What lung function data are relevant concerning the assessment of COPD patients for out patient rehabilitation?
|
|
|
- Brian Lewis
- 6 years ago
- Views:
Transcription

1 What lung function data are relevant concerning the assessment of COPD patients for out patient rehabilitation? An information package on lung function tests and interpretation of test data in identifying limitations in COPD out patients. Professional assignment of Lena Fick and Geraldine Mullins European School of Physiotherapy Hogeschool van Amsterdam Amsterdam, February 2006
2 Preface We wish to acknowledge and thank all those who helped and gave us support and advice throughout this project. Mr Bob van den Berg, our coach. European School of Physiotherpay, Hogeschool van Amsterdam. Mr Geert Vijsma and all the staff at the lung function test department at Sint Lucas Andreas Hospital. Mr Janno Barlage and Mr Murni Latif and all the staff at the physiotherapy department at Sint Lucas Andreas Hospital. 2
3 Summary Chronic Obstructive Pulmonary Disease is a growing worldwide problem. It has been proved that participating in a rehabilitation programme improves the patient s quality of life and exercise capacity. Physiotherapists are key figures in planning and implementing patients rehabilitation programmes. It is recommended in the KGNF guidelines that physiotherapists should have the relevant expertise and the diagnostic and therapeutic skills necessary to treat these patients and that they should be familiar with the measuring instruments used in pulmonary assessment and be familiar with the interpretation of incremental exercise test results. Pulmonary function testing includes amongst others, spirometry, plethysmography and cardio pulmonary exercise testing (CPET). The data obtained from spirometry and plethysmography is useful for diagnosing, measuring the severity of and evaluating the effects of treatment of COPD. The data from the CPET is indispensable for identifying exercise limitations such as cardiovascular and ventilatory restrictions. The ability to interpret the data provides the physiotherapist with an invaluable tool to assist with the planning, implementation and evaluation of the individual s treatment plan. 3
4 Introduction The topic we chose for our assignment is the interpretation of pulmonary function test data, focusing on the limitations affecting COPD patients when planning outpatient rehabilitation programmes. Chronic Obstructive Pulmonary Disease is a major cause of morbidity and mortality throughout the world. Its prevalence is increasing and it is the only major leading cause of death that is increasing. Pulmonary rehabilitation programmes are firmly established as a successful method to treat the patient. The physiotherapist is a key figure in the rehabilitation programme and responsible for planning and implementing the exercise component of the programme. In order to be able to competently structure an individual s treatment, it is essential that the therapist is able to recognise the limitations to exercise that the COPD patient can present with. The patients programme can then be adapted to minimise the effect of the particular limitation. Pulmonary function testing is frequently part of routine pre rehabilitation programme assessment. The data obtained are used to diagnose, plan treatment, monitor and evaluate effects of treatment. They are used to identify the limitations to exercise. The results provide the physiotherapist with an important tool for planning the patients rehabilitation programme because they provide a means of identification of the limiting factors that will affect the patients progress or ability to participate or benefit from the programme. According to the guidelines produced by the KNGF, physiotherapists working in the area of pulmonary rehabilitation should have the relevant expertise and the diagnostic and therapeutic skills needed to treat these patients. (KNGF 2003, pp. 12) It is also recommended that the therapist should be familiar with the measuring instruments used in pulmonary assessment and be familiar with the interpretation of incremental exercise test results. The focus of our project is the interpretation and analysis of the data from lung function tests for junior physiotherapists or student physiotherapists and the application of the data to the physiotherapy treatment of COPD out patients. Chapter 1 provides the reader with a general introduction to COPD; outpatient s rehabilitation programmes and briefly describes the limitations that can influence the structure and planning of the patient s individual programme. Chapter 2 provides the reader with a description of the individual tests and how they are performed. Chapter 3 describes the interpretation of the tests, focusing on COPD out patient rehabilitation. The interpretation is based on the particular tests that are performed at the St. Lucas Andreas hospital. 4
5 Table of contents PREFACE... 2 SUMMARY... 3 INTRODUCTION... 4 TABLE OF CONTENTS... 5 CHAPTER ONE... 6 COPD... 6 Emphysema... 6 Chronic bronchitis... 6 REHABILITATION PROGRAMMES FOR COPD OUT-PATIENTS... 8 EXERCISE LIMITATIONS... 9 CHAPTER TWO BRIEF HISTORY REFERENCE CRITERIA SPIROMETRY PLETHYSMOGRAPHY SINGLE BREATH DIFFUSING CAPACITY MAXIMAL INSPIRATORY PRESSURE (MIP OR PIMAX) AND THE MAXIMAL EXPIRATORY PRESSURE (MEP OR PEMAX) TEST CARDIOPULMONARY EXERCISE TEST (CEPT)/ MAXIMAL AEROBIC CAPACITY TEST CHAPTER THREE SPIROMETRY (THE MEASURING OF BREATH) PLETHYSMOGRAPHY DIFFUSING CAPACITY (PULMONARY GAS TRANSFER INDEX) Degree of severity of decrease in diffusing capacity for carbon monoxide.. 23 MAXIMAL INSPIRATORY PRESSURE AND MAXIMAL EXPIRATORY PRESSURE MAXIMAL BIKE TEST (CARDIOPULMONARY EXERCISE TEST) Ventilatory limitation: Cardiovascular limitation: Peripheral muscle limitation: Psychosocial limitation or poor effort: ARTERIAL BLOOD GASES (ABG) Normal values CONCLUSION REFERENCES FURTHER READINGS Appendix 1 (Cardiopulmonary exercise test flowchart) Appendix 2 (Glossary) APPENDIX 3 (LUNG FUNCTION TEST DATA)
6 Chapter one The first chapter will provide the reader with general information on COPD and some statistics and epidemiology. COPD out patient rehabilitation programmes are described and information on possible exercise limitations in COPD patients is provided. COPD Chronic obstructive pulmonary disease COPD is a condition of chronic diffuse irreversible airway obstruction. It is defined by progressive, irreversible airflow limitation and an inflammatory response of the lungs, usually to cigarette smoke (Lapperre et al. 2004, pp. 499). COPD is a disease mainly of adults over 45 years old who usually have a history of risk factors such as cigarette smoking or exposure to airborne pollution. It is a slowly progressive disease of the airways characterized by gradual loss of lung function. COPD has been recognized as a disorder with components of chronic bronchitis, small airways disease, emphysema, and, in some patients perhaps, features of asthma (Mannino 2002, pp.122). Emphysema Emphysema is characterized by the destruction of the alveolar walls, as well as atrophy and collapse of the lower airways - those from the terminal bronchioles on down. The lungs actually undergo self destruction by proteolytic enzymes secreted by leucocytes in the lungs in response to a variety of factors. Cigarette smoking is by far the most important of these factors; it exerts its action by stimulating the release of the proteolytic enzymes and by destroying the other enzymes that normally protect the lung against the proteolytic enzymes. As a result of alveolar-wall loss, adjacent alveoli fuse to form fewer but larger alveoli, and there is a loss of the pulmonary capillaries that were originally in the walls. The merging of alveoli, often into huge balloon-like structures, reduces the total surface area available for diffusion, and this impairs gas exchange. Moreover, even more important, because the destructive changes are not uniform throughout the lungs, some areas may receive large amounts of air and little blood, while others have just the opposite pattern; the result is marked ventilation-perfusion inequality. In addition to problems in gas exchange, emphysema is associated with a marked increase in airway resistance, which greatly increases the work of breathing and, if severe enough, may cause hypoventilation. The airway obstruction in emphysema is due to the collapse of the lower airways due to the destruction of the elastic tissues in the lung. (Vander 2004, pp.477). It (emphysema) is defined pathologically as the presence of permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis (Snider et all. 1986, pp.182). Chronic bronchitis Chronic bronchitis is characterized by excessive mucus production in the bronchi and chronic inflammatory changes in the small airways. The cause of obstruction 6
7 is an accumulation of mucus in the airways and thickening of the inflamed airways (Vander 2004, pp 480). In patients with COPD either of those conditions may be present. However, the relative contribution of each to the disease process is often difficult to determine as the conditions can and frequently do co exist. COPD is not only a disorder of the lungs but also has serious implications for the patient s systemic health. The negative impact of airflow obstruction begins in the early natural history of COPD. Mild airflow limitation early in the disease can result in reduced activities of daily living and a gradual and possibly imperceptible reduction in activity level. A cycle of reduced activity and reduced aerobic endurance is introduced and contributes to a state of premature morbidity well before advanced states of airflow obstruction and COPD occur. The psychological effects of COPD which include anxiety, depression and somatic preoccupation (Petty 1994, pp.1637) will increase the negative impact. Food intake may be decreased because of smoking, dyspnoea or excessive sputum production with resulting deficits in caloric intake, protein intake and a lack of antioxidant vitamins. This will result in multiorgan effects including immune system deficiency and increased susceptibility to infection with resulting metabolic and nutritional stresses on the patient. Progressive functional decline is inevitable. The cost of COPD is high. It has effects on morbidity, mortality and economics. It is estimated that the condition affects 600 million people worldwide and its incidence is increasing (WHO 1998). COPD was the cause of 2.74 million deaths in 2000 (WHO 2001). According to the American Lung Association, COPD is an increasing problem and is an area of growing demand on health services worldwide. It is the fourth leading cause of death in the U.S. (ALA 2005). Respiratory disease is the third most common cause of death in the E.U. (Siafakes et al. 1995, pp.1416). The national heart, lung and blood institute in the United States has estimated COPD to have cost the health system there $37.2 billion in It is the reason for 16 million doctor visits and 500,000 hospital admissions annually. Lost productivity due to COPD has a particularly high impact on the economy, accounting for 67% of overall costs in France, 50% in the Netherlands and 41% in the UK (Wouters 2003, pp.12) In the Netherlands, 46% of COPD patients are unable to hold down a full time job due to symptoms. The average sick leave for a working person in the Netherlands is 22 days. This is much increased in COPD patients with figures of 77 days annually for chronic bronchitis patients and 167 days annually off sick for emphysema patients. Prevalence figures for COPD are believed to be underestimated. It has been estimated that 75% of COPD cases in the general population remain undiagnosed. (Siafakas et al, 1995, pp. 1400) It is difficult to accurately estimate the prevalence of COPD in the general population because it is often undiagnosed for several reasons. Reference criteria and diagnostic criteria differ amongst countries. The disease is often asymptomatic in its early stages and the symptoms have an insidious pattern so the patient in the early or moderate stage of the disease is unaware of its presence. Symptoms are often not evident until 7
8 the patient is middle aged or elderly and can be attributed to increasing age. Sufferers tend not to seek medical advice until the disease has progressed and the condition is severe and by the time the disease is diagnosed, often < 50% of lung function has already been lost and the need for healthcare is high. (Engstrom et al. 2001, pp. 74). According to National Heart, Lung and Blood Institute (1998), COPD is the only major leading cause of death that is increasing. Coronary heart disease, stroke and other CVDs all show consistent and substantial reduction. The cost to the quality of life of the patient is also high. The symptoms of the disease contribute to functional deficits with up to almost three out of four patients with COPD report difficulty in the simplest of everyday activities, being out of breath after simply walking upstairs (Vermeire 2002, pp.s7). Significant exercise limitation is present in patients with only modest degrees of airflow obstruction (Carter et al. 1993, pp. 746). Participation in everyday activities and restrictions regarding work and social activities lead to a reduction in quality of life, with 80% of patients hospitalized following an exacerbation reporting a health status rated or quoted by a physician as being worse than death (O Reilly et al 2003). Social isolation and resulting depression is common amongst patients and also their carers are affected with one study on a small population of patients with COPD in Australia demonstrating that levels of loneliness, social isolation and depression are similar among carers and their patients. Rehabilitation Programmes for COPD Out-Patients Out-patients rehabilitation programs have been proven to be effective. It has been shown that patients who take part in a rehabilitation program show significant improvement in the 6 minutes walking test in comparison to a control group (Finnerty et al. 2001, pp.1708, Salman et al. 2003, pp.215). Furthermore significant improvement in quality of life in patients with COPD has been shown in comparison to control groups of COPD patients (Finnerty et al. 2001, pp.1707). It also has been proved that exercise increases the bronchial mucus transport (Oldenburg et al. 1979, pp. 744). Furthermore it has been shown that exercise programs as a part of the rehabilitation program has a positive effect on the maximal and sub maximal exercise capacity of COPD patients (Pies et al. 1995, pp. 830). In general an improvement in exercise capacity, reduction in exertional dyspnoea and an improvement in health status can be observed after rehabilitation programs (American Thoracic Society & European Respiratory Society. 2004, pp.100). However, it should be noted that there is nearly no improvement of the actual lung function data (American Thoracic Society & European Respiratory Society.2004, pp.100). Also it has been shown that patients with mild or moderate COPD can benefit from long and short term rehabilitation programs while patients with severe COPD need a rehabilitation program for at least 6 months before they benefit from it (Salman et al.2003, pp ). The main goals of rehabilitation programs for COPD patients are reduction of the patient s disability and to promote a general improvement of quality of life. 8
9 The minimum of an outpatients rehabilitation programme should be 6 weeks with 2 supervised sessions per week and additional instruction to train at home on a daily basis (British Thoracic Society. 2001, pp. 829). A regular rehabilitation programme contains physical exercise, disease education as well as nutritional, psychological, social and behavioural interventions (British Thoracic Society. 2001, pp.829). According to the KNGF guidelines (2003, pp.9, 26) a rehabilitation program should include physical exercises, educational intervention and support for the patient. The physical exercises include aerobic training, peripheral muscle strengthening as well as inspiratory muscle training. It is important that rehabilitation programs involve a multidisciplinary team and the patient s family; however it is also important to look at the individuals needs. Exercise limitations In order to plan the patient s rehabilitation program it is essential to know which factor is limiting the patients exercise capacity. The KNGF guidelines from 2003 mention five different exercise capacity limitations, which are cardio circulatory limitation, ventilatory limitation, oxygen transport limitation, peripheral muscle weakness and other factors such as psychosocial limitation. A cardio circulatory limitation implicates that there is a problem with the cardiovascular system. The cardiovascular system consists of the heart and the two networks of blood vessels the systemic circulation and the pulmonary circulation. Failure of the cardiovascular system has effects on the circulation of the blood around the body and therefore it also has effects on oxygen transport to the tissue and the removal of waste products from the tissue. In the case of a ventilatory limitation, the ventilatory requirement can not be met because it is normally increased in COPD patients while the ventilatory capacity tends to be decreased. In the case of emphysema the ventilatory capacity is reduced due to an increased airflow obstruction in combination with reduced lung elastic recoil while in the case of chronic bronchitis and asthma the reduced ventilatory capacity is caused by an increased airflow resistance. In COPD patients the increased ventilatory requirement is mainly caused by inefficient ventilation of the lung as a consequence of mismatching of ventilation to perfusion. Limitation of oxygen transport can be caused by different factors such as diffusion problems which are commonly seen in COPD patients. These problems occur due to alveolar wall breakdown which results amongst other things in decreased surface area for gas exchange and loss of pulmonary capillaries affecting perfusion and the diffusion of gases. Peripheral muscle weakness can become an exercise limitation and is not uncommon in COPD patients. It can be caused by different factors such as metabolic changes, or immobility. The KNGF guidelines also identify other factors that can act as exercise limitations such as psychosocial issues and exercise fear. It is always important to have this in the back of your mind and it can be taken into account by giving the patient education during the rehabilitation program. 9
10 Chapter two In this chapter a brief history of pulmonary lung function testing will be given. The different pulmonary function tests, which are performed at the St Lucas Andreas Hospital, will be described. Each pulmonary function test is described in its own section and the description is done in the same order as the tests are performed at the St Lucas Andreas Hospital. Brief history Pulmonary function test has long history. In A.D. Galen discovered that inspiration-expiration (tidal volumes) volumes do not change over a period of time. The first measurement of inspiration was done by Borelli in R. Menzies was the first person who used the method of body plethysmography in In this cylinder the subject was placed and the changes of water level were measured during inspiration and expiration. In 1844 Hutchinson who was working with spirometers showed that there is a linear relationship between vital capacity and height but that there is no relationship between vital capacity and the body weight. Reference Criteria Reference values are a set of laboratory test values obtained from an individual or from a group in a defined state of health. Many pulmonary function test data are expressed as a percentage of a predetermined normal value. The information for these normal values is derived from the reference criteria. Reference values are taken from studies of healthy individuals of same sex, similar stature, age, and other characteristics such as ethnic origin with no known previous or present conditions that adversely affect their ventilatory function. The characteristics of the healthy reference population should match the study group as much as is possible. The equipment, techniques, and measurement conditions used in the health studies to determine reference criteria should be similar to those used in actual patient testing in order to provide accurate and reliable data. (In fact, the best reference value is the value observed in the subject during a period when the disease is stable and minimal for that person.) At the St Lucas hospital, the reference values are already programmed on the lung function equipment by the manufacturing company and are based on age, body size and gender. However, race is not taken into account so the person interpreting the data has to take into account that there can be a discrepancy in the results that is affected by the subject s race. The person interpreting the test results in any department should be aware of which reference values are used to predict the normal preset values that the patients results are compared to. There are no specific recommended reference criteria in Europe. Therefore there is an urgent need to standardize techniques, equipment and methods of analysis, 10

11 so that individual data from different laboratories can be collated in the future (Stocks and Quanjer 1995). Spirometry The objective of Spirometry is to assess ventilatory function. Spirometry is used to test pulmonary volumes, measuring volume and air flow times. It is used to diagnose, measure the severity of and evaluate the progress of obstructive lung disease. Spirometry is best performed with the patient seated and in an upright position. The patient is required to inhale fully and form a seal around the mouthpiece with their lips. The patient is then required to exhale fully to RV. (Residual Volume). The exhalation must continue until no more air can be exhaled and must last at least 6 seconds. (It may take up to 15 seconds). It is essential that the patient co operates fully. Spirometry results will only be of value if the expirations are performed satisfactorily and consistently. The test results are expressed in 2 graphs on the computer (appendix 3) - a flow volume loop and a time volume curve (Figure 1). The test should be repeated in the same fashion 3 times. Both FVC (Forced Vital Capacity) and FEV1 (Forced Expiratory Volume in 1 second) should be the largest value obtained from any of 3 technically satisfactory curves and the FVC and FEV1 values in these three curves should vary by no more than 5% or 100 ml, whichever is greater. The FEV1/FVC is calculated using the maximum FEV1 and FVC from technically acceptable (not necessarily the same) curves. Figure 1. Spirometry results depicted in graph form during lung function testing. 11

12 Plethysmography Plethysmography is used to measure changes in volume within the body or part of the body from fluctuations in the amount of air or blood it contains. It works by detecting changes in pressure. It is used to measure absolute lung volumes i.e. residual volume, functional residual capacity and total lung capacity. (Spirometry is the standard method for measuring most relative lung volumes; however, it is incapable of providing information about absolute volumes of air in the lung.) Plethysmography is performed with the patient sitting in an upright position inside an airtight box (Figure 2). The patient breathes through a tube with a valve. Initially the patient continues with his/her normal breathing cycle. During the breathing cycle and on instruction from the tester the patient inhales or exhales to a particular volume (usually FRC) and the tester closes a shutter in the valve of the breathing tube for a few seconds. The patient is required to make respiratory efforts against the closed shutter. This feels and looks like panting although no actual breathing takes place as the valve is closed. Each time the patient tries to pant out, the air in the lungs is decompressed slightly and the gas in the box surrounding the patient is compressed slightly. When the patient tries to breathe in, the opposite occurs i.e. the volume of air in the chest decreases and the volume in the box increases. The pressure changes are measured and the amount of gas in the patient s lungs can be calculated. Figure 2. Body Plethysmography is performed in an airtight box. Single Breath Diffusing Capacity The single breath diffusing capacity, or DLCO, is a measure of the ability of the lungs to diffuse oxygen into, and carbon dioxide from, the bloodstream. The test is performed at the same time as plethysmography with the patient sitting in an upright position. The patient expired to RV and then inhales fully to TLC, breathing from a supply of test gas containing a preset amount of carbon monoxide. (Figure 3). The breath is held by the patient for ten seconds and then 12

13 expired forcefully. The concentration of carbon monoxide present in the test gas is measured prior to the test. The initial portion of the final expirate is discarded, and a portion of the remainder is analyzed. Generally, the difference between the concentrations present before the breathhold and after the breathhold indicates the amount of gas that diffuses through the lungs and into the bloodstream. Figure 3. Diffusion capacity equipment and gas. Maximal Inspiratory Pressure (MIP or PImax) and the Maximal Expiratory Pressure (MEP or PEmax) Test The maximal inspiratory pressure (MIP or PImax) and the maximal expiratory pressure (MEP or PEmax) tests are performed as a part of the body plethysmography. For these tests it is necessary that the patient wears a nose clip to avoid breathing through the nose. It is also important that the breathing tube is totally enclosed by the subject s lips. An upright sitting position is essential to ensure the optimal respiratory muscle function. Furthermore it is important that the manoeuvre is performed several of times to reach consistency, two measurements should be within 10% of the highest measured pressure. An adequate period of rest in-between the different manoeuvres is needed. The test obtains two time-pressure graphs one for the inspiration manoeuvre and one for the expiration manoeuvre. Each graph consists of several curves one curve for each manoeuvre. The maximal inspiratory pressure (MIP or PImax) is the greatest sub atmospheric pressure that can be developed during inspiration against an occluded airway. It is normally measured at the residual volume (RV) (Bañez 2000). This measurement is used to assess the strength of inspiration muscles. There are two way to measure the MIP. The maximum static manoeuvre (no flow; Pi, max) and the sniff manoeuvre (with flow through a well defined leak; Psniff, max). At 13
14 the St Lucas Andreas Hospital the maximum static manoeuvre is performed and therefore will only be described. The subject is asked to maximally exhale through a breathing tube until, only the residual volume (RV) is left in the lungs. Then a shutter closes the breathing tube and the subject has to inhale as forcefully as possible and hold this for 1-2 seconds. The shutter is then opened and the patient breaths normally. This test results are expressed in a time-pressure graphs and the most accurate graphs will be used for the interpretation (appendix 3). MEP is usually measured at total lung capacity (TLC). This is an estimation of expiratory muscle strength. To measure the maximal expiratory pressure (MEP or PEmax) the subject is ask to inhale up to the total lung capacity (TLC). At the maximal inspiration a shutter closes the breathing tube and the subject has to exhale as forcefully as possible against the shutter. The patient is again asked to hold this position for 1 2 seconds and then continue to breathe normally. It is advisable that the patient holds his hands against his/her cheeks to reduce the chance of a leak between the lips and the tube. This test results are also expressed in a time-pressure graphs and the most accurate graphs will be used for the interpretation. Cardiopulmonary Exercise Test (CEPT)/ Maximal Aerobic Capacity Test The cardiopulmonary exercise test (CPET) is used for diagnostic and prognostic purposes and also as an assessment tool to assess the response of the patient to treatment. In regards to the COPD patient the cardiopulmonary test is used to detect exercise limitations and to identify potential contributing factors such as heart diseases (e. g. to detect ischemic changes that occur during exercise). It is also used to detect the degree of hypoxemia that occurs during exercise and therefore can be a useful guide to determining if a patient needs supplementary O2 during exercise or rehabilitation. At the St Lucas Andreas Hospital the maximal cardiopulmonary test is performed on a static cycle (figure 4). Before the actual bike test is performed the predicted values are calculated according to Wasserman et al (1999). The predicted values are based on factors such as the patient s weight, height, ethnicity and the level of activity in daily life. The patient s predicted maximal load indicates which protocol is used. The predicted maximal load has to be reached within 10 minutes and the increments in load are dictated by the individual s protocol. For example if the patients predicted maximal load is 100W the 10W/min protocol is used while if the patient s predicted maximal load is 150W the protocol for an increase of 15W/min is used. At the St Lucas Andreas Hospital the following protocols are used: 10 W/min: every 6 sec 1 W increase warm-up 15 W 15 W/min: every 4 sec 1 W increase warm-up 15 W 20 W/min: every 3 sec 1 W increase warm-up 20 W 25 W/min: every 5 sec 2 W increase warm-up 25 W 14

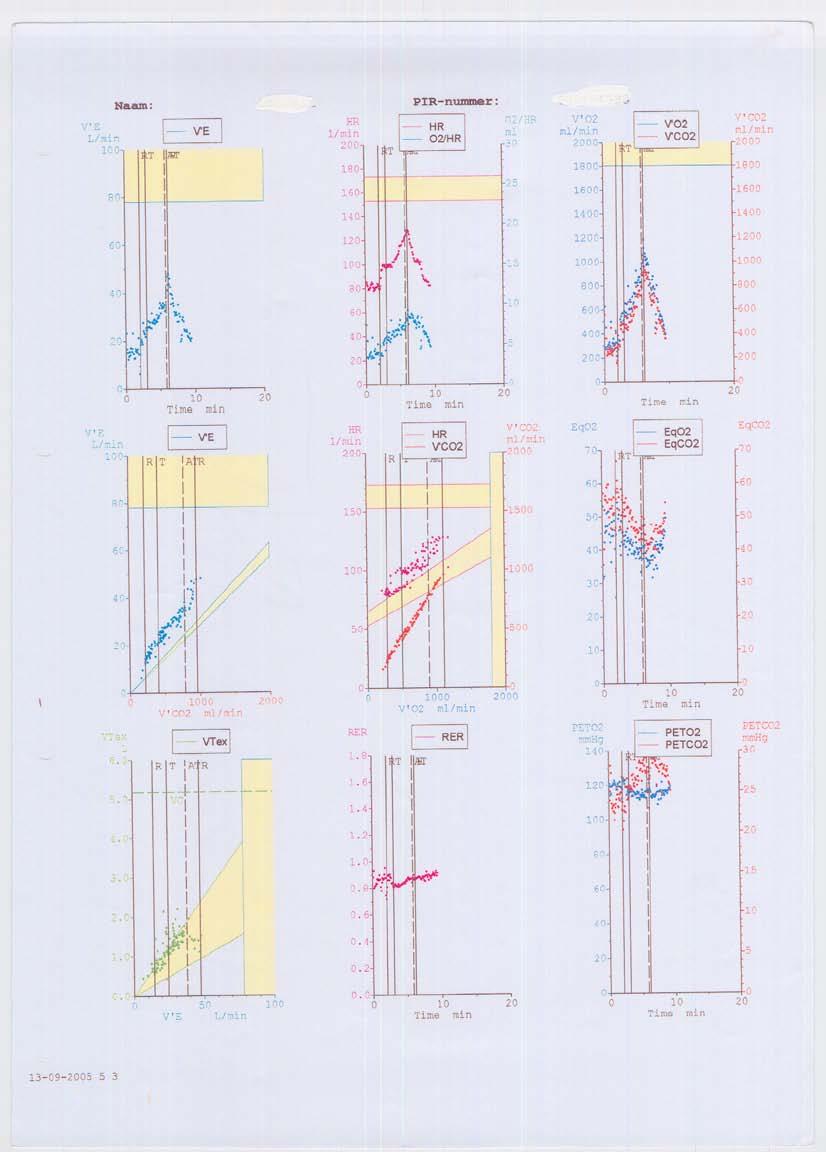
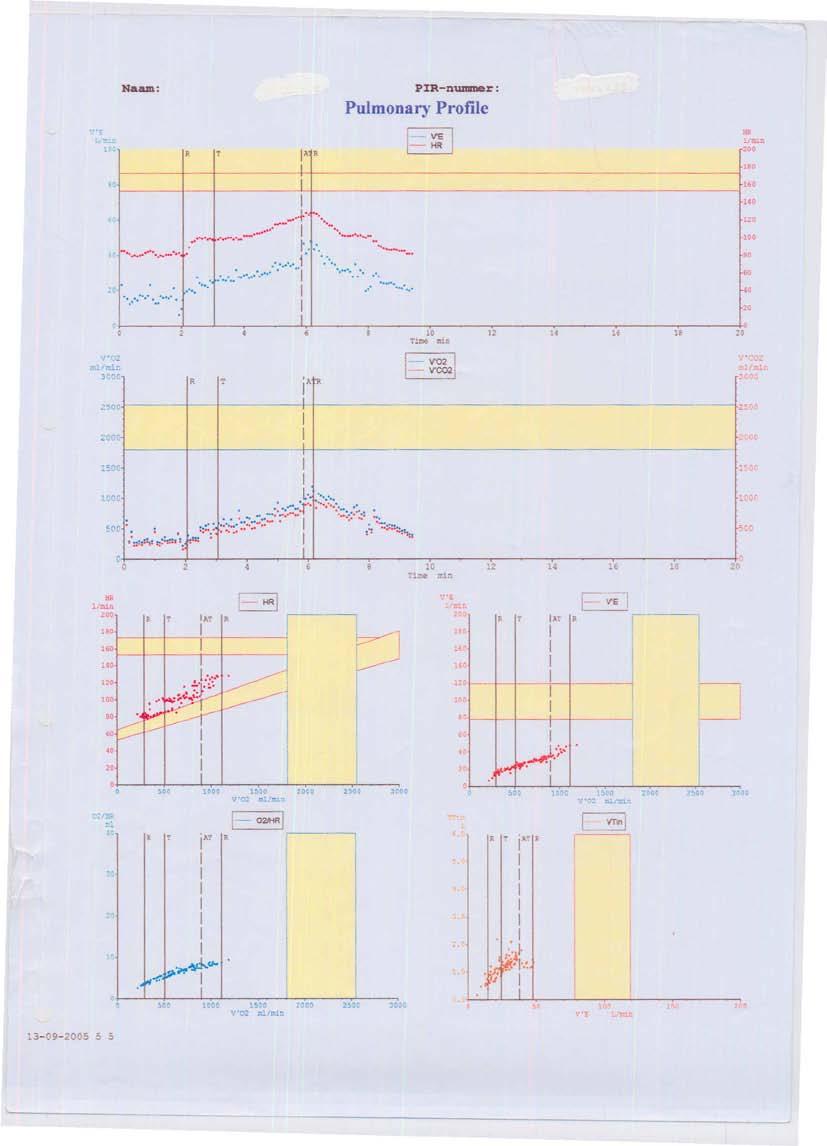
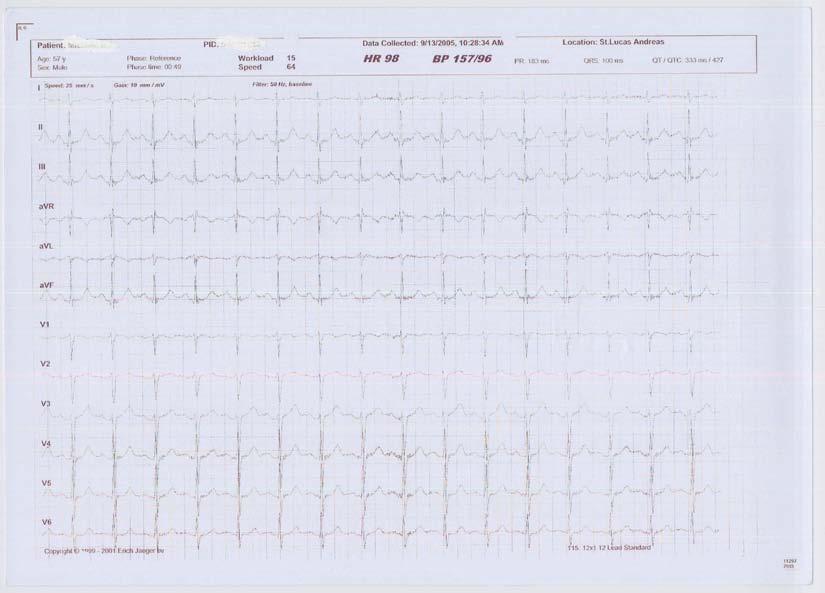
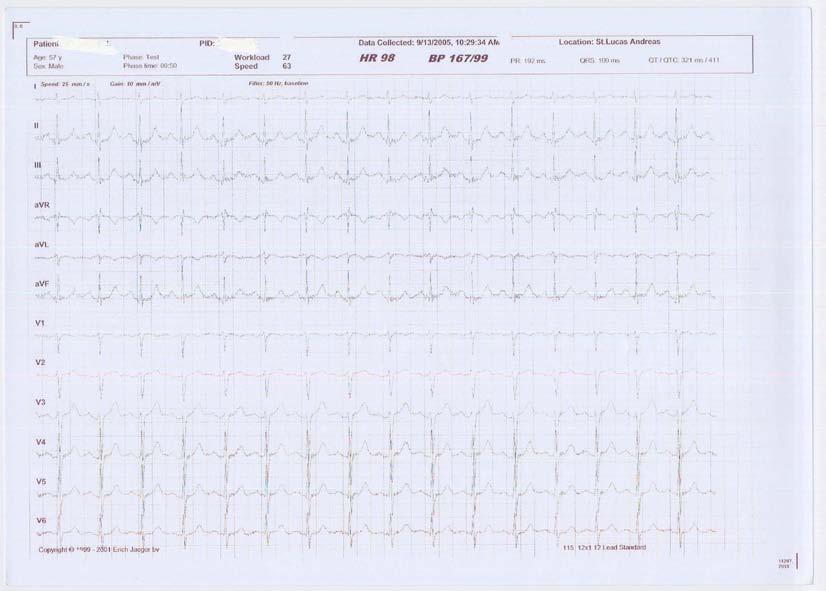
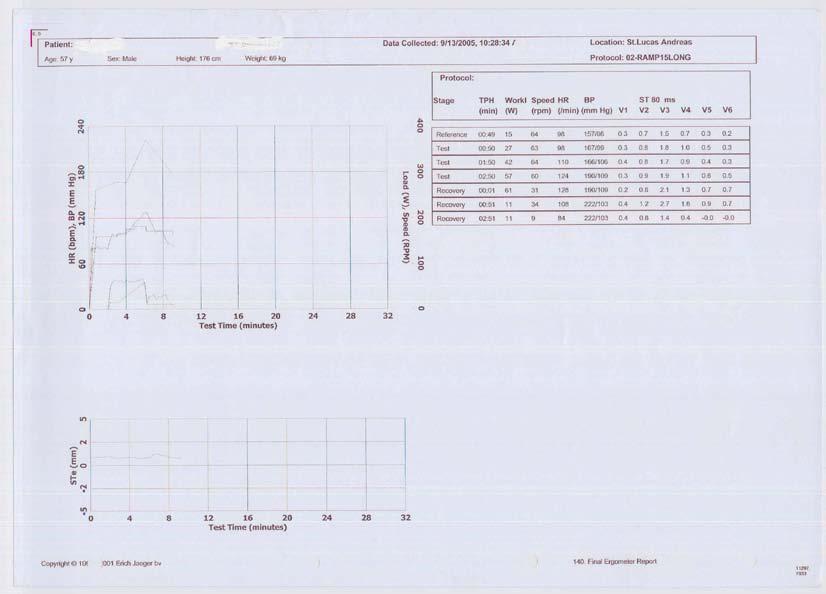
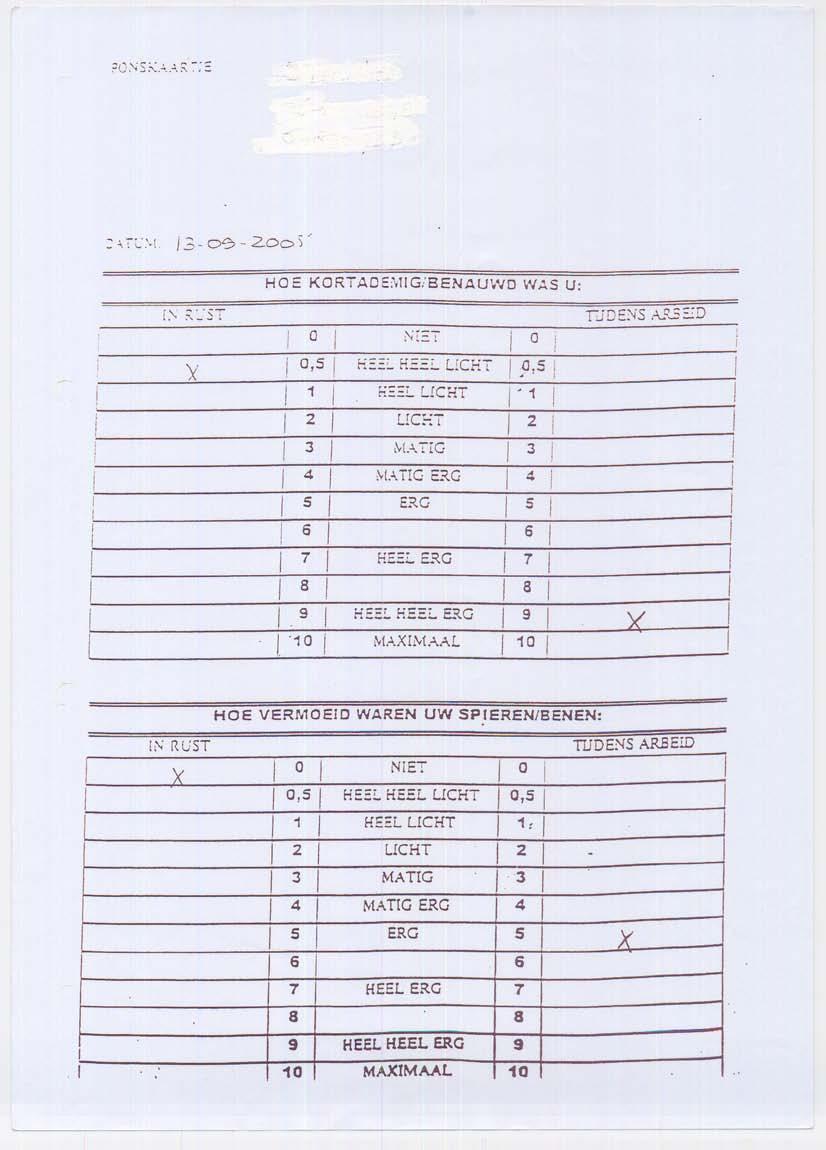
15 30 W/min: every 6 sec 3 W increase warm-up 30 W 40 W/min: every 3 sec 2 W increase warm-up 40 W After calculating the predicted values the patient is positioned on the ergometer and the machine is set up for the maximal exercise test. The patient s condition is monitored throughout the test, a physician is always present and ECG is constantly monitored and the blood pressure is measured. There are certain criteria to stop the exercise test immediately such as chest pain and some ECG or blood pressure irregularities. The subject wears a face masked in order to measure ventilatory values. The O2 saturation is measured by pulse oximetry. Arterial blood is taken by the physician at the beginning of the test and again when the patient reaches his anaerobic threshold (or if not, at the end of the test) to monitor blood gas levels. The procedure is explained to the patient and he is asked to keep a constant repetition per minute (rpm) between rpm throughout the whole test. The subject then starts the test with an unloaded cycling phase for two minutes and from then on, the load is increased steadily according to the individual s protocol. At the completion of the cardiopulmonary exercise test the patient is asked to fill out the Borg-scale (see appendix 3) which provides a subjective estimation of dyspnoea and muscle fatigue. At the St Lucas Andreas Hospital the patient also fills out 3 different Chronic Respiratory Questionnaires (CRQ) (Self reported). Figure 4. Maximal bike test in progress. 15
16 Chapter three Chapter three provides the reader with information on interpretation of the different pulmonary function tests and enables the reader to identify the patient s specific limitation. Spirometry (the measuring of breath) Spirometry is the most common pulmonary function test. The objective of spirometry is to assess ventilatory function by means of measuring lung volumes and the flow or speed that air can be inhaled or exhaled. Spirometry is used for diagnosing, measuring the severity and evaluating the effects of treatment of lung conditions such as COPD and asthma. Spirometry provides measurement of: FVC forced vital capacity FEV1 forced expiratory volume in the first second FEV 1 / FVC - This is the ratio of FEV 1 and FVC, which showing the amount of the FVC that can be expelled in one second. FEF25-75% - Forced Expiratory Flow 25-75% or 25-50% - This is the average flow (or speed) of air coming out of the lung during the middle portion of the expiration (also sometimes referred to as the MMEF, for maximal mid-expiratory flow). MVV maximum voluntary ventilation maximal volume of air that can be breathed per minute Peak Expiratory Flow(PEF) - This is the speed of the air moving out of the lungs at the beginning of the expiration, measured in liters per second, FET Forced Expiratory Time - This measures the length of the expiration in seconds. (Spirometry also provides information about inspiratory parameters but for this project these will not be discussed.) Spirometry primarily detects airways obstruction. In healthy individuals, approximately 80% of forced vital capacity (FVC) is expelled in the first second. (FEV1) This is not the case in people with obstructive lung disease. In obstructive lung diseases such as emphysema or chronic bronchitis, the FEV1 is reduced disproportionately more than the FVC resulting in an FEV1/FVC ratio less than 70-80%. This reduced ratio is the primary criteria for diagnosing obstructive lung disease by spirometry. Asthma can be differentiated from COPD using spirometry because in asthmatic patients the obstruction is reversible. This is demonstrated by administrating prescribed bronchodilators and observing improved test results subsequently. The severity of the disease can also be measured using this method. A reduction in the ratio of FEV1/FVC indicates the severity. 16
17 FEV1 > 80% predicted normal 65-80% mild 50-65% moderate < 50% severe Depending on the severity of the obstruction, the FVC may be reduced as well as the FEV1. However there should continue to be a disproportionate reduction in FEV1 as evidenced by the FEV1/FVC ratio. Spirometry results are commonly expressed diagrammatically and as raw data. The diagrams consist of a time volume curve (Figures 5 & 6) showing volume in liters along the Y-Axis and time (seconds) along the X-Axis and a flow volume loop (Figure 7) which graphically depicts the flow of air compared to the total volume inspired or expired. Forced Expired Volume in 1 Second (FEV 1 ) and Forced Vital Capacity (FVC) Maximum inspiration Volume (litres) Maximum expiration Forced Vital Capacity (FVC) 1 sec Time (seconds) Forced Expired Volume in 1 second (FEV 1 ) Figure 5. Time Volume Curve (Gross 2005) Effect of Airways Obstruction Maximum inspiration Volume (litres) Maximum expiration Normal 1 sec Time (seconds) Obstruction: FEV 1 FEV 1 /FVC Figure 6. Obstructive disease is suggested on the time volume curve by a slower progression to maximum volume than that of a healthy individual. Also, the curve ascends more gradually than that of a healthy individual suggesting a longer expiratory time is needed due to the impairment. (Gross 2005) 17
18 Figure 7. A flow volume loop demonstrating the spirometry flow parameters (Wales 2003). The presence of COPD changes the shape of the flow volume loop (Figure 7). There may be a reduction in the size of the initial peak on the graph (PEF). The curve descends quickly and takes on a concave shape (Figure 8). This indicates a reduction in the FEF25-75 (the volume of air in the mid portion of the exhalation) which occurs when there is collapse of small airways. (This result when expressed in the presence of other normal values can indicate early obstructive disease). This pattern becomes more exaggerated with increasing severity of COPD. Figure 8. Flow Volume Loop COPD. The PEF is reduced, the curve has a concave shape and the expiration time is prolonged (Gross 2005). 18
19 The raw data are expressed as a percent of predicted values for patients of similar physical characteristics (e.g. height, weight, age, sex and race) (Figure 9). Figure 9. Spirometry data of a healthy individual. Generally speaking, results nearest to 100% predicted are the most normal, and generally results over 80% are often considered normal. The results of the test (appendix 3) will only be accurate if the test is performed correctly. The patient must exhale until RV. This must last for at least 6 seconds. Therefore the patient must be able to co operate with the technician. FVC and FEV1 should be the greatest values taken from a selection of 3 technically correct graphs and the FVC and FEV1 values in these three curves should vary by no more than 5% or 100 ml, whichever is greater. The FEV1/FVC is calculated using the maximum FEV1 and FVC from technically acceptable curves. The data can be taken from different curves so the best reading should be used. Those with chest pain or frequent cough may be unable to perform a satisfactory test and this should be noted. There is a normal age-related decline in the FEV1/FVC ratio, so normal elderly patients without airway obstruction will have a ratio below 70-80% (Dykstra et al 1999, pp. 69). The mid-range flows (FEF25-75) are always reduced in obstructive airways disease. However, some patients have normal spirometry with the exception of a reduced FEF It is then important to look at the predicted value and the level that the patient reached. A mid-range flow less than 50% is likely to be abnormal and is suggestive of possible small airways dysfunction and potentially early obstruction, but it should not be interpreted as meeting obstructive criteria. In this case the patient may need further investigation to exclude asthma or the results may be interpreted (with history and symptoms) as a possible early indicator of smoking related lung disease. 19

20 Plethysmography Although spirometry is the standard method of measuring lung volumes, it is not possible to measure absolute lung volumes through this means. Therefore an alternate method has to be used. There are two commonly used methods used to measure absolute lung volumes. These are gas dilution tests and body plethysmography. Gas dilution tests involve inhaling a preset amount of helium. The patient is requested to breathe the helium diluted air several times until the helium gas has equilibrated between the bag and the patient's lungs. The new mixed concentration of helium is then recorded. This method is only used at St Lucas Andreas hospital when the patient is unable to tolerate plethysmography. This method is unable to detect air pockets in the lungs of an emphysema patient so is therefore not as accurate as body plethysmography and also takes longer. Body plethysmography provides a means to measure thoracic gas volume (VTG). Thoracic gas volumes can be used to determine static lung volumes including the total lung capacity (TLC), the residual volume (RV), and the functional residual capacity (FRC). Measurement of lung volumes and capacities (a lung capacity is a combination of 2 or more standard lung volumes) is the second most common pulmonary function test performed. (Other tests that can be administered in the body plethysmograph include airways resistance (Raw), Spirometry, bronchial challenge, diffusing capacity (D LCO ), single-breath nitrogen (N 2 ), multiple-breath N 2 washout, pulmonary compliance, and occlusion pressure. (These will not be discussed as part of this project). A pressure plethysmograph is usually measured at the end-expiratory level in order to measure the amount of air remaining in the lungs after a maximal expiration. (RV) (Figure 10). The mouth pressure and box pressure changes that are measured during tidal breathing and panting maneuvers which are performed during the test by the patient at the end of expiration are sent to a microprocessor unit that calculates thoracic gas volume. Airway resistance (Raw) can also be measured using this method. According to Allen (1997, pp. 70) this measurement may be useful in detecting asthma which is associated with increased airway tone and although this measurement may have some advantages over FEV1 the clinical indications for measuring airway resistance remains uncertain. Figure 10. Measurement of lung volumes (Wales 2003). 20

21 Measurements of lung volumes and TLC is more useful for diagnosing restrictive lung disease rather than obstructive. The measurement is expressed as a percentage of a predicted norm and the lower the ratio of TLC to the predicted norm, the greater the restriction. Measurement of lung volumes can however indicate some obstructive factors e.g. a greater than predicted RV suggests air trapping suggesting obstructive disease and an increase in FRC suggests hyperinflation which is a recognized clinical feature of COPD. Lesser degrees of hyperinflation exist in the progression of COPD due to changes in the elastic and recoil properties of the lungs. This can be determined on the plethysmograph by the ratio of residual volume (RV) to total lung capacity (TLC). Dykstra et al (1999) reported measurements of lung volumes in 4774 patients with airflow obstruction (FEV 1 : FVC < 70%) and noted that hyperinflation, as determined by the ratio of residual volume (RV) to TLC was strongly correlated with the degree of airflow obstruction. Figure 11. Plethysmograph showing increased RV and TLC (Gross 2005). Test results should be obtained from a minimum of 3 to 5 separate clinically acceptable panting maneuvers (appendix 3). The results should indicate whether the volume was measured at FRC or RV. If gas dilution tests are performed, results should be compared. The plethysmograph involves spending a short period of time in an enclosed box. This can cause feelings of claustrophobia in some patients and is therefore unsuitable. Prolonged confinement in the plethysmograph chamber could result in hypercapnia or hypoxia; however, because of the limited length of the test, this is an uncommon occurrence. Transmission of infection is possible via improperly cleaned equipment (i.e. mouthpieces) or as a consequence of the inadvertent spread of droplet nuclei or body fluids. Diffusing Capacity (Pulmonary gas transfer index) Pulmonary gas transfer index is a measure of the rate of uptake of a particular gas across the alveolar-capillary bed for a specified driving pressure for that gas. (Wasserman et al. 1999, pp. 526). 21
22 Diffusing capacity provides an estimate of how well a gas is able to move from the alveoli into the blood. The test is used to estimate the gas exchanging capability of the lungs so provides an estimate of the transfer of oxygen from alveoli to capillary and the transfer of carbon dioxide from capillary to alveoli. The total process is a measure of the interaction of Alveolar surface area Alveolar capillary perfusion The physical properties of the alveolar capillary interface Capillary volume Haemoglobin concentration The reaction rate of CO and haemoglobin The measurement is obtained by measuring the diffusion of a preset amount of Carbon Monoxide from the alveoli to the pulmonary capillary. Generally, the difference between the concentrations present before the breathhold and after the breathhold indicates the amount of gas that diffuses through the lungs and into the bloodstream. Carbon monoxide is most commonly used in this test as the tracer gas for measurement because of its high affinity for binding to the haemoglobin molecule. This property allows a better measurement of pure diffusion, because the movement of the CO is mainly dependent on the properties of the diffusion barrier and the amount of haemoglobin. CO transfer is not affected by perfusion rate. The transfer of CO into the capillary is diffusion limited as opposed to perfusion limited. This test is usually performed during pulmonary function testing when the patient is having plethysmography and Spirometry. Diffusion capacity is affected by surface area, partial pressure difference, gas solubility and the thickness of the tissue of the alveolar- capillary barrier. The test is pertinent for patients with COPD because in patients with emphysema, the surface area of the lung is usually reduced due to destruction of alveolar tissue leading to loss of functioning alveolar-capillary bed. The diffusion capacity in COPD patients can also be reduced because of failure of inspired air to reach the alveoli during exacerbations of the condition or due to poor ventilation-perfusion ratio. It is also useful for differentiating among chronic bronchitis, emphysema, and asthma in patients with obstructive patterns and it is useful to predict arterial desaturation during exercise in these patients. The patients HB level will also affect the result so all data is adjusted according to the individuals HB during the test. (American Association of Respiratory Care, 2001) Interpretation should not be done in isolation but in conjunction with spirometric and lung volume assessment. The results are based on a ratio between the uptake of CO in ml per minute divided by the average alveolar pressure of CO. Overall TLCO is expressed as the uptake of CO in mmol of gas per minute and per kpa driving pressure of CO - mmol/min/kpa and is expressed as a percentage of a predicted normal value. 22
23 Results of the following parameters are expressed on the data (see also appendix 3) VIN TLC He RV He RV%TLC-He VA TLCO SB TLCO/VA HB TLCOc SB TLCOc/VA Inspiratory volume Total lung capacity Residual Volume RV expressed as a % of the TLC Alveolar Volume Transfer factor of CO for a single breath Transfer factor of CO as a % of Alveolar volume Haemoglobin LCO SB adjusted as per patients HB TLCO as % VA adjusted as per patients HB The most important result for the therapist is the HB adjusted transfer factor of CO expressed as a % of VA. This figure can be used to estimate the degree of severity of diffusion limitations and can be interpreted as follows: Degree of severity of decrease in diffusing capacity for carbon monoxide Mild >60% and <LLN Moderate 40-60% Severe <40% The TLco results will be abnormal in patients with lung disease due to effects on the distribution of diffusion properties and alterations in alveolar volume and capillary blood flow. Reduced diffusion capacity will be found in patients with decreased alveolar surface area and diminished capillary bed/blood volume. This is typical of emphysema patients. In emphysema, where there is hyperinflation and destruction of the alveolar architecture, the lung volumes are increased and DL- CO/VA is decreased. Poor diffusion would be expected in patients with decreased pulmonary tissue, increased diffusion distance, or those with anaemia. The patients with simple chronic bronchitis do not usually have hyperinflation; therefore, their lung volumes are normal. Because their lung architecture is normal, the diffusion capacity is not affected. Although gas dilution techniques are based on a simple principle, are widely used, and provide a good measurement of all air in the lungs that communicates with the airways, a limitation of this technique is that it does not measure air in noncommunicating bullae and, therefore, may underestimate TLC, especially in patients with severe emphysema. The patient is required to be able to co operate with the technician performing the test and be able to follow instructions. Patients should be alert, oriented, able 23
24 to exhale completely and inhale to total lung capacity, able to maintain an airtight seal on a mouthpiece, and able to hold a large breath for 10 seconds. The patient should refrain from smoking for several hours before the test and also to refrain from alcohol for the previous 8 hours as alcohol vapours can affect the accuracy of CO analyzers. Maximal Inspiratory Pressure and Maximal Expiratory Pressure As mentioned earlier the maximal inspiratory pressure (MIP or PImax) and the maximal expiratory pressure (MEP or PEmax) are used to assess the respiratory muscle strength. However it should be noted that this is only estimation due to the fact that respiratory muscle force is indirectly measured through the pressure generated during inspiration or expiration. The pressures which are used to estimate the muscle strength reflect pressure changes against atmospheric pressure. Therefore it is not possible to assess strength of an individual muscle involved in respiration, the strength of all the muscles involved in inspiration or expiration is measured together. Furthermore the pressure measured during maximal inspiration or expiration is influenced by the elastic recoil of the lungs and chest wall. Because maximal expiratory pressure is measured at the TLC, the recorded pressures are the combination of the effort of the expiratory muscles and the elastic lung recoil at TLC. The maximal inspiratory pressure is measured at RV and is therefore a combination of the action of the inspiratory muscles, and the pressure generated by the tendency of the chest wall to expand at RV. To avoid these two aspects it would be necessary to measure the maximal pressures at the functional residual volume because the elastic recoil of the lungs and the chest wall generate equal pressures. Therefore any additional pressure measured during inspiration or expiration is exclusively caused by the strength of respiratory muscles at this particular lung volume. However, it is easier for the patient to perform the test at the RV or TLC instead of the functional residual volume and therefore these to lung volumes are used as a starting position of the tests. There are some contraindications for these tests, which are pathological conditions where relatively large pressure changes in the thorax or abdomen should be avoided (e.g. aneurism, uncontrolled hypertension, and urinary incontinence). During the test the peak pressure should be reached directly at the beginning of the maneuver. The pressure which is maintained for at least 1 s is generally called the MIP or MEP (plateau pressure). This can be also found in the obtained graphs (figure 13). Healthy subjects can reach pressures bigger than 30 kpa during the tests (Troosters et al. 2005, pp.60). Normally the absolute number of MEP is approximately twice the absolute number of MIP (Troosters et al 2005, pp.62). In some diseases (e.g. spinal cord injury, below C3-5, multiple sclerosis) the reduction of MEP is higher than the reduction of MIP. 24
 (see figure 12). However, it has to be noted that these tests do not state anything about the endurance of the respiratory muscles.")
25 If the values for MIP are 70 % or less of the predicted values it indicates that the respiratory muscles are weak and respiratory muscle strength training should be applied (KNGF 2003, pp.34-35) (see figure 12). However, it has to be noted that these tests do not state anything about the endurance of the respiratory muscles. Greatly reduced expiratory muscle strength can cause problems with expectoration. However, this is normally not problem of COPD patients which are participating in out-patients rehabilitation programs. Maximal inspiratory pressure (MIP/PImax) 70% of predicted value 70% of predicted value No indication for respiratory muscle strength training Figure 12. Flowchart for interpreting the MIP test values. Respiratory muscle strength training should be applied Figure 13. The obtained data from MEP and MIP test in the St Lucas Andreas Hospital. 25
26 Maximal Bike Test (Cardiopulmonary Exercise Test) The cardiopulmonary test is an important assessment tool to analyse the exercise limitation in a patient. By knowing the exercise limitation it is already possible to make a prognosis for the degree of benefit of a pulmonary rehabilitation program. For example according to Plankee et al (2005, pp ) patients with cardiopulmonary limitation have a better prognosis to show an improvement in their V O2 peak then patients with a ventilatory limitation. Furthermore the cardiopulmonary test is especially useful to determine deficits in the function of the cardiovascular and ventilatory systems, because the defects are amplified during exercise. It is important to know that in Cardiopulmonary testing there are certain criteria which lead to an immediate stop of the exercise test. The symptoms and/or finding are according to ATS/ACCP (2001, pp. 227) are the following one: Chest pain suggestive of ischemia Ischemic ECG changes Complex ectopy Second or third degree heart block Fall in systolic pressure > 20 mm Hg from the highest value during the test Hypertension (> 250 mm Hg systolic; >120 mm Hg diastolic) Severe desaturation: SaO2 80% when accompanied by symptoms and signs of severe hypoxemia Sudden pallor Loss of coordination Mental confusion Dizziness or faintness Signs of respiratory failure In the case of a completed maximal bike test the test is stopped because the subject s RER > 1,2, which is an indication that the subject has reached his/her anaerobic threshold. However, in the case of COPD patients it is not uncommon that the cardiopulmonary test is stopped before the patient reaches his/her anaerobic threshold due to dyspnea, muscle pain/fatigue or other symptoms. By interpreting the maximal bike test you can identify 4 different limitations and get links to 2 others. The four limitations are ventilatory, cardiovascular, peripheral muscle and psychological. Furthermore the bike test can be an indication for diffusion problems and abnormal O2 content. In this section we will concentrate on the 4 limitation which were just mentioned. A flowchart for identifying these limitations can be found in appendix 1. The following points can indicate a ventilatory limitation. Ventilatory limitation: Max. V E during exercise exceeds the value of 70% of MVV this means that a ventilation limitation can be suspected (Cesar et al 2003, pp.527). This particular value is not calculated or measured during the maximal 26
27 bike test at the St Lucas Andreas Hospital. However this value equals a breathing reserve (BR %) of 30% (BR=1-(V E max/mvv) (Wasserman et al 1999, pp.535)), which is mentioned in the obtained data. The Breathing reserve (BR) is low at the point when the exercise test is stopped (ATS/ACCP 2001 pp.248,252), this indicates a ventilation limitation because the breathing reserve reflects the relationship of ventilatory demand to ventilatory capacity. The absence of an anaerobic threshold during exercise (Babb 1991 pp.18). This can be found if the exercise test was stopped before the subject reached his/her anaerobic threshold for example due to dyspnea. Max V O2 and anaerobic threshold are not reached (Weber et al 1988 pp.845). An individual is considered to reach V O2max when, during maximal exercise, the progressive increase in the loads does not increase V O2 by more than 150 ml/min, and a plateau is graphically obtained (Taylor et al 1995 pp.877). When this plateau is not reached, the highest V O2 is called peak oxygen consumption (V O2 peak) (Wasserman et al 1999 pp.528). An increased for the ratio of V E/V CO2 and an abnormal VD/VT response (ATS/ACCP 2001 pp. 248) Determination of the flow-volume loop during exercise as compared with the flow-volume loop at rest may indicate a limitation in the expiratory flow. In this paragraph the abnormalities of values which could indicate a cardiovascular limitation are outlined. Cardiovascular limitation: Reduction of age related maximum heart rate (HR) (KNGF 2003, pp.16) The Test was stopped at a V O2 peak < V O2 max but normal predicted HR. In this case there are different possibilities. Initially, exercise could be limited by cardiovascular function and/or it could be limited by O2 content factor and/or limited by skeletal muscle dysfunction (ATS/ACCP 2001 pp.252). The case of an O2 content factor limitation is discussed in more details under blood gasses. The case of a skeletal muscle dysfunction is not in detail discussed in this information pack because it a huge subject on his own. Abnormal value for the ratio of V E/V CO2 and VD/VT responses without O2 desaturation.this indicates a moderate to severe heart failure (ATS/ACCP 2001 pp.252). Max. V E during exercise does not exceed the value of 50% of MVV (Cesar et al 2003, pp.527). As already mentioned earlier this particular value is not calculated or measured during the maximal bike test at the St Lucas Andreas Hospital. However, these value equals a breathing reserve (BR%) of 50% (BR=1-(V E max/mvv) (Wasserman et al 1999 pp.535)), which is mentioned in the obtained data. If the breathing reserve (BR) is high when the exercise test is stopped it is more likely to be a cardiovascular limited test. (ATS/ACCP 2001 pp.248, 252). 27
28 If the heart rate reserve (HRR) is low when the exercise test is stopped it is more likely to be a cardiovascular limited test (ATS/ACCP 2001 pp. 252) No increase of blood pressure during exercise testing could indicate cardiac limitations or abnormality of sympathetic control of blood pressure can be strongly suggested (ATS/ACCP 2001 pp.233). Peripheral muscle limitation: The cardiopulmonary exercise test can also be limited by peripheral muscle dysfunction. This limitation can be indicated by a max test which is stopped due to muscle fatigue or pain. In this case it is also important to take the Borg scale into account; a high number for muscle fatigue on the Borg scale supports the possibility of a muscle limitation (KNGF 2003, pp.17). As mentioned earlier the skeletal muscle dysfunction is not discussed in more detail in this information pack due to the fact that it is quite a big subject on its own. Psychosocial limitation or poor effort: In patients it is relatively common that a cardiopulmonary exercise test is stopped before it is actually completed due to symptoms but there is also a chance that it is limited due to psychological reasons. A psychological limitation or a poor effort can be suspected in the case of a decreased V O2 peak, a high Breathing Reserve (BR) as well as a high Heart Rate Reserve (HRR) and a low RER without apparent peripheral problems (e.g. lung transplantation) (ATS/ACCP 2001 pp.253). Finally it should be noted that in most of the COPD patients it is not possible to identify only one limitation due to the fact that in most cases there is a combination of limitations present. Arterial Blood Gases (ABG) Arterial blood ph and arterial partial pressure of oxygen have to be maintained within a narrow range for the various systems in the body to function optimally. Arterial blood gas samples provide information about these factors and can also provide essential information on cardio respiratory conditions. The blood is taken from the radial, brachial or femoral artery. ABG analysis shows oxygenation and carbon dioxide levels within the body and also provides information about acid-base disturbances. It provides information on ventilation by measuring ph and the partial pressure of oxygen (PaO2) and carbon dioxide (PaCO2) indicating the amount of oxygen delivered to the blood from the lungs and the lungs capacity to eliminate CO2. ABG analysis is used in acute cardio respiratory conditions such as exacerbation of COPD and severe asthma but is also used to assess and monitor the patient s response to exercise during cardiopulmonary exercise testing. Assessment of PaO2 will inform the tester about the levels of blood oxygenation. This is particularly relevant during CPET in order to detect O2 transport limitations. There is a chemical relationship between arterial blood ph, HCO3-28
29 and PaCO2. If one of these parameters changes, the others will also have to undergo change. Therefore an increase in PCO2 will have the effect altering blood ph and the base excess HCO3- levels will also alter as the body compensates in order to maintain ph within the optimal range. Normal values Normal Values Range Mean PH 7.36 to PaCO2 35 to mmhg HCO3 23 to meq/l PaO2 80 to 100 mmhg Lower when older Base Excess -4 to +4 0 Reid & Chung (2004) When examining ABG results it is essential to note that older adults have progressively lower PaO2 (Lundbäck et al 2003, pp. 7). A healthy young adult has a PaO2 of 100mmHg whereas a health 70 to 80 year old has a PaO2 of approximately 75 to 80 mmhg) 29
30 Conclusion According to the KNGF guidelines, it is recommended for physiotherapists to have knowledge of and to be educated about COPD, out-patients rehabilitation programs and to be able to use the provided data to identify possible exercise limitations in COPD patients. This knowledge and education is essential for the physiotherapist caring for CODP outpatients in order to provide individual care and therapy. It is also helpful if the therapist is knowledgeable about the actual pulmonary function testing as it can provide information about the patients exercise capabilities and also about the limitations that can occur during the actual testing. It is very important for Physiotherapists to be able to interpret the data which is obtained by pulmonary function tests. The interpretation of the pulmonary function test data is an essential part of planning a patient s rehabilitation program. Depending on the exercise limitation the rehabilitation program has to be adjusted and has to focus on different aspects. Cardiovascular limited patients should perform an endurance training to improve their exercise capacity (KNGF 2003, pp. 16). While a rehabilitation program for ventilatory limited patients should focus more on respiratory muscle training to improve their strength and endurance and consequently improve their ventilatory capacity (KNGF 2003, pp. 17). In the case of an oxygen transport limitation it is essential that patients learn to use their bodies more efficiently (KNGF 2003, pp.17). Also the training of specific breathing exercise can help to reduce the dead space. However, supplementary oxygen might be necessary (KNGF 2003, pp.17). In patients with psychosocial limitation physical exercise is a useful tool to reduce exercise limiting factors (KNGF 2003, pp.17). For patients with a peripheral muscle limitation the physiotherapist should consider peripheral muscle strength training as an important part of patient s specific rehabilitation program. The content of this information package is aimed at junior physiotherapists and senior student. Although respiratory physiotherapy is covered in the Dutch education system, it is not covered in a separate respiratory module. This area is an area of growing demand because of the increasing incidence of the condition. However, it is important to notice that the interpretation of pulmonary function test is a huge and complicated subject and therefore it is not possible to discuss all aspects of the subject in detail in the professional assignment project. This professional assignment is supposed to give the physiotherapist a short explanation of topics such as COPD, out-patients rehabilitation program and possible exercise limitations. It also provides the reader with an explanation of the different pulmonary function tests and the interpretation of the obtained data. Although the data provided by pulmonary function testing is a valuable diagnostic tool, it is not supposed to give a total and detailed interpretation of the patient s condition. That can only be achieved when the patients is assessed in a holistic manner and his diagnosis is made from a combination of information obtained from patient history, symptoms and the results of the investigtigations. 30
31 References: ALLEN, J James Allen, M.D. Home Page {online}. Available: [Accessed 8 February 2006] AMERICAN ASSOCIATION FOR RESPIRATORY CARE Body Plethysmography: 2001 revision and update. Respir Care 46(5): AMERICAN THORACIC SOCIETY Pulmonary Rehabilitation Am. J. Respir. Crit. Care Med 159 (5): AMERICAN THORACIC SOCIETY & EUROPEAN RESPIRATORY SOCIETY TASK FORCE Standards for the Diagnosis and Management of Patients with COPD [Internet] Version 1.2. New York: American Thoracic Society; 2004 Available: AMERICAN THORACIC SOCIETY (ATS) and AMERICAN COLLEGE OF CHEST PHYSICIANS (ACCP) ATS/ACCP Statement on Cardiopulmonary Exercise Testing. Am J Respir Crit Care Med, 167, THE AUSTRALIAN LUNG FOUNDATION, The COPDX Plan: Australian and New Zealand Guidelines for the management of Chronic Obstructive Pulmonary Disease. The Medical Journal of Australia, 178(6): S1-S4. BABB, T.G Mechanical ventilatory constraints in aging, lung disease, and obesity: perspectives and brief review. Med. Sci. Sports Exerc, Suppl: BANEZ GALLARDO, J., Pulmonary Mechanics [online]. Available: IP)%20and%20Maximal%20Expiratory%20Pressure%20(MEP) [Accessed 2 February 2006] CARTER, R., NICOLTA, B., BLEVINS, W. & HOLIDAY, D Altered exercise gas exchange and cardiac function in patients with mild chronic obstructive pulmonary disease. Chest, 103: CESAR CASTRO DE M., CAMELIER, A., JARDIM, J.R., MONTESANO, F.T., TEBEXRENI, A.S. & BARROS T.L Functional Cardiorespiratory Limitation in Patients with Chronic Obstructive Pulmonary Disease and Congestive Heart Failure. Arq Bras Cardiol, 80: COOPER, C.B Assessment of Pulmonary Function in COPD. Semin Respir Crit Care Med. 26(2): DILLARD, T.A., PIANTADOSI, S., RAJAGOPAL, K.R Prediction of ventilation at maximal exercise in chronic air-flow obstruction. Am Rev Respir Dis, 132:
32 DYKSTRA, B.J., SCANLON, P.D., KESTER, M.M., BECK, K.C. & ENRIGHT, P.L Lung Volumes in 4,774 Patients with Obstructive Lung Disease. CHEST, 115(1): ENGSTRÖM, C.P., PERSSON, L.O., LARSON, S. & Sullivan, M Healthrelated quality of life in COPD: Why both disease-specific and generic measures should be used. Eur Respir J, 18: FINNERTY, J.P., KEEPING, I., BULLOUGH, I. & JONES, J., The Effectiveness of Outpatient Pulmonary Rehabilitation in Chronic Lung Disease: A Randomized Controlled Trial. Chest, 119: GROSS, T Virtual Hospital Interpretation of Pulmonary Function Tests: Spirometry: Interpreting Spirometry {online}. Available: [Accessed 22 December 2005] HANSEN, J.E., SUE, D.Y. & WASSERMAN, K Predicted values for clinical exercise testing. Am Rev Respir Dis, 129: KNGF, Clinical practice guidelines for physical therapy in patients with chronic obstructive pulmonary disease. The Netherlands. V-03/2003/US LAPPERRE, T.S., SNOECL-STROBAND, J.B., GOSMAN, M.M.E., STOLK,J., SONT, J.K., JANSEN, D.F., KERSTJENS, H.A.M., POSTMA, D.S. & STERK,P.J Dissociation of Lung Function and Airway Inflammation in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med {online}. 170: Available: LUNDBÄCK, B., GULSVIK, A., ALBERS, M., BAKKE, P., RÖNMARK, E., VAN DEN BOOM, G., BRÖGGER, J., LARSSON, L.G., WELLE, I., VAN WEEL,C. & OMENAAS, E Epidemiological aspects and early detection of chronic obstructive airway diseases in the elderly. Eur Respir J, 21: 3-9. MANNINO, D.M COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest, 121: supp. 5, 121S 126S. MORGAN, M.D.L., CALVERLEY, P.M.A., CALRK, C.J., DAVIDSON, A.C., GARROD, R., GOLDMAN, J.M., GRIFFTHS, T.L., ROBERTS, E., SAWICKA, E., SINGH, S.J., WALLACE, L. & WHITE, R Standards of Care Subcommittee on Pulmonary Rehabilitation. Pulmonary rehabilitation. Thorax, 56: NATIONAL HEART, LUNG AND BLOOD INSTITUTE Morbidity and mortality: chartbook on cardiovascular, lung and blood diseases. Bethesda, MD: US Department of Health and Human Services. OLDENBURG, F.A., DOLOVICH, M.B., MONTGOMERY, J.M. & NEWHOUSE, M.T Effects of postural drainage, exercise and cough on mucus clearance in chronic bronchitis. Am Rev Respir Dis, 120:
33 O REILLY, J., WILLIAMS, A.E., LEDGER, G. & RICE, L Health utility burden for exacerbation of COPD requiring admission into hospital as measured by the EQ-5D. Blackpool Victoria Hospital NHS Trust, Blackpool, UK PETTY, T.L Pulmonary rehabilitation of early COPD: COPD as a systemic disease - chronic obstructive pulmonary disease. Chest, 105: PIES, A.L., KAPLAN, R.M., LIMBERG, T.M. & PREWITT, L.M Effects of pulmonary rehabilitation on physiological and psychosocial outcomes in patient with chronic obstructive pulmonary disease. Ann Intern Med, PLANKEEL, J. F., MCMULLEN, B. & MACINTYRE, N. R Exercise Outcomes After Pulmonary Rehabilitation Depend on the Initial Mechanism of Exercise Limitation Among Non-Oxygen-Dependent COPD Patients. Chest, 127: REID, W.D. & CHUNG, F Clinical Management Notes and Cases Histories in Cardiopulmonary Physical Therapy. New York: SLACK Incorporated. SALMAN, G.F., MOSIER, M.C., BEASLEY, B.W. & CALKINS, DR Rehabilitation for Patients With Chronic Obstructive Pulmonary Disease: Metaanalysis of Randomized Controlled Trails: JGIM, 18: SIAFAKAS, N.M., VERMEIRE, P., PRIDE, N.B ERS-Consensus statement. Optimal assessment and management of chronic obstructive pulmonary disease. Eur Respir Rev, 8: SNIDER, G.L., KLEINERMAN, J., THURLBECK, W.M. & BENGALI, Z.K The definition of emphysema: report of a National Heart, Lung and Blood Institute, Division of Lung Diseases, Workshop. Am Rev Respir Dis. {online}, 132: STOCKS, J. & QUANJER, P.H Reference values for residual volume, functional capacity and total lung capacity. Eur Respir J, 8: TAYLOR, H.l., BUSKIRK, E. & HENSCHEL, A Maximal oxygen intake as an objective measure of cardiorespiratory performance. J Appl Physiol, 8: TROOSTERS, T., GOSSELINK, R. & DECRAMER, M Respiratory muscle assessment. Eur Respir Mon, 31: VERMEIRE, P The burden of chronic obstructive pulmonary disease. Respiratory Mediicine, 96: Suppl C. S3-S10 WALES, J Spirometry. {Online} Available: [Accessed 23 January 2006] WASSERMAN, K., HANSEN, J.E., SUE, D.Y., CASABURI, R. & WHIPP, B.J Principles of exercise testing and interpretation. Baltimore: Lippincott Williams & Wilkins. 33
34 WEBER, K.T., JANICKI, J.S., MCELROY, P.A. & REDDY, H.K Concepts and applications of cardiopulmonary exercise testing. Chest, 93: WIDMAIER, E.P., RAFF, H. & STRANG, K.T., Vander, Sherman, Luciano s Human Physiology: The Mechanisms of body function. 9 th ed. New York: McGRAW-HILL. WORLD HEALTH ORGANISATION, Life in the 21st Century: A vision for all. Geneva WOUTERS, E.F.M The societal impact of COPD in North America and Europe: an economic analysis of the Confronting COPD survey. Respir Med 97: Suppl C S3-S14. Further readings: FOSS, M. L. & KETEYIAN, S.J Fox s Physiological Basis for Exercises and Sport. 6 th ed. Singapore: Mc Graw Hill. GREEN, J.H An Introduction to Human Physiology. 4 th ed. Oxford: Oxford Medical Publications. GOULD, B.E Pathophysiology for Health Professions. 2 nd ed. Philadelphia: W.B. Saunders Company. WEST J.B Respiratory Physiology-the essentials. 3 rd Williams & Wilkins. ed. Baltimore: Appendix 1 (Cardiopulmonary exercise test flowchart) 34
35 In this appendix you can find a flowchart (next page) which can help you to identify the patient s exercise limitation. This flowchart should be used as a tool for interpretation of exercise limitations in conjunction with the obtained CPET data. The flow chart is used by initially identifying the reason the patient stopped the test (the first row of the chart) and by systematically following the relevant branch the following limitations can be identified. Cardiovascular limitations Diffusion limitations Skeletal muscle limitations Psychosocial limitations Ventilatory limitations Gas transfer limitations 35
36 36
37 Appendix 2 (Glossary) (Wasserman et al 1999, ATS/ACCP et al 2001) AT (anaerobic threshold): Exercise O 2 that marks the transition between no change or little change in arterial lactate concentration and the sustained increase in concentration of lactate (also known as the lactate threshold). Postulated by some authors to be the O 2 above which anaerobic energy production substantially supplements aerobic energy production. FEV1 (forced expiratory volume in 1 second): Volume of exhaled from the lungs during the first second of a forced expiratory manoeuvre (FVC), expressed in litres (btps). HR (heart rate): Number of heart beats per. HRR (heart rate reserve): Difference between the highest heart rate attained during a maximal exercise test and the maximal value predicted for that subject. Expressed in units of beats per minute. MVV (maximal voluntary ventilation): Maximal volume of air that can be breathed per minute by a subject. This is conventionally measured from a maximal volitional breathing effort for a short period of time (e.g., 12 seconds) over which the exhaled volume is summed and expressed in units of liters per minute (BTPS). In case that MVV was not measured it can be calculated MVV=FEV1*35-40 (ATS/ACCP 2001), MVVs estimated by this method were not discernibly different from MVVs directly measured in COPD patients (Dillard et al 1885, Hansen et al 1984). O 2 pulse (oxygen pulse): The oxygen uptake (V O2) divided by the heart rate (HR). Hence, it represents the amount of oxygen extracted by the tissues of the body from he O2 carried in each stroke volume. RER or R (respiratory exchange ratio): Ratio of CO 2 output to O 2 uptake per unit of time (measured at the mouth). This ratio reflects not only tissue metabolic exchange of the gases, but also that resulting from transient changes in the body's gas stores. For example, the gas exchange ratio exceeds the respiratory quotient as additional CO 2 is evolved from the body stores during hyperventilation; similarly, the gas exchange ratio is less than the respiratory quotient when CO 2 is being retained during hypoventilation Sa O2 (arterial oxygen saturation): Actual amount of O 2 bound to hemoglobin in a given volume of arterial blood and expressed as a percentage of the total capacity for O 2 binding of the hemoglobin in that blood volume. VD (physiologic dead space): Notional volume of inspired gas that does not reach a gas-exchanging unit. The physiologic dead space is therefore the sum of the anatomic dead space (see below) and the alveolar dead space (the volume of alveoli that are ventilated but unperfused and a component of those that are underperfused). It is expressed in units of millilitres or litres (BTPS) 37
38 VD/VT (ratio of physiologic dead space to tidal volume): Proportion of tidal volume that is made up of the physiologic dead space. It is a dimensionless quantity, conventionally expressed as a fraction. Used as an index of ventilation perfusion mismatching. E (minute ventilation): Volume of expired air exhaled from the lungs in 1 minute. This is conventionally expressed in units of litres per minute (BTPS) Emax (maximal exercise ventilation): Highest minute ventilation achieved during a maximal exercise test. This is usually determined by tests that tax large muscle masses, such as cycle ergometry or treadmill. It is conventionally expressed in litres per minute (BTPS) E/MVV = BR (Breathing reserve): Expresses the relationship of ventilatory demand as reflected by peak E to ventilatory capacity. MVV is conventionally used as an index of ventilatory capacity. This ratio is expressed as ( Emax/MVV) x 100. The term is synonymous with ventilatory reserve. E/ CO 2 (ventilatory equivalent for carbon dioxide): Ratio of the subject's minute ventilation (BTPS) to CO 2 output (STPD). It is a dimensionless quantity. This ratio indicates how many litres of air are being breathed to eliminate 1 litre of CO 2. It is used as a noninvasive estimator of appropriateness of ventilation E/ O 2 (ventilatory equivalent for oxygen): Ratio of the subject's minute ventilation (BTPS) to O 2 uptake (STPD). It is a dimensionless quantity. This ratio indicates how many litres of air are being breathed for each litre of O 2 uptake O 2 (oxygen uptake): Volume of O 2 extracted from inspired air in a given period of time, expressed in millilitres per minute or litres per minute (STPD). This can differ from O 2 consumption under conditions in which O 2 is flowing into or being utilized from the body's stores. O 2 consumption is the amount of O 2 utilized by the body's metabolic processes in a given time, expressed in units of litres per minute (STPD). In the steady state, O 2 uptake equals O 2 consumption O 2 max (maximal oxygen uptake): Traditionally the highest attainable O 2 uptake for a given subject. It is determined during dynamic exercise from a "plateauing" of O 2 despite work rate continuing to increase. In the absence of a discernible plateau, the highest O 2 actually attained on the test is more properly termed V O2 peak. Both O 2 max and O 2 peak are conventionally expressed in units of millilitres per minute or litres per minute (STPD) or, corrected for body weight, as millilitres per minute per kilogram O 2 peak (oxygen uptake at peak exercise): Highest O 2 achieved on a test performed to the limit of tolerance. No additional criteria are needed for its determination, such as evidence of plateauing, to justify a O 2 max. It is conventionally expressed in units of litres per minute or millilitres per minute (STPD) 38
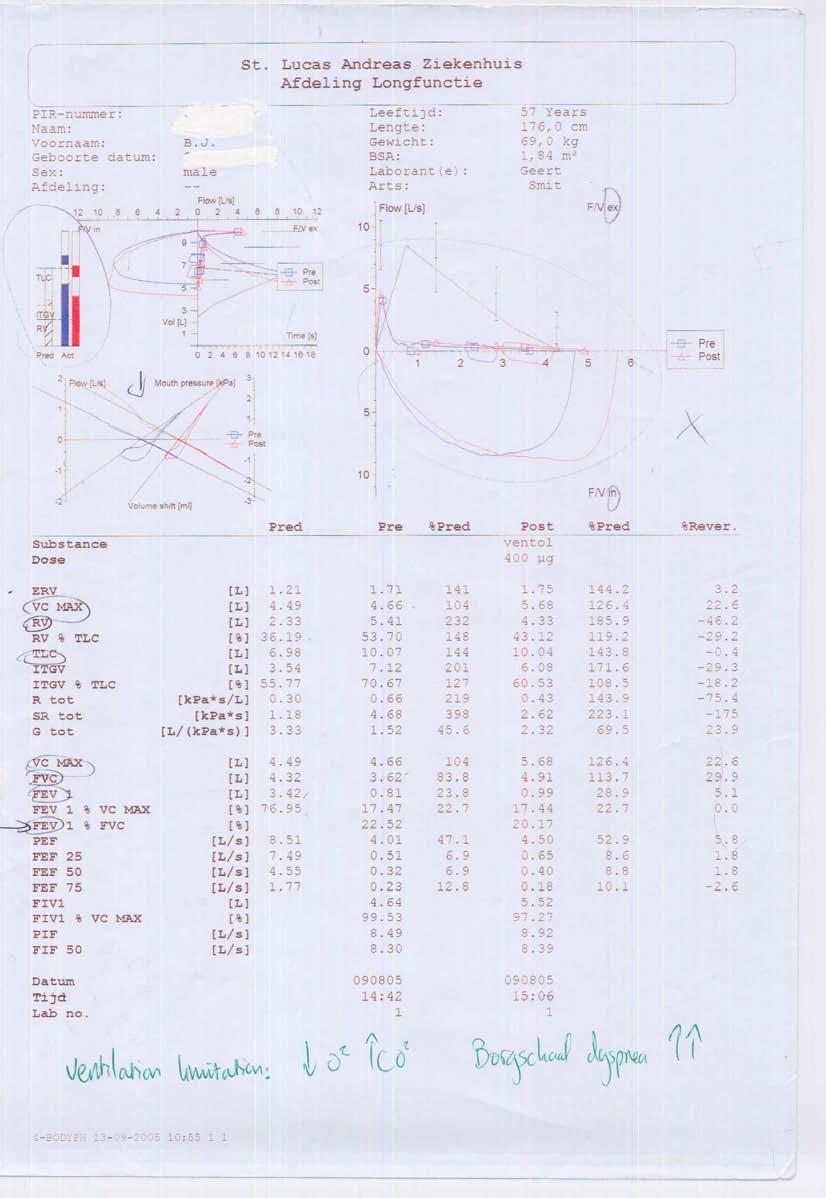
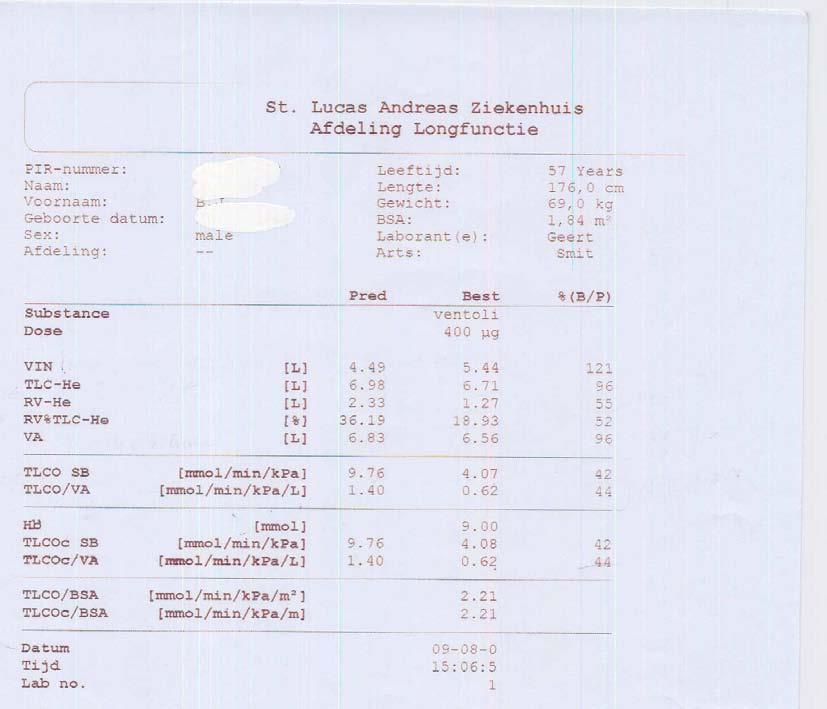
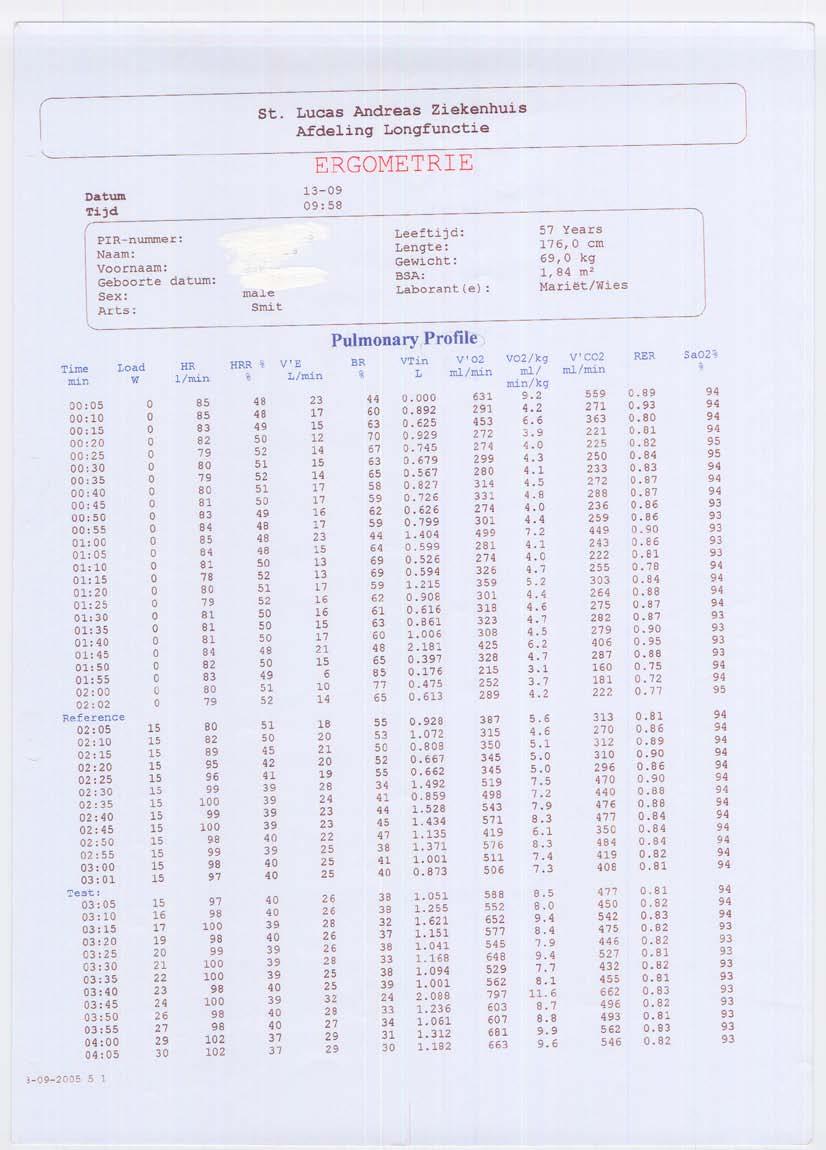
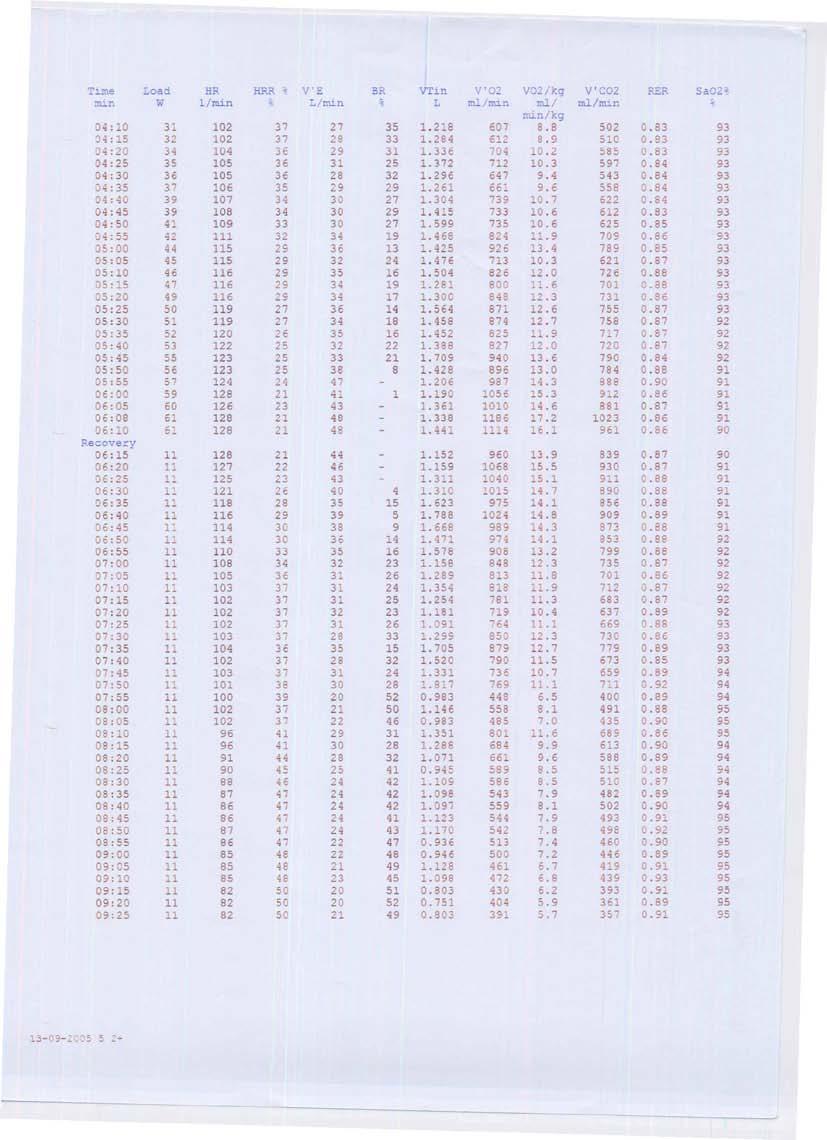
39 O 2 / WR: Increase in O 2 uptake in response to a simultaneous increase in work rate (see below). Under appropriate conditions, this may be used to estimate the efficiency of muscular work. It is usually expressed in units of millilitres of O 2 per minute (STPD) per watt VT (tidal volume): Volume of air inhaled or exhaled with each breath. Could be the volume of a particular breath or the average breath volume over a specified period of time usually 1 minute. It is conventionally expressed in units of millilitres or litres (BTPS). WR (work rate or power): Reflects the rate at which work is performed (i.e., work performed per unit of time). Work rate is usually measured in watts. Appendix 3 (Lung function test data) In this appendix you can find an example of the lung function test data that the physiotherapist receives from the lung function department of the St Lucas Andreas Hospital. (Next page) In general it is not essential to be able to read the different ECGs as a physiotherapist and therefore it is not necessary to look at them. 39
40 40
41 41
42 42
43 43
44 44
45 45
46 46
47 47
48 48
49 49
50 50
51 51
52 52

53 53
54 54
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
6- Lung Volumes and Pulmonary Function Tests
 6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
6- Lung Volumes and Pulmonary Function Tests s (PFTs) are noninvasive diagnostic tests that provide measurable feedback about the function of the lungs. By assessing lung volumes, capacities, rates of
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual can
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Chapter 3. Pulmonary Function Study Assessments. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Chapter 3 Pulmonary Function Study Assessments 1 Introduction Pulmonary function studies are used to: Evaluate pulmonary causes of dyspnea Differentiate between obstructive and restrictive pulmonary disorders
Spirometry in primary care
 Spirometry in primary care Wednesday 13 th July 2016 Dr Rukhsana Hussain What is spirometry? A method of assessing lung function Measures volume of air a patient can expel after a full inspiration Recorded
Spirometry in primary care Wednesday 13 th July 2016 Dr Rukhsana Hussain What is spirometry? A method of assessing lung function Measures volume of air a patient can expel after a full inspiration Recorded
Pulmonary Function Testing
 In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
In the Clinic Pulmonary Function Testing Hawa Edriss MD, Gilbert Berdine MD The term PFT encompasses three different measures of lung function: spirometry, lung volumes, and diffusion capacity. In this
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
PULMONARY FUNCTION. VOLUMES AND CAPACITIES
 PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
PULMONARY FUNCTION. VOLUMES AND CAPACITIES The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer (spiro = breath, meter = to measure). A bell spirometer
Pulmonary Function Tests. Mohammad Babai M.D Occupational Medicine Specialist
 Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
Pulmonary Function Tests Mohammad Babai M.D Occupational Medicine Specialist www.drbabai.com Pulmonary Function Tests Pulmonary Function Tests: Spirometry Peak-Flow metry Bronchoprovocation Tests Body
SPIROMETRY TECHNIQUE. Jim Reid New Zealand
 Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Jim Reid New Zealand The Basics Jim Reid Spirometry measures airflow and lung volumes, and is the preferred lung function test in COPD. By measuring reversibility of obstruction, it is also diagnostic
Respiratory Physiology In-Lab Guide
 Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Spirometry: FEVER DISEASE DIABETES HOW RELIABLE IS THIS? 9/2/2010 BUT WHAT WE PRACTICE: Spirometers are objective tools
 SPIROMETRY PRINCIPLES, PROCEDURE AND QA Spirometry: Dr. Rahul Kodgule CHEST RESEARCH FOUNDATION, PUNE FEVER ISCHAEMIC HEART DISEASE DIABETES BUT WHAT WE PRACTICE: Spirometers are objective tools to diagnose
SPIROMETRY PRINCIPLES, PROCEDURE AND QA Spirometry: Dr. Rahul Kodgule CHEST RESEARCH FOUNDATION, PUNE FEVER ISCHAEMIC HEART DISEASE DIABETES BUT WHAT WE PRACTICE: Spirometers are objective tools to diagnose
A Primer on Reading Pulmonary Function Tests. Joshua Benditt, M.D.
 A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
A Primer on Reading Pulmonary Function Tests Joshua Benditt, M.D. What Are Pulmonary Function Tests Used For? Pulmonary function testing provides a method for objectively assessing the function of the
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
behaviour are out of scope of the present review.
 explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
explained about the test, a trial may be done before recording the results. The maneuver consists initially of normal tidal breathing. The subject then inhales to maximally fill the lungs. This is followed
Spirometry: an essential clinical measurement
 Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Shortness of breath THEME Spirometry: an essential clinical measurement BACKGROUND Respiratory disease is common and amenable to early detection and management in the primary care setting. Spirometric
Respiratory System Mechanics
 M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
Respiratory System. Chapter 9
 Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Clinical pulmonary physiology. How to report lung function tests
 Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Clinical pulmonary physiology or How to report lung function tests Lung function testing A brief history Why measure? What can you measure? Interpretation/ reporting Examples and case histories Exercise
Content Indica c tion Lung v olumes e & Lung Indica c tions i n c paci c ties
 Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
Spirometry Content Indication Indications in occupational medicine Contraindications Confounding factors Complications Type of spirometer Lung volumes & Lung capacities Spirometric values Hygiene &
SPIROMETRY METHOD. COR-MAN IN / EN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
SPIROMETRY METHOD COR-MAN-0000-006-IN / EN Issue A, Rev. 2 2013-07 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
Breathing and pulmonary function
 EXPERIMENTAL PHYSIOLOGY EXPERIMENT 5 Breathing and pulmonary function Ying-ying Chen, PhD Dept. of Physiology, Zhejiang University School of Medicine bchenyy@zju.edu.cn Breathing Exercise 1: Tests of pulmonary
EXPERIMENTAL PHYSIOLOGY EXPERIMENT 5 Breathing and pulmonary function Ying-ying Chen, PhD Dept. of Physiology, Zhejiang University School of Medicine bchenyy@zju.edu.cn Breathing Exercise 1: Tests of pulmonary
PULMONARY FUNCTION TEST(PFT)
") PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
PULMONARY FUNCTION TEST(PFT) Objectives: By the end of the present lab, students should be able to: 1. Record lung volumes and capacities and compare them with those of a typical person of the same gender,
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Spirometry: Introduction
 Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
PULMONARY FUNCTION TESTING. By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS)
 Tehran University of Medical Sciences (TUMS)") PULMONARY FUNCTION TESTING By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS) PULMONARY FUNCTION TESTS CATEGORIES Spirometry Lung volumes
PULMONARY FUNCTION TESTING By: Gh. Pouryaghoub. MD Center for Research on Occupational Diseases (CROD) Tehran University of Medical Sciences (TUMS) PULMONARY FUNCTION TESTS CATEGORIES Spirometry Lung volumes
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Respiratory System. Introduction. Atmosphere. Some Properties of Gases. Human Respiratory System. Introduction
 Introduction Respiratory System Energy that we consume in our food is temporarily stored in the bonds of ATP (adenosine triphosphate) before being used by the cell. Cells use ATP for movement and to drive
Introduction Respiratory System Energy that we consume in our food is temporarily stored in the bonds of ATP (adenosine triphosphate) before being used by the cell. Cells use ATP for movement and to drive
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
UNIT TWO: OVERVIEW OF SPIROMETRY. A. Definition of Spirometry
 UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
UNIT TWO: OVERVIEW OF SPIROMETRY A. Definition of Spirometry Spirometry is a medical screening test that measures various aspects of breathing and lung function. It is performed by using a spirometer,
BETTER SPIROMETRY. Marijke Currie (CRFS) Care Medical Ltd Phone: Copyright CARE Medical ltd
 Care Medical Ltd Phone: Copyright CARE Medical ltd") BETTER SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual
BETTER SPIROMETRY Marijke Currie (CRFS) Care Medical Ltd Phone: 0800 333 808 Email: sales@caremed.co.nz What is spirometry Spirometry is a physiological test that measures the volume of air an individual
Lung function testing
 ACTIVITY BRIEF Lung function testing The science at work Common respiratory complaints include asthma and COPD (chronic obstructive pulmonary disease). Peak flow meters and spirometers can be used by health
ACTIVITY BRIEF Lung function testing The science at work Common respiratory complaints include asthma and COPD (chronic obstructive pulmonary disease). Peak flow meters and spirometers can be used by health
Physiology lab (RS) First : Spirometry. ** Objectives :-
 First : Spirometry. ** Objectives :-") Physiology lab (RS) ** Objectives :- 1. Spirometry in general. 2. Spirogram (volumes and capacities). 3. The importance of vital capacity in diagnosis. 4. Flow volume loop. 5. Miss Arwa s part (the practical
Physiology lab (RS) ** Objectives :- 1. Spirometry in general. 2. Spirogram (volumes and capacities). 3. The importance of vital capacity in diagnosis. 4. Flow volume loop. 5. Miss Arwa s part (the practical
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
S P I R O M E T R Y. Objectives. Objectives 3/12/2018
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
-SQA-SCOTTISH QUALIFICATIONS AUTHORITY. Hanover House 24 Douglas Street GLASGOW G2 7NQ NATIONAL CERTIFICATE MODULE DESCRIPTOR
 -SQA-SCOTTISH QUALIFICATIONS AUTHORITY Hanover House 24 Douglas Street GLASGOW G2 7NQ NATIONAL CERTIFICATE MODULE DESCRIPTOR -Module Number- 0099111 -Session-1989-90 -Superclass- PB -Title- PRINCIPLES
-SQA-SCOTTISH QUALIFICATIONS AUTHORITY Hanover House 24 Douglas Street GLASGOW G2 7NQ NATIONAL CERTIFICATE MODULE DESCRIPTOR -Module Number- 0099111 -Session-1989-90 -Superclass- PB -Title- PRINCIPLES
Analysis of Lung Function
 Computer 21 Spirometry is a valuable tool for analyzing the flow rate of air passing into and out of the lungs. Flow rates vary over the course of a respiratory cycle (a single inspiration followed by
Computer 21 Spirometry is a valuable tool for analyzing the flow rate of air passing into and out of the lungs. Flow rates vary over the course of a respiratory cycle (a single inspiration followed by
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
Respiratory Pathophysiology Cases Linda Costanzo Ph.D.
 Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Spirometry. Obstruction. By Helen Grim M.S. RRT. loop will have concave appearance. Flows decreased consistent with degree of obstruction.
 1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
1 2 Spirometry By Helen Grim M.S. RRT 3 4 Obstruction loop will have concave appearance. Flows decreased consistent with degree of obstruction. Volumes may be normal, but can decrease with severity of
Chapter 10. The Respiratory System Exchange of Gases. Copyright 2009 Pearson Education, Inc.
 Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
S P I R O M E T R Y. Objectives. Objectives 2/5/2019
 S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
S P I R O M E T R Y Dewey Hahlbohm, PA-C, AE-C Objectives To understand the uses and importance of spirometry testing To perform spirometry testing including reversibility testing To identify normal and
#7 - Respiratory System
 #7 - Respiratory System Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Perform spirometry to measure lung volumes Define and understand the lung volumes and
#7 - Respiratory System Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Perform spirometry to measure lung volumes Define and understand the lung volumes and
Spirometry and Flow Volume Measurements
 Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Spirometry and Flow Volume Measurements Standards & Guidelines December 1998 To serve the public and guide the medical profession Revision Dates: December 1998 Approval Date: June 1998 Originating Committee:
Chronic Obstructive Pulmonary Disease (COPD) is a systematic disease with
 is a systematic disease with") Chronic Obstructive Pulmonary Disease (COPD) is a systematic disease with considerable impact on several dimensions of daily life. Those that suffer from COPD can be submitted to rehabilitation programmes.
Chronic Obstructive Pulmonary Disease (COPD) is a systematic disease with considerable impact on several dimensions of daily life. Those that suffer from COPD can be submitted to rehabilitation programmes.
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Pulmonary Function Testing
 Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Pulmonary Function Testing Let s catch our breath Eddie Needham, MD, FAAFP Program Director Emory Family Medicine Residency Program Learning Objectives The Astute Learner will: Become familiar with indications
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Chapter 11 The Respiratory System
 Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
BiomedicalInstrumentation
 University of Zagreb Faculty of Electrical Engineering and Computing BiomedicalInstrumentation Measurementofrespiration prof.dr.sc. Ratko Magjarević October 2013 Respiratorysystem Consistsofthelungs, airways
University of Zagreb Faculty of Electrical Engineering and Computing BiomedicalInstrumentation Measurementofrespiration prof.dr.sc. Ratko Magjarević October 2013 Respiratorysystem Consistsofthelungs, airways
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Reference Guide for Group Education
 A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 1 Introduction to Living Well with COPD Education Program Participants Expectations Towards the Program Health in COPD
A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 1 Introduction to Living Well with COPD Education Program Participants Expectations Towards the Program Health in COPD
Interpreting pulmonary function tests: Recognize the pattern, and the diagnosis will follow
 REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
REVIEW FEYROUZ AL-ASHKAR, MD Department of General Internal Medicine, The Cleveland Clinic REENA MEHRA, MD Department of Pulmonary and Critical Care Medicine, University Hospitals, Cleveland PETER J. MAZZONE,
Emphysema. Lungs The lungs help us breathe in oxygen and breathe out carbon dioxide. Everyone is born with 2 lungs: a right lung and a left lung.
 Emphysema Introduction Emphysema is a type of chronic obstructive pulmonary disease, or COPD. COPD affects millions of people worldwide. Emphysema involves damage to the air sacs in the lungs. This makes
Emphysema Introduction Emphysema is a type of chronic obstructive pulmonary disease, or COPD. COPD affects millions of people worldwide. Emphysema involves damage to the air sacs in the lungs. This makes
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease
 Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Alpha-1 Antitrypsin Deficiency Alpha-1 Lung Disease Chronic obstructive pulmonary disease (COPD) affects millions of people each year. Chronic means long term, obstructive means it is hard to get air in
Chapter 10 Respiration
 1 Chapter 10 Respiration Introduction/Importance of the Respiratory System All eukaryotic organisms need oxygen to perform cellular respiration (production of ATP), either aerobically or anaerobically.
1 Chapter 10 Respiration Introduction/Importance of the Respiratory System All eukaryotic organisms need oxygen to perform cellular respiration (production of ATP), either aerobically or anaerobically.
PomPom SHOOTER. Activity Background: Common Obstructive Lung Disorders:
 CAUTION: Students with asthma or other respiratory problems should NOT perform the breathing exercises in this activity because they involve repeated maximal inhalations and exhalations and use of a breathing
CAUTION: Students with asthma or other respiratory problems should NOT perform the breathing exercises in this activity because they involve repeated maximal inhalations and exhalations and use of a breathing
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
The Respiratory System Structures of the Respiratory System Structures of the Respiratory System Structures of the Respiratory System Nose Sinuses
 CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation. Susan Blonshine RRT, RPFT, AE-C, FAARC
 Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
Getting Spirometry Right It Matters! Performance, Quality Assessment, and Interpretation Susan Blonshine RRT, RPFT, AE-C, FAARC Objectives Sample Title Recognize acceptable spirometry that meets the start
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Patient assessment - spirometry
 Patient assessment - spirometry STEP 1 Learning objectives This module will provide you with an understanding of spirometry and the role it plays in aiding the diagnosis of lung diseases, particularly
Patient assessment - spirometry STEP 1 Learning objectives This module will provide you with an understanding of spirometry and the role it plays in aiding the diagnosis of lung diseases, particularly
Office Based Spirometry
 Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Osteopathic Family Physician (2014)1, 14-18 Scott Klosterman, DO; Woodson Crenshaw, OMS4 Spartanburg Regional Family Medicine Residency Program; Edward Via College of Osteopathic Medicine - Virginia Campus
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Pulmonary Func-on Tes-ng. Chapter 8
 Pulmonary Func-on Tes-ng Chapter 8 Pulmonary Func-on Tes-ng Which of the following is the true pulmonary func-on test? Spirometry Lung volumes Diffusion capacity ABG Pulmonary Func-on Tes-ng Process of
Pulmonary Func-on Tes-ng Chapter 8 Pulmonary Func-on Tes-ng Which of the following is the true pulmonary func-on test? Spirometry Lung volumes Diffusion capacity ABG Pulmonary Func-on Tes-ng Process of
Spirometric protocol
 Spirometric protocol Spirometry is the most common of the Pulmonary Function Test, that measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
Spirometric protocol Spirometry is the most common of the Pulmonary Function Test, that measures lung function, specifically the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
In order to diagnose lung diseases doctors
 You Take My Breath Away Activity 5C NOTE: This activity is designed to follow You Really Are Full of Hot Air! Activity Objectives: After completing You Really Are Full of Hot Air! Activity 5B, students
You Take My Breath Away Activity 5C NOTE: This activity is designed to follow You Really Are Full of Hot Air! Activity Objectives: After completing You Really Are Full of Hot Air! Activity 5B, students
Chapter 10. Respiratory System and Gas Exchange. Copyright 2005 Pearson Education, Inc. publishing as Benjamin Cummings
 Chapter 10 Respiratory System and Gas Exchange Function of the Respiratory System To obtain oxygen (O 2 ) for all cells in the body. To rid the cells of waste gas (CO 2 ). Oxygen (O 2 ) is vital chemical
Chapter 10 Respiratory System and Gas Exchange Function of the Respiratory System To obtain oxygen (O 2 ) for all cells in the body. To rid the cells of waste gas (CO 2 ). Oxygen (O 2 ) is vital chemical
SPIROMETRY. Performance and Interpretation for Healthcare Professionals. Faculty of Respiratory Physiology IICMS. Version 1 April 2015
 SPIROMETRY Performance and Interpretation for Healthcare Professionals Faculty of Respiratory Physiology IICMS Version 1 April 2015 Authors: Maria Mc Neill & Geraldine Nolan www.iars.ie Contents Page Background
SPIROMETRY Performance and Interpretation for Healthcare Professionals Faculty of Respiratory Physiology IICMS Version 1 April 2015 Authors: Maria Mc Neill & Geraldine Nolan www.iars.ie Contents Page Background
LUNGS. Requirements of a Respiratory System
 Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects
 Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
Lung Function Basics of Diagnosis of Obstructive, Restrictive and Mixed Defects Use of GOLD and ATS Criteria Connie Paladenech, RRT, RCP, FAARC Benefits and Limitations of Pulmonary Function Testing Benefits
CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT
 Circular Instruction 195 CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT COMPENSATION FOR OCCUPATIONAL INJURIES
Circular Instruction 195 CIRCULAR INSTRUCTION REGARDING ESTABLISHMENT OF IMPAIRMENT DUE TO OCCUPATIONAL LUNG DISEASE FOR THE PURPOSES OF AWARDING PERMANENT DISABLEMENT COMPENSATION FOR OCCUPATIONAL INJURIES
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
Tuesday, December 13, 16. Respiratory System
 Respiratory System Trivia Time... What is the fastest sneeze speed? What is the surface area of the lungs? (hint... think of how large the small intestine was) How many breaths does the average person
Respiratory System Trivia Time... What is the fastest sneeze speed? What is the surface area of the lungs? (hint... think of how large the small intestine was) How many breaths does the average person
How to Perform Spirometry
 Purpose How to Perform Spirometry This guideline provides recommendations regarding best practice to support high quality spirometry practice for KINNECT Pre-Employment Medicals. Scope This guideline provides
Purpose How to Perform Spirometry This guideline provides recommendations regarding best practice to support high quality spirometry practice for KINNECT Pre-Employment Medicals. Scope This guideline provides
UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1)
") UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1) Textbook of medical physiology, by A.C. Guyton and John E, Hall, Twelfth Edition,
UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1) Textbook of medical physiology, by A.C. Guyton and John E, Hall, Twelfth Edition,
#8 - Respiratory System
 Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Page1 #8 - Objectives: Study the parts of the respiratory system Observe slides of the lung and trachea Equipment: Remember to bring photographic atlas. Figure 1. Structures of the respiratory system.
Credential Maintenance Program
 First Quarter of the Calendar 5 I. INSTRUMENTATION / EQUIPMENT 1 4 5 A. Set Up, Maintain, Calibrate 1 2 3 1. Blood gas analyzers 2. CO-oximeters / hemoximeters 3. Spirometers (for example, diagnostic,
First Quarter of the Calendar 5 I. INSTRUMENTATION / EQUIPMENT 1 4 5 A. Set Up, Maintain, Calibrate 1 2 3 1. Blood gas analyzers 2. CO-oximeters / hemoximeters 3. Spirometers (for example, diagnostic,
Pulmonary Function Test
 Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Lung Pathophysiology & PFTs
 Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
Interpretation of Pulmonary Function Tests (PFTs) Course # 1612 2:00 5:00pm Friday February 22, 2013 Lung Pathophysiology & PFTs Mark F. Sands MD, FCCP, FAAAAI Division of Allergy, Immunology & Rheumatology
PDF of Trial CTRI Website URL -
 Clinical Trial Details (PDF Generation Date :- Wed, 31 Oct 2018 11:13:48 GMT) CTRI Number Last Modified On 17/01/2015 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Clinical Trial Details (PDF Generation Date :- Wed, 31 Oct 2018 11:13:48 GMT) CTRI Number Last Modified On 17/01/2015 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing
 Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing Components of the respiratory system Nasal cavity Pharynx Trachea Bronchi Bronchioles Lungs
Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing Components of the respiratory system Nasal cavity Pharynx Trachea Bronchi Bronchioles Lungs
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities
 Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Asthma Management Introduction, Anatomy and Physiology
 Asthma Management Introduction, Anatomy and Physiology University of Utah Center for Emergency Programs and The Utah Asthma Program Incidence, Impact and Goals of Asthma Management Prevalence, Morbidity
Asthma Management Introduction, Anatomy and Physiology University of Utah Center for Emergency Programs and The Utah Asthma Program Incidence, Impact and Goals of Asthma Management Prevalence, Morbidity
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------