Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
|
|
|
- Abigail Lucas
- 6 years ago
- Views:
Transcription
1 Improving Outcomes in the Management & Treatment of Asthma April 21, Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University of Kentucky, College of Public Health Disclosures Research Grants GlaxoSmithKline Pfizer Novartis Astra-Zeneca Advisory Boards GlaxoSmithKline Pfizer Astra-Zeneca Novartis Merck Nycomed Forest Amgen Expert Witness In Environmental Tobacco Smoke exposure cases (Plaintiffs) Diacetyl exposure cases (Defense) Tobacco and Lung Disease cases (Plaintiffs) Chief Scientific Officer - COPD Foundation 1
2 Objectives Identify the safety and efficacy of emerging treatment strategies for poorly controlled asthma Discuss appropriate treatment strategies for patients with persistent asthma uncontrolled on inhaled corticosteroids Analyze the available and emerging biologic agents for treatment options in patients with severe asthma Review the potential implications of new guidelines and data on patient selection and treatment options to control symptoms, reduce exacerbations and improve the quality of life of severe asthma patients Assess different strategies to overcome barriers of care and educate patients on the importance of adherence to better understand and manage their asthma 2


3 Assessment of Asthma Severity Severe Asthma Phenotypes Moore et al, AJRCCM

4 Severe Asthma Phenotypes Moore et al, AJRCCM 2010 Assessment of Asthma Control 4


5 Factors Affecting Asthma Control P-A-C-T Perception Locus of control, cultural Adherence Comorbidities GERD, sinus disease, allergic rhinitis Triggers Tobacco smoke, pets, cockroaches, etc How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct errors; recheck frequently. Have an empathic discussion about barriers to adherence. Confirm the diagnosis of asthma If lung function normal during symptoms, consider halving ICS dose and repeating lung function after 2 3 weeks. Remove potential risk factors. Assess and manage comorbidities Check for risk factors or inducers such as smoking, beta-blockers, NSAIDs, allergen exposure. Check for comorbidities such as rhinitis, obesity, GERD, depression/anxiety. Consider treatment step-up Consider step up to next treatment level. Use shared decision-making, and balance potential benefits and risks. Refer to a specialist or severe asthma clinic If asthma still uncontrolled after 3 6 months on Step 4 treatment, refer for expert advice. Refer earlier if asthma symptoms severe, or doubts about diagnosis. GINA 2015, Box 2-4 (5/5) 5

6 Intermittent Asthma Step 1 Preferred: SABA PRN Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn, Nedocromil, or Theophylline Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 care or higher is required. Consider consultation at step 3. Step 3 Step 4 Preferred: Medium-dose Preferred: ICS + LABA Medium-dose ICS Alternative: OR Medium-dose ICS + either Low-dose ICS LTRA or + either Theophylline LABA, LTRA, or Theophylline Step 5 Preferred: High-dose ICS + LABA Alternative: High-dose ICS + either LTRA or Theophylline AND Omalizumab may be considered for patients who have allergies Step 6 Preferred: High-dose ICS + LABA + oral corticosteroid Alternative: High-dose ICS + either LTRA or Theophylline + oral corticosteroid AND Omalizumab may be considered for patients who have allergies Patient Education and Environmental Control at Each Step Step up if needed (first, check adherence and environmental control and comorbid conditions) Assess control Step down if possible (and asthma is well controlled at least 3 months) EPR Stepwise management - pharmacotherapy Diagnosis Symptom control & risk factors (including lung function) Inhaler technique & adherence Patient preference Symptoms Exacerbations Side-effects Patient satisfaction Lung function Asthma medications Non-pharmacological strategies Treat modifiable risk factors STEP 5 PREFERRED CONTROLLER CHOICE Other controller options RELIEVER STEP 1 STEP 2 Consider low dose ICS Low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* As-needed short-acting beta2-agonist (SABA) STEP 3 Low dose ICS/LABA* STEP 4 Med/high ICS/LABA Med/high dose ICS Add tiotropium# Add Low dose ICS+LTRA High dose ICS (or + theoph*) + LTRA (or + theoph*) As-needed SABA or low dose ICS/formoterol** Refer for add-on treatment e.g. anti-ige tiotropium# Add low dose OCS *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/ formoterol maintenance and reliever therapy # Tiotropium by soft-mist inhaler is indicated as add-on treatment for adults ( 18 yrs) with a history of exacerbations GINA 2015, Box 3-5 (2/8) (upper part) 6

7 Cochrane Review Overall, efficient inhaler technique 46-59% did OK Mistakes in MDIs 37% Mistakes in DPIs 35% Switching is a problem 50% loss of control Ram FSF, Brocklebank DDM, White J, Wright JJ, Jones P. Cochrane Database of Systematic Reviews Accessed August 24, Adherence Compare what the patient answered to asthma meds. Is it the same as what you prescribed? Look at comments about why medication is taken Are they taking the right one for the right reason? Rescue vs Controller Look at comments about why medication is not taken Fear Too expensive Become dependent Too complicated Don t need it all the time no symptoms = no asthma 7
8 Inhaler Videos Available Available on drug company websites Available on AARC website ( New ones available on website specifically developed for primary care: You can review Patient can review at home Family can review Medications to Treat Asthma: Using an MDI Inhaler technique should be evaluated at each visit part of medication reconciliation. Source: Global Initiative for Asthma. You Can Control Your Asthma. Accessed August 24,


9 Office Spirometers Asthma Control Assessment is Sparse Clinicians don t ask Patients don t report Clinicians don t document 9
10 Treating modifiable risk factors Provide skills and support for guided asthma self-management This comprises self-monitoring of symptoms and/or PEF, a written asthma action plan and regular medical review Prescribe medications or regimen that minimize exacerbations ICS-containing controller medications reduce risk of exacerbations Encourage avoidance of tobacco smoke (active or ETS) Provide smoking cessation advice and resources at every visit For patients with severe asthma Refer to a specialist center, if available, for consideration of add-on medications and/or sputum-guided treatment For patients with confirmed food allergy: Appropriate food avoidance Ensure availability of injectable epinephrine for anaphylaxis GINA 2015, Box 3-8 Non-pharmacological interventions Avoidance of tobacco smoke exposure Physical activity Occupational asthma Ask patients with adult-onset asthma about work history. Remove sensitizers as soon as possible. Refer for expert advice, if available Avoid medications that may worsen asthma (Allergen avoidance) (Not recommended as a general strategy for asthma) This slide shows examples of interventions with high quality evidence GINA 2015, Box



11 Reviewing response and adjusting treatment How often should asthma be reviewed? 1-3 months after treatment started, then every 3-12 months During pregnancy, every 4-6 weeks After an exacerbation, within 1 week Stepping up asthma treatment Sustained step-up, for at least 2-3 months if asthma poorly controlled Important: first check for common causes (symptoms not due to asthma, incorrect inhaler technique, poor adherence) Short-term step-up, for 1-2 weeks, e.g. with viral infection or allergen May be initiated by patient with written asthma action plan Day-to-day adjustment For patients prescribed low-dose ICS/formoterol maintenance and reliever regimen* Stepping down asthma treatment Consider step-down after good control maintained for 3 months Find each patient s minimum effective dose, that controls both symptoms and exacerbations *Approved only for low dose beclometasone/formoterol and low dose budesonide/formoterol GINA 2015 Managing Asthma: Sample Asthma Action Plan Describes medicines to use and actions to take Adapted from NAEPP, NHBLI, NIH. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma; Full Report Bethesda, MD: US Dept of Health and Human Services: August NIH publication Available Accessed August 24,
12 General principles for stepping down controller treatment Aim To find the lowest dose that controls symptoms and exacerbations, and minimizes the risk of side-effects When to consider stepping down When symptoms have been well controlled and lung function stable for 3 months No respiratory infection, patient not travelling, not pregnant Prepare for step-down Record the level of symptom control and consider risk factors Make sure the patient has a written asthma action plan Book a follow-up visit in 1-3 months Step down through available formulations Stepping down ICS doses by 25 50% at 3 month intervals is feasible and safe for most patients See GINA 2015 report Box 3-7 for specific step-down options Stopping ICS is not recommended in adults with asthma GINA 2015, Box 3-7 Step 1 as-needed inhaled short-acting beta 2 -agonist (SABA) STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP 3 Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-ige Other controller options RELIEVER Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS Low dose ICS+LTRA (or + theoph*) Add tiotropium# High dose ICS + LTRA (or + theoph*) As-needed SABA or low dose ICS/formoterol** Add tiotropium# Add low dose OCS *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy # Tiotropium by soft-mist inhaler is indicated as add-on treatment for patients with a history of exacerbations; it is not indicated in children <18 years. GINA 2015, Box 3-5, Step 1 (4/8) 12
13 Step 2 low-dose controller + as-needed inhaled SABA STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP 3 Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-ige Other controller options RELIEVER Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS Low dose ICS+LTRA (or + theoph*) Add tiotropium# High dose ICS + LTRA (or + theoph*) As-needed SABA or low dose ICS/formoterol** Add tiotropium# Add low dose OCS *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy # Tiotropium by soft-mist inhaler is indicated as add-on treatment for patients with a history of exacerbations; it is not indicated in children <18 years. GINA 2015, Box 3-5, Step 2 (5/8) Step 2 Low dose controller + as-needed SABA Preferred option: regular low dose ICS with as-needed inhaled SABA Low dose ICS reduces symptoms and reduces risk of exacerbations Other options Leukotriene receptor antagonists (LTRA) with as-needed SABA Less effective than low dose ICS Combination low dose ICS/long-acting beta2-agonist (LABA) with as-needed SABA Reduces symptoms and increases lung function compared with ICS Intermittent ICS with as-needed SABA for purely seasonal allergic asthma with no interval symptoms Start ICS immediately symptoms commence, and continue for 4 weeks after pollen season ends GINA
 Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS")

14 Step 3 one or two controllers + as-needed inhaled reliever STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP 3 Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-ige Other controller options RELIEVER Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS Low dose ICS+LTRA (or + theoph*) Add tiotropium# High dose ICS + LTRA (or + theoph*) As-needed SABA or low dose ICS/formoterol** Add tiotropium# Add low dose OCS *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy # Tiotropium by soft-mist inhaler is indicated as add-on treatment for patients with a history of exacerbations; it is not indicated in children <18 years. GINA 2015, Box 3-5, Step 3 (6/8) Step 3 one or two controllers + as-needed inhaled reliever Before considering step-up Check inhaler technique and adherence, confirm diagnosis Adults/adolescents: preferred options are either combination low dose ICS/LABA maintenance with as-needed SABA Adding LABA reduces symptoms and exacerbations and increases FEV 1, while allowing lower dose of ICS Other options Adults/adolescents: Increase ICS dose or add LTRA or theophylline (less effective than ICS/LABA) GINA

15 Step 4 two or more controllers + as-needed inhaled reliever UPDATED! STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP 3 Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-ige Other controller options RELIEVER Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS Add tiotropium# Low dose ICS+LTRA High dose ICS (or + theoph*) + LTRA (or + theoph*) As-needed SABA or low dose ICS/formoterol** Add tiotropium# Add low dose OCS *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy # Tiotropium by soft-mist inhaler is indicated as add-on treatment for patients with a history of exacerbations; it is not indicated in children <18 years. GINA 2015, Box 3-5, Step 4 (7/8) Step 4 two or more controllers + as-needed inhaled reliever Before considering step-up Check inhaler technique and adherence UPDATED! Adults or adolescents: preferred option is combination medium dose ICS/LABA with as-needed SABA Other options (adults or adolescents) Tiotropium by soft-mist inhaler may be used as add-on therapy for adult patients ( 18 years) with a history of exacerbations Trial of high dose combination ICS/LABA, but little extra benefit and increased risk of side-effects Increase dosing frequency (for budesonide-containing inhalers) Add-on LTRA or low dose theophylline GINA
 Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS Add")
16 Step 5 higher level care and/or add-on treatment UPDATED! STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP 3 Low dose ICS/LABA* Med/high ICS/LABA Refer for add-on treatment e.g. anti-ige Other controller options RELIEVER Consider low dose ICS Leukotriene receptor antagonists (LTRA) Low dose theophylline* As-needed short-acting beta 2 -agonist (SABA) Med/high dose ICS Add tiotropium# Low dose ICS+LTRA High dose ICS (or + theoph*) + LTRA (or + theoph*) As-needed SABA or low dose ICS/formoterol** Add tiotropium# Add low dose OCS *For children 6-11 years, theophylline is not recommended, and preferred Step 3 is medium dose ICS **For patients prescribed BDP/formoterol or BUD/formoterol maintenance and reliever therapy # Tiotropium by soft-mist inhaler is indicated as add-on treatment for patients with a history of exacerbations; it is not indicated in children <18 years. GINA 2015, Box 3-5, Step 5 (8/8) Step 5 higher level care and/or add-on treatment UPDATED! Preferred option is referral for specialist investigation and consideration of add-on treatment If symptoms uncontrolled or exacerbations persist despite Step 4 treatment, check inhaler technique and adherence before referring Add-on omalizumab (anti-ige) is suggested for patients with moderate or severe allergic asthma that is uncontrolled on Step 4 treatment Other add-on treatment options at Step 5 include: Tiotropium: for adults ( 18 years) Sputum-guided treatment: this is available in specialized centers; Add-on low dose oral corticosteroids ( 7.5mg/day prednisone equivalent): this may benefit some patients, but has significant systemic side-effects. Assess and monitor for osteoporosis See Severe Asthma Guidelines (Chung et al, ERJ 2014) for more detail GINA
 2016 Severe asthma Bronchial Thermoplasty 2010 Severe and persistent asthma not well controlled with ICS and LABA")
17 Approved New Therapies for Severe Asthma Omalizumab (Xolair) Severe Eosinophilic asthma Mepolizumab (Nucala) Severe Eosinophilic asthma Reslizumab (Cinquair) 2016 Severe asthma Bronchial Thermoplasty 2010 Severe and persistent asthma not well controlled with ICS and LABA 17
18 Mepolizumab in Asthma Mepolizumab in Asthma 18

19 Mepolizumab in Asthma- Steroid Reduction 19
20 20




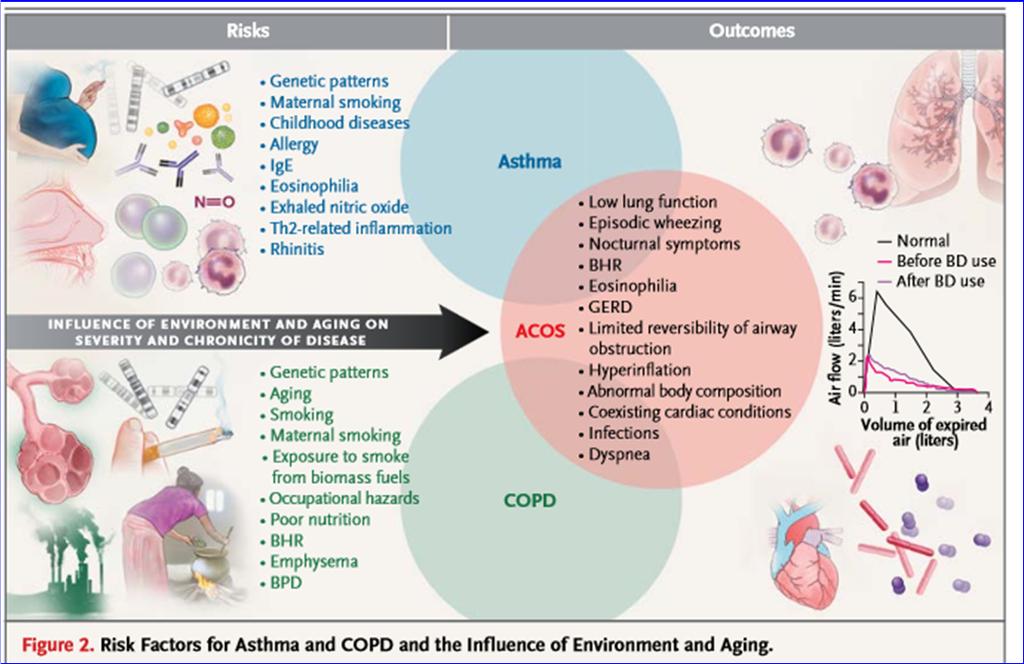
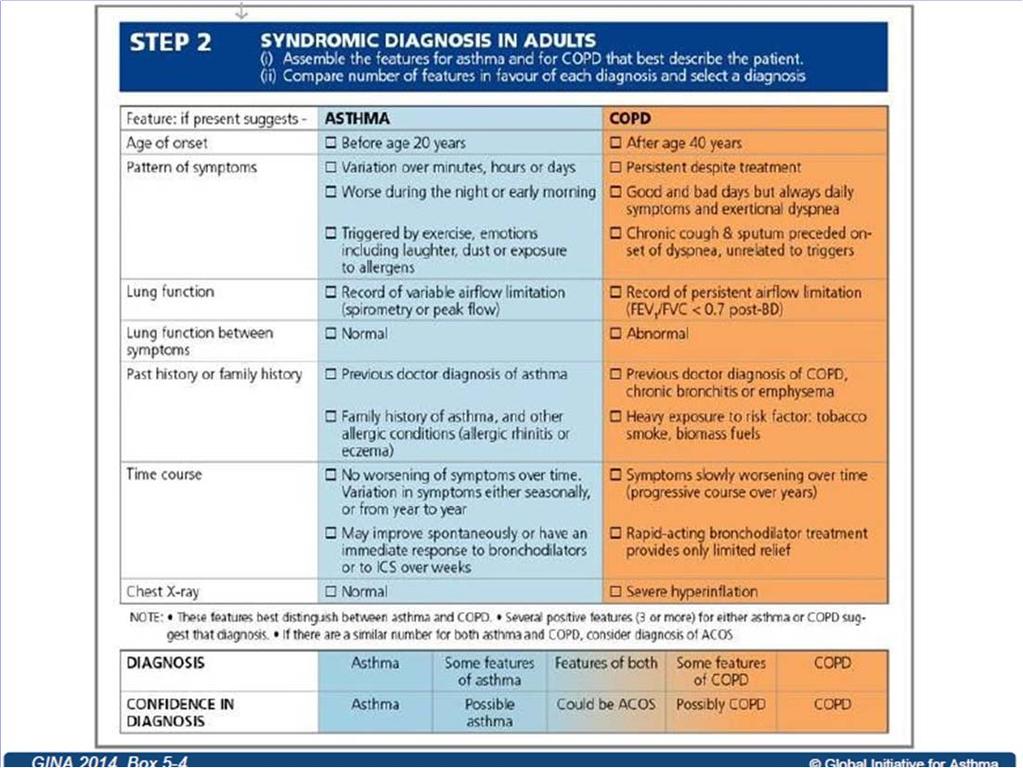
21 Clinical Overlap Between COPD and Asthma COPD Smoking history Progressive dyspnea; productive cough Bronchodilator response: AC>BA Asthma Early and/or family history Intermittent wheezing; hay fever; atopy Bronchodilator response: BA>AC Neutrophilic inflammation Eosinophilic inflammation AC= Anticholinergic BA= 2 -agonist. Airflow Limitation Adapted by Christopher B. Cooper, MD. Barnes. Chest. 2000;117:10S-14S; Balmes et al, for the American Thoracic Society. Am J Respir Crit Care Med. 2003;167:
22 22
23 23

24 Summary Asthma is a complex group of diseases with multiple phenotypes and treatments Asthma severity is an intrinsic characteristic that guides therapy Asthma control can be influenced by a number of important modifiable factors Asthma and COPD can coexist in a significant proportion of patients. 24



25 25
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D.
 Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
Global Initiative for Asthma (GINA) What s new in GINA 2015?
 What s new in GINA 2015?") Global Initiative for Asthma (GINA) What s new in GINA 2015? GINA Global Strategy for Asthma Management and Prevention What s new in GINA 2015 (1) Add-on tiotropium by soft-mist inhaler is a new other
Global Initiative for Asthma (GINA) What s new in GINA 2015? GINA Global Strategy for Asthma Management and Prevention What s new in GINA 2015 (1) Add-on tiotropium by soft-mist inhaler is a new other
Global Initiative for Asthma (GINA) What s new in GINA 2017?
 What s new in GINA 2017?") Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Asma e BPCO: le strategie terapeutiche
 Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Asma e BPCO: le strategie terapeutiche Dott. Marco Contoli ctm@unife.it Sezione di Medicina Interna e Cardio-Respiratoria Dipartimento di Scienze Mediche Università di Ferrara COPD Definition Chronic Obstructive
Do We Need Biologics in Pediatric Asthma Management?
 Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma
 The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2018 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications
 The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital
 Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Traiter l asthme sévère par le phénotype. Dr. Alain Michils CUB-Hôpital Erasme
 Traiter l asthme sévère par le phénotype Dr. Alain Michils CUB-Hôpital Erasme Darwin 25 mars 2017 Step 5 treatment (GINA 2016) STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP
Traiter l asthme sévère par le phénotype Dr. Alain Michils CUB-Hôpital Erasme Darwin 25 mars 2017 Step 5 treatment (GINA 2016) STEP 5 STEP 4 PREFERRED CONTROLLER CHOICE STEP 1 STEP 2 Low dose ICS STEP
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters
 Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
Changing Epidemiology: Quick Facts 9/28/2018. During the year New Treatment Options for COPD: Phenotypes, Endotypes or Treatable Traits?
 New Treatment Options for COPD: Phenotypes, Endotypes or Treatable Traits? Conflict of Interest Statement 2018 Speakers Bureau Astra Zeneca Boehringer Ingelheim Genentech Sunovion Ron Balkissoon MD DIH
New Treatment Options for COPD: Phenotypes, Endotypes or Treatable Traits? Conflict of Interest Statement 2018 Speakers Bureau Astra Zeneca Boehringer Ingelheim Genentech Sunovion Ron Balkissoon MD DIH
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Who can get most benefit
 Who can get most benefit from tiotropium in asthma? Y-M. Oh Asan Medical Center Univ. of Ulsan College of Medicine Seoul, Korea Tiotripium for Asthma 1 New in GINA 2015 Add-on tiotropium by soft-mist inhaler
Who can get most benefit from tiotropium in asthma? Y-M. Oh Asan Medical Center Univ. of Ulsan College of Medicine Seoul, Korea Tiotripium for Asthma 1 New in GINA 2015 Add-on tiotropium by soft-mist inhaler
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2017 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Health Professionals Updated 2017 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
New TLD Indication: Asthma RELIEF-1 Study. Nick ten Hacken, MD Study Co-Principal Investigator
 New TLD Indication: Asthma RELIEF-1 Study Nick ten Hacken, MD Study Co-Principal Investigator The Burden of Asthma WW Adult Asthma Prevalence 230.5 Million Mild/Intermittent 161.9 Million (70%) Moderate
New TLD Indication: Asthma RELIEF-1 Study Nick ten Hacken, MD Study Co-Principal Investigator The Burden of Asthma WW Adult Asthma Prevalence 230.5 Million Mild/Intermittent 161.9 Million (70%) Moderate
CHALLENGES OF REAL LIFE ASTHMA MANAGEMENT. Dr Chris Lewis Respiratory Physician and Director of Prevocational Training Auckland District Health Board
 CHALLENGES OF REAL LIFE ASTHMA MANAGEMENT Dr Chris Lewis Respiratory Physician and Director of Prevocational Training Auckland District Health Board CONFLICT OF INTEREST Employee of Auckland District Health
CHALLENGES OF REAL LIFE ASTHMA MANAGEMENT Dr Chris Lewis Respiratory Physician and Director of Prevocational Training Auckland District Health Board CONFLICT OF INTEREST Employee of Auckland District Health
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA
, BRONCHIAL ASTHMA") CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Asthma Update Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine
 Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine Goals/Objectives Review of 2014 GINA guidelines Significant
Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine Goals/Objectives Review of 2014 GINA guidelines Significant
Management of Severe Asthma Including Biologics and Bronchial Thermoplasty. Karen L. Gregory, DNP, APRN, CNS, RRT, AE-C, FAARC
 Management of Severe Asthma Including Biologics and Bronchial Thermoplasty Karen L. Gregory, DNP, APRN, CNS, RRT, AE-C, FAARC Disclosures ALK speaker Monaghan Medical Corporation speaker Novartis speaker
Management of Severe Asthma Including Biologics and Bronchial Thermoplasty Karen L. Gregory, DNP, APRN, CNS, RRT, AE-C, FAARC Disclosures ALK speaker Monaghan Medical Corporation speaker Novartis speaker
ACTIVITY DISCLAIMER. Additional Disclosure DISCLOSURE. Learning Objectives. Asthma in Adults: A Breathless Update. COL Douglas Maurer, DO, MPH, FAAFP
 ACTIVITY DISCLAIMER Asthma in Adults: A Breathless Update COL Douglas Maurer, DO, MPH, FAAFP The material presented here is being made available by the American Academy of Family Physicians for educational
ACTIVITY DISCLAIMER Asthma in Adults: A Breathless Update COL Douglas Maurer, DO, MPH, FAAFP The material presented here is being made available by the American Academy of Family Physicians for educational
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Severe Asthma & Exacerbations: Dawn of a New Era?
 Severe Asthma & Exacerbations: Dawn of a New Era? Christophe von Garnier Department of Pulmonary Medicine Syndromes, Phenotypes & Endotypes Asthma Syndrome Variable symptoms, expiratory airflow limitation,
Severe Asthma & Exacerbations: Dawn of a New Era? Christophe von Garnier Department of Pulmonary Medicine Syndromes, Phenotypes & Endotypes Asthma Syndrome Variable symptoms, expiratory airflow limitation,
December 7, 2010 Future Use of Biologics in Allergy and Asthma
 December 7, 2010 Future Use of Biologics in Allergy and Asthma Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
December 7, 2010 Future Use of Biologics in Allergy and Asthma Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Brooke L. Gildon, Pharm.D., BCPS, BCPPS, AE C
 Brooke L. Gildon, Pharm.D., BCPS, BCPPS, AE C Associate Professor of Pharmacy Practice Southwestern Oklahoma State University College of Pharmacy Oklahoma Society of Health System Pharmacists Annual Meeting
Brooke L. Gildon, Pharm.D., BCPS, BCPPS, AE C Associate Professor of Pharmacy Practice Southwestern Oklahoma State University College of Pharmacy Oklahoma Society of Health System Pharmacists Annual Meeting
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION
 POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Revised 2014 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
POCKET GUIDE FOR ASTHMA MANAGEMENT AND PREVENTION (for Adults and Children Older than 5 Years) A Pocket Guide for Physicians and Nurses Revised 2014 BASED ON THE GLOBAL STRATEGY FOR ASTHMA MANAGEMENT AND
Asthma 2015: Establishing and Maintaining Control
 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015 Asthma Prevalence Approx. 26
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Asthma Upate 2018: What s New Since the 2007 Asthma Guidelines of NAEPP?
 10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Step up if needed (first, check adherence, environmental control and comorbid conditions) Patients ASSESS CONTROL. Step down if possible
 Patients ASSESS CONTROL. Step down if possible") 12/9/212 Pharmacogenomics Treating the Individual Asthma Patient Elliot Israel, M.D. Professor of Medicine Harvard Medical School Brigham & Women s Hospital Partners Asthma Center Too much of a good thing?
12/9/212 Pharmacogenomics Treating the Individual Asthma Patient Elliot Israel, M.D. Professor of Medicine Harvard Medical School Brigham & Women s Hospital Partners Asthma Center Too much of a good thing?
New Therapies for Asthma
 New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
PCRS-UK briefing document Asthma guidelines. November 2017
 PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
ASTHMA BEST PRACTICES FOR SCHOOL NURSES. School Nurses November 2015
 ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Methacholine versus Mannitol Challenge in the Evaluation of Asthma Clinical applications of methacholine and mannitol challenges
 Methacholine versus Mannitol Challenge in the Evaluation of Asthma Clinical applications of methacholine and mannitol challenges AAAAI San Antonio Tx February 2013 Catherine Lemière MD, MSc Hôpital du
Methacholine versus Mannitol Challenge in the Evaluation of Asthma Clinical applications of methacholine and mannitol challenges AAAAI San Antonio Tx February 2013 Catherine Lemière MD, MSc Hôpital du
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Respiratory Subcommittee of PTAC meeting held 5 February (minutes for web publishing)
") Respiratory Subcommittee of PTAC meeting held 5 February 2010 (minutes for web publishing) Respiratory Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Respiratory Subcommittee of PTAC meeting held 5 February 2010 (minutes for web publishing) Respiratory Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma in Pregnancy. Michael Schatz, MD, MS Department of Allergy Kaiser Permanente Medical Center San Diego, CA. Introduction
 Asthma in Pregnancy Michael Schatz, MD, MS Department of Allergy Kaiser Permanente Medical Center San Diego, CA Introduction Asthma is the most common potentially serious medical problem to complicate
Asthma in Pregnancy Michael Schatz, MD, MS Department of Allergy Kaiser Permanente Medical Center San Diego, CA Introduction Asthma is the most common potentially serious medical problem to complicate
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
LINEE GUIDA DELL ASMA: UP TO DATE
 LINEE GUIDA DELL ASMA: UP TO DATE Azienda Ospedaliera Pisana Università degli Studi di Pisa Pierluigi Paggiaro GINA International Executive Committee, Chairman GINA ITaly Cardio-Thoracic and Vascular Department,
LINEE GUIDA DELL ASMA: UP TO DATE Azienda Ospedaliera Pisana Università degli Studi di Pisa Pierluigi Paggiaro GINA International Executive Committee, Chairman GINA ITaly Cardio-Thoracic and Vascular Department,
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred inhaler choices
 ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches
 Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Long Term Care Formulary RS -29
 RESTRICTED USE Asthma/COPD Management 1 of 6 PROTOCOL: Asthma Glossary of Medication Acronyms: SABA: short-acting beta agonist (e.g. salbutamol) SABD: short-acting bronchodilator (e.g. ipratropium or SABA)
RESTRICTED USE Asthma/COPD Management 1 of 6 PROTOCOL: Asthma Glossary of Medication Acronyms: SABA: short-acting beta agonist (e.g. salbutamol) SABD: short-acting bronchodilator (e.g. ipratropium or SABA)
Add on therapy in asthma. Local experience in context J Paul Dilworth, Nicola Marks, Lauren Geddes
 Add on therapy in asthma Local experience in context J Paul Dilworth, Nicola Marks, Lauren Geddes Programme Omalizumab Evidence and assessment Local Experience Dysfunctional breathing The other effective
Add on therapy in asthma Local experience in context J Paul Dilworth, Nicola Marks, Lauren Geddes Programme Omalizumab Evidence and assessment Local Experience Dysfunctional breathing The other effective
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Methods to Diagnose Adherence Status
 Methods to Diagnose Adherence Status March 4, 2014 Andrew G Weinstein MD Associate Clinical Professor Pediatrics Jefferson Medical College President, Adherence Management Systems Disclosures President,
Methods to Diagnose Adherence Status March 4, 2014 Andrew G Weinstein MD Associate Clinical Professor Pediatrics Jefferson Medical College President, Adherence Management Systems Disclosures President,
Asthma Update I have no professional or personal financial conflicts of interest to disclose.
 Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update Jennifer W. McCallister, MD, FACP, FCCP
 Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
DoH Guidelines for the Initial Diagnosis and Management of Asthma in adults ( 18yrs) by Primary Healthcare Providers
 by Primary Healthcare Providers") DoH Guidelines for the Initial Diagnosis and Management of Asthma in adults ( 18yrs) by Primary Healthcare Providers April 2018 1 Page Document Title: DoH Guidelines for the Initial Diagnosis and Management
DoH Guidelines for the Initial Diagnosis and Management of Asthma in adults ( 18yrs) by Primary Healthcare Providers April 2018 1 Page Document Title: DoH Guidelines for the Initial Diagnosis and Management
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Preschool Asthma What you need to know in 10 minutes
 Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Adult Summary flowchart for Asthma Switch and Step Down to preferred inhaler choices
 HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Injectable Asthma Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Injectable Asthma Agents Xolair (omalizumab) Prime Therapeutics will
Injectable Asthma Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Injectable Asthma Agents Xolair (omalizumab) Prime Therapeutics will
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Case-Compare Impact Report
 Case-Compare Impact Report October 8, 20 For CME Activity: Developed through an independent educational grant from Genentech: Moderate to Severe Persistent Asthma: A Case-Based Panel Discussion (March
Case-Compare Impact Report October 8, 20 For CME Activity: Developed through an independent educational grant from Genentech: Moderate to Severe Persistent Asthma: A Case-Based Panel Discussion (March
Treatment of Severe Asthma: Biologics to Bronchial Thermoplasty. Disclosures
 Treatment of Severe Asthma: Biologics to Bronchial Thermoplasty Monica Kraft, M.D. Robert and Irene Flinn Professor of Medicine Chair, Department of Medicine Deputy Director, Asthma and Airway Disease
Treatment of Severe Asthma: Biologics to Bronchial Thermoplasty Monica Kraft, M.D. Robert and Irene Flinn Professor of Medicine Chair, Department of Medicine Deputy Director, Asthma and Airway Disease
Objectives. Asthma in Primary Care. Definition. Epidemiology. Pathophysiology
 Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Objectives Asthma in Primary Care Jed Grant, PA-C Program Director, SJVC PA Program Staff PA, AMCH Emergency Department Apply the NAEPP guideline measures of severity and control including current impairment
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Pediatric and Adult. Disclosure. Asthma. Learning Objectives. EPR-3: What s Changed? Asthma: Pediatric and Adult
 Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Treatment Options for Complicated/Severe Asthma. Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology
 Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the