Pediatric Spine Tumors (and other masses)
|
|
|
- Gertrude Casey
- 5 years ago
- Views:
Transcription


1 Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle
2 Commercial disclosures None
3 Pediatric spine tumors the challenges Pediatric spine tumors can be challenging to clinicians because they often present with varied, nonspecific, and delayed symptoms. Pediatric spinal tumors can be challenging for pediatric radiologists because they are uncommon, heterogeneous, and imaging features can be nonspecific. Other spinal masses can mimic spine tumors on imaging.
4 Objectives To generate a differential diagnosis of spinal tumors based on location (intramedullary, intraduralextramedullary, extradural, and extradural/osseous) To describe imaging features of pediatric spinal tumors To review spinal masses that can mimic spine tumors

5 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
6 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
7 IA. Intramedullary pediatric spine tumors Astrocytoma Ependymoma Ganglioglioma Hemangioblastoma Incidence 60% 30% 5% <5% Age 10 years 14 years (NF2) 12 years (NF2) Location Eccentric in cord Central in cord Eccentric in cord Multiple levels 14 years (VHL) Eccentric in cord Imaging Infiltrative Most enhance T2 hyperintense Cysts WHO grade WHO I to IV (Pilocytic, fibrillary, anaplastic and GBM) Treatment Surgery with extent determined by tumor plane +/- Radiation, chemotherapy Well circumscribed Most enhance T2 hyperintense Hemorrhage Metastasis Variable Cysts T1 heterogeneous Calcification Lack of peritumoral edema WHO II to IV WHO 1 typically WHO I Surgery +/- Radiation Well circumscribed Robust Flow voids, hemorrhage Surgery Surgery Radiosurgery
8 IA. Intramedullary pediatric spine tumors Astrocytoma Ependymoma Ganglioglioma Hemangioblastoma Incidence 60% 30% 5% <5% Age 10 years 14 years (NF2) 12 years (NF2) Location Eccentric in cord Central in cord Eccentric in cord Multiple levels 14 years (VHL) Eccentric in cord Imaging Infiltrative Most enhance T2 hyperintense Cysts WHO grade WHO I to IV (Pilocytic, fibrillary, anaplastic and GBM) Treatment Surgery with extent determined by tumor plane +/- Radiation, chemotherapy Well circumscribed Most enhance T2 hyperintense Hemorrhage Metastasis Variable Cysts T1 heterogeneous Calcification Lack of peritumoral edema WHO II to IV WHO 1 typically WHO I Surgery +/- Radiation Well circumscribed Robust Flow voids, hemorrhage Surgery Surgery Radiosurgery
")


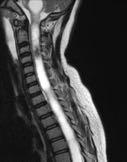
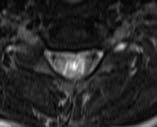
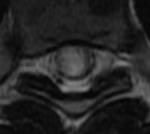
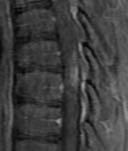
9 Pilocytic astrocytoma (WHO I) Case IA.1: Two-year-old girl with one month of abdominal pain and new torticollis. T2 T1+ ADC










10 Piloytic astrocytoma more examples Case IA.2 12 yo with syrinx T2 T2 T1 T1+ Case IA.3 15 yo with neck pain and abnormal sensation Case IA.4 2 yo with rapidly progressing scoliosis



11 Fibrillary astrocytoma (WHO II) Case IA.5: Thirteen-year-old boy with chronic neck and back pain. T2 T2 T1+



12 Glioblastoma (WHO IV) Case IA.6: Eight-year-old girl with one month of neck pain, torticollis and right hand numbness/weakness. T2 T1+ T1+










13 Glioblastoma more examples Case IA.7 2 yo with back pain and abnormal gait T2 T2 T1 T1+ Case IA.8 16 yo with back pain Case IA.9 15 yo with neck pain
14 IA. Intramedullary pediatric spine tumors Astrocytoma Ependymoma Ganglioglioma Hemangioblastoma Incidence 60% 30% 5% <5% Age 10 years 14 years (NF2) 12 years (NF2) Location Eccentric in cord Central in cord Eccentric in cord Multiple levels 14 years (VHL) Eccentric in cord Imaging Infiltrative Most enhance T2 hyperintense Cysts WHO grade WHO I to IV (Pilocytic, fibrillary, anaplastic and GBM) Treatment Surgery with extent determined by tumor plane +/- Radiation, chemotherapy Well circumscribed Most enhance T2 hyperintense Hemorrhage Metastasis Variable Cysts T1 heterogeneous Calcification Lack of peritumoral edema WHO II to IV WHO 1 typically WHO I Surgery +/- Radiation Well circumscribed Robust Flow voids, hemorrhage Surgery Surgery Radiosurgery



15 Ependymoma Case IA.10: Sixteen-year-old girl with back pain. T2 T1 T1+












16 Ependymoma more examples Case IA yo with back pain T2 T1 T1+ T1+ Case IA yo with neck pain Case IA yo with NF2
17 IA. Intramedullary pediatric spine tumors Astrocytoma Ependymoma Ganglioglioma Hemangioblastoma Incidence 60% 30% 5% <5% Age 10 years 14 years (NF2) 12 years (NF2) Location Eccentric in cord Central in cord Eccentric in cord Multiple levels 14 years (VHL) Eccentric in cord Imaging Infiltrative Most enhance T2 hyperintense Cysts WHO grade WHO I to IV (Pilocytic, fibrillary, anaplastic and GBM) Treatment Surgery with extent determined by tumor plane +/- Radiation, chemotherapy Well circumscribed Most enhance T2 hyperintense Hemorrhage Metastasis Variable Cysts T1 heterogeneous Calcification Lack of peritumoral edema WHO II to IV WHO 1 typically WHO I Surgery +/- Radiation Well circumscribed Robust Flow voids, hemorrhage Surgery Surgery Radiosurgery



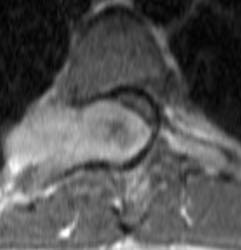
18 Ganglioglioma Case 1A.14: Seven-year-old girl with head tilt. T2 T1 T1+


19 Ganglioglioma follow-up Case 1A.14: Six years later
20 IA. Intramedullary pediatric spine tumors Astrocytoma Ependymoma Ganglioglioma Hemangioblastoma Incidence 60% 30% 5% <5% Age 10 years 14 years (NF2) 12 years (NF2) Location Eccentric in cord Central in cord Eccentric in cord Multiple levels 14 years (VHL) Eccentric in cord Imaging Infiltrative Most enhance T2 hyperintense Cysts WHO grade WHO I to IV (Pilocytic, fibrillary, anaplastic and GBM) Treatment Surgery with extent determined by tumor plane +/- Radiation, chemotherapy Well circumscribed Most enhance T2 hyperintense Hemorrhage Metastasis Variable Cysts T1 heterogeneous Calcification Lack of peritumoral edema WHO II to IV WHO 1 typically WHO I Surgery +/- Radiation Well circumscribed Robust Flow voids, hemorrhage Surgery Surgery Radiosurgery



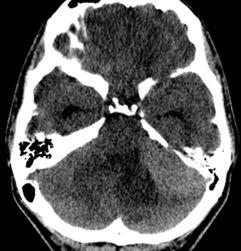
21 Hemangioblastoma Case 1A.15: 11-year-old girl with nausea, vomiting, and abnormal head CT. T2 T2 T1+
22 IA. Intramedullary pediatric spine tumors Astrocytoma Ependymoma Ganglioglioma Hemangioblastoma Incidence 60% 30% 5% <5% Age 10 years 14 years (NF2) 12 years (NF2) Location Eccentric in cord Central in cord Eccentric in cord Multiple levels 14 years (VHL) Eccentric in cord Imaging Infiltrative Most enhance T2 hyperintense Cysts WHO grade WHO I to IV (Pilocytic, fibrillary, anaplastic and GBM) Treatment Surgery with extent determined by tumor plane +/- Radiation, chemotherapy Well circumscribed Most enhance T2 hyperintense Hemorrhage Metastasis Variable Cysts T1 heterogeneous Calcification Lack of peritumoral edema WHO II to IV WHO 1 typically WHO I Surgery +/- Radiation Well circumscribed Robust Flow voids, hemorrhage Surgery Surgery Radiosurgery
23 IB. Intramedullary tumor mimics Case IB.1 Case IB.2 Case IB.3 T2 T2 Case IB.4 T2 T2



24 Intramedullary tumor mimics Case 1B.1: Six-year-old girl with neck and arm pain/weakness after trampoline injury. T2 Sag T1+ TWIST Intramedullary glomus arteriovenous malformation


25 Intramedullary tumor mimics Case 1B.2: Seventeen-year-old boy with remote history of craniospinal radiation for pineoblastoma. T2 T1 T1+ Radiation therapy-related cavernous malformation with acute hemorrhage



26 Intramedullary tumor mimics Case 1B.3: Twelve-year-old boy with rapid onset tetraplegia. T2 +5 days T2 +5 days T2 Spinal cord infarct (fibrocartilaginous embolism)



27 Intramedullary tumor mimics Case 1B.4: Five-year-old girl with acute left sided weakness. T2 +3 days T2 +3 days T1+ Longitudinally extensive transverse myelitis



28 IB. Intramedullary tumor mimics Case IB.1 AVM Case IB.2 Cavernous malformation Case IB.3 Spinal cord infarct T2 T2 Case IB.4 Transverse myelitis T2 T2
29 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
30 IIA. Intradural-extramedullary pediatric spine tumors Leptomeningeal metastasis Myxopapillary ependymoma Nerve sheath tumor Incidence Common 15% Uncommon Rare Demographic Various Adolescent Neurofibroma NF1 Schwannoma NF2 Imaging Nerve roots Nodular Enhancement (Can be intramedullary) Pathology Various Medulloblastoma Filum terminale T1 heterogeneous T2 hyperintense Avid WHO I Ependymoma subtype Highly vascular Neuroforamen T1 isointense T2 hyperintense Avid Neurofibroma - dark T2 center Schwannoma - cystic or fatty degeneration Most benign Neurofibroma NF1 Schwannoma NF2 Can be malignant Meningioma NF2 Prior radiation T1 and T2 isointense Avid Dural tail Cystic Clear-cell type more agressive Treatment Chemotherapy Radiation Surgery Recurrence and CSF dissemination Radiation Surgery Surgery
31 IIA. Intradural-extramedullary pediatric spine tumors Leptomeningeal metastasis Myxopapillary ependymoma Nerve sheath tumor Incidence Common 15% Uncommon Rare Demographic Various Adolescent Neurofibroma NF1 Schwannoma NF2 Imaging Nerve roots Nodular Enhancement (Can be intramedullary) Pathology Various Medulloblastoma Filum terminale T1 heterogeneous T2 hyperintense Avid WHO I Ependymoma subtype Highly vascular Neuroforamen T1 isointense T2 hyperintense Avid Neurofibroma - dark T2 center Schwannoma - cystic or fatty degeneration Most benign Neurofibroma NF1 Schwannoma NF2 Can be malignant Meningioma NF2 Prior radiation T1 and T2 isointense Avid Dural tail Cystic Clear-cell type more agressive Treatment Chemotherapy Radiation Surgery Recurrence and CSF dissemination Radiation Surgery Surgery



32 Leptomeningeal metastasis Case IIA.1: Five-year-old girl with lifelong history of vomiting. ADC T1+ T1+



33 Leptomeningeal metastasis - intramedullary Case IIA.2: Five-year-old girl with medulloblastoma. T1+ T1+ T1+



34 Leptomeningeal metastasis another example? Case IIA.3: Eight-year-old girl with developmental delay, worsening tremor, and abnormal gait. ADC T1+ T1+ NF2
35 IIA. Intradural-extramedullary pediatric spine tumors Leptomeningeal metastasis Myxopapillary ependymoma Nerve sheath tumor Incidence Common 15% Uncommon Rare Demographic Various Adolescent Neurofibroma NF1 Schwannoma NF2 Imaging Nerve roots Nodular Enhancement (Can be intramedullary) Pathology Various Medulloblastoma Filum terminale T1 heterogeneous T2 hyperintense Avid WHO I Ependymoma subtype Highly vascular Neuroforamen T1 isointense T2 hyperintense Avid Neurofibroma - dark T2 center Schwannoma - cystic or fatty degeneration Most benign Neurofibroma NF1 Schwannoma NF2 Can be malignant Meningioma NF2 Prior radiation T1 and T2 isointense Avid Dural tail Cystic Clear-cell type more agressive Treatment Chemotherapy Radiation Surgery Recurrence and CSF dissemination Radiation Surgery Surgery



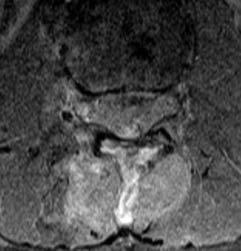
36 Myxopapillary ependymoma Case IIA.4: Fourteen-year-old boy with back pain. T2 T2 T1+












37 Myxopapillary ependymoma more examples Case IIA.5 15 yo with chronic back pain T2 T2 T1 T1+ Case IIA.6 15 yo with back pain and urinary retention after trauma Case IIA.7 17 yo with Chiari II and new twitching
38 IIA. Intradural-extramedullary pediatric spine tumors Leptomeningeal metastasis Myxopapillary ependymoma Nerve sheath tumor Incidence Common 15% Uncommon Rare Demographic Various Adolescent Neurofibroma NF1 Schwannoma NF2 Imaging Nerve roots Nodular Enhancement (Can be intramedullary) Pathology Various Medulloblastoma Filum terminale T1 heterogeneous T2 hyperintense Avid WHO I Ependymoma subtype Highly vascular Neuroforamen T1 isointense T2 hyperintense Avid Neurofibroma - dark T2 center Schwannoma - cystic or fatty degeneration Most benign Neurofibroma NF1 Schwannoma NF2 Can be malignant Meningioma NF2 Prior radiation T1 and T2 isointense Avid Dural tail Cystic Clear-cell type more agressive Treatment Chemotherapy Radiation Surgery Recurrence and CSF dissemination Radiation Surgery Surgery


39 Nerve sheath tumor schwannoma Case IIA.8: Thirteen-year-old girl with stumbling. T2 T2 T1+












40 Nerve sheath tumor more examples Case IIA.9 7 yo with back and hip pain after fall from horse T2 T2 T1 T1+ Case IIA yo with metastatic renal rhabdoid tumor with back pain Case IIA yo with NF2
41 IIA. Intradural-extramedullary pediatric spine tumors Leptomeningeal metastasis Myxopapillary ependymoma Nerve sheath tumor Incidence Common 15% Uncommon Rare Demographic Various Adolescent Neurofibroma NF1 Schwannoma NF2 Imaging Nerve roots Nodular Enhancement (Can be intramedullary) Pathology Various Medulloblastoma Filum terminale T1 heterogeneous T2 hyperintense Avid WHO I Ependymoma subtype Highly vascular Neuroforamen T1 isointense T2 hyperintense Avid Neurofibroma - dark T2 center Schwannoma - cystic or fatty degeneration Most benign Neurofibroma NF1 Schwannoma NF2 Can be malignant Meningioma NF2 Prior radiation T1 and T2 isointense Avid Dural tail Cystic Clear-cell type more agressive Treatment Chemotherapy Radiation Surgery Recurrence and CSF dissemination Radiation Surgery Surgery



42 Meningioma Case IIA.12: 20-year-old with NF2. T2 T1+ T1+
43 IIA. Intradural-extramedullary pediatric spine tumors Leptomeningeal metastasis Myxopapillary ependymoma Nerve sheath tumor Incidence Common 15% Uncommon Rare Demographic Various Adolescent Neurofibroma NF1 Schwannoma NF2 Imaging Nerve roots Nodular Enhancement (Can be intramedullary) Pathology Various Medulloblastoma Filum terminale T1 heterogeneous T2 hyperintense Avid WHO I Ependymoma subtype Highly vascular Neuroforamen T1 isointense T2 hyperintense Avid Neurofibroma - dark T2 center Schwannoma - cystic or fatty degeneration Most benign Neurofibroma NF1 Schwannoma NF2 Can be malignant Meningioma NF2 Prior radiation T1 and T2 isointense Avid Dural tail Cystic Clear-cell type more agressive Treatment Chemotherapy Radiation Surgery Recurrence and CSF dissemination Radiation Surgery Surgery
44 IIB. Intradural-extramedullary tumor mimics Case IIB.1 Case IIB.2 Case IIB.3 T1+ T1+ Case IIB.4 T1+ T2



45 IIB. Intradural-extramedullary tumor mimics Case IIB.1: 25-year-old male with new diagnosis medulloblastoma status post resection. CT T1 T1+ Post-operative subdural not metastasis




46 IIB. Intradural-extramedullary tumor mimics Case IIB.2: Four-year-old girl with abnormal gait for two weeks. T1 T1+ T1+ Chronic inflammatory demyelinating polyneuropathy not leptomeningeal metastasis



47 IIB. Intradural-extramedullary tumor mimics Case IIB.3: Seventeen-year-old boy with posterior fossa ependymoma and aspergillus infection. T2 T1+ T1+ Leptomeningeal aspergillosis fungal infection not dropped metastasis



48 IIB. Intradural-extramedullary tumor mimics Case IIB.4: Thirteen-year-old girl with leg weakness and hyperreflexia. T2 DWI T1+ Ventral neurenteric cyst


49 IIB. Intradural-extramedullary tumor mimics Case IIB.1 Post op subdural Case IIB.2 CIDP Case IIB.3 Fungal infection T1+ T1+ Case IIB.4 Neurenteric cyst T1+ T2
50 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
51 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
52 IIIA. Extradural pediatric spine tumors Neuroblastoma Incidence Relatively common Up to 15% develop spinal cord compression Myeloid sarcoma ( chloroma ) Relatively rare Demographic 1 to 5-years-old Patients with AML Imaging Large paraspinal soft tissue mass with intraspinal extension Mildly T2 hyperintense T2 hypointense areas may represent calcification Variable T1 isointense with homogeneous T2 hypointensity Pathology Neural crest cell origin Solid tumor of myelogenous stem cells Typically AML Treatment Chemotherapy Radiation Surgery Chemotherapy Radiation Surgery not usually necessary
53 IIIA. Extradural pediatric spine tumors Neuroblastoma Incidence Relatively common Up to 15% develop spinal cord compression Myeloid sarcoma ( chloroma ) Relatively rare Demographic 1 to 5-years-old Patients with AML Imaging Large paraspinal soft tissue mass with intraspinal extension Mildly T2 hyperintense T2 hypointense areas may represent calcification Variable T1 isointense with homogeneous T2 hypointensity Pathology Neural crest cell origin Solid tumor of myelogenous stem cells Typically AML Treatment Chemotherapy Radiation Surgery Chemotherapy Radiation Surgery not usually necessary


54 Neuroblastoma Case IIIA.1: Two-year-old girl unable to bear weight. T2 T2 T1+
55 IIIA. Extradural pediatric spine tumors Neuroblastoma Incidence Relatively common Up to 15% develop spinal cord compression Myeloid sarcoma ( chloroma ) Relatively rare Demographic 1 to 5-years-old Patients with AML Imaging Large paraspinal soft tissue mass with intraspinal extension Mildly T2 hyperintense T2 hypointense areas may represent calcification Variable T1 isointense with homogeneous T2 hypointensity Pathology Neural crest cell origin Solid tumor of myelogenous stem cells Typically AML Treatment Chemotherapy Radiation Surgery Chemotherapy Radiation Surgery not usually necessary



56 Meyloid sarcoma Case IIIA.2: Three-year-old boy with AML and worsening upper back pain. T2 T2 T1+
57 IIIA. Extradural pediatric spine tumors Neuroblastoma Incidence Relatively common Up to 15% develop spinal cord compression Myeloid sarcoma ( chloroma ) Relatively rare Demographic 1 to 5-years-old Patients with AML Imaging Large paraspinal soft tissue mass with intraspinal extension Mildly T2 hyperintense T2 hypointense areas may represent calcification Variable T1 isointense with homogeneous T2 hypointensity Pathology Neural crest cell origin Solid tumor of myelogenous stem cells Typically AML Treatment Chemotherapy Radiation Surgery Chemotherapy Radiation Surgery not usually necessary
58 IIIB. Extradural tumor mimics Case IIIB.1 Case IIIB.2 T2 T1+ T2



59 IIIB. Extradural tumor mimics Case IIIB.1: Two-year-old, follow up cystic lesion seen during evaluation for possible tethered cord. T2 T2 T1+ Epidural arachnoid cyst


60 IIIB. Extradural tumor mimics Case IIIB.2: Eleven-year-old girl with intermittent back pain awakening her at night with sudden worsening. T2 T1+ T1+ Venous vascular malformation with epidural hemorrhage


61 IIIB. Extradural tumor mimics Case IIIB.1 Arachnoid cyst Case IIIB.2 Venous vascular malformation T2 T1+ T2
62 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
63 IVA. Osseous pediatric spine tumors Ewing Sarcoma Langerhans cell histiocytosis (LCH) Incidence Relatively common Relatively uncommon Chordoma Rare Osteoblastoma (and osteoid osteoma) Relatively uncommon Demographic 5 to 13-years-old 1 to 3-years-old 10-years-old Male adolescent Imaging Osseous and/or extraosseous Permeative, lytic osseous lesion Soft tissue mass T1 and T2 iso to hypointense Variable Lytic lesion Vertebra plana Soft tissue component Heterogeneous Lytic, destructive lesion T2 hyperintense with septations Variable Soft tissue mass Focal sclerotic nidus Posterior spinal elements Marked edema / May have soft tissue component Pathology Neuroectodermal small round-cell sarcoma Dysregulated growth and activity of Langerhans cells Neoplastic? Arises from notochordal remants Highly vascular nidus of osteoid bone with surrounding reactive osteosclerosis Treatment Chemotherapy Radiation Surgery Conservative Chemotherapy Surgery Radiation Surgery Radiation Surgery NSAID RFA
64 IVA. Osseous pediatric spine tumors Ewing Sarcoma Langerhans cell histiocytosis (LCH) Incidence Relatively common Relatively uncommon Chordoma Rare Osteoblastoma (and osteoid osteoma) Relatively uncommon Demographic 5 to 13-years-old 1 to 3-years-old 10-years-old Male adolescent Imaging Osseous and/or extraosseous Permeative, lytic osseous lesion Soft tissue mass T1 and T2 iso to hypointense Variable Lytic lesion Vertebra plana Soft tissue component Heterogeneous Lytic, destructive lesion T2 hyperintense with septations Variable Soft tissue mass Focal sclerotic nidus Posterior spinal elements Marked edema / May have soft tissue component Pathology Neuroectodermal small round-cell sarcoma Dysregulated growth and activity of Langerhans cells Neoplastic? Arises from notochordal remants Highly vascular nidus of osteoid bone with surrounding reactive osteosclerosis Treatment Chemotherapy Radiation Surgery Conservative Chemotherapy Surgery Radiation Surgery Radiation Surgery NSAID RFA



65 Ewing sarcoma Case IVA.1: Thirteen-year-old boy with back pain after skateboarding injury with new numbness and weakness. T2 T1+ CT
66 IVA. Osseous pediatric spine tumors Ewing Sarcoma Langerhans cell histiocytosis (LCH) Incidence Relatively common Relatively uncommon Chordoma Rare Osteoblastoma (and osteoid osteoma) Relatively uncommon Demographic 5 to 13-years-old 1 to 3-years-old 10-years-old Male adolescent Imaging Osseous and/or extraosseous Permeative, lytic osseous lesion Soft tissue mass T1 and T2 iso to hypointense Variable Lytic lesion Vertebra plana Soft tissue component Heterogeneous Lytic, destructive lesion T2 hyperintense with septations Variable Soft tissue mass Focal sclerotic nidus Posterior spinal elements Marked edema / May have soft tissue component Pathology Neuroectodermal small round-cell sarcoma Dysregulated growth and activity of Langerhans cells Neoplastic? Arises from notochordal remants Highly vascular nidus of osteoid bone with surrounding reactive osteosclerosis Treatment Chemotherapy Radiation Surgery Conservative Chemotherapy Surgery Radiation Surgery Radiation Surgery NSAID RFA



67 Langerhans cell histiocytosis Case IVA.2: Two-year-old boy with torticollis. DX FLAIR T1+
68 IVA. Osseous pediatric spine tumors Ewing Sarcoma Langerhans cell histiocytosis (LCH) Incidence Relatively common Relatively uncommon Chordoma Rare Osteoblastoma (and osteoid osteoma) Relatively uncommon Demographic 5 to 13-years-old 1 to 3-years-old 10-years-old Male adolescent Imaging Osseous and/or extraosseous Permeative, lytic osseous lesion Soft tissue mass T1 and T2 iso to hypointense Variable Lytic lesion Vertebra plana Soft tissue component Heterogeneous Lytic, destructive lesion T2 hyperintense with septations Variable Soft tissue mass Focal sclerotic nidus Posterior spinal elements Marked edema / May have soft tissue component Pathology Neuroectodermal small round-cell sarcoma Dysregulated growth and activity of Langerhans cells Neoplastic? Arises from notochordal remants Highly vascular nidus of osteoid bone with surrounding reactive osteosclerosis Treatment Chemotherapy Radiation Surgery Conservative Chemotherapy Surgery Radiation Surgery Radiation Surgery NSAID RFA



69 Chordoma Case IVA.3: Eleven-year-old girl with right lower quadrant pain and spine abnormality on abdomen CT. CT STIR T1+
70 IVA. Osseous pediatric spine tumors Ewing Sarcoma Langerhans cell histiocytosis (LCH) Incidence Relatively common Relatively uncommon Chordoma Rare Osteoblastoma (and osteoid osteoma) Relatively uncommon Demographic 5 to 13-years-old 1 to 3-years-old 10-years-old Male adolescent Imaging Osseous and/or extraosseous Permeative, lytic osseous lesion Soft tissue mass T1 and T2 iso to hypointense Variable Lytic lesion Vertebra plana Soft tissue component Heterogeneous Lytic, destructive lesion T2 hyperintense with septations Variable Soft tissue mass Focal sclerotic nidus Posterior spinal elements Marked edema / May have soft tissue component Pathology Neuroectodermal small round-cell sarcoma Dysregulated growth and activity of Langerhans cells Neoplastic? Arises from notochordal remants Highly vascular nidus of osteoid bone with surrounding reactive osteosclerosis Treatment Chemotherapy Radiation Surgery Conservative Chemotherapy Surgery Radiation Surgery Radiation Surgery NSAID RFA



71 Osteoblastoma Case IVA.4: Twelve-year-old boy with back pain. CT STIR +2 years CT












72 Osteoblastoma more examples Case IVA.5 11 yo with back pain CT CT STIR T1+ Case IVA.6 9 yo with neck pain Case IVA.7 5 yo with neck pain
73 IVA. Osseous pediatric spine tumors Ewing Sarcoma Langerhans cell histiocytosis (LCH) Incidence Relatively common Relatively uncommon Chordoma Rare Osteoblastoma (and osteoid osteoma) Relatively uncommon Demographic 5 to 13-years-old 1 to 3-years-old 10-years-old Male adolescent Imaging Osseous and/or extraosseous Permeative, lytic osseous lesion Soft tissue mass T1 and T2 iso to hypointense Variable Lytic lesion Vertebra plana Soft tissue component Heterogeneous Lytic, destructive lesion T2 hyperintense with septations Variable Soft tissue mass Focal sclerotic nidus Posterior spinal elements Marked edema / May have soft tissue component Pathology Neuroectodermal small round-cell sarcoma Dysregulated growth and activity of Langerhans cells Neoplastic? Arises from notochordal remants Highly vascular nidus of osteoid bone with surrounding reactive osteosclerosis Treatment Chemotherapy Radiation Surgery Conservative Chemotherapy Surgery Radiation Surgery Radiation Surgery NSAID RFA
74 IVB. Osseous tumor mimics Case IVB.1 Case IVB.2 Case IVB.3 T1+ T1+ Case IVB.4 T2 CT



75 IVB. Osseous tumor mimics Case IVB.1: 11-year-old boy with history of back pain and new leg weakness. CT T2 T1+ Intraosseous low flow/venous malformation



76 IVB. Osseous tumor mimics Case IVB.2: Fourteen-year-old boy with history of tuberculosis. T2 T1+ CT Tuberculous discitis



77 IVB. Osseous tumor mimics Case IVB.3: Nine-year-old boy with history of choroid plexus carcinoma and neck pain. CT STIR T1+ Aneurysmal bone cyst



78 IVB. Osseous tumor mimics Case IVB.4: Seventeen-year-old girl with low back pain. STIR T1 CT Myositis ossificans


79 IVB. Osseous tumor mimics Case IVB.1 Intraosseous hemangioma / vascular malformation Case IVB.2 Tuberculous discitis Case IVB.3 Aneurysmal bone cyst T1+ T1+ Case IVB.4 Myositis ossificans T2 CT
80 Pediatric spine masses Key to differential diagnosis is to identify the location 35% 15% 20% I. Intramedullary II. Intradural-Extramedullary 30% III. Extradural IV. Extradural/Osseous
81 Takeaways Identify the location and extent of a spinal mass to determine the differential diagnosis Consider non-neoplastic causes of spinal masses
Spinal Neoplasms. First Things First!! Localize the Lesion!! Ependymomas. Common Intramedullary Lesions
 Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
1/9/2013 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE. Introduction. Classification for Extramedullary Tumors
 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
Imaging the Spinal Cord & Intradural Disease
 Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
A Journey Down The Canal
 A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
Spinal cord tumours Luc van den Hauwe et al.
 overview spinal cord tumours L. van den Hauwe 1,2, D. Balériaux 3, J.W. Van Goethem 2, C. Venstermans 2, F. De Belder 2, P.M. Parizel 2 introduction imaging spinal tumour classification spinal cord tumours
overview spinal cord tumours L. van den Hauwe 1,2, D. Balériaux 3, J.W. Van Goethem 2, C. Venstermans 2, F. De Belder 2, P.M. Parizel 2 introduction imaging spinal tumour classification spinal cord tumours
Kathleen R. Fink, MD Virginia Mason Medical Center. 6 th Nordic Emergency Radiology Course 2017
 Kathleen R. Fink, MD Virginia Mason Medical Center 6 th Nordic Emergency Radiology Course 2017 Disclosure My spouse receives research salary support from: Guerbet Outline Acute neck and back pain Acute
Kathleen R. Fink, MD Virginia Mason Medical Center 6 th Nordic Emergency Radiology Course 2017 Disclosure My spouse receives research salary support from: Guerbet Outline Acute neck and back pain Acute
Introduction to Neuroimaging spine. John J. McCormick MD
 Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Spine. Neuroradiology. Spine. Spine Pathology. Distribution of fractures. Radiological algorithm. Role of radiology 18/11/2015
 Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Vertebral and Paravertebral Diseases
 Department of Radiology University of California San Diego Vertebral and Paravertebral Diseases John R. Hesselink, M.D. Vertebral / Paravertebral Disease (Extradural) Metastatic disease Primary bone tumors
Department of Radiology University of California San Diego Vertebral and Paravertebral Diseases John R. Hesselink, M.D. Vertebral / Paravertebral Disease (Extradural) Metastatic disease Primary bone tumors
Ependymoma of the spine
 Ependymoma of the spine Tenny Zhang, MS-3 Harvard Medical School 1 Case presentation: history and exam HPI: A 30-year-old man with no significant past medical history presents with one week of bilateral
Ependymoma of the spine Tenny Zhang, MS-3 Harvard Medical School 1 Case presentation: history and exam HPI: A 30-year-old man with no significant past medical history presents with one week of bilateral
Patients Treated with Leksell Gamma Knife
 Patients Treated with Leksell Gamma Knife 1968-2016 TREATMENTS REPORTED 2016 BY REGION AND INDICATION INDICATION Asia excl. Europe Latin Middle East & Africa North Grand Total Benign Tumors 12283 9778
Patients Treated with Leksell Gamma Knife 1968-2016 TREATMENTS REPORTED 2016 BY REGION AND INDICATION INDICATION Asia excl. Europe Latin Middle East & Africa North Grand Total Benign Tumors 12283 9778
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Supra- and infratentorial brain tumors from childhood to maternity
 Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Posterior fossa tumors: clues to differential diagnosis with case-based review
 Posterior fossa tumors: clues to differential diagnosis with case-based review Poster No.: C-0323 Congress: ECR 2017 Type: Educational Exhibit Authors: H. A. Aboughalia, M. Abdelhady; Doha/QA Keywords:
Posterior fossa tumors: clues to differential diagnosis with case-based review Poster No.: C-0323 Congress: ECR 2017 Type: Educational Exhibit Authors: H. A. Aboughalia, M. Abdelhady; Doha/QA Keywords:
IMAGING OF A CASE OF SPINAL MENINGIOMA- A CASE REPORT
 IMAGING OF A CASE OF SPINAL MENINGIOMA- A CASE REPORT Ramneet Wadi 1, Anil Kumar Shukla 2, Seetha Pramila V. V 3, Sabyasachi Basu 4, Sonam Sanjay 5 1Postgraduate Student, Department of Radiodiagnosis,
IMAGING OF A CASE OF SPINAL MENINGIOMA- A CASE REPORT Ramneet Wadi 1, Anil Kumar Shukla 2, Seetha Pramila V. V 3, Sabyasachi Basu 4, Sonam Sanjay 5 1Postgraduate Student, Department of Radiodiagnosis,
Intradural spinal tumours and their mimics: a review of radiographic features
 Department of Radiology, Royal Melbourne Hospital, Parkville, Victoria, Australia Correspondence to Dr Sara Wein, Radiology Department, Royal Melbourne Hospital, Grattan Street, Parkville, VIC 3050, Australia;
Department of Radiology, Royal Melbourne Hospital, Parkville, Victoria, Australia Correspondence to Dr Sara Wein, Radiology Department, Royal Melbourne Hospital, Grattan Street, Parkville, VIC 3050, Australia;
NEURORADIOLOGY. Part III. Angela Csomor University of Szeged Department of Radiology
 NEURORADIOLOGY Part III Angela Csomor University of Szeged Department of Radiology DISEASES OF SPINE AND SPINAL CORD I. Non-tumourous diseases developmental anomalies vascular disorders inflammatory processes
NEURORADIOLOGY Part III Angela Csomor University of Szeged Department of Radiology DISEASES OF SPINE AND SPINAL CORD I. Non-tumourous diseases developmental anomalies vascular disorders inflammatory processes
Laurie A. Loevner, MD
 Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors and tumorlike lesions of the craniovertebral junction
 Tumors and tumorlike lesions of the craniovertebral junction Poster No.: C-2632 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: S.-C. Hung, Y. L. Chen, W.-Y. Guo, G.-M. Yang ; Taoyuan/
Tumors and tumorlike lesions of the craniovertebral junction Poster No.: C-2632 Congress: ECR 2010 Type: Educational Exhibit Topic: Neuro Authors: S.-C. Hung, Y. L. Chen, W.-Y. Guo, G.-M. Yang ; Taoyuan/
Pediatric back pain and diagnostic strategies
 ANDREA ROSSI, MD Department of Pediatric Neuroradiology G. Gaslini Children s Research Hospital Genoa Italy Pediatric back pain and diagnostic strategies Pediatric back pain: an underestimated problem
ANDREA ROSSI, MD Department of Pediatric Neuroradiology G. Gaslini Children s Research Hospital Genoa Italy Pediatric back pain and diagnostic strategies Pediatric back pain: an underestimated problem
RINGS N THINGS: Imaging Patterns in Differential Diagnosis. Anne G. Osborn, M.D.
 RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
Case Studies in the Skull Base
 Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Pediatric Spinal Anomalies
 Department of Radiology University of California San Diego Pediatric Spinal Anomalies John R. Hesselink, M.D. Spine Embryogenesis 1. Primitive streak 2. Proliferation of cells at primitive pit (Hensen's
Department of Radiology University of California San Diego Pediatric Spinal Anomalies John R. Hesselink, M.D. Spine Embryogenesis 1. Primitive streak 2. Proliferation of cells at primitive pit (Hensen's
11 May Disclosure. + Outline: Acute Spine Emergencies
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet K Fink Nordic
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet K Fink Nordic
Spinal Vascular Lesions
 Spinal Vascular Lesions Spinal Vascular Lesions Spinal cord infarction Hemangioblastoma Cavernous malformation Vascular malformations (Type 1-4) Spinal artery aneurysm Troy Hutchins, MD Assistant Professor
Spinal Vascular Lesions Spinal Vascular Lesions Spinal cord infarction Hemangioblastoma Cavernous malformation Vascular malformations (Type 1-4) Spinal artery aneurysm Troy Hutchins, MD Assistant Professor
Imaging of Sacral Masses: Self-Assessment Module
 1.5 CME AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Imaging of Sacral Masses: Self-Assessment Module Alice S. Ha 1, Felix S. Chew ABSTRACT The educational objectives for this self-assessment
1.5 CME AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Imaging of Sacral Masses: Self-Assessment Module Alice S. Ha 1, Felix S. Chew ABSTRACT The educational objectives for this self-assessment
4/14/2017. Unknown Case #1 Intramedullary Lesion
 4/14/2017 Intradural, Intramedullary Tumor or Mimic Intradural, Extramedullary Tumor or Mimic Extradural Tumor or Mimic Unknown Case #1 Intramedullary Lesion Unknown Case #1 -POST - MAG AXIAL Cranial Caudal
4/14/2017 Intradural, Intramedullary Tumor or Mimic Intradural, Extramedullary Tumor or Mimic Extradural Tumor or Mimic Unknown Case #1 Intramedullary Lesion Unknown Case #1 -POST - MAG AXIAL Cranial Caudal
Spine and spinal cord
 NEURORADIOLOGY Spine and spinal cord Erika Vörös University of Szeged Department of Radiology SZEGED DISEASES OF SPINE AND SPINAL CORD I. Non-tumourous diseases developmental anomalies vascular disorders
NEURORADIOLOGY Spine and spinal cord Erika Vörös University of Szeged Department of Radiology SZEGED DISEASES OF SPINE AND SPINAL CORD I. Non-tumourous diseases developmental anomalies vascular disorders
SHORT OVERVIEW OF SPINAL CORD TUMORS
 SHORT OVERVIEW OF SPINAL CORD TUMORS 1 INTRODUCTION RARE HETEROGENEOUS GROUP OF TUMORS. 15%OFALLPRIMARYCNSNEOPLASMSARISEINTHESC. INCIDENCE HIGHER IN MALES THAN FEMALES AGE 10TO40YRS MOST PRIMARIES ARE
SHORT OVERVIEW OF SPINAL CORD TUMORS 1 INTRODUCTION RARE HETEROGENEOUS GROUP OF TUMORS. 15%OFALLPRIMARYCNSNEOPLASMSARISEINTHESC. INCIDENCE HIGHER IN MALES THAN FEMALES AGE 10TO40YRS MOST PRIMARIES ARE
NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE
 THE UNIVERSITY OF NORTH CAROLINA at CHAPEL HILL SEPTEMBER 2013 NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE Claudia da Costa Leite, MD, PhD Thomas Bouldin, MD CASE 1 6 y-o female with headaches and vomiting
THE UNIVERSITY OF NORTH CAROLINA at CHAPEL HILL SEPTEMBER 2013 NEURORADIOLOGY-NEUROPATHOLOGY CONFERENCE Claudia da Costa Leite, MD, PhD Thomas Bouldin, MD CASE 1 6 y-o female with headaches and vomiting
Outline. Neuroradiology. Diffusion Imaging in. Clinical Applications of. Basics of Diffusion Imaging. Basics of Diffusion Imaging
 Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Clinical Applications of Diffusion Imaging in Neuroradiology No disclosures Stephen F. Kralik Assistant Professor of Radiology Indiana University School of Medicine Department of Radiology and Imaging
Role of Magnetic Resonance Imaging in the Evaluation of Compressive Myelopathy in Rohilkhand Region, India
 Mohit Agarwal et al Original article 10.5005/jp-journals-10050-10091 Role of Magnetic Resonance Imaging in the Evaluation of Compressive Myelopathy in Rohilkhand Region, India 1 Mohit Agarwal, 2 Pramod
Mohit Agarwal et al Original article 10.5005/jp-journals-10050-10091 Role of Magnetic Resonance Imaging in the Evaluation of Compressive Myelopathy in Rohilkhand Region, India 1 Mohit Agarwal, 2 Pramod
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Tumors and pseudotumors of the spine: a review of the main aspects in computed tomography and magnetic resonance imaging.
 Tumors and pseudotumors of the spine: a review of the main aspects in computed tomography and magnetic resonance imaging. Poster No.: C-1851 Congress: ECR 2012 Type: Educational Exhibit Authors: A. A.
Tumors and pseudotumors of the spine: a review of the main aspects in computed tomography and magnetic resonance imaging. Poster No.: C-1851 Congress: ECR 2012 Type: Educational Exhibit Authors: A. A.
ORIGINAL ARTICLE. Abstract. Aim. Materials and methods. Introduction. Results
 Is anatomical distribution helpful for differentiating TB spondylitis from neoplastic causes of extradural spinal cord compression in children? A pilot study Reena George, MD, MMed Rad, FRCR (UK) Savvas
Is anatomical distribution helpful for differentiating TB spondylitis from neoplastic causes of extradural spinal cord compression in children? A pilot study Reena George, MD, MMed Rad, FRCR (UK) Savvas
Paraspinal Venous Malformation Joseph Junewick, MD FACR
 Paraspinal Venous Malformation Joseph Junewick, MD FACR 06/04/2010 History 2 year old with history of fall. Rule out spinal injury. Diagnosis Paraspinal Venous Malformation Additional Clinical CT of the
Paraspinal Venous Malformation Joseph Junewick, MD FACR 06/04/2010 History 2 year old with history of fall. Rule out spinal injury. Diagnosis Paraspinal Venous Malformation Additional Clinical CT of the
SACRAL LESIONS: Differential diagnosis for the general radiologist
 SACRAL LESIONS: Differential diagnosis for the general radiologist Poster No.: C-2147 Congress: ECR 2017 Type: Educational Exhibit Authors: M. R. Campos Arenas, M. C. Sánchez-Porro, J. Garrido Rull ; 1
SACRAL LESIONS: Differential diagnosis for the general radiologist Poster No.: C-2147 Congress: ECR 2017 Type: Educational Exhibit Authors: M. R. Campos Arenas, M. C. Sánchez-Porro, J. Garrido Rull ; 1
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Tumors of the Central Nervous System
 Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Tumors of the Central Nervous System 1 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Introduction General: Brain tumors are lesions that have mass effect
Bone Tumors Clues and Cues
 William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
Small lesions involving scalp and skull in pediatric age.
 Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/ Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/ Keywords: Education and training, Education,
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
SMALL ROUND BLUE CELL LESION OF BONE
 DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
Metastasis. 57 year old with progressive Headache and Right Sided Visual Loss
 Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions
 CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
JMSCR Vol 04 Issue 04 Page April 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i4.13 Malignant Nerve Sheath Tumor with Secondary
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i4.13 Malignant Nerve Sheath Tumor with Secondary
Small lesions involving scalp and skull in pediatric age.
 Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/KR Keywords: Education and training, Education,
Small lesions involving scalp and skull in pediatric age. Poster No.: C-1149 Congress: ECR 2013 Type: Educational Exhibit Authors: M. J. Yi, J. H. Yoo; Seoul/KR Keywords: Education and training, Education,
AMSER Rad-Path Case of the Month January 2019
 AMSER Rad-Path Case of the Month January 2019 Intradural Spinal Tumor Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Dr. Matthew Hartman M.D., Allegheny Health Network Dr. David Oliver-Smith
AMSER Rad-Path Case of the Month January 2019 Intradural Spinal Tumor Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Dr. Matthew Hartman M.D., Allegheny Health Network Dr. David Oliver-Smith
Adult - Cerebrovascular. Adult - Cranio-Cervical Junction. Adult - Epilepsy. Adult - Hydrocephalus
 list for SET and IMG Neurosurgery Adult - Cerebrovascular Aneurysm - Clipping: Anterior circulation Aneurysm - Clipping: Posterior circulation AVM excision Carotid endarterectomy Carotid trapping Cavernoma
list for SET and IMG Neurosurgery Adult - Cerebrovascular Aneurysm - Clipping: Anterior circulation Aneurysm - Clipping: Posterior circulation AVM excision Carotid endarterectomy Carotid trapping Cavernoma
PITUITARY PARASELLAR LESIONS. Kim Learned, MD
 PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
Brain Tumors. Medulloblastoma. Pilocytic astrocytoma: Ahmed Koriesh, MD. Pathological finding
 NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
In-Training Examination for Diagnostic Radiology Residents Rationales
 28th Annual In-Training Examination for Diagnostic Radiology Residents Rationales Sponsored by: Commission on Education Committee on Residency Training in Diagnostic Radiology February 3, 2005 The American
28th Annual In-Training Examination for Diagnostic Radiology Residents Rationales Sponsored by: Commission on Education Committee on Residency Training in Diagnostic Radiology February 3, 2005 The American
Intradural and extradural dorsal spinal pediatric lesions
 Intradural and extradural dorsal spinal pediatric lesions Poster No.: C-2520 Congress: ECR 2015 Type: Educational Exhibit Authors: L. Riaza, M. Pérez Rubiralta, C. Perez Balagueró, M. Rebollo, 1 2 4 3
Intradural and extradural dorsal spinal pediatric lesions Poster No.: C-2520 Congress: ECR 2015 Type: Educational Exhibit Authors: L. Riaza, M. Pérez Rubiralta, C. Perez Balagueró, M. Rebollo, 1 2 4 3
Surgical Treatment of special Tumours. Winnie Achilles Tierklinik Hollabrunn Lastenstrasse Hollabrunn
 Surgical Treatment of special Tumours Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de Hepatocellular Tumours Hepatocellular Carcinoma, hepatocellular adenoma, and hepatoblastoma
Surgical Treatment of special Tumours Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de Hepatocellular Tumours Hepatocellular Carcinoma, hepatocellular adenoma, and hepatoblastoma
H Haloes cautions, 57 neurocytomas, perinuclear, 56 Headache blue cell tumors, 147 cautions, 135, 147, 152 clinical history, 132, 144, 148
 Index A ADC. See Apparent diffusion coefficient Adult. See also Supratentorial mass, adult cerebral tumor, 1 headache and ataxia cysts, mural nodules, 118 sporadic tumors, 118 headaches and visual changes,
Index A ADC. See Apparent diffusion coefficient Adult. See also Supratentorial mass, adult cerebral tumor, 1 headache and ataxia cysts, mural nodules, 118 sporadic tumors, 118 headaches and visual changes,
Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine
 Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine Christopher Ames MD Professor of Neurosurgery and Orthopedic Surgery Director of Spine Tumor And Deformity Surgery UCSF Department
Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine Christopher Ames MD Professor of Neurosurgery and Orthopedic Surgery Director of Spine Tumor And Deformity Surgery UCSF Department
IMAGING OF SPINE TUMORS
 IMAGING OF SPINE TUMORS Laszlo Mechtler, MD, FAAN, FASN SUMMARY Historic classification of spine tumors based on computed tomography myelopgraphy. (A) Normal, (B) extradural extramedullary, (C) intradural
IMAGING OF SPINE TUMORS Laszlo Mechtler, MD, FAAN, FASN SUMMARY Historic classification of spine tumors based on computed tomography myelopgraphy. (A) Normal, (B) extradural extramedullary, (C) intradural
Imaging of Hearing Loss
 Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Contemporary Imaging of Sensorineural Hearing Loss Imaging of Hearing Loss Discussion Outline (SNHL) Imaging Approaches Anatomic Relationships Lesions: SNHL KL Salzman, MD University of Utah School of
Brain tumors: tumor types
 Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Back pain in children presents less frequently than in
 Published November 19, 2009 as 10.3174/ajnr.A1832 REVIEW ARTICLE D.P. Rodriguez T.Y. Poussaint Imaging of Back Pain in Children SUMMARY: While back pain presents less frequently in children than in adults,
Published November 19, 2009 as 10.3174/ajnr.A1832 REVIEW ARTICLE D.P. Rodriguez T.Y. Poussaint Imaging of Back Pain in Children SUMMARY: While back pain presents less frequently in children than in adults,
A Comprehensive Review of Intraspinal tumors: Diagnostic, classification and radio-pathologic correlation.
 A Comprehensive Review of Intraspinal tumors: Diagnostic, classification and radio-pathologic correlation. Award: Magna Cum Laude Poster No.: C-2112 Congress: ECR 2013 Type: Educational Exhibit Authors:
A Comprehensive Review of Intraspinal tumors: Diagnostic, classification and radio-pathologic correlation. Award: Magna Cum Laude Poster No.: C-2112 Congress: ECR 2013 Type: Educational Exhibit Authors:
Masses of the Corpus Callosum
 Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Masses of the Corpus Callosum Kesav Raghavan, HMS Year III Dr. Agenda Corpus Callosum Development and Anatomy Our Patient: Clinical Presentation Differential Diagnosis of Masses in the Corpus Callosum
Case Studies in CPA/IAC
 Outline Case Studies in CPA/IAC Atul K Mallik MD PhD Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA Case based review of cerebellopontine
Outline Case Studies in CPA/IAC Atul K Mallik MD PhD Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA Case based review of cerebellopontine
Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions
 Original Research Article Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions Kalpesh Patel 1*, Siddharth Zala 2, C. Raychaudhuri 3 1 Assistant Professor, 2 1
Original Research Article Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions Kalpesh Patel 1*, Siddharth Zala 2, C. Raychaudhuri 3 1 Assistant Professor, 2 1
Spinal Imaging. Bearbeitet von Herwig Imhof. 1. Auflage Taschenbuch. 312 S. Paperback ISBN Format (B x L): 12,5 x 19 cm
: 12,5 x 19 cm") Spinal Imaging Bearbeitet von Herwig Imhof 1. Auflage 2007. Taschenbuch. 312 S. Paperback ISBN 978 3 13 144071 6 Format (B x L): 12,5 x 19 cm Weitere Fachgebiete > Medizin > Sonstige Medizinische Fachgebiete
Spinal Imaging Bearbeitet von Herwig Imhof 1. Auflage 2007. Taschenbuch. 312 S. Paperback ISBN 978 3 13 144071 6 Format (B x L): 12,5 x 19 cm Weitere Fachgebiete > Medizin > Sonstige Medizinische Fachgebiete
Role of MRI in the Evaluation of Compressive Myelopathy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 4 Ver. XIII (Apr. 2016), PP 21-26 www.iosrjournals.org Role of MRI in the Evaluation of Compressive
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 4 Ver. XIII (Apr. 2016), PP 21-26 www.iosrjournals.org Role of MRI in the Evaluation of Compressive
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
Extramedullary Spinal SOL Outcome of Surgery
 TAJ June 2009; Volume 22 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Original Article Extramedullary Spinal SOL Outcome of Surgery M Zahed Hossain 1, Monzurul Hoque 2 Abstract
TAJ June 2009; Volume 22 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Original Article Extramedullary Spinal SOL Outcome of Surgery M Zahed Hossain 1, Monzurul Hoque 2 Abstract
Spinal tumour: primary cervical extradural meningioma at an unusual location
 Case Report Spinal tumour: primary cervical extradural meningioma at an unusual location Ishita Pant 1, Vinod Kumar Singh Gautam 2, Rima Kumari 3, Sujata Chaturvedi 1 1 Department of Pathology, 2 Department
Case Report Spinal tumour: primary cervical extradural meningioma at an unusual location Ishita Pant 1, Vinod Kumar Singh Gautam 2, Rima Kumari 3, Sujata Chaturvedi 1 1 Department of Pathology, 2 Department
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED DISEASES OF CNS BRAIN Developmental anomalies Cerebrovascular disorders Tumours Inflammatory diseases Trauma DISEASES
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED DISEASES OF CNS BRAIN Developmental anomalies Cerebrovascular disorders Tumours Inflammatory diseases Trauma DISEASES
K-1 (Kyung Hee University, S )
") Case History K-1 (Kyung Hee University, S12-00829) A 17-year-old male presented with posterior neck pain and numbness in both upper extremities after a diving injury. He had no relevant medical history.
Case History K-1 (Kyung Hee University, S12-00829) A 17-year-old male presented with posterior neck pain and numbness in both upper extremities after a diving injury. He had no relevant medical history.
Magnetic Resonance Imaging of Intrinsic Spinal Cord Lesions: A Pictorial Review
 Magnetic Resonance Imaging of Intrinsic Spinal Cord Lesions: A Pictorial Review Award: Guerbet Best Registrar Exhibit Prize Poster No.: R-0024 Congress: RANZCR ASM 2013 Type: Educational Exhibit Authors:
Magnetic Resonance Imaging of Intrinsic Spinal Cord Lesions: A Pictorial Review Award: Guerbet Best Registrar Exhibit Prize Poster No.: R-0024 Congress: RANZCR ASM 2013 Type: Educational Exhibit Authors:
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
MRI XR, CT, NM. Principal Modality (2): Case Report # 2. Date accepted: 15 March 2013
: Case Report # 2. Date accepted: 15 March 2013") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
CLIC Sargent Eligibility Criteria
 1 Eligibility Criteria DOCUMENT GOVERNANCE: Eligibility criteria Produced by J. Hawkins & Grants Team Sponsored by Dara de Burca Version Approval by Executive Team 10 th June 2014 Board of Trustees 3 rd
1 Eligibility Criteria DOCUMENT GOVERNANCE: Eligibility criteria Produced by J. Hawkins & Grants Team Sponsored by Dara de Burca Version Approval by Executive Team 10 th June 2014 Board of Trustees 3 rd
A Comprehensive Review of Intraspinal tumors: Diagnostic, classification and radio-pathologic correlation.
 A Comprehensive Review of Intraspinal tumors: Diagnostic, classification and radio-pathologic correlation. Award: Magna Cum Laude Poster No.: C-2112 Congress: ECR 2013 Type: Educational Exhibit Authors:
A Comprehensive Review of Intraspinal tumors: Diagnostic, classification and radio-pathologic correlation. Award: Magna Cum Laude Poster No.: C-2112 Congress: ECR 2013 Type: Educational Exhibit Authors:
NEURORADIOLOGY DIL part 5
 NEURORADIOLOGY DIL part 5 Masses and tumors K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL part
NEURORADIOLOGY DIL part 5 Masses and tumors K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL part
MARK D. MURPHEY MD, FACR. Physician-in-Chief, AIRP. Chief, Musculoskeletal Imaging
 ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
Adult Brain Tumours: an approach based on imaging findings
 Adult Brain Tumours: an approach based on imaging findings Robert J Sevick, MD, FRCPC, FACR Professor, Radiology and Clinical Neurosciences Cumming School of Medicine University of Calgary Learning objectives:
Adult Brain Tumours: an approach based on imaging findings Robert J Sevick, MD, FRCPC, FACR Professor, Radiology and Clinical Neurosciences Cumming School of Medicine University of Calgary Learning objectives:
Disclosures. Posterior Fossa Masses. I m from the Government. and I here to help! Differential Diagnosis
 Posterior Fossa Masses Differential Diagnosis James G. Smirniotopoulos, M.D. Radiology, Neurology, Biomedical Informatics Uniformed Services University Bethesda, Maryland http://rad.usuhs.edu http://medpix.usuhs.edu
Posterior Fossa Masses Differential Diagnosis James G. Smirniotopoulos, M.D. Radiology, Neurology, Biomedical Informatics Uniformed Services University Bethesda, Maryland http://rad.usuhs.edu http://medpix.usuhs.edu
Mark D. Murphey, MD, FACR
 Fundamental Concepts of Musculoskeletal Neoplasm: CT and MRI Mark D. Murphey, MD, FACR Important Features in Evaluation of Musculoskeletal Masses Differential diagnosis Preoperative assessment and staging
Fundamental Concepts of Musculoskeletal Neoplasm: CT and MRI Mark D. Murphey, MD, FACR Important Features in Evaluation of Musculoskeletal Masses Differential diagnosis Preoperative assessment and staging
Neuroimaging Core Curriculum
 Neuroimaging Core Curriculum Program Content The purpose of the training program is to prepare the physician for the independent practice of neuroimaging. Neuroimaging is the subspecialty of Neurology
Neuroimaging Core Curriculum Program Content The purpose of the training program is to prepare the physician for the independent practice of neuroimaging. Neuroimaging is the subspecialty of Neurology
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Pediatric Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Pediatric Neurosurgery Pediatric neurosurgeons
Introduction to Neurosurgical Subspecialties: Pediatric Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Pediatric Neurosurgery Pediatric neurosurgeons
Sacral bone Tumor Imaging
 Sacral bone Tumor Imaging Poster No.: C-1651 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Zaouali, M. Ben Ammar, A. DAGHFOUS, M. Matri, L. REZGUI; tunis/tn Keywords: Bones, Oncology, Neuroradiology
Sacral bone Tumor Imaging Poster No.: C-1651 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Zaouali, M. Ben Ammar, A. DAGHFOUS, M. Matri, L. REZGUI; tunis/tn Keywords: Bones, Oncology, Neuroradiology
The role of CT and MRI in evaluation of Osteoid Oteoma
 The role of CT and MRI in evaluation of Osteoid Oteoma Elene Iordanishvili Tbilisi Sate Medical University Instructor: Prof. Dr. Ketevan Kotetishvili Department of Physics Georgian Technical University
The role of CT and MRI in evaluation of Osteoid Oteoma Elene Iordanishvili Tbilisi Sate Medical University Instructor: Prof. Dr. Ketevan Kotetishvili Department of Physics Georgian Technical University
Neurosurgery. Neurosurgery
 Neurosurgery Neurosurgery Neurosurgery Telephone Numbers: Appointment: 202-476-3020 Fax: 202-476-3091 Administration: 202-476-3020 Evenings and Weekends: 202-476-5000 Robert Keating, MD, Chief The Division
Neurosurgery Neurosurgery Neurosurgery Telephone Numbers: Appointment: 202-476-3020 Fax: 202-476-3091 Administration: 202-476-3020 Evenings and Weekends: 202-476-5000 Robert Keating, MD, Chief The Division
Essentials of Clinical MR, 2 nd edition. 65. Benign Hepatic Masses
 65. Benign Hepatic Masses Pulse sequences acquired for abdominal MRI typically consist of fast acquisition schemes such as single-shot turbo spin echo (i.e. HASTE) and gradient echo schemes such as FLASH
65. Benign Hepatic Masses Pulse sequences acquired for abdominal MRI typically consist of fast acquisition schemes such as single-shot turbo spin echo (i.e. HASTE) and gradient echo schemes such as FLASH
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal,
 Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
Magnetic resonance imaging of intramedullary spinal cord lesions
 Magnetic resonance imaging of intramedullary spinal cord lesions Poster No.: C-1762 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Abdelkafi, H. Derbel, H. Abid, S. Haddar, B. Souissi, N. 1 1
Magnetic resonance imaging of intramedullary spinal cord lesions Poster No.: C-1762 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Abdelkafi, H. Derbel, H. Abid, S. Haddar, B. Souissi, N. 1 1
A Patient s Guide to Spinal Tumors
 A Patient s Guide to Spinal Tumors 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Spinal Tumors 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma
 AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
MAGNETIC RESONANCE IMAGING OF SPINAL TUMORS
 MAGNETIC RESONANCE IMAGING OF SPINAL TUMORS A study using a 0.3 T vertical magnetic field MING HUA LI - HEXL- Lund 992 Organization LUND UNIVERSITY Department of Radiology University Hospital S-22 85 Lund,
MAGNETIC RESONANCE IMAGING OF SPINAL TUMORS A study using a 0.3 T vertical magnetic field MING HUA LI - HEXL- Lund 992 Organization LUND UNIVERSITY Department of Radiology University Hospital S-22 85 Lund,
ASJ. Myxopapillary Ependymoma of the Cauda Equina in a 5-Year-Old Boy. Asian Spine Journal. Introduction
 Asian Spine Journal 846 Masashi Case Uehara Report et al. Asian Spine J 2014;8(6):846-851 http://dx.doi.org/10.4184/asj.2014.8.6.846 Asian Spine J 2014;8(6):846-851 Myxopapillary Ependymoma of the Cauda
Asian Spine Journal 846 Masashi Case Uehara Report et al. Asian Spine J 2014;8(6):846-851 http://dx.doi.org/10.4184/asj.2014.8.6.846 Asian Spine J 2014;8(6):846-851 Myxopapillary Ependymoma of the Cauda