Asthma mimics Vocal cord dysfunction (VCD): Will commonly have dysphonia and inspiratory wheezing Respond poorly to standard therapy Diagnosed via laryngoscopy
50 Follow up Other essential components of asthma management include: Serial peak flow measurements or symptom diaries (for at-risk patients) Patient education Action plan (written)

51 2 major reasons: Diagnostic Therapeutic When to consider specialist referral
52 When to refer Dx Diagnosis is in question Atypical symptoms Complicating features (GERD, VCD, ABPA, nasal polyps, etc) Need for further testing Possible occupational asthma
53 When to refer - therapy Life-threatening exacerbation or more than 2 bursts of steroids/yr Poor control even with step 4 or higher therapy Considering immunotherapy Need for education/counseling
54 Exacerbations The first rule of treating an exacerbation (esp. in a high risk patient) is to not underestimate it s severity
")

55 GINA 2014, Box 4-3 (2/3) Global Initiative for Asthma
")


56 GINA 2014, Box 4-3 (3/3) Global Initiative for Asthma Global Initiative for Asthma
57 Exacerbations Corticosteroid dosing: Putting a method to the madness
58 Exacerbations Corticosteroid dosing: Prednisone/prednisolone 1mg/kg to a maximum of 50mg (adults) 1-2 mg/kg, max. 40 mg (children) Treat for 5-7 days, without a taper Medrol dosepaks have no role or even an actual physiologic or pharmacologic basis in lung disease
59 Exacerbations Unlike COPD, antibiotics are not indicated or thought to be beneficial Depending on the current controller medication, it should be increased immediately and continued at the higher dose for at least 2-12 weeks Symbicort (low dose) can be used as a combination controller/rescue inhaler short term
60 Management of severe asthma Optimize dose of ICS/LABA Complete resistance to ICS is rare Consider therapeutic trial of higher dose Consider low dose maintenance oral corticosteroids Monitor for and manage side-effects, including osteoporosis Add-on treatments without phenotyping Theophylline, LTRA limited benefit Tiotropium not yet approved for asthma by a major regulator Phenotype-guided treatment Sputum-guided treatment to reduce exacerbations and/or steroid dose Severe allergic asthma: suggest add-on anti-ige treatment (omalizumab) Aspirin-exacerbated respiratory disease: consider add-on LTRA Non-pharmacological interventions Consider bronchial thermoplasty for selected patients Comprehensive adherence-promoting program For detailed guidelines, see Chung et al, ERJ 2014 GINA 2014, Box 3-14 (2/2) Global Initiative for Asthma
61 Severe asthma and other therapies In most cases patients with severe asthma in whom these therapies are being considered should be referred to a specialist before starting them
62 Other therapies Omalizumab (Xolair) Anticholinergics Bronchial thermoplasty
63 Omalizumab (Xolair) A monoclonal antibody against IgE Prevents its interaction with basophils and mast cells This pathway is not inhibited by steroids Does not interact with bound IgE, so of no value in acute asthma
64 INNOVATE trial, patients on at least high-dose ICS + LABA 20% were on chronic prednisone 26% reduction in exacerbations ~50% in hospitalizations NNT to prevent one exacerbation: 2.2 Humbert, et al. Allergy Mar;60(3):309-16
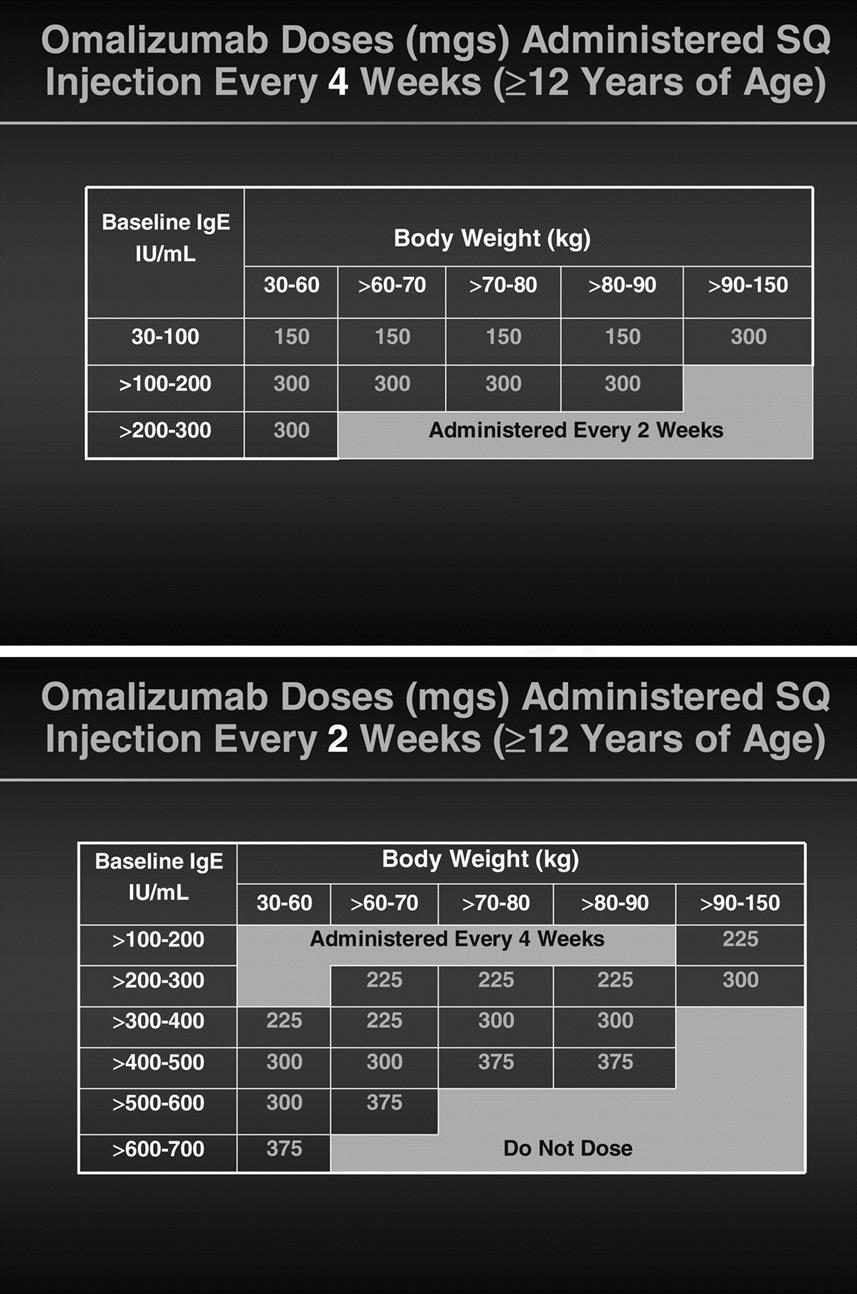
65 Omalizumab Typical criteria 12 years of age or older Inadequate control with ICS + LABA (step 4 or 5) Skin or serum allergen testing positive for a year-round allergen such as dust mites, molds, animal dander, et cetera An elevation in total serum IgE
66 IgE levels Typically IU/mL Dosing is based on weight and IgE Theoretically, levels above 700 are too high and would overwhelm the omalizumab In practice many ignore this ceiling and give the highest dose
67
68 Follow up Patients need to be monitored closely for anaphylaxis when the drug is given and should have an epi-pen Patients should be kept on the drug for weeks to determine whether or not they will respond
69 Bronchial thermoplasty Bronchoscopic procedure in which bronchial smooth muscle mass is reduced by (essentially) RF ablation Series of 3 procedures Not covered by most insurances Carries an increased risk of asthma exacerbation immediately after the procedure
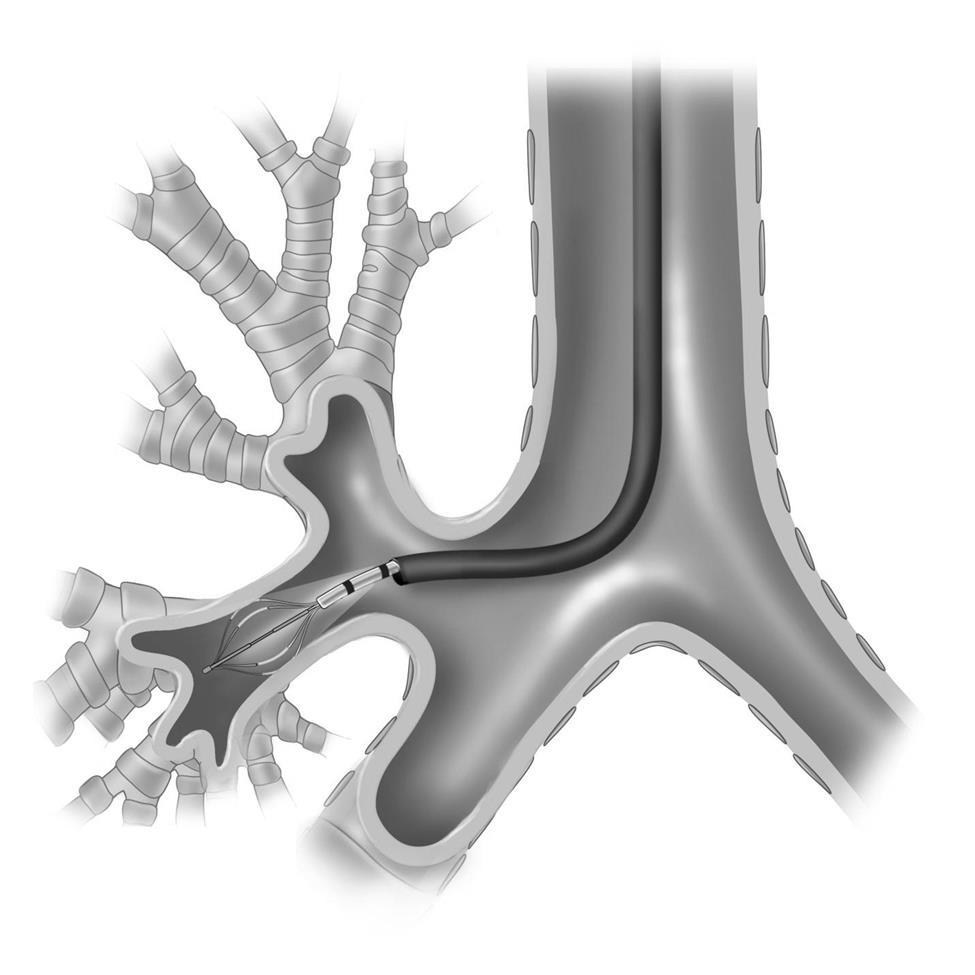
70
71 Bronchial thermoplasty FDA labeling is for severe persistent asthma inadequately controlled on ICS + LABA It s current role in therapy is highly controversial Many interventionalists use the AIR2 study inclusion criteria
72 Simplified AIR2 criteria High dose ICS + LABA Oral steroids OK if stable dose MTX and others excluded Less than 3 hospitalizations or 4 pulses of oral steroids in last year Stable meds for 4+ weeks Nonsmokers (<10 pack-years) Castro, et al. Amer J Respir Crit Care Med 2010 Jan 15;181(2):116-24
73 Tiotropium (Spiriva) FDA approved for COPD TALC trial was a noninferiority study with 3 arms (210 patients on low-dose ICS alone at baseline) Double dose of ICS Add LABA to low-dose ICS Add tiotropium to low-dose ICS Peters, et al. N Engl J Med 2010; 363:
 So: Tiotropium = LABA Peters, et al.")
74 TALC trial Tiotropium was at least non-inferior to adding a LABA to low-dose ICS in all outcomes Tiotropium was superior to doubling the dose of ICS in almost all of the outcomes (so is LABA) So: Tiotropium = LABA Peters, et al. N Engl J Med 2010; 363:
75 Ipratropium (Atrovent) Ipratropium has weak data supporting use as an alternative to albuterol for those who cannot tolerate it Has been shown to have additive benefit to albuterol in treatment of moderate-severe exacerbations Not much to suggest any other role in asthma therapy
76 Special topics Pregnancy AERD
77 Pregnancy and asthma 1/3 of pregnant women have worse asthma control, 1/3 better control, 1/3 no change Exacerbations, however, are common, especially in the second trimester
78 Pregnancy and asthma The general principle of treating a pregnant patient with asthma is that poorly controlled asthma is a much greater threat to the fetus than any medications Inhaled budesonide (pulmicort) is pregnancy category B and is the preferred ICS All other ICS are category C
79 Pregnancy and asthma LTRA s (zafirlukast/montelukast) are also category B Zileuton should be avoided LABA s are category C based on oral high-dose animal studies (use when benefit outweighs risk) Omalizumab is also category B
80 Pregnancy and asthma Oral corticosteroids are indicated for severe exacerbations or if the patient is steroid-dependant at baseline, again on the premise that uncontrolled asthma is the greater risk No definite link to adverse maternal or fetal outcomes
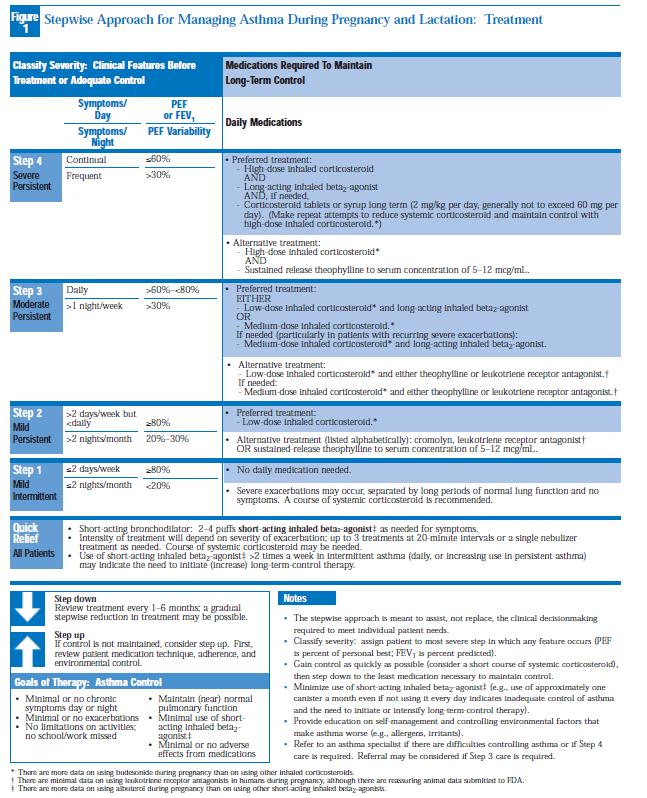
81 Pregnancy and asthma Bottom line: Asthma is bad for the baby The management table (EPR-3) for pregnant/breastfeeding patients is virtually identical to the normal one The key is to monitor the patients very closely and use the lowest doses possible
82
83 AERD Aspirin Exacerbated Respiratory Disease Aka Samter s triad Actually a tetrad: Asthma, nasal polyps, ASA allergy, and persistent rhinosinusitis
84 AERD 10-20% of asthmatics 30-40% of asthmatics with nasal polyps
85 AERD Either the asthma or sinusitis can present first Gold standard for diagnosis is an ASA challenge History of an asthma attack following taking aspirin is suggestive but 16% of patients who give such a history have a negative challenge
86 AERD: Treatment 2 main treatment options Avoidance of all NSAIDS/COX-1 inhibitors ASA desensitization and continuous therapy Leukotriene antagonists?
87 Leukotriene antagonists Thought to be beneficial and possibly very effective as add-on therapy with ASA desensitization ASA therapy is most clearly effective for the sinus disease LTRA s work almost exclusively in the lower airways (except zileuton)
88 ASA desensitization First case report from 1922 Multiple trials have shown improvement in both sinus and respiratory symptoms with asa therapy Also a decrease in steroid use and exacerbations
89 ASA desensitization Why does it work? ASA allergy is not the underlying mechanism It is a marker for an unspecified defect of arachidonic acid metabolism High-dose ASA therapy modulates these pathways (IL-4?)
90 Questions? Guidelines available at: EPR-3 & pregnancy: nhlbi.nih.gov/guidelines/asthma GINA: ginasthma.org
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D.
 Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA
, BRONCHIAL ASTHMA") CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2017 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2017 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Symptoms are worse at night and in the morning and includes cough, whz, chest tightness.
 Asthma Review ETIOLOGY Airflow limitation is caused by the following: - bronchoconstriction - mucous pluggin - airway inflammation Sudden death - heavy mucous plugging is common - typically occurs between
Asthma Review ETIOLOGY Airflow limitation is caused by the following: - bronchoconstriction - mucous pluggin - airway inflammation Sudden death - heavy mucous plugging is common - typically occurs between
Global Initiative for Asthma (GINA) What s new in GINA 2017?
 What s new in GINA 2017?") Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Global Initiative for Asthma (GINA) What s new in GINA 2015?
 What s new in GINA 2015?") Global Initiative for Asthma (GINA) What s new in GINA 2015? GINA Global Strategy for Asthma Management and Prevention What s new in GINA 2015 (1) Add-on tiotropium by soft-mist inhaler is a new other
Global Initiative for Asthma (GINA) What s new in GINA 2015? GINA Global Strategy for Asthma Management and Prevention What s new in GINA 2015 (1) Add-on tiotropium by soft-mist inhaler is a new other
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
Asma e BPCO: le strategie terapeutiche
 Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Revised 2014 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Revised 2014 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017
 Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Protocol Title: Adult Asthma Protocol Effective Date: 4/27/2016 Version: 1.0 Approval By: CCC Clinical Delivery Steering Planned Review Date: 4/27/2017 1 Purpose & Objective This protocol provides evidence-based
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Learning Objective. Asthma. Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Asthma 2/22/2017
 Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Marianne Curran, PA C 3/1/17 Learning Objective Discuss the pathophysiology, clinical presentation, diagnosis, and treatment of Definition many variations Chronic Disorder with Reversible (Intermittent
Pharmacological Management of Obstructive Airways in Humans. Introduction to Scientific Research. Submitted: 12/4/08
 Pharmacological Management of Obstructive Airways in Humans Introduction to Scientific Research Submitted: 12/4/08 Introduction: Obstructive airways can be characterized as inflammation or structural changes
Pharmacological Management of Obstructive Airways in Humans Introduction to Scientific Research Submitted: 12/4/08 Introduction: Obstructive airways can be characterized as inflammation or structural changes
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications
 The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Asthma medications: Know your options - MayoClinic.com. Asthma medications: Know your options
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
New Therapies for Asthma
 New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma
 The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Asthma Update I have no professional or personal financial conflicts of interest to disclose.
 Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update Jennifer W. McCallister, MD, FACP, FCCP
 Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Objectives. Asthma in Primary Care. Definition. Epidemiology. Pathophysiology
 Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital
 Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Do We Need Biologics in Pediatric Asthma Management?
 Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Asthma. Definition. Symptoms
 Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Asthma Definition Asthma is a condition in which your airways narrow and swell and produce extra mucus. This can make breathing difficult and trigger coughing, wheezing and shortness of breath. For some
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters
 Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Adult Asthma Clinical Practice Guideline Summary
 Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Interventions to improve adherence to inhaled steroids for asthma. Respiratory department
 Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
In 2002, it was reported that 72 of 1000
 REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
LINEE GUIDA DELL ASMA: UP TO DATE
 LINEE GUIDA DELL ASMA: UP TO DATE Azienda Ospedaliera Pisana Università degli Studi di Pisa Pierluigi Paggiaro GINA International Executive Committee, Chairman GINA ITaly Cardio-Thoracic and Vascular Department,
LINEE GUIDA DELL ASMA: UP TO DATE Azienda Ospedaliera Pisana Università degli Studi di Pisa Pierluigi Paggiaro GINA International Executive Committee, Chairman GINA ITaly Cardio-Thoracic and Vascular Department,
UPDATE ON ASTHMA MEDICATIONS INCLUDING BIOLOGICS FOR SEVERE PERSISTENT ASTHMA JOAN O LEAR FNP AE- C KENWOOD ALLERGY AND ASTHMA CENTER
 JOAN O LEAR FNP AE- C KENWOOD ALLERGY AND ASTHMA CENTER UPDATE ON ASTHMA MEDICATIONS INCLUDING BIOLOGICS FOR SEVERE PERSISTENT ASTHMA OBJECTIVES Describe Describe asthma medications that have been added
JOAN O LEAR FNP AE- C KENWOOD ALLERGY AND ASTHMA CENTER UPDATE ON ASTHMA MEDICATIONS INCLUDING BIOLOGICS FOR SEVERE PERSISTENT ASTHMA OBJECTIVES Describe Describe asthma medications that have been added
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
Asthma in the college health setting: diagnosis, treatment, pitfalls
 Asthma in the college health setting: diagnosis, treatment, pitfalls A 20-year-old college student with a history of asthma and allergic rhinitis, which were diagnosed in childhood, presents with cough
Asthma in the college health setting: diagnosis, treatment, pitfalls A 20-year-old college student with a history of asthma and allergic rhinitis, which were diagnosed in childhood, presents with cough
Australian Asthma Handbook. Key table and figures Version 1.2
 Australian Asthma Handbook Key table and figures Version 1.2 DIAGNOSIS OF ASTHMA Figure. Steps in the diagnosis of asthma in adults Table. Findings that increase or decrease the probability of asthma in
Australian Asthma Handbook Key table and figures Version 1.2 DIAGNOSIS OF ASTHMA Figure. Steps in the diagnosis of asthma in adults Table. Findings that increase or decrease the probability of asthma in
Nucala (mepolizumab injection for subcutaneous use)
") Nucala (mepolizumab injection for subcutaneous use) Policy Number: 5.01.612 Last Review: 01/2018 Origination: 02/2016 Next Review: 02/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Nucala (mepolizumab injection for subcutaneous use) Policy Number: 5.01.612 Last Review: 01/2018 Origination: 02/2016 Next Review: 02/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
Asthma - An update BTS Asthma Guidelines 2016
 Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Omalizumab (Xolair ) ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication
 ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September Indication") ( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
( Genentech, Inc., Novartis Pharmaceuticals Corp.) September 2003 Indication The FDA recently approved Omalizumab on June 20, 2003 for adults and adolescents (12 years of age and above) with moderate to
National Asthma Educator Certification Board Detailed Content Outline
 I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
I. THE ASTHMA CONDITION 9 20 1 30 A. Pathophysiology 4 6 0 10 1. Teach an individual with asthma and their family using simple language by illustrating the following with appropriate educational aids a.
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
COPD COPD. Update on COPD and Asthma
 Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Cinqair (reslizumab injection for intravenous use)
") Cinqair (reslizumab injection for intravenous use) Policy Number: 5.02.522 Last Review: 04/2018 Origination: 04/2016 Next Review: 04/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Cinqair (reslizumab injection for intravenous use) Policy Number: 5.02.522 Last Review: 04/2018 Origination: 04/2016 Next Review: 04/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Some Facts About Asthma
 Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Some Facts About Asthma Contents What is asthma? Diagnosing asthma Asthma symptoms Asthma triggers Thanks What is asthma?? Asthma is a chronic lung-disease that inflames and narrows the airways (tubes
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting