Diagnosis and management of Asthma in Adults. (Version 1.1)
|
|
|
- Osborne Crawford
- 6 years ago
- Views:
Transcription
1 Pan-Birmingham Respiratory Clinical Network Diagnosis and management of Asthma in Adults (Version 1.1) Revision History Guideline Author: Guideline Sponsor: Date of Approval: 23/03/2017 Approved by: Date of Joint CCG Q&S Guideline Sub Group Ratification: Duncan Wilson in conjunction with pan-birmingham Respiratory Clinical Network Dr Raj Ramachandran, Chair of pan-birmingham Respiratory Clinical Network Pan-Birmingham Respiratory Clinical Network 25/05/2017 Review Date: March 2018 Related Policies / Topic / Driver BTS/SIGN British Guideline on the management of asthma, September 2016 Version No Date of Issue Author Reason for Issue 0.1 Duncan Wilson First Draft /05/2017 Duncan Wilson Ratified /07/2017 Karen Ennis Minor amendment in Step-Down Protocol
2 Table of Contents 1 Overview/Introduction Objectives of Guideline Diagnosis Management For all patients Occupational asthma Pregnancy & asthma Monitoring asthma control Pharmacological management Step-wise management SABA therapy Regular preventer therapy Initial add-on therapy Additional add-on therapies High dose therapies Continuous or frequent use of oral steroids Severe Difficult to Treat Asthma Management of Acute Severe Asthma Adherence Overlap between COPD and asthma Methodology Implementation Application of the Guideline Launch and Implementation Plan for Clinical Guidelines Appendices: Appendix 1: Plan on a Page Appendix 2: Step down Appendix 3: Management of acute asthma in General Practice
3 1 Overview/Introduction This guideline is intended to support the Respiratory Chapter of the Birmingham, Sandwell, Solihull and environs APC formulary by providing guidance on the diagnosis and management of asthma in adults. The British Thoracic Society (BTS) guideline on the management of Asthma produced in conjunction with the Scottish Intercollegiate Guidelines Network (SIGN) since 1999, has been updated several times since its first publication in The latest version was published in September 2016 and can be accessed at: The BTS-SIGN guideline informs the general framework of this local asthma guideline. The National Institute for Health and Care Excellence (NICE) was due to publish guidance on diagnosis and monitoring of asthma before the end of 2015 but this is currently suspended pending further consultation. NICE guidance on management of asthma is expected in October Objectives of Guideline To encourage consistency in Asthma diagnosis To encourage rational and consistent prescribing in patients diagnosed with asthma 3

4 3 Diagnosis Chapter 3 (page 13) of the BTS/SIGN guideline covers diagnosis and monitoring of asthma and includes an updated diagnostic algorithm summarising the recommended approach to the diagnosis of asthma in adults: Figure 1: Diagnostic Algorithm - British Thoracic Society 2016 Diagnosis of asthma should be confirmed using this algorithm until such time as a universally accepted change is adopted It should be noted that future guidelines will undoubtedly demand the introduction of more objective tests of airflow obstruction (spirometry, reversibility, peak flow monitoring and challenge testing) and of airway inflammation (exhaled Nitric Oxide FeNO) that are included as options for investigation in the BTS/SIGN algorithm. 4
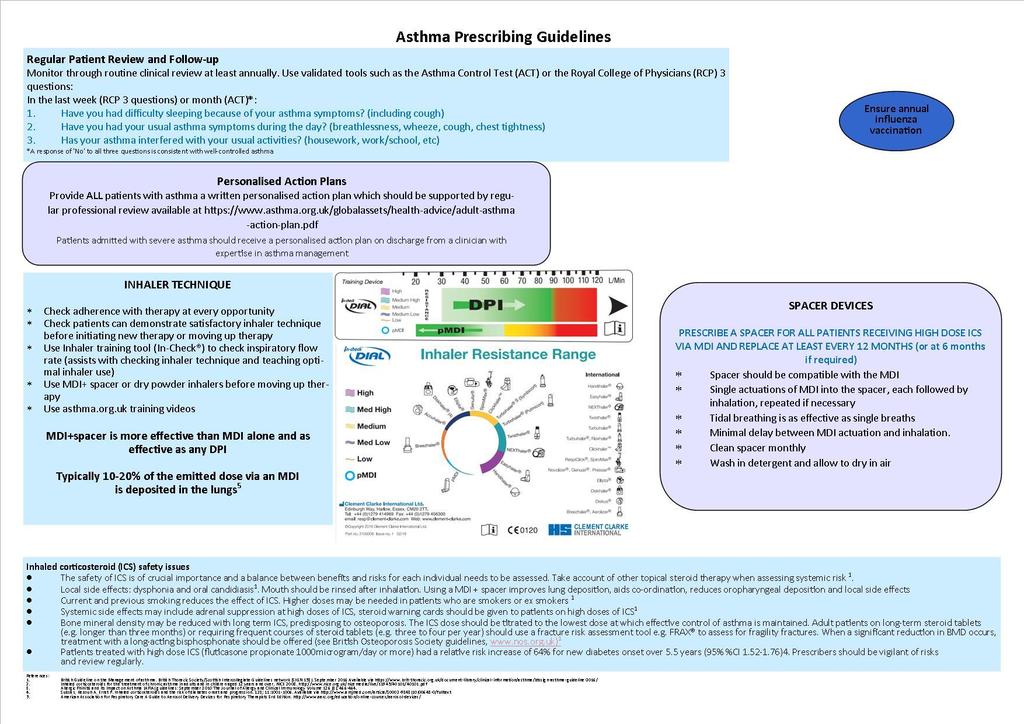
5 4 Management 4.1 For all patients Take a detailed allergy history ask about and treat rhinitis symptoms Start SABA (Salbutamol or Terbutaline) prn and check inhaler technique Consider immediate introduction of preventive therapy (inhaled corticosteroids) Ensure that the patient has an asthma self-management plan. The format of the document may vary to meet the needs of the individual patient but it is recommended that it should detail as a minimum: o Recognition of exacerbations o Response to changes in symptoms or peak flow measurements o Where to obtain advice e.g. Asthma nurse, GP o Offer/refer to smoking cessation if appropriate o Annual influenza immunisation (unless contraindicated) 4.2 Occupational asthma An occupational history should be taken from all patients to identify both current and past possible sensitisers. Patients should be asked whether symptoms occur, or are worse, at work and are improved during periods away from work. When work-related asthma is suspected refer to the specialist occupational asthma service at the Birmingham Chest Clinic (Dr Gareth Walters) 4.3 Pregnancy & asthma Some patients with asthma, particularly if severe, become unstable during pregnancy. These patients should be monitored carefully and referred for specialist assessment if control is difficult to maintain. 5
6 4.4 Monitoring asthma control Asthma control can be assessed by a variety of means: Short symptom-based questionnaires such as the RCP 3 questions or the Asthma Control Test (ACT) give a simple numerical readout and can demonstrate serial change. Peak Expiratory Flow Rate (PEFR) monitoring is useful when patients demonstrate consistent technique and know their best or usual values. PEFR forms the basis of many individualised asthma action plans. Fraction of Exhaled Nitric Oxide (FeNO) is a rapidly emerging tool that assesses the extent of airway inflammation and predicts instability. It is likely that FeNO will feature in monitoring guidance and future management guidelines. FeNO is recommended as an option to support asthma management in people who are symptomatic despite using inhaled corticosteroids Pharmacological management Abbreviation SABA LABA ICS ICS/LABA LAMA LTRA Full name Short acting beta agonist Long acting beta agonist Inhaled Corticosteroid Combination of ICS and LABA Long acting muscarinic antagonist Leukotriene Receptor Antagonist Theophylline Table 1: Drug class abbreviations 1 NICE diagnostics guidance [DG12] April

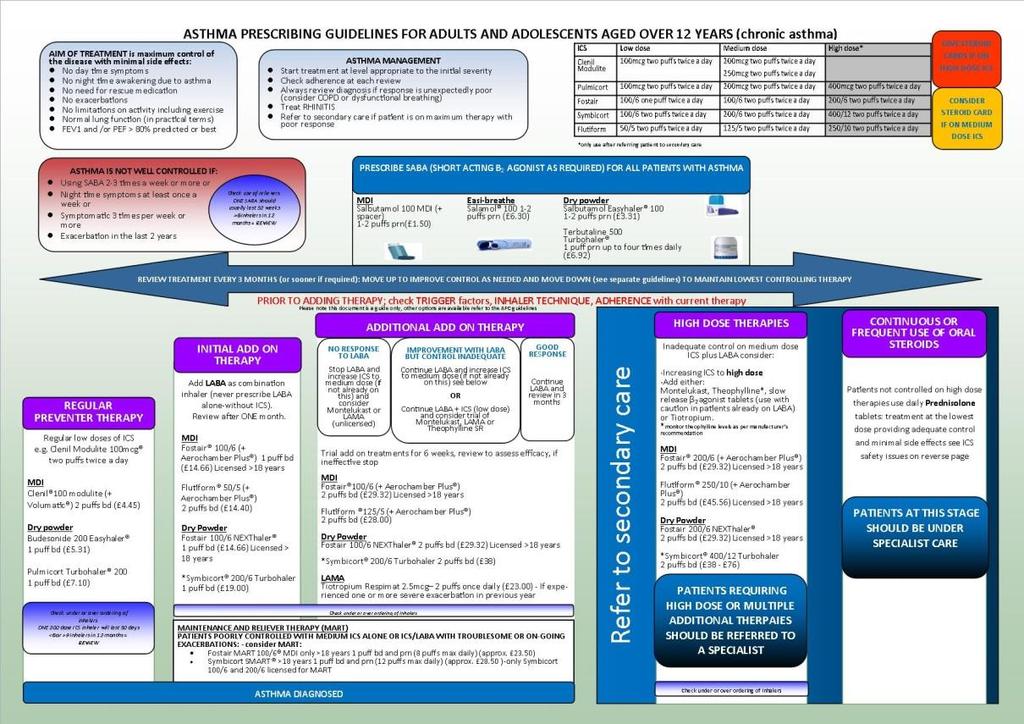
7 4.5.1 Step-wise management Central to the BTS/SIGN guideline is the well established step-wise approach to the management of asthma. This has been updated for the 2016 guideline to reflect a lower threshold for the initiation of regular inhaled corticosteroid therapy in the aftermath of the 2014 National Review of Asthma Deaths 2. This updated series of steps has been adapted for this guideline and may be found in Appendix 1 Successful treatment of asthma with inhaled therapy is dependent on the interaction between patient, drug and device. An assessment of inhaler technique should take place before the initiation of any new inhaled therapy. It should be noted that there is a general move toward dry powder inhalers in preference to pmdi for sustainability reasons so where there is no clear preference for an individual patient a dry powder device should be chosen as first line. 2 National Review of Asthma Deaths, Royal College of Physicians,
8 4.5.2 SABA therapy All patients should be prescribed a SABA to be taken as required Choice is limited to Salbutamol and Terbutaline. Salbutamol is available in a variety of devices and the most suitable device for the patient should be determined by assessing inhaler technique. Terbutaline is only available as Bricanyl Turbohaler. Use of a SABA more than 2-3 times per week is a marker of poor asthma control and such high volume usage should trigger a review. Nebulised SABA [Salbutamol (formulary status Green) and Terbutaline (formulary status Amber)] should only be initiated on specialist advice Regular preventer therapy Low dose inhaled corticosteroid (ICS) therapy is the cornerstone of asthma management in most patients and should be commenced as soon as the diagnosis has been confirmed. There are a number of available preparations and again a choice should be made after a device assessment and the dose selected according to history of symptoms and exacerbations. First line regular preventer therapy would normally be Beclometasone from a fine particle CFC free inhaler taken through a spacer device e.g. Clenil Modulite 100mcg 2 puffs twice daily. Second line ICS are shown in Appendix 1 Notes: There is no clear evidence of any difference in efficacy between ICS preparations at equivalent doses and the most suitable drug and device for the individual patient should be selected as appropriate to the severity of the disease 3. Fluticasone Propionate (Flixotide) is now reserved for paediatric use. 3 NICE Technology Appraisal guidance [TA138] March
9 Localised side effects, which are common to most ICS, such as oral candidiasis and dysphonia can be minimised by using correct inhaler technique particularly utilising a spacer with MDI preparations, followed by rinsing the mouth and throat out with water. Ciclesonide is a fine particle ICS that is delivered from an MDI as a pro-drug and converted into active drug in the lungs. As such it offers an alternative when local side effects prevent use of other ICS. It also has an emerging role in patients with severe asthma requiring additional ICS to adequately control airway inflammation. It is currently included on the formulary with Red status hospital prescription only (for new initiation.) Initial add-on therapy If asthma is uncontrolled despite optimal therapy with low dose ICS then a LABA should be added. In most cases this will involve the change to a combination inhaler. There is a wide choice of preparations and those included on the formulary are shown in Appendix 1. Notes: Choice of preparation should be made based on severity of asthma and device assessment. It is usually possible to achieve consistency of device e.g. Clenil to Fostair, Pulmicort to Symbicort. It is important that patients with asthma are NOT treated with stand-alone LABA therapy without ICS. 4 Formoterol and Salmeterol (Green formulary status) are both available as individual drugs, but MUST be used in conjunction with an ICS Maintenance And Reliever Therapy (MART) is a regime in which a single combination inhaler is used for both maintenance therapy and symptom relief. Fostair 100/6 (pmdi) and Symbicort 200/6 (DPI) (Green formulary status) are licensed for this indication. 4 Pesola et al. Long Acting Beta agonists and their relation to increased Asthma morbidity and mortality The FDA meta-analysis. The internet journal of Asthma, Allergy and Immunology. 2008, 7(1) 9
10 Seretide this combination is now only on formulary for paediatric patients. There is, however, a large cohort of legacy patients who should only be switched to an alternative preparation after clinical review and device assessment. Generic prescribing new products containing established combinations in new devices (such as Sirdupla MDI, Duoresp Spiromax, AirFluSal Forspiro, AirFluSal MDI) have recently been licensed. Care must be taken to prescribe combination products BY BRAND to negate the possibility of inadvertent switching to an unfamiliar device. Relvar This is the latest ICS/LABA combination inhaler (Fluticasone Furoate/Vilanterol trifenatate.) It is licensed for asthma and COPD and has recently been added to the formulary for COPD Additional add-on therapies Leukotriene Receptor Antagonists Montelukast 10mg daily is first line (Green formulary status) Zafirlukast 20mg BD is second line if montelukast is not tolerated (Green formulary status). It is recommended that these medications are given for a six week initial trial period followed by objective review to assess efficacy and determine continuation of therapy. Side effects are unusual but there are reports of a potential increased risk of vasculitis (Churg-Strauss type.) Long-acting muscarinic antagonist (LAMA) Tiotropium taken via the respimat device in a dose of 5 micrograms (2 puffs) once daily is the only LAMA available for the treatment of asthma. It is licensed as an add-on maintenance bronchodilator in adults with asthma who are receiving maintenance treatment with a combination of ICS (at least 800 micrograms of Budesonide per day or equivalent) and LABA and who have experienced 1 or more severe exacerbations in the previous year. 5 5 NICE ESNM55 March
11 Theophyllines Methylxanthines have been used as bronchodilators for many years. All have a low therapeutic ratio meaning that side effects (nausea, palpitations) are fairly common even at therapeutic doses. Available formulary preparations (Green formulary status) include Phyllocontin Continus (225mg tablets) and Phyllocontin Forte Continus (350mg) brand of aminophylline and Uniphyllin Continus (200mg, 300mg and 400mg slow release tablets) brand of theophylline. Other non-formulary brands are available (such as Slo-phyllin and Nuelin SA) but as adsorption from modified-release preparations can vary between brands, patients should be maintained on the same brand that they were initiated and stabilised on. Patients should be initiated on low doses which can be titrated up as tolerated. Therapeutic drug monitoring is possible but is only clinically useful in assessing concordance. Oral beta agonists These are not recommended as routine treatment in adults and should only be initiated on specialist advice. Salbutamol (2mg and 4mg tablets and 2mg/5ml liquid, Green formulary status) and terbutaline (Bricanyl 5mg) are available in oral preparations as is Bambuterol (Bambec 10mg and 20mg, Amber formulary status) When asthma is well controlled it may be possible to step-down treatment to the lowest level that maintains control. Advice on achieving this goal is include at Appendix High dose therapies This treatment step covers patients treated with high dose ICS and additional addon therapies as above. All patients requiring high dose or multiple additional therapies should be referred to a specialist asthma clinic in secondary care Continuous or frequent use of oral steroids When asthma is not controlled and frequent exacerbations continue to occur despite optimal high dose treatment, then use of oral corticosteroid maintenance treatment should be considered. 11
12 Treatment should be kept at the lowest dose possible and side effects minimised through careful monitoring of BP and blood glucose and prescription of appropriate bone protection treatment. Daily oral corticosteroid therapy should not be discontinued abruptly and assessment of the HPA axis by Short Synacthen Test should be considered if therapy is to be withdrawn after a prolonged period. Consideration should be given to bone protection in patients having regular or frequent courses of oral steroids. The RCP produced a guide for the management of glucocorticoid-induced osteoporosis which can be accessed via the link coid-induced_osteoporosis[1].pdf Patients on continuous oral steroids should be under the care of a secondary care clinic run by a consultant with an interest in asthma. 4.6 Severe Difficult to Treat Asthma Patients with Severe Difficult to Treat Asthma (SDTA) remain symptomatic and have exacerbations despite adherence to treatment at guideline limits. Such patients should be referred to the Birmingham Regional Severe Asthma Service (BRSAS) which is centered on Birmingham Heartlands Hospital (Dr Adel Mansur) and has sites at the Queen Elizabeth Hospital Birmingham (Dr Duncan Wilson & Dr Ben Sutton) and Sandwell and West Birmingham Hospital (Dr Arvind Rajasekaran & Dr Adeel Sahal.) BRSAS offers comprehensive structured assessment and access to high cost therapies such as Omalizumab, other emerging monoclonal antibody therapies and Bronchial Thermoplasty as well as attention to other physical and psychological co-morbidities including Vocal Cord Dysfunction, dysfunctional breathing and gastro-oesophageal reflux disease amenable to surgery. 12
13 Referral criteria for the BRSAS are: Patients who are still symptomatic despite high dose therapy Those with previous near fatal/itu episodes Oral Corticosteroid dependency Diagnostic uncertainty with difficult to control symptoms e.g. psychological, dysfunctional breathing, hyperventilation syndromes and vocal cord dysfunction Those who would be suitable for biological agents treatments (meeting xolair criteria) Bronchial thermoplasty treatment (indication: uncontrolled on combination treatment with 3rd/4th controller, no significant bronchiectasis and evident bronchial reversibility, and patient wishes to be considered for treatment) Other presentations that may benefit from BRSAS include ABPA, and those who are interested in clinical trials for severe asthma. Further information, including contact details, are available at Management of Acute Severe Asthma The BTS-SIGN guideline contains clear guidance on the management of Acute Severe Asthma in adults which can be found at Annexes 2-4 of the September 2016 guideline (pages ) and at Appendix 3 of this guideline. Particular attention is drawn to the need for accurate assessment of severity (utilising symptoms, respiratory rate, heart rate and PEFR) which drives decisions regarding safe location for ongoing treatment, and the importance of early administration of systemic steroids. Requirements for follow up after acute exacerbation are clearly articulated and include an appointment in primary care within 48 hours of initial treatment. This consultation presents an opportunity for a systematic review including recognition of triggers, smoking cessation advice, assessment of treatment level and concordance, review of the personalised action plan and consideration of standby therapy or secondary care referral. 13
14 4.8 Adherence The biggest reason for failure of asthma treatment is lack of compliance with therapy. Attention should be paid to this at all stages of treatment inhaler technique should be checked and corrected and monitoring of drug levels considered when non-compliance is suspected. Most inhaler devices have dose counters built in and more sophisticated remote monitoring technologies are emerging to support the monitoring of compliance e.g. the smartinhaler Overlap between COPD and asthma A significant number of patients with longstanding asthma develop fixed airflow obstruction, whether or not they are smokers. There is, therefore, a grey area between pure asthma at one end of a spectrum and pure COPD at the other end. The term asthma-copd overlap syndrome (ACOS) has been applied to this group and this is explored in more detail in the sister guideline to this one for COPD. Treatment decisions are increasingly being tailored to the individual, based on the phenotype of their airways disease. In general we would advocate use of the guideline for the condition most prominent in the patient (i.e. patients with COPD who exhibit reversibility to bronchodilators should be treated using the COPD guideline and those with lifelong asthma, with fixed airflow obstruction, should be treated using the asthma guideline.) All smokers should be strongly encouraged to quit and supported robustly in their quit attempts. 5 Methodology This guideline was developed by the UHBFT asthma lead (Dr Duncan Wilson) in conjunction with the pan-birmingham Respiratory Clinical Network and refined after discussion with colleagues representing the Birmingham Regional Severe Asthma Service (BRSAS) at HEFT, UHB and Sandwell and West Birmingham Hospitals. 6 NICE. Medtech innovation briefing [MIB90]. January
15 6 Implementation This guidance is intended for general use by all staff and will be linked to the APC website. The guideline will be actively promoted in primary care. Within secondary care, Trusts will each have their own mechanism for promotion, which may include departmental teaching sessions to junior doctors, s to medical consultants, promotion via grand rounds and discussion with staff in other key departments (such as acute medicine). Inhaler technique education sessions run in local CCGs for non-medical staff will also be used as an opportunity to distribute and promote the guideline. 7 Application of the Guideline The guideline applies to patients with asthma at all HEFT, Sandwell and UHBFT secondary care sites, and to Cross-City, Sandwell/West Birmingham, Solihull and South Central CCGs. Key beneficiaries will be patients, local CCGs and respiratory departments, as this is where cost savings and efficiency gains will be most apparent. Implementation should be by all staff seeing patients with asthma. 8 Launch and Implementation Plan for Clinical Guidelines The asthma and COPD guidelines will be launched together in the spring of The launch will be supported by a series of promotional events for healthcare professionals. Provision of information for patients will be in line with the requirements of the Accessible Information Standard August
16 9 Appendices: 9.1 Appendix 1: Plan on a Page Appendix 1 - Plan on a Page.pdf 16
17 17
18 18
19 9.2 Appendix 2: Step down Full guidance document: Updated BCC CCG step down guidance v 19

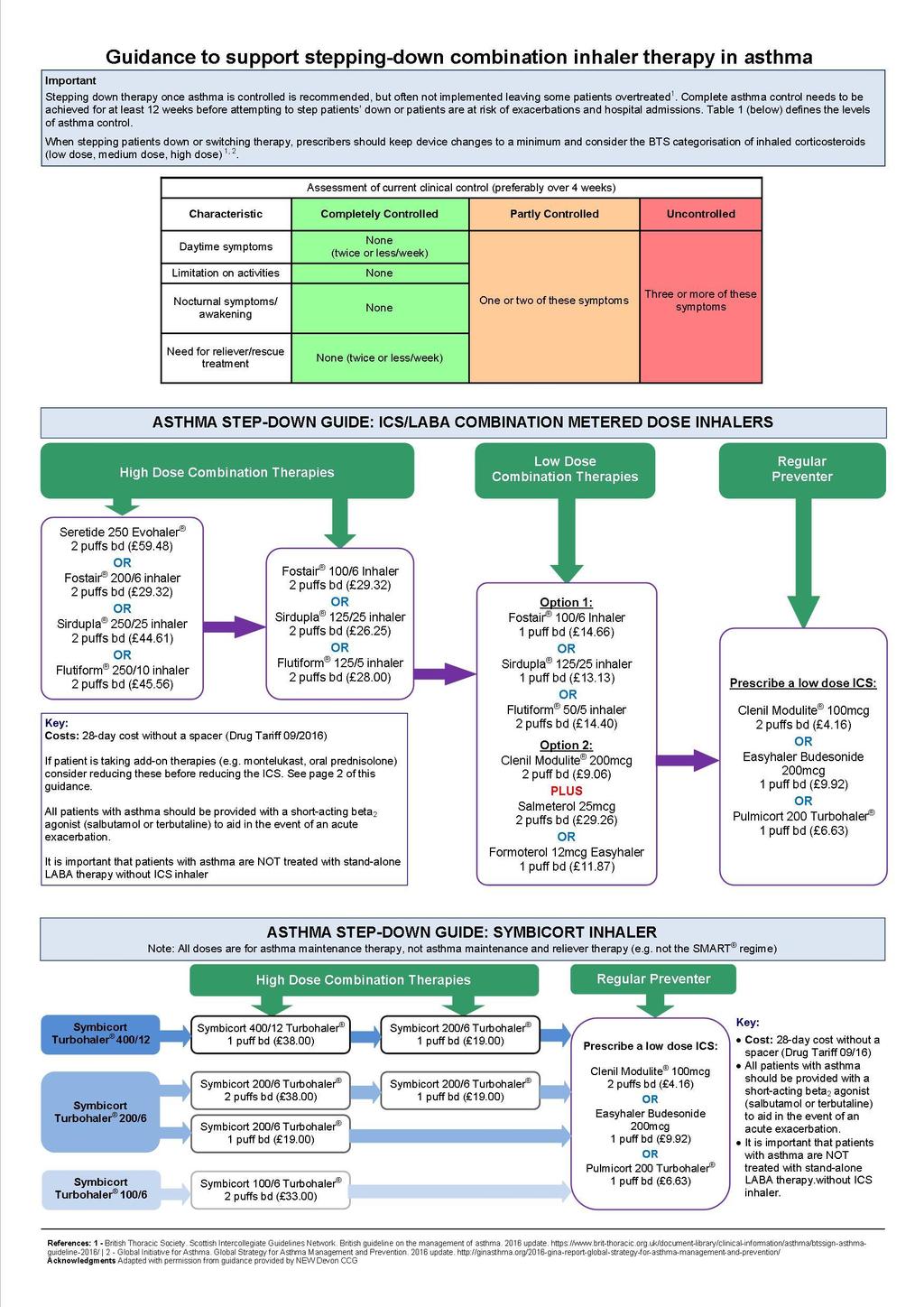
20 Guidance to support stepping-down combination inhaler therapy in asthma: Important Stepping down therapy once asthma is controlled is recommended, but often not implemented leaving some patients overtreated 1. Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients down or patients are at risk of exacerbations and hospital admissions. Table 1 (below) defines the levels of asthma control. When stepping patients down or switching therapy, prescribers should keep device changes to a minimum and consider the BTS categorisation of inhaled corticosteroids (low dose, medium dose, high dose) 1, 2. What do the guidelines say about stepping-down? The BTS/SIGN guidance 1 should be used to treat patients at the step most appropriate to their severity of asthma. The decision to step-down therapy should be jointly made between the clinician and the patient. Reductions should be considered every three months, but only if patients have complete asthma control 1,2. When reducing inhaled corticosteroids (ICS) clinicians should remember that patients deteriorate at different rates. Stepping down ICS doses by 25-50% at three month intervals is reasonable for most patients 1,2. BTS guidance advises that combination devices may increase adherence to therapy 1. LABA should only be started in patients who are already on ICS and the effect properly monitored before considering dose increase 3 as per MHRA guidance. Choice of preparation should be made based on severity of asthma and assessment of device technique. If control is maintained for three months after stepping-down, further reductions in the ICS should be attempted until a low dose is reached, when the LABA may be stopped 2. Once a day inhaled corticosteroids at the same total daily dose can be considered if good control is established 1. Characteristic Daytime symptoms Limitation on activities Nocturnal symptoms/awakening Need for reliever/rescue treatment Table 1: LEVELS OF ASTHMA CONTROL 2 Assessment of current clinical control (preferably over 4 weeks) Completely Controlled None (twice or less/week) None None None (twice or less/week) Partly Controlled One or two of these symptoms Uncontrolled Three or more of these symptoms References: 1. British Thoracic Society. Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma update Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention update Medicines & Healthcare products Regulatory Agency. Asthma Long-acting β2 agonists: use and safety. MHRA guidance Acknowledgments Adapted with permission from guidance provided by NEW Devon CCG 20
21 Asthma Step-down Guide: ICS/LABA combination metered dose inhalers Note: Seretide is formulary option for paediatric patients only. There is, however, a large cohort of legacy patients who should only be switched to an alternative preparation after clinical review and device assessment. All doses are for asthma maintenance therapy, not asthma maintenance and reliever therapy (i.e. not the MART regime) High Dose Combination Therapies Low Dose Combination Therapies Regular Preventer Seretide 250 Evohaler 2 puffs bd ( 59.48) OR Fostair 200/6 inhaler 2 puffs bd ( 29.32) OR Sirdupla 250/25 inhaler 2 puffs bd ( 44.61) OR Flutiform 250/10 inhaler 2 puffs bd ( 45.56) Key: Costs: 28-day cost without a spacer (Drug Tariff 09/2016) Fostair 100/6 Inhaler 2 puffs bd ( 29.32) OR Sirdupla 125/25 inhaler 2 puffs bd ( 26.25) OR Flutiform 125/5 inhaler 2 puffs bd ( 28.00) If patient is taking add-on therapies (e.g. montelukast, oral prednisolone) consider reducing these before reducing the ICS. See page 2 of this guidance. All patients with asthma should be provided with a short-acting beta 2 agonist (salbutamol or terbutaline) to aid in the event of an acute exacerbation. It is important that patients with asthma are NOT treated with stand-alone LABA therapy without ICS inhaler Option 1: Fostair 100/6 Inhaler 1 puff bd ( 14.66) OR Flutiform 50/5 inhaler 2 puffs bd ( 14.40) Option 2: Clenil Modulite 200mcg 2 puff bd ( 9.06) PLUS Salmeterol 25mcg; 2 puffs bd ( 29.26) OR Formoterol 12mcg Easyhaler; 1 puff bd ( 11.87) Prescribe a low dose ICS: Clenil Modulite 100mcg 2 puffs bd ( 4.16) OR Easyhaler Budesonide 200mcg 1 puff bd ( 9.92) OR Pulmicort 200 Turbohaler 1 puff bd ( 6.63) 21
22 Asthma Step-down Guide Symbicort Turbohaler Note: all doses are for asthma maintenance therapy, not asthma maintenance and reliever therapy (e.g. not the SMART regime) High Dose Combination Therapies Regular Preventer Symbicort Turbohaler 400/12 Symbicort 400/12 Turbohaler 1 puff bd ( 38.00) Symbicort 200/6 Turbohaler 1 puff bd ( 19.00) Symbicort Turbohaler 200/6 Symbicort Turbohaler 100/6 Symbicort 200/6 Turbohaler 2 puffs bd ( 38.00) Symbicort 200/6 Turbohaler 1 puff bd ( 19.00) Symbicort 100/6 Turbohaler 2 puffs bd ( 33.00) Symbicort 200/6 Turbohaler 1 puff bd ( 19.00) Prescribe a low dose ICS: Clenil Modulite 100mcg 2 puffs bd ( 4.16) OR Easyhaler Budesonide 200mcg 1 puff bd ( 9.92) OR Pulmicort 200 Turbohaler 1 puff bd ( 6.63) Key: Cost: 28-day cost without a spacer (Drug Tariff 09/16) All patients with asthma should be provided with a short-acting beta 2 agonist (salbutamol or terbutaline) to aid in the event of an acute exacerbation. It is important that patients with asthma are NOT treated with stand-alone LABA therapy without ICS inhaler. 22
23 Plan on a page (see below): Asthma Step Down.pdf 23
24 24

25 9.3 Appendix 3: Management of acute asthma in General Practice 25
Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs
 Step Down guidance Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs Important Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients
Step Down guidance Stepping-down combination ICS/LABA asthma inhaler therapy: Adults 18yrs Important Complete asthma control needs to be achieved for at least 12 weeks before attempting to step patients
ASTHMA TREATMENT GUIDE (ADULTS)
") ASTHMA TREATMENT GUIDE (ADULTS) The BTS/SIGN guideline provides a wide range of information and guidance on the treatment of patients with asthma. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/
ASTHMA TREATMENT GUIDE (ADULTS) The BTS/SIGN guideline provides a wide range of information and guidance on the treatment of patients with asthma. https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-asthma-guideline-2016/
CHARM ASTHMA TREATMENT GUIDELINE
 NHS City and Hackney Prescribing Guidelines Adults ( 12 years of age) CHARM ASTHMA TREATMENT GUIDELINE Written by: Hetal Dhruve (Specialist Respiratory Pharmacist, City and Hackney CCG) Checked by: Prof
NHS City and Hackney Prescribing Guidelines Adults ( 12 years of age) CHARM ASTHMA TREATMENT GUIDELINE Written by: Hetal Dhruve (Specialist Respiratory Pharmacist, City and Hackney CCG) Checked by: Prof
Adult Summary flowchart for Asthma Switch and Step Down to preferred inhaler choices
 HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
HVCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to preferred
Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred inhaler choices
 ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
ENHCCG Adult Asthma Switch and Step Down Algorithms - Approved by Hertfordshire Medicines Management Committee June 2016 Page 1 of 6 Adult Summary flowchart for Asthma Switch and Step Down to ENHCCG preferred
Position within the Organisation
 ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
ASTHMA TREATMENT GUIDELINES Document Description Document Type Service Application Guidelines All healthcare professionals(hcps) caring for patients with asthma Version 4.0 Ratification date September
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Asthma Treatment Guideline for Adults (aged 17 and over)
") Asthma Treatment Guideline for Adults (aged 17 and over) Sharon Andrew MLCSU January 2019 (Review date 0 January 2022) VERSION CONTROL. Please access via the LMMG website to ensure that the correct version
Asthma Treatment Guideline for Adults (aged 17 and over) Sharon Andrew MLCSU January 2019 (Review date 0 January 2022) VERSION CONTROL. Please access via the LMMG website to ensure that the correct version
ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12
 North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
North Hampshire CCG Asthma Prescribing Guidelines June 2015 ASTHMA PRESCRIBING GUIDELINES FOR ADULTS AND CHILDREN OVER 12 These guidelines are based on the British Thoracic Society (BTS) and Scottish Intercollegiate
Include patients: with a confirmed diagnosis of asthma who have been free of asthma symptoms for 3 months or more.
 Corby Clinical Commissioning Group Kettering General Hospital NHS Trust Nene Clinical Commissioning Group rthampton General Hospital NHS Trust rthamptonshire Healthcare Foundation Trust Stepping down asthma
Corby Clinical Commissioning Group Kettering General Hospital NHS Trust Nene Clinical Commissioning Group rthampton General Hospital NHS Trust rthamptonshire Healthcare Foundation Trust Stepping down asthma
Stepping down asthma treatment guidelines
 Stepping down asthma treatment guidelines The potential for inhaled corticosteroids (ICS) to cause dose-related side-effects has led to asthma management guidelines recommending a dose reduction once asthma
Stepping down asthma treatment guidelines The potential for inhaled corticosteroids (ICS) to cause dose-related side-effects has led to asthma management guidelines recommending a dose reduction once asthma
Prescribing guidelines: Management of COPD in Primary Care
 Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) TREATMENT GUIDELINES Document Description Document Type Service Application Version Guidelines All healthcare professionals(hcps) caring for patients with asthma
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE
 BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE December 2014 Review Date: December 2017 Bulletin 206 : DuoResp Spiromax 160 / 4.5 and 320 / 9 budesonide & formoterol dry powder inhaler JPC Recommendations
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE December 2014 Review Date: December 2017 Bulletin 206 : DuoResp Spiromax 160 / 4.5 and 320 / 9 budesonide & formoterol dry powder inhaler JPC Recommendations
Respiratory Inhalers. Identification Guide Version 3
 Respiratory Inhalers Identification Guide Version 3 This booklet has been prepared by NHSGGC Medicines Information. Endorsed by NHSGGC Respiratory Managed Clinical Network, February 2017. Designed by Medical
Respiratory Inhalers Identification Guide Version 3 This booklet has been prepared by NHSGGC Medicines Information. Endorsed by NHSGGC Respiratory Managed Clinical Network, February 2017. Designed by Medical
Algorithm for the use of inhaled therapies in COPD
 Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Chapter 3: Respiratory System (7 th Edition)
") Chapter 3: Respiratory System (7 th Edition) The Sheffield respiratory guidelines (April 2015) have been removed from the intranet. This is because the COPD section has been superseded by the COPD treatment
Chapter 3: Respiratory System (7 th Edition) The Sheffield respiratory guidelines (April 2015) have been removed from the intranet. This is because the COPD section has been superseded by the COPD treatment
Guide to Inhaled Treatment Choices
 Guide to Inhaled Treatment Choices Note: this is guidance only, it is important to consider which device is best suited to the patient. This may NOT be the first line choice (but should be on the joint
Guide to Inhaled Treatment Choices Note: this is guidance only, it is important to consider which device is best suited to the patient. This may NOT be the first line choice (but should be on the joint
Guide to Inhaled Treatment Choices
 Guide to Inhaled Treatment Choices Note: this is guidance only, it is important to consider which device is best suited to the patient. This may NOT be the first line choice (but should be on the joint
Guide to Inhaled Treatment Choices Note: this is guidance only, it is important to consider which device is best suited to the patient. This may NOT be the first line choice (but should be on the joint
Medicines Management of Chronic Obstructive Pulmonary Disease (COPD)
") Medicines Management of Chronic Obstructive Pulmonary Disease (COPD) (Chronic & Acute) Guidelines for Primary Care Guideline Authors: Shaneez Dhanji (Wandsworth CCG) Samantha Prigmore (St George s Hospital)
Medicines Management of Chronic Obstructive Pulmonary Disease (COPD) (Chronic & Acute) Guidelines for Primary Care Guideline Authors: Shaneez Dhanji (Wandsworth CCG) Samantha Prigmore (St George s Hospital)
Algorithm for the use of inhaled therapies in COPD Version 2 May 2017
 Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Progress, Paediatrics and Protocols. Dr Andy Powell Dr Lesley Ayling West Hampshire CCG
 Progress, Paediatrics and Protocols Dr Andy Powell Dr Lesley Ayling West Hampshire CCG Progress Solutions CQUIN discharge bundle (including personal action plan), specialist review, immediate management
Progress, Paediatrics and Protocols Dr Andy Powell Dr Lesley Ayling West Hampshire CCG Progress Solutions CQUIN discharge bundle (including personal action plan), specialist review, immediate management
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
beclometasone 100 MDI 2 puffs twice a day (recently changed to non CFC (Clenil Modulite))
)") Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Case 1 Mr Thomson, a 32 year old asthmatic who is well known to you comes into your pharmacy. He is known to have a best peak flow of 640 L/min. He tells you that over the last few weeks he has been wakening
Wirral COPD Prescribing Guidelines
 Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
Asthma Guidelines and Pharmacological Treatment. Dr James Wilkinson
 Asthma Guidelines and Pharmacological Treatment Dr James Wilkinson Asthma is a common disease in the UK 5.4 million people in the UK are currently receiving treatment for asthma: 4.3 million adults (1
Asthma Guidelines and Pharmacological Treatment Dr James Wilkinson Asthma is a common disease in the UK 5.4 million people in the UK are currently receiving treatment for asthma: 4.3 million adults (1
BNF CHAPTER 3: RESPIRATORY
 3.1 BRONCHODILATORS BNF CHAPTER 3: RESPIRATORY 3.1.1.1 SELECTIVE BETA 2 -AGONISTS Short acting Salbutamol 100 micrograms/actuation aerosol inhaler 100 micrograms/actuation breath-actuated (e.g., Easi-Breathe
3.1 BRONCHODILATORS BNF CHAPTER 3: RESPIRATORY 3.1.1.1 SELECTIVE BETA 2 -AGONISTS Short acting Salbutamol 100 micrograms/actuation aerosol inhaler 100 micrograms/actuation breath-actuated (e.g., Easi-Breathe
Medicines Optimisation Team Standard Operating Procedure for Audit: High Dose Inhaled Corticosteroids
 Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
THEOPHYLLINE WITH INHALED CORTICOSTEROIDS (TWICS) TRIAL SELF MANAGMENT / ACTION PLANS GENUAIR INHALERS: POTENTIAL SAFETY ISSUE
 TRIAL SELF MANAGMENT / ACTION PLANS GENUAIR INHALERS: POTENTIAL SAFETY ISSUE") I S S U E 4 M A R C H / A R P I L 2 0 1 6 Endorsed December 2014 I N S I D E T H I S I S S U E : Theophylline with Inhaled Corticosteroids (TWICS) Trial Genuair Inhaler: Potential Safety Issue 1 Self Management
I S S U E 4 M A R C H / A R P I L 2 0 1 6 Endorsed December 2014 I N S I D E T H I S I S S U E : Theophylline with Inhaled Corticosteroids (TWICS) Trial Genuair Inhaler: Potential Safety Issue 1 Self Management
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
3. Respiratory System
 1 3. Respiratory System Also see Appendix 3A Guidance on Management of Also see Appendix 3B Preferred Inhaler Devices for Adults Also see Appendix 3C Preferred Inhaler Devices for Adolescents (12-18 years)
1 3. Respiratory System Also see Appendix 3A Guidance on Management of Also see Appendix 3B Preferred Inhaler Devices for Adults Also see Appendix 3C Preferred Inhaler Devices for Adolescents (12-18 years)
500 micrograms/dose Turbohaler dry powder device 500 micrograms/ml injection. 12 micrograms/dose Turbohaler dry powder device
 3.1 BRONCHODILATORS 3.1.1.1 SELECTIVE BETA 2 -AGONISTS Short acting Salbutamol Terbutaline 100 micrograms/actuation aerosol inhaler 100 micrograms/actuation breath-actuated e.g. Easi-Breathe 200 micrograms/dose
3.1 BRONCHODILATORS 3.1.1.1 SELECTIVE BETA 2 -AGONISTS Short acting Salbutamol Terbutaline 100 micrograms/actuation aerosol inhaler 100 micrograms/actuation breath-actuated e.g. Easi-Breathe 200 micrograms/dose
fluticasone furoate / vilanterol 92/22, 184/22 micrograms inhalation powder (Relvar Ellipta ) SMC No. (966/14) GlaxoSmithKline UK
 SMC No. (966/14) GlaxoSmithKline UK") fluticasone furoate / vilanterol 92/22, 184/22 micrograms inhalation powder (Relvar Ellipta ) SMC No. (966/14) GlaxoSmithKline UK 09 May 2014 The Scottish Medicines Consortium (SMC) has completed its assessment
fluticasone furoate / vilanterol 92/22, 184/22 micrograms inhalation powder (Relvar Ellipta ) SMC No. (966/14) GlaxoSmithKline UK 09 May 2014 The Scottish Medicines Consortium (SMC) has completed its assessment
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Asthma - An update BTS Asthma Guidelines 2016
 Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Asthma - An update BTS Asthma Guidelines 2016 Dr Ian Clifton Overview Diagnosis Supported self-management Non-pharmacological management Drugs / inhaled therapy Difficult asthma services Case discussions
Medicines Management of Asthma
 Wandsworth Borough Team Medicines Management of Guidelines for Primary Care September 2011 Version 1 Guideline Authors: Shaneez Dhanji (Wandsworth borough) Reena Rabheru-Dodhy (Sutton & Merton borough)
Wandsworth Borough Team Medicines Management of Guidelines for Primary Care September 2011 Version 1 Guideline Authors: Shaneez Dhanji (Wandsworth borough) Reena Rabheru-Dodhy (Sutton & Merton borough)
SABA: VENTOLIN EVOHALER (SALBUTAMOL) SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA
 SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA") COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Dose. Route. Units. Given. Dose. Route. Units. Given
 Chapter 4 Respiratory Andrew Stanton SALBUTAMOL (in acute asthma) 5 in acute asthma Nebulised (driven by oxygen not air) 4 6 hourly In acute severe asthma not responding to initial treatment or in life-threatening
Chapter 4 Respiratory Andrew Stanton SALBUTAMOL (in acute asthma) 5 in acute asthma Nebulised (driven by oxygen not air) 4 6 hourly In acute severe asthma not responding to initial treatment or in life-threatening
PCRS-UK briefing document Asthma guidelines. November 2017
 PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
PCRS-UK briefing document Asthma guidelines November 2017 1 1. Background The Scottish Intercollegiate Guidelines Network (SIGN) and British Thoracic Society (BTS) have been collaborating on producing
The clinical effectiveness and costeffectiveness. treatment of chronic asthma in children under the age of 12 years
 The clinical effectiveness and costeffectiveness of corticosteroids for the treatment of chronic asthma in children under the age of 12 years Submission of evidence from AstraZeneca UK Ltd regarding the
The clinical effectiveness and costeffectiveness of corticosteroids for the treatment of chronic asthma in children under the age of 12 years Submission of evidence from AstraZeneca UK Ltd regarding the
Why Asthma Still Kills The National Review of Asthma Deaths (NRAD)
") APPROVED FINAL VERSION NHS Protect Why Asthma Still Kills The National Review of Asthma Deaths (NRAD) Summary of Recommendations for GP Practices and Community Pharmacies Author: Anne Henry Contact: anne.henry@nhs.net
APPROVED FINAL VERSION NHS Protect Why Asthma Still Kills The National Review of Asthma Deaths (NRAD) Summary of Recommendations for GP Practices and Community Pharmacies Author: Anne Henry Contact: anne.henry@nhs.net
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
NHS Dumfries & Galloway Triple therapy in COPD patients over 16 years
 Title of Project: NHS Dumfries & Galloway Triple therapy in COPD patients over 16 years 1 Reason for the review Respiratory prescribing is long term and can be costly. Appropriate choice and use of inhaled
Title of Project: NHS Dumfries & Galloway Triple therapy in COPD patients over 16 years 1 Reason for the review Respiratory prescribing is long term and can be costly. Appropriate choice and use of inhaled
Putting NICE guidance into practice. Resource impact report: Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Putting NICE guidance into practice Resource impact report: Asthma: diagnosis, monitoring and chronic asthma management (NG80) Published: November 2017 Summary This report focuses on the recommendations
Putting NICE guidance into practice Resource impact report: Asthma: diagnosis, monitoring and chronic asthma management (NG80) Published: November 2017 Summary This report focuses on the recommendations
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Summary of Lothian Joint Formulary Amendments
 Summary of Lothian Joint Formulary Amendments The purpose of this summary is to detail the main changes to the LJF sections and provide additional information on the reasons for some of the changes. The
Summary of Lothian Joint Formulary Amendments The purpose of this summary is to detail the main changes to the LJF sections and provide additional information on the reasons for some of the changes. The
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
A primary care perspective on the new British asthma guideline
 A primary care perspective on the new British asthma guideline Bronwen Thompson discusses the revisions to the BTS/SIGN guideline with Dr Hilary innock This guideline update 1 is significant. It builds
A primary care perspective on the new British asthma guideline Bronwen Thompson discusses the revisions to the BTS/SIGN guideline with Dr Hilary innock This guideline update 1 is significant. It builds
Please also see section on Drugs used in substance dependence for patients with established chemical dependence
 Respiratory System Algorithm for the selection of the most appropriate inhaler device for patients with chronic stable asthma Information on Inhaler devices Devices β 2 agonist bronchodilators Antimuscarinic
Respiratory System Algorithm for the selection of the most appropriate inhaler device for patients with chronic stable asthma Information on Inhaler devices Devices β 2 agonist bronchodilators Antimuscarinic
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Respiratory Health. Asthma and COPD
 Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
Respiratory Health Asthma and COPD Definition of asthma Working definition by AAH 2014: Chronic lung disease Can be controlled not cured Large variation in lung function Large variation in respiratory
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
Not available 100/6mcg 2 BD formoterol (Fostair MDI) 100/6mcg 33
 100/6mcg 33") COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP FLUTICASONE FUROATE/VILANTEROL COMBINATION INHALER - ASTHMA Policy agreed by Vale of York CCG (date) Drug, Treatment, Device name Fluticasone
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP FLUTICASONE FUROATE/VILANTEROL COMBINATION INHALER - ASTHMA Policy agreed by Vale of York CCG (date) Drug, Treatment, Device name Fluticasone
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
What s new in Asthma? Dr Alexandra Nanzer-Kelly Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Asthma is an inflammatory disease Relaxed smooth muscles Air trapped in alveoli Tightened
Scottish Medicines Consortium
 Scottish Medicines Consortium montelukast 10mg tablets (Singulair ) No. (185/05) Merck, Sharp & Dohme Ltd (MSD) New indication: for asthmatic patients in whom montelukast is indicated in asthma, montelukast
Scottish Medicines Consortium montelukast 10mg tablets (Singulair ) No. (185/05) Merck, Sharp & Dohme Ltd (MSD) New indication: for asthmatic patients in whom montelukast is indicated in asthma, montelukast
Technology appraisal guidance Published: 28 November 2007 nice.org.uk/guidance/ta131
 Inhaled corticosteroids for the treatment of chronic asthma in children under the age of 12 years Technology appraisal guidance Published: 28 November 2007 nice.org.uk/guidance/ta131 NICE 2018. All rights
Inhaled corticosteroids for the treatment of chronic asthma in children under the age of 12 years Technology appraisal guidance Published: 28 November 2007 nice.org.uk/guidance/ta131 NICE 2018. All rights
Beclometasone dipropionate (BDP) Prophylactic management of mild, moderate or severe asthma in adults
 Prophylactic management of mild, moderate or severe asthma in adults") CLENIL MODULITE Beclometasone dipropionate (BDP) Prophylactic management of mild, moderate or severe asthma in adults Corticosteroids for the treatment of chronic asthma in adults and children aged 12
CLENIL MODULITE Beclometasone dipropionate (BDP) Prophylactic management of mild, moderate or severe asthma in adults Corticosteroids for the treatment of chronic asthma in adults and children aged 12
Inhaled corticosteroids for the treatment of chronic asthma in children under the age of 12 years. Issue date: November 2007
 Issue date: November 2007 Review date: November 2012 Inhaled corticosteroids for the treatment of chronic asthma in children under the age of 12 years NICE technology appraisal guidance 131 NICE technology
Issue date: November 2007 Review date: November 2012 Inhaled corticosteroids for the treatment of chronic asthma in children under the age of 12 years NICE technology appraisal guidance 131 NICE technology
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Address Comorbidities
 Greater Manchester COPD Management Plan Non-pharmacological management for ALL patients Smoking Cessation Annual Flu Vaccination Pulmonary Rehabilitation Increase daily activity Inhaler Technique Measure
Greater Manchester COPD Management Plan Non-pharmacological management for ALL patients Smoking Cessation Annual Flu Vaccination Pulmonary Rehabilitation Increase daily activity Inhaler Technique Measure
Inhaled Corticosteroids for the Treatment of Chronic Asthma in Adults & Adolescents aged 12 years & over
 Manufacturer Submission To The National Institute for Health and Clinical Excellence By GlaxoSmithKline UK Inhaled Corticosteroids for the Treatment of Chronic Asthma in Adults & Adolescents aged 12 years
Manufacturer Submission To The National Institute for Health and Clinical Excellence By GlaxoSmithKline UK Inhaled Corticosteroids for the Treatment of Chronic Asthma in Adults & Adolescents aged 12 years
NICE guideline Published: 29 November 2017 nice.org.uk/guidance/ng80
 Asthma: diagnosis, monitoring and chronic asthma management NICE guideline Published: 29 November 2017 nice.org.uk/guidance/ng80 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Asthma: diagnosis, monitoring and chronic asthma management NICE guideline Published: 29 November 2017 nice.org.uk/guidance/ng80 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Global Initiative for Asthma (GINA) What s new in GINA 2017?
 What s new in GINA 2017?") Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Getting Asthma treatment right. Dr David Cremonesini Specialist Pediatrician American Hospital
 Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
Getting Asthma treatment right Dr David Cremonesini Specialist Pediatrician American Hospital cdavid@ahdubai.com } Consultant Paediatrician from UK of 5.5 years } Speciality in Allergy / Asthma (PG Certificate)
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ASTRAZENECA v GLAXOSMITHKLINE
 CASE AUTH/1986/4/07 ASTRAZENECA v GLAXOSMITHKLINE Symbicort and Seretide cost comparisons AstraZeneca complained about cost comparisons made by GlaxoSmithKline between AstraZeneca s Symbicort (budesonide/formoterol)
CASE AUTH/1986/4/07 ASTRAZENECA v GLAXOSMITHKLINE Symbicort and Seretide cost comparisons AstraZeneca complained about cost comparisons made by GlaxoSmithKline between AstraZeneca s Symbicort (budesonide/formoterol)
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Ivax Pharmaceuticals UK Sponsor Submission to the National Institute for Health and Clinical Excellence
 Ivax Pharmaceuticals UK Sponsor Submission to the National Institute for Health and Clinical Excellence Clinical and cost-effectiveness of QVAR for the treatment of chronic asthma in adults and children
Ivax Pharmaceuticals UK Sponsor Submission to the National Institute for Health and Clinical Excellence Clinical and cost-effectiveness of QVAR for the treatment of chronic asthma in adults and children
GMMMG Asthma Formulary Inhaler Options August 2017
 Regular Preventer Beclometasone Beclometasone Beclometasone Brand name Qvar Easi-Breathe Clenil Modulite Easyhaler Device MDI MDI DPI Strengths 50 microgram 100 microgram 200 microgram Adult asthma 2 inhalations
Regular Preventer Beclometasone Beclometasone Beclometasone Brand name Qvar Easi-Breathe Clenil Modulite Easyhaler Device MDI MDI DPI Strengths 50 microgram 100 microgram 200 microgram Adult asthma 2 inhalations
Report generated from BNF provided by FormularyComplete (www.pharmpress.com). Accessed Formulary Status. TA Number. Section.
. Accessed Formulary Status. TA Number. Section.") Report generated from BNF provided by FormularyComplete (www.pharmpress.com). Accessed 16 02 2017 Title Formulary Status Section TA Number TA Link Annotation ACLIDINIUM BROMIDE bronchodilators ADRENALINE/EPINEPHRINE
Report generated from BNF provided by FormularyComplete (www.pharmpress.com). Accessed 16 02 2017 Title Formulary Status Section TA Number TA Link Annotation ACLIDINIUM BROMIDE bronchodilators ADRENALINE/EPINEPHRINE
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Developed By Name Signature Date
 Patient Group Direction 2155 version 2.0 Administration / Supply of Inhaled Salbutamol in Asthma by Registered Practitioners employed by Torbay and South Devon NHS Foundation Trust Date of Introduction:
Patient Group Direction 2155 version 2.0 Administration / Supply of Inhaled Salbutamol in Asthma by Registered Practitioners employed by Torbay and South Devon NHS Foundation Trust Date of Introduction:
Seretide 250mcg/125mcg Evohaler switch to Fostair 100/6 MDI in COPD.
 Seretide 250mcg/125mcg Evohaler switch to Fostair 100/6 MDI in COPD. Applies to HaRD CCG employed Pharmacists and Medicines Optimisation Technicians These protocols are produced by the NY&AWC MM team hosted
Seretide 250mcg/125mcg Evohaler switch to Fostair 100/6 MDI in COPD. Applies to HaRD CCG employed Pharmacists and Medicines Optimisation Technicians These protocols are produced by the NY&AWC MM team hosted
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
COPD RESOURCE PACK Section 5. Drug Treatment & Inhalers in Stable COPD
 COPD RESOURCE PACK Section 5 Drug Treatment & Inhalers in Stable COPD In this section: 1. Links to Fife Formulary 2. Pharmacological Management of Stable COPD 3. How to use a Metered Dose Inhaler 4. How
COPD RESOURCE PACK Section 5 Drug Treatment & Inhalers in Stable COPD In this section: 1. Links to Fife Formulary 2. Pharmacological Management of Stable COPD 3. How to use a Metered Dose Inhaler 4. How
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
APPENDIX 1 Printable point-of-care tables Asthma Action Plan Yellow Zone Formulation Table Region: Europe
 APPENDIX 1 Printable point-of-care tables Asthma Action Plan Yellow Zone Formulation Table Region: Europe Instructions: Print on 8.5 x14 (216 x 279 mm) paper (Legal size) Medication in Green Zone Change
APPENDIX 1 Printable point-of-care tables Asthma Action Plan Yellow Zone Formulation Table Region: Europe Instructions: Print on 8.5 x14 (216 x 279 mm) paper (Legal size) Medication in Green Zone Change
aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A.
 SMC No. (810/12) Almirall S.A.") aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A. 05 October 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
aclidinium 322 micrograms inhalation powder (Eklira Genuair ) SMC No. (810/12) Almirall S.A. 05 October 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
British Guideline on the Management of Asthma
 British Guideline on the Management of Asthma A national clinical guideline British Thoracic Society Scottish Intercollegiate Guidelines Network Revised edition November 2005 British Guideline on the Management
British Guideline on the Management of Asthma A national clinical guideline British Thoracic Society Scottish Intercollegiate Guidelines Network Revised edition November 2005 British Guideline on the Management
Pathway diagrams Annex F
 Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Bulletin Independent prescribing information for NHS Wales
 Bulletin Independent prescribing information for NHS Wales Respiratory disease September 2014 Respiratory diseases account for one in seven of all deaths in Wales the third largest cause of mortality for
Bulletin Independent prescribing information for NHS Wales Respiratory disease September 2014 Respiratory diseases account for one in seven of all deaths in Wales the third largest cause of mortality for
Better Living with Obstructive Pulmonary Disease A Patient Guide
 Better Living with Obstructive Pulmonary Disease A Patient Guide Second Edition November 2012 Queensland Health a Better Living with Chronic Obstructive Pulmonary Disease A Patient Guide is a joint project
Better Living with Obstructive Pulmonary Disease A Patient Guide Second Edition November 2012 Queensland Health a Better Living with Chronic Obstructive Pulmonary Disease A Patient Guide is a joint project
Scottish Medicines Consortium
 Scottish Medicines Consortium budesonide/formoterol 100/6, 200/6 turbohaler (Symbicort SMART ) No. (362/07) Astra Zeneca UK Limited 9 March 2007 (Issued May 2007) The Scottish Medicines Consortium (SMC)
Scottish Medicines Consortium budesonide/formoterol 100/6, 200/6 turbohaler (Symbicort SMART ) No. (362/07) Astra Zeneca UK Limited 9 March 2007 (Issued May 2007) The Scottish Medicines Consortium (SMC)
NHS Northern, Eastern and Western Devon Clinical Commissioning Group NHS South Devon and Torbay Clinical Commissioning Group
 NHS Northern, Eastern and Western Devon Clinical Commissioning Group NHS South Devon and Torbay Clinical Commissioning Group Inhaler technique and respiratory conditions Guidance Sheet 16 When diagnosed
NHS Northern, Eastern and Western Devon Clinical Commissioning Group NHS South Devon and Torbay Clinical Commissioning Group Inhaler technique and respiratory conditions Guidance Sheet 16 When diagnosed
Community Pharmacy Asthma Audit 2016/17. Contents
 Community Pharmacy Contents Community Pharmacy... 1 Executive Summary... 2 Introduction... 4 Background... 4 Method... 5 Results... 5 Section One: Community Pharmacy Guidelines Awareness and Training...
Community Pharmacy Contents Community Pharmacy... 1 Executive Summary... 2 Introduction... 4 Background... 4 Method... 5 Results... 5 Section One: Community Pharmacy Guidelines Awareness and Training...
Medicines Management Programme Inhaled Medicines for Chronic Obstructive Pulmonary Disease (COPD)
") Medicines Management Programme Inhaled Medicines for Chronic Obstructive Pulmonary Disease (COPD) Approved by Prof. Michael Barry, Clinical Lead, MMP. Date approved Version 1 July 2014 Date updated Version
Medicines Management Programme Inhaled Medicines for Chronic Obstructive Pulmonary Disease (COPD) Approved by Prof. Michael Barry, Clinical Lead, MMP. Date approved Version 1 July 2014 Date updated Version
Online supplementary material
 Online supplementary material Add-on long-acting β2-agonist (LABA) in a separate inhaler as asthma step-up therapy versus increased dose of inhaled corticosteroid (ICS) or ICS/LABA combination inhaler
Online supplementary material Add-on long-acting β2-agonist (LABA) in a separate inhaler as asthma step-up therapy versus increased dose of inhaled corticosteroid (ICS) or ICS/LABA combination inhaler
Choosing an inhaler for COPD made simple. Dr Simon Hart Castle Hill Hospital
 Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies
Choosing an inhaler for COPD made simple Dr Simon Hart Castle Hill Hospital 1 Declaration of interests I have received speaker fees, sponsorship to attend conferences, and funding for research from companies