Central Nervous System Tumors in Children. Dr.Mina Tajvidi
|
|
|
- Solomon George
- 5 years ago
- Views:
Transcription
1 Central Nervous System Tumors in Children. Dr.Mina Tajvidi
2 CNS Central nervous system (CNS) tumors account for 20% to 25% of all malignancies that occur in childhood(united States) The incidence is highest among children 0 to4 years (4.6 per 100,000 person-years) and lowest among 10- to 19-year-olds (3.7 per 100,000 person-years). Only 2% to 5% can be ascribed to a genetic predisposition [neurofibromatosis types 1 and 2, tuberous sclerosis, nevoid basal cell (Gorlin's) syndrome, the adenomatous polyposis syndromes, and Li-Fraumeni syndrome]
3 CNS An even smaller percentage can be attributed to ionizing radiation used for diagnostic or therapeutic purposes For the majority of patients, no predisposing factors can be identified, although many have been suggested, including viral agents, preand postnatal environmental exposures, and birth characteristics, such as weight and head circumference
4 survival * the 5-year relative survival rate is estimated at 72% for all CNS tumors occurring in the 0- to 19-year age
5 Radiotherapy for Pediatric Central Nervous System Tumors General Principles The planning and delivery of radiotherapy for children with CNS tumors is technically challenging For children younger than age 4 or 5 years, daily anesthesia will almost always be necessary
6 Long-Term Effects of Radiotherapy for Central Nervous System Tumors The quality of survival of children with brain tumors may be compromised by long-term sequelae The magnitude of the deficit depends most importantly on age at treatment, but many other host (e.g., NF-1 or not), tumor (e.g., location, hydrocephalus or not), and treatment factors (e.g., radiotherapy volume and dose, use of chemotherapy), the development of other deficits, such as behavioral difficulties related to the location of the tumor and/or surgery There is increasing evidence that intervention using cognitive or behavioral therapy or pharmacotherapy may be useful, and that this should start soon after treatment for best results Endocrine deficits are very common after radiotherapy
7 strategies A number of strategies have been devised in an attempt to minimize the long-term effects of treatment for pediatric brain tumors. These include the following
8 strategies Avoidance of radiotherapy altogether (e.g., in patients with lowgrade astrocytoma for whom surgery alone may be a good option) Delay to radiotherapy for young children (i.e., those younger than age 3 to 8 years) by the use of chemotherapy Use of focal rather than extended-field radiotherapy when evidence suggests that extended field (whole-brain, craniospinal) radiotherapy does not influence survival (e.g., ependymoma) Use of daily anesthesia and of improved immobilization techniques (e.g., rigid casts or a stereotactic frame for small-volume focal radiotherapy for all or part of the treatment) that allow the use of reduced margins around the target volume Use of image-based treatment planning using CT,magnetic resonance imaging (MRI) or positron emission tomography (PET) coregistration and better treatment-planning techniques that result in greater sparing of normal brain tissue (e.g., three-dimensional conformal radiation therapy [3DCRT] and intensity-modulated radiation therapy [IMRT])
9 strategies. Use of new radiation modalities (e.g., proton beams that allow even greater sparing of the surrounding normal brain and organs at risk) Reduction of the dose of radiotherapy (e.g., in patients with standard risk medulloblastoma for whom in the North American studies the dose for craniospinal irradiation has been reduced progressively from 35 to 36 Gy to 23.4 Gy and, in current studies, to 18 Gy) Use of smaller fraction sizes where appropriate (e.g., a fraction size of 1.5 Gy each day for patients with radiosensitive tumors such as germinoma). Use of hyperfractionated radiotherapy (HFRT) (e.g., as in the current European studies for standard risk medulloblastoma)
10 Radiation Dose and Dose-Fractionation Regimens The conventional daily fraction size for the treatment of most pediatric CNS tumors is 1.8 Gy typical dose-fractionation regimen is 54 Gy in 30 daily fractions of 1.8 Gy, which carries a very low risk of radionecrosis When treating a primary tumor of the spinal cord it is conventional to use a lower total dose (e.g., 50.4 Gy). It is also usual to reduce the radiotherapy dose for children younger than age 3 years to reduce the risk of neurocognitive deficits When treating radiosensitive tumors such as intracranial germinoma, radiotherapy may be delivered using a lower dose per fraction (e.g., 1.5 Gy) and lower total doses of 30 to 50 Gy When the target contains only a small volume of normal brain tissue, dose escalation may be feasible. HFRT may be a useful strategy in situations where dose escalation cannot be achieved safely using conventional fractionation.
11 Follow-Up During and After Radiotherapy These days nausea and vomiting secondary to treatment almost always can be prevented by the use of the 5HT-3 antagonists Headache is not common in children and should be investigated by physical examination for signs of raised intracranial pressure and by imaging as appropriate Steroids, if used, usually can be tapered by the third or fourth week of treatment Fatigue is a rather common symptom and is cumulative The neurologic status of the patient, especially coordination and gait disorders, may appear to worsen during the last weeks of treatment because of this. Children usually recover relatively quickly, however, and often can get back to their usual routine by 6 weeks to 2 months following completion of hormonal deficits, especially growth-hormone deficit secondary to inclusion of the hypothalamicâ pituitary axis and primary hypothyroidism when craniospinal irradiation (CSI) is delivered using photons
12 Specific Tumor Types Specific Tumor Types There are important differences between tumors seen in childhood and those occurring in adults In children, almost half of all tumors arise in the infratentorial compartment Low-grade astrocytic tumors as a group account for approximately one third to half of all CNS tumors, but medulloblastoma is the most common distinct entity High-grade gliomas, are much less common in children.
13 Astrocytic Tumors Diffusely infiltrating astrocytomas, Diffuse astrocytomas (WHO grade II), Anaplastic astrocytoma (WHO grade III), Glioblastoma multiforme (WHO grade IV) and variants Pilocytic astrocytoma (WHO grade I), Pleomorphic xanthoastrocytoma (surgery is usually curative) Desmoplastic cerebral astrocytoma of infancy(surgery is usually curative) Subependymal giant cell astrocytoma. (surgery is usually curative)
14 Low-Grade Astrocytomas (WHO Grades I and II) overall survival rates at 10 and 15 years as high as 80% to 100% Most LGA occurring in childhood are of one of two types: pilocytic astrocytoma and low-grade astrocytoma of diffuse or fibrillary type(pilocytic astrocytomas are designated as grade I, All other low-grade astrocytomas are designated as grade II) Pilocytic astrocytomas are the most common type in the pediatric age group, accounting for almost all of the LGA at certain sites (e.g., the anterior optic pathway, the cerebellum). Diffuse, or fibrillary, low-grade astrocytomas account for only approximately 15% of all LGA in children Symptoms and signs of raised intracranial pressure may be seen in patients with midline and cerebellar tumors. Patients with posterior fossa tumors may present with neck stiffness and a head tilt as a manifestation of raised intracranial pressure, causing tonsillar herniation, altitudinal diplopia, or spinal-accessory nerve irritation Seizures are present in as many as three quarters of patients with hemispheric lesions
15 Management of Low-Grade Astrocytomas: General Principles Some children with LGA may not require any tumor-specific treatment. These include, for example, patients with NF-1, as many as 15% of whom have optic pathway tumors(active intervention is reserved for patients who develop progressive disease that is symptomatic) Progression-free survival without treatment may be very good as well for patients with tectal lesions who present with hydrocephalus without localizing brainstem signs
16 Management of Low-Grade Astrocytomas: General Principles The common characteristics of these very indolent tumors are their small size (<1.5 or 2 cm) and the fact that on imaging they are hypodense/hypointense and nonenhancing. Close follow-up with regular MRI is essential to identify patients with progressive lesions as manifested by increasing size and/or enhancement with gadolinium. Treatment (usually radiotherapy but sometimes now surgery) at the time of progression is associated with a high probability of long-term tumor control. If in doubt, a period of surveillance generally will be an acceptable initial approach Surgery is the mainstay of treatment for LGA Currently, complete resection is achieved in approximately 80% of cerebral, cerebellar, and spinal-cord tumors and 40% of diencephalic tumors.
17 Management of Low-Grade Astrocytomas: General Principles Children with LGA who undergo complete resection fare very well, with long-term disease-free and overall survival rates of 80% to 100%,postoperative adjuvant therapy is clearly not indicated. For children who undergo less than complete resection, the progression-free survival rate after surgery alone is less satisfactory, patients who had undergone subtotal resection (<1.5 cm residual tumor) were observed without adjuvant treatment, the 5-year progression-free survival rate was only 65%, However, the majority of patients can be salvaged with a second surgical resection and/or radiotherapy, overall survival at 5 years was 95% Consequently, the usual recommendation following subtotal resection will be close follow-up. The role of postoperative radiotherapy following lesser degrees of tumor resection remains unclear. In most series, the use of radiotherapy in this situation results in improved disease-free survival without any benefit in terms of overall survival
18 Management of Low-Grade Astrocytomas: General Principles Children with LGA who undergo complete resection fare very well, with long-term disease-free and overall survival rates of 80% to 100%,postoperative adjuvant therapy is clearly not indicated. For children who undergo less than complete resection, the progressionfree survival rate after surgery alone is less satisfactory, patients who had undergone subtotal resection (<1.5 cm residual tumor) were observed without adjuvant treatment, the 5-year progression-free survival rate was only 65%, However, the majority of patients can be salvaged with a second surgical resection and/or radiotherapy, overall survival at 5 years was 95% Consequently, the usual recommendation following subtotal resection will be close follow-up. The role of postoperative radiotherapy following lesser degrees of tumor resection remains unclear. In most series, the use of radiotherapy in this situation results in improved disease-free survival without any benefit in terms of overall survival

19 Algorithm for management
20 Radiotherapy in Low-Grade Astrocytomas Indications for Radiotherapy Radiotherapy is not indicated after complete resection. Radiotherapy may be indicated following incomplete resection in situations when tumor progression would compromise neurologic function (e.g., â œthreat to visionâ ). The clearest indication for radiotherapy is in patients with progressive and/or symptomatic disease that is unresectable
21 Radiotherapy Target Volume The radiotherapy target volume (the gross tumor volume or GTV) consists of the tumor bed and any macroscopic disease seen on MRI prior to treatment margins that were considered standard practice (i.e., 2 to 3 cm) are overly generous, particularly for the well-circumscribed pilocytic tumors; margins of 0.5 cm around the GTV as seen on T1 weighted gadolinium-enhanced images probably represent an adequate clinical target volume (CTV) for such tumors More generous margins of 1 to 1.5 cm around the GTV as seen on T2 weighted or FLAIR images are more appropriate for the more infiltrative diffuse fibrillary tumors. With thermoplastic masks it will be necessary to add an additional 3 to 4 mm around the CTV to arrive at the planning target volume (PTV), but the use of rigid or stereotactic localization systems may require an additional margin of only 1 to 2 mm
22 Radiotherapy Dose the recommendation for children with LGA would be a â œstandardâ dose of 50 to 54 Gy depending on the age of the child and the location of the tumor and its relationship to critical normal structures, such as the optic chiasm Radiotherapy Technique The radiotherapy technique to be used is that which provides homogeneous irradiation of the CTV and spares the greatest volume of normal tissue
23 Radiosurgery: may not be optimal for slowly growing tumors, particularly those comprised of tumor cells embedded in rather than displacing normal brain, as is the case for diffuse or fibrillary LGA Although such treatment may be of interest for part or even all of the treatment for pilocytic astrocytomas
24 Other options: Brachytherapy: Brachytherapy series necessarily select for smaller tumors, and there is no evidence that brachytherapy is a better treatment option than external-beam radiotherapy instillation of radioactive solutions such as phosphorus- 32 ( 32 P), yttrium-90 ( 90 Y), gold-198 ( 198 Au), and rhenium-186 ( 186 Re): Radioactive solutions may be useful in cystic LGA, particularly for patients with recurrent disease after radiotherapy in whom symptoms not infrequently relate more to the cyst than to the solid component of tumor
25 High-Grade Astrocytomas (WHO Grades III and IV) anaplastic astrocytoma Glioblastoma multiforme (GBM): is the most malignant astrocytic tumor Both AA and GBM may develop from diffuse or fibrillary astrocytomas (WHO grade II) High-grade astrocytomas (HGA) account for 5% of all CNS tumors in the pediatric age group Two thirds of HGA are located in the cerebral hemispheres
26 High-Grade Astrocytomas (WHO Grades III and IV) Patients with HGA usually present with symptoms of short duration (<6 months) that relate to the location of the lesion. maximal surgical resection compatible with a good neurologic outcome should be the goal for all patients, regardless of tumor location or histology A second surgical procedure should be considered if there is significant residual tumor after the first Postoperative radiotherapy is always indicated radiotherapy target volume is local with a GTV that consists of the tumor bed and any macroscopic residual disease plus a margin for the CTV of 1.5 to 2 cm
27 High-Grade Astrocytomas (WHO Grades III and IV) to consider a field-size reduction at 50 to 54 Gy to a CTV that consists of the tumor bed and any macroscopic residual disease plus a margin of 1 to 1.5 cm The dose to the CTV should be at least 54 Gy given over 6 weeks, but a dose of 59 to 60 Gy is more usual if feasible. There is no evidence that higher doses, as delivered using radiosurgery or stereotactic boosts, boosts with brachytherapy, or HFRT, result in improved outcomes, but newer approaches such as IMRT, which allows accelerated treatment to a component of the target volume (such as the GTV), may be of interest if only to decrease the overall treatment time. Chemotherapy: The role of chemotherapy remains to be defined There have been few phase III randomized trials of chemotherapy in HGA inchildren
28 High-Grade Astrocytomas (WHO Grades III and IV) Off study it may be difficult to make a recommendation with respect to adjuvant chemotherapy, although the poor prognosis, particularly for patients with macroscopic residual disease following surgery, usually is given as an argument for the use of the â œcurrent bestâ regimen The prognosis for children with HGA is poor Patients with lesions in the cerebral hemispheres fare better than those with tumors in other locations The prognosis for children with bithalamic lesions is particularly poor, and these patients are managed similarly to patients with diffuse intrinsic pontine tumors
29 High-Grade Astrocytomas (WHO Grades III and IV) infants with HGA appear to fare somewhat better than older children istologic grade (AA versus GBM) has not been shown consistently to affect outcome p53 overexpression and a high MIB-1 labeling index appear to identify patients with a particularly adverse prognosis who might be appropriate candidates for novel therapeutic approaches
30 Astrocytic Tumors. in Specific locations
31 Optic Pathway Gliomas approximately 5% of all CNS tumors in the pediatric age group the peak age incidence is between 2 and 6 years One third of patients have NF-1 tumors confined to the optic nerve(s), tumors of the optic chiasm with or without optic nerve involvement, and tumors that involve the hypothalamus or adjacent structures Optic nerve gliomas may involve one or both optic nerves. Bilateral involvement is pathognomonic of NF-1 the optic nerve tumors are incidental findings on routine imaging, and patients may remain asymptomatic with nonprogressive lesions over long periods; even spontaneous regressions are well documented
32 Optic Pathway Gliomas management of patients with optic nerve tumors will usually consist initially of close follow-up with regular ophthalmologic examinations and MRI, with active intervention, usually chemotherapy, reserved for patients with clear evidence of progression that is symptomatic Patients with unilateral optic nerve involvement may not have NF-1. They present most frequently with proptosis that may be relatively long standing On MRI, optic nerve tumors are usually relatively small and well circumscribed, with bright enhancement typical for pilocytic astrocytoma. Biopsy is not necessary to make a diagnosis Treatment usually, although not always, will be necessary, and the approach will depend on whether there is useful vision surgical resection will be the treatment of choice If useful vision is preserved, chemotherapy would be the preferred option for infants, very young children up to the age of 3 to 5 years, and for patients of all ages with NF-1 Radiotherapy could be considered for older children. Long-term tumor control approaches 100% with either modality(chemotherapy&radiotherapy)
33 Chiasmatic gliomas Chiasmatic gliomas are tumors that involve the optic chiasm and sometimes one or both optic nerves as well Patients typically present with loss of visual acuity and temporal field defects Biopsy is usually not necessary A period of surveillance is appropriate initial management, particularly for patients with NF-1 For patients without NF-1, especially those who present before the age of 5, Surgery is rarely an option for tumors in this location As for optic nerve tumors, chemotherapy usually will be the treatment of choice for infants and young children and for patients with NF-1 Radiotherapy is reserved for salvage postchemotherapy and for definitive treatment of older children without NF-1 Overall survival for patients with chiasmatic tumors is in the 90% to 100% range.
34 Posterior, or chiasmatic/hypothalamic, gliomas Posterior, or chiasmatic/hypothalamic, gliomas account for approximately 70% of all optic pathway gliomas in children They are typically rather large lesions that probably arise in the optic chiasm and extend to involve the hypothalamus They often fill the third ventricle, eventually causing hydrocephalus Early findings consist of nystagmus, impaired visual acuity, and visual field deficits; only later do patients present with increasing head circumference and/or symptoms and signs of raised intracranial pressure Treatment consists of CSF diversion, if necessary, and surgical resection particularly if tumor is growing exophytically into the basal cisterns In most patients, however, resection will be incomplete a period of surveillance is reasonable, although most patients will require adjuvant therapy
35 Posterior, or chiasmatic/hypothalamic, gliomas The treatment of choice for children younger than 5 and those with NF-1 usually will be chemotherapy, most often now using a carboplatin-based regimen The indications for radiotherapy are (a) progressive disease on chemotherapy for children younger than 10 years and (b) progressive disease at diagnosis or after surgery for older patients given to local fields to a dose of 45 to 50 Gy for younger children and of 50 to 54 Gy for those older than 5 years Overall, however, the results of treatment are less satisfactory for this group of patients than for those with anterior tumors Patients with NF-1are also at greater risk for Moyamoya syndrome, a progressive vaso-occlusive process involving the circle of Willis, This may be seen without radiotherapy when radiotherapy is used in patients with NF-1 it is important to include MR angiography as part of the regular follow-up imaging protocol and to intervene surgically if necessary to avoid a cerebrovascular accident
36 Brainstem Gliomas Tumors arising in the midbrain, pons, and medulla oblongata account for 10% to 15% of all CNS tumors in the pediatric age group improvements in neurosurgical techniques and perioperative care have made surgery not only feasible but the treatment of choice for all except the diffuse intrinsic tumors Focal tumors may occur at any level in the brainstem but are most frequently seen in the midbrain and medulla Signs and symptoms of raised intracranial pressure are uncommon except in patients with tumors arising in the tectal region that may cause aqueduct stenosis while still small.
37 Brainstem Gliomas patients with nonenhancing focal tumors in the tectal region who present with only hydrocephalus may do well without any treatment other than CSF diversionary procedures, Active intervention, including biopsy, is reserved for patients with clinical and radiologic evidence of progressive tumor Surgery is the treatment of choice for focal tumors at other locations that are surgically accessible (meaning either that they extend toward the surface of the brainstem laterally or at the floor of the fourth ventricle) and have imaging characteristics suggestive of low-grade histology

38
39 . ith bulky tumors and for patients with tumors in the medulla with lower cranial nerve deficits who are at high risk of developing postoperative complications. There are several treatment options for patients with surgically inaccessible focal lesions(conventional radiotherapy, HFRT and with interstitial irradiation using iodine-125, radiosurgery and stereotactic irradiation) with the advent of improved treatment planning and conformal radiotherapy treatment techniques, standard treatment for these lesions should be considered to be external-beam radiotherapy, using limited treatment volumes with a margin for the CTV of 0.5 cm, to a total dose of the order of 54 Gy given over 6 weeks, as for LGA at other locations
40 Dorsal exophytic tumors Dorsal exophytic tumors arise from the floor of the fourth ventricle They are usually large, filling the fourth ventricle, but do not invade the brainstem to any significant extent Surgery is the treatment of choice for dorsal exophytic tumors Ultrasound guidance is essential to achieve a maximal degree of tumor resectio the majority of children do well following surgery, and routine postoperative adjuvant therapy is not indicated Radiotherapy should be considered for the rare patient who is found to have a high-grade lesion or for patients with low-grade tumors who are found to have progressive disease in the early (0 to 9 months) postoperative period For patients whose tumors recur later, further surgery should be considered and radiotherapy should be reserved for those with inoperable disease The radiotherapy volume and dose should be similar to those used for LGA in other locations. the prognosis for patients wit
41 Cervicomedullary tumors Cervicomedullary tumors arise in the upper cervical cord and grow rostrally beyond the foramen magnum. Most are low-grade lesions Surgery is the treatment of choice no indication for routine postop
42 Diffuse intrinsic brainstem tumors Diffuse intrinsic brainstem tumors account for 70% to 80% of all brainstem tumors They arise in the pons and cause diffuse enlargement of the brainstem In contrast to the other types of brainstem tumors, the majority of diffuse intrinsic tumors are fibrillary astrocytomas with a propensity for malignant change and a very poor prognosis. Diffuse intrinsic tumors typically present with a short duration of symptoms (median 1 month) consisting of multiple, bilateral, cranial nerve deficits (especially VI and VII) as well as long tract signs and ataxia Only 10% of patients have hydrocephalus at diagnosis Surgery has no role in the management of patients with diffuse intrinsic lesions
43 Diffuse intrinsic brainstem tumors Even biopsy, a relatively nonmorbid procedure now, no longer is considered necessary because in the context of a typical clinical presentation, the MRI findings are characteristic and histology does not influence treatment Treated with conventional radiotherapy, the majority (75% or more) of patients with diffuse intrinsic tumors will improve clinically the progression-free interval is short (median <6 months) and survival is poor, with median survival <1 year and survival rates at 2 years <20%. Alternative approaches that use chemotherapy in combination with radiotherapy also have been disappointing New agents and novel chemotherapyâ radiotherapy combinations are under investigation by the pediatric cooperative groups in North America and Europe standard treatment for diffuse intrinsic brainstem tumors consists of radiotherapy given to the GTV as demonstrated by T2-weighted or FLAIR MRI with a margin for the CTV of 1 to 1.5 cm to a dose of 54 Gy given in 30
44 Low-Grade Astrocytomas of the Spinal Cord Intramedullary spinal cord tumors account for 3% to 6% of all CNS tumors in the pediatric age group About 60% are astrocytomas, the majority of which are of low histologic grade Patients typically present with symptoms of long duration, usually pain and motor deficits Resection is more difficult and less likely to be complete in patients with grade II astrocytoma because of the more infiltrative nature of these tumors and the absence of a plane of cleavage. Since outcome following complete or subtotal resection for LGA is very good, with long-term progression-free survival in the 70% to 90% range, routine postoperative adjuvant therapy is not indicated For children in whom complete or subtotal resection is not possible, options will be as for patients with LGA in other locations, that is, early second surgery or close follow-up with second surgery and/or radiotherapy at the time of progression
45 Low-Grade Astrocytomas of the Spinal Cord As for LGA in other locations, chemotherapy may be an alternative to radiotherapy for infants and very young children in this situation Immediate treatment would be indicated for patients with a highgrade astrocytoma The radiotherapy target volume for LGA usually will consist only of the solid portion of the tumor (including intratumoral cysts) with a margin for the CTV of 0.5 to 1 cm around the GTV The usual dose would be 50.4 Gy given in 28 daily fractions over approximately 6 weeks patients with high-grade lesions, most of whom will have had only a biopsy; a margin beyond the entire lesion of 1.5 cm would be more appropriate, The dose prescription usually will be as for low-grade lesions because of a substantial risk of morbidity at higher doses, but often chemotherapy will be given as wel
46 Ependymal Tumors Ependymomas account for 5% to 10% of all brain tumors in the pediatric age group with a predilection for infants and children younger than age 5 years two-thirds arise in the ependymal lining of the fourth ventricle gadolinium-enhanced MRI of the whole CNS and CSF cytology are essential components of the work-up for all patients, the risk of leptomeningeal seeding at diagnosis is at most 5% to 10%. The completeness of the surgical resection is the factor that has the greatest impact on the outcome of children with ependymoma, regardless of tumor location complete resection is possible in 70% to 85% of supratentorial ependymomas and in a similar percentage of spinal ependymomas complete resection is lower in patients with infratentorial ependymo
47 Ependymal Tumors Since residual disease is associated with a much worse outcome, â œsecond-lookâ surgery should be considered, if feasible, either after the realignment of structures that takes place following resection of an initially bulky tumor or after chemotherapy Postoperative radiotherapy is the standard of care for all children with ependymoma Radiotherapy for patients who have undergone complete resection: such a strategy results in worse disease-free and perhaps also overall survival and therefore can be considered acceptable only for (a) patients with ependymoma of the spinal cord who have undergone complete resection for whom disease-free survival in contemporary series approaches 100% and (b) selected patients with supratentorial ependymoma, such as those with intraventricular tumors or with extraventricular tumors that are solid and located in noneloquent areas and can be resectedwith a wider margin
48 Ependymal Tumors optimal radiotherapy target volume, dose, and dosefractionation schedule: using a GTV that is a composite of the tumor bed, based on preoperative imaging, and including any macroscopic residual disease, with a margin for the CTV of 1 cm the current standard is a dose of at least 54 to 55 Gy for lesions in the brain because failure most often occurs at the site of macroscopic residual disease, even higher doses may be desirable, HFRT has been explored in ependymoma for this reason
49 Ependymal Tumors The role of chemotherapy in ependymoma remains to be defined, Response rates to chemotherapy are quite poor In infants and very young children chemotherapy has been used because of the desire to delay or even avoid altogether radiotherapy local treatment consisting of the tumor bed and any macroscopic residual disease with a margin for the CTV of 1.5 cm is used for patients with localized disease; only patients with leptomeningeal seeding at diagnosis receive CSI As for ependymomas, the dose should be 54 to 55 Gy, with a boost to macroscopic residual disease, if feasible, to 59 to 60 Patients with leptomeningeal dissemination at diagnosis fare extremely poorly despite aggressive treatment with craniospinal radiotherapy and systemic chemotherapy.
50 Myxopapillary Ependymoma Myxopapillary ependymomas are slowly growing lesions almost always located in the conus-filum terminale region of the spinal cord They are the most common spinal cord tumor in this location Surgical resection is the treatment of choice If the tumor is not resected en bloc or if there is macroscopic residual tumor, postoperative radiotherapy should be used since outcome appears to be significantly worse in these situations The radiotherapy target volume is local (macroscopic disease plus a margin cephalad and caudad of 1.5 cm for the CTV) and the dose, 50.4 Gy Leptomeningeal seeding: patients should be treated with curative intent with CSI followed by a boost to the primary site
51 Choroid Plexus Tumors The WHO classification lists two different entities: choroid plexus papilloma (WHO grade I) and choroid plexus carcinoma (WHO grade III). Surgery is the treatment of choice for choroid plexus papillomas both for the primary lesion and for macroscopic metastatic deposits, if feasible Blood loss may be considerable The role of radiotherapy following incomplete resection is unclear(choroid plexus papillomas), close follow-up would seem
52 Choroid Plexus Tumors The WHO classification lists two different entities: choroid plexus papilloma (WHO grade I) and choroid plexus carcinoma (WHO grade III). Surgery is the treatment of choice for choroid plexus papillomas both for the primary lesion and for macroscopic metastatic deposits, if feasible Blood loss may be considerable The role of radiotherapy following incomplete resection is unclear(choroid plexus papillomas), close follow-up would seem
53 Ganglioglioma and Anaplastic Ganglioglioma Gangliogliomas are well-differentiated, slowly growing tumors composed of mature ganglion cells in combination with neoplastic glial cells WHO grade I or II. Although these tumors can arise anywhere within the CNS, most in children arise in the temporal region and typically present with seizures. Surgery is the treatment of choice The indications for radiotherapy would be as for patients with LGA, that is, for patients with progressive or recurrent disease that is not resectable postoperative radiotherapy: for patients with anaplastic gangliogliomas who have undergone less than complete resection
54 Pineal Parenchymal Tumors Pineal region tumors account for 2% to 8% of intracranial tumors in children. Approximately half are germ-cell tumors, onefourth to one-third are pineal parenchymal tumors, and most of the remainder are astrocytic tumors. WHO classification: pineoblastoma (WHO grade IV), pineocytoma (WHO grade II), and pineal parenchymal tumor of intermediate differentiation.
55 Pineoblastoma Pineoblastoma is a highly malignant primitive embryonal tumor Leptomeningeal spread is seen in as many as 50% of patients at diagnosis Surgery for lesions in the pineal region is particularly delicate, and complete resection is often not possible Postoperatively, older children are treated with CSI and chemotherapy, as for medulloblastoma and supratentorial primitive neuroectodermal tumor (S-PNETs) infants who are treated with chemotherapy without radiotherapy
56 Pineocytoma Pineocytoma is a slow-growing tumor They account for approximately half of pineal parenchymal tumors and in childhood most commonly occur in the teenage years Some will have symptoms of upper mesencephalic tegmental dysfunction (Parinaud's syndrome) Treatment consists of surgical resection If complete or subtotal resection is accomplished, the outcome is probably quite favorable even without any adjuvant treatment Following lesser degrees of resection, postoperative radiotherapy usually is recommended using local fields consisting of macroscopic residual disease, with a margin of 1 to 1.5 cm and a dose of 50 to 55 Gy over 6 weeks
57 Embryonal Tumors Embryonal tumors as a group are the second most common type of CNS tumor in the pediatric age group Ependymoblastoma Medulloblastoma, Supratentorial PNET. Medulloepithelioma, Atypical teratoid/rhabdoid tumor
58 Medulloblastoma Medulloblastoma accounts for 15% to 20% of all CNS tumors in the pediatric age group The median age at presentation is 6 years In the majority of cases the tumor arises in the cerebellar vermis and projects into the fourth ventricle Patients typically present with symptoms and signs of raised intracranial pressure, that is, headache and morning vomiting The frequency of spinal seeding at diagnosis is approximately 30% to 35%, and investigation at diagnosis must include a gadolinium-enhanced MRI of the spinal axis and CSF cytology.
59 Medulloblastoma The former should be obtained whenever possible preoperatively or else at least 2 to 3 weeks postoperatively to avoid misinterpretation resulting from artifactual changes seen in the later postoperative period CSF cytology: which should be obtained by lumbar puncture, often cannot be obtained preoperatively because of the presence of raised intracranial pressure and more commonly is obtained at approximately 3 weeks postoperatively Medulloblastoma is one of the few CNS tumors to spread outside the CNS (to lymph nodes, bone), although this is an uncommon event.
60
61 risk categories Patients are allocated to one of two risk categories: standard and high risk Standard risk: Those who have undergone complete or subtotal resection with <1.5 cm 2 of residual tumor and no evidence of CSF dissemination (M0) complete or near-total resection is accomplished in approximately 80% of cases two thirds of patients will be Standard risk and one third will be high risk.
62 Management of Standard-Risk Medulloblastoma Several treatment strategies designed to reduce the morbidity associated with the use of radiotherapy have been tested Until relatively recently, the standard of care for patients older than 3 years with standard-risk disease consisted of postoperative radiotherapy to the craniospinal axis to a dose of 35 to 36 Gy followed by a boost to the whole posterior fossa to a total dose of 54 to 55.8 Gy reduce the radiotherapy target volume to avoid supratentorial radiation produced disastrous results HFRT to a CSI dose of 36 Gy without chemotherapy reduced-dose CSI (23.4 Gy) followed by a boost to the posterior fossa to a total dose of 55.8 Gy in combination with systemic chemotherapy
63 Management of Standard-Risk Medulloblastoma reduced-dose (23.4 Gy) CSI in combination with weekly vincristine, followed by adjuvant systemic chemotherapy consisting of vincristine 1.5 mg/m 2, CCNU 75 mg/m 2, and cisplatin 75 mg/m 2 CCNU was replaced by cyclophosphamide such an approach is now considered to be the standard of care for children with standard-risk medulloblastoma in North America. Current studies are testing the safety of an even lower dose of CSI (18 Gy) in children aged 3 to 8 years and of a reduced-volume posterior fossa boost in children of all ages
64 Management of High-Risk Medulloblastoma for patients with residual disease, M0, it would be logical to consider using a radiotherapy dose to residual disease in the posterior fossa higher than the standard 55.8 Gy, and this may be feasible using stereotactic radiotherapy or 3D conformal technique Patients with M1 disease may do well using a standard CSI dose of 35 to 36 Gy; results for patients with M2, 3 disease remain quite poor, although the use of a higher radiotherapy dose (40 Gy CSI plus a boost of 5 Gy to macroscopic disease) produced excellent early results in POG 9031, approaching those for patients with less advanced disease. The hyperfractionated accelerated radiotherapy (HART) regimen under investigation by the U.K. group may prove to be an equally efficacious and safer way to deliver high dose CSI. Preradiotherapy chemotherapy may also be of interest in this group of patients preradiotherapy chemotherapy may allow identification of patients who do not respond and who might benefit from more aggressive chemotherapy, such as high-dose chemotherapy with stem cell rescue in combination with conventional radiotherapy, HFRT, or HART
65 Management of Medulloblastoma in Infants Medulloblastoma accounts for 20% to 40% of all CNS tumors in infants and carries a worse prognosis than in older children Medulloblastoma accounts for 20% to 40% of all CNS tumors in infants and carries a worse prognosis than in older children Infants with M0 disease who have undergone total resection may do well with chemotherapy alone Infants with M2â, 3 disease fare poorly and require more aggressive treatment such as high-dose chemotherapy with stem cell rescue and/or chemotherapy given using alternative routes of administration, such as intrathecal or intraventricular, with or without radiotherapy.
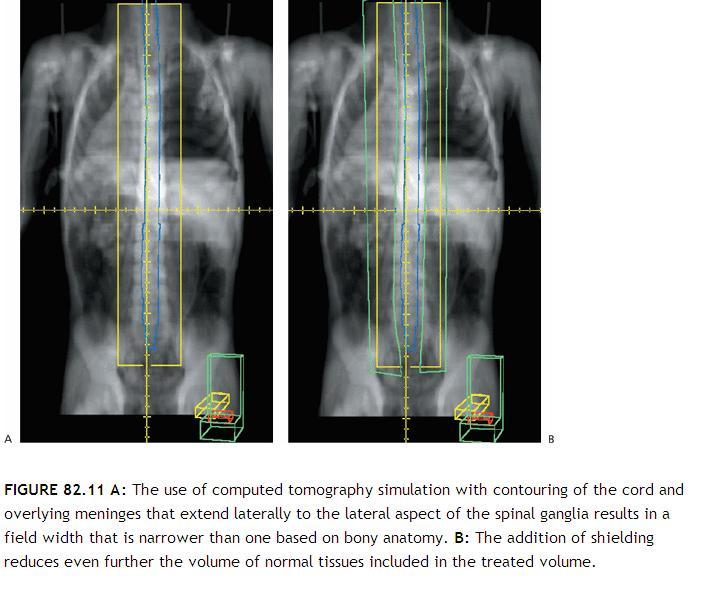
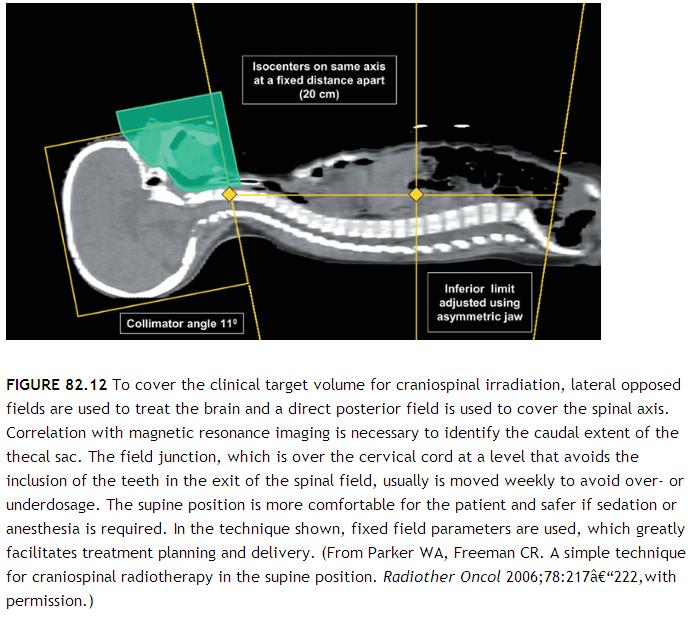
66 Radiotherapy for Medulloblastoma The CTV for CSI has an irregular shape that consists of the whole of the brain and spinal cord and overlying meninges Patients have traditionally received CSI in the prone position, but modern technology allows safe treatment in the supine position that in general is more comfortable CT simulation is invaluable for target volume definition for patients with medulloblastoma With current cataract surgical techniques, it is preferable to cover the target volume, keeping shielding of the lenses a secondary objective MRI is required to determine the lower limit of CTV for the spine field Traditionally the lower border of the spine field was placed at the lower border of the second sacral vertebra, but it is well documented that the lower border of the thecal sac can be as high as L5 or as low as S3 In the interest of both CTV coverage and normal tissue sparing it is important that the lower border be individualized according to the MRI findings.
67 .
68 Type & dose of energy In general, photons in the 6 to 10 MV range provide satisfactory coverage of the PTV Care is required if using electrons to treat the spinal axis The use of electrons to treat the spinal axis most often is justified by reduced acute gastrointestinal toxicity Because available data regarding late effects suggest that there may be little or no advantage to the use of electrons Traditionally, the entire posterior fossa has been treated to a total dose of 54 to 55.8 Gy
69 .
70 Radiotherapy for Medulloblastoma The optimal CTV for a reduced-volume posterior fossa remains to be defined, although it probably consists of a composite of any macroscopic residual tumor and the surgical bed plus a margin of 1 to 1.5 cm A few centers have reported their results using protons for treatment of medulloblastoma Delay to radiotherapy may be associated with poorer outcomes and CSI ideally should start within 28 days following surgery
71 Supratentorial Primitive Neuroectodermal Tumor S-PNETs account for <5% of all CNS tumors in the pediatric age group. The median age at presentation is 3 years Leptomeningeal seeding is present at diagnosis in up to 40% of patients, and MRI of the spinal axis and CSF cytology are mandatory prior to treatment. often using the same protocols as for high-risk medulloblastoma often using the same protocols as for high-risk medulloblastoma For now, the standard of care for children older than 3 years with S- PNETs without leptomeningeal spread consists of maximal surgical resection followed by postoperative radiotherapy (CSI plus a boost to doses similar to those used for high-risk medulloblastoma) followed by chemotherapy Experimental regimens such as preradiotherapy chemotherapy and high-dose chemotherapy with rescue are used in infants and young children and in patients with M2&3 disease
72 Atypical Teratoid/Rhabdoid Tumor highly malignant embryonal tumor unique to childhood outcome was very poor and the majority of patients died within 1 year of diagnosis Radiotherapy is an important component of treatment radiotherapy should be delivered early even in infants, and this may mean using a modified radiotherapy target volume (i.e., tumor bed and any macroscopic residual disease plus a margin Children older than 3 years should receive early CSI.
73 Germ Cell Tumors In the West, CNS germ cell tumors are relatively rare, accounting for 3% to 5% of all CNS tumors in the pediatric age group. They are more common in Asia The peak age incidence is 10 to 12 years. Boys are affected more frequently than girls, with a ratio of approximately 3:1 CNS germ cell tumors arise from primordial germ cells in structures about the third ventricle, with the region of the pineal gland being the most common site of origin, followed by the suprasellar region Nongerminomatous germ cell tumors (NGGCT) are the most common tumor type in the former area, and germinomas in the latter. Tumors in the pineal region cause obstruction to CSF flow at the aqueduct of Sylvius,
74 Germ Cell Tumors Another characteristic presentation of tumors in this region is Parinaud's syndrome as a result of dorsal midbrain compression Measurement of serum and CSF tumor markers is another essential part of the initial work-up In the past, many lesions arising in or about the third ventricle were treated without histologic confirmation of diagnosis all patients should undergo biopsy unless CSF and/or serum markers confirm the presence of a NGGCT (elevated AFP and/or B- hcg >100 IU/mL) or unless a histologic diagnosis is made by other means (e.g., CSF cytology) Occasionally complete resection will be possible; this would be a reasonable strategy for patients with NGGCT, particularly for mature teratomas if it can be accomplished without major morbidity because in that situation it would obviate the need for adjuvant treatm
75 Germinoma In the past, standard treatment for patients with germinoma was radiotherapy alone Whole ventricle irradiation alone may be acceptable for a patient with a unifocal lesion with no evidence of leptomeningeal dissemination a number of reasonable options for patients with unifocal germinoma without evidence of leptomeningeal dissemination. These include craniospinal radiotherapy, limited volume (whole-ventricle) radiotherapy alone, and chemotherapy followed by whole ventricle or local radiotherapy regardless of the target volume so that patients at increased risk for systemic failure (e.g., those with ventriculoperitoneal shunts) may be best treated with a combined chemotherapy&radiotherapy approach For patients with bi- or multifocal disease by imaging or by inference (for example, in a patient with a pineal region primary who has diabetes insipidus) and those with leptomeningeal spread at diagnosis, radiotherapy alone using CSI with boosts to macroscopic disease is certainly an option, although in North America a combination chemotherapy and radiotherapy regimen consisting of two cycles of chemotherapy followed by CSI followed by a boost to all sites of involvement would be the more usual approach.
76 Germinoma Because subependymal spread is common, such treatment logically would include the lateral, third, and fourth ventricles with a margin of 1 to 1.5 cm Better sparing can be achieved using CT planning and a four-field arrangement Better sparing can be achieved using CT planning and a four-field arrangement Results are excellent with a CSI dose as low as 21 Gy even in patients with leptomeningeal spread. The total dose to the primary site has typically been 40 to 45 Gy but probably can be reduced to 30 Gy in patients who have undergone complete resection or those who have been treated with a combined chemotherapy and adiotherapy regimen with a complete response to chemotherapy The total dose to the primary site has typically been 40 to 45 Gy but probably can be reduced to 30 Gy in patients who have undergone complete resection or those who have been treated with a combined chemotherapyâ radiotherapy regimen with a complete response to chemotherapy
77 Nongerminomatous Germ Cell Tumors For NGGCTs the diagnosis can be made in as many as one third of all patients on the basis of imaging findings (location, appearance) plus tumor markers.
78 .
79 teratomas Patients with mature teratomas without any associated malignant elements can be managed with surgery alone, while those with mature teratoma with germinomatous elements will be treated as germinomas the current standard of care therefore consists of platinum-based chemotherapy followed by radiotherapy There is controversy with respect to the radiotherapy target volume for NGGCT
80 NGGCT In the current North American study, CSI is used for all patients with NGGCT. A dose of 36 Gy is used, followed by a boost to the primary site to a total dose of 54 Gy Patients who have less than a complete response to chemotherapy: Second-look surgery may be useful to both exclude the possibility that the residual imaging abnormality represents mature teratoma and/or resect residual viable tumor, If the latter, this would be followed by CSI and then more aggressive chemotherapy, such as high-dose chemotherapy with stem cell rescue


81 Tumors of the. Sellar Region Craniopha ryngioma Xanthogr anuloma, Pituitary adenomas
82 Pituitary adenomas craniopharyngiomas are benign partly cystic epithelial tumors that arise in the sellar region from remnants of Rathke's pouch with a peak incidence between the ages of 5 and 14 years. In the majority of patients, craniopharyngiomas have both suprasellar and intrasellar components Children typically present with neuroendocrine deficits, especially diabetes insipidus and growth failure Visual-field deficits often go unnoticed initially patients with tumors that are smaller and/or subdiaphragmatic in location and without hypothalamic symptoms would be managed surgically, while other patients at higher risk for complications secondary to surgery would be managed with biopsy, cyst decompression, if necessary, and radiotherapy
83 Pituitary adenomas A lesion with a small solid component and a simple cyst, for example, may be treated with intracavitary injection of liquid radioactive material A lesion with a small solid component and a simple cyst, for example, may be treated with intracavitary injection of liquid radioactive material conventionally fractionated external-beam irradiation using modern techniques may be a better option with a lower risk of morbidity for all except very small tumors External-beam radiotherapy also will be the treatment of choice for patients with residual disease following surgery who are at high risk for progressive disease even relatively early following surgery or for those in whom surgical resection is not feasible.
84 Pituitary adenomas o A margin of 0.5 cm seems reasonable using contemporary planning and delivery techniques. o A dose of 54 to 55 Gy given in 30 daily fractions over 6 weeks appears to be necessary to achieve a high o A margin of 0.5 cm seems reasonable using contemporary planning and delivery techniques. A dose of 54 to 55 Gy given in 30 daily fractions over 6 weeks appears to be necessary to achieve a high, usually consisting of cyst decompression, is essential o When complete resection is not feasible, biopsy, subtotal resection, or simply cyst decompression followed by external-beam radiotherapy is a better choice o There is equal if not better probability of tumor control in this situation with a lower risk of potentially devastating sequelae than with â œheroicâ surgery, particularly in less-experienced hands.
85 Pituitary Adenomas Pituitary adenomas are rare in childhood Most are functioning adenomas that present with endocrine dysfunction, most often menstrual irregularities and galactorrhea in girls and delayed puberty in boys Transphenoidal surgery appears to be feasible and safe in children, even in those with poor pneumatization of the sphenoid sinus, using neuronavigational tools Radiotherapy is indicated if surgical resection is not possible or if hormone levels remain elevated following surgery Conformal fields with a margin of 0.5 cm beyond macroscopic residual disease (the GTV) are used The usual dose, as in the adult population, will be 45 to 50 Gy over 5 to 6 weeks
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Brain tumors: tumor types
 Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours. Colin Kennedy March 2015
 Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours Colin Kennedy March 2015 Glioma of the optic chiasm. T1-weighted MRI with gadolinium enhancement, showing intense irregular uptake of contrast. The
Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours Colin Kennedy March 2015 Glioma of the optic chiasm. T1-weighted MRI with gadolinium enhancement, showing intense irregular uptake of contrast. The
Supra- and infratentorial brain tumors from childhood to maternity
 Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM GERM CELL TUMOURS CNS Site Group Germ Cell Tumours Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM GERM CELL TUMOURS CNS Site Group Germ Cell Tumours Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
CHAPTER 11 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas
 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Adult Central Nervous System Tumors Treatment (PDQ )
") 1 di 20 28/06/2016 11.18 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
1 di 20 28/06/2016 11.18 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
Adult Brain and Spinal Cord Tumors
 Adult Brain and Spinal Cord Tumors An adult central nervous system (CNS) tumor is a disease in which abnormal cells form in the tissues of the brain and or the spinal cord. Major Parts of the Brain Anatomy
Adult Brain and Spinal Cord Tumors An adult central nervous system (CNS) tumor is a disease in which abnormal cells form in the tissues of the brain and or the spinal cord. Major Parts of the Brain Anatomy
Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management. Timothy M. George, MD, FACS, FAAP
 Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management Timothy M. George, MD, FACS, FAAP PEDIATRIC BRAIN TUMORS BACKGROUND: Incidence: Third most common pediatric tumor type (leukemia, neuroblastoma,
Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management Timothy M. George, MD, FACS, FAAP PEDIATRIC BRAIN TUMORS BACKGROUND: Incidence: Third most common pediatric tumor type (leukemia, neuroblastoma,
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Protocol for management of patients with pineal region tumours v1
 Protocol for management of patients with pineal region tumours v1 West Midlands Cancer Alliance Coversheet for Cancer Alliance Expert Advisory Group Agreed Documentation This sheet is to accompany all
Protocol for management of patients with pineal region tumours v1 West Midlands Cancer Alliance Coversheet for Cancer Alliance Expert Advisory Group Agreed Documentation This sheet is to accompany all
Childhood Brain and Spinal Cord Tumors Treatment Overview (PDQ )
") 1 di 14 27/11/2016 17.42 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
1 di 14 27/11/2016 17.42 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
We are IntechOpen, the first native scientific publisher of Open Access books. International authors and editors. Our authors are among the TOP 1%
 We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
SURGICAL MANAGEMENT OF BRAIN TUMORS
 SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
Case Report Tackling a Recurrent Pinealoblastoma
 Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Case Studies in Sella/Parasellar Region. Child thirsty, increased urination. Imaging. Suprasellar Germ Cell Tumor (Germinoma) No Disclosures
 No Disclosures") Case Studies in Sella/Parasellar Region No Disclosures 2018 Head and Neck Imaging Conference Child thirsty, increased urination Suprasellar Germ Cell Tumor (Germinoma) Midline Pineal >> Suprasellar > Other
Case Studies in Sella/Parasellar Region No Disclosures 2018 Head and Neck Imaging Conference Child thirsty, increased urination Suprasellar Germ Cell Tumor (Germinoma) Midline Pineal >> Suprasellar > Other
Financial Disclosures I have no financial interests to disclose. Templar Eye Foundation Oppenheimer Family Foundation
 Financial Disclosures I have no financial interests to disclose. Templar Eye Foundation Oppenheimer Family Foundation 2 Case 7 year old girl Initially parents noticed photophobia Then started to complain
Financial Disclosures I have no financial interests to disclose. Templar Eye Foundation Oppenheimer Family Foundation 2 Case 7 year old girl Initially parents noticed photophobia Then started to complain
Tumors of the Central Nervous System
 Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Aria Fallah MD, MSc, FRCSC
 Aria Fallah MD, MSc, FRCSC Department of Neurosurgery David Geffen School of Medicine at UCLA Pineal Region Tumors Brain Tumor Symposium August 22, 2015 Disclosures None Pineal Gland Arises from an invagination
Aria Fallah MD, MSc, FRCSC Department of Neurosurgery David Geffen School of Medicine at UCLA Pineal Region Tumors Brain Tumor Symposium August 22, 2015 Disclosures None Pineal Gland Arises from an invagination
Q&A. Fabulous Prizes. Collecting Cancer Data:CNS 2/7/12. NAACCR Webinar Series Collecting Cancer Data Central Nervous System
 Collecting Cancer Data Central Nervous System NAACCR 2012 2013 Webinar Series 2/7/2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data Central Nervous System NAACCR 2012 2013 Webinar Series 2/7/2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS
 Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Brain Tumor Treatment
 Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Scan for mobile link. Brain Tumor Treatment Brain Tumors Overview A brain tumor is a group of abnormal cells that grows in or around the brain. Tumors can directly destroy healthy brain cells. They can
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Year 2003 Paper two: Questions supplied by Tricia
 question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
Chapter 5 Section 3.1
 Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
Radiology Chapter 5 Section 3.1 Issue Date: March 27, 1991 Authority: 32 CFR 199.4(b)(2), (b)(2)(x), (c)(2)(viii), and (g)(15) 1.0 CPT 1 PROCEDURE CODES 37243, 61793, 61795, 77261-77421, 77427-77799, 0073T
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
Metastasis. 57 year old with progressive Headache and Right Sided Visual Loss
 Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Brain Tumors. What is a brain tumor?
 Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI)
 for Craniospinal Irradiation (CSI)") Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Brain Tumors. Medulloblastoma. Pilocytic astrocytoma: Ahmed Koriesh, MD. Pathological finding
 NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
Neuro-oncology Update Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013
 Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Neuro-oncology Update 2013 Andrew Kokkino, MD Medical Director, The Neurosciences Institute at Sacred Heart at Riverbend May 20, 2013 Case 1 58 year old man with recent facial droop and HA s Thin, cachectic
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Childhood Brain and Spinal Cord Tumors Treatment Overview (PDQ )
") 1 di 8 04/03/2017 07.31 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
1 di 8 04/03/2017 07.31 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
The Brain and Spinal Cord 33
 The Brain and Spinal Cord 33 shiao Y. Woo TOLERANCE OF THE CENTRAL NERVOUS SYSTEM TO IRRADIATION Postirradiation Cerebral Necrosis Postirradiation Myelopathy Other Late Effects CENTRAL NERVOUS SYSTEM NEOPLASMS
The Brain and Spinal Cord 33 shiao Y. Woo TOLERANCE OF THE CENTRAL NERVOUS SYSTEM TO IRRADIATION Postirradiation Cerebral Necrosis Postirradiation Myelopathy Other Late Effects CENTRAL NERVOUS SYSTEM NEOPLASMS
Neurosurgical Management of Brain Tumours. Nicholas Little Neurosurgeon RNSH
 Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Case 7391 Intraventricular Lesion
 Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Case 7391 Intraventricular Lesion Bastos Lima P1, Marques C1, Cabrita F2, Barbosa M2, Rebelo O3, Rio F1. 1Neuroradiology, 2Neurosurgery, 3Neuropathology, Coimbra University Hospitals, Portugal. University
Meningioma tumor. Meningiomas are named according to their location (Fig. 1) and cause various symptoms: > 1
 and cause various symptoms: > 1") Meningioma tumor Overview A meningioma is a type of tumor that grows from the protective membranes, called meninges, which surround the brain and spinal cord. Most meningiomas are benign (not cancer) and
Meningioma tumor Overview A meningioma is a type of tumor that grows from the protective membranes, called meninges, which surround the brain and spinal cord. Most meningiomas are benign (not cancer) and
Histopathological Study and Categorisation of Brain Tumors
 Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
What is Brain Cancer? What is the brain?
 What is Brain Cancer? The brain and spinal column make up the central nervous system (CNS), where all vital functions of the body are controlled. When tumors arise in the central nervous system, they are
What is Brain Cancer? The brain and spinal column make up the central nervous system (CNS), where all vital functions of the body are controlled. When tumors arise in the central nervous system, they are
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Childhood brain tumours
 Childhood brain tumours Our bodies are made up of billions of cells. Normally, these cells reproduce and repair themselves in a controlled way and do not cause us any problems. If for some reason this
Childhood brain tumours Our bodies are made up of billions of cells. Normally, these cells reproduce and repair themselves in a controlled way and do not cause us any problems. If for some reason this
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
EVIDENCE BASED MANAGEMENT FOR Paediatric Brain tumours
 EVIDENCE BASED MANAGEMENT FOR Paediatric Brain tumours In children, tumours of the central nervous system comprise 20% of all tumours and are second most common after leukaemia. Unlike adults, almost half
EVIDENCE BASED MANAGEMENT FOR Paediatric Brain tumours In children, tumours of the central nervous system comprise 20% of all tumours and are second most common after leukaemia. Unlike adults, almost half
Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas
 1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
1 Carol Boyd Comprehensive Case Study July 11, 2013 Evaluation of Three-dimensional Conformal Radiotherapy and Intensity Modulated Radiotherapy Techniques in High-Grade Gliomas Abstract: Introduction:
Intracranial AT RT / radiotherapy. Therapeutic dilemma / radiotherapy
 Therapeutic dilemma / radiotherapy Agressive tumour, poor outcome Past treatments based on MB concepts (RT CSA) MB Overall survival Mean age : 6.52 years n=36, 5 year 75% 1. Tumour occurs in the very young
Therapeutic dilemma / radiotherapy Agressive tumour, poor outcome Past treatments based on MB concepts (RT CSA) MB Overall survival Mean age : 6.52 years n=36, 5 year 75% 1. Tumour occurs in the very young
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
FOCUSING ON TUMORS. Ependymoma
 FOCUSING ON TUMORS Ependymoma A Word About ABTA Founded in 1973, the not-for-profit American Brain Tumor Association has a proud history of funding research, providing patient services, and educating people
FOCUSING ON TUMORS Ependymoma A Word About ABTA Founded in 1973, the not-for-profit American Brain Tumor Association has a proud history of funding research, providing patient services, and educating people
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for CNS Embryonal Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_cns_embryonal_tumors
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for CNS Embryonal Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_cns_embryonal_tumors
CS Tumor Size CS Extension CS Tumor Size/Ext Eval CS Lymph Nodes CS Lymph Nodes Eval Reg LN Pos Reg LN Exam CS Mets at DX CS Mets Eval
 C70.0, C71.0-C71.9 C70.0 Cerebral meninges C71.0 Cerebrum C71.1 Frontal lobe C71.2 Temporal lobe C71.3 Parietal lobe C71.4 Occipital lobe C71.5 Ventricle, NOS C71.6 Cerebellum, NOS C71.7 Brain stem C71.8
C70.0, C71.0-C71.9 C70.0 Cerebral meninges C71.0 Cerebrum C71.1 Frontal lobe C71.2 Temporal lobe C71.3 Parietal lobe C71.4 Occipital lobe C71.5 Ventricle, NOS C71.6 Cerebellum, NOS C71.7 Brain stem C71.8
BRAIN TUMORS IN INFANTS
 BRAIN TUMORS IN INFANTS Dr Sergio Valenzuela M.D-( ISPN-ESPN-FLANC)&cols. Head Pediatric Neurosurgery Unit I Instituto de NeurocirugiaAsenjo Santiago CHILE RATE OF MENINGEAL,BRAIN AND OTHER CNS MALIGNANT
BRAIN TUMORS IN INFANTS Dr Sergio Valenzuela M.D-( ISPN-ESPN-FLANC)&cols. Head Pediatric Neurosurgery Unit I Instituto de NeurocirugiaAsenjo Santiago CHILE RATE OF MENINGEAL,BRAIN AND OTHER CNS MALIGNANT
Neuroimaging Core Curriculum
 Neuroimaging Core Curriculum Program Content The purpose of the training program is to prepare the physician for the independent practice of neuroimaging. Neuroimaging is the subspecialty of Neurology
Neuroimaging Core Curriculum Program Content The purpose of the training program is to prepare the physician for the independent practice of neuroimaging. Neuroimaging is the subspecialty of Neurology
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions
 CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
Dr.Dafalla Ahmed Babiker Jazan University
 Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
The technique of craniospinal irradiation of paediatric patients in supine position
 The technique of craniospinal irradiation of paediatric patients in supine position Pavel Šlampa 1, Zuzana Seneklova 1, Jiri Simicek 1, Renata Soumarova 1, Petr Burkon 2, Ludmila Burianova 2 1 Masaryk
The technique of craniospinal irradiation of paediatric patients in supine position Pavel Šlampa 1, Zuzana Seneklova 1, Jiri Simicek 1, Renata Soumarova 1, Petr Burkon 2, Ludmila Burianova 2 1 Masaryk
Original Date: April 2016 Page 1 of 7 FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIATION THERAPY: STEREO RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: Please refer to pages 5-6 LCD
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
SPECIAL SLIDE SEMINAR CASE 3
 SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT. G. Tamburrini, Rome
 INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT G. Tamburrini, Rome Incidence 2% of occasional neuroradiological findings From clinical studies (1960 s): 0.4-1% of intracranial space occupying
INTRACRANIAL ARACHNOID CYSTS: CLASSIFICATION AND MANAGEMENT G. Tamburrini, Rome Incidence 2% of occasional neuroradiological findings From clinical studies (1960 s): 0.4-1% of intracranial space occupying
Complex Hydrocephalus
 2012 Hydrocephalus Association Conference Washington, DC - June 27-July1, 2012 Complex Hydrocephalus Marion L. Walker, MD Professor of Neurosurgery & Pediatrics Primary Children s Medical Center University
2012 Hydrocephalus Association Conference Washington, DC - June 27-July1, 2012 Complex Hydrocephalus Marion L. Walker, MD Professor of Neurosurgery & Pediatrics Primary Children s Medical Center University
Joana Ramalho, MD C. Ryan Miller, MD, PhD
 Joana Ramalho, MD C. Ryan Miller, MD, PhD Case 1 3 month old baby girl Presented with new onset of seizures Newborn. Questionable blurring of the gray-white junction within the right occipital lobe. Findings
Joana Ramalho, MD C. Ryan Miller, MD, PhD Case 1 3 month old baby girl Presented with new onset of seizures Newborn. Questionable blurring of the gray-white junction within the right occipital lobe. Findings
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Brain Tumors. Andrew J. Fabiano, MD FAANS. Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine
 Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
COG-ACNS1123: Phase 2 Trial of Response-Based Radiation Therapy for Patients with Localized Central Nervous System Germ Cell Tumors (CNS GCT)
") Page 1 of 6 COG-ACNS1123: Phase 2 Trial of Response-Based Radiation Therapy for Patients with Localized Central Nervous System Germ Cell Tumors (CNS GCT) FAST FACTS Eligibility Reviewed and Verified By
Page 1 of 6 COG-ACNS1123: Phase 2 Trial of Response-Based Radiation Therapy for Patients with Localized Central Nervous System Germ Cell Tumors (CNS GCT) FAST FACTS Eligibility Reviewed and Verified By
Brain tumors are, as a group, the most common
 See the corresponding editorial in this issue, pp 133 134. J Neurosurg Pediatrics 8:000 000, 8:135 148, 2011 Multidisciplinary management of childhood brain tumors: a review of outcomes, recent advances,
See the corresponding editorial in this issue, pp 133 134. J Neurosurg Pediatrics 8:000 000, 8:135 148, 2011 Multidisciplinary management of childhood brain tumors: a review of outcomes, recent advances,
Pediatric Spine Tumors (and other masses)
") Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
AMERICAN BRAIN TUMOR ASSOCIATION. Proton Therapy
 AMERICAN BRAIN TUMOR ASSOCIATION Proton Therapy ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit
AMERICAN BRAIN TUMOR ASSOCIATION Proton Therapy ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit
Cancer Management Chapter 23: Primary and metastatic brain tumors
 Cancer Management: A Multidisciplinary Approach, 12th Edition (2009). Cancer Management Chapter 23: Primary and metastatic brain tumors By Lisa M. DeAngelis, MD, Jay S. Loeffler, MD, and Adam N. Mamelak,
Cancer Management: A Multidisciplinary Approach, 12th Edition (2009). Cancer Management Chapter 23: Primary and metastatic brain tumors By Lisa M. DeAngelis, MD, Jay S. Loeffler, MD, and Adam N. Mamelak,
Pediatric low-grade glioma
 J Radiat Oncol (2013) 2:129 133 DOI 10.1007/s13566-012-0078-z REVIEW Pediatric low-grade glioma Anita Mahajan Received: 21 October 2012 / Accepted: 6 November 2012 / Published online: 19 November 2012
J Radiat Oncol (2013) 2:129 133 DOI 10.1007/s13566-012-0078-z REVIEW Pediatric low-grade glioma Anita Mahajan Received: 21 October 2012 / Accepted: 6 November 2012 / Published online: 19 November 2012
Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child
 Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Case Reports in Oncological Medicine Volume 2013, Article ID 815923, 4 pages http://dx.doi.org/10.1155/2013/815923 Case Report Atypical Presentation of Atypical Teratoid Rhabdoid Tumor in a Child Y. T.
Detection of Leptomeningeal CNS Metastases in Children
 Detection of Leptomeningeal CNS Metastases in Children Noah D. Sabin, M.D. Julie H. Harreld M.D. Kathleen J. Helton M.D. Zoltan Patay M.D., Ph.D. St. Jude Children s Research Hospital Memphis, TN Leptomeningeal
Detection of Leptomeningeal CNS Metastases in Children Noah D. Sabin, M.D. Julie H. Harreld M.D. Kathleen J. Helton M.D. Zoltan Patay M.D., Ph.D. St. Jude Children s Research Hospital Memphis, TN Leptomeningeal
ARRO Case: Diffuse Intrinsic Pontine Glioma
 ARRO Case: Diffuse Intrinsic Pontine Glioma Nicholas DeNunzio, MD, PhD (PGY-3) Faculty Advisor: Louis S. Constine, MD, FASTRO Department of Radiation Oncology University of Rochester Case Presentation
ARRO Case: Diffuse Intrinsic Pontine Glioma Nicholas DeNunzio, MD, PhD (PGY-3) Faculty Advisor: Louis S. Constine, MD, FASTRO Department of Radiation Oncology University of Rochester Case Presentation
STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER
 IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Original Article STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER Grishma P. Jobanputra Tutor, Department of Pathology, B.J. Medical College,
IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Original Article STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER Grishma P. Jobanputra Tutor, Department of Pathology, B.J. Medical College,
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA
 1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA QUESTIONS TO BE ADDRESSED: SUMMARY 1. What is the evidence for the clinical
1 EVIDENCE SUMMARY REPORT FOR PUBLIC CONSULTATION ONLY STEREOTACTIC RADIOSURGERY/ STEROTACTIC RADIOTHERAPY FOR PILOCYTIC ASTROCYTOMA QUESTIONS TO BE ADDRESSED: SUMMARY 1. What is the evidence for the clinical
Small and Big Operations: New Tools of the Trade for Brain Tumors. Disclosure. Incidence of Childhood Cancer
 Small and Big Operations: New Tools of the Trade for Brain Tumors Nalin Gupta MD PhD Chief, Division of Pediatric Neurosurgery Departments of Neurosurgery and Pediatrics University of California San Francisco
Small and Big Operations: New Tools of the Trade for Brain Tumors Nalin Gupta MD PhD Chief, Division of Pediatric Neurosurgery Departments of Neurosurgery and Pediatrics University of California San Francisco
Dosimetry, see MAGIC; Polymer gel dosimetry. Fiducial tracking, see CyberKnife radiosurgery
 Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Subject Index Acoustic neuroma, neurofibromatosis type 2 complications 103, 105 hearing outcomes 103, 105 outcome measures 101 patient selection 105 study design 101 tumor control 101 105 treatment options
Laurie A. Loevner, MD
 Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION. Mustafa Rashid Issa
 THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
Introduction. In adults, the commonest tumors are gliomas, metastases and meniongiomas; most lie in the supratentorial compartment
 Introduction Primary brain tumor 6 persons/100000/year Metastatic brain tumor 6 persons/100000/year 1 in 15 primary brain tumors occur in children under 15 years In adults, the commonest tumors are gliomas,
Introduction Primary brain tumor 6 persons/100000/year Metastatic brain tumor 6 persons/100000/year 1 in 15 primary brain tumors occur in children under 15 years In adults, the commonest tumors are gliomas,
Chemotherapy for Childhood Medulloblastoma and Primitive Neuroectodermal Tumors
 Chemotherapy for Childhood and Primitive Neuroectodermal Tumors ROGER J. PACKER, a JONATHAN L. FINLAY b a Department of Neurology, Children s National Medical Center, Washington DC, USA; b Departments
Chemotherapy for Childhood and Primitive Neuroectodermal Tumors ROGER J. PACKER, a JONATHAN L. FINLAY b a Department of Neurology, Children s National Medical Center, Washington DC, USA; b Departments
Childhood Central Nervous System Embryonal Tumors Treatment (PDQ )
") 1 di 18 06/07/2016 14.53 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
1 di 18 06/07/2016 14.53 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
about brain tumors a primer for patients and caregivers
 about brain tumors a primer for patients and caregivers brain about tumors a primer for patients and caregivers 8550 W. Bryn Mawr Avenue, Suite 550 Chicago, IL 60631 CareLine: - -ABTA ( ) Email: info@abta.org
about brain tumors a primer for patients and caregivers brain about tumors a primer for patients and caregivers 8550 W. Bryn Mawr Avenue, Suite 550 Chicago, IL 60631 CareLine: - -ABTA ( ) Email: info@abta.org